Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3)
|
|
|
- Kory Richardson
- 5 years ago
- Views:
Transcription

1 Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K


2 New England Journal of Medicine Promissing to change everything to know about Hypertension
3

4 Primary Outcome and Primary Hypothesis Primary outcome CVD composite: first occurrence of Myocardial infarction (MI) Acute coronary syndrome (non-mi ACS) Stroke Acute decompensated heart failure (HF) Cardiovascular disease death Primary hypothesis* CVD composite event rate lower in intensive compared to standard treatment *Estimated power of 88.7% to detect a 20% difference - based on recruitment of 9,250 participants, 4-6 years of follow-up and loss to follow-up of 2%/year.

5 1.8 vs vs 2.8
6
7 ACHIEVED SBP/DBP VALUES (mmhg) IN SPRINT 1 YEAR FINAL. STANDARD INTENSIVE 136.2/ / / /67.2 BP difference 13 mm Hg: Stroke reduction p: NS MI and no MI ACS p: NS 3861
8 BP Reductions as Small as 2 mmhg Reduce the Risk of CV Events by Up to 10% Meta-analysis of 61 prospective, observational studies 1 million adults 12.7 million person-years 2 mmhg decrease in mean SBP 7% reduction in risk of IHD mortality 10% reduction in risk of stroke mortality Prospective Studies Collaboration. Lancet. 2002;360:
9 SPRINT Primary Outcome and its Components Event Rates and Hazard Ratios Intensive Standard No. of Events Rate, %/year No. of Events Rate, %/year HR (95% CI) P value Primary Outcome (0.64, 0.89) <0.001 All MI (0.64, 1.09) 0.19 Non-MI ACS (0.64, 1.55) 0.99 All Stroke (0.63, 1.25) 0.50 All HF (0.45, 0.84) CVD Death (0.38, 0.85) 0.005
10 Participants with CKD at Baseline Renal Disease Outcomes Intensive Standard Events %/yr Events %/yr HR (95% CI) P Primary CKD outcome (0.42, 1.87) % reduction in (0.36, 2.07) 0.75 egfr * Dialysis (0.19, 1.54) 0.27 Kidney transplant Secondary CKD Outcome Incident albuminuria** (0.48, 1.07) 0.11 Participants without CKD at Baseline Secondary CKD outcomes 30% reduction in egfr* (2.44, 5.10) <.0001 Incident albuminuria** (0.63, 1.04) 0.10 *Confirmed on a second occasion 90 days apart **Doubling of urinary albumin/creatinine ratio from <10 to >10 mg/g
11 Is it possible that in SPRINT patients randomized to lower BP target were 1) originally healthier? 2) more carefully followed? Should GLs recommend to start drug treatment in the high normal BP range in both middle age and elderly pts? In SPRINT entry BP 139.7/78.1mmHg but patients were treated!

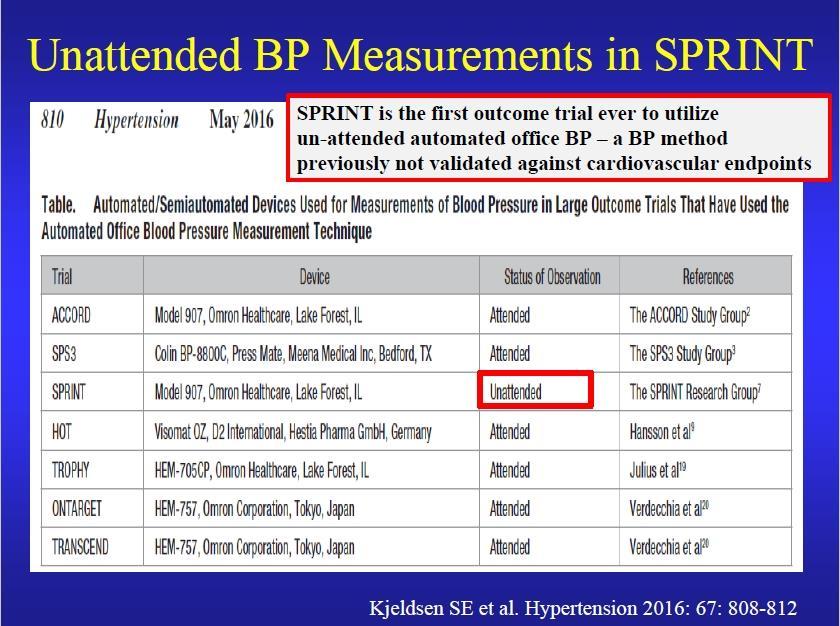
12 Office Blood Pressure Measurement

13 Unattended Automatic office BP Measurement 5min alone in the room-sbp/dbp fell by 15.7/8.0mmHg for unattended automatic office BP compared to regular OBP. The limit for hypertension of 140/90mmHg,according to office BP corresponded to 125/82mmHg for unattended automatic OBP Filipovsky Blood Pressure 2016

14 ROME 2016 ESC
15
16


17 High-risk+Age 50ys+SBP 130mmHg Consider SBP 120mmHG Guided by AOBP measurements
18


19 SPRINT TRIAL No Nnnon s Yes
20
21

22 Influence in Hyp Guidelines in EU???? NO SPRINT TRIAL SPRINT TRIAL



23 The Pathway Project Single vs Combination diuretic in patients with low-renin HTN Optimal therapy of RH Monotherapy vs. Combination for initial treatment
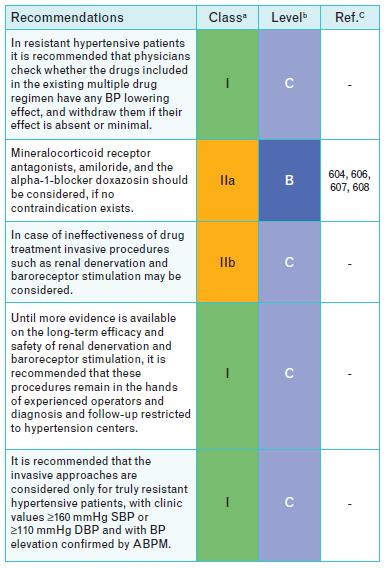
24 Therapeutic Strategies in Patients with Resistant Hypertension
: a")
25 A Double blinded, Placebo-Controlled, Crossover Study Williams, Bryan, et al. "Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial." The Lancet 2015;386:

26 A Double blinded, Placebo-Controlled, Cross-over Study Comparison of: Spironolactone, mg/daily with Placebo Doxazocin, 4-8 mg/daily Bisoprolol, 5-10 mg/daily

 130 mmhg despite")

27 PATHWAY-2: Study Design Inclusion criteria: Patients aged years Seated clinic SBP 140 mmhg (or 135 mmhg for patients with diabetes) Home SBP (18 readings over 4 days) 130 mmhg despite treatment for 3 months with maximally tolerated doses of 3 drugs From 12 secondary and 2 primary care sites in the UK
28 PATHWAY-2: Primary endpoints Difference in average home systolic BP (HSBP) between: Spironolactone and placebo Spironolactone and average of the other 2 active drugs (doxazosin and bisoprolol) Spironolactone and each of the other 2 active drugs
29 PATHWAY-2: Secondary endpoints Clinic BP responses to randomized treatments BP control rates with each treatment (HSBP <135 mmhg) Whether baseline plasma renin concentrations, whilst on treatment with A+C+D, predicted the best drug for individual patients Safety and adverse events during each treatment cycle

30 PATHWAY-2: Primary Outcome
31 There was an inverse and linear relationship between renin and BP response to spironolactone

32 Only six of 285 (2%) patients exposed to spironolactone developed a serum potassium on a single occasion greater than 6 0 mmol/l, with a maximum of 6 5 mmol/l
33 Limitations of the study Short duration of treatment (3 months) Exclusion of patients with egfr <45 ml/min (no data) Inclusion of predominantly white Caucasians (unclear whether the results are applicable to other ethnic groups) Absence of washout periods Absence of data for morbidity and mortality outcomes (BP lowering as a powerful surrogate for clinical benefit in this highrisk group of patients)

34 PATHWAY-2 Only 15 of 285 patients assessed on spironolactone failed to achieve a HSBP <150 mmhg, equivalent to a CSBP 160 mmhg, the usual eligibility criterion for denervation - Spironolactone was clearly the most effective treatment for RH and thus should influence future treatment guidelines and clinical practice globally - Patients should not be defined as RH unless their BP remains uncontrolled on spironolactone!!!

35 Spironolactone 25-50mg daily: Conclusions Is the most effective drug treatment for RH Controls BP in almost 60% of patients with RH and is 3-times as likely to be more effective than doxazocin or bisoprolol
36 The Heart Outcomes Prevention Evaluation (HOPE) 3 Trial Eva Lonn, Jackie Bosch, Salim Yusuf For the HOPE-3 Investigators Population Health Research Institute, (PHRI) McMaster University and Hamilton Health Sciences, Hamilton, Canada Unrestricted grants from the Canadian Institutes of Health Research and AstraZeneca
37 Unique Aspects of HOPE-3 BP lowering trial with wide range of BP entry criteria Cholesterol lowering treatment based on risk opposed to baseline LDL or HDL measurement Diverse population

38 HOPE-3 Baseline characteristics
39 Cumulative Hazard Rates CV Death, MI, Stroke, Cardiac Arrest, Revascularization, Heart Failure HR (95% CI) = 0.95 ( ) P-value = 0.51 Placebo Candesartan + HCTZ No. at Risk Cand + HCTZ Placebo Years
40 Prespecified Subgroups: By Thirds of SBP CV Death, MI, Stroke, Cardiac Arrest, Revasc, HF Cutoffs SBP Mean Diff Placebo Event Rate% HR (95% CI) P Trend ( ) ( ) > ( ) Candesartan + HCTZ Better Placebo Better
41 BP Lowering Arm: Conclusions Fixed dose combination of Candesartan 16 mg + HCTZ 12.5 mg/day reduced BP by 6.0/3.0 mmhg, but did not reduce CV events CV events were significantly reduced in the highest third of SBP SBP >143.5 mmhg, mean 154 mmhg Results were neutral in the middle third, and trended towards harm in the lowest third of SBP Treatment increased lightheadedness, but not syncope or renal dysfunction
42 Cholesterol Lowering Arm Results Jackie Bosch
43 Cholesterol Lowering: Outcomes Outcome Rosuvastatin N (%) Placebo N (%) HR (95% CI) p Co-Primary (3.7) 304 (4.8) 0.76 ( ) Co-Primary (4.4) 363 (5.7) 0.75 ( ) Secondary 1 306(4.8) 393 (6.2) 0.77 ( ) CV Death 154 (2.4) 171 (2.7) 0.89 ( ) 0.31 MI 45 (0.7) 69 (1.1) 0.65 ( ) 0.02 Stroke 70 (1.1) 99 (1.6) 0.70 ( ) 0.02 CV Hosp. 281 (4.4) 369 (5.8) 0.75 ( )
44 Cumulative Hazard Rates CV Death, MI, Stroke, Cardiac Arrest, Revasc, Heart Failure HR (95% CI) = 0.75 ( ) P-value = Placebo Rosuvastatin Rosuva Placebo Years
45 HOPE-3 & Other Studies of LDL Lowering and CVD
46 Cholesterol Lowering: Conclusions Rosuvastatin 10mg/day reduced: LDL-C by 34.6 mg/dl (0.9 mmol/l; i.e. 27% in LDL-C) CVD by 25% Consistent benefits regardless of: LDL-C SBP Risk CRP Ethnicity Excess in muscle pain/weakness (reversible) and perhaps cataract surgery No excess in rhabdomyolysis, myopathy or new diabetes
47 Combined BP & Cholesterol Lowering vs Double Placebo Salim Yusuf
48 Unique Aspects of BP & Chol Lowering First formal testing of polypill concept on clinical events Demonstrates that the concept is valid in people with elevated BP; in others there is no benefit
49 Cumulative Hazard Rates CV Death, MI, Stroke, Cardiac Arrest, Revasc, Heart Failure Double Placebo Combination HR (95% CI) = 0.72 ( ) P-value = Combination Rosuvastatin Candesartan/HCTZ Double Placebo Years
50 RRR RRR RRR of Combination and Each Intervention vs Double Placebo Co-Primary 2 50% 40% 30% 28% Overall 26% 20% 10% 6% 50% 40% 30% 20% 40% 0% Combo Highest Third of SBP 24% 20% Rosuva Only 50% 40% 30% 20% Cand + HCTZ Only Lower Two Thirds of SBP 19% 31% 10% 10% Cand + HCTZ Only 0% Combo Rosuva Only Cand+HCTZ Only 0% Combo Rosuva Only -8%
51 Clinical Implications Statins beneficial in intermediate-risk individuals without CVD BP lowering benefits only those with elevated BP Combined BP & cholesterol lowering: Leads to a 40% risk reduction in hypertensives (benefits from both BP lowering and statin) In others, 30% RRR from statin alone Pragmatic strategy: No Lipid or BP entry criteria or targets No Dose titration Infrequent safety monitoring Strategy used in HOPE-3 is simple, safe and effective and widely applicable

52 Ευχαριστώ!!!
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Heart Outcomes Prevention Evaluation (HOPE) - 3 Combined Lipid Lowering and Blood Pressure Lowering in Moderate Risk People
 - 3 Combined Lipid Lowering and Blood Pressure Lowering in Moderate Risk People") November September 23, 20, 20102012 Heart Outcomes Prevention Evaluation (HOPE) - 3 Combined Lipid Lowering and Blood Pressure Lowering in Moderate Risk People Eva Lonn, Jackie Bosch, Jane Castelli, Andrea
November September 23, 20, 20102012 Heart Outcomes Prevention Evaluation (HOPE) - 3 Combined Lipid Lowering and Blood Pressure Lowering in Moderate Risk People Eva Lonn, Jackie Bosch, Jane Castelli, Andrea
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
ROLE OF INFLAMMATION IN HYPERTENSION. Dr Barasa FA Physician Cardiologist Eldoret
 ROLE OF INFLAMMATION IN HYPERTENSION Dr Barasa FA Physician Cardiologist Eldoret Outline Inflammation in CVDs the evidence Basic Science in Cardiovascular inflammation: The Main players Inflammation as
ROLE OF INFLAMMATION IN HYPERTENSION Dr Barasa FA Physician Cardiologist Eldoret Outline Inflammation in CVDs the evidence Basic Science in Cardiovascular inflammation: The Main players Inflammation as
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
How do we diagnose hypertension today? Presentation Subtitle
 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
RAS Blockade Across the CV Continuum
 A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf
 Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf Disclosure None Polypill & CVD Prevention 1. Why do we need a polypill? 2. What components in the polypill?
Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf Disclosure None Polypill & CVD Prevention 1. Why do we need a polypill? 2. What components in the polypill?
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4)
 and The International Polycap Study 3 & 4 (TIPS 3 & 4)") The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study
 LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study") Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
surtout qui n est PAS à risque?
 3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events
 Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
MS Sabatine, RP Giugliano, AC Keech, PS Sever, SA Murphy and TR Pedersen, for the FOURIER Steering Committee & Investigators
 Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Should I use statins?
 I know the trials in heart failure but how do I manage my patient? Should I use statins? Aldo P Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Disclosures Aldo P Maggioni served as a member of
I know the trials in heart failure but how do I manage my patient? Should I use statins? Aldo P Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Disclosures Aldo P Maggioni served as a member of
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
KDIGO conference on high CV risk associated with CKD. The role of BP in CKD stage 1-4
 KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes?
 Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
The ACCELERATE Trial
 The ACCELERATE Trial Impact of the Cholesteryl Ester Transfer Protein Inhibitor Evacetrapib on Cardiovascular Outcome Stephen J Nicholls for the ACCELERATE investigators Disclosure Research support: AstraZeneca,
The ACCELERATE Trial Impact of the Cholesteryl Ester Transfer Protein Inhibitor Evacetrapib on Cardiovascular Outcome Stephen J Nicholls for the ACCELERATE investigators Disclosure Research support: AstraZeneca,
What s the evidence, why do guidelines differ, and what should the GP do?
 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Blood Pressure Measurement in SPRINT
 Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
New evidences in heart failure: the GISSI-HF trial. Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy
 New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 6 October 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 6 October 2010 CRESTOR 5 mg, film-coated tablet B/30 (CIP code: 369 853-8) B/90 (CIP code: 391 690-0) CRESTOR 10 mg,
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 6 October 2010 CRESTOR 5 mg, film-coated tablet B/30 (CIP code: 369 853-8) B/90 (CIP code: 391 690-0) CRESTOR 10 mg,
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A