High Value Evaluation of Chest Pain. Zoom Tips
|
|
|
- Shanna Terry
- 5 years ago
- Views:
Transcription

1 High Value Evaluation of Chest Pain California Quality Collaborative s Cardiology Webinar Series Webinar 1 December 7, 2017 Zoom Tips Attendees are automatically MUTED upon entry Refrain from using the hold button Type your questions in the chat box; we will address them during the Q&A session at the end of the presentation Message Jen through the chat box if you have any technical issues 2
2 Today s Speakers Bart Wald, MD California Quality Collaborative Raymond Zimmer, MD Cedars-Sinai Medical Center 3 Cardiology Webinar Series High-Value Treatment of Chest Pain: 12/07/17 High-Value Treatment of Congestive Heart Failure 01/23/18 High-Value Interventional Cardiology - Date TBD High-Value Electrophysiology - Date TBD 4

3 High Value Evaluation of Chest Pain Raymond Zimmer, MD, FACC Attending Cardiologist Cedars Sinai Medical Group Los Angeles, California December 7, 2017 None Disclosures

4 Objectives Briefly review chest pain epidemiology Evaluate value based strategies for prehospital and ED evaluation of chest pain Compare the indications, appropriateness, and value of diagnostic cardiac tests for chest pain assessment Highlight emerging technologies and practices that can facilitate evidence based, costeffective chest pain evaluation Chest pain epidemiology More than 8 10 million U.S. ED visits per year Second most common reason for ED visit Cardiac etiology accounts for less than 1/3 of ED visits for chest pain Most common causes of chest pain in outpatients are actually musculoskeletal (one third to one half of patients) and gastrointestinal (10 20%)

 Yet, less than 10% of patients presenting to the ED with chest pain are ultimately diagnosed with an acute coronary")
5 A symptom with many faces Fear vs. Fact More than 50% of ED patients presenting with chest pain receive comprehensive cardiac evaluation (serial biomarkers, noninvasive imaging, observation period, etc.) Yet, less than 10% of patients presenting to the ED with chest pain are ultimately diagnosed with an acute coronary syndrome (ACS) Only 1.5% of patients presenting to PCP with chest pain will have unstable angina/acute MI However, 1.5 2% of patients with acute MI are unrecognized at ED evaluation



6 $10 13 billion per year spent for unnecessary chest pain hospital admissions and evaluations

7 History, history, history Obtaining a detailed history is critical for differentiating cardiac vs. non cardiac causes of chest pain History alone can reduce referrals for testing that is likely to be low yield History, history, history Descriptions increasing likelihood of cardiac pain Exertional Diffuse pressure/heaviness Radiation to either arm/shoulder and neck Associated nausea/vomiting Associated diaphoresis Similar to previous MI Descriptions decreasing likelihood of cardiac pain Non exertional Sharp Positional Reproducible with palpation Well localized Associated with meals Short duration (few seconds or less) Atypical symptoms (particularly in women, the elderly, and diabetics) can include isolated jaw/neck/arm discomfort, exertional dyspnea, palpitations, nausea/vomiting, and generalized fatigue


8 Developing an accurate pretest probability ACC/AHA definitions of chest pain Typical Angina Substernal chest pain or discomfort Provoked by exertion or emotional stress Relieved by rest or sublingual nitroglycerin Atypical Angina Lacks one of the characteristics Non anginal chest pain Chest pain or discomfort that only meets one of the criteria The probability of coronary disease depending on the quality of chest pain test probability of cad cad consortium

9 ECG ECG should be performed for almost all patients with new onset chest pain Sensitivity for diagnosing cardiac ischemia is about 68%, while specificity about 97%* Normal ECG reduces likelihood of acute MI as etiology of active chest pain, but does not completely exclude myocardial ischemia 2% frequency of MI in patients with non ischemic EKG and no history of CAD (4% in patients with history of CAD) Serial ECGs generally recommended in acute evaluation *Ioannidis JP, Salem D, Chew PW, Lau J. Accuracy and clinical effect of out of hospital electrocardiography in the diagnosis of acute cardiac ischemia: A meta analysis. Ann Emer Med2001;37:
10 Troponin Should be checked in all patients suspected of myocardial ischemia Positive troponin suggests myocardial ischemia (though can have multiple causes) Negative troponin does not completely rule out acute coronary syndrome Current assays can identify most acute MIs within 3 hours of ED arrival Newer high sensitivity troponin increases sensitivity but decreases specificity Point of care troponin assay (POCT) Reduce delays that might be seen with transport and processing in a central lab, or lack of availability Results from POCT assays have previously been qualitative rather than quantitative Concerns regarding lower sensitivity, especially in early hours after symptom onset Cost effectiveness has not been well demonstrated May decrease cost by reducing referrals to higher levels of care May also lead to increased cost due to additional testing that might not otherwise have been pursued and which may not have any clinical benefit Studies evaluating changes in LOS and outcomes have had mixed results
11

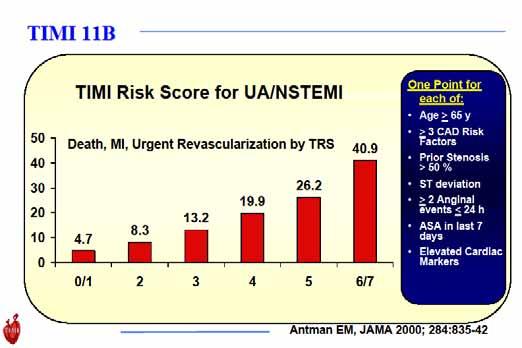
12 Risk scores
13 Neth Heart J 2008;16: GRACE risk score


14


15 Chest pain centers (CPCs) Key role in the evaluation of low to moderate risk patients presenting with chest pain Over 1,000 accredited CPCs in the U.S. Accredited through the American College of Cardiology Staffed by ED physicians, cardiologists, and/or ancillary staff (NP, PA, etc.) Facilitate rapid triage and management using accelerated diagnostic protocols
 vs.")
16 Chest pain centers (CPCs) Multiple studies have demonstrated significant advantages of CPCs without increase in adverse cardiac events Reduction in care variability Decreased length of stay Decreased readmission rates Decreased cost of care Consistent process improvement Compared admission rate, total cost, and LOS in low risk patients treated using accelerated diagnostic protocols (ADP) vs. inpatient controls Parameter ADP Control P value Admission rate 45.2% 100% < Mean total cost per $1528 $2095 < patient Mean LOS (hours) < 0.01
17 Diagnostic Testing





18 Valuable diagnostic tool for evaluation of chest pain Readily available Relatively low cost No radiation Can evaluate multiple potential etiologies of chest pain simultaneously Useful to help rule out ischemia as cause of active chest pain Echocardiogram


19 Handheld Ultrasound Provides most of the same diagnostic information as a full echocardiogram Advantages Rapid Accurate Superior sensitivity and specificity compared to physical exam Portable, lightweight, durable Improves access to care Can evaluate multiple organ systems Disadvantages Requires training Possibly limited imaging windows Cost of device (?)

20
21 Exercise Stress Test Main confirmatory test in accelerated diagnostic protocols and generally always preferred Exercise variables which have been shown to have prognostic value exercise duration chronotropic incompetence heart rate recovery exercise induced hypotension exercise induced hypertension ventricular ectopy If a person can walk for more than 5 minutes on flat ground or up one to two flights of stairs without needing to stop, they most likely can achieve an adequate workload during exercise stress testing. Type of stress Sensitivity Specificity LR + (95%CI) LR (95%CI) Exercise treadmill test (ETT) 68 % 77 % 3.57 ( ) 0.34 ( ) Stress echo 76% 88% 7.94 ( ) 0.24 ( ) SPECT radionuclide myocardial perfusion imaging 88% 77% 6.14 ( ) 0.24 ( ) Banarjee A et al., Diagnostic accuracy of exercise stress testing for coronary artery disease: a systematic review and metaanalysis of prospective studies ICJP April, 2012
")
22 ETT alone or with Imaging? Generally ETT alone should still be the first test for patients who: Can exercise Have an interpretable ECG (RBBB included) Annual event rates in patients with a low risk exercise treadmill stress test are as low as %



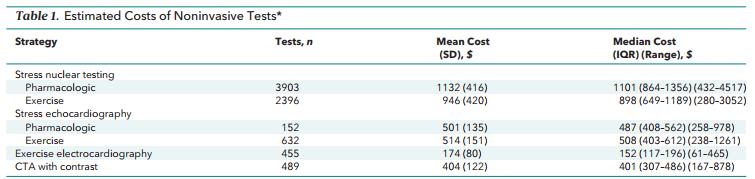
23 Relative strengths of ETT vs. Imaging Tests ETT More widely available Less technically demanding Lower cost No radiation SPECT/Echo Pharmacologic stress Localization of ischemia Ancillary information Higher diagnostic accuracy Higher prognostic accuracy Key point: across a range of pretest likelihood of obstructive CAD, no strategy that employed initial testing by imaging was costeffective
24 Cardiac Imaging Tests Favored by some as initial test for symptomatic patients with at least intermediate pre test probability of CAD Superior ability to diagnose CAD Superior ability to reclassify CAD likelihood Superior power for predicting CAD events Improved ability to guide subsequent short term and long term treatment Superior diagnostic ability in patients with prior PCI Clinical Considerations in Choosing the Cardiac Imaging Modality Myocardial Perfusion Imaging LBBB Ventricular pacing Atrial fibrillation Stress echocardiography Desire to minimize radiation Valvular information needed Hemodynamic information desired Significant resting wall motion abnormality on echo Obesity Contraindication to dobutamine



25 A role for the calcium score? Taylor AJ, et al Appropriate Use Criteria for Cardiac Computed Tomography J Am Coll Cardiol. 2010;56(22): Timothy S. Church, Benjamin D. Levine, Darren K. McGuire, Michael J. LaMonte, Shannon J. FitzGerald, et al., Coronary artery calcium score, risk factors, and incident coronary heart disease events, Atherosclerosis, Volume 190, Issue 1, January 2007
 had CAC = 0 95.4% of those patients had no CAD 3.9% had non obstructive CAD 0.")
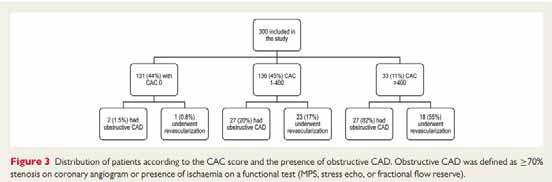
26 Retrospective study of 5129 patients with acute chest pain presenting to ED from identified as low to intermediate risk of ACS (TIMI < 2, negative troponins, normal/nondiagnostic EKG) and referred for coronary calcium scan More than half of the patients (2895; 56%) had CAC = % of those patients had no CAD 3.9% had non obstructive CAD 0.7% (21 patients) had obstructive CAD, of whom 11 had undergone stenting Rate of obstructive CAD was twice as high in smokers and patients with type 2 diabetes CAC test had sensitivity 96% (NPV 99.3%), specificity 62% (PPV 22.4%)
27
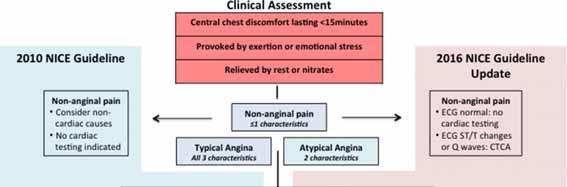
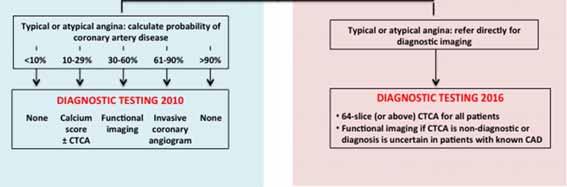



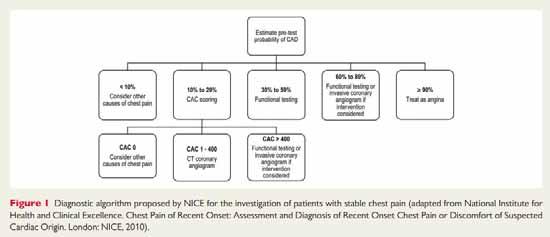
28 NICE Guidelines Coronary CT angiography
29 Coronary CT angiography Sensitivity ranges from % for detection of CAD (high negative predictive value) Specificity of about 80% Decreased accuracy in patients with increasing calcium scores (> 400) Relatively low radiation exposure Often less than 5 msv Can be reduced to less than 1 msv with newer CT scans and prospective gating protocols Availability Limitations of Coronary CT Angiography Need for expertise in analysis of studies Evaluation may be limited in patients with arrhythmias Renal impairment

30 Coronary CT angiography High utility in patients with lower ranges of pretest probability of CAD Multiple recent studies have suggested that the use of CCTA in the ED evaluation of chest pain results in: Reduced ED LOS Reduced admissions Increase accuracy for identification of CAD Concern for increased need for downstream testing Followed completion of ROMICAT, which showed that 8% of patients screened for ACS in EDs actually have ACS Evaluated 1,000 chest pain patients with suspected ACS Randomized 1:1 to CCTA or standard care (MD discretion) Primary end point: LOS Secondary endpoints: rates of ED discharge, MACE at 28 days, cumulative costs
 CCTA reduced chest pain patients average hospital stay from 31 hours to 23 hours vs. standard approach (P = 0.0002) CCTA patients much more likely to be discharged directly from ED (46.7% vs. 12.")
31 Key findings from ROMICAT II Average time to diagnosis was 10.4 hours in CCTA group vs hours in control group (P = 0.001) CCTA reduced chest pain patients average hospital stay from 31 hours to 23 hours vs. standard approach (P = ) CCTA patients much more likely to be discharged directly from ED (46.7% vs. 12.4%) and slightly less likely to be admitted to hospital (25.4% vs. 31.7%) No missed cases of ACS in either group and similar 30 day MACE rates in both groups CCTA costs were similar to standard approach despite more overall diagnostic testing in the CCTA group CCTA cost about 19% less per patient Hospital costs were about 50% more with CCTA approach underwent more angiography (12% vs. 8%, p = 0.04) and a statistically insignificant greater number of coronary interventions
32
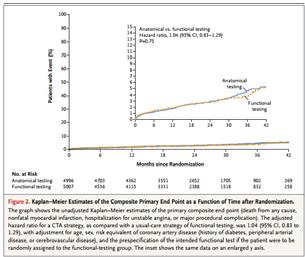
33 So which test do I pick? (If I need one) Ideal diagnostic strategy will: Clarify diagnosis Provide prognostic information Inform the need for additional care Maximize efficiency while minimizing cost Optimize clinical outcomes Many choices available, and despite multiple studies, after ETT, there is still no clear best choice Important to remember that among stable patients with chest pain, the prevalence of obstructive CAD is actually very low 88% of patients in the PROMISE trial had no obstructive CAD on CCTA May be more important to evaluate strategies for improving patient selection for additional cardiac testing



34 Patients with clinical evaluation alone had shorter LOS (20.3 vs hours, P < 0.001) Clinical evaluation alone associated with lower rates of diagnostic testing and angiography Clinical evaluation alone associated with lower median cost ($2261 vs. $2584, P = 0.009) No difference in rates of PCI, CABG, return ED visits, or MACE in the 28 day follow up period
35 Conclusions Costs for chest pain evaluation are high despite relatively low event rates Optimal utilization of clinical assessment can help to better identify lower risk patients in whom additional diagnostic testing would be low yield Exercise treadmill test is an appropriate initial diagnostic cardiac test for the evaluation of chest pain No clear best diagnostic cardiac test after ETT based on current data Increasing prevalence of emerging technologies may provide further opportunities to practice high value, cost effective care in cardiology
36 THANK YOU!
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Current and Future Imaging Trends in Risk Stratification for CAD
 Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
Simon A. Mahler MD, MS, FACEP Associate Professor Department of Emergency Medicine Wake Forest School of Medicine
 Simon A. Mahler MD, MS, FACEP Associate Professor Department of Emergency Medicine Wake Forest School of Medicine Research funding: American Heart Association Donaghue Foundation/ Association of American
Simon A. Mahler MD, MS, FACEP Associate Professor Department of Emergency Medicine Wake Forest School of Medicine Research funding: American Heart Association Donaghue Foundation/ Association of American
The 2016 NASCI Keynote: Trends in Utilization of Cardiac Imaging: The Coronary CTA Conundrum. David C. Levin, M.D.
 The 2016 NASCI Keynote: Trends in Utilization of Cardiac Imaging: The Coronary CTA Conundrum David C. Levin, M.D. October 16, 2016 MPI Utilization Rates/1000[includes PET] total radiologists 2014 total
The 2016 NASCI Keynote: Trends in Utilization of Cardiac Imaging: The Coronary CTA Conundrum David C. Levin, M.D. October 16, 2016 MPI Utilization Rates/1000[includes PET] total radiologists 2014 total
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why?
 Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Unnecessary hospitalisation and investigation of low risk patients presenting to hospital with chest pain
 Unnecessary hospitalisation and investigation of low risk patients presenting to hospital with chest pain Michael Perera Advanced Trainee in General and Acute Medicine Leena Aggarwal Director, Medical
Unnecessary hospitalisation and investigation of low risk patients presenting to hospital with chest pain Michael Perera Advanced Trainee in General and Acute Medicine Leena Aggarwal Director, Medical
Stress ECG is still Viable in Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh
 Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Risk Stratification for CAD for the Primary Care Provider
 Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
The Role of Computed Tomography in the Diagnosis of Coronary Atherosclerosis
 The Role of Computed Tomography in the Diagnosis of Coronary Atherosclerosis Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiology The Ohio State University
The Role of Computed Tomography in the Diagnosis of Coronary Atherosclerosis Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiology The Ohio State University
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
Patient-centered Imaging in Coronary Artery Disease. Jason H Cole, MD, MS, FACC January 10, 2015
 Patient-centered Imaging in Coronary Artery Disease Jason H Cole, MD, MS, FACC January 10, 2015 Non-invasive coronary imaging Non-invasive cardiac imaging has improved assessment of cardiac function, anatomy,
Patient-centered Imaging in Coronary Artery Disease Jason H Cole, MD, MS, FACC January 10, 2015 Non-invasive coronary imaging Non-invasive cardiac imaging has improved assessment of cardiac function, anatomy,
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Stress Testing:Which Study is Indicated for My Patient?
 Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
CHRONIC CAD DIAGNOSIS
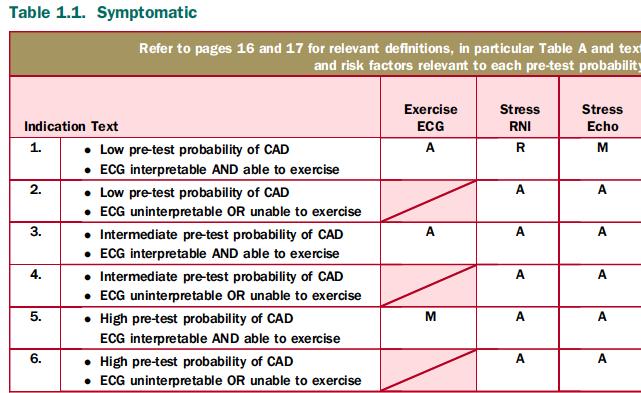
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
P F = R. Disorder of the Breast. Approach to the Patient with Chest Pain. Typical Characteristics of Angina Pectoris. Myocardial Ischemia
 Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
Choosing the Right Cardiac Test. Outline
 Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
The NICE chest pain guideline 1 year on. Jane S Skinner Consultant Community Cardiologist The Newcastle upon Tyne Hospitals NHS Foundation Trust
 The NICE chest pain guideline 1 year on Jane S Skinner Consultant Community Cardiologist The Newcastle upon Tyne Hospitals NHS Foundation Trust The Society for Acute Medicine, 5 th International Conference,
The NICE chest pain guideline 1 year on Jane S Skinner Consultant Community Cardiologist The Newcastle upon Tyne Hospitals NHS Foundation Trust The Society for Acute Medicine, 5 th International Conference,
Exercise Test: Practice and Interpretation. Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine
 Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test
 Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test Jang-Ho Bae, MD., PhD., FACC. Konyang University Hospital Daejeon, Korea Chest pain in Women ACS Atypical Stable angina F/29
Chest Pain in Women ;What is Your Diagnostic Plan? No Need for Noninvasive Test Jang-Ho Bae, MD., PhD., FACC. Konyang University Hospital Daejeon, Korea Chest pain in Women ACS Atypical Stable angina F/29
Which Test When? Avoid the Stress of Stress Testing. Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute
 Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
9/2/2016 CARDIOLOGY TESTING WHAT TO ORDER WHEN REFERENCE OBJECTIVES
 CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
CASE from South Korea
 CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
CASE from South Korea Bon-Kwon Koo, MD, PhD, Seoul, Korea Outpatient clinic of a non-interventional cardiologist F/56 Chief complaint: Angina with recent aggravation, CCS II~III Brief history: # Stroke
The Emerging Role of Cardiac CT in Cardiovascular Imaging. Anthony Gemignani, MD Vermont Cardiac Network April 28, 2016
 The Emerging Role of Cardiac CT in Cardiovascular Imaging Anthony Gemignani, MD Vermont Cardiac Network April 28, 2016 Conflict Disclosures I have no significant financial relationship with any companies
The Emerging Role of Cardiac CT in Cardiovascular Imaging Anthony Gemignani, MD Vermont Cardiac Network April 28, 2016 Conflict Disclosures I have no significant financial relationship with any companies
21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease
 21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease Noninvasive Evaluation of Coronary Artery Disease: Anatomical, Functional, Clinical May 5, 2018 Mark Hansen MD FRCPC Cardiologist,
21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease Noninvasive Evaluation of Coronary Artery Disease: Anatomical, Functional, Clinical May 5, 2018 Mark Hansen MD FRCPC Cardiologist,
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
A Cardiologist s Guide to Love
 A Cardiologist s Guide to Love A brief overview of what everyone should know about Palpitations, Heartache and Heartbreak! Eric J Dueweke, MD FACC Disclosure No one has yet to offer to pay me for my opinion.
A Cardiologist s Guide to Love A brief overview of what everyone should know about Palpitations, Heartache and Heartbreak! Eric J Dueweke, MD FACC Disclosure No one has yet to offer to pay me for my opinion.
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Patient referral for elective coronary angiography: challenging the current strategy
 Patient referral for elective coronary angiography: challenging the current strategy M. Santos, A. Ferreira, A. P. Sousa, J. Brito, R. Calé, L. Raposo, P. Gonçalves, R. Teles, M. Almeida, M. Mendes Cardiology
Patient referral for elective coronary angiography: challenging the current strategy M. Santos, A. Ferreira, A. P. Sousa, J. Brito, R. Calé, L. Raposo, P. Gonçalves, R. Teles, M. Almeida, M. Mendes Cardiology
. θωρακικούάλγουςστα εξωτερικά ιατρεία
 . θωρακικούάλγουςστα εξωτερικά ιατρεία Ε.Γ. ΑΛΑΜΑΓΚΑ ΚΑΡ ΙΟΛΟΓΟΣ ιδάκτωρ Ιατρικής Σχολής ΑΠΘ ΓΕΝΙΚΗ ΚΛΙΝΙΚΗ ΘΕΣΣΑΛΟΝΙΚΗΣ ΕΠΙΣΤΗΜΟΝΙΚΟΣ ΣΥΝΕΡΓΑΤΗΣ Α ΚΑΡ ΙΟΛΟΓΙΚΗΣ ΚΛΙΝΙΚΗΣ ΝΟΣΟΚΟΜΕΙΟ ΑΧΕΠΑ Panic attack
. θωρακικούάλγουςστα εξωτερικά ιατρεία Ε.Γ. ΑΛΑΜΑΓΚΑ ΚΑΡ ΙΟΛΟΓΟΣ ιδάκτωρ Ιατρικής Σχολής ΑΠΘ ΓΕΝΙΚΗ ΚΛΙΝΙΚΗ ΘΕΣΣΑΛΟΝΙΚΗΣ ΕΠΙΣΤΗΜΟΝΙΚΟΣ ΣΥΝΕΡΓΑΤΗΣ Α ΚΑΡ ΙΟΛΟΓΙΚΗΣ ΚΛΙΝΙΚΗΣ ΝΟΣΟΚΟΜΕΙΟ ΑΧΕΠΑ Panic attack
Guideline Number: NIA_CG_024 Last Review Date: January 2011 Responsible Department: Last Revised Date: May 2, 2011 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
Welcome! To submit questions during the presentation: or Text:
 Welcome! To participate in the interactive Q & A please do the following: 1. Download the Socrative Student App 2. Enter Teacher s Room Code: ZD0F3X5Q 3. Select Quiz: Intermountain Cardiac Stress Testing
Welcome! To participate in the interactive Q & A please do the following: 1. Download the Socrative Student App 2. Enter Teacher s Room Code: ZD0F3X5Q 3. Select Quiz: Intermountain Cardiac Stress Testing
CHEST PAIN CDU INCLUSION CRITERIA
 CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
Is computed tomography angiography really useful in. of coronary artery disease?
 Is computed tomography angiography really useful in screening patients with high risk of coronary artery disease? Myeong-Ki Hong, M.D. Ph D Professor of Medicine Division of Cardiology, Severance Cardiovascular
Is computed tomography angiography really useful in screening patients with high risk of coronary artery disease? Myeong-Ki Hong, M.D. Ph D Professor of Medicine Division of Cardiology, Severance Cardiovascular
FFR-CT Not Ready for Primetime
 FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
Chest Pain. Dr Robert Huggett Consultant Cardiologist
 Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Overview. Health and economic burden of coronary artery disease (CAD) Pitfalls in care of patients suspected of having CAD
 Pitfalls in care of patients suspected of having CAD") Quality Challenges and Pitfalls in the Evaluation of Patients with Suspected Heart Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine
Quality Challenges and Pitfalls in the Evaluation of Patients with Suspected Heart Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Team members: Felix Krainski, Besiana Liti, William Lane Duvall (ASNC member)
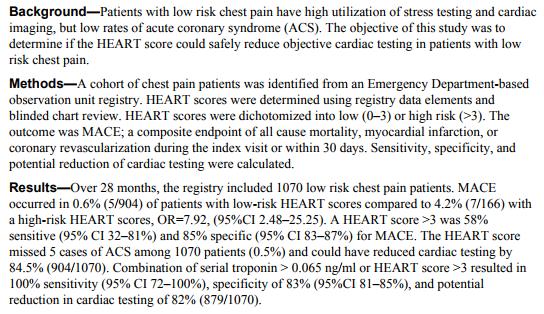
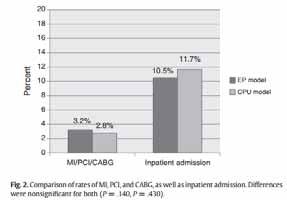
") ASNC Choosing Wisely Challenge 2016 An outpatient pathway for chest pain visits to the emergency department reduces length of stay, radiation exposure, and is patient-centered, safe and cost-effective.
ASNC Choosing Wisely Challenge 2016 An outpatient pathway for chest pain visits to the emergency department reduces length of stay, radiation exposure, and is patient-centered, safe and cost-effective.
Diagnostic Algorithms
 Diagnostic Algorithms Udo Sechtem Robert-Bosch-Krankenhaus Stuttgart Germany Montalescot G et al. ESC Guideline on the Management of Stable Coronary Artery Disease Eur Heart J. 2013;34:2949-3003. European
Diagnostic Algorithms Udo Sechtem Robert-Bosch-Krankenhaus Stuttgart Germany Montalescot G et al. ESC Guideline on the Management of Stable Coronary Artery Disease Eur Heart J. 2013;34:2949-3003. European
British Cardiac Society. Clinical and laboratory cardiac facilities required in the UK
 Page 1 of 15 British Cardiac Society Clinical and laboratory cardiac facilities required in the UK David Hackett Professional Standards & Peer Review Committee December 2004 Summary: Clinical cardiac facilities
Page 1 of 15 British Cardiac Society Clinical and laboratory cardiac facilities required in the UK David Hackett Professional Standards & Peer Review Committee December 2004 Summary: Clinical cardiac facilities
Case Question. Evaluation of Chest pain in the Office and Cardiac Stress Testing
 Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
2018 HPN Provider Summary Guide. Adult Cardiology Patients (18 Years and Older) Referral Guidelines
 Referral Guidelines") 12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
Kavitha Yaddanapudi Stony brook University New York
 Kavitha Yaddanapudi Stony brook University New York 8 million ER visits a year for chest pain 2-10% have Acute coronary syndrome (ACS) Coronary CTA(CCTA) -safe alternative to standard of care (SOC) and
Kavitha Yaddanapudi Stony brook University New York 8 million ER visits a year for chest pain 2-10% have Acute coronary syndrome (ACS) Coronary CTA(CCTA) -safe alternative to standard of care (SOC) and
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
STRESSED ABOUT STRESS TESTS
 STRESSED ABOUT STRESS TESTS Problem Based Lecture Jennifer W. Hsieh Department of Emergency Medicine PGY-3 Question 6 What is the diagnostic accuracy of cardiac testing in low risk chest pain patients?
STRESSED ABOUT STRESS TESTS Problem Based Lecture Jennifer W. Hsieh Department of Emergency Medicine PGY-3 Question 6 What is the diagnostic accuracy of cardiac testing in low risk chest pain patients?
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
There are 3 principle types of stress tests which do not involve the measurement of radiolabelled distribution within the body.
 National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING HEART (CARDIAC) PET SCAN STRESS ECHOCARDIOGRAM (Non-emergent outpatient testing) CPT4 Codes: Refer to pages 11-12 LCD
National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING HEART (CARDIAC) PET SCAN STRESS ECHOCARDIOGRAM (Non-emergent outpatient testing) CPT4 Codes: Refer to pages 11-12 LCD
Benoy N Shah 1,2,3, Gothandaraman Balaji 1, Abdalla Alhajiri 1, Ihab Ramzy 1, Shahram Ahmadvazir 1 & Roxy Senior 1,2,3
 STRESS ECHOCARDIOGRAPHY PREDICTS ALL-CAUSE MORTALITY IN PATIENTS ADMITTED WITH SUSPECTED ACUTE CORONARY SYNDROME, NON-DIAGNOSTIC ECG AND NEGATIVE TROPONIN European Society of Cardiology Annual Congress
STRESS ECHOCARDIOGRAPHY PREDICTS ALL-CAUSE MORTALITY IN PATIENTS ADMITTED WITH SUSPECTED ACUTE CORONARY SYNDROME, NON-DIAGNOSTIC ECG AND NEGATIVE TROPONIN European Society of Cardiology Annual Congress
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
The PAIN Pathway for the Management of Acute Coronary Syndrome
 2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Subha V. Raman, MD, MSEE, FACC, FAHA
 OSU Cardiovascular MR/CT Update April 27, 2018 Contemporary Approaches to Myocardial Ischemia Subha V. Raman, MD, MSEE, FACC, FAHA Professor and Medical Director, CMR/CCT Disclosures Institutional research
OSU Cardiovascular MR/CT Update April 27, 2018 Contemporary Approaches to Myocardial Ischemia Subha V. Raman, MD, MSEE, FACC, FAHA Professor and Medical Director, CMR/CCT Disclosures Institutional research
TROPONIN POSITIVE 2/20/2015 WHAT DOES IT MEAN? When should a troponin level be obtained?
 TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
ROMICAT II - Rule Out Myocardial
 ROMICAT II - Rule Out Myocardial Ischemia/Infarction Using Computer Assisted Tomography NHLBI U01HL092040 A Multicenter Randomized Comparative Effectiveness Trial of Cardiac CTA vs. Standard Evaluation
ROMICAT II - Rule Out Myocardial Ischemia/Infarction Using Computer Assisted Tomography NHLBI U01HL092040 A Multicenter Randomized Comparative Effectiveness Trial of Cardiac CTA vs. Standard Evaluation
The Value of Stress MRI in Evaluation of Myocardial Ischemia
 The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Diagnosis of CAD S Richard Underwood
 Diagnosis of CAD S Richard Underwood Professor of Cardiac Imaging Royal Brompton Hospital & Imperial College Faculty of Medicine London, UK The history and diagnosis 89% Non-cardiac chest pain 50% Atypical
Diagnosis of CAD S Richard Underwood Professor of Cardiac Imaging Royal Brompton Hospital & Imperial College Faculty of Medicine London, UK The history and diagnosis 89% Non-cardiac chest pain 50% Atypical
DIAGNOSTIC TESTING IN PATIENTS WITH STABLE CHEST PAIN
 DIAGNOSTIC TESTING IN PATIENTS WITH STABLE CHEST PAIN DISCLOSURES financial or pharmaceutical affiliations related to topic JOSHUA MESKIN, MD, FACC -Medical College of Wisconsin -Associate Professor of
DIAGNOSTIC TESTING IN PATIENTS WITH STABLE CHEST PAIN DISCLOSURES financial or pharmaceutical affiliations related to topic JOSHUA MESKIN, MD, FACC -Medical College of Wisconsin -Associate Professor of
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Contrast-Enhanced Coronary Computed Tomography Angiography (CCTA) Page 1 of 27 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Contrast-Enhanced Coronary Computed
Contrast-Enhanced Coronary Computed Tomography Angiography (CCTA) Page 1 of 27 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Contrast-Enhanced Coronary Computed
Maria Angela S. Cruz-Anacleto, MD
 Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
How to investigate (Cardiac) Chest Pain
 Chest Pain") RCP UPDATE IN MEDICINE 27 th November 2017 How to investigate (Cardiac) Chest Pain Justin Carter Consultant Cardiologist North Tees and Hartlepool NHS Trust The spectrum of coronary disease No Disease
RCP UPDATE IN MEDICINE 27 th November 2017 How to investigate (Cardiac) Chest Pain Justin Carter Consultant Cardiologist North Tees and Hartlepool NHS Trust The spectrum of coronary disease No Disease
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Evidence for Everyone: Expanding the Reach of Health Technology Assessment 2016 CADTH Symposium, April 10-12, Shaw Centre, Ottawa
 Dr. Ross Davies President Dr. Benjamin Chow Vice-President Dr. Jonathan Leipsic Secretary/Treasurer Office 222 Queen Street Suite 1403 Ottawa, ON K1P 5V9 www.ccs.ca/ nuclear_ct@ccs.ca Evidence for Everyone:
Dr. Ross Davies President Dr. Benjamin Chow Vice-President Dr. Jonathan Leipsic Secretary/Treasurer Office 222 Queen Street Suite 1403 Ottawa, ON K1P 5V9 www.ccs.ca/ nuclear_ct@ccs.ca Evidence for Everyone:
Cardiology Updates: Syncope and Stress Testing. Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital
 Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Reducing the Population Health Burden of Cardiovascular Disease
 Reducing the Population Health Burden of Cardiovascular Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine Disclosures: K23 HL116787
Reducing the Population Health Burden of Cardiovascular Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine Disclosures: K23 HL116787
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Impact of Chest Pain Protocol Targeting Intermediate Cardiac Risk Patients in an Observation Unit of an Academic Tertiary Care Center
 Elmer ress Original Article J Clin Med Res. 2016;8(2):111-115 Impact of Chest Pain Protocol Targeting Intermediate Cardiac Risk Patients in an Observation Unit of an Academic Tertiary Care Center Tariq
Elmer ress Original Article J Clin Med Res. 2016;8(2):111-115 Impact of Chest Pain Protocol Targeting Intermediate Cardiac Risk Patients in an Observation Unit of an Academic Tertiary Care Center Tariq
Diagnostic and Prognostic Value of Coronary Ca Score
 Diagnostic and Prognostic Value of Coronary Ca Score Dr. Ghormallah Alzahrani Cardiac imaging division, Adult Cardiology department Prince Sultan Cardiac Center ( PSCC) Madina, June 2 Coronary Calcium
Diagnostic and Prognostic Value of Coronary Ca Score Dr. Ghormallah Alzahrani Cardiac imaging division, Adult Cardiology department Prince Sultan Cardiac Center ( PSCC) Madina, June 2 Coronary Calcium
CLINICIAN INTERVIEW RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE. An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA
 RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
STANDARDIZED PROCEDURE CARDIAC STRESS TESTING-EXERCISE TESTING (Adult)
") 1 I. Definition: During the exercise test, the patient exercises on a bike or treadmill while being monitored with a 12 lead ECG, blood pressure device, pulse oximetry oxygen consumption, and perhaps imaging
1 I. Definition: During the exercise test, the patient exercises on a bike or treadmill while being monitored with a 12 lead ECG, blood pressure device, pulse oximetry oxygen consumption, and perhaps imaging
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users
 Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
2017 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2017 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 15 performance measures that were approved by CMS for use in ASC's 2017 Qualified Clinical Data
2017 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 15 performance measures that were approved by CMS for use in ASC's 2017 Qualified Clinical Data
