How to Diagnose Heart Failure
|
|
|
- Muriel Garrett
- 5 years ago
- Views:
Transcription

1 How to Diagnose Heart Failure Patrick J Gallagher 12 th November 2014
2 Sudden Cardiac Death Davies Criteria 1. Acute coronary event ± infarction 2. Coronary narrowing + healed infarction 3. Coronary narrowing but no infarction 4. Heart failure (without coronary narrowing) 5. Structurally normal heart
3 History and Epidemiology Descriptions of heart failure from ancient Egypt, Greece and India The Romans may have used foxglove (digitalis). William Withering saw the benefical effects in 1785 Blood letting was a popular treatment for many symptoms during the 18 th and 19 th Centuries


4
5

6 Edward Jenner Museum
7 History and Epidemiology Cardiac failure is increasing in prevalence and is one of the most important serious illnesses in practice Prevalence is between 3 and 20 per 1000 population. An important cause of death in many 3 rd world countries Median survival is less than 3 years, much worse than cancer of the large bowel or breast
8 Cardiac Failure in Different Population Groups Coronary heart disease and hypertension are the leading causes in the West Hypertension is an important cause of cardiac failure in Afro-Caribbeans A combination of coronary heart disease and diabetes is important in Asians Valve disease is especially important in India and parts of Central Africa
9
10 Pathophysiology of Heart Faiure Heart failure is a multisystem disorder characterised by abnormalities in cardiac and skeletal muscle and renal function. There is stimulation of the sympathetic nervous system, activation of the renin-angiotensinaldosterone system and other neurohormonal changes
11 Pathophysiological Changes Baroreceptors sense arterial underfilling Activation of the renin-angiotensinaldosterone system stimulates vasoconstriction and sodium retention. Blood volume increases by up to 25% Aldosterone causes endothelial and LV dysfunction and ventricular fibrosis Sympathetic stimulation increases heart rate and causes further
12 Pathophysiological Changes Anti-diuretic hormone (ADH) concentrations are increased. ADH causes further sodium and water retention by counteracting the normal waterproofing of the distal tubule. Hyponatraemia. Atrial stretch causes increased secretion of natriuetic peptide hormones (ANP and BNP). These promote sodium secretion. Broken down by endopeptidases, such as naprilysin
13 Why is it so difficult to diagnose Heart Failure at Autopsy Details of signs, symptoms, medications and lab results may not be in the GP fax BNP estimations, CXR/CT and ECHO reports may not be available In treated patients the pathological changes may not be present It is difficult to accept that sudden death is a feature of early disease
14 Arrhythmias and Sudden Death in Heart Failure Patients with heart failure commonly die suddenly Generally the worse the symptoms and the lower the EF the greater the risk of SD 15% annual incidence SD with EF 9-20%, 6% with EF 31-40% AF is commoner in older patients, they have lower EFs and higher risk of SD Cleland et al Heart Failure Reviews 7;2002:299
15 Cardiac failure at Autopsy Pulmonary Oedema Mechanism of agonal pulmonary oedema is unknown A study of nearly 1000 cardiac deaths showed no relation between cause of cardiac death and lung weight Head injury and drug overdoses are causes of pulmonary oedema Chronic uraemia is rare in our PM population
16 Cardiac Failure at Autopsy Effusions and Oedema Bilateral pleural effusions provide strong evidence of chronic heart failure Are also seen in combination with ascites in liver failure Assess lower limb oedema carefully, sensitive not specific for HF Look for venous disease, estimate the degree of induration, look for venous ulceration

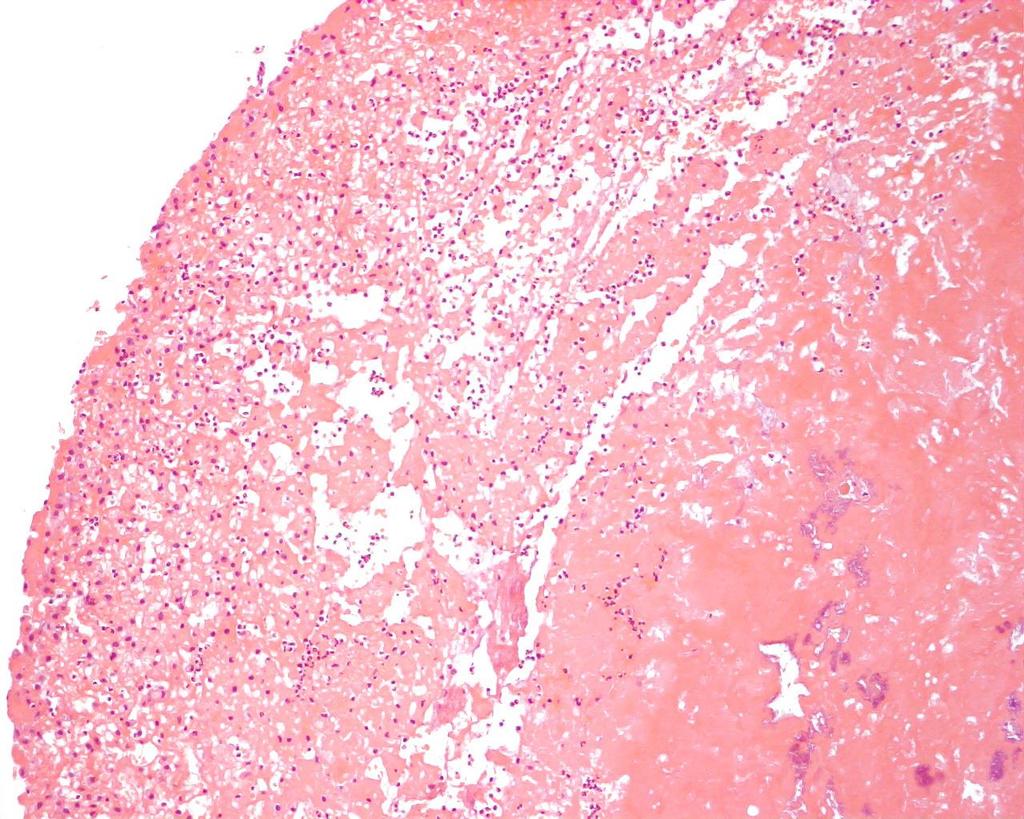
17 Careful Grading of Hepatic Congestion is Important
18
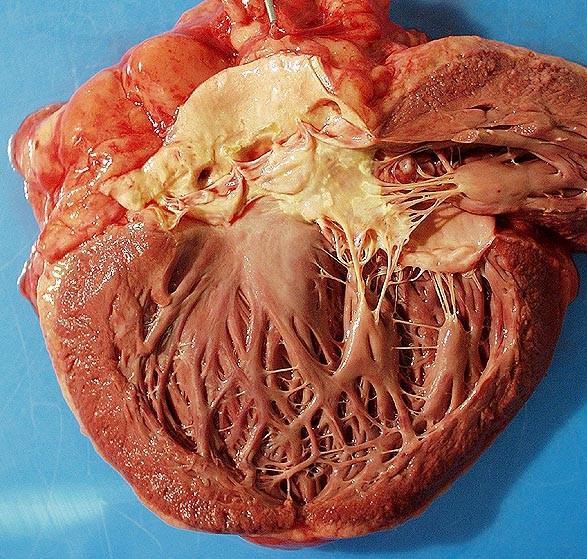
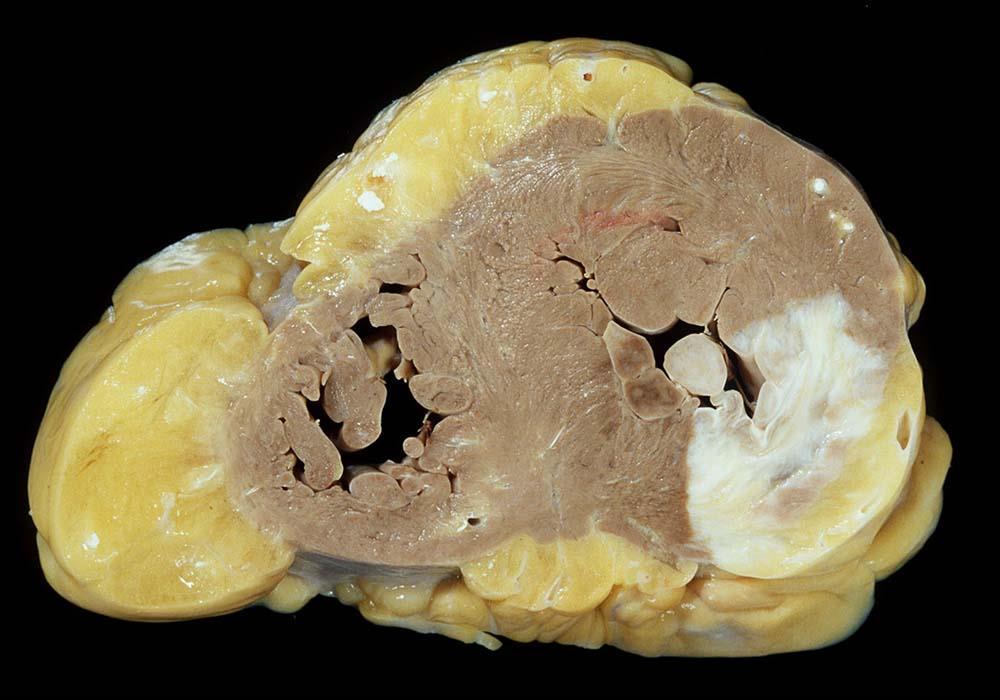
19 Diastolic Heart Failure HFpEF Most patients with heart failure have echo evidence of poor ventricular contraction Some have normal LV function. Is the problem poor diastolic filling? The syndrome is more or less defined physiologically but not pathologically Look for evidence of heart failure in patients with small hearts, hypertrophied ventricles, small cavities but no other causes of heart failure
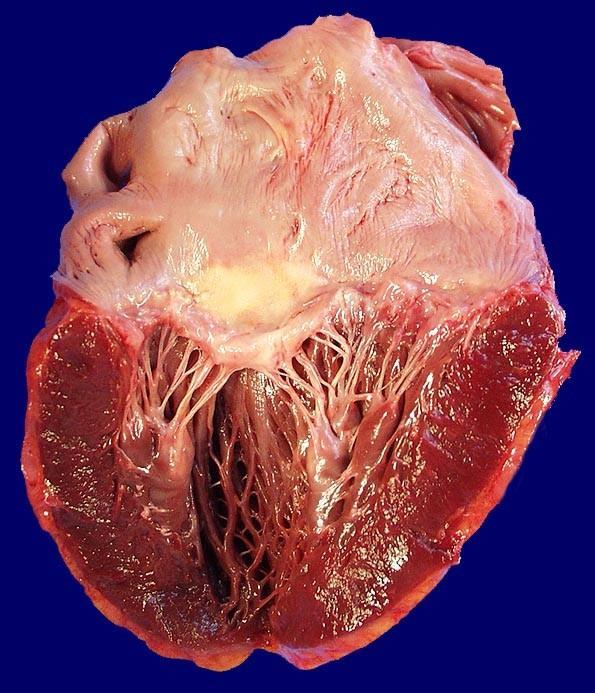
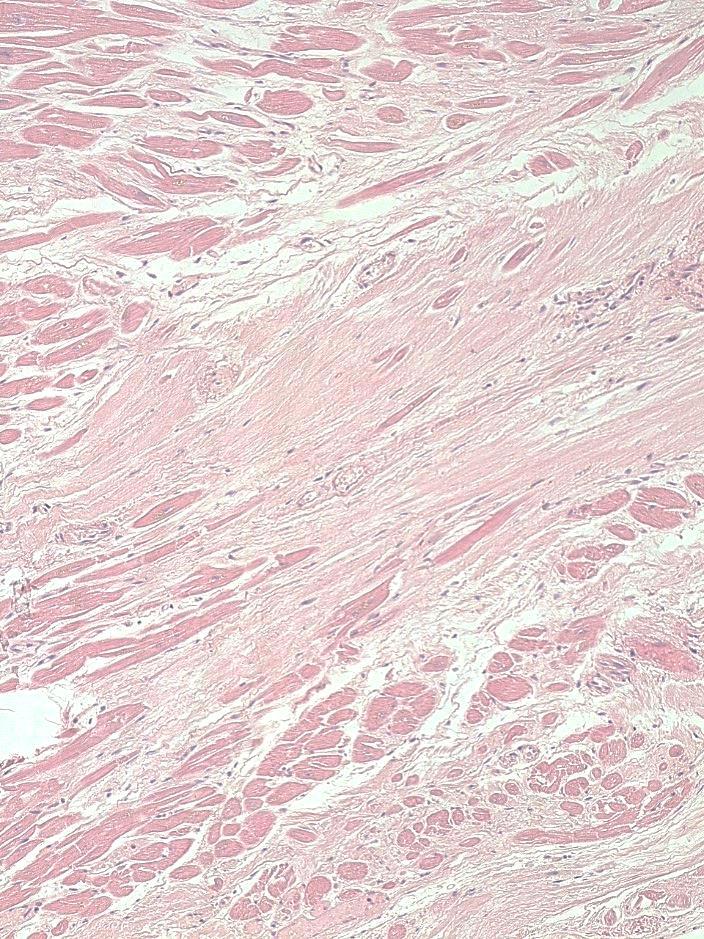
20 Cardiac Muscle Pathology Marked variation in heart weight, up to ~ 600g, but can be in the normal range Many cases have no scars and