Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None
|
|
|
- Agnes Gallagher
- 5 years ago
- Views:
Transcription
, FACC,")
 None Off")
1 Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1


2 2,000 Noninvasive Procedures 1,600 Units of Service/ 1,000 Beneficiaries 1, Evaluation and Management 400 Invasive Procedures Andrus and Welch, Circ Cardiovasc Qual Outcomes. 2012;5: Journal of Cardiac Failure Vol. 20 No
3 Appropriate Use ECG uninterpretable Symptomatic Unable to exercise Intermediate (10-90%) to high (>90%) pretest likelihood** Asymptomatic Typical (Definite): 1. Substernal chest pain or discomfort; 2. provoked by exertion or emotional stress; 3. relieved by rest and/or nitrogylcerin Atypical (Probable): Chest pain or discomfort that lacks one of the Characteristics for definite or typical angina. Nonanginal Chest Pain: Chest pain or discomfort that meets one or none of the Typical angina characteristics. 3
 Reduced Perfusion Decline in function Abnormal ECG Symptoms Occlusion Time Sensitivity")
4 Appropriate Use ECG uninterpretable Symptomatic Asymptomatic Unable to exercise Intermediate (10-90%) to high (>90%) pretest likelihood** High risk of CAD event or Intermediate risk (unable to exercise or ECG uninterpretable^ High Coronary Calcium Score (> AU) Reduced Perfusion Decline in function Abnormal ECG Symptoms Occlusion Time Sensitivity Specificity 4
 Significant prognostic implications for predicting Mortality and MACE.")

5 16.7% of patients who did not develop chest pain or ischemic ECG changes developed new or worsening regional wall motion abnormalities (+ Exercise Echo) Significant prognostic implications for predicting Mortality and MACE. J Am Coll Cardiol 2009;53: Characteristics and Outcomes of Patients With Abnormal Stress Echocardiograms and Angiographically Mild Coronary Artery Disease <50% Stenosis or Normal Coronary Arteries J Am Soc Echocardiogr 2010;23:
 <50% stenoses ( false-positive ) 50%")

6 Surviving Surviving 4/4/2017 Dobutamine Outcome Exercise <50% stenoses ( false-positive ) <50% stenoses ( false-positive ) 50% stenoses ( true-positive ) 50% stenoses ( true-positive ) P=0.13 P=0.49 Years Years From et al. J Am Soc Echocardiogr 2010;23:

7 73 year old male No antecedent CV disease history. Asymptomatic Reduced functional capacity due to orthopedic limitations Hypertension, diabetes Pre-operative cardiac risk stratification prior to an orthopedic procedure Ischemic Heart Disease, Cerebral Vascular Disease, Compensated or prior heart failure, Diabetes (requiring insulin), Renal Insufficiency (Scr > 2.0) May be appropriate Appropriate Poor or Unknown Functional Capacity (<4 METs) - Intermediate-risk surgery - > 1 clinical risk factor - Vascular surgery - > 1 clinical risk factor - Kidney Transplant - Liver Transplant Journal of Cardiac Failure Vol. 20 No




8 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery 8

9 9
10 10


11 1. Stress Modalities 2. Interpretation 3. Test Characteristics: Diagnosis 4. Prognostic Value 5. Safety 6. Other Uses 7. Appropriate Use 11






12 Modalities Treadmill Bicycle -Supine -Upright Pharmacologic Dobutamine / Atropine Vasodilator -Dipyradamole -Adenosine Other Handgrip Pacing Rest A4C Treadmill Stress A4C Most common is multistage Bruce protocol Modified Stress Bruce and Naughton Stress protocols are lower intensity A4C exercise protocols A4C used in those with limited exercise capacity Cornell protocol provides a more gradual increase in speed and incline compared to the Bruce protocol 12
.")

13 Bicycle The cycles are calibrated in kiloponds or Watts which can then be converted to metabolic equivalents (METs). It may allow image acquisition during exercise Doppler information. Hemodynamic Effects Duration and Maximum Workload > Heart Rate > End-diastolic Volume > Mean Arterial Pressure > Wall Stress > Myocardial Oxygen Demand > Filling Pressures > 13
 Technical difficulties with ECG or blood pressure monitoring Patient s desire to stop Indications To Stop Relative Arrhythmias other than")

 As dobutamine dose increases there is a greater β-2 response resulting in peripheral vasodilation which may lead to a drop in BP")
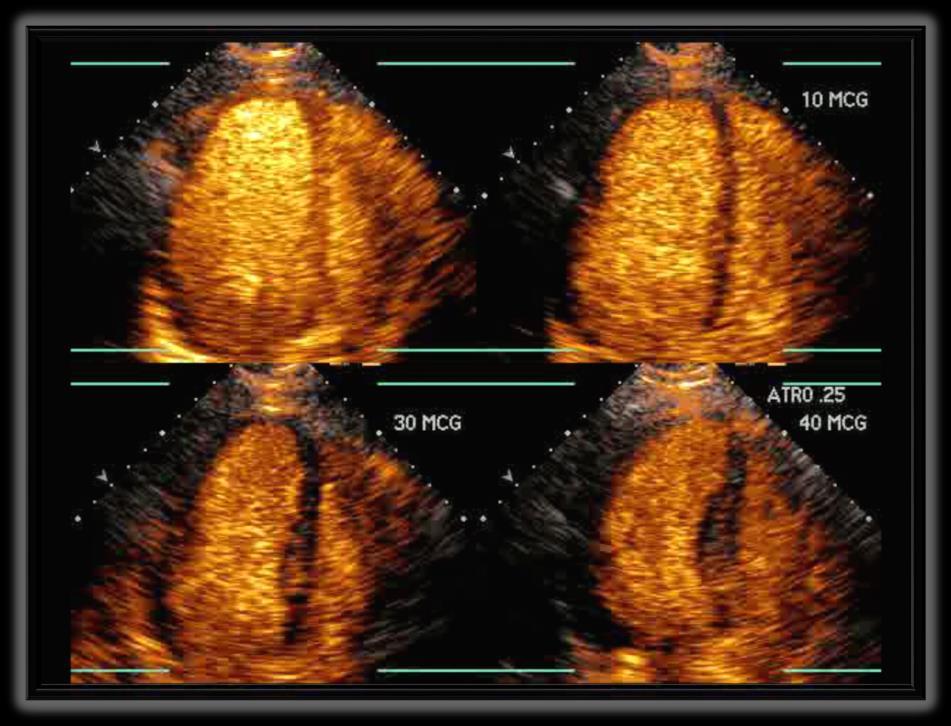
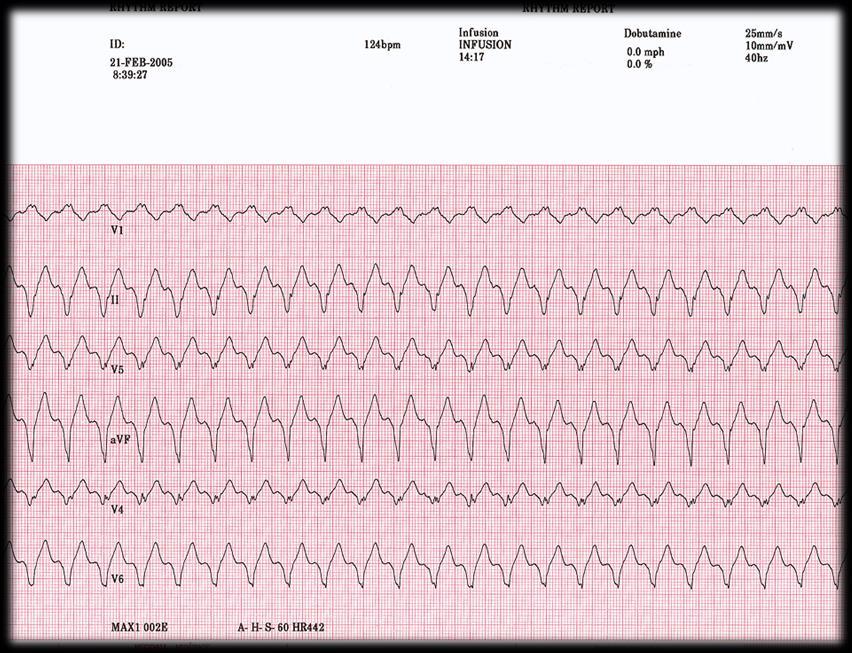
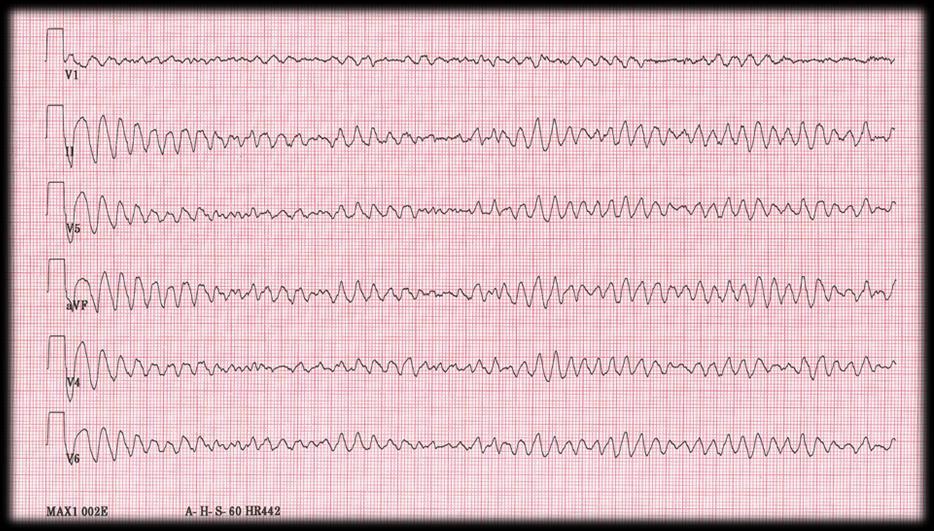
14 Absolute ST elevation 1 mm in leads without Q waves Ventricular tachycardia Decrease in systolic blood pressure > 10 mm Hg from baseline with other signs of ischemia Moderate to severe angina Nervous system symptoms Signs of poor perfusion (cyanosis, pallor) Technical difficulties with ECG or blood pressure monitoring Patient s desire to stop Indications To Stop Relative Arrhythmias other than ventricular tachycardia ST or QRS changes including horizontal or downsloping ST depression > 2 mm Development of bundle branch block or intraventricular conduction delay that cannot be distinguished from ventricular tachycardia Increasing chest pain Decrease in systolic blood pressure > 10 mm Hg from baseline without other signs of ischemia Fatigue, shortness of breath, wheezing, leg cramps, claudication Hypertensive response (> 250 mm Hg systolic and/or > 115 mm Hg diastolic) Pharmacologic Inotropic / Dobutamine Dobutamine acts directly on β-1 adrenergic receptors Increase in HR and Contractility (4x in normal subjects and < 2x in those with DCM) As dobutamine dose increases there is a greater β-2 response resulting in peripheral vasodilation which may lead to a drop in BP Compared with exercise LV volumes and wall stress increase less with dobutamine. 14




15 Pharmacologic Vasodilators Dipyridamole, adenosine, regadenoson Small decrease in BP and increase in HR If obstructive epicardial disease or microcirculatory dysfunction Heterogeneity of coronary blood flow between areas subtended by stenosis Vs. normal coronary arteries. Lang RM et al. J Am Soc Echocardiogr 2015;28:

 No")
16 Lang RM et al. J Am Soc Echocardiogr 2015;28:1-39 Interpretation Change in LV Ejection Fraction Increase EF: Normal (global contractile reserve in patients with no resting dysfunction is defined by > 5% increase in LVEF) No change or decrease: Abnormal Change in LV end-systolic size / volume Decrease: Normal (Flow reserve is defined by > 20% increase in forward stroke volume) No change or increase: Abnormal (**supine bike) Regional LV Function Evaluation Wall thickening, Wall motion Score Index 16
 2 = Hypokinetic: delay in the velocity or onset of")


17 1 = Normal or hyperdynamic: (systolic increase in thickness >50%) 2 = Hypokinetic: delay in the velocity or onset of contraction (<30-40% systolic increase in thickness) 3 = Akinesis or minimal thickening: <10% 4 = Dyskinetic: Systolic outward motion of the segment 5 = Aneurysmal: Bulging during systolic and diastole Wall Motion Score Index = 1.0 Wall Motion Score Index = 38/16 =
18 Rest Stress Interpretation Normokinetic Normal-hyperkinetic Normal Normokinetic Hypokinetic Resting Dysfunction Resting Dysfunction Wall Motion abnormality (segment worsens function) Akinetic / Dyskinetic (segment worsens function) Fixed / No Change in Function Slow Sustained Improvement Ischemic Response Ischemic Response Infarct / Necrotic Stunning or Cardiomyopathy Resting Dysfunction Biphasic Response Hibernating Akinetic Dyskinetic Passive / Mechanical Wall Motion Abnormalities at Rest Ischemic heart disease -Infarction -Stunned / Hibernating Conduction -Pacing -LBBB Cardiomyopathy Myocarditis Right ventricular volume / pressure overload 18


19 Function Function Function 4/4/2017 Blood Flow Ventricular Function Time Dobutamine Dose Blood Flow Time Ventricular Function 19

20 Wall Motion Abnormalities at Rest Ischemic heart disease -Infarction -Stunned / Hibernating Conduction -Pacing -LBBB Cardiomyopathy Myocarditis Right ventricular volume / pressure overload Conduction 20

21 Lang RM et al. J Am Soc Echocardiogr 2015;28:1-39 Conduction 21




22 Wall Motion Abnormalities Wall Motion Abnormalities at Rest during Stress Ischemic heart Ischemia disease with -Infarction obstructive epicardial -Stunned / Hibernating CAD Ischemia in the absence of epicardial obstruction -hypertensive response Conduction -Pacing -LBBB -microvascular disease Cardiomyopathy Myocarditis Cardiomyopathy Right ventricular Rate-related volume / LBBB pressure overload Pulmonary Diameter Stenosis < 85% narrow rest > 50% narrowing stress - collaterals - level of exertion/stress - wall thickness 22
 Lieberman et al.")
23 Systolic Thickening (%) 4/4/2017 p< p< p = Infarct Thickness (%) Lieberman et al. Circulation 1981;63; Chordal Center Line Analysis (Centroids)



24 = Infarct = Tethered = Normal





25 Floating Epicardial 1 Center of Mass 8 2 Centroid Exercise Echo Dobutamine Echo 86 SPECT % Sensitivity Specificity Schuijf Eur J Nucl Med Mol Imaging 2006;33:93 25
26 100 Patients Pre test Likelihood 10% CAD + 10 pts Sensitivity = 90% Specificity = 80% CAD - 90 pts false - 1 pts True + 9 pts false + 18 pts 27 + tests: 33% positive predictive value True - 72 pts CAD + 40 pts 100 Patients Pre test Likelihood 40% Sensitivity = 90% Specificity = 80% CAD - 60 pts false - 4 pts True + 36 pts false + 12 pts 48 + tests: 75% positive predictive value True - 48 pts 26



27 Diagnostic Criteria Sensitivity 1 Segment, > 1 Segment, LV dilation Specificity Exercise Echo vs SPECT Tl % Ex Echo SPECT TI vessel 2 vessels 3 vessels Sensitivity Specificity Quinones et al: Circ,



28 Risk of adverse event Prognosis Detection/Exclusion CAD Diagnosis Physical or Pharmacologic Very Low Risk < 1% per year risk of MI, cardiac death or late revascularization Low Risk 1-3% per year risk of MI, cardiac death or late revascularization -submaximal stress (men <7 METS, women < 5 METS) -LVEF <40% Mertz et al. J Am Coll Cardiol 2007;49: Sicari et al. European Heart Journal (2009) 30,
 47 (0.7%) Supervised <0.001 55 (0.36%) by Arrhythmia Registered Requiring Nurses: Rx 4 (0.")
 VT / VF 0 6 (0.09%) <0.005 6 (0.")
 5 (0.07) 0.56 8 (0.05%) 1 (0.01%) 3 (0.04%) 0.44 4 (0.03%) Transfer to Hospital 5 J (0.")
29 ExEcho n=8592 DSE n= 6755 P value Total n = 5349 Safety Overall Complication of Stress RateEchocardiography 8 (0.09%) 47 (0.7%) Supervised < (0.36%) by Arrhythmia Registered Requiring Nurses: Rx 4 (0.05%) Results 39 (0.58%) of a 2-Year <0.001 Audit 43 (0.28%) of 15,404 Patients SVT / AF 4 (0.05%) 33 (0.49%) < (0.24%) VT / VF 0 6 (0.09%) < (0.04%) Markedly + / Prolonged CP requiring hospitalization Symptomatic hypotension requiring hospitalization 3 (0.03%) 5 (0.07) (0.05%) 1 (0.01%) 3 (0.04%) (0.03%) Transfer to Hospital 5 J (0.06%) Am Soc21 Echocardiogr (0.31%) :21; (0.17) Cardiac Rupture or Death


30 J Am Soc Echocardiogr 2005;18:63-8 What do we expect? E vel e vel 30


31 55 year old male No known CAD Hypertension & exertional dyspnea 31




32 Pre Post E=0.6 E/e =8 E=0.9 E/e =8 e =0.8 e = year old male No known CAD Diabetes and hypertension Complains of dyspnea on exertion (NYHA II) 32



33 E/e =6 Pre E=0.5 Post E/e =14 E=1.1 e =0.8 e =



34 Recovery 5 min Ha et al J Am Soc Echocardiol 2005;18:63-8 Those with increased filling pressure at baseline will further increase filling pressure with exercise Therefore, those who benefit most from diastolic stress testing are those with normal resting LVFP but abnormal relaxation (grade I) 34


35 Courtesy Rob McCully Ischemia 4% 10% 5% 8% Elevated LVFP Pulm HTN 6% 7% 14% None 46% Ischemia 27% Pulmonary HTN 22% Elevated LVFP 34% Any abnormality 54% n=630 Elevated LVFP: ex. E/e >13 Pulm HTN: ex. RVSP >50 mm Hg Women <5 METs, Men <7 METS Courtesy Rob McCully Ischemia 6.3% 12.5% 11.7% 6.3% 7% 11.7% Elevated LVFP 19.5% Pulm HTN Ischemia 32% Pulmonary HTN 36% Elevated LVFP 45% Any abnormality 75% n=128 None 25% Elevated LVFP: ex. E/e >13 Pulm HTN: ex. RVSP >50 mm Hg 35





36 Mayo Clinic, Rochester, MN Baseline EF, RWMAs, valves Color flow + LA Volume Diastolic E, A,E/A, Function DT RV e, systolic E/e pressure TR Vmax Post-exercise Quads for EF, LVESV resp, RWMAs + Then TR Vmax RV systolic pressure LV filling Thenpressure E, e, E/e Depressed EF / Myocardial Disease and Normal EF When Is Diastolic Stress Testing Indicated? E/A < E < 50cm/s E/A < E > 50 cm/ OR E/A > < 2 Rule of 2 s E/A > 2 Normal LAP Grade I DD 1. > Av 2 negative E/e > TR > 2.8 m/s 3. LA vol > 34 cc/m 2 If symptomatic - Consider CAD - Proceed to Diastolic Stress Test Grade III DD 36

 E/e < 10 2. Peak TR velocity < 2.")

37 RVSP (mm Hg) RVSP (mm Hg) 4/4/2017 Interpretation t Definitely Abnormal 1. Average E/e > 14 or Septal >15 2. Septal e < 7 cm/sec or J Am Soc Echocardiogr 2016;29: Lateral e < 10 cm/sec 3. Peak TR velocity > 2.8 m/sec Normal 1. Average (or septal) E/e < Peak TR velocity < 2.8 m/sec Post-TM Exercise % limit Age group (yr) < mean Rest % limit mean 10 Age group (yr) < RAP 5 mm Hg Kane et al (n=469), Slide courtesy Rob McCully 37


38 1. Exertional dyspnea portends a poor prognosis (> angina). 2. An exercise induced increase in E/e relates to changes in filling pressure and its finding has adverse prognostic significance. 3. The post exercise E/e can be measured minutes into recovery, ideally as soon as the discrete waves are appreciated. 4. The ideal patient is one with exertional dyspnea and baseline grade I diastolic dysfunction. 38

 determine prognosis.")
39 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease Class IIa Exercise testing is reasonable in selected patients with asymptomatic severe VHD to 1) confirm the absence of symptoms, or 2) assess the hemodynamic response to exercise, or 3) determine prognosis. (Level of Evidence: B) J Am Soc Echocardiogr 2017;30:

 severity not matching with symptoms Asymptomatic moderate-severe VHD (MR, MS, AR, AS) Symptoms, Δ blood")
40 Asymptomatic (Stage C) LVEF > 50% LVESD < 50mm LVEDD < 65mm LVEF > 50% Vmax <5m/s ΔPmean <60mmHg Normal ETT ΔVmax <0.3m/s/yr LVEF >60% LVESD <40mm Sinus Rhythm PASP <50mmHg Successful Repair <95% Or Mortality >1% Very Severe MVA<1cm 2 T 1/2 > Unfavorable morphology, LA clot, > mild MR Severe MVA<1.5cm 2 T 1/2 > 150 -Sinus rhythm -Afib with unfavorable morphology, LA clot, > mild MR Positive Stress Test Aortic Regurgitation* Aortic Stenosis Mitral Regurgitation Mitral Stenosis (rheumatic) Active Valve Surveillance Intervention *ACC/AHA not ESC guidelines VHD (MR, MS, AR, AS) severity not matching with symptoms Asymptomatic moderate-severe VHD (MR, MS, AR, AS) Symptoms, Δ blood pressure, exercise tolerance Valve Ventricle Hemodynamics Δ 18-20mmHg MPG in AS MPG >15-18mmHg in MS >10-13mm 2 EROA in MR Δ < 4-5% LVEF (lack of CR) Δ < 2% GLS (lack of CR) Δ SV < 20% (lack or FR) Δ E/e (LV filling pressure) Δ WMSI (ischemia) PH (SPAP > 60mmHg) LV dyssynchrony RV dysfunction (TAPSE < 19mm) Match symptoms with the cardiac involvement Risk stratification Guide decision making and guide optimal timing for valve intervention J Am Soc Echocardiogr 2017;30:
 with a AVA < 1.0cm AV Area 2 valve area < 1.")
41 Baseline Doppler hemodynamics Class IIa AVR is reasonable in symptomatic patients with lowflow/low-gradient severe AS with reduced LVEF (stage D2) with a low-dose dobutamine stress study that shows an Vmax aortic Mean > velocity 4.0m/sec gradient > m/s (or mean pressure Mean gradient > 40 mm Hg) with a AVA < 1.0cm AV Area 2 valve area < 1.0 cm2 at any AV Area dobutamine dose True Severe AS (D2) IIa Pseudo Severe AS 1. Understand the differences and indications for the various stress modalities. 2. Know the walls and their coronary supply. 3. Understand the methods and interpretation of wall motion. 4. Viability: stunning versus hibernation. 5. Understand the test characteristics. 6. Emerging uses: Valve Disease and SOB. 7. Appropriate use. 41
42 42
Exercise Test: Practice and Interpretation. Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine
 Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이
 Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
Tissue Doppler and Strain Imaging
 Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Tissue Doppler and Strain Imaging
 Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
History of Stress Testing. Disclosure. Overview. Stress Echocardiography New Applications. and Comparison with Other Stress.
 Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ;
 Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Getting the Most Out of Stress Echo
 Getting the Most Out of Stress Echo Vera H. Rigolin, MD, FASE, FACC, FAHA Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern
Getting the Most Out of Stress Echo Vera H. Rigolin, MD, FASE, FACC, FAHA Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Michigan Society of Echocardiography 30 th Year Jubilee
 Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Stress ECG is still Viable in Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh
 Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Risk Stratification for CAD for the Primary Care Provider
 Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress echo workshop STRESSORS
 Stress echo workshop STRESSORS Adham Ahmed, MD Lecturer of Cardiology, Ain Shams Indications of Stress Echo CAD Diagnosis Prognosticat ion 1 Physiologic Basis 1930s: Tennant and Wiggers Relationship between
Stress echo workshop STRESSORS Adham Ahmed, MD Lecturer of Cardiology, Ain Shams Indications of Stress Echo CAD Diagnosis Prognosticat ion 1 Physiologic Basis 1930s: Tennant and Wiggers Relationship between
Cardiovascular Imaging Stress Echo
 Cardiovascular Imaging Stress Echo Theodora A Zaglavara, MD, PhD Cardiac Imaging Department INTERBALKAN MEDICAL CENTER Thessaloniki GREECE Evolution of Stress Echo: From Innovation to a Widely Established
Cardiovascular Imaging Stress Echo Theodora A Zaglavara, MD, PhD Cardiac Imaging Department INTERBALKAN MEDICAL CENTER Thessaloniki GREECE Evolution of Stress Echo: From Innovation to a Widely Established
CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O.
 CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O. INTRODUCTION Form of imprisonment in 1818 Edward Smith s observations TECHNIQUE Heart rate Blood pressure ECG parameters Physical appearance INDICATIONS
CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O. INTRODUCTION Form of imprisonment in 1818 Edward Smith s observations TECHNIQUE Heart rate Blood pressure ECG parameters Physical appearance INDICATIONS
Affecting the elderly Requiring new approaches. Echocardiographic Evaluation of Hemodynamic Severity. Increasing prevalence Mostly degenerative
 Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Contra-indications, Risks, and Safety Precautions for Stress Testing. ACSM guidelines, pg 20 7 ACSM RISK FACTORS. Risk Classifications pg 27
 Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
1. LV function and remodeling. 2. Contribution of myocardial ischemia due to CAD, and
 1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Echo in CAD: Wall Motion Assessment
 Echo in CAD: Wall Motion Assessment Joe M. Moody, Jr, MD UTHSCSA and STVHCS October 2007 Relevant References ACC/AHA/ASE 2003 Guideline Update for the Clinical Application of Echocardiography Bayes de
Echo in CAD: Wall Motion Assessment Joe M. Moody, Jr, MD UTHSCSA and STVHCS October 2007 Relevant References ACC/AHA/ASE 2003 Guideline Update for the Clinical Application of Echocardiography Bayes de
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona
, FASE Mayo Clinic, Arizona") Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
P F = R. Disorder of the Breast. Approach to the Patient with Chest Pain. Typical Characteristics of Angina Pectoris. Myocardial Ischemia
 Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Cardiology Updates: Syncope and Stress Testing. Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital
 Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy
 Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania My conflicts of interest: I have
Left ventricular diastolic function and filling pressure in patients with dilated cardiomyopathy Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania My conflicts of interest: I have
3/27/2014. Introduction.
 Introduction. Myocardial perfusion & contractility becomes abnormal immediately after the onset of ischaemia, even before the development of the symptoms & ST segment changes. 1 Myocardial Wall Motion
Introduction. Myocardial perfusion & contractility becomes abnormal immediately after the onset of ischaemia, even before the development of the symptoms & ST segment changes. 1 Myocardial Wall Motion
Choosing the Right Cardiac Test. Outline
 Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Diastolic Function Assessment New Guideline Update Practical Approach
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Guideline Number: NIA_CG_024 Last Review Date: January 2011 Responsible Department: Last Revised Date: May 2, 2011 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Chapter 21: Clinical Exercise Testing Procedures
 Publisher link: thepoint http://thepoint.lww.com/book/show/2930 Chapter 21: Clinical Exercise Testing Procedures American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise
Publisher link: thepoint http://thepoint.lww.com/book/show/2930 Chapter 21: Clinical Exercise Testing Procedures American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Graded exercise testing (GXT): extension of medical history and physical examination
: extension of medical history and physical examination") Related Readings Fletcher, G. F., Balady, G. J., Amsterdam, E. A., Chaitman, B., Eckel, R., Fleg, J., et al. (2001). Exercise standards for testing and training: A statement for healthcare professionals
Related Readings Fletcher, G. F., Balady, G. J., Amsterdam, E. A., Chaitman, B., Eckel, R., Fleg, J., et al. (2001). Exercise standards for testing and training: A statement for healthcare professionals
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
The Value of Stress MRI in Evaluation of Myocardial Ischemia
 The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Assessment of Ischemia and Viability
 EAE Teaching Course Bucharest, 2010 Assessment of Ischemia and Viability Jens-Uwe Voigt Dpt. of Cardiology University Leuven Belgium Assessment of Ischemia & Viability resting wall motion Stress Testing
EAE Teaching Course Bucharest, 2010 Assessment of Ischemia and Viability Jens-Uwe Voigt Dpt. of Cardiology University Leuven Belgium Assessment of Ischemia & Viability resting wall motion Stress Testing
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY
 OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD
 Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Case Question. Evaluation of Chest pain in the Office and Cardiac Stress Testing
 Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
The new Guidelines: Focus on Chronic Heart Failure
 The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
Aortic Valvular Stenosis
 Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
The Patient with Atrial Fibrilation
 Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Cardiovascular Listings. August 25, 2009 Institute of Medicine
 Cardiovascular Listings August 25, 2009 Institute of Medicine Updating the Cardiovascular Listings Laurence Desi, Sr., M.D., M.P.H. Medical Officer Office of Medical Listings Improvement 2 IOM General
Cardiovascular Listings August 25, 2009 Institute of Medicine Updating the Cardiovascular Listings Laurence Desi, Sr., M.D., M.P.H. Medical Officer Office of Medical Listings Improvement 2 IOM General
J. Schwitter, MD, FESC Section of Cardiology
 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Corrective Surgery in Severe Heart Failure. Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio
 Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Rational use of imaging for viability evaluation
 EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
GENERAL PRINCIPLES FOR ECHO ASSESSMENT OF DIASTOLIC FUNCTION (For full recommendation refer to the Left Ventricular Diastolic Function Guideline)
") 1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Chest Pain Wave I. Making Dollars and Sense Out of Stress Testing
 Chest Pain Wave I Making Dollars and Sense Out of Stress Testing Presenters Kristin Newby, MD, FACC Michael Kontos, MD, FACC Disclosures Dr. Newby: None specifically related to this activity All RWI are
Chest Pain Wave I Making Dollars and Sense Out of Stress Testing Presenters Kristin Newby, MD, FACC Michael Kontos, MD, FACC Disclosures Dr. Newby: None specifically related to this activity All RWI are
An Integrated Approach to Study LV Diastolic Function
 An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
CHEST PAIN CDU INCLUSION CRITERIA
 CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery
 Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Patient-centered Imaging in Coronary Artery Disease. Jason H Cole, MD, MS, FACC January 10, 2015
 Patient-centered Imaging in Coronary Artery Disease Jason H Cole, MD, MS, FACC January 10, 2015 Non-invasive coronary imaging Non-invasive cardiac imaging has improved assessment of cardiac function, anatomy,
Patient-centered Imaging in Coronary Artery Disease Jason H Cole, MD, MS, FACC January 10, 2015 Non-invasive coronary imaging Non-invasive cardiac imaging has improved assessment of cardiac function, anatomy,
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
ADVANCED CARDIOVASCULAR IMAGING. Medical Knowledge. Goals and Objectives PF EF MF LF Aspirational
 Medical Knowledge Goals and Objectives PF EF MF LF Aspirational Know the basic principles of magnetic resonance imaging (MRI) including the role of the magnetic fields and gradient coil systems, generation
Medical Knowledge Goals and Objectives PF EF MF LF Aspirational Know the basic principles of magnetic resonance imaging (MRI) including the role of the magnetic fields and gradient coil systems, generation
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference