IABP to prevent pulmonary edema under VA-ECMO
|
|
|
- Olivia Wade
- 5 years ago
- Views:
Transcription



1 IABP to prevent pulmonary edema under VA-ECMO Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris 6
2 Conflict of interest Principal Investigator: HEROICS trial HVHF after complicated heart surgery NCT Sponsored by GAMBRO Principal Investigator: EOLIA trial VV ECMO in ARDS NCT Sponsored MAQUET, Getinge Group Received honoraria from MAQUET, Getinge Group Gambro

3 Pulmonary edema under VA ECMO
4
5 Pulmonary edema Due to an increase in LV afterload created by the backward ECMO flow More frequent With peripheral ECMO If no residual LV ejection Increase in LV afterload Aortic/Mitral regurgitation, LV dilation LV end-diastolic pressure, PCWP Pulmonary edema Laminar flow Alteration of microcirculation?


6 Pulmonary edema under VA-ECMO

7 Hemodynamic impact of the IABP Diastolic inflation coronary blood flow myocardial O2 supply myocardial ischemia Systolic deflation afterload et cardiac output myocardial O2 consumption LV work et LV volume Pulsatile blood flow Improvement of microcirculation?
8 Retrospective study


9 December 2007 to December peripheral VA-ECMO 90 patients with laminar flow LVEF <15% ITV < 8 cm Δ SBP-DBP <15mmHg
10 PVA ECMO Post-cardiotomy 117 Refractory MOF<48h 96 Chronic pulmonary disease 26 Massive mitral regurgitation 21 Refractory septic shock 14 Femoro-axillary cannulation 10 ARDS 8 Isolate RV dysfunction 8 Prior impella implantation 5 Pulse pressure 15 mmhg 48 or TVI 8 cm IABP for APO 5 APO after IABP explantation 5 ECMO centralisation for other reasons than APO 4 90 patients No-IABP 56 IABP 34
11 Patients s characteristics Parameter No-IABP IABP Median (25 th -75 th ) n=56 n=34 p Age, y 46,5 (32-54) 51,5 (43-59,5) * 0,02 Male, % 57 % 73 % 0,12 BMI 24,6 (20,6-27,8) 26,6 (24,8-30,7) * 0,02 Charlson score 2 (1-3) 2 (1-3) 0,14 Year 2009 ( ) 2011 ( ) ***p<0,0001 Saps-II score 65 (56-72,5) 75 (54-81) 0,11 SOFA score 11 (6,5-13) 11 (8-14,5) 0,39 Etiology, % Cardiac arrest AMI Myocarditis DCM 28,5% 35,7% 32,1% 32,1% 41,1% 64,7% 11,7% 23,5% 0,22 ** 0,007 *0,03 0,38 Inotrope score, g/kg/min 76,5 (41-127,5) 49 (30-77) *0,03 LVEF, % 10 (7-10) 10 (6-11) 0,73 TVI, cm 4 (2-5) 4 (2-5) 0,38 Mechanical ventilation, % 87,5 % 94,1 % 0,42 PaO2/FiO2 ratio 270 ( ) 296 ( ) 0,69 PEEP, cmh2o 4 (2-5) 4 (4-6) 0,14 ph 7,25 (7,18-7,35) 7,25 (7,12-7,32) 0,40 Lactatemia, mmoles/l 8,0 (5,7-10,9) 7,3 (5,0-11,5) 0,98 Q ECMO, L/min 3,97 (3,33-4,45) 4,22 (3,73-4,61) 0,09
12 Radiologic component of the LIS Radiologic score 4 3 IABP No IABP 2 1 *** *** *** *** 0 D0 D1 D2 D3 D7 D15 Time from ECMO implantation
13 Percent survival free from Pulmonary edema P<0,0001 by Logrank test IABP No-IABP Time (days)
14 Impact of IABP use IABP switch for central ECMO Major pulmonary edema

15 Need for central ECMO % vs 5.9% 75 ***, p= IABP
16 Independent predictors of pulmonary edema occurrence Variables OR IC 95% P No IABP < ph <7.25 at ECMO initiation Inotropic Score >66 at ECMO initiation
17 Outcomes Parameter Median (25 th -75 th ) No-IABP n=56 IABP n=34 IABP duration, d - 5,5 (3,5-7,5) ECMO duration, d 5 (2,5-7,5) 6 (4-10) 0,06 p Follow-up, % Death under peripheral ECMO Death under central ECMO Death under temporary assistance Myocardial recovery Cardiac transplant Bridge to long term assistance 12,5 14,2 32,1 35,7 17,9 14,3 26,5 0 26,5 35,3 5,9 32,3 0,09-0,57 0,97 0,10 0,04* Weaning from MV under ECMO, % 30,4 38,2 0,44 Time on MV under ECMO, % 100 (66,3-100) 100 (40,4-100) 0,52 ICU mortality, % 35,7 29,4 0,54 ICU duration, d 14 (6-30) 10 (6-21) 0,24 Temporary circulatory assistance duration, d 9 (5,5-13) 6 (4-10) 0,13 Mechanical ventilation duration, d 6 (3-15) 5 (3-12,5) 0,29 RRT duration, d 5,5 (1-42) 2 (0-6) 0,69
18 Prospective study
19 Study objectives Evaluate the impact of the combination of Peripheral veno-arterial ECMO Counterpulsation with IABP On general hemodynamics and microcirculation In patients with refractory cardiogenic shock
20 Methods Prospective monocenter crossover study 12 months-study period 12 patients Admitted for refractory cardiogenic shock requiring emergent peripheral veno-arterial ECMO Low or non-ejecting heart : laminar blood flow Evaluation Evaluation under IABP support, after 30 min interruption and 30 min after restarting the IABP
21 Evaluation of macrocirculation Clinical parameters Arterial blood pressure Echocardiographic parameters Aortic VTI, LVEF, LVEDD, LVESD E/A and E/Ea ratios, mitral annulus S wave CO, CI Pulmonary artery catheter: PAPs, PAPd, PAPm, PAOP Blood gases


22 Evaluation of microcirculation Sidestream Dark Field imaging SDF Sublingual videomicroscopy sequences Semi-quantitative and dynamic evaluation of microcirculation


23 Thenar eminence microcirculation InSpectra StO 2 - NIRS Early indicator of tissular hypoperfusion? Models : arteriopathy, septic shock Parameters : Baseline StO2 Vascular occlusion test VOT : T1, T2 Hyperemia (StO2 overshoot)



24 Brain microcirculation Equanox Nonin Early indicator of brain hypoperfusion Models : cardiac surgery Parameters : Left and right rso2
25 Patients characteristics Variable Value Range Age, yr 57 ± Men, n (%) 9 (75%) SAPS2 79 ± Before inclusion Days of ECMO 6.3 ± Days of IABP 4.7 ± Diagnosis, n (%) Acute myocardial infarction 8 (67%) Acute valvular dysfunction 2 (17%) Dilated cardiomyopathy 1 (8%) Fulminant myocarditis 1 (8%) During study protocol ECMO flow, L/min 4.3 ± Catecholamines Dobutamine (n = 4), µg/kg/min 7.5 ± Norepinephrine (n = 1), mg/h 0,6 Epinephrine (n = 5), mg/h 3.0 ± Patients on mechanical ventilation, n (%) 12 (100%)
 74 ± 17 88 ± 16 72 ± 16 0.02 MBP (mmhg) 87 ± 14 92 ± 16 84 ± 16 0.06 Pulse pressure (mmhg) 29 ± 22 15 ± 13 29 ± 24 0.")
26 Hemodynamic data Parameter IABP on IABP off IABP restart P Heart rate 99 ± ± ± SBP (mmhg) 103 ± ± ± DBP (mmhg) 74 ± ± ± MBP (mmhg) 87 ± ± ± Pulse pressure (mmhg) 29 ± ± ± DBP increase (mmhg) 134 ± ± 26
27 Pulmonary artery catheter Parameter IABP on IABP off IABP restart P SBP, mmhg 24 ± 9 29 ± ± DBP, mmhg 16 ± 7 19 ± ± MBP, mmhg 19 ± 8 24 ± ± PAOP, mmhg 15 ± 8 19 ± ± Central venous oxygen saturation, % 73 ± ± ±
28 Pulmonary Artery Occlusion Pressure IABP to prevent pulmonary edema under peripheral ECMO
29 Echocardiographic data Parameter IABP on IABP off IABP restart P LVEDD (mm) 52 ± ± ± 13* $ LVESD (mm) 50 ± ± ± 13* 0.05 $ Velocity time integral (mm) 25 ± ± ± Cardiac output (l/min) 0.79 ± ± ± Diastolic velocity Transmitral early peak (E) (cm/s) 49 ± ± ± Transmitral late (A) (cm/s) 32 ± ± 9 31 ± E/A 1.26 ± ± ± Lateral mitral early annular (Ea) (cm/s) 6.4 ± ± ± E/Ea 8.6 ± ± ± S (cm/s) 4.9 ± ± ±
 1.26 ± 0.76 1.28 ± 0.70 1.28 ± 0.58 0.21 Range 0.56; 3.20 0.67;2.55 0.57;2.95 Cerebral hemisphere rso 2 Right, % 69.1 ± 5.")
30 NIRS data Near-infrared spectroscopy IABP on IABP off Thenar IABP restart P Baseline StO 2, % 82 ± 6 79 ± 8 82 ± Tissue desaturation during VOT, (%/s) 0.13 ± ± ± Range 0.04; ; ; 0.28 Tissue resaturation after VOT (%/s) 1.26 ± ± ± Range 0.56; ; ;2.95 Cerebral hemisphere rso 2 Right, % 69.1 ± ± ± Left, % 67.4 ± ± ±
31 PV (%) neity index MFI Heterogeneity index PPV (%) FCD (cm/cm² PPV (%) MFI SDF sublingual imaging IABP on IABP off IABP on again IABP on IABP off IABP on again 50
32 If Pulmonary edema occurs
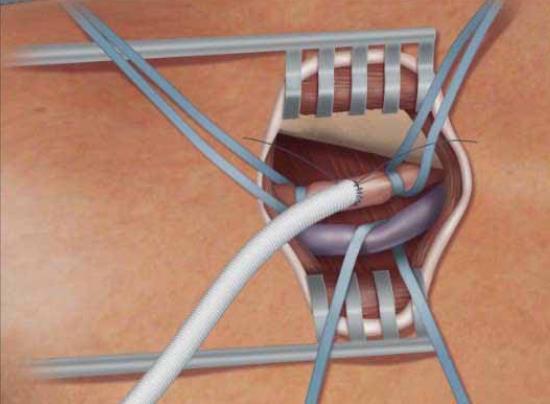