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Conflict of Interest Disclosure
 Challenges and Opportunities for SPECT & PET in 2013: Implementing Latest Acquisition and Processing Protocols Timothy M. Bateman M.D. Co-Director, Cardiovascular Radiologic Imaging Mid America Heart Institute
Challenges and Opportunities for SPECT & PET in 2013: Implementing Latest Acquisition and Processing Protocols Timothy M. Bateman M.D. Co-Director, Cardiovascular Radiologic Imaging Mid America Heart Institute
Effect of intravenous atropine on treadmill stress test results in patients with poor exercise capacity or chronotropic incompetence ABSTRACT
 Effect of intravenous atropine on treadmill stress test results in patients with poor exercise capacity or chronotropic incompetence Samad Ghaffari, MD, Bahram Sohrabi, MD. ABSTRACT Objective: Exercise
Effect of intravenous atropine on treadmill stress test results in patients with poor exercise capacity or chronotropic incompetence Samad Ghaffari, MD, Bahram Sohrabi, MD. ABSTRACT Objective: Exercise
Acute Coronary Syndrome
 ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
Stress Echo Cases Sunday, October 8, :10 3:30 PM 20 min
 2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
Guideline Number: NIA_CG_024 Last Revised Date: August 2011 Responsible Department: Implementation Date: January 2014 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING (aka NUCLEAR CARDIAC IMAGING STUDY) CPT Code: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78499 Original
National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING (aka NUCLEAR CARDIAC IMAGING STUDY) CPT Code: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78499 Original
Disclosures. GETTING TO THE HEART OF THE MATTER WITH MULTIMODALITY CARDIAC IMAGING Organ Review Meeting 25 September. Overview
 GETTING TO THE HEART OF THE MATTER WITH MULTIMODALITY CARDIAC IMAGING Organ Review Meeting 25 September Disclosures None relevant to this presentation Mini Pakkal Assistant Professor of Radiology University
GETTING TO THE HEART OF THE MATTER WITH MULTIMODALITY CARDIAC IMAGING Organ Review Meeting 25 September Disclosures None relevant to this presentation Mini Pakkal Assistant Professor of Radiology University
Guideline Number: NIA_CG_024 Last Revised Date: August 2011 Responsible Department: Clinical. Implementation Date: January 2014 Operations
 National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING MYOCARDIAL PERFUSION STUDY CPT Code: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78499 Original Date: October
National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING MYOCARDIAL PERFUSION STUDY CPT Code: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78499 Original Date: October
Physician Self-referral and Health Care Utilization. Rita F. Redberg, MD, MSc Professor of Medicine UCSF Medical Center
 Physician Self-referral and Health Care Utilization Rita F. Redberg, MD, MSc Professor of Medicine UCSF Medical Center Physician self-referral why should we care? Extent of occurrences Impact of physician
Physician Self-referral and Health Care Utilization Rita F. Redberg, MD, MSc Professor of Medicine UCSF Medical Center Physician self-referral why should we care? Extent of occurrences Impact of physician
Noninvasive cardiac imaging refers
 CARDIOLOGY PATIENT PAGE Introduction to Noninvasive Cardiac Imaging Ron Blankstein, MD Noninvasive cardiac imaging refers to a combination of methods that can be used to obtain images related to the structure
CARDIOLOGY PATIENT PAGE Introduction to Noninvasive Cardiac Imaging Ron Blankstein, MD Noninvasive cardiac imaging refers to a combination of methods that can be used to obtain images related to the structure
Richard Grocott Mason
 Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Invited Experts' Case Presentation and 5-Slides Focus Review
 Invited Experts' Case Presentation and 5-Slides Focus Review FFR and IVUS in Myocardial Bridging Haegeun, Song. M.D. Heart Institute, Asan Medical Center, Seoul, Korea Myocardial Bridging Common congenital
Invited Experts' Case Presentation and 5-Slides Focus Review FFR and IVUS in Myocardial Bridging Haegeun, Song. M.D. Heart Institute, Asan Medical Center, Seoul, Korea Myocardial Bridging Common congenital
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines
 Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Rapid Disposition of Chest Pain Patients February 2019
 UCSF High Risk Emergency Medicine Rapid Disposition of Chest Pain Patients February 2019 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International
UCSF High Risk Emergency Medicine Rapid Disposition of Chest Pain Patients February 2019 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International
Baseline Data Collection Tool
 Endorsed by the Vanderbilt Department of Emergency Medicine Research Partner of the ED Benchmarking Alliance Baseline Data Collection Tool The data collected via this form is the baseline member data for
Endorsed by the Vanderbilt Department of Emergency Medicine Research Partner of the ED Benchmarking Alliance Baseline Data Collection Tool The data collected via this form is the baseline member data for