CHEST TRAUMA. Dr Naeem Zia FCPS,FACS,FRCS
|
|
|
- Buck Francis
- 6 years ago
- Views:
Transcription

1
2 CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS
3 Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring immediate management Investigations for a patient with thoracic trauma Management of urgent thoracic conditions
4 Trauma, or injury, is defined as cellular disruption caused by an exchange with environmental energy that is beyond the body's resilience Trauma remains the most common cause of death for all individuals between the ages of 1 and 44 years and is the third most common cause of death regardless of age
5 Initial Evaluation and Resuscitation of the Injured Patient ATLS The initial management of seriously injured patients consists of the primary survey, concurrent resuscitation, the secondary survey, diagnostic evaluation, and definitive care.
6 Primary survey identify and treat conditions that constitute an immediate threat to life. A B C D E

7 Anatomy of chest
8 Main Causes of Chest Trauma Blunt Trauma- Blunt force to chest. Penetrating Trauma- Projectile that enters chest causing small or large hole. Compression Injury- Chest is caught between two objects and chest is compressed.
9 Injuries of chest Simple/Closed Pneumothorax Open Pneumothorax Tension Pneumothorax Flail Chest Cardiac Tamponade Traumatic Aortic Rupture Diaphragmatic Rupture
10 Fractures and Dislocations Spine Ribs Clavicles Sternum Shoulders

11 Trauma Chest Radiograph Usually AP, often supine, frequently in poor inspiration. So, a challenge to interpret.

12 CT Chest More sensitive and specific

13 Rib Fractures In themselves, not too much of a problem, but may be an indicator of underlying pleura, lung, liver, spleen, kidney injuries.
14 AIR where it shouldn t be Pneumothorax Pneumomediastinum Subcutaneous emphysema Systemic venous air embolism Pneumopericardium Pneumoperitoneum/retroperitoneum

15

16 Simple/Closed Pneumothorax Opening in lung tissue that leaks air into chest cavity Blunt trauma is main cause May be spontaneous Usually self correcting

17 S/S of Simple/Closed Pneumothorax Chest Pain Dyspnea Tachypnea Decreased Breath Sounds on Affected Side
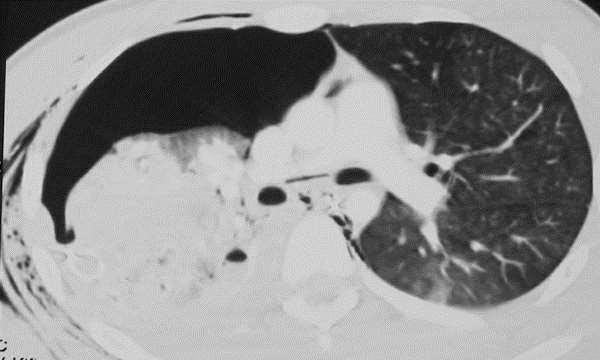
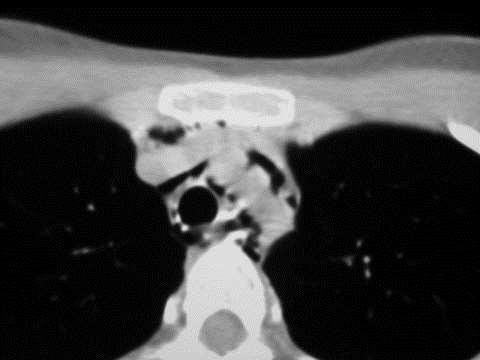
18 PNEUMOTHORAX: CT Much more sensitive than plain films. Even a small traumatic pneumothorax is important, especially if patient mechanically ventilated or going to OR: A simple pneumothorax can be converted into a life- threatening tension pneumothorax
19
20 Treatment for Simple/Closed Pneumothorax ABC s with C-spine control Airway Assistance as needed Provide supportive care Monitor for Development of Tension Pneumothorax In significant chest inj. + p.p. mechanical ventilation prophylactic tube thoracostomy (prevention of tension P.)

21 Open Pneumothorax Opening in chest cavity that allows air to enter pleural cavity Causes the lung to collapse due to increased pressure in pleural cavity Can be life threatening and can deteriorate rapidly If the opening in the chest wall is approximately 2/3 rd of the diameter of trachea air passes preferentially through the chest wall defect with each respiratory effort.
22 S/S of Open Pneumothorax Dyspnea Sudden sharp pain Subcutaneous Emphysema Decreased lung sounds on affected side Red Bubbles on Exhalation from wound wound) ( a.k.a. Sucking chest
23 Subcutaneous Emphysema Air collects in subcutaneous fat from pressure of air in pleural cavity Feels like rice crispies or bubble wrap Can be seen from neck to groin area

24 Sucking Chest Wound
25 Treatment for Open Pneumothorax ABC s with c-spine control as indicated High Flow oxygen Listen for decreased breath sounds on affected side Apply three way occlusive dressing to wound as a temporary measure A chest tube remote from the wound should be placed as soon as possible


26 Occlusive Dressing Three way occlusive dressng
27 Tension Pneumothorax Air builds in pleural space with no where for the air to escape Results in collapse of lung on affected side that results in pressure on mediastium,the other lung, and great vessels
28 Tension Pneumothorax Each time we inhale, the lung collapses further. There is no place for the air to escape..
29 Tension Pneumothorax The trachea is pushed to the good side Heart is being compressed
30 S/S of Tension Pneumothorax Anxiety/Restlessness Severe Dyspnea Absent Breath sounds on affected side Tachypnea Tachycardia Poor Color Accessory Muscle Use JVD Narrowing Pulse Pressures Hypotension Tracheal Deviation (late if seen at all)

31
32
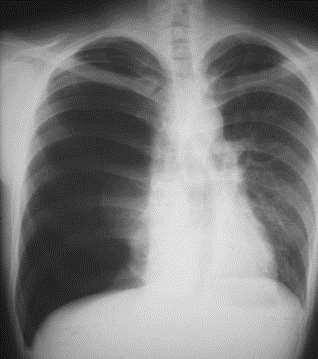
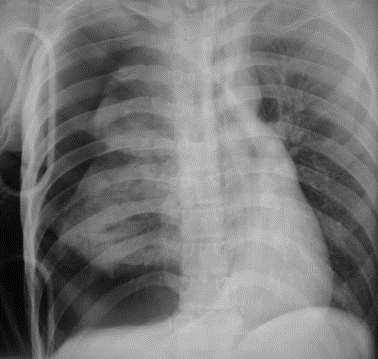
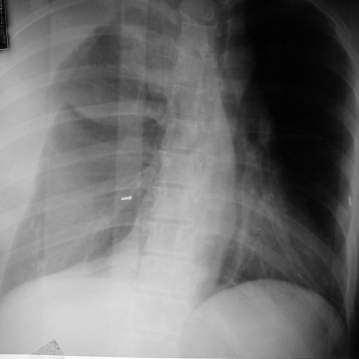
33 Erect AP/PA view best Shift of mediastinum/heart/trachea away from PTX side Depressed hemidiaphragm Degree of lung collapse is variable
34
35 Treatment of Tension Pneumothorax ABC s with c-spine as indicated High Flow oxygen Treat for S/S of Shock If Open Pneumothorax promptly close the defect with a sterile occlusive dressing. Tape it securely on three sides to provide a flutter type valve effect
36 Monitor Cardiac Rhythm Establish IV access and Draw Blood Samples Airway control including Intubation Needle Decompression of Affected Side followed by tube thoracostomy.
37 Needle Decompression Locate 2-3 Intercostal space midclavicular line Cleanse area using aseptic technique Insert catheter ( 14g or larger) at least 3 in length over the top of the 3 rd rib( nerve, artery, vein lie along bottom of rib) Remove Stylette and listen for rush of air Place Flutter valve over catheter Reassess for Improvement

38 Needle Decompression
39 Hemothorax Occurs when pleural space fills with blood Usually occurs due to lacerated blood vessel in thorax As blood increases, it puts pressure on heart and other vessels in chest cavity Each Lung can hold 1.5 liters of blood
40 PNEUMOMEDIASTIUM Usually from ruptured alveoli. Can also be from trachea, bronchi, esophagus, bowel and neck injuries.
41 PNEUMOMEDIASTINUM: Signs Linear paratracheal lucencies Air along heart border V sign at aortic-diaphragm junction Continuous diaphragm sign
42

43 PNEUMOMEDIASTINUM: Continuous diaphragm sign
44 PNEUMOMEDIASTINUM: CT
45

46 Trachea/bronchi injuries Tears occur within 2cm of carina Persistant pneumothorax Large pneumomediastinum Fallen lung

47 Subcutaneous Emphysema Causes: Same as pneumomediastinum
48 Hemothorax
49 Hemothorax May put pressure on the heart
50 Hemothorax Where does the blood come from. Lots of blood vessels
51
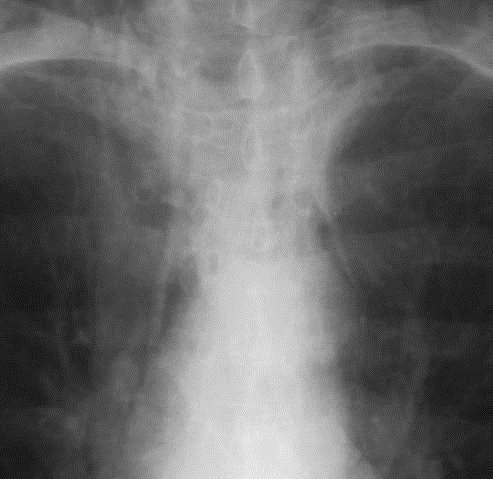
52 HEMOTHORAX Venous or arterial bleeding 60% controlled by chest tube, 40% need operative management Can miss hundreds of cc s on supine film Can be tension
53
54 HEMOTHORAX
55 S/S of Hemothorax Anxiety/Restlessness Tachypnea Signs of Shock Frothy, Bloody Sputum Diminished Breath Sounds on Affected Side Tachycardia Flat Neck Veins
56

57 CT: HEMOTHORAX
58 Treatment for Hemothorax ABC s with c-spine control as indicated Secure Airway assist ventilation if necessary General Shock Care due to Blood loss Airway management to include Intubation If Development of Hemo/Pneumothorax needle decompression may be indicated followed by tube thoracostomy

59 Flail Chest The breaking of 2 or more ribs in 2 or more places

60 Flail Chest

61 Flail Chest Multiple rib fractures, especially if individual ribs fractured more than once, may cause paradoxical motion. The major problem actually is associated pulmonary contusion
62 S/S of Flail Chest Shortness of Breath Paradoxical Movement Bruising/Swelling Crepitus( Grinding of bone ends on palpation)
63 Treatment of Flail Chest ABC s with c-spine control as indicated High Flow oxygen Airway management to include Intubation and ventilation for prevention of hypoxia. Monitor Patient for signs of Pneumothorax or Tension Pneumothorax Pain control by either intermittent intercostal nerve blocks or epidural anaesthesia.
64 Pericardial Tamponade pericardial sac Blood and fluids leak into the pericardial sac which surrounds the heart. As the pericardial sac fills, it causes the sac to expand until it cannot expand anymore
65 Pericardial Tamponade Once the pericardial sac can t expand anymore, the fluid starts putting pressure on the heart Now the heart can t fully expand and can t pump effectively.
66 Pericardial Tamponade With poor pumping the blood pressure starts to drop. The heart rate starts to increase to compensate but is unable The patient s level of conscious drops, and eventually the patient goes in cardiac arrest
67 S/S of Pericardial Tamponade BECK S TRIAD Distended Neck Veins Muffled heart sounds Hypotension KUSSMAUL S SIGN Rise in venous pressure with inspiration when breathing spontaneously
68 Treatment of Pericardial Tamponade ABC s with c-spine control as indicated High Flow oxygen Treat S/S of shock What patient needs is pericardiocentesis
69 Pericardiocentesis Using aseptic technique, Insert at least 3 needle at the angle of the Xiphoid Cartilage at the 7 th rib Advance needle at 45 degree towards the clavicle while aspirating syringe till blood return is seen Continue to Aspirate till syringe is full then discard blood and attempt again till signs of no more blood Closely monitor patient due to small about of blood aspirated can cause a rapid change in blood pressure
70

71 Pneumopericardium Causes: penetrating trauma Rare
72 Traumatic Aortic Rupture The heart, more or less, just hangs from the aortic arch Much like a big pendulum. If enough motion is placed on the heart (i.e.. Deceleration From a motor vehicle accident, striking a tree while skiing etc) the heart may tear away from the aorta.

73 Traumatic Aortic Rupture The chances of survival are very slim and are based on the degree of the tear. If there is just a small tear then the patient may survive. If the aorta is completely transected then the patient will die instantaneously
74 S/S Of Traumatic Aortic Rupture Burning or Tearing Sensation in chest or shoulder blades Rapidly dropping Blood Pressure Pulse Rapidly Increasing Decreased or loss of pulse or b/p on left side compared to right side Rapid Loss of Consciousness
75 Treatment of Traumatic Aortic Rupture ABC s with c-spine control as indicated High Flow oxygen Treatment for Shock Emergency surgical repair
76 Diaphragmatic Rupture A tear in the Diaphragm that allows the abdominal organs enter the chest cavity More common on Left side due to liver helps protect the right side of diaphragm Associated with multipile injury patients

77 Diaphragm Rupture
78 S/S of Diaphragmatic Rupture Abdominal Pain Shortness of Air Decreased Breath Sounds on side of rupture Bowel Sounds heard in chest cavity
79 Treatment of Diaphragmatic Rupture ABC s with c-spine control as indicated High Flow oxygen Treat Associated Injuries Observe for Pneumothorax due to compression on lung by abdominal contents Possible insertion of NG tube to help decompress the stomach to relieve pressure Patient needs BRIGHT LIGHTS AND COLD STEEL
80 Penetrating injuries
81 Blast injuries
82 SUMMARY Chest Injuries are common and often life threatening in trauma patients. So, Rapid identification and treatment of these patients is paramount to patient survival. Airway management is very important and aggressive management is sometimes needed for proper management of most chest injuries.
Chest Trauma.
 Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Chapter 29 - Chest Injuries
 1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
9/10/2012. Chapter 49. Learning Objectives. Learning Objectives (Cont d) Thoracic Trauma
 Thoracic Trauma") Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
CHEST INJURIES. Jacek Piątkowski M.D., Ph. D.
 CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous structures - Significant thoracic inj
 PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
The Management of Chest Trauma. Tom Scaletta, MD FAAEM Immediate Past President, AAEM
 The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma
: Penetrating Cardiac Trauma") Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
INJURIES CHEST, ABDOMEN, LIMBS. FN Brno November 2011
 INJURIES CHEST, ABDOMEN, LIMBS FN Brno November 2011 Injury Chest Abdomen Limbs Injury to the rib cage Fractured one or more ribs Sharp pain at the site of fracture Pain on taking a deep breath Shallow
INJURIES CHEST, ABDOMEN, LIMBS FN Brno November 2011 Injury Chest Abdomen Limbs Injury to the rib cage Fractured one or more ribs Sharp pain at the site of fracture Pain on taking a deep breath Shallow
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
You Are the Emergency Medical Responder
 Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Chapter 34. Objectives. Objectives 01/09/2013. Chest Trauma
 Chapter 34 Chest Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 34 Chest Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Chapter 3: Thorax. Thorax
 Chapter 3: Thorax Thorax Thoracic Cage I. Thoracic Cage Osteology A. Thoracic Vertebrae Basic structure: vertebral body, pedicles, laminae, spinous processes and transverse processes Natural kyphotic shape,
Chapter 3: Thorax Thorax Thoracic Cage I. Thoracic Cage Osteology A. Thoracic Vertebrae Basic structure: vertebral body, pedicles, laminae, spinous processes and transverse processes Natural kyphotic shape,
Advances in MDCT of Thoracic Trauma
 Baltic Congress of Radiology, Riga 2010 Advances in MDCT of Thoracic Trauma Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General
Baltic Congress of Radiology, Riga 2010 Advances in MDCT of Thoracic Trauma Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General
Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury
 Blunt Thoracic Trauma HELI.CLI.09 Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury Procedure Management of Blunt Thoracic Traumatic Injury For Review
Blunt Thoracic Trauma HELI.CLI.09 Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury Procedure Management of Blunt Thoracic Traumatic Injury For Review
Chapter 13. Injuries to the Thorax and Abdomen
 Chapter 13 Injuries to the Thorax and Abdomen Anatomy Review Thoracic cage has 12 pairs of ribs. The first 7 pairs connect directly to sternum. Pairs 8 through 10 connect via common costal cartilage. Pairs
Chapter 13 Injuries to the Thorax and Abdomen Anatomy Review Thoracic cage has 12 pairs of ribs. The first 7 pairs connect directly to sternum. Pairs 8 through 10 connect via common costal cartilage. Pairs
Adult Intubation Skill Sheet
 Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Pneumothorax. Defined as air in the pleural space which can occur through a number of mechanisms
 Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA THE PREHOSPITAL APPROACH TO CHEST INJURY MANAGEMENT
 Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
Critical Care Monitoring. Indications. Pleural Space. Chest Drainage. Chest Drainage. Potential space. Contains fluid lubricant
 Critical Care Monitoring Indications 1-2- 2 Pleural Space Potential space Contains fluid lubricant Can fill with air, blood, plasma, serum, lymph, pus 3 1 Pleural Space Problems when contain abnormal substances:
Critical Care Monitoring Indications 1-2- 2 Pleural Space Potential space Contains fluid lubricant Can fill with air, blood, plasma, serum, lymph, pus 3 1 Pleural Space Problems when contain abnormal substances:
Procedure: Chest Tube Placement (Tube Thoracostomy)
") Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Evaluation & Management of Penetrating Wounds to the NECK
 Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
(SKILLS/HANDS-ON) Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC
 Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC") (SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
(SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
Thoracic Trauma The Spectrum
 Thoracic Trauma The Spectrum Joseph Mathew Consultant, s & Emergency dept. 2 Thoracic Trauma Responsible for 20-25% of all deaths attributed to trauma. Contributing cause of death in an additional 25%
Thoracic Trauma The Spectrum Joseph Mathew Consultant, s & Emergency dept. 2 Thoracic Trauma Responsible for 20-25% of all deaths attributed to trauma. Contributing cause of death in an additional 25%
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Dana Alrafaiah. - Moayyad Al-Shafei. -Mohammad H. Al-Mohtaseb. 1 P a g e
 - 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
- 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Thoracic trauma. 1 The majority of deaths occur after the. FEBRUARY 2001 The Surgical Technologist
 Thoracic trauma Richard Wills, MD, MBA, ACSM, Michael Norton, DC, and Kathryn DeLaney Approximately 25% of nonmilitary trauma-related deaths are due to thoracic trauma. 1 The majority of deaths occur after
Thoracic trauma Richard Wills, MD, MBA, ACSM, Michael Norton, DC, and Kathryn DeLaney Approximately 25% of nonmilitary trauma-related deaths are due to thoracic trauma. 1 The majority of deaths occur after
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Professional Development & Training MM3. Firefighter Prehospital Care Program. Maintenance Module 3 Course Mill Version
 Professional Development & Training MM3 Firefighter Prehospital Care Program F T Maintenance Module 3 Course Mill Version S Objectives Upon successful completion of the Firefighter Prehospital Care Maintenance
Professional Development & Training MM3 Firefighter Prehospital Care Program F T Maintenance Module 3 Course Mill Version S Objectives Upon successful completion of the Firefighter Prehospital Care Maintenance
Anatomy notes-thorax.
 Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
CHEST DRAIN PROTOCOL
 CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC
 Interpretation Brent Burbridge, MD, FRCPC") Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
Chest X-ray (CXR) Interpretation Brent Burbridge, MD, FRCPC An approach to reviewing a chest x-ray will create a foundation that will facilitate the detection of abnormalities. You should create your own
Initial Assessment and Management of the Trauma Patient
 Initial Assessment and Management of the Trauma Patient 1 Epidemiology Road Traffic Accidents are major cause of long term morbidity and mortality in developing nations WHO predicts that by 2020, Road
Initial Assessment and Management of the Trauma Patient 1 Epidemiology Road Traffic Accidents are major cause of long term morbidity and mortality in developing nations WHO predicts that by 2020, Road
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
Introduction (1 of 3)
") Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
H. Mitchell Shulman MDCM FRCPC CSPQ Assistant Professor, Dept. of Surgery, McGill Medical School Attending Physician, Royal Victoria Hospital,
 H. Mitchell Shulman MDCM FRCPC CSPQ Assistant Professor, Dept. of Surgery, McGill Medical School Attending Physician, Royal Victoria Hospital, Montreal General Hospital, McGill University Health Center
H. Mitchell Shulman MDCM FRCPC CSPQ Assistant Professor, Dept. of Surgery, McGill Medical School Attending Physician, Royal Victoria Hospital, Montreal General Hospital, McGill University Health Center
Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions
 NWC EMSS Sept 2017 CE: Head & Chest Trauma. Credit Questions - page 1 Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions Name: EMS Agency EMSC/Educator reviewer: Date
NWC EMSS Sept 2017 CE: Head & Chest Trauma. Credit Questions - page 1 Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions Name: EMS Agency EMSC/Educator reviewer: Date
Session Number 219 A BLUNT REVIEW OF THE PENETRATING ISSUES IN CHEST TRAUMA
 Session Number 219 A BLUNT REVIEW OF THE PENETRATING ISSUES IN CHEST TRAUMA Lisa C. Laphan-Morad, MSN, APN-C Administrative Director of Surgical & Ambulatory Services Nurse Practitioner Virtua Health Marlton,
Session Number 219 A BLUNT REVIEW OF THE PENETRATING ISSUES IN CHEST TRAUMA Lisa C. Laphan-Morad, MSN, APN-C Administrative Director of Surgical & Ambulatory Services Nurse Practitioner Virtua Health Marlton,
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
RCH Trauma Guideline. Management of Traumatic Pneumothorax & Haemothorax. Trauma Service, Division of Surgery
 RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
: TORSO & PELVIC TRAUMA
 INTRODUCTION Torso injuries include those involving the chest, back, flanks, and abdomen. This guideline also includes assessment and management of pelvic injuries. Neurological Trauma guideline and Management
INTRODUCTION Torso injuries include those involving the chest, back, flanks, and abdomen. This guideline also includes assessment and management of pelvic injuries. Neurological Trauma guideline and Management
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D.
 1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
LESSON ASSIGNMENT. LESSON 2 Heart Attack and Cardiopulmonary Resuscitation. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 2 Heart Attack and Cardiopulmonary Resuscitation. TEXT ASSIGNMENT Paragraphs 2-1 through 2-9. LESSON OBJECTIVES After completing this lesson, you should be able to: 2-1. Define
LESSON ASSIGNMENT LESSON 2 Heart Attack and Cardiopulmonary Resuscitation. TEXT ASSIGNMENT Paragraphs 2-1 through 2-9. LESSON OBJECTIVES After completing this lesson, you should be able to: 2-1. Define
5/2/2018. Notice. Putting Humpty Dumpty Back Together Again
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Kinetic Energy Energy in Motion KE = Mass (weight) X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT
 X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT") 1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
BELLWORK page 343. Apnea Dyspnea Hypoxia pneumo pulmonary Remember the structures of the respiratory system 1
 BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
BELLWORK page 343 Apnea Dyspnea Hypoxia pneumo pulmonary respiratory system 1 STANDARDS 42) Review case studies that involve persons with respiratory disorders, diseases, or syndromes. Citing information
Pediatric Trauma Care
 2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
Introduction to Advanced Trauma Life Support ATLS
 Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
Lines and tubes. 1 Nasogastric tubes Endotracheal tubes Central lines Permanent pacemakers Chest drains...
 Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
Pneumothorax and Chest Tube Problems
 Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 5 Respiratory Disorders. TEXT ASSIGNMENT Paragraphs 5-1 through 5-17. LESSON OBJECTIVES After completing this lesson, you should be able to: 5-1. Identify the characteristics,
LESSON ASSIGNMENT LESSON 5 Respiratory Disorders. TEXT ASSIGNMENT Paragraphs 5-1 through 5-17. LESSON OBJECTIVES After completing this lesson, you should be able to: 5-1. Identify the characteristics,
Thoracic Injuries. Chapter 16
 Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the torso. Those injuries involving the vasculature of the mediastinum (heart, great vessels, and pulmonary
Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the torso. Those injuries involving the vasculature of the mediastinum (heart, great vessels, and pulmonary
Internal Injury Documentation Guidelines
 Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
Chapter 16. Thoracic Injuries
 Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
Thoracic Trauma: 5/19/2010. Keihan Golshani, MD, Assistant Professor of emergency Medicine, Isfahan Medical University,
 Thoracic Trauma: 1 Thoracic trauma: A significant cause of mortality. Many patients with thoracic trauma: die after reaching the hospital Many of them can be prevented by: Prompt diagnosis and treatment.
Thoracic Trauma: 1 Thoracic trauma: A significant cause of mortality. Many patients with thoracic trauma: die after reaching the hospital Many of them can be prevented by: Prompt diagnosis and treatment.
CHAPTER 3. The Human Body National Safety Council
 CHAPTER 3 The Human Body The Human Body Composed of many different organs and tissues All parts work together: To sustain life Allow activity Injury or illness impairs functions 3-3 Cranial located in
CHAPTER 3 The Human Body The Human Body Composed of many different organs and tissues All parts work together: To sustain life Allow activity Injury or illness impairs functions 3-3 Cranial located in
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Thorax Lecture 2 Thoracic cavity.
 Thorax Lecture 2 Thoracic cavity. Spring 2016 Dr. Maher Hadidi, University of Jordan 1 Enclosed by the thoracic wall. Extends between (thoracic inlet) & (thoracic outlet). Thoracic inlet At root of the
Thorax Lecture 2 Thoracic cavity. Spring 2016 Dr. Maher Hadidi, University of Jordan 1 Enclosed by the thoracic wall. Extends between (thoracic inlet) & (thoracic outlet). Thoracic inlet At root of the
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress THE LAST GASP II: LUNGS AND THORAX David Holt, BVSc, Diplomate ACVS University of Pennsylvania School of Veterinary
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress THE LAST GASP II: LUNGS AND THORAX David Holt, BVSc, Diplomate ACVS University of Pennsylvania School of Veterinary
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
MANAGEMENT OF THORACIC TRAUMA. Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA
 MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
CHAPTER 3. The Human Body National Safety Council
 CHAPTER 3 The Human Body Lesson Objectives 1. Describe the primary areas of the body. 2. List the 10 body systems and explain a key function of each. 3. For each body system, describe at least 1 injury
CHAPTER 3 The Human Body Lesson Objectives 1. Describe the primary areas of the body. 2. List the 10 body systems and explain a key function of each. 3. For each body system, describe at least 1 injury
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Disclosure. Clinical Chest Radiography Interpretation Part I
 Clinical Chest Radiography Interpretation Part I Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma Surgery
Clinical Chest Radiography Interpretation Part I Anthony M. Angelow, PhD(c), MSN, ACNPC, AGACNP-BC, CEN Associate Lecturer, Fitzgerald Health Education Associates Clinical practice Division of Trauma Surgery
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Lung & Pleura. The Topics :
 Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
INTERNATIONAL TRAUMA LIFE SUPPORT
 INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
Pediatric Trauma Practice. Guideline for Management of the Child in Shock. Background
 Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
NEO 111 Melanie Jorgenson, RN, BSN
 NEO 111 Melanie Jorgenson, RN, BSN Inspection: performing deliberate, purposeful observations in a systematic manner Palpation: using the sense of touch Percussion: striking one object against another
NEO 111 Melanie Jorgenson, RN, BSN Inspection: performing deliberate, purposeful observations in a systematic manner Palpation: using the sense of touch Percussion: striking one object against another
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013
 Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Don t Panic! Dr. Karau s Guide to Respiratory Emergencies November 4, 2018
 Don t Panic! Dr. Karau s Guide to Respiratory Emergencies November 4, 2018 Objectives Oxygen delivery methods Emergent diagnostic tests Differentiating between upper and lower respiratory disease Respiratory
Don t Panic! Dr. Karau s Guide to Respiratory Emergencies November 4, 2018 Objectives Oxygen delivery methods Emergent diagnostic tests Differentiating between upper and lower respiratory disease Respiratory