33 Impella 5.0
34 Conclusion For cardiogenic shock patients with little/no residual LV ejection while on peripheral VA-ECMO Restoring pulsatility and decreasing LV afterload with IABP Associated with smaller LV dimensions and lower pulmonary artery pressures But no impact on microcirculation parameters IABP might prevent severe hydrostatic pulmonary edema in this context



35 May
NE refractoriness: From Definition To Treatment... Prof. Alain Combes
 NE refractoriness: From Definition To Treatment... Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre
NE refractoriness: From Definition To Treatment... Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre
ECMO for Refractory Septic Shock Prof. Alain Combes
 ECMO for Refractory Septic Shock Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris
ECMO for Refractory Septic Shock Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris
Which mechanical assistance for cardiogenic shock?
 Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
Severe Myocarditis: A 2012 update
 Severe Myocarditis: A 2012 update Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris 6
Severe Myocarditis: A 2012 update Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris 6
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
ECMO/ECCO 2 R in Acute Respiratory Failure
 ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
ECMO as a bridge to durable LVAD therapy. Jonathan Haft, MD Department of Cardiac Surgery University of Michigan
 ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
ICU Volume 14 - Issue 1 - Spring Matrix
 ICU Volume 14 - Issue 1 - Spring 2014 - Matrix The ECMO Retrieval Team Authors Alain Combes, MD Medical-Surgical Intensive Care Unit ican, Institute of Cardiometabolism and Nutrition Hôpital de la Pitié
ICU Volume 14 - Issue 1 - Spring 2014 - Matrix The ECMO Retrieval Team Authors Alain Combes, MD Medical-Surgical Intensive Care Unit ican, Institute of Cardiometabolism and Nutrition Hôpital de la Pitié
Acute heart failure, beyond conventional treatment: persisting low output
 Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Andrew Civitello MD, FACC
 Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
The Role of Mechanical Circulatory Support in Cardiogenic Shock: When to Utilize
 The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Disclosure Information : No conflict of interest
 Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Echo assessment of patients with an ECMO device
 Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Acute Mechanical Circulatory Support Right Ventricular Support Devices
 Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Cardiogenic Shock Protocol
 Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support
 Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Introduction to Acute Mechanical Circulatory Support
 Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Acute peri-operative. Alexandre Mebazaa, Hôpital Lariboisière, Université Paris 7 U942 Inserm
 Acute peri-operative left heart failure Alexandre Mebazaa, Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts for this lecture Acute peri-operative
Acute peri-operative left heart failure Alexandre Mebazaa, Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts for this lecture Acute peri-operative
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities
 The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
MANAGEMENT OF CARDIOGENIC SHOCK
 MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction
 Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
Mechanical Cardiac Support in Acute Heart Failure. Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research
 Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Cardiogenic shock: Current management
 Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
LV Distension and ECLS Lungs
 LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
Adult Extracorporeal Life Support (ECLS)
") Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
CARDIOGENIC SHOCK. Antonio Pesenti. Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI)
") CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO)
") Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Ventricular Assisting Devices in the Cathlab. Unrestricted
 Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD
 A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
Καθετηριασμός δεξιάς κοιλίας. Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ
 Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Hemodynamic monitoring beyond cardiac output
 Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Treatment of patients after cardiac surgery. Training program Intensive Care Radboud University Nijmegen Medical Centre
 Treatment of patients after cardiac surgery Training program Intensive Care Radboud University Nijmegen Medical Centre General remarks Cardiac surgery reserved for complex cases Sicker patients with multiple
Treatment of patients after cardiac surgery Training program Intensive Care Radboud University Nijmegen Medical Centre General remarks Cardiac surgery reserved for complex cases Sicker patients with multiple
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
4/22/2016 Updated. AllinaHealthSystem. Cardiogenic Shock: Definition. No Disclosures. Cardiogenic Shock: Declining (But Still High) Case Fatality Rate
 Case Fatality Rate") 4/22/216 Updated Definition End-organ hypoperfusion secondary to cardiac failure Advanced Cardiopulmonary Support for the Critically Ill Adult April 22, 216 Cardiogenic Shock Michael A. Samara, MD FACC
4/22/216 Updated Definition End-organ hypoperfusion secondary to cardiac failure Advanced Cardiopulmonary Support for the Critically Ill Adult April 22, 216 Cardiogenic Shock Michael A. Samara, MD FACC
Ted Feldman, M.D., MSCAI FACC FESC
 Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
(Peripheral) Temperature and microcirculation
 Temperature and microcirculation") (Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
(Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
AATS/Cardiothoracic Critical Care Symposium
 AATS/Cardiothoracic Critical Care Symposium Balancing Pharmacologic and Mechanical Support Robert L Kormos MD, FACS, FRCS(C), FAHA I have no disclosures and will not discuss off label use of drugs or devices
AATS/Cardiothoracic Critical Care Symposium Balancing Pharmacologic and Mechanical Support Robert L Kormos MD, FACS, FRCS(C), FAHA I have no disclosures and will not discuss off label use of drugs or devices
A Future for the IABP in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany
 University of Lübeck, Germany") A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
Guideline compliance, utilization trends
 Guideline compliance, utilization trends and device selection Tilmann Schwab Cardiology / Intensive care Cardiac support IABP LVAD Transluminal l LVAD Cardiac support Emergency cardiac life support (ECLS)
Guideline compliance, utilization trends and device selection Tilmann Schwab Cardiology / Intensive care Cardiac support IABP LVAD Transluminal l LVAD Cardiac support Emergency cardiac life support (ECLS)
Section 6 Intra Aortic Balloon Pump
 Section 6 Intra Aortic Balloon Pump The Intra Aortic Balloon Pump (IABP) The balloon is synthetic and is made for single use only. It is threaded into the aorta, usually via a femoral approach. The balloon
Section 6 Intra Aortic Balloon Pump The Intra Aortic Balloon Pump (IABP) The balloon is synthetic and is made for single use only. It is threaded into the aorta, usually via a femoral approach. The balloon
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Understanding the Pediatric Ventricular Assist Device
 Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
Understanding the Pediatric Ventricular Assist Device W. James Parks, MSc., MD Pediatric Cardiologist Assistant Professor of Pediatrics and Radiology Children s Healthcare of Atlanta Sibley Heart Center
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
ECLS. The Basics. Jeannine Hermens Intensive Care Center UMC Utrecht
 ECLS The Basics Jeannine Hermens Intensive Care Center UMC Utrecht Conflict of interest None Terminology ECMO - ExtraCorporeal Membrane Oxygenation ECLS - ExtraCorporeal Life Support PLS - Veno-venous
ECLS The Basics Jeannine Hermens Intensive Care Center UMC Utrecht Conflict of interest None Terminology ECMO - ExtraCorporeal Membrane Oxygenation ECLS - ExtraCorporeal Life Support PLS - Veno-venous
To ECMO Or Not To ECMO Challenges of venous arterial ECMO. Dr Emily Granger St Vincent s Hospital Darlinghurst NSW
 To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
10/16/2017. Review the indications for ECMO in patients with. Respiratory failure Cardiac failure Cardiorespiratory failure
 Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS
 ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
ST-Elevation Myocardial Infarction & Cardiogenic Shock. - What Should We Do?
 ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ
 Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
Low cardiac output & Mechanical Support นายแพทย อรรถภ ม ส ศ ภอรรถ ศ ลยศาสตร ห วใจและทรวงอก โรงพยาบาล ราชว ถ Low cardiac output/cardiogenic Shock State of end-organ hypoperfusion due to cardiac failure.
Rhondalyn C. McLean. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume VII, A. Study Purpose and Rationale
 A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
Management of Severe Heart Failure Exacerbation
 Management of Severe Heart Failure Exacerbation Rocky Mountain Hospital Medicine Symposium November 5, 2017 Larry A. Allen, MD. MHS Medical Director, Advanced Heart Failure Presenter Disclosure Information
Management of Severe Heart Failure Exacerbation Rocky Mountain Hospital Medicine Symposium November 5, 2017 Larry A. Allen, MD. MHS Medical Director, Advanced Heart Failure Presenter Disclosure Information
IABP Timing & Fidelity. Pocket Reference Guide
 IABP Timing & Fidelity Pocket Reference Guide Correct IABP Timing A = One complete cardiac cycle R B = Unassisted aortic end diastolic pressure P T C = Unassisted systolic pressure D = Diastolic augmentation
IABP Timing & Fidelity Pocket Reference Guide Correct IABP Timing A = One complete cardiac cycle R B = Unassisted aortic end diastolic pressure P T C = Unassisted systolic pressure D = Diastolic augmentation
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University
 Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Diastology State of The Art Assessment
 Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
Circulatory Support: From IABP to LVAD
 Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Update on Mechanical Circulatory Support. AATS May 5, 2010 Toronto, ON Canada
 Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Update on Mechanical Circulatory Support AATS May 5, 2010 Toronto, ON Canada Disclosures NONE Emergency Circulatory Support ECMO Tandem Heart Impella Assessment Cardiac Function Pulmonary function Valvular
Epidemiology of Heart Failure in Adults
 Cardiac Critical Care : Focused on IABP & PCPS Epidemiology of Heart Failure in Adults Prevalence Incidence Mortality 2004 Hospital Cost 2007 2004 Age 20+ (New Cases) All Ages Discharges Age 35+ 2004 All
Cardiac Critical Care : Focused on IABP & PCPS Epidemiology of Heart Failure in Adults Prevalence Incidence Mortality 2004 Hospital Cost 2007 2004 Age 20+ (New Cases) All Ages Discharges Age 35+ 2004 All
Recovering Hearts. Saving Lives.
 Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Fluid responsiveness and extravascular lung water
 Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management
 Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Counterpulsation. John N. Nanas, MD, PhD. Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece
 John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft
 Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Modern Left Ventricular Assist Devices (LVAD) : An Intro, Complications, and Emergencies
 : An Intro, Complications, and Emergencies") Modern Left Ventricular Assist Devices (LVAD) : An Intro, Complications, and Emergencies ERIC T. ROME D.O. HEART FAILURE, MECHANICAL ASSISTANCE AND TRANSPLANTATION CVI Left Ventricular Assist Device An
Modern Left Ventricular Assist Devices (LVAD) : An Intro, Complications, and Emergencies ERIC T. ROME D.O. HEART FAILURE, MECHANICAL ASSISTANCE AND TRANSPLANTATION CVI Left Ventricular Assist Device An
Extracorporeal Membrane Oxygenation in Cardiac Intensive Care Unit
 10 Review Article THIEME Extracorporeal Membrane Oxygenation in Cardiac Intensive Care Unit Venkat Goyal 1 Pranay Oza 1 1 Riddhi Vinayak Critical Care and Cardiac Centre, Mumbai, Maharashtra, India J Card
10 Review Article THIEME Extracorporeal Membrane Oxygenation in Cardiac Intensive Care Unit Venkat Goyal 1 Pranay Oza 1 1 Riddhi Vinayak Critical Care and Cardiac Centre, Mumbai, Maharashtra, India J Card
Prof. Dr. Iman Riad Mohamed Abdel Aal
 The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive