Improvement of drug adherence using single pill combinations:
|
|
|
- Annabel King
- 5 years ago
- Views:
Transcription
1 Improvement of drug adherence using single pill combinations: what is the evidence? Prof. Michel Burnier Service of Nephrology and Hypertension, CHUV, Lausanne, Switzerland
2 Potentialcauses of non-adherence Health system: Disease: Patient : Therapy: Socio-economic: Poor quality of provider-patient relationship Poor communication, lack of access to healthcare Lack of continuity of care Asymptomatic chronic disease, Mental health disorder Physical impairment, cognitive impairment Psychological/behavioral; younger age, race Complexity of regimen, side-effects Low literacy; higher medication costs Poor social support
3 FDC in Disease Management Patients require multiple medications to reach targets Single pill combinations offer some advantages: Efficacy Adherence Cost Convenience Patient-perceived wellness Side effects
4 Question In all reviews, single-pill combinations are mentionned as potential tools to improve drug adherence. What is the evidence for this assumption? What is the importance of the effect?
5 What is known!
6 Compliance rates by dosing frequency Percent Compliance n = 7-11 studies QD BID TID QID P.Ruud, AHJ, 1995
7 Number of comedications and pharmacies used as factors related to compliance Odds ratio Number of medications Number of pharmacies 0.6 Monane et al, AJH, > >1
8 Long-term persistence by initially prescribed drug class Patients cumulative persistence rate (%) ACE inhibitor CCB Beta blocker Diuretic Time (yrs) N= 22,918 newly diagnosed hypertensive patients in Saskatchevan, Canada Caro et al CMAJ, 1999; 160:41-46
9 Persistence rates by antihypertensive class 100 Patients remainin g on therapy at 1 year (%) * AIIRAs ACE inhibitors CCBs Beta blockers Diuretic Bloom S. Clin Ther 1998, 20:
10 One year persistence of use of lipid-lowering medications in USA and Canada Avorn et al, JAMA, NewJersey Quebec Days Covered (%) Cholest Niacin Gemfib Probuc Colest Clofib HMG CoA
11 Compliance to the morning and evening dose of an AT 1 receptor blocker in hypertensive patients ** *** * ** Compliance to drug ( %) am pm am pm am pm am pm Losartan o.d. Losartan bid Irbesartan o.d. Irbesartan bid Würzner et al, J Hypertens, 2001
12 Drug adherence varies during the week and during the day Vrijens, B. et al. BMJ 2008;336:
13 Better Persistence of Treatment in Established Hypertensive Patients Caro et al, Can J Med Assoc. 1999; 160:31
14 The studies! The first studies assessing the potential benefits of single-pill combinations have been performed in the fields of: infectious diseases (Tbc, HIV, malaria ) hypertension diabetes


15 Connor et al, Bulletin of WHO, 2003
16 Persistence to Lisinopril/HCTZ Fixed-dose Combination Versus Free Combination Persisten nce (%) *p<0.05 US pharmacy benefit manager data (n=2,268) Month Lisinopril/HCTZ (single pill) Lisinopril + diuretic (two pills) 68.7% 18.8%* 57.8% Dezii. Manag Care 2000;9 (Suppl):S2 S6
17 Compliance with Fixed-dose Combination Amlodipine Besylate/Benazepril HCL Versus Component-based Therapy Medication possession ra atio (MPR) US database analysis (n=5,732) * * * 80.8 * 77.9 * * * 73.8 * Amlodipine/Benazepril (single pill) Component-based therapy (n=2,754) (n=2,978) *p<0.001 Age group Overall Taylor et al. CHF 2003;9:324 32
18 Persistence to ACE Inhibitor/HCTZ Fixed-dose Combination Versus Free Combination ients on treatment Fraction of pati Cohort study of general practice research data (n=755) *p< Month since start of therapy Fixed dose combination therapy Co-administration of two pills 12%* Sturkenboom. J Hypertens 2005;23 (Suppl 2):S326
19 Percentage of Patients Fully Compliant with ACE Inhibitor/HCTZ Fixed-dose Combination Versus Free Combination Patients fu ully compliant (%) Cohort study of general practice research data (n=755) 21% 17% Months since start of therapy Fixed-dose combination therapy Co-administration of two pills Patients on free combination had a higher odds ratio (OR) of being non-compliant than patients on fixed-dose combination OR 2.09 (95% CI, ) Sturkenboom. J Hypertens 2005;23(Suppl 2):S326
20 Compliance with Amlodipine/atorvastatin Fixeddose Combination versus Free-Combination in Patients on Multiple Therapies for CV Risk AM/AT FD: Amlodipine/atorvastatin (fixed-dose) AM+AT FC: Amlodipine plus atorvastatin (free) OC+OS FC: Other CCB plus other statin (free) Patients compliant (%) AM/AT FD AM+AT FC OC+OS FC Patel et al. J Hypertens 2006;24(Suppl 6):S65
21 Compliance to the morning and evening dose of an AT 1 receptor blocker in hypertensive patients ** *** * ** Compliance to drug ( %) am pm am pm am pm am pm Losartan o.d. Losartan bid Irbesartan o.d. Irbesartan bid Würzner et al, J Hypertens, 2001


22 A 2 nd meta-analysis : characteristics of the studies Bangalore et al, Am J Med, 2007
23 Fixed doses combinations improve persistence! Bangalore et al, Am J Med, 2007
24 Fixed doses combinations in randomized controlled studies Bangalore et al, Am J Med, 2007
25 Fixed doses combinations in hypertension studies Bangalore et al, Am J Med, 2007
26 A 3 rd meta-analysis: Systolic and diastolic BP reduction with use of an FDC as compared with its free-drug combination Gupta, A. K. et al. Hypertension 2010;55:
27 Adverse effects associated with the use of an FDC as compared with its free-drug combination Gupta, A. K. et al. Hypertension 2010;55:
28 What are the limitations of actual studies on FDC? Many studies are retrospective Studies are often too small and do not have enough power The definition of drug adherence is variable and most studies investigated persistence to therapy Most studies are of short duration (6 months) Most studies do not assessed any clinical endpoint Confounding factors are not taken into account
29 Methods to measure drug adherence Non-invasive methods Electronic monitoring Directly observed therapy Patient interview Patient diary Adherence questionnaire Prescription record review Pill count Drug measurement in body fluids Biomarker measurement in body fluids Invasive methods Less accurate Precision of the method
30 Effect of home blood pressure monitoring on compliance to antihypertensive therapy 7.0 Vrijens, Home BP measurements n = 66 Number of pills per week No measurements (n= 61) weeks
31 Physician visits and comorbid cardiac disease as factors related to compliance Number of visits Presence of CHF or CAD Odds ratio >8 No Yes
32 Persistence with antihypertensive agents Patients 60 persistent with 40 therapy (%) 20 AIIRAs* ACE inhibitors CCBs Beta blockers Diuretics Combination Other Time (months) Database from Saskatchewan, Canada. Regimen is initially prescribed class filled between 1/1/95 and 1/9/98. *P<0.001 AIIRAs vs all other classes combined at all time points. Chaput AJ. Can J Cardiol. 2000;16(suppl F):194F.
33 During multiple drug therapies, is non-adherence homogenous with all drugs?


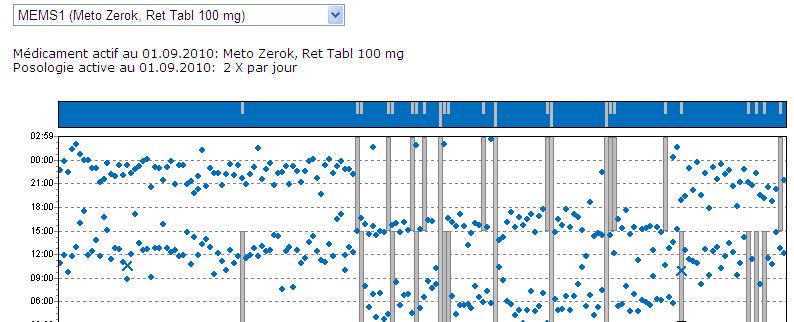
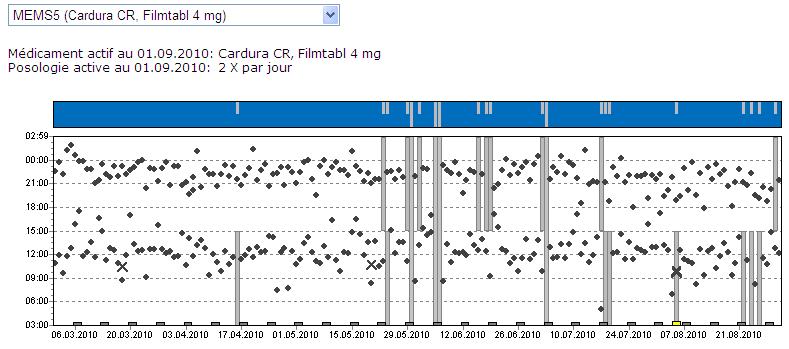
34 A clinical example FDC
35
36 One year monitoring of compliance in hypertensive patients Compliance (%) Drug A Drug B Drug A Drug B Drug A Drug B Patient number
37 The consequences of non-adherence with drug therapy "Rebound" hypertension (e.g., beta blocker stopped suddenly) increases MI risk acutely and perhaps the CV risk. Direct costs to healthcare system Wasted pills (purchased, not taken) "Wasted" doctor visits (advice not taken) Opportunity ("Indirect") costs Tradeoff between not avoiding clinical events and averting the need to treat uncomplicated hypertension
38 Drug adherence is a very irregular and dynamic process. Arrows indicate days on which medication was not taken Vrijens, B. et al. BMJ 2008;336:
39 Variability of BP during visits and cardiovascular risk Rothwell et al, Lancet 2010
40 Hazard ratios for risks of stroke and acute coronary events in ASCOT-BPLA patients according to BP variability within visits
41 Effects of 2 missed doses on blood pressure control On-treatment After 2 missed doses Changes in BP (mmhg) * Diltiazem Amlodipine Diltiazem Amlodipine Leenen et al, 1996
42 Predicted mean SBP reduction with aliskiren, irbesartan or ramipril for different levels of adherence Palatini et al, J Hum Hypertens 2010, and Burnier et al, submitted
43 Mean office SBP-lowering effect and off-rate a for aliskiren, irbesartan and ramipril Antihypertensive agent Mean office SBPlowering effect, mmhg Off-rate, a mmhg/day Aliskiren 300 mg Irbesartan 300 mg Ramipril 10 mg a Rate of loss of antihypertensive effect when treatment is stopped. SBP, systolic blood pressure Burnier et al, submitted

 Burnier et al,")
44 Predicted reduction in absolute CVD risk, event for aliskiren, irbesartan or ramipril at different adherence levels Level of adherence (%) Burnier et al, submitted
45 Impact of missed doses of single pill combinations Blood Pressure Ttt Missed Doses Rebound? Short acting drug Long acting drug Single-pill combin. Time
46 Conclusions 1. The evidence that single pill combinations improve drug adherence are relatively weak and the improvement appears to be small. 2. The impact of single pill combinations on clinical endpoints remains to be demonstrated 3. Methodologically adequate prospective studies need to be carried out.
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
State of the art treatment of hypertension: established and new drugs. Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland
 State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
Potential synergy between lipid-lowering and blood-pressure-lowering, and Single pill benefit in patient s adherence
 Potential synergy between lipid-lowering and blood-pressure-lowering, and Single pill benefit in patient s adherence Park, Chang Gyu Korea University Guro Hospital ASCOT-BPLA and LLA Primary Objectives
Potential synergy between lipid-lowering and blood-pressure-lowering, and Single pill benefit in patient s adherence Park, Chang Gyu Korea University Guro Hospital ASCOT-BPLA and LLA Primary Objectives
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Getting Hypertension Under Control
 Getting Hypertension Under Control Learning Objectives EXPLAIN the factors involved in patient medication non-adherence. OUTLINE the results of studies focusing on medication adherence issues in patients
Getting Hypertension Under Control Learning Objectives EXPLAIN the factors involved in patient medication non-adherence. OUTLINE the results of studies focusing on medication adherence issues in patients
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
ASSOCIATION MEDICAMENTEUSE ET OBSERVANCE THERAPEUTIQUE: QUOI DE NEUF? Philippe van de Borne Service de cardiologie,hopital Erasme, Bruxelles,Belgique
 ASSOCIATION MEDICAMENTEUSE ET OBSERVANCE THERAPEUTIQUE: QUOI DE NEUF? Philippe van de Borne Service de cardiologie,hopital Erasme, Bruxelles,Belgique Adherence, compliance, persistence: definitions Adherence
ASSOCIATION MEDICAMENTEUSE ET OBSERVANCE THERAPEUTIQUE: QUOI DE NEUF? Philippe van de Borne Service de cardiologie,hopital Erasme, Bruxelles,Belgique Adherence, compliance, persistence: definitions Adherence
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Improve the Adherence, Save the Life
 Improve the Adherence, Save the Life Park, Chang Gyu Korea University Guro Hospital Cardiovascular Center Seoul, Korea Modifiable CVD Risk Factors Obesity BMI Hypertension Cholesterol LDL HDL Diabetes
Improve the Adherence, Save the Life Park, Chang Gyu Korea University Guro Hospital Cardiovascular Center Seoul, Korea Modifiable CVD Risk Factors Obesity BMI Hypertension Cholesterol LDL HDL Diabetes
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Rationale for the use of Single Pill Combination. Yong Jin Kim, MD Seoul National University Hospital
 Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Individual management of arterial hypertension. Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki
 Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Ferrari R, Fox K, Bertrand M, Mourad J.J, Akkerhuis KM, Van Vark L, Boersma E.
 Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
Don t let the pressure get to you:
 Balanced information for better care Don t let the pressure get to you: Current evidence-based goals for treating hypertension A cornerstone of primary care: Lowering high blood pressure prevents cardiovascular
Balanced information for better care Don t let the pressure get to you: Current evidence-based goals for treating hypertension A cornerstone of primary care: Lowering high blood pressure prevents cardiovascular
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Pre-ALLHAT Drug Use. Diuretics. ß-Blockers. ACE Inhibitors. CCBs. Year. % of Treated Patients on Medication. CCBs. Beta Blockers.
 Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Blood pressure treatment target in diabetes. Should it be <130 mmhg?
 Blood pressure treatment target in diabetes Should it be
Blood pressure treatment target in diabetes Should it be
Adherence to medication in cardiovascular disease
 Working Groups of the Hellenic Society of Cardiology 2016 Adherence to medication in cardiovascular disease Gregory Giamouzis, MD, PhD Associate Professor of Cardiology Department of Cardiology, Larissa
Working Groups of the Hellenic Society of Cardiology 2016 Adherence to medication in cardiovascular disease Gregory Giamouzis, MD, PhD Associate Professor of Cardiology Department of Cardiology, Larissa
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico
 Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Traitements associés chez l hypertendu: Statines, Aspirine
 Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC
 and Asian data of ARB/CCB SPC") Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Valsartan Amlodipine HCT Combination: Control To Goal. Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI. Prof of cardiology Ain Shams University
 Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017
 Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017 The most important reason for treating hypertension in primary care is to prevent
Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017 The most important reason for treating hypertension in primary care is to prevent
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Supplement materials:
 Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Impact of compliance with antihypertensive and lipid-lowering treatment on cardiovascular risk Benefits
 R E V I E W Hellenic Journal of Atherosclerosis 1(1):18 25 Impact of compliance with antihypertensive and lipid-lowering treatment on cardiovascular risk Benefits of fixed-dose combinations F. Barkas,
R E V I E W Hellenic Journal of Atherosclerosis 1(1):18 25 Impact of compliance with antihypertensive and lipid-lowering treatment on cardiovascular risk Benefits of fixed-dose combinations F. Barkas,
ALLHAT. ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status
 ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
Clinical cases with Coversyl 10 mg
 Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Causes of Poor BP control Rates
 Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
IJRPC 2011, 1(3) Patel et al. ISSN: INTERNATIONAL JOURNAL OF RESEARCH IN PHARMACY AND CHEMISTRY
 Patel et al. ISSN: INTERNATIONAL JOURNAL OF RESEARCH IN PHARMACY AND CHEMISTRY") INTERNATIONAL JOURNAL OF RESEARCH IN PHARMACY AND CHEMISTRY Available online at www.ijrpc.com Research Article EVALUATION OF COMPLIANCE AND BLOOD PRESSURE REDUCTION IN PATIENTS TREATED WITH AMLODIPINE
INTERNATIONAL JOURNAL OF RESEARCH IN PHARMACY AND CHEMISTRY Available online at www.ijrpc.com Research Article EVALUATION OF COMPLIANCE AND BLOOD PRESSURE REDUCTION IN PATIENTS TREATED WITH AMLODIPINE
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
HYPERTENSION IN THE ELDERLY A BALANCED APPROACH. Barry Goldlist October 31, 2014
 HYPERTENSION IN THE ELDERLY A BALANCED APPROACH Barry Goldlist October 31, 2014 DISCLOSURE I have not accepted any money for myself from any pharmaceutical company in the 21 st century I have accepted
HYPERTENSION IN THE ELDERLY A BALANCED APPROACH Barry Goldlist October 31, 2014 DISCLOSURE I have not accepted any money for myself from any pharmaceutical company in the 21 st century I have accepted
REDUCING COSTS AND IMPROVING HYPERTENSION MANAGEMENT
 REDUCING COSTS AND IMPROVING HYPERTENSION MANAGEMENT Vida Stankus 1, Brenda Hemmelgarn 2, Norm RC Campbell 2, Guanmin Chen 2, Finlay A McAlister 1, Ross T Tsuyuki 1 1 EPICORE Centre, Department of Medicine,
REDUCING COSTS AND IMPROVING HYPERTENSION MANAGEMENT Vida Stankus 1, Brenda Hemmelgarn 2, Norm RC Campbell 2, Guanmin Chen 2, Finlay A McAlister 1, Ross T Tsuyuki 1 1 EPICORE Centre, Department of Medicine,
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
High blood pressure (BP) significantly. After the Diagnosis: Adherence and Persistence With Hypertension Therapy REPORTS
 significantly. After the Diagnosis: Adherence and Persistence With Hypertension Therapy REPORTS") After the Diagnosis: Adherence and Persistence With Hypertension Therapy Abstract Poor adherence to therapy is a major reason that a large percentage of patients with hypertension fail to achieve good
After the Diagnosis: Adherence and Persistence With Hypertension Therapy Abstract Poor adherence to therapy is a major reason that a large percentage of patients with hypertension fail to achieve good
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Selecting an ACE inhibitor:
 Selecting an ACE inhibitor: A Question of Class Effect? All members of a drug class are not therapeutically equivalent. In recent years, the concept of class effect has been under considerable debate,
Selecting an ACE inhibitor: A Question of Class Effect? All members of a drug class are not therapeutically equivalent. In recent years, the concept of class effect has been under considerable debate,
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
ABSTRACT KEYWORDS: The prevalence of hypertension varies from percentages in all
 85 P a g e International Standard Serial Number (ISSN): 2319-8141 International Journal of Universal Pharmacy and Bio Sciences 6(6): November-December 2017 INTERNATIONAL JOURNAL OF UNIVERSAL PHARMACY AND
85 P a g e International Standard Serial Number (ISSN): 2319-8141 International Journal of Universal Pharmacy and Bio Sciences 6(6): November-December 2017 INTERNATIONAL JOURNAL OF UNIVERSAL PHARMACY AND
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
The problem of uncontrolled hypertension
 (2002) 16, S3 S8 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh The problem of uncontrolled hypertension Department of Public Health and Clinical Medicine, Norrlands
(2002) 16, S3 S8 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh The problem of uncontrolled hypertension Department of Public Health and Clinical Medicine, Norrlands
High-dose monotherapy vs low-dose combination therapy of calcium channel blockers and angiotensin receptor blockers in mild to moderate hypertension
 (2005) 19, 491 496 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE High-dose monotherapy vs low-dose combination therapy of calcium channel blockers
(2005) 19, 491 496 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE High-dose monotherapy vs low-dose combination therapy of calcium channel blockers
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Patient persistence with antihypertensive drugs in France, Germany and the UK
 Patient persistence with antihypertensive drugs in France, Germany and the UK B. Ehlken (1), K. Kostev (1), A. Sandberg (2), B. Holz (1), A. M. S. Oberdiek (2) (1) IMS Health Frankfurt / Munich, Germany
Patient persistence with antihypertensive drugs in France, Germany and the UK B. Ehlken (1), K. Kostev (1), A. Sandberg (2), B. Holz (1), A. M. S. Oberdiek (2) (1) IMS Health Frankfurt / Munich, Germany
Adapted d from Federation of Health Regulatory Colleges of Ontario Template Last Updated September 18, 2017
 Insert Logo or Org Name Here Primary Care Medical Directive for Hypertension Management Adapted d from Federation of Health Regulatory Colleges of Ontario Template Last Updated September 18, 2017 Title:
Insert Logo or Org Name Here Primary Care Medical Directive for Hypertension Management Adapted d from Federation of Health Regulatory Colleges of Ontario Template Last Updated September 18, 2017 Title:
Value of cardiac rehabilitation Prof. Dr. L Vanhees
 Session: At the interface of hypertension and coronary heart disease haemodynamics, heart and hypertension Value of cardiac rehabilitation Prof. Dr. L Vanhees ESC Stockholm August 2010 Introduction There
Session: At the interface of hypertension and coronary heart disease haemodynamics, heart and hypertension Value of cardiac rehabilitation Prof. Dr. L Vanhees ESC Stockholm August 2010 Introduction There
The impact of fixed- dose combination versus free- equivalent combination therapies on adherence for hypertension: A meta- analysis
 Received: 11 December 2017 Revised: 1 February 2018 Accepted: 13 February 2018 DOI: 10.1111/jch.13272 ORIGINAL PAPER The impact of fixed- dose combination versus free- equivalent combination therapies
Received: 11 December 2017 Revised: 1 February 2018 Accepted: 13 February 2018 DOI: 10.1111/jch.13272 ORIGINAL PAPER The impact of fixed- dose combination versus free- equivalent combination therapies
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Drug-Induced Diabetes May Not Be Harmful But Should Be Prevented. Jeffrey A. Cutler, MD, MPH
 Drug-Induced Diabetes May Not Be Harmful But Should Be Prevented Jeffrey A. Cutler, MD, MPH Overview Focus on thiazide-like diuretics (not BB) Diuretic-induced versus diureticassociated diabetes Role of
Drug-Induced Diabetes May Not Be Harmful But Should Be Prevented Jeffrey A. Cutler, MD, MPH Overview Focus on thiazide-like diuretics (not BB) Diuretic-induced versus diureticassociated diabetes Role of
International Journal of Advancements in Research & Technology, Volume 2, Issue 6, June-2013 ISSN
 ISSN 2278-7763 295 Study of Prescriptive Patterns of Antihypertensive Drugs in South India Popuri Rupa Sindhu, Malladi Srinivas Reddy St. Peters Institute of Pharmaceutical Sciences, Hanamkonda, Warangal-506001,
ISSN 2278-7763 295 Study of Prescriptive Patterns of Antihypertensive Drugs in South India Popuri Rupa Sindhu, Malladi Srinivas Reddy St. Peters Institute of Pharmaceutical Sciences, Hanamkonda, Warangal-506001,
Volume 2 Number 2 (2011)
") Review of Global Medicine and Healthcare Research Volume 2 Number 2 (211) Publisher: DRUNPP Managed by: IOMC Group Website: www.iomcworld.com/rgmhr/ Drug Utilization Pattern and Co-morbidtities Among Hypertensive
Review of Global Medicine and Healthcare Research Volume 2 Number 2 (211) Publisher: DRUNPP Managed by: IOMC Group Website: www.iomcworld.com/rgmhr/ Drug Utilization Pattern and Co-morbidtities Among Hypertensive
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded