Risk factor modification Blood pressure/cholesterol etc. James McCormack, B.Sc. (Pharm), Pharm.D. Professor Faculty of Pharmaceutical Sciences
|
|
|
- Franklin Lamb
- 5 years ago
- Views:
Transcription
1 Risk factor modification Blood pressure/cholesterol etc James McCormack, B.Sc. (Pharm), Pharm.D. Professor Faculty of Pharmaceutical Sciences
2 What Will You Do? You are approximately 45 y/o You have been diagnosed properly with elevated blood pressure You have tried non-drug measures for 6 months and still your blood pressure remains elevated QUESTION ABOVE What Blood Pressure Would YOU Take A Drug Every Day For The Next 5 Years? What drug and dose would you start with?
3 Objectives To be able to design an effective, safe and cost-effective therapeutic plan for the treatment of patients with high blood pressure/cholesterol
4 Non-drug measures Activity Nutrition Lose weight Smoking? Salt? Potassium
5 High Blood Pressure Measurement must be determined under relaxed conditions and should be done on at least 3 separate occasions (3 sets of 3 readings with an interval of at least 2 weeks between readings unless the initial level is very high >120 mmhg or target organ damage is present) patient should sit or lie down quietly for at least five minutes before blood pressure measurement avoid smoking or eating within the 30 minutes prior to measurement
6 Drug-Induced Prescription Drugs: NSAIDs, including coxibs Corticosteroids and anabolic steroids Oral contraceptive and sex hormones Vasoconstricting/sympathomimetic decongestants Calcineurin inhibitors (cyclosporin, tacrolimus) Erythropoietin and analogues Monoamine oxidase inhibitors (MAOIs) Midodrine Other substances: Licorice root. Stimulants including cocaine, Salt, Excessive alcohol use From CHEP 2006



7 Smoking and risk IHD All Cancer Overall mortality Bandolier
8 BMI and risk Cardiovascular mortality in patients with CAD Total mortality for all groups Lancet 2006;368:666 78
9 BMI and risk Age All-cause mortality J Am Geriatr Soc 2010;58:234 41
10 Quality of life comparisons QOL utilities Mild stroke 0.70 Angina 0.64 Diabetic neuropathy 0.66 Comprehensive diabetes care 0.64 Diabetes Care 2007;30:
11 Patient values and risk assessment As in previous years, it needs to be reiterated that the CHEP hypertension management recommendations are based solely on efficacy data. Considerations relating to individual patient/ physician preferences and cost-effectiveness of different drug classes have not been a component of this process and need to be considered by the physician and patient when individualizing therapy
12 Describing Benefits The chance WITH NO TREATMENT The chance WITH TREATMENT
13 Risk of what and over how long Definitions WHAT CVD is cardiovascular disease Typically = CHD + cerebrovascular CHD = coronary heart disease = fatal and non-fatal MIs and sometimes angina Cerebrovascular disease = fatal and non-fatal strokes - and sometimes TIAs CVD sometimes includes other conditions - heart failure, peripheral vascular disease HOW LONG - 5 or 10 years

14 How accurately can we predict risk? CIs +/- 5% 0% 5% 10% 15% 20% 25% 30% Low Intermediate High J Cardiovasc Risk 2002;9:183-90
15
16
17
18 How good is the Framingham risk estimate? UK - overestimates mortality from CHD by 47% and non-fatal CHD by 57% Germany, Italy, and Denmark - overestimates risk by 50% BMJ 2003;327:1-6

19 Lancet 2008;371: National Health and Nutrition Examination Survey (NHANES) prospective cohort study of 14,407 US participants non-laboratory-based risk factors predicted cardiovascular events as accurately as one that relied on laboratorybased values

20 What do you REALLY need to know to make a reasonable estimate of CVD risk???? Eur J Card Prev Rehab May 2009 Similar findings Age gender SBP Smoker Diabetes Obese - just look!! CHOLESTEROL OR CRP really not needed
21 55 year-old male non-smoker, Chol 5, HDL 1.25 JNC 6 JNC 7 Systolic 10 year risk (%) Non diabetic Diabetic mm Hg CHD Stroke CHD Stroke Optimal Normal Normal Prehtn Borderline Prehtn Stage 1 Stage Stage 1 Stage Stage 2 Stage Stage 2 Stage
22 AGE SBP WOMEN MEN A) normal BMI B) overweight BMI C) obese BMI - >30 A B C 5-year CVD 1 risk (%) 2 > <5% Smoking or diabetes approx. doubles the risk 1.CVD = death, MI, stroke, CHF, and coronary revascularisation including CABG and PTCA 2.1/2-2/3 are hard endpoints - fatal/nonfatal MI or stroke A B C Lancet 2008;371:923 31
23 Factors to consider when choosing a drug 1.Efficacy at lowering risk of cardiovascular disease 2.Tolerability/allergies 3.Frequency of dosing 4. 2-fers - for blood pressure 5.Cost
24 Efficacy at lowering blood pressure all high blood pressure drugs presently available are equally effective at lowering blood pressure there is important variability between patients and not every drug will necessarily work in every patient
25 Lipid-lowering drugs
26
27
28 Evidence for CVD benefit - typically over 5 years BASELINE (%) Mortality Thiazide 0.89 Total stroke Total CHD Total CVD Withdrawal due to adverse effects (0.83,0.96) 0.63 (0.57,0.71) 0.84 (0.75,0.95) 0.70 (0.66,0.76) 3.22 (2.90,3.57) BB 0.96 (0.86,1.07) 0.83 ( ) 0.90 (0.78,1.03) 0.89 (0.81,0.98) 4.59 (4.11,5.13) CCB (0.68,1.09) (0.41,0.84) (0.55,1.09) (0.57,0.87) BASELINE (%) NR ACEI 0.83 (0.72,0.95) 0.65 (0.52,0.82) 0.81 (0.70,0.94) 0.76 (0.67,0.85)
29 Treatment of Hypertension in the Elderly typically over 5 years years for the over 80 Mortality CV mortality and morbidity Withdrawal due to adverse effects BASELINE (%) years or older 0.9 (0.84,0.97) 0.72 (0.68,0.77) 1.71 (1.45,2.00) BASELINE (%) NR 80 years or older 0.98 (0.87,1.10) 0.75 (0.65,0.87) Cochrane Library
30 Objective: To determine if lower BP targets ( 135/85 mmhg) are associated with reduction in mortality and morbidity as compared with standard BP targets ( / mmhg) Arguedas JA, Perez MI, Wright JM. Treatment blood pressure targets for hypertension. Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No.: CD DOI: / CD pub2.
31 7 RCTs, N=22,089 Despite a -4/-3 mmhg greater achieved reduction in systolic/diastolic BP, p< 0.001, attempting to achieve lower targets instead of standard targets did not change total mortality (RR 0.92, 95% CI ) myocardial infarction (RR 0.90, 95% CI ) stroke (RR 0.99, 95% CI ) heart failure (RR 0.88, 95% CI ) major cardiovascular events(rr 0.94, 95% CI ) end-stage renal disease (RR 1.01, 95% CI ) Arguedas JA, Perez MI, Wright JM. Treatment blood pressure targets for hypertension. Cochrane Database of Systematic Reviews 2009, Issue 3. Art. No.: CD DOI: / CD pub2.
 have not been shown to reduce mortality or morbidity in RCTs Treatment caused 9% of patients to discontinue treatment due to adverse effects.")
32 Antihypertensive drugs used in the treatment of adults (primary prevention) with mild hypertension (systolic BP mmhg and/or diastolic BP mmhg) have not been shown to reduce mortality or morbidity in RCTs Treatment caused 9% of patients to discontinue treatment due to adverse effects. August 2012
33 ALLHAT - high-risk hypertensive patients randomized to ACE inhibitor or calcium channel blocker vs. diuretic Patients 33,357 patients with hypertension and 1 or more risk factors - mean age 67, 47% women, diabetics (36%), history of heart disease (25%), smoker (22%), HDL < 0.9 mmol/l (12%) Treatment chlorthalidone, amlodipine or lisinopril 2nd line therapy allowed was atenolol, clonidine or reserpine Duration 4.9 years Results Blood pressure differences at 5 years compared with chlorthalidone group Systolic amlodipine 0.8 mmhg higher, lisinopril 2.0 mmhg higher Diastolic amlodipine 0.8 mmhg lower, lisinopril no difference JAMA 2002;288:
34 Fatal CHD or non-fatal MI (%) Mortality (%) Combined CHD (%) Stroke (%) Combined CVD (%) Chlorthalidone Amlodipine Lisinopril Relative risk reduction Absolute risk reduction 6 year data NSS 11* 7* NNT * p <0.05 lisinopril vs. chlorthalidone JAMA 2002;288:
35 ESRD (%) Cancer (%) CHF (%) Angina (%) Coronary Revasc (%) PVD (%) Chlorthalidone Amlodipine Lisinopril Relative risk reduction Absolute risk reduction 6 year data NSS 25** 11* NSS NNT NSS *** # p <0.05 lisinopril vs. chlorthalidone ** p <0.05 lisinopril vs. amlodipine *** p = 0.05 lisinopril vs. chlorthalidone, p = 0.06 amlodipine vs. chlorthalidone # p = 0.06 amlodipine vs. chlorthalidone JAMA 2002;288:
36 Meta-analysis of 4 HTN trials 6,825 patients - atenolol versus placebo/no treatment All deaths (%) CVD death (%) MIs (%) Atenolol Placebo Strokes (%) RR ARR NNT NSS Lancet 2004;364:1684 9
37 Meta-analysis of 5 HTN trials 17,671 patients - atenolol versus other agents (thiazides,acei CCB) All deaths (%) CVD death (%) MIs (%) Atenolol Other RR NSS 15 ARR NNT Strokes (%) Lancet 2004;364:1684 9

38 13 beta-blocker vs other anti-htn trials 105,951 patients No difference for MI or mortality, 16% more strokes in BB group 7 beta-blocker versus placebo or no treatment trials 27,433 patients No reduction for MI or mortality, 19% decrease in stroke (approx 0.2% ARR?) No change in any endpoint in either the atenolol or nonatenolol sub-group Lancet Oct
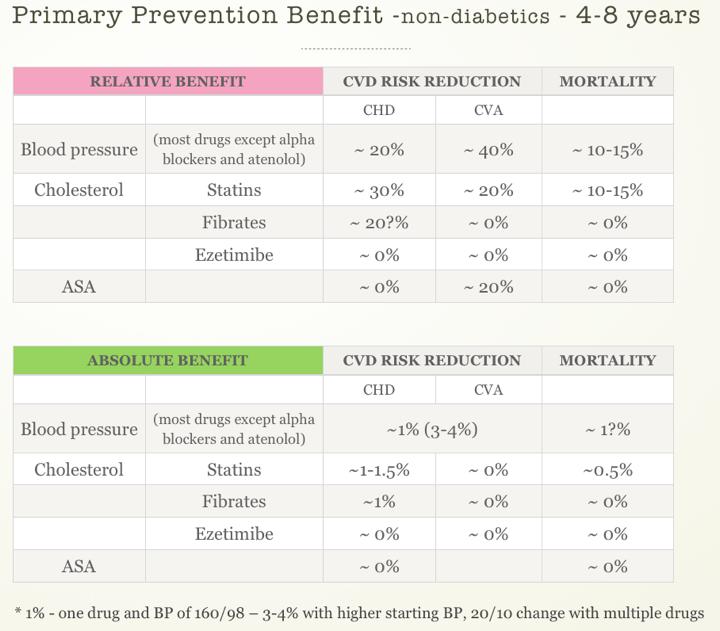
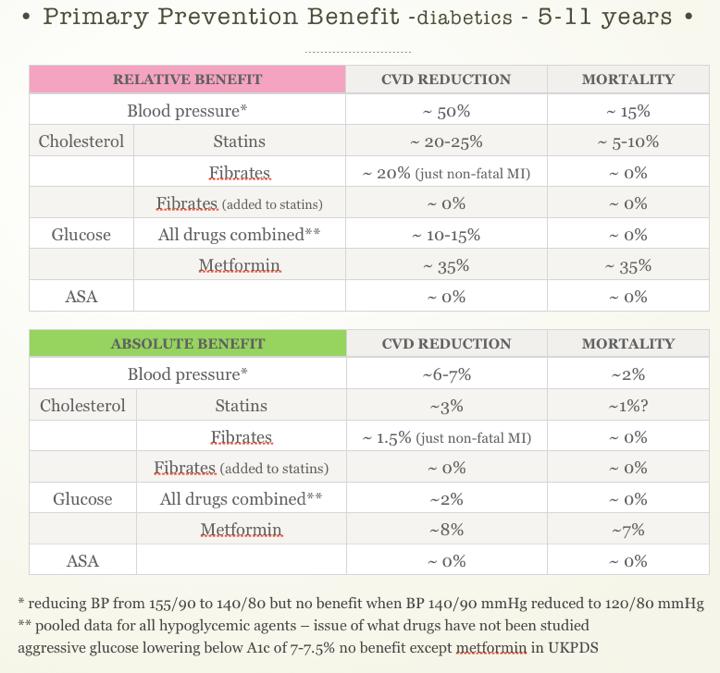
39 CHOLESTEROL There are NO studies that have looked at getting patients to different cholesterol levels BLOOD PRESSURE Less than 135/85 Despite a -4/-3 mmhg greater achieved reduction in systolic/diastolic BP, attempting to achieve lower targets instead of standard targets did not change total mortality, MI, stroke, CHF, major CV events or ESRD DIABETES three end points - Overall CHD - Strokes, Overall Mortality 5 years - lower HbA1c by 1% - compared to "standard" treatment CHD - they state there was a 1.5% in CHD one table from Strokes - NSS, Mortality - NSS Hypoglycemic events Levels and break points Cochrane Review 2009;Issue 3:CD from 28.6% to 38.1% - Severe -1.2% to 2.3% Participants gained 2.5 kg more in the intensive group Lancet 2009;373:

40 After initial change only measure every 3-5 years Ann Intern Med 2008;148: Need changes of at least 10/5 mmhg before you can say there has been a change Am J Hyper 2008;21:3 4
41 After initial change only measure every 3-5 years Average increase in chol is 0.5-1%/year Within-person coefficient of variation is ~7% Single measurement 95% CI Total chol ~ to 0.80 mmol/l LDL chol ~ -0.5 to 0.5 mmol/l Ann Intern Med 2008;148:656-61
42 60 % reduction in LDL cholesterol mg 20mg 40mg 80mg 0 Rosuvastatin Atorvastatin Simvastatin Pravastatin % reduction in LDL cholesterol Ezetimibe 0 mg 0.25mg 1mg 5mg 10mg
\" Statins in secondary prevention 10-20 mg - 5-6% ARR in MIs and strokes Inc.")
43 LDL cholesterol mmol/l 4.5" 4" 3.5" 3" 2.5" 2" 1.5" 1" 0.5" 0" 95% CI ~ +/ " 2.8" A r b i t r a y t h r e s h o l d Baseline"LDL" 33%"dec"(10720mg)" 2.5" Add"10%"dec"(40780mg)" Statins in secondary prevention mg - 5-6% ARR in MIs and strokes Inc. dose 4-8X you get an additional 1-2% ARR short- term variability - a combination of analytic variability and week- to- week biological fluctuation around a stable aver- age
44 Tolerability almost all high blood pressure medications produce a similar incidence of side effects and are equally well tolerated however, the types of side effects are different
45 Examples of 2-fers Ischemic heart disease (BB, CCB) Previous MI (BB, ACEI) CHF (DIUR, ACEI, BB, A2B) COPD and asthma (avoid BB for asthma) Type-2 diabetes (ACEI?, ARB? avoid CCB?) Type-1 diabetes (ACEI?) Hyperlipidemia (avoid anything that would worsen lipids enough to require drug therapy) Atrial fibrillation (BB, CB) Migraine (BB, ACEI?) Remember issue of betablockers

46 Key point Start with a LOW!!!!!! dose
47 Thiazides TOXICITY (thiazides) Hypokalemia Gout Hypomagnesemia Hypercalcemia Hyperlipidemia Blood dyscrasias Photosensitivity Gynecomastia (spironolactone)
48 Betablockers acebutolol (Sectral, Monitan) atenolol (Tenormin, generics) bisoprolol (Monocor) carvedilol (Coreg) nadolol (Corgard, generics) metoprolol (Lopressor, Betaloc, generics) oxprenolol (Trasicor, Slow-Trasicor) propranolol (Inderal, Inderal LA, generics) sotalol (Sotacor) pindolol (Visken, generics)
49 Betablockers CONTRAINDICATIONS Asthma or chronic bronchitis with bronchospasm Raynauds Intermittent claudication? Bradycardia, atrio-ventricular conduction defects TOXICITY Fatigue Bradycardia Asthma CNS effects Cold extremities
50 ACE Inhibitors benazepril (Lotensin) captopril (Capoten, generics) cilazapril (Inhibace) enalapril (Vasotec, generics) fosinopril (Monopril) lisinopril (Prinivil, Zestril, generics) quinapril (Accupril) ramipril (Altace) trandolapril (Mavik)
51 Thiazides hydrochlorothiazide (HCTZ, Hydrodiuril, generics) chlorthalidone (Hygroton, generics) indapamide (Lozide) amiloride/hctz (Moduret, generics) spironolactone/hctz(aldactazide, generics) triamterene/hctz(dyazide, generics)
52 ACE Inhibitors CONTRAINDICATIONS Intolerance or allergic reaction to ACE inhibitors Pregnancy Rapidly worsening renal failure Severe hypotension Bilateral renal artery stenosis, unilateral renal artery stenosis in a patient with one kidney TOXICITY Acute renal failure - esp if volume depleted Hyperkalemia Hypotension Dry cough Rash, mucosal ulcerations Angioedema
53 Angiotensin II receptor antagonists losartan (Cozaar) candesartan (Atacand) irbesartan (Avapro) telmisartan (Micardis) valsartan (Diovan)
54 Angiotensin II receptor antagonists CONTRAINDICATIONS Intolerance or allergic reaction to ARBs Pregnancy Rapidly worsening renal failure Severe hypotension Bilateral renal artery stenosis, unilateral renal artery stenosis in a patient with one kidney TOXICITY Acute renal failure - esp if volume depleted Hyperkalemia Hypotension Angioedema - reported??/
55 Calcium channel blockers amlodipine (Norvasc) diltiazem (Cardizem SR, Cardizem CD, generics) felodipine SR (Plendil, Renedil) nicardipine (Cardene) nifedipine (Adalat, Adalat PA, Adalat XL, generics) verapamil (Isoptin, Isoptin SR, generics)
56 Calcium channel blockers CONTRAINDICATIONS Severe left ventricular dysfunction (EF< 20-30%) Second- or third-degree AV block or sick sinus syndrome (unless a functioning ventricular pacemaker is in place) Wolff-Parkinson-White syndrome Wide-complex ventricular tachycardia TOXICITY Hypotension Headache Bradycardia (verapamil) Dizziness or lightheadedness Exacerbation of congestive heart failure (verapamil) Constipation Peripheral edema Heart burn
57 Alpha blockers prazosin (Minipress, generics) doxazosin (Cardura, generics) terazosin (Hytrin, generics)
58 Centrally acting agents clonidine (Catapres, generics) methyldopa (Aldomet, generics) reserpine (Serpasil)
59 When to stop Stepped-down therapy should be considered in patients whose blood pressures during the previous few visits have been well controlled approximately 50% of patients with wellcontrolled blood pressures successfully undergo either a reduction in dosage or number of drugs and remain normotensive for a time
60 How to stop very gradual dosage and drug discontinuation a precise discussion of why drug reduction is being done dosage should be reduced by 50%, with reassessment of blood pressure at 2 weeks if the patient is still normotensive, reduce the dosage by another 50% (i.e., to 25% of the initial dose) and recheck the blood pressure in another 2 weeks
61 Resins cholestyramine colestipol (Colestid) Lipid-lowering drugs Cholesterol Absorption Inhibitor ezetimibe (Ezetrol) HMG CoA Reductase Inhibitors atorvastatin fluvastatin (Lescol) lovastatin (Mevacor, generics) pravastatin (Pravachol, generics) rosuvastatin (Crestor) simvastatin (Zocor, generics)
62 Lipid-lowering drugs Niacin (Nicotinic Acid) derivatives niacin, immediate release niacin, slow release (SR) niacin, extended release (ER) Fibrates bezafibrate (Bezalip) fenofibrate (Generics) fenofibrate microcoated (Lipidil Supra, generic) fenofibrate micronized (Lipidil Micro, generics) fenofibrate nanocrystals (Lipidil EZ, generics) gemfibrozil (Lopid, generics)
63 Lipid-lowering drugs Resins Common: Constipation (>10%), bloating, abdominal fullness, flatulence, triglycerides, transaminases (reversible). Rare: hyperchloremic acidosis, cholecystitis, cholelithiasis, pancreatitis, malabsorption syndrome, GI bleeding, peptic ulceration. Cholesterol Absorption Inhibitor Common: back pain, arthralgia, diarrhea, abdominal pain, fatigue, dizziness, headache. Rare: myopathy, rhabdomyolysis, hepatitis, acute pancreatitis, thrombocytopenia. HMG CoA Reductase Inhibitors Common: CPK, transaminases (reversible), mild upper GI disturbances, myalgias (with and without CPK elevation), sleep disturbances, headache, rash.
64 Lipid-lowering drugs Niacin (Nicotinic Acid) derivatives Common: hot flushes and pruritus, dry skin, acanthosis nigricans (reversible), reactivation of peptic ulcer, GI disturbances, blood glucose, glucose intolerance, uric acid and transaminases. Rare: torsades de pointes, severe hepatotoxicity (more frequent with slowrelease formulation), blood glucose, uric acid, transaminases. Fibrates Upper GI disturbances (nausea, abdominal pain, flatulence), myalgias, bile lithogenicity, CK, creatinine (not representative of renal function deterioration).
Information in these slides is used with permission from St. Mary s Cardiac Rehab
 Information in these slides is used with permission from St. Mary s Cardiac Rehab Prescription Pointers Heart Medications Questions!! 2-4% of patients who visit ER s have experienced a medication misadventure
Information in these slides is used with permission from St. Mary s Cardiac Rehab Prescription Pointers Heart Medications Questions!! 2-4% of patients who visit ER s have experienced a medication misadventure
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Adapted d from Federation of Health Regulatory Colleges of Ontario Template Last Updated September 18, 2017
 Insert Logo or Org Name Here Primary Care Medical Directive for Hypertension Management Adapted d from Federation of Health Regulatory Colleges of Ontario Template Last Updated September 18, 2017 Title:
Insert Logo or Org Name Here Primary Care Medical Directive for Hypertension Management Adapted d from Federation of Health Regulatory Colleges of Ontario Template Last Updated September 18, 2017 Title:
PassAssured's Pharmacy Technician Training Systems. Medication Review. Cardiovascular Drugs. Pharmacy Technician Training Systems Passassured, LLC
 Medication Review Cardiovascular Drugs Pharmacy Technician Training Systems Passassured, LLC p1 Medication Review, Cardiovascular Drugs Click Here for Glossary Index! Click Here to Print Topic Help File
Medication Review Cardiovascular Drugs Pharmacy Technician Training Systems Passassured, LLC p1 Medication Review, Cardiovascular Drugs Click Here for Glossary Index! Click Here to Print Topic Help File
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Cardiac Medications At A Glance
 Cardiac Medications At A Glance 1) Anticoagulants (Also known as Blood Thinners.) Dalteparin (Fragmin), Danaparoid (Orgaran) Enoxaparin (Lovenox) Heparin (various) Tinzaparin (Innohep) Warfarin (Coumadin)
Cardiac Medications At A Glance 1) Anticoagulants (Also known as Blood Thinners.) Dalteparin (Fragmin), Danaparoid (Orgaran) Enoxaparin (Lovenox) Heparin (various) Tinzaparin (Innohep) Warfarin (Coumadin)
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Cardiovascular Risk Reduction in Diabetic Mellitus. Presenter: Dr. Martin N. Wanyoike MB.CHB., M. Med.(internal med) Physician / Cardiologist
 Physician / Cardiologist") Cardiovascular Risk Reduction in Diabetic Mellitus Presenter: Dr. Martin N. Wanyoike MB.CHB., M. Med.(internal med) Physician / Cardiologist Cardiovascular Risk Reduction in Diabetic Mellitus Disclosures
Cardiovascular Risk Reduction in Diabetic Mellitus Presenter: Dr. Martin N. Wanyoike MB.CHB., M. Med.(internal med) Physician / Cardiologist Cardiovascular Risk Reduction in Diabetic Mellitus Disclosures
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
8/19/2016. No Conflicts. I struggled with everything cardiac in nursing school.
 Cindy Weston, DNP, RN, CCRN, CNS CC, FNP BC Assistant Professor, Texas A&M Health Science Center College of Nursing Describe and define epidemiology and pathophysiology of hypertension Differentiate JNC8
Cindy Weston, DNP, RN, CCRN, CNS CC, FNP BC Assistant Professor, Texas A&M Health Science Center College of Nursing Describe and define epidemiology and pathophysiology of hypertension Differentiate JNC8
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Hypertension, Hyperlipidemia and Obesity. Mi-CCSI
 Hypertension, Hyperlipidemia and Obesity Mi-CCSI Objectives Review the prevalence of hypertension, hyperlipidemia and obesity Correlation of the 3 conditions Discuss why it is important to treat these
Hypertension, Hyperlipidemia and Obesity Mi-CCSI Objectives Review the prevalence of hypertension, hyperlipidemia and obesity Correlation of the 3 conditions Discuss why it is important to treat these
Medications for Type 2 Diabetes CDE Exam Preparation. Wendy Graham, RD, CDE Mentor, WWD Angela Puim, RPh, CDE, CRE Preston Medical Pharmacy
 Medications for Type 2 Diabetes CDE Exam Preparation Wendy Graham, RD, CDE Mentor, WWD Angela Puim, RPh, CDE, CRE Preston Medical Pharmacy Competency for CDE Exam 3.1.A Oral Medications for Type 2 Diabetes
Medications for Type 2 Diabetes CDE Exam Preparation Wendy Graham, RD, CDE Mentor, WWD Angela Puim, RPh, CDE, CRE Preston Medical Pharmacy Competency for CDE Exam 3.1.A Oral Medications for Type 2 Diabetes
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
LESSON ASSIGNMENT. After completing this lesson you will be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
12.5mg, 25mg, 50mg. 25mg, 50mg. 2.5mg, 5mg, 10mg. 5mg, 10mg, 20mg, 100mg. 25mg. -- $2.81 Acetazolamide (IR, 125mg, 250mg, 500mg (ER)
") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 9/15, 2/13, 2/08, 5/07 LOB
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 9/15, 2/13, 2/08, 5/07 LOB
CARDIAC IMAGING QUESTIONNAIRE
 Date of test: / / Month day year Last name First name Middle initial Street address City State Zip code Home phone ( ) - Work phone ( ) - Cell Phone ( ) - Email: Age: Demographics: What is your ethnicity?
Date of test: / / Month day year Last name First name Middle initial Street address City State Zip code Home phone ( ) - Work phone ( ) - Cell Phone ( ) - Email: Age: Demographics: What is your ethnicity?
Top 200 Section 4. Cardiovascular Drugs
 Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
State of the art treatment of hypertension: established and new drugs. Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland
 State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Preventing and Managing High Blood Pressure
 MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Preventing and Managing High Blood Pressure About This Kit Fortunately, high blood pressure is easily detected and
MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Preventing and Managing High Blood Pressure About This Kit Fortunately, high blood pressure is easily detected and
Physician/Clinic Collaborative Practice Agreement
 Physician/Clinic Collaborative Practice Agreement Effective October 1, 2010, Connecticut Senate Bill 428 (PA 10-117) extends to all settings and medical conditions the opportunity for licensed pharmacists
Physician/Clinic Collaborative Practice Agreement Effective October 1, 2010, Connecticut Senate Bill 428 (PA 10-117) extends to all settings and medical conditions the opportunity for licensed pharmacists
12.5mg, 25mg, 50mg. 25mg, 50mg. 250mg, 500mg, 250mg/5ml. 2.5mg, 5mg, 10mg. 5mg, 10mg, 20mg, 100mg. 25mg
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 9/11/2018 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 5/17, 9/15, 2/13, 2/08, LOB
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 9/11/2018 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 5/17, 9/15, 2/13, 2/08, LOB
ACEBUTOLOL HCL 100MG TABLET GENERIC BETA BLOCKERS ALISKIREN 150MG TABLET RASILAZ RENIN INHIBITOR
 S/N ME OF MEDICATIONS BRANDED/GENERIC DRUG CLASS * UNIT PRICE RANGE (SGD$) 1 ACEBUTOLOL HCL 100MG CAPSULE SECTRAL BETA BLOCKERS 0.50 2 ACEBUTOLOL HCL 100MG TABLET GENERIC BETA BLOCKERS 0.33 3 ALISKIREN
S/N ME OF MEDICATIONS BRANDED/GENERIC DRUG CLASS * UNIT PRICE RANGE (SGD$) 1 ACEBUTOLOL HCL 100MG CAPSULE SECTRAL BETA BLOCKERS 0.50 2 ACEBUTOLOL HCL 100MG TABLET GENERIC BETA BLOCKERS 0.33 3 ALISKIREN
Value-Based Drug List for ABCs of Diabetes
 Effective January 1, 2019 Value-Based Drug List for ABCs of Diabetes PCPS provides a Value-Based Benefit Design (VBD) to qualified participants in the ABCs of Diabetes. This means you will have lower out-of-pocket
Effective January 1, 2019 Value-Based Drug List for ABCs of Diabetes PCPS provides a Value-Based Benefit Design (VBD) to qualified participants in the ABCs of Diabetes. This means you will have lower out-of-pocket
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Mi-CCSI welcomes you to the 2 nd in our 4 part Basics of Disease Management Webinar Series
 Our speaker today is: Susan Vos, BSN, RN, CCM Mi-CCSI welcomes you to the 2 nd in our 4 part Basics of Disease Management Webinar Series We will be starting shortly A few housekeeping items: We will be
Our speaker today is: Susan Vos, BSN, RN, CCM Mi-CCSI welcomes you to the 2 nd in our 4 part Basics of Disease Management Webinar Series We will be starting shortly A few housekeeping items: We will be
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Doctor discussion guide:
 Bring this printout to your next doctor s appointment. It will help you and your doctor work together to set goals for treatment, evaluate the success of your treatment, and reduce your risk of side effects.
Bring this printout to your next doctor s appointment. It will help you and your doctor work together to set goals for treatment, evaluate the success of your treatment, and reduce your risk of side effects.
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Heart Disease and Prevention PRESENTED BY: DOTTIE CRAIG NP- C, JANE ARCHER NP-C, KATHY DAPPER RN, NICCI FRAVEL RN
 Heart Disease and Prevention PRESENTED BY: DOTTIE CRAIG NP- C, JANE ARCHER NP-C, KATHY DAPPER RN, NICCI FRAVEL RN Objectives Identify Normal Systolic and Diastolic Blood pressures Recognize common Antihypertensive
Heart Disease and Prevention PRESENTED BY: DOTTIE CRAIG NP- C, JANE ARCHER NP-C, KATHY DAPPER RN, NICCI FRAVEL RN Objectives Identify Normal Systolic and Diastolic Blood pressures Recognize common Antihypertensive
Doctor discussion guide:
 Doctor discussion guide: MAnaging Cholesterol Bring this printout to your next doctor s appointment. It will help you and your doctor work together to set goals for treatment, evaluate the success of your
Doctor discussion guide: MAnaging Cholesterol Bring this printout to your next doctor s appointment. It will help you and your doctor work together to set goals for treatment, evaluate the success of your
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Annual Review of Antihypertensives - Fiscal Year 2009
 Annual Review of Antihypertensives - Fiscal Year 2009 Oklahoma HealthCare Authority April 2010 Current Prior Authorization Criteria There are 7 categories of antihypertensive medications currently included
Annual Review of Antihypertensives - Fiscal Year 2009 Oklahoma HealthCare Authority April 2010 Current Prior Authorization Criteria There are 7 categories of antihypertensive medications currently included
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
NOTES: Anemia Medical condition in which the number of red blood cells (the blood count) is reduced.
 is reduced.") Advance care planning A process in which you decide what you would like to happen to you, or not happen to you, if you become unable to make decisions about your healthcare treatment or if you are unable
Advance care planning A process in which you decide what you would like to happen to you, or not happen to you, if you become unable to make decisions about your healthcare treatment or if you are unable
Prof. Ramzy H. El Mawardy. Cairo Egypt 2009
 Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Hypertension (HTN) Lecture Note
 Lecture Note") Hypertension (HTN) Lecture Note October, 2009 Chuang-Ye Hong, MD, PhD, FACP Wan-Fang Hospital Taipei Medical University Outline Definition Epidemiology Measurement of BP Secondary cause Target organ damage
Hypertension (HTN) Lecture Note October, 2009 Chuang-Ye Hong, MD, PhD, FACP Wan-Fang Hospital Taipei Medical University Outline Definition Epidemiology Measurement of BP Secondary cause Target organ damage
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
The ADDITION Study: A study about screening for diabetes. Screening Case Report Form
 ADDITION Study, Leicester Participant Identification Label: Date: / / The ADDITION Study: A study about screening for diabetes Screening Case Report Form You will need to have the following things done
ADDITION Study, Leicester Participant Identification Label: Date: / / The ADDITION Study: A study about screening for diabetes Screening Case Report Form You will need to have the following things done
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
CHAPTER 2. Knowing YOUR MEDICATIONS. Image: istock.com/bakibg. Knowing Your Medications 23
 CHAPTER 2 Knowing YOUR MEDICATIONS Knowing Your Medications 23 Image: istock.com/bakibg MEDICATION Prescription medications help your heart get better and protect you from more harm. People who take their
CHAPTER 2 Knowing YOUR MEDICATIONS Knowing Your Medications 23 Image: istock.com/bakibg MEDICATION Prescription medications help your heart get better and protect you from more harm. People who take their
Diabetes Complications Guideline Based Screening, Management, and Referral
 Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
4/3/2014 OBJECTIVES BLOOD PRESSURE BASICS. Discuss the new blood pressure guidelines (JNC 8) and recognize the changes from JNC 7
 and recognize the changes from JNC 7") 1 OBJECTIVES Discuss the new blood pressure guidelines (JNC 8) and recognize the changes from JNC 7 Review mechanisms for the main drug classes used to treat hypertension Describe the dosing strategies
1 OBJECTIVES Discuss the new blood pressure guidelines (JNC 8) and recognize the changes from JNC 7 Review mechanisms for the main drug classes used to treat hypertension Describe the dosing strategies
Hypertension is also an important risk factor in the development of chronic kidney disease and heart failure.
 Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
ACE Inhibitors and ARBs To Protect Your Heart? A Guide for Patients Being Treated for Stable Coronary Heart Disease
 ACE Inhibitors and ARBs To Protect Your Heart? A Guide for Patients Being Treated for Stable Coronary Heart Disease Is This Guide Right for Me? This Guide Is for You If: You have coronary heart disease,
ACE Inhibitors and ARBs To Protect Your Heart? A Guide for Patients Being Treated for Stable Coronary Heart Disease Is This Guide Right for Me? This Guide Is for You If: You have coronary heart disease,
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Medications for Type 2 Diabetes CDE Exam Preparation
 Medications for Type 2 Diabetes CDE Exam Preparation Medications for Type 2 Diabetes CDE Exam Preparation Wendy Graham, RD, CDE Mentor, WWD Angela Puim, RPh, CDE, CRE Preston Medical Pharmacy Agenda Medication
Medications for Type 2 Diabetes CDE Exam Preparation Medications for Type 2 Diabetes CDE Exam Preparation Wendy Graham, RD, CDE Mentor, WWD Angela Puim, RPh, CDE, CRE Preston Medical Pharmacy Agenda Medication
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Medications and Falls Part 1
 Medications and Falls Part 1 Introduction with General Principles and Risk Evaluation for Cardiovascular Medications Dennis J Chapron Medication Safety Pharmacist Saint Francis Hospital and Medical Center
Medications and Falls Part 1 Introduction with General Principles and Risk Evaluation for Cardiovascular Medications Dennis J Chapron Medication Safety Pharmacist Saint Francis Hospital and Medical Center
Some Facts. Medications and Falls Part 1. Centers for Disease Control (CDC) Falls Statistics for Older Adults ( 65yrs) 11/27/2018
 Falls Statistics for Older Adults ( 65yrs) 11/27/2018") Medications and Falls Part 1 Introduction with General Principles and Risk Evaluation for Cardiovascular Medications Dennis J Chapron reports no real or potential conflicts of interest relevant to this
Medications and Falls Part 1 Introduction with General Principles and Risk Evaluation for Cardiovascular Medications Dennis J Chapron reports no real or potential conflicts of interest relevant to this
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Additional Standard Generics HSA Preventive Drug List Effective January 1, 2019
 Additional Standard Generics HSA Preventive Drug List Effective January 1, 2019 Employers can elect to include an additional generic HSA Preventive Drug coverage feature with your prescription benefit
Additional Standard Generics HSA Preventive Drug List Effective January 1, 2019 Employers can elect to include an additional generic HSA Preventive Drug coverage feature with your prescription benefit
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Don t let the pressure get to you:
 Balanced information for better care Don t let the pressure get to you: Current evidence-based goals for treating hypertension A cornerstone of primary care: Lowering high blood pressure prevents cardiovascular
Balanced information for better care Don t let the pressure get to you: Current evidence-based goals for treating hypertension A cornerstone of primary care: Lowering high blood pressure prevents cardiovascular
LESSON ASSIGNMENT. After you finish this lesson you should be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 3 Therapeutics III. Cardiac Drugs. LESSON ASSIGNMENT Paragraphs 3-1--3-15. OBJECTIVES After you finish this lesson you should be able to: 3-1. From a group of
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 3 Therapeutics III. Cardiac Drugs. LESSON ASSIGNMENT Paragraphs 3-1--3-15. OBJECTIVES After you finish this lesson you should be able to: 3-1. From a group of
Beta-blockers. Atenolol. Propranolol. Bisoprolol. Metoprolol. Labetalol. Carvedilol.
 Drugs of CVS Beta-blockers Atenolol. Propranolol. Bisoprolol. Metoprolol. Labetalol. Carvedilol. Atenolol.cardioselective Propranolol, nonselective Bisoprolol, cardioselective Metoprolol Carvedilol, alpha
Drugs of CVS Beta-blockers Atenolol. Propranolol. Bisoprolol. Metoprolol. Labetalol. Carvedilol. Atenolol.cardioselective Propranolol, nonselective Bisoprolol, cardioselective Metoprolol Carvedilol, alpha
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in