Fluid responsiveness and extravascular lung water
|
|
|
- Samuel Dalton
- 5 years ago
- Views:
Transcription
1 Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France
2 Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
3 Critically ill patients often experience hemodynamic instability Clinicians are tempted to give fluid to restore adequate hemodynamic conditions However, often, patients were already fluid-resuscitated for hours or days potential fluid overload with subsequent risks of pulmonary edema especially in conditions of increased lung permeability positive cumulative fluid balance: independent predictor of death
4

5 Highest positive fluid balance
6

7
8 Critically ill patients often experience hemodynamic instability Clinicians are tempted to give fluid to restore adequate hemodynamic conditions However, often, patients were already fluid-resuscitated for hours or days potential fluid overload with subsequent risks of pulmonary edema especially in conditions of increased lung permeability positive cumulative fluid balance: independent predictor of death no certainty of fluid responsiveness
9 CHEST 2002, 121: Only 52% of patients responded to fluid administration in terms of CO increase
10 Critically ill patients often experience hemodynamic instability However, Clinicians are tempted to give fluid to restore adequate hemodynamic conditions Fluid infusion benefit / risk ratio? often, patients were already fluid-resuscitated for hours or days potential fluid overload with subsequent risks of pulmonary edema especially in this condition of increased lung permeability Predictors of fluid responsiveness are required positive cumulative fluid balance: independent predictor of death no certainty of fluid responsiveness Markers of lung edema are required
11 SSC «static» approach «dynamic» approach
12 SSC approach: Stop IV fluids when a certain level of CVP has been reached Stroke Volume preload unresponsiveness CVP
13 Initial resuscitation 1. Protocolized, quantitative resuscitation of patients with sepsis-induced hypoperfusion (defined as hypotension persisting after initial fluid challenge or blood lactate 4 mmol/l). Goals during the first 6h of resuscitation: (a) pressure 8-12 mmhg Central venous pressure 8-12 mmhg (b) Mean arterial pressure (MAP) 65 mmhg (c) Urine output 0.5 ml.kg -1 h (d) Central venous or mixed venous oxygen saturation 70 or 65%, respectively (grade 1C) Central venous pressure mmhg if MV
14 normal heart preload responsiveness Stroke volume failing heart preload unresponsiveness. CVP
15 Responders Nonresponders

16 Crit Care Med 2013; 41: pts Summary AUC 0.56 Predicting fluid responsiveness with CVP is like
17 SSC «static» approach «dynamic» approach No. Statement/recommendation GRADE level of recommendation; quality of evidence 30. We recommend not to target any absolute value of ventricular filling pressure or volume 31. We recommend using dynamic over static variables to predict fluid responsiveness, when applicable Level 1; QoE moderate (B) Level 1; QoE moderate (B)
18 Dynamic indices of preload responsiveness normal heart Stroke volume preload responsiveness failing heart. preload unresponsiveness Ventricular preload
19 Stroke volume preload responsiveness preload unresponsiveness A B Ventricular preload

20 Sensitivity PPV CVP PAOP 1 - Specificity


21 Anesth Analg 2011; 113:523-8 Chest 2005;128; Chest 2004, 126: PPV Crit Care Med 2005;33: M. Cannesson, J. Slieker, O. Desebbe, F. Fahdi,O. Bastien, JJ. Lehot X. Monnet 1,2*,L. Guerin 1,2,M. Jozwiak 1,2,A. Bataille 1,2,F. Julien 1,2,C. Richard 1,2,J-L. Teboul 1,2



22 Pulse Pressure Variation Calculated automatically and displayed in real-time by usual hemodynamic monitors
23

24 Threshold: 12% AUC: 0.94
25 Arterial pressure waveform analysis Stroke volume Arterial Pressure Stroke Volume Variation Calculated automatically and displayed in real-time by new hemodynamic monitors

26 Arterial pressure waveform analysis Stroke volume Arterial Pressure




27 X. Monnet 1,2* L., Guerin 1,2,M. Jozwiak 1,2,A. Bataille 1,2 F., Julien 1,2,C. Richard 1,2,J-L. Teboul 1,2 Assessing fluid responsiveness by stroke volume variation in mechanically ventilated patients with severe sepsis G. Marx, T. Cope, L. McCrossan, S. Swaraj, C. Cowan, SM. Mostafa, R. Wenstone, M. Leuwer European Journal of Anaesthesiology 2004; 21: Chest 2005;128;
28 685 pts

29 In all these situations and in case of any doubt about interpretation other reliable dynamic tests are required and are now available
30
31 Stroke Volume PLR mimics fluid challenge preload responsiveness b' a' Unlike fluid challenge, no fluid is infused, preload unresponsiveness and, the effects are reversible and transient b a The hemodynamic response to PLR A PLR B Ventricular preload can predict the hemodynamic response to volume infusion

32 Crit Care 2015, 19:18

33 Real-time CO response to PLR 2012
34 PLR-induced changes in CO PLR-induced changes in AP Study name sample size AUC Study name sample size AUC Monnet CCM Lafanéchère CC Lamia ICM Maizel ICM Monnet CCM Thiel CC Biais CC Preau CCM Monnet CCM Monnet CCM Preau CCM
35 n = 30 pts n = 30 pts
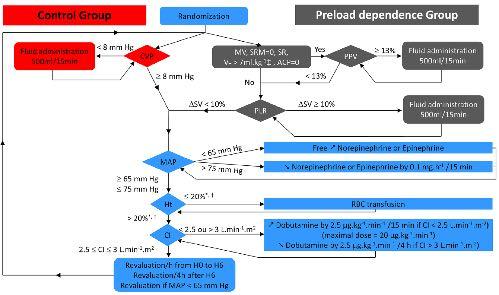
36 Preload dependence group Control group

37 Control Preload dependence
38 Critically ill patients often experience hemodynamic instability Fluid infusion benefit / risk ratio? Predictors of fluid responsiveness are required Markers of lung edema are required
39 How to assess the risk of pulmonary edema? PAOP?
40 Increased lung capillary permeability Increased inflammation volume of lung edema 12 Pcrit mmhg Pulmonary artery occlusion pressure
41 Increased inflammation Amount of pulmonary edema Increased lung capillary permeability 12 mmhg Pcrit Pulmonary artery occlusion pressure
42 EVLW ml/kg PAOP mmhg
43 How to assess the risk of pulmonary edema? PAOP? EVLW? cannot reliably assess the risk of pulmonary edema


44 Central Venous Catheter (cold bolus injection) Thermodilution femoral arterial catheter
45 200 pts D 28 mortality: 54% Odds Ratio ( CI 95%) p value Maximal blood lactate 1.29 ( ) Mean PEEP 0.78 ( ) Minimal PaO 2 / FiO ( ) SAPS II 1.03 ( ) 0.02 EVLW max 1.07 ( ) Mean fluid balance ( ) 0.02
46
47 Cumulative fluid balance (L) 7 5 * * * * PAOP group 3 1 EVLW group * p < vs time Time (hours)
48 * * PAOP group EVLW group 5 0 MV days ICU days

49 PVPI = EVLW/Pulmonary blood volume PVPI marker of lung µvessels permeability
50 200 pts D 28 mortality: 54% Odds Ratio ( CI 95%) p value Maximal blood lactate 1.27 ( ) Mean PEEP 0.78 ( ) Minimal PaO 2 / FiO ( ) SAPS II 1.03 ( ) PVPI max 1.07 ( ) 0.03 Mean fluid balance ( ) 0.03
51 Decision of starting fluid administration presence of hemodynamic instability/peripheral hypoperfusion (mottled skin, hypotension, oliguria, hyperlactatemia ) and presence of preload responsiveness and limited risks of fluid overload
52 Decision of stopping fluid administration disappearance of hemodynamic instability/peripheral hypoperfusion or appearance of preload unresponsiveness or appearance of fluid overload or marked increase in EVLW
53 Conclusion Before infusing fluids in critically ill patients, and especially in ARDS patients Fluid infusion benefit / risk ratio should be assessed patient per patient Predictors of fluid responsiveness are required Markers of lung edema are required


54
Preload optimisation in severe sepsis and septic shock
 Preload optimisation in severe sepsis and septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris South France Conflicts of interest Member of themedical Advisory Board ofpulsion
Preload optimisation in severe sepsis and septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris South France Conflicts of interest Member of themedical Advisory Board ofpulsion
Hemodynamic monitoring beyond cardiac output
 Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy
 Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Jan M. Headley, R.N. BS
 Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Using Functional Hemodynamic Indicators to Guide Fluid Therapy
 CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
Prof. Dr. Iman Riad Mohamed Abdel Aal
 The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL. Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
Functional Hemodynamic Monitoring and Management A practical Approach
 Functional Hemodynamic Monitoring and Management A practical Approach Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf University Hospital Hamburg, Germany Euronaesthesia
Functional Hemodynamic Monitoring and Management A practical Approach Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf University Hospital Hamburg, Germany Euronaesthesia
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies. Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC
 Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
3/14/2017. Disclosures. None. Outline. Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM
 Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
Hemodynamic monitoring should be kept as simple as possible. But not simpler!
 Hemodynamic monitoring should be kept as simple as possible. But not simpler! Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University,
Hemodynamic monitoring should be kept as simple as possible. But not simpler! Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University,
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
The cornerstone of treating patients with hypotension,
 Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Disclaimer. Improving MET-based patient care using treatment algorithms. Michael R. Pinsky, MD, Dr hc. Different Environments Demand Different Rules
 Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
PCV and PAOP Old habits die hard!
 PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
Shock - from Diagnostic to Therapeutic Implications
 Shock - from Diagnostic to Therapeutic Implications Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. LEARNING OBJECTIVES Review the markers of tissue
Shock - from Diagnostic to Therapeutic Implications Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. LEARNING OBJECTIVES Review the markers of tissue
Oregon Health and Science University Portland, Oregon USA
 Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists
Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care
 28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Hemodynamic Monitoring in Critically ill Patients in Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory
 Hemodynamic Monitoring in Critically ill Patients in 2017 Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory Rationale for Hemodynamic Monitoring Identify the presence of hemodynamic instability Identify
Hemodynamic Monitoring in Critically ill Patients in 2017 Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory Rationale for Hemodynamic Monitoring Identify the presence of hemodynamic instability Identify
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
Jarisch A. Kreislauffragen, Dünser et al. Critical Care 2013, 17:326 Sunday, March 30, 14
 It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
The Hemodynamic Puzzle
 The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge*
 Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge* David Osman, MD; Christophe Ridel, MD; Patrick Ray, MD; Xavier Monnet, MD, PhD; Nadia Anguel, MD; Christian
Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge* David Osman, MD; Christophe Ridel, MD; Patrick Ray, MD; Xavier Monnet, MD, PhD; Nadia Anguel, MD; Christian
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Norepinephrine in septic shock
 Norepinephrine in septic shock Prof. Zsolt Molnár zsoltmolna@gmail.com Department of Anaesthesia and Intensive Therapy University of Szeged, Hungary A few months ago should we give it earlier? (Courtesy
Norepinephrine in septic shock Prof. Zsolt Molnár zsoltmolna@gmail.com Department of Anaesthesia and Intensive Therapy University of Szeged, Hungary A few months ago should we give it earlier? (Courtesy
How can the PiCCO improve protocolized care?
 How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR
 IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
PulsioFlex Patient focused flexibility
 PulsioFlex Patient focused flexibility Modular platform with intelligent visualisation for advanced patient Minimally invasive perioperative cardiac output trend with ProAQT Enables calibrated cardiac
PulsioFlex Patient focused flexibility Modular platform with intelligent visualisation for advanced patient Minimally invasive perioperative cardiac output trend with ProAQT Enables calibrated cardiac
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
ENDPOINTS OF RESUSCITATION
 ENDPOINTS OF RESUSCITATION Fred Pieracci, MD, MPH Acute Care Surgeon Denver Health Medical Center Assistant Professor of Surgery University of Colorado Health Science Center OUTLINE Recognition and characterization
ENDPOINTS OF RESUSCITATION Fred Pieracci, MD, MPH Acute Care Surgeon Denver Health Medical Center Assistant Professor of Surgery University of Colorado Health Science Center OUTLINE Recognition and characterization
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the PreSep oximetry catheter for
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the PreSep oximetry catheter for continuous central venous oximetry (ScvO 2 ) 3 The Vigileo
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the PreSep oximetry catheter for continuous central venous oximetry (ScvO 2 ) 3 The Vigileo
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! seminaires iris. Daniel De Backer
 Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles
Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
How Do I Integrate Hemodynamic Variables When Managing Septic Shock?
 Korean J Crit Care Med 2016 November 31(4):265-275 / ISSN 2383-4870 (Print) ㆍ ISSN 2383-4889 (Online) Review How Do I Integrate Hemodynamic Variables When Managing Septic Shock? Olfa Hamzaoui, M.D. 1,
Korean J Crit Care Med 2016 November 31(4):265-275 / ISSN 2383-4870 (Print) ㆍ ISSN 2383-4889 (Online) Review How Do I Integrate Hemodynamic Variables When Managing Septic Shock? Olfa Hamzaoui, M.D. 1,
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children?
 Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Dr Sameer Jog Consultant Intensivist, Deenanath Mangeshkar Hospital, Pune MD ( Int Med) EDIC IDCCM
 EDIC IDCCM") Dr Sameer Jog Consultant Intensivist, Deenanath Mangeshkar Hospital, Pune MD ( Int Med) EDIC IDCCM How I give fluids? - Obvious!! How I give fluids?not so obvious Nobody is correct!! Deenanath Mangeshkar
Dr Sameer Jog Consultant Intensivist, Deenanath Mangeshkar Hospital, Pune MD ( Int Med) EDIC IDCCM How I give fluids? - Obvious!! How I give fluids?not so obvious Nobody is correct!! Deenanath Mangeshkar
NONINVASIVE/MINIMALLY INVASIVE HEMODYNAMIC MONITORING
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Hemodynamic Monitoring To Guide Volume Resuscitation
 Hemodynamic Monitoring To Guide Volume Resuscitation Nick Johnson, MD Acting Assistant Professor Division of Emergency Medicine Attending Physician, Medical & Neuro-Intensive Care Units Harborview Medical
Hemodynamic Monitoring To Guide Volume Resuscitation Nick Johnson, MD Acting Assistant Professor Division of Emergency Medicine Attending Physician, Medical & Neuro-Intensive Care Units Harborview Medical
EVOLUCIÓN DE LA MONITORIZACIÓN CARDIOVASCULAR EN LA UCI
 EVOLUCIÓN DE LA MONITORIZACIÓN CARDIOVASCULAR EN LA UCI Antonio Artigas Critical Care Center Sabadell Hospital CIBER Enfermedades Respiratorias Autonomos University of Barcelona Spain aartigas@tauli.cat
EVOLUCIÓN DE LA MONITORIZACIÓN CARDIOVASCULAR EN LA UCI Antonio Artigas Critical Care Center Sabadell Hospital CIBER Enfermedades Respiratorias Autonomos University of Barcelona Spain aartigas@tauli.cat
Review Article Echocardiographic Assessment of Preload Responsiveness in Critically Ill Patients
 Cardiology Research and Practice Volume 2012, Article ID 819696, 7 pages doi:10.1155/2012/819696 Review Article Echocardiographic Assessment of Preload Responsiveness in Critically Ill Patients Alexander
Cardiology Research and Practice Volume 2012, Article ID 819696, 7 pages doi:10.1155/2012/819696 Review Article Echocardiographic Assessment of Preload Responsiveness in Critically Ill Patients Alexander
WE NEED TO REDISCOVER PHYSIOLOGY!
 WE NEED TO REDISCOVER PHYSIOLOGY! MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK DECLARATIONS OF INTEREST GE Healthcare (manufacturer of Venue ultrasound/echo)
WE NEED TO REDISCOVER PHYSIOLOGY! MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK DECLARATIONS OF INTEREST GE Healthcare (manufacturer of Venue ultrasound/echo)
(Peripheral) Temperature and microcirculation
 Temperature and microcirculation") (Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
(Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
How to resuscitate the patient in early sepsis? A physiological approach. J.G. van der Hoeven, Nijmegen
 How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
Response to Fluid Boluses in the Fluid and Catheter Treatment Trial
 [ Original Research Critical Care ] Response to Fluid Boluses in the Fluid and Catheter Treatment Trial Matthew R. Lammi, MD ; Brianne Aiello, MD ; Gregory T. Burg, MD ; Tayyab Rehman, MD ; Ivor S. Douglas,
[ Original Research Critical Care ] Response to Fluid Boluses in the Fluid and Catheter Treatment Trial Matthew R. Lammi, MD ; Brianne Aiello, MD ; Gregory T. Burg, MD ; Tayyab Rehman, MD ; Ivor S. Douglas,
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS
 Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
An algorithmic approach to the very high risk surgical patient
 An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients
 Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
Fluid bolus of 20% Albumin in post-cardiac surgical patient: a prospective observational study of effect duration
 Fluid bolus of 20% Albumin in post-cardiac surgical patient: a prospective observational study of effect duration Investigators: Salvatore Cutuli, Eduardo Osawa, Rinaldo Bellomo Affiliations: 1. Department
Fluid bolus of 20% Albumin in post-cardiac surgical patient: a prospective observational study of effect duration Investigators: Salvatore Cutuli, Eduardo Osawa, Rinaldo Bellomo Affiliations: 1. Department
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Sepsis and septic shock Practical hemodynamic consequences. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Predicting cardiac output responses to passive leg raising by a PEEP-induced increase in central venous pressure, in cardiac surgery patients
 Chapter 10 Predicting cardiac output responses to passive leg raising by a PEEP-induced increase in central venous pressure, in cardiac surgery patients Bart Geerts, Leon Aarts, Johan Groeneveld and Jos
Chapter 10 Predicting cardiac output responses to passive leg raising by a PEEP-induced increase in central venous pressure, in cardiac surgery patients Bart Geerts, Leon Aarts, Johan Groeneveld and Jos
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
FloTrac Sensor and Edwards PreSep Central Venous Oximetry Catheter Case Presentations
 Edwards FloTrac Sensor & Edwards Vigileo Monitor FloTrac Sensor and Edwards PreSep Central Venous Oximetry Catheter Case Presentations 1 Topics System Configuration FloTrac Sensor and PreSep Catheter Thoracotomy
Edwards FloTrac Sensor & Edwards Vigileo Monitor FloTrac Sensor and Edwards PreSep Central Venous Oximetry Catheter Case Presentations 1 Topics System Configuration FloTrac Sensor and PreSep Catheter Thoracotomy
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
ICU Volume 12 - Issue 4 - Winter 2012/ Matrix Features
 ICU Volume 12 - Issue 4 - Winter 2012/2013 - Matrix Features Fluid Management in Critically Ill Patients: A Guided Approach Prof. Antonio Artigas, MD, PhD ICU Management & Practice Editorial Board Member
ICU Volume 12 - Issue 4 - Winter 2012/2013 - Matrix Features Fluid Management in Critically Ill Patients: A Guided Approach Prof. Antonio Artigas, MD, PhD ICU Management & Practice Editorial Board Member
Sepsis & Beyond Guidelines & Goal-Directed Therapy
 Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Bioreactance-based passive leg raising test can predict fluid responsiveness in elderly patients with septic shock
 Original Article Page 1 of 6 Bioreactance-based passive leg raising test can predict fluid responsiveness in elderly patients with septic shock Caibao Hu 1 *, Guolong Cai 1 *, Jing Yan 1, Hongjie Tong
Original Article Page 1 of 6 Bioreactance-based passive leg raising test can predict fluid responsiveness in elderly patients with septic shock Caibao Hu 1 *, Guolong Cai 1 *, Jing Yan 1, Hongjie Tong
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Assessing Patients During Septic Shock Resuscitation
 CE 1.5 HOURS Continuing Education Assessing Patients During Septic Shock Resuscitation How to integrate capillary refill time and skin mottling score into the six-hour bundle. ABSTRACT: In 2015, the Surviving
CE 1.5 HOURS Continuing Education Assessing Patients During Septic Shock Resuscitation How to integrate capillary refill time and skin mottling score into the six-hour bundle. ABSTRACT: In 2015, the Surviving
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University
 Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma