PIXHOOK/iSTOCK. 40 l Nursing2014 l January. Copyright 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
|
|
|
- Duane Bradley
- 6 years ago
- Views:
Transcription









1 PIXHOOK/iSTOCK 40 l Nursing2014 l January
2 2.3 ANCC CONTACT HOURS Chest X-ray interpretation NOT JUST BLACK AND WHITE By William Pezzotti, MSN, RN, ACNP-BC, CEN CHEST X-RAYS (CXRs) are one of the oldest noninvasive methods for identifying abnormalities in the chest. Even though healthcare providers prescribe CXRs and interpret the results, nurses are often the first to read the radiologist s report and provide the interpretation to the attending physician or a designate. 1 In many hospital systems across the United States, nurses who work in the ICU or ED routinely implement specific standing orders, including obtaining a CXR for an unexpected issue such as chest pain, respiratory distress, unexplained hypoxemia, or unequal breath sounds. 1 This article reviews how to recognize basic normal anatomy and life-threatening abnormalities on a CXR. Understanding CXRs X-rays are short wavelengths of electromagnetic radiation that penetrate matter. 2 They re basically photographs, but instead of light they use radiation to provide contrast. The amount of radiation that X-rays produce is very small (0.2 millisieverts, or msv; this unit belongs to the same family as the liter and kilogram) and cause only % of fatal cancers in the United States. 3,4 Evaluating a CXR is a skill that requires careful observation and a good understanding of chest anatomy. 4 (See Structures of the lung.) The technique used to obtain the CXR determines its overall quality. Two of the most common views used in the acute care setting are posteroanterior (PA) and anteroposterior (AP), or frontal views of the chest. 2 For PA January l Nursing2014 l 41

3 views, the X-ray beam passes through the chest from the back to the front. The patient must stand while this CXR is taken. In AP views, the beam passes through the chest from the front to the back. Portable CXRs should generally be reserved for acutely ill patients and others who can t stand. 2 Portable CXRs performed at the patient s bedside are AP views. 2,4 A major disadvantage of an AP view is that the structures in the anterior part of the chest, including the heart, look bigger because of magnification. This could lead to an incorrect diagnosis of cardiomegaly. 4 A lateral view may reveal lesions behind the heart, near the mediastinum, or near the diaphragm. The frontal and lateral views provide a three-dimensional view of the chest and let the clinician localize infiltrates or other lesions that might otherwise be difficult to find. 2 CXRs should always be taken during maximum inspiration to allow visualization of any pulmonary abnormalities. 5 When the patient inspires deeply, the diaphragm should be seen at the segment of the 6th rib anteriorly. 6 If 10 posterior ribs can be counted above the diaphragm, it s an excellent inspiratory CXR. If fewer than 10 ribs can be counted above the diaphragm, it s either poor inspiratory effort or a sign of low lung volume. 2 The right hemidiaphragm is usually higher than the left because of the location of the liver. Poor inspiratory effort can cause the CXR to appear whiter, with increased lung markings, and can also give a false impression that a lower lobe pneumonia is present. 3 Penetrating issues X-rays distinguish objects based on relative densities. The four basic densities on a CXR are bone (or metal), water (soft tissue), fat, and gas (air). 2,7 Bone/metal density appears all white, or completely radiopaque, as do bullets, coins, ECG electrodes, and pacemakers. 5,8 Water (soft tissue) density looks white to gray on the CXR. The heart, liver, diaphragm, spleen, and blood vessels will also cause this appearance. This is largely because the organs are the same density as water. 8 In erect CXRs, fluid can often be seen collecting at the lung bases and appear as dense opacities blocking adjacent structures in the chest cavity. 5 This is the most common location of pleural effusions on a CXR. Fat appears gray. This tissue is less dense than bone/metal but more dense than air and is most often seen in CXRs involving the breasts and fat pads. Gas (air) density is black, or radiolucent, and is seen on review of Structures of the lung The main lung structures as seen in an anterior view; the carina is at the bifurcation of the right and left mainstem bronchi. Right main bronchus Right superior lobe bronchus Superior lobe Middle lobe Right middle lobe bronchus Left mainstem bronchus Left pulmonary artery Left pulmonary veins Right inferior lobe bronchus Inferior lobe Right Left 42 l Nursing2014 l January

4 the lungs, trachea, bronchi, and alveoli. 5 Air tends to rise to the highest point in the chest cavity, so a pneumothorax is most commonly seen at the lung apices when the patient is erect. 5 The penetration of a CXR is affected by the duration of exposure and the power of the beam. A poorly penetrated CXR looks light and soft tissue structures are hard to see, especially those behind the heart. An overpenetrated CXR looks dark and lung markings are hard to see. 9 When a CXR has good penetration, the lower thoracic vertebral bodies can be seen through the heart. 10 Chest X-ray interpretation Recognizing normal anatomy on the CXR is key to understanding and interpreting abnormalities. Before interpreting a CXR, identify the patient by first and last name and date of birth. Verify that you have the correct X-ray taken on the correct date and identify the view of the CXR. Most facilities now use a digital image instead of photographic film contained in a cassette. These digital images are stored on a picture archiving and communication system (PACS). Images from the PACS can be viewed at any computer workstation, and they can be manipulated to change brightness or magnify images. 2 Make it a habit to always view the CXR as if the patient is facing you; the right side of the CXR is the patient s left side, and vice versa. 2,4 Next, determine the quality of the CXR. Is there good penetration? If so, the thoracic vertebral bodies will be visible. Is there good inspiration? Remember to count the ribs. Determine rotation by measuring the distance from the medial end of each clavicle to the spinous process of the vertebrae at the same level. These distances should be equal. 4 Anterior structures on a CXR are the right and left heart borders, the ascending aorta, bilateral upper lung lobes, and the middle lobe of the right lung. 8 Posterior structures are the descending aorta, hemidiaphragms, and both lower lung lobes. 8 Review all aspects of the CXR by using the ABCDEF approach. 1 A: Airway Always look at the trachea and assess if it s midline or shifted to the right or left. The trachea should be midline but may shift slightly to the right around the aortic notch. 8 If the trachea is shifted or deviated, it may indicate improper patient positioning, thyroid enlargement, or a tension pneumothorax. 4,6 Next, examine the carina (the area where the trachea bifurcates into the right and left bronchi). It should lie between T4 and T6. If the patient is endotracheally intubated, examine the CXR for correct tube placement. The endotracheal tube (ETT) is correctly placed when the tip of the ETT is 3 to 5 cm (approximately 2 in) above the carina. 4 B: Bones When looking at the bones on a CXR, pay close attention to the clavicles, ribs, scapulae, and vertebrae, and assess for any fractures. Sometimes turning the CXR on its side can help make rib fractures easier to see. 8 On a CXR with maximum inspiration, expect to see 9 to 10 posterior ribs. 2 In order to tell the difference between anterior and posterior ribs on the CXR, remember that posterior ribs slope downward to form the Visualizing the diaphragm The right hemidiaphragm should be higher than the left by about 3 cm because of the liver. The outline of the diaphragm should be smooth. costovertebral angle. The anterior ribs appear more horizontal. 4 When reviewing the ribs and other bones, examine the intercostal spaces for symmetry. Remember that each intercostal space is numbered according to the rib above it. Widened intercostal spaces may be associated with hyperinflation of the lungs. 2 C: Circulation Examine the heart for normal size and shape. One of the easiest observations to make is the cardiothoracic ratio: the widest horizontal width of the heart compared to the widest width of the thorax. 8 The heart should be 50% the size of the thorax. Anything greater than 50% suggests cardiomegaly or a possible pericardial effusion. 4 Also examine the mediastinum. Its borders should be clear, although some haziness may be present at the January l Nursing2014 l 43
5 angle between the heart and diaphragm. 1,8 If the mediastinum appears enlarged, consider disorders that could cause this, such as an aortic aneurysm. 5 D: Diaphragm The diaphragm is dome-shaped and has the same density as water. The right hemidiaphragm should be higher than the left because of the liver. (See Visualizing the diaphragm.) The difference should be only about 3 cm. The outline of the diaphragm should be smooth. 8 Diaphragmatic elevation occurs when fewer than 10 ribs are visible and can be caused by atelectasis, abdominal distension, and phrenic nerve compression. 2 Diaphragmatic depression is often present when 11 or 12 ribs are visible. A depressed or flattened diaphragm is often seen in patients who have chronic obstructive pulmonary disease (COPD) or a pneumothorax. 1,2 Below the left hemidiaphragm, the gastric air bubble is visible. Absence of a gastric bubble could indicate a hiatal hernia. 5 E: Edges Inspect the lung borders (edges) for fluid or air collection. Look specifically at the costophrenic angles, which should have well-defined acute angles. 8 A pneumothorax, hemothorax, or pleural effusion can distort the normal lung edges or borders. 5 F: Fields The lung fields consist mainly of air and very little tissue or blood. 2,6 Remember normal lung anatomy, including the location of the lobes, when reviewing CXRs. 2 Keep in mind that many patients who are erect or semierect for the CXR and have fluid accumulation will have abnormal fluid accumulation at the lung bases. If the CXR is taken with the patient in supine position, fluid tends to settle in the lower lobes posteriorly. 5 The lung fields should be of equal density; one shouldn t be lighter or darker than the other on a normal CXR. Remember that the lungs are divided into lobes by fissures. The right lung has three lobes and the left lung has two lobes. Try to find the horizontal fissure of the right lung when looking at the CXR. A fissure is a space between the lung lobes that looks like a narrow white line on a CXR. 2 This fissure, which can be difficult to visualize, is seen in 50% to 60% of patients. 5,8 It should extend from the right hilum to the 6th rib in the axillary line. The hilum is a triangular area above and behind the cardiac border where the structures that form the root of the lung, such as the pulmonary artery and lymphatic vessels, enter and leave the lung. 1 A displaced fissure may indicate pneumothorax. 8 Locating devices on a CXR 4 Device Proper location on CXR ET tube Chest tubes Nasogastric tube Dobhoff feeding tube Central venous catheter and peripherally inserted central catheter Temporary double-lumen hemodialysis catheter Pulmonary artery catheter Intra-aortic balloon pump Temporary single-lead transvenous pacemaker Implantable cardioverter defibrillator 3 to 5 cm (1.18 to 1.97 in) above the carina All openings of the chest tube are inside the chest wall; tube tip placed anteriorly and superiorly for air (pneumothorax); posteriorly and inferiorly for fluids (pleural effusion) Below the diaphragm with tip and side holes 10 cm (3.94 in) into the stomach Tip should be in the duodenum (confirmed with abdominal X-ray) Tip should be in the superior vena cava, above the right atrium Tip should be in the superior vena cava Tip should be in the proximal left or right pulmonary artery about 2 cm (0.79 in) from hilum Tip should be in the descending aorta, distal to the origin of the left subclavian artery Tip is usually located in the apex of the right ventricle Leads should be in the superior vena cava or brachiocephalic vein, and the apex of the right ventricle 44 l Nursing2014 l January
 Common abnormalities The following disorders are commonly seen in acute care settings and may be visible on CXRs.")
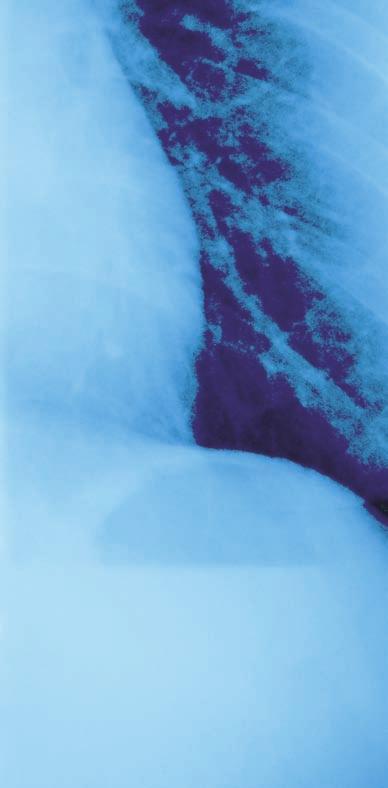
6 Once the CXR has been reviewed in a systematic fashion, examine the CXR for devices such as catheters, tubes, drains, or wires. Get into the habit of checking their position. (See Locating devices on a CXR.) Common abnormalities The following disorders are commonly seen in acute care settings and may be visible on CXRs. Pleural effusions are excess fluid collections in the pleural space. In order for a pleural effusion to be visible on a CXR, approximately 200 to 400 ml must be present. A clue that a pleural effusion is present is blunting of the costophrenic angle. 1 A right-sided pleural effusion is often associated with heart failure. 5 However, bilateral pleural effusions are present in 70% of patients with congestive heart failure (CHF). 9 Pulmonary edema is the most common pattern of diffuse lung disease in patients with CHF. 1,6 A diffuse lung disease pattern will always involve both lungs but may involve only part of each lung. Acute pulmonary edema is the rapid collection of an abnormal amount of fluid in the alveoli or pulmonary interstitial spaces. 1 As the amount of fluid increases in the alveoli, the fluid can cause a butterfly or batwing pattern to appear on the CXR. This pattern causes the central or perihilar area of the lungs to appear white. If this process goes unnoticed and progresses, the image on CXR will look like ground glass. 1,2 A ground-glass appearance may indicate overhydration, heart failure, aspiration pneumonia, an infectious process, or even acute respiratory distress syndrome (ARDS). 2 Kerley B lines can also be seen on a CXR in a patient with pulmonary edema. (See Kerley B lines.) These are thin, horizontal lines of fluid, no more than 2 cm long, which can be seen in the lung periphery near the costrophrenic angles and lateral wall. 2 Pneumonia can best be found on a CXR when a silhouette sign is revealed. A silhouette sign occurs when two structures of equal density are next to each other but the border of neither structure can be seen. (See Silhouette sign.) The silhouette sign is sometimes used to distinguish anterior from posterior structures on a CXR. The silhouette sign can help the practitioner determine which lung lobe is affected. 8 However, pneumonia can also present as a localized infiltrate, opacity, or consolidation. 2 These infiltrates can affect any lobe. When attempting to decide which lobe the infiltrate occupies, look for the silhouette sign. When the silhouette sign is seen in the anterior structures, the pneumonia is in the left or right upper lobe of the lung. 5 If the silhouette sign obscures the border of the right or left hemidiaphragm, this indicates a lower lobe pneumonia. When the right lower lobe border is lost but the right hemidiaphragm is visible, a right middle lobe pneumonia is present. 8 Atelectasis causes the alveoli to lose their volume and collapse and may lead to pneumonia. It can be prevented or alleviated by having the patient deep breathe and cough, Kerley B lines In this close view of the right lower lung in a patient with heart failure, Kerley B lines appear as horizontal lines running to the edge of the lung. ambulate, and perform incentive spirometry. 2 To distinguish between consolidation in pneumonia and consolidation atelectasis, assess lung volume. If lung volume is reduced, the consolidation indicates atelectasis. If not, it may be due to an infiltrate. 8 Left lower lobe atelectasis, which is very common after surgery, often appears on a CXR as an increase in density. 2,4,5 Keep in mind that a lateral view CXR may be needed to confirm atelectasis of a lower lobe. 2 When reviewing the CXR, note that in consolidation from atelectasis, the alveolar spaces can become filled with fluid, causing the alveoli to appear white and collapse. January l Nursing2014 l 45


7 Close inspection of a consolidation may reveal an air bronchogram sign. This is a tubular outline of an airway made visible by filling of the surrounding alveoli by fluid or inflammatory exudates. This will cause the airway to appear black against a white background. 8 Intrinsic obstruction can cause atelectasis and is usually a result of secretions or foreign bodies in the airway. Extrinsic airway obstruction is usually caused by compression, likely from a tumor. The most common lobe to become atelectatic is the right middle lobe, due to the lung being surrounded by lymph node tissue and the slope and length of the bronchial tube. 1 ARDS is indicated when a normal CXR progresses to one showing bilateral infiltrates, then pulmonary edema. This is likely caused by cellular damage due to an inflammatory response or events such as trauma. 4 Fluid-filled alveoli result in alveolar consolidation in the periphery of the lung fields. This tends to happen within a 12-hour time frame after injury to the alveoli-capillary membrane. 2,8 Whiteout or ground glass opacities on a CXR may follow peripheral consolidation. 4 Pneumothorax is caused by air in the pleural space, which can at times be more difficult to find on a CXRs should always be taken during maximum inspiration to allow visualization of any pulmonary abnormalities. CXR than fluid, especially if only a very small amount of air is present. Look for an increase in radiolucency (dark images on the CXR) and a decrease in lung vascular markings. 4 The visceral pleura may be displaced from the parietal pleura due to air in the pleural space. If this is the case, a thin white line would represent the displaced visceral pleura. 2,5 Silhouette sign The patient s previous X-ray is on the left; in the follow-up X-ray at right, the silhouette sign is visible as middle-lobe infiltrates obscure the border of the heart. Examine the apex of each lung in detail, as air will always rise while the patient is in an erect position. 4 Pneumothoraces can occur spontaneously or be caused by the insertion of central venous access devices, trauma, bleb rupture, or chest compressions during CPR. 5 Tension pneumothorax occurs when air leaks from the lung into the pleural space and can t escape, increasing intrapleural pressure. This causes the affected lung to collapse and shifts the mediastinum toward the unaffected side. 4 The mediastinal shift impairs cardiac filling and can quickly lead to cardiovascular collapse. Usually, mediastinal landmarks such as the trachea, aortic notch, and the right heart border are clearly seen displaced to the unaffected side. 8 COPD includes emphysema and chronic bronchitis. This type of lung disease causes airway obstruction, air trapping, and increased residual volume. 4 A flattened diaphragm associated with hyperinflation of the lung is often the best indicator of COPD on a CXR. You may also notice that the lungs look very black because of vascular destruction. The black appearance of the lung is called hyperlucency. 8 Hyperinflation of the lungs also cause the lungs to appear larger, darker, and longer. 4 It s also important to look for bullae on a CXR of a patient with COPD. These bullae are densely black areas of the lung, usually round and surrounded by fine curvilinear shadows. 8 They re usually caused by air trapping. 4 Other lung disorders The following disorders, although not as common, are also visible on CXR. Lung nodules are discrete areas of whiteness within the lung field. They re usually less than 3 cm in diameter and can be singular or found in multiples. If a lesion is larger than 3 cm, it s called a mass. 5,8 46 l Nursing2014 l January
8 The main worry about finding these lesions is the possibility of carcinoma. 8 Other possibilities are areas of consolidation, an abscess, or pleural abnormality. Inspect the lesions edges. A speculated, irregular, or lobulated edge may indicate a malignancy, especially if you see more than one. 8 Large masses found in the upper lobes are likely to be malignant. 4 Malignant tumors may be associated with mediastinal lymphadenopathy or bone metastasis. If the nodule appears dense and white and appears to be the same density as bone, it s most likely a calcification. 4,8 Tuberculosis (TB) is seen as patchy, nodular infiltrates on a CXR located primarily on the upper lobe lung fields. Cavitation of the lung, or a darker gray center over a white lesion on the CXR, is also seen with TB. An old and healed TB lesion appears on a CXR as a well-defined, dense nodule with sharp margins. 4 Perforation of the bowel is seen as free air under the diaphragm on a CXR. Air should never appear in the peritoneal cavity outside the gastrointestinal tract. If air is found in this location, it s called pneumoperitoneum, which is a medical emergency. It can be caused by a ruptured appendix, perforated ulcer, or ruptured diverticulum. 4 Nursing implications Nurses can use CXRs as an additional tool to confirm physical assessment findings. Acutely ill patients can have a multitude of nonspecific signs and symptoms. Nurses with a basic understanding of CXR interpretation can sharpen their assessment skills, promote patient safety, and optimize care. REFERENCES 1. Tarrac SE. A systematic approach to chest x-ray interpretation in the perianesthesia unit. J Perianesth Nurs. 2009;24(1): Siela D. Chest radiograph evaluation and interpretation. AACN Adv Crit Care. 2008;19(4): International Atomic Energy Agency. Radiation safety. Radiation/radsafe.html. 4. Ku V. A fresh look at chest X-rays. Nurs Crit Care. 2012;7(6): Puddy E, Hill C. Interpretation of the chest radiograph. Contin Educ Anaesth Crit Care Pain. 2007; 7(3): Barkley T, Myers C. Practice Guidelines for Acute Care Nurse Practitioners. 2nd ed. St. Louis, MO: Elsevier; Siela D. Using chest radiography in the intensive care unit. Crit Care Nurse. 2002;22(4): Corne J, Pointon K. Chest X-ray Made Easy. 3rd ed. St. Louis, MO: Elsevier; Rull G. Chest X-ray: systematic approach Systematic-Approach.htm. 10. Dick E. Chest X-rays made easy. Student BMJ. 2000;8: William Pezzotti is a critical care NP at The Chester County Hospital in West Chester, Pa. The author and planners have disclosed that they have no financial relationships related to this article. DOI /01.NURSE > < For more than 10 additional continuing education articles related to diagnostic tools, go to NursingCenter.com/CE. Earn CE credit online: Go to and receive a certificate within minutes. INSTRUCTIONS Chest X-ray interpretation: Not just black and white TEST INSTRUCTIONS To take the test online, go to our secure website at On the print form, record your answers in the test answer section of the CE enrollment form on page 48. Each question has only one correct answer. You may make copies of these forms. Complete the registration information and course evaluation. Mail the completed form and registration fee of $21.95 to: Lippincott Williams & Wilkins, CE Group, 74 Brick Blvd., Bldg. 4, Suite 206, Brick, NJ We will mail your certificate in 4 to 6 weeks. For faster service, include a fax number and we will fax your certificate within 2 business days of receiving your enrollment form. You will receive your CE certificate of earned contact hours and an answer key to review your results. There is no minimum passing grade. Registration deadline is January 31, DISCOUNTS and CUSTOMER SERVICE Send two or more tests in any nursing journal published by Lippincott Williams & Wilkins together by mail, and deduct $0.95 from the price of each test. We also offer CE accounts for hospitals and other healthcare facilities on nursingcenter. com. Call for details. PROVIDER ACCREDITATION Lippincott Williams & Wilkins, publisher of Nursing2014 journal, will award 2.3 contact hours for this continuing nursing education activity. Lippincott Williams & Wilkins is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on Accreditation. Lippincott Williams & Wilkins is also an approved provider of continuing nursing education by the District of Columbia and Florida # This activity is also provider approved by the California Board of Registered Nursing, Provider Number CEP for 2.3 contact hours. Your certificate is valid in all states. The ANCC s accreditation status of Lippincott Williams & Wilkins Department of Continuing Education refers only to its continuing nursing educational activities and does not imply Commission on Accreditation approval or endorsement of any commercial product. January l Nursing2014 l 47
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
X-Rays. Kunal D Patel Research Fellow IMM
 X-Rays Kunal D Patel Research Fellow IMM The 12-Steps } 1: Name 2: Date 3: Old films 4: What type of view(s) 5: Penetration } Pre-read 6: Inspiration 7: Rotation Quality Control 8: Angulation 9: Soft tissues
X-Rays Kunal D Patel Research Fellow IMM The 12-Steps } 1: Name 2: Date 3: Old films 4: What type of view(s) 5: Penetration } Pre-read 6: Inspiration 7: Rotation Quality Control 8: Angulation 9: Soft tissues
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC
 Interpretation Brent Burbridge, MD, FRCPC") Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
Disclosure. Clinical Chest Radiography Interpretation Part I
 Clinical Chest Radiography Interpretation Part I Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma Surgery
Clinical Chest Radiography Interpretation Part I Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma Surgery
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Radiological Anatomy of Thorax. Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem
 Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Interpreting thoracic x-ray of the supine immobile patient: Syllabus
 Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Interpreting thoracic x-ray of the supine immobile patient: Syllabus Johannes Godt Dep. of Radiology and Nuclear Medicine Oslo University Hospital Ullevål NORDTER 2017, Helsinki Content - Why bedside chest
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
B-I-2 CARDIAC AND VASCULAR RADIOLOGY
 (YEARS 1 3) CURRICULUM FOR RADIOLOGY 13 B-I-2 CARDIAC AND VASCULAR RADIOLOGY KNOWLEDGE To describe the normal anatomy of the heart and vessels including the lymphatic system as demonstrated by radiographs,
(YEARS 1 3) CURRICULUM FOR RADIOLOGY 13 B-I-2 CARDIAC AND VASCULAR RADIOLOGY KNOWLEDGE To describe the normal anatomy of the heart and vessels including the lymphatic system as demonstrated by radiographs,
PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES
 PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES Robert Harwood, MSA, RRT-NPS Objectives At the end of this presentation the student should be able to: Describe the indications of a chest radiograph.
PATIENT DATA EVALUATION AND RECOMMENDATION: IMAGING STUDIES Robert Harwood, MSA, RRT-NPS Objectives At the end of this presentation the student should be able to: Describe the indications of a chest radiograph.
Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis?
. What is the diagnosis?") 1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
1 Interpreting Chest X-Rays CASE 1 Fig. 1.1 Case 1. A 35-year-old male presented with fever, cough, and purulent sputum for one week. This was his CXR (Fig. 1.1). What is the diagnosis? CASE 1 Interpreting
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Alexander A Schult, M.D., FCCP. October 21, 2017 Revised 1/10/18
 Alexander A Schult, M.D., FCCP October 21, 2017 Revised 1/10/18 Identifying normal anatomy Identifying various pathologic states Identifying placement of hardware Identifying limitations of portable CXR
Alexander A Schult, M.D., FCCP October 21, 2017 Revised 1/10/18 Identifying normal anatomy Identifying various pathologic states Identifying placement of hardware Identifying limitations of portable CXR
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013
 Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai
 Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai Lecture 16 Radiology in diagnosis of Tuberculosis Session 01 So, welcome to the session Radiology in
Manage TB Dr. A. Chitrakumar Madras Medical College and RGGGH Institute of Thoracic Medicine, Chennai Lecture 16 Radiology in diagnosis of Tuberculosis Session 01 So, welcome to the session Radiology in
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
The External Anatomy of the Lungs. Prof Oluwadiya KS
 The External Anatomy of the Lungs Prof Oluwadiya KS www.oluwadiya.com Introduction The lungs are the vital organs of respiration Their main function is to oxygenate the blood by bringing inspired air into
The External Anatomy of the Lungs Prof Oluwadiya KS www.oluwadiya.com Introduction The lungs are the vital organs of respiration Their main function is to oxygenate the blood by bringing inspired air into
Undergraduate Teaching
 Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
Prof. James F Meaney Undergraduate Teaching Chest X-Ray Understanding the normal anatomical by reference to cross sectional imaging Radiology? It s FUN! Cryptic puzzle Sudoku (Minecraft?) It s completely
Right lung. -fissures:
 -Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
-Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
Lines and tubes. 1 Nasogastric tubes Endotracheal tubes Central lines Permanent pacemakers Chest drains...
 Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
Interpretation of the chest radiograph Elizabeth Puddy MB ChB FCARCSI Catherine Hill MB ChB MRCP FRCR
 Interpretation of the chest radiograph Elizabeth Puddy MB ChB FCARCSI Catherine Hill MB ChB MRCP FRCR The traditional technique used in the acquisition and development of a chest radiograph uses methods
Interpretation of the chest radiograph Elizabeth Puddy MB ChB FCARCSI Catherine Hill MB ChB MRCP FRCR The traditional technique used in the acquisition and development of a chest radiograph uses methods
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Introduction to Chest Radiography
 Introduction to Chest Radiography RSTH 366: DIAGNOSTIC TECHNIQUES Alan Alipoon BS, RCP, RRT Instructor Department of Cardiopulmonary Sciences 1 Introduction Discovered in 1895 by Wilhelm Roentgen Terminology
Introduction to Chest Radiography RSTH 366: DIAGNOSTIC TECHNIQUES Alan Alipoon BS, RCP, RRT Instructor Department of Cardiopulmonary Sciences 1 Introduction Discovered in 1895 by Wilhelm Roentgen Terminology
Radiology of the respiratory disease
 Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Radiology of the respiratory disease [ Color index: Important Notes Extra ] [ Editing file Feedback Share your notes Shared notes ] Resources: - 435 Slides - 434 Team - 435 Notes Done by: - Mai Alageel
Interactive Lecture. Lecture 7 - Interactive. Radiology of cardiorespiratory disease. Editing File. Done By. Color Coding Important Notes Extra
 Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
Lecture 7 - Interactive 436 Teams Interactive Lecture Radiology of cardiorespiratory disease Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Ghaida Alsaeed Maha Alissa Nawwaf AlHarbi
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Anatomy Lecture 8. In the previous lecture we talked about the lungs, and their surface anatomy:
 Anatomy Lecture 8 In the previous lecture we talked about the lungs, and their surface anatomy: 1-Apex:it lies 1 inch above the medial third of clavicle. 2-Anterior border: it starts from apex to the midpoint
Anatomy Lecture 8 In the previous lecture we talked about the lungs, and their surface anatomy: 1-Apex:it lies 1 inch above the medial third of clavicle. 2-Anterior border: it starts from apex to the midpoint
Approach to CXR. Terminology. 1.Identification. Greg Blecher SCH Respir Fellow. Correct patient Correct date and time Correct examination
 Approach to CXR Greg Blecher SCH Respir Fellow From Rob Posteraro http://home.earthlink.net/~rhpos/cxr_interpret.txt.html ; http://home.earthlink.net/~rhpos/cxr_main.txt.html) Approach to viewing Chest
Approach to CXR Greg Blecher SCH Respir Fellow From Rob Posteraro http://home.earthlink.net/~rhpos/cxr_interpret.txt.html ; http://home.earthlink.net/~rhpos/cxr_main.txt.html) Approach to viewing Chest
Dana Alrafaiah. - Moayyad Al-Shafei. -Mohammad H. Al-Mohtaseb. 1 P a g e
 - 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
- 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
Radiological conference. Left upper lobe collapse. Citation Hong Kong Practitioner, 1998, v. 20 n. 9, p
 Title Radiological conference. Left upper lobe collapse Author(s) Wong, LLS; Peh, WCG Citation Hong Kong Practitioner, 1998, v. 20 n. 9, p. 513-517 Issued Date 1998 URL http://hdl.handle.net/10722/44672
Title Radiological conference. Left upper lobe collapse Author(s) Wong, LLS; Peh, WCG Citation Hong Kong Practitioner, 1998, v. 20 n. 9, p. 513-517 Issued Date 1998 URL http://hdl.handle.net/10722/44672
FUNDAMENTALS OF CXR INTERPRETATION THE BASICS
 FUNDAMENTALS OF CXR INTERPRETATION THE BASICS PART I QUALITY ASSESSMENT 1 PATIENT-DEPENDENT FACTORS 3 REVIEW OF IMPORTANT ANATOMY 7 LUNGS AND PLEURA 11 DIAPHRAGMS 13 BONES AND SOFT TISSUES 14 A BRIEF LOOK
FUNDAMENTALS OF CXR INTERPRETATION THE BASICS PART I QUALITY ASSESSMENT 1 PATIENT-DEPENDENT FACTORS 3 REVIEW OF IMPORTANT ANATOMY 7 LUNGS AND PLEURA 11 DIAPHRAGMS 13 BONES AND SOFT TISSUES 14 A BRIEF LOOK
Lung & Pleura. The Topics :
 Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
X-rays. Dr Will Dooley
 X-rays Dr Will Dooley Plan Chest X-Rays Abdominal X-Rays Exam approach Presentation skills EMQ EMQ- answers Chest X-Ray - Systematic Approach D R Details RIP Image Quality +/- OBVIOUS ABNORMALITY A B C
X-rays Dr Will Dooley Plan Chest X-Rays Abdominal X-Rays Exam approach Presentation skills EMQ EMQ- answers Chest X-Ray - Systematic Approach D R Details RIP Image Quality +/- OBVIOUS ABNORMALITY A B C
Thorax Lecture 2 Thoracic cavity.
 Thorax Lecture 2 Thoracic cavity. Spring 2016 Dr. Maher Hadidi, University of Jordan 1 Enclosed by the thoracic wall. Extends between (thoracic inlet) & (thoracic outlet). Thoracic inlet At root of the
Thorax Lecture 2 Thoracic cavity. Spring 2016 Dr. Maher Hadidi, University of Jordan 1 Enclosed by the thoracic wall. Extends between (thoracic inlet) & (thoracic outlet). Thoracic inlet At root of the
Shades of Gray Interpretation of Perioperative Imaging
 Stanford Hospital and Clinics DEPARTMENT OF CARDIOTHORACIC SURGERY-THORACIC AORTIC SURGERY UNIT FALK CARDIOVASCULAR RESEARCH CENTER STANFORD, CALIFORNIA 94305-5407 MICHAEL SHEEHAN, MSN, RNFA, NPC TELEPHONE
Stanford Hospital and Clinics DEPARTMENT OF CARDIOTHORACIC SURGERY-THORACIC AORTIC SURGERY UNIT FALK CARDIOVASCULAR RESEARCH CENTER STANFORD, CALIFORNIA 94305-5407 MICHAEL SHEEHAN, MSN, RNFA, NPC TELEPHONE
PLEURAE and PLEURAL RECESSES
 PLEURAE and PLEURAL RECESSES By Dr Farooq Aman Ullah Khan PMC 26 th April 2018 Introduction When sectioned transversely, it is apparent that the thoracic cavity is kidney shaped: a transversely ovoid space
PLEURAE and PLEURAL RECESSES By Dr Farooq Aman Ullah Khan PMC 26 th April 2018 Introduction When sectioned transversely, it is apparent that the thoracic cavity is kidney shaped: a transversely ovoid space
Neonatal Chest X-Ray Interpretation
 CHAPTER 7 Neonatal Chest X-Ray Interpretation Prof. Praveen Kumar Neonatal unit, Department of Pediatrics, PGIMER, Chandigarh Learning Objectives At the end of this session, you should be able to: 1. Schematically
CHAPTER 7 Neonatal Chest X-Ray Interpretation Prof. Praveen Kumar Neonatal unit, Department of Pediatrics, PGIMER, Chandigarh Learning Objectives At the end of this session, you should be able to: 1. Schematically
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code
 Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Objectives. What is a Chest X Ray? CXR Workshop. Definition (diagnostic tool/internal PE) Types. Cost
 Types. Cost") Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments
 Done By : Rahmeh Alsukkar Date : 26 /10/2017 slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments Each segmental bronchus passes to a structurally
Done By : Rahmeh Alsukkar Date : 26 /10/2017 slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments Each segmental bronchus passes to a structurally
CHEST & ABDOMINAL X-RAYS MALIKA IBRAHIM CORE MEDICAL TRAINEE BLACKPOOL VICTORIA HOSPITAL DATA INTERPRETATION COURSE FEB 20, 2017
 CHEST & ABDOMINAL X-RAYS MALIKA IBRAHIM CORE MEDICAL TRAINEE BLACKPOOL VICTORIA HOSPITAL DATA INTERPRETATION COURSE FEB 20, 2017 1. Sample x-rays 2. Basic chest x-ray interpretation skills 3. Chest x-ray
CHEST & ABDOMINAL X-RAYS MALIKA IBRAHIM CORE MEDICAL TRAINEE BLACKPOOL VICTORIA HOSPITAL DATA INTERPRETATION COURSE FEB 20, 2017 1. Sample x-rays 2. Basic chest x-ray interpretation skills 3. Chest x-ray
Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th & 12 th Eds.)
") PLEURAL CAVITY AND LUNGS Dr. Milton M. Sholley SELF STUDY RESOURCES Essential Clinical Anatomy 3 rd ed. (ECA): pp. 70 81 Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th &
PLEURAL CAVITY AND LUNGS Dr. Milton M. Sholley SELF STUDY RESOURCES Essential Clinical Anatomy 3 rd ed. (ECA): pp. 70 81 Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th &
X-Rays. Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady
 X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
Chest and cardiovascular
 Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
10/14/2018 Dr. Shatarat
 2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
Anatomy notes-thorax.
 Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Signs in Chest Radiology
 Signs in Chest Radiology Jonathan H. Chung, MD Disclosures No pertinent disclosures Jonathan H. Chung, MD Assistant Professor Institute t of fadvanced d Biomedical Imaging National Jewish Health Denver,
Signs in Chest Radiology Jonathan H. Chung, MD Disclosures No pertinent disclosures Jonathan H. Chung, MD Assistant Professor Institute t of fadvanced d Biomedical Imaging National Jewish Health Denver,
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Disclosure. Clinical Chest Radiography Interpretation Part II
 Clinical Chest Radiography Interpretation Part II Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma
Clinical Chest Radiography Interpretation Part II Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma
Dr. Weyrich G07: Superior and Posterior Mediastina. Reading: 1. Gray s Anatomy for Students, chapter 3
 Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Imaging of Respiratory Disorders: M2 Pathology correlated with Radiology
 Imaging of Respiratory Disorders: M2 Pathology correlated with Radiology by (c) Dr Goh Poh Sun MBBS(Melb), FRCR(UK), FAMS(Singapore), MHPE(Maastricht) Senior Consultant Radiologist and Associate Professor
Imaging of Respiratory Disorders: M2 Pathology correlated with Radiology by (c) Dr Goh Poh Sun MBBS(Melb), FRCR(UK), FAMS(Singapore), MHPE(Maastricht) Senior Consultant Radiologist and Associate Professor
Chapter 5: Other mediastinal structures. The Large Arteries. The Aorta. Ascending aorta
 Chapter 5: Other mediastinal structures The Large Arteries The Aorta The aorta is the main arterial trunk of the systemic circulation and in the healthy state its wall contain a large amount of yellow
Chapter 5: Other mediastinal structures The Large Arteries The Aorta The aorta is the main arterial trunk of the systemic circulation and in the healthy state its wall contain a large amount of yellow
THE GOOFY ANATOMIST QUIZZES
 THE GOOFY ANATOMIST QUIZZES 7. LUNGS Q1. Fill in the blanks: the lung has lobes and fissures. A. Right, three, two. B. Right, two, one. C. Left, three, two. D. Left, two, three. Q2. The base of the lung
THE GOOFY ANATOMIST QUIZZES 7. LUNGS Q1. Fill in the blanks: the lung has lobes and fissures. A. Right, three, two. B. Right, two, one. C. Left, three, two. D. Left, two, three. Q2. The base of the lung
Introduction to Chest CT Interpretation. Objectives 8/28/2017
 Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
BOGOMOLETS NATIONAL MEDICAL UNIVERSITY DEPARTMENT OF HUMAN ANATOMY. Guidelines. Module 2 Topic of the lesson Aorta. Thoracic aorta.
 BOGOMOLETS NATIONAL MEDICAL UNIVERSITY DEPARTMENT OF HUMAN ANATOMY Guidelines Academic discipline HUMAN ANATOMY Module 2 Topic of the lesson Aorta. Thoracic aorta. Course 1 The number of hours 3 1. The
BOGOMOLETS NATIONAL MEDICAL UNIVERSITY DEPARTMENT OF HUMAN ANATOMY Guidelines Academic discipline HUMAN ANATOMY Module 2 Topic of the lesson Aorta. Thoracic aorta. Course 1 The number of hours 3 1. The
Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous structures - Significant thoracic inj
 PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
Lab #3. Mohammad Hisham Al-Mohtaseb. Jumana Jihad. Ammar Ramadan. 0 P a g e
 Lab #3 Mohammad Hisham Al-Mohtaseb Jumana Jihad Ammar Ramadan 0 P a g e Last anatomy lab: Lungs and structure on the mediastinal surfs: 1-the right lung: How do we know it s the right lung??? -the 3 lobes
Lab #3 Mohammad Hisham Al-Mohtaseb Jumana Jihad Ammar Ramadan 0 P a g e Last anatomy lab: Lungs and structure on the mediastinal surfs: 1-the right lung: How do we know it s the right lung??? -the 3 lobes
Anatomy Sheet #5. In the previous lecture, we finished discussion about the larynx; now we continue with trachea, lungs and pleura.
 Anatomy Sheet #5 In the previous lecture, we finished discussion about the larynx; now we continue with trachea, lungs and pleura. Trachea and lungs The knowledge about the pleura and lungs is very important
Anatomy Sheet #5 In the previous lecture, we finished discussion about the larynx; now we continue with trachea, lungs and pleura. Trachea and lungs The knowledge about the pleura and lungs is very important
Focused Assessment Sonography of Trauma (FAST) Scanning Protocol
 Scanning Protocol") Focused Assessment Sonography of Trauma (FAST) Scanning Protocol Romolo Gaspari CHAPTER 3 GOAL OF THE FAST EXAM Demonstrate free fluid in abdomen, pleural space, or pericardial space. EMERGENCY ULTRASOUND
Focused Assessment Sonography of Trauma (FAST) Scanning Protocol Romolo Gaspari CHAPTER 3 GOAL OF THE FAST EXAM Demonstrate free fluid in abdomen, pleural space, or pericardial space. EMERGENCY ULTRASOUND
Mediastinum and pericardium
 Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
Concepts in Small Animal Thoracic Radiology Thoracic Radiology
 Concepts in Small Animal Thoracic Radiology + Radiology of the Pleural Space VMB 960 2/21/2011 Optimizing Image Quality Inherent subject contrast Thorax has high inherent subject contrast c/f abdomen Primarily
Concepts in Small Animal Thoracic Radiology + Radiology of the Pleural Space VMB 960 2/21/2011 Optimizing Image Quality Inherent subject contrast Thorax has high inherent subject contrast c/f abdomen Primarily
Cardiovascular system:
 Cardiovascular system: Mediastinum: The mediastinum: lies between the right and left pleura and lungs. It extends from the sternum in front to the vertebral column behind, and from the root of the neck
Cardiovascular system: Mediastinum: The mediastinum: lies between the right and left pleura and lungs. It extends from the sternum in front to the vertebral column behind, and from the root of the neck
Sectional Anatomy Quiz - III
 Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Lecture 3. Inflammatory Processes
 Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
Pneumothorax. Defined as air in the pleural space which can occur through a number of mechanisms
 Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
TIPS AND PITFALLS IN PLAIN FILM INTERPRETATION
 TIPS AND PITFALLS IN PLAIN FILM INTERPRETATION Dr Philip Touska MBBS, BMedSci(Hons), MRCS, DO-HNS, FRCR Radiology Fellow Guy s & St Thomas Hospitals LEARNING OBJECTIVES Where do we go wrong? Common pitfalls
TIPS AND PITFALLS IN PLAIN FILM INTERPRETATION Dr Philip Touska MBBS, BMedSci(Hons), MRCS, DO-HNS, FRCR Radiology Fellow Guy s & St Thomas Hospitals LEARNING OBJECTIVES Where do we go wrong? Common pitfalls
DESCRIPTION: This is the part of the trunk, which is located between the root of the neck and the superior border of the abdominal region.
 1 THE THORACIC REGION DESCRIPTION: This is the part of the trunk, which is located between the root of the neck and the superior border of the abdominal region. SHAPE : T It has the shape of a truncated
1 THE THORACIC REGION DESCRIPTION: This is the part of the trunk, which is located between the root of the neck and the superior border of the abdominal region. SHAPE : T It has the shape of a truncated
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Anatomy of the Lungs. Dr. Gondo Gozali Department of anatomy
 Anatomy of the Lungs Dr. Gondo Gozali Department of anatomy 1 Pulmonary Function Ventilation and Respiration Ventilation is the movement of air in and out of the lungs Respiration is the process of gas
Anatomy of the Lungs Dr. Gondo Gozali Department of anatomy 1 Pulmonary Function Ventilation and Respiration Ventilation is the movement of air in and out of the lungs Respiration is the process of gas
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O
 ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
ANATOMY OF THE PLEURA. Dr Oluwadiya KS
 ANATOMY OF THE PLEURA Dr Oluwadiya KS www.oluwadiya.sitesled.com Introduction The thoracic cavity is divided mainly into: Right pleural cavity Mediastinum Left Pleural cavity Pleural cavity The pleural
ANATOMY OF THE PLEURA Dr Oluwadiya KS www.oluwadiya.sitesled.com Introduction The thoracic cavity is divided mainly into: Right pleural cavity Mediastinum Left Pleural cavity Pleural cavity The pleural
Imaging of Pleural Effusion: Comparing Ultrasound, X-Ray and CT findings
 Imaging of Pleural Effusion: Comparing Ultrasound, X-Ray and CT findings Poster No.: C-2067 Congress: ECR 2017 Type: Educational Exhibit Authors: J. M. Almeida, N. Antunes, C. Leal, L. Figueiredo ; Lisboa/PT,
Imaging of Pleural Effusion: Comparing Ultrasound, X-Ray and CT findings Poster No.: C-2067 Congress: ECR 2017 Type: Educational Exhibit Authors: J. M. Almeida, N. Antunes, C. Leal, L. Figueiredo ; Lisboa/PT,
THE DESCENDING THORACIC AORTA
 Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
Techniques of examination of the thorax and lungs. Dr. Szathmári Miklós Semmelweis University First Department of Medicine 24. Sept
 Techniques of examination of the thorax and lungs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 24. Sept. 2013. Inspection of the thorax Observe: the shape of chest Deformities
Techniques of examination of the thorax and lungs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 24. Sept. 2013. Inspection of the thorax Observe: the shape of chest Deformities
Advances in MDCT of Thoracic Trauma
 Baltic Congress of Radiology, Riga 2010 Advances in MDCT of Thoracic Trauma Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General
Baltic Congress of Radiology, Riga 2010 Advances in MDCT of Thoracic Trauma Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General
Surface anatomy of Cardiovascular system
 Surface anatomy of Cardiovascular system Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The lines cover the front, side, and back of the thorax Midsternal
Surface anatomy of Cardiovascular system Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The lines cover the front, side, and back of the thorax Midsternal
Mediastinum It is a thick movable partition between the two pleural sacs & lungs. It contains all the structures which lie
 Dr Jamila EL medany OBJECTIVES At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum. List the boundaries and contents of
Dr Jamila EL medany OBJECTIVES At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum. List the boundaries and contents of
Identify the lines used in anatomical surface descriptions of the thorax. median line mid-axillary line mid-clavicular line
 L 14 A B O R A T O R Y Thorax THORACIC WALL Identify the lines used in anatomical surface descriptions of the thorax. median line mid-axillary line mid-clavicular line Identify the surface landmarks of
L 14 A B O R A T O R Y Thorax THORACIC WALL Identify the lines used in anatomical surface descriptions of the thorax. median line mid-axillary line mid-clavicular line Identify the surface landmarks of
RADIOLOGY FOR FINALS THE ULTIMATE REVISION GUIDE
 RADIOLOGY FOR FINALS THE ULTIMATE REVISION GUIDE By Lina Fazlanie (4th year medical student) & Ian Bickle (Radiology SpR) This short focused revision guide features 20 of the most popular x-rays that are
RADIOLOGY FOR FINALS THE ULTIMATE REVISION GUIDE By Lina Fazlanie (4th year medical student) & Ian Bickle (Radiology SpR) This short focused revision guide features 20 of the most popular x-rays that are
BIOE221. Session 5. Examination of Thorax- Respiratory system. Bioscience Department. Endeavour College of Natural Health endeavour.edu.
 BIOE221 Session 5 Examination of Thorax- Respiratory system Bioscience Department Session Objectives Understand the structure of the thorax and the organs contained in this cavity Understand the importance
BIOE221 Session 5 Examination of Thorax- Respiratory system Bioscience Department Session Objectives Understand the structure of the thorax and the organs contained in this cavity Understand the importance
The Thoracic wall including the diaphragm. Prof Oluwadiya KS
 The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!!
 The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function
 The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Bronchioles. Alveoli. Type I alveolar cells are very thin simple squamous epithelial cells and form most of the lining of an alveolus.
 276 Bronchioles Bronchioles continue on to form bronchi. The primary identifying feature is the loss of hyaline cartilage. The epithelium has become simple ciliated columnar, and there is a complete ring
276 Bronchioles Bronchioles continue on to form bronchi. The primary identifying feature is the loss of hyaline cartilage. The epithelium has become simple ciliated columnar, and there is a complete ring
Bio 322 Human Anatomy Objectives for the laboratory exercise Respiratory System
 Bio 322 Human Anatomy Objectives for the laboratory exercise Respiratory System Required reading before beginning this lab: Saladin, KS: Human Anatomy 5 th ed (2017) Chapter 23 For this lab you will use
Bio 322 Human Anatomy Objectives for the laboratory exercise Respiratory System Required reading before beginning this lab: Saladin, KS: Human Anatomy 5 th ed (2017) Chapter 23 For this lab you will use
Yara saddam & Dana Qatawneh. Razi kittaneh. Maher hadidi
 1 Yara saddam & Dana Qatawneh Razi kittaneh Maher hadidi LECTURE 10 THORAX The thorax extends from the root of the neck to the abdomen. The thorax has a Thoracic wall Thoracic cavity and it is divided
1 Yara saddam & Dana Qatawneh Razi kittaneh Maher hadidi LECTURE 10 THORAX The thorax extends from the root of the neck to the abdomen. The thorax has a Thoracic wall Thoracic cavity and it is divided
PULMONARY COLLAPSE Whole lung collapse: There is complete opacity of the L hemi-thorax. The mediastinum is invisible and displaced into
 1 PULMONARY COLLAPSE: A cause of opacity on chest X-ray but there are several features to distinguish it from alveolar shadowing or interstitial lung disease. The loss of lung volume may affect the position
1 PULMONARY COLLAPSE: A cause of opacity on chest X-ray but there are several features to distinguish it from alveolar shadowing or interstitial lung disease. The loss of lung volume may affect the position
Tests Your Pulmonologist Might Order. Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital
 Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Tests Your Pulmonologist Might Order Center For Cardiac Fitness Pulmonary Rehab Program The Miriam Hospital BASIC ANATOMY OF THE LUNGS Lobes of Lung 3 lobes on the Right lung 2 lobes on the Left Blood
Mohammad Almohtaseb. Lubna Allawi. Ammar Ramadan. 0 P a g e
 5 Mohammad Almohtaseb Lubna Allawi Ammar Ramadan 0 P a g e Trachea and Lungs The trachea The trachea is a flexible tube that extends from lower border of the larynx (lower border of cricoid cartilage at
5 Mohammad Almohtaseb Lubna Allawi Ammar Ramadan 0 P a g e Trachea and Lungs The trachea The trachea is a flexible tube that extends from lower border of the larynx (lower border of cricoid cartilage at
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress THE LAST GASP II: LUNGS AND THORAX David Holt, BVSc, Diplomate ACVS University of Pennsylvania School of Veterinary
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress THE LAST GASP II: LUNGS AND THORAX David Holt, BVSc, Diplomate ACVS University of Pennsylvania School of Veterinary
CHEST TRAUMA. Dr Naeem Zia FCPS,FACS,FRCS
 CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
Mohammad Hisham Al-Mohtaseb. Lina Mansour. Enas Ajarma
 6 Mohammad Hisham Al-Mohtaseb Lina Mansour Enas Ajarma Some recommended videos are attached to this sheet ( if u are studying online click on them, if not u can reach them by typing their names on the
6 Mohammad Hisham Al-Mohtaseb Lina Mansour Enas Ajarma Some recommended videos are attached to this sheet ( if u are studying online click on them, if not u can reach them by typing their names on the