Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
|
|
|
- Pearl Lynch
- 5 years ago
- Views:
Transcription
 FAST Unstable patients ; immediate transfer to the operating room (no time for imaging )")
1 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle decompression of PNX Circulation ;2 large bore IVs No more than 2 L crystalloids (early use of MTP) FAST Unstable patients ; immediate transfer to the operating room (no time for imaging ) Neck Injuries Zone I = clavicle to cricoid II =Cricoid to angle of mandible III= angle of mandible to base of skull Zones I and III require angiography before exploration,unless patient is severely unstable Zone II,controversial Stable = needs angio+laryngo+brochoscopy+ oesphago+gastrographin swallow Unstable needs surgical exploration What are the signs of instability? Large expanding or pulsatile haematoma-active external bleeding-hoarsness-subcutaneous emphysema-dysphagia-oropharngeal bleedneuro deficit.. 1

2 Internal juglar v= ligation Carotid= always repair even in hemiplegia. May need a graft. Only time to ligate is coma Vertebral artery =embolize if contralateral is intact.if found at exploration ligate Esophagus =repair with drainage in most cases.if delayed Dx or severe associated injuries do cervical oesphagostomy,ligate GE junction and Jejunostomy Larynx and trachea Tracheostomy.most are repaired by collar incision. For thoracic trachea =R thoracotomy Thoracic Duct =common in left subclavian inj.commonly missed at first exploration.effusion ;triglycerides>200.protein>3gm lymphocytes>60% Conservative ttt for three weeks. If fail =ligate.where to ligate Cardiac /thoracic trauma Cardiac trauma Patient may present with hypotension, and shock, haemothorax or in tamponade) Beck triad (Tamponade) ; distended neck veins- muffled heart sounds hypotension Shock with elevated CVP; Tamponade # tension PNX Difference > Air way pressure Cardiac trauma (diagnosis) Echocardiogram (FAST) Should be available in the ER. > 90 % sensitivity and specificity Pericardiocentesis Not a diagnostic test,only done for temporary relief of blood in the way to the OR. Blood is not clotted 2
 Indications")
 ER thoracotomy, open pericardium ER THORACOTOMY (Steps) Traumatic Rupture of Aorta Left anterolateral thoracotomy down to the table Control obvious source of bleeding e.")
3 Cardiac trauma (diagnosis) Subxiphoidal exploration (Pericardial window) Definitive diagnostic test in stable patient Good test to rule out tamponade in patients who do not have tamponade Positive pericardiocentesis or window = Blood = median sternotomy Most 95% cardiac injuries are repaired without Bypass Sub xiphoidal pericardial window ER ( RESUSCITATIVE THORACOTOMY ) Indications 1)penetrating chest injuries with failure of aggressive resusc to raise BP >80mmhg (12% survival) 2)penetrating chest or abd injuries who lost vitals during transfer 3) blunt injuries who had vitals before arrival (3% survival) ER thoracotomy, open pericardium ER THORACOTOMY (Steps) Traumatic Rupture of Aorta Left anterolateral thoracotomy down to the table Control obvious source of bleeding e.g left hilum Open pericardium,watch phrenic nerve If no injury is seen,extend to the right chest Open cardiac massage. Clamp the Aorta Rapid deceleration injury with shearing force Most common site is just distal to the left subclavian 60%. Followed by distal thoracic aorta 20% 60% die at the scene. 40 % make it to the hospital, third of which die during initial resuscitation 3
 1- control of bleeding (Suturing or resection) 2- Debridement of devitalized pancreatic tissues 3- leaving a drain 4- Ductal injury suspected (distal pancreatectomy")
- second part of duodenum can not be resected so")
4 Stents in thoracic aorta Abdominal trauma Penetrating ; GSW Laprotomy Stab wound ; may start with laparoscopy Blunt ; CT abdomen pelvis + FAST Pancreatic injury Principles of treating pancreatic injury ;(must open lesser sac ) 1- control of bleeding (Suturing or resection) 2- Debridement of devitalized pancreatic tissues 3- leaving a drain 4- Ductal injury suspected (distal pancreatectomy for head and tail which include injuries to the left of SMA, SMV ductal injury of head and neck are treated by drainage ) Duodenal injuries Simple lacerations with less than 50% circumferance are repaired primarily More complex injuries ; in first part of duodenum can be treated by resection (antrectomy and resection of first part of duodenum)- second part of duodenum can not be resected so repair has to be done with other complex manuvers e.g adding pyloric exclusion which is closing the pylorus with absorbable sutures which give 4 weeks for duodenum to heal before it re open. Another open to avoid stricture in large injuries is using jejunal serosal patch Whipple is only rarely used in very severe non reconstructable combined head pancreas and duodenal injury with distal common bile duct injury (mortality is very high in Whipple trauma) 4

5 Spleen injuiries Colon injuries Haemodynamically stable are treated non operatively with serial H/H. The presence of blush on CT scan is an indication of embolisation. Also grades IV and III Haemodynamically unstable need immediate splenectomy Primary repair is possible in most stab wounds For severe injuries, right colon can be resected with primary anastmosis (right hemicolectomy with ileotransverse anastomosis). Left colon may also be repaired primarly but has higher chance of leak compared to right Pelvic fractures Rectal injuries Should be suspected in bleeding per rectum in any trauma patient. Severe pelvic fracture patients. Diverting colostomy Hypovolemic shock Unstable patients to the OR for laparotomy, up to 40% have associated solid organ injury (liver, spleen) as the reason for shock Angioembolisation of hypogastric vessel External fixation Abdominal vascular trauma Retroperitoneal haematoma Zones Vascular Control (proximal distal) Supra celiac control 5

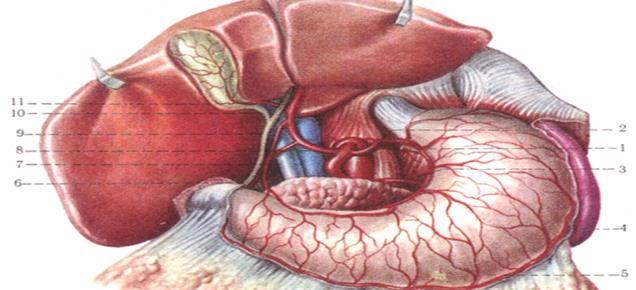




6 Visceral rotations 6
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Evaluation & Management of Penetrating Wounds to the NECK
 Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma
: Penetrating Cardiac Trauma") Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
Tips & Techniques in Operative Surgery II: Neck Exploration
 Tips & Techniques in Operative Surgery II: Neck Exploration ศ.ดร.นพ. พรช ย โอเจร ญร ตน สาขาว ชาศ ลยศาสตร ศ รษะ-คอ และเต านม ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Indications to Explore a Neck Removing
Tips & Techniques in Operative Surgery II: Neck Exploration ศ.ดร.นพ. พรช ย โอเจร ญร ตน สาขาว ชาศ ลยศาสตร ศ รษะ-คอ และเต านม ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Indications to Explore a Neck Removing
Penetrating Neck Trauma. Herve J. LeBoeuf, MD Francis B. Quinn, MD
 Penetrating Neck Trauma Herve J. LeBoeuf, MD Francis B. Quinn, MD Introduction 5-10% of all trauma Overall mortality rate as high as 11% Major vessel injury fatal in 65%, including prehospital deaths Attending
Penetrating Neck Trauma Herve J. LeBoeuf, MD Francis B. Quinn, MD Introduction 5-10% of all trauma Overall mortality rate as high as 11% Major vessel injury fatal in 65%, including prehospital deaths Attending
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Emergency Department Thoracotomy
 Emergency Department Thoracotomy November 3, 2017 North Oaks Shock Trauma Symposium Jeremy R. Timmer, M.D., FACS Objectives Background of RT Indications for RT Contraindications for RT Survival Benefits
Emergency Department Thoracotomy November 3, 2017 North Oaks Shock Trauma Symposium Jeremy R. Timmer, M.D., FACS Objectives Background of RT Indications for RT Contraindications for RT Survival Benefits
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
CHEST TRAUMA. Dr Naeem Zia FCPS,FACS,FRCS
 CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Acute Pericardial Tamponade
 Acute Pericardial Tamponade Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed. Epidemiology The reported incidence of acute pericardial tamponade is approximately 2% in patients
Acute Pericardial Tamponade Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed. Epidemiology The reported incidence of acute pericardial tamponade is approximately 2% in patients
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
The Management of Chest Trauma. Tom Scaletta, MD FAAEM Immediate Past President, AAEM
 The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
Surgical Training for Austere Environments
 Surgical Training for Austere Environments Programme Course Director: Mr Vascular and Trauma Surgeon, St Marys Hospital, London Acknowledgements The Royal College of Surgeons of England is a charitable
Surgical Training for Austere Environments Programme Course Director: Mr Vascular and Trauma Surgeon, St Marys Hospital, London Acknowledgements The Royal College of Surgeons of England is a charitable
Trauma Workshop! Skills Centre, St George Hospital! Saturday 15 March 2014!
 Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
CHEST INJURIES. Jacek Piątkowski M.D., Ph. D.
 CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Pre-Hospital and Emergency Department Resuscitative Thoracotomy
 Pre-Hospital and Emergency Department Programme Directors: Mr Jim Connolly Consultant A&E Surgeon Accident and Emergency Department, Royal Victoria Infirmary Dr Paul Wallman Consultant in Emergency Medicine
Pre-Hospital and Emergency Department Programme Directors: Mr Jim Connolly Consultant A&E Surgeon Accident and Emergency Department, Royal Victoria Infirmary Dr Paul Wallman Consultant in Emergency Medicine
ED Thoracotomy Left chest opened and extended across sternum with 1000mL blood drained Pericardium opened with 100mL blood drained 1cm laceration in t
 Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Priorities in Penetrating Chest Trauma
 Priorities in Penetrating Chest Trauma K. Inaba, MD FRCSC FACS Division of Trauma Surgery & Critical Care LAC+USC Medical Center University of Southern California ü None. DISCLOSURES OBJECTIVES ü Practical
Priorities in Penetrating Chest Trauma K. Inaba, MD FRCSC FACS Division of Trauma Surgery & Critical Care LAC+USC Medical Center University of Southern California ü None. DISCLOSURES OBJECTIVES ü Practical
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT
 The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
Chest Trauma.
 Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
INJURIES CHEST, ABDOMEN, LIMBS. FN Brno November 2011
 INJURIES CHEST, ABDOMEN, LIMBS FN Brno November 2011 Injury Chest Abdomen Limbs Injury to the rib cage Fractured one or more ribs Sharp pain at the site of fracture Pain on taking a deep breath Shallow
INJURIES CHEST, ABDOMEN, LIMBS FN Brno November 2011 Injury Chest Abdomen Limbs Injury to the rib cage Fractured one or more ribs Sharp pain at the site of fracture Pain on taking a deep breath Shallow
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
A CASE PRESENTATION AND DISCUSSION ON HEAD AND NECK TRAUMA
 A CASE PRESENTATION AND DISCUSSION ON HEAD AND NECK TRAUMA Nolan Ortega Aludino, M.D. Department of Surgery Ospital ng Maynila Medical Center General Data: B.R. 64 year old Male Tondo Manila Chief Complaint:
A CASE PRESENTATION AND DISCUSSION ON HEAD AND NECK TRAUMA Nolan Ortega Aludino, M.D. Department of Surgery Ospital ng Maynila Medical Center General Data: B.R. 64 year old Male Tondo Manila Chief Complaint:
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Exam. On call that evening
 On call that evening 27 y/o M, law student, GSW R. chest x 2 Breathing comfortably, phonating BP 118/p, 83, 22, GCS=15 A&A&O one GSW, R. axilla one GSW, R. lateral chest, ~ 3 rd intersp. One bullet palpable,
On call that evening 27 y/o M, law student, GSW R. chest x 2 Breathing comfortably, phonating BP 118/p, 83, 22, GCS=15 A&A&O one GSW, R. axilla one GSW, R. lateral chest, ~ 3 rd intersp. One bullet palpable,
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die
 account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Chapter 16. Thoracic Injuries
 Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
Emergency Department Thoracotomy. Khalid Al Johani. MD EM & Trauma consultant
 Emergency Department Thoracotomy Khalid Al Johani. MD EM & Trauma consultant Background Thoracic trauma is one of the leading causes of death worldwide in all age groups and accounts for 25-50% of all
Emergency Department Thoracotomy Khalid Al Johani. MD EM & Trauma consultant Background Thoracic trauma is one of the leading causes of death worldwide in all age groups and accounts for 25-50% of all
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA THE PREHOSPITAL APPROACH TO CHEST INJURY MANAGEMENT
 Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
Traumatic A-V A V Fistula
 Traumatic A-V A V Fistula PRESENT HISTORY PAST HISTORY 30 year-old, male ( XX); Denied other systemic disease before. PRESENT HISTORY A deep stabbing wound (3*1 cm) noted on 07/01/2002 over Right anterior
Traumatic A-V A V Fistula PRESENT HISTORY PAST HISTORY 30 year-old, male ( XX); Denied other systemic disease before. PRESENT HISTORY A deep stabbing wound (3*1 cm) noted on 07/01/2002 over Right anterior
Arteriovenostomy for renal dialysis 39.27, 39.42
 Surgery categories NHSN Surgery codes (Reference: NHSN Operative Procedure Category Mappings to ICD-9-CM Codes, October 2010 www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf) Operative aortic aneurysm
Surgery categories NHSN Surgery codes (Reference: NHSN Operative Procedure Category Mappings to ICD-9-CM Codes, October 2010 www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf) Operative aortic aneurysm
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
PEDIATRIC PENETRATING TRAUMA. Laura Boomer 11/18/15
 PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Oral and Maxillofacial Surgeons and the seriously injured patient. Barts and The London NHS Trust
 Oral and Maxillofacial Surgeons and the seriously injured patient Barts and The London NHS Trust How do you assess this? Primary Survey A B C D E Airway & Cervical Spine Breathing & Ventilation Circulation
Oral and Maxillofacial Surgeons and the seriously injured patient Barts and The London NHS Trust How do you assess this? Primary Survey A B C D E Airway & Cervical Spine Breathing & Ventilation Circulation
TEVAR FOR! THORACIC AORTIC TRAUMA"
 10th HKL Vascular Surgery Conference and Workshop" TEVAR FOR! THORACIC AORTIC TRAUMA" Dr Hanif Hussein" Vascular and General Surgeon" Department of Surgery" Hospital Kuala Lumpur" Source: MIROS! Thoracic
10th HKL Vascular Surgery Conference and Workshop" TEVAR FOR! THORACIC AORTIC TRAUMA" Dr Hanif Hussein" Vascular and General Surgeon" Department of Surgery" Hospital Kuala Lumpur" Source: MIROS! Thoracic
Thoracic Injuries. Chapter 16
 Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the torso. Those injuries involving the vasculature of the mediastinum (heart, great vessels, and pulmonary
Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the torso. Those injuries involving the vasculature of the mediastinum (heart, great vessels, and pulmonary
Ballistic Trauma. L Yuko Shimotake, MD Kings County Hospital Center September 22, 2016
 Ballistic Trauma L Yuko Shimotake, MD Kings County Hospital Center September 22, 2016 Case Presentation Most cases at Kings County Hospital Case Presentation HPI: 22yo male presented as Level I Trauma
Ballistic Trauma L Yuko Shimotake, MD Kings County Hospital Center September 22, 2016 Case Presentation Most cases at Kings County Hospital Case Presentation HPI: 22yo male presented as Level I Trauma
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
ISPUB.COM. Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots. B Phillips CASE REPORT THE OPERATING ROOM
 ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
Internal Injury Documentation Guidelines
 Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
THORACIC AORTIC DISSECTION
 The Essence of Aortic Dissection THORACIC AORTIC DISSECTION Aortic dissection can be classified as acute if it s onset has been less than 14 days or chronic if its onset has been more than 14 days. Mortality
The Essence of Aortic Dissection THORACIC AORTIC DISSECTION Aortic dissection can be classified as acute if it s onset has been less than 14 days or chronic if its onset has been more than 14 days. Mortality
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Penetrating Cardiac Injury
 Penetrating Cardiac Injury Getting to the Heart of the Matter Marilyn Ng, MD Dept. of Surgery Conference Downstate Medical Center Aug 11, 2011 Case Presentation 28 yo M with unknown PMHx Level 1 notification
Penetrating Cardiac Injury Getting to the Heart of the Matter Marilyn Ng, MD Dept. of Surgery Conference Downstate Medical Center Aug 11, 2011 Case Presentation 28 yo M with unknown PMHx Level 1 notification
: Your Haemorrhage Control Solution
 : Your Haemorrhage Control Solution Shoulder Injury Leg Injury TM HAEMORRHAGE New solutions to control difficult bleeding are needed in emergent care, including pre-hospital, hospital and tactical environments.
: Your Haemorrhage Control Solution Shoulder Injury Leg Injury TM HAEMORRHAGE New solutions to control difficult bleeding are needed in emergent care, including pre-hospital, hospital and tactical environments.
BODY SYSTEMS BODY CAVITIES THE RESPIRATORY SYSTEM. Movements BODY CAVITIES. Pediatric Considerations In Respiratory System
 BODY SYSTEMS A body system is a group of organs and other structures work together to carry out specific functions. The following systems work together to carry out a function needed for life: Respiratory
BODY SYSTEMS A body system is a group of organs and other structures work together to carry out specific functions. The following systems work together to carry out a function needed for life: Respiratory
Having an operation on the pancreas
 Having an operation on the pancreas Let us assume you (the reader) are going to have a pancreatic resection. The following section attempts to answer some of the questions you may have in mind, and the
Having an operation on the pancreas Let us assume you (the reader) are going to have a pancreatic resection. The following section attempts to answer some of the questions you may have in mind, and the
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic
 Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Emergency Approach to the Subclavian and Innominate Vessels
 Emergency Approach to the Subclavian and Innominate Vessels Joseph J. Amato, M.D., Robert M. Vanecko, M.D., See Tao Yao, M.D., and Milton Weinberg, Jr., M.D. T he operative approach to an acutely injured
Emergency Approach to the Subclavian and Innominate Vessels Joseph J. Amato, M.D., Robert M. Vanecko, M.D., See Tao Yao, M.D., and Milton Weinberg, Jr., M.D. T he operative approach to an acutely injured
Epidemiology. 16% incidence in knee. dislocation
 Epidemiology Highest risk group: Young male between 15 and 45 years (USA) Mortality Ratio after trauma : male/female: 7/1 Peripheral vascular injuries : 70%-80% of all cases of vascular trauma : Vascular
Epidemiology Highest risk group: Young male between 15 and 45 years (USA) Mortality Ratio after trauma : male/female: 7/1 Peripheral vascular injuries : 70%-80% of all cases of vascular trauma : Vascular
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D.
 1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
9/10/2012. Chapter 49. Learning Objectives. Learning Objectives (Cont d) Thoracic Trauma
 Thoracic Trauma") Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
Initial Management of Pelvic Injuries
 Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 29 - Chest Injuries
 1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
May Clinical Director, Peninsula Trauma Network (Edited for PTN)
") Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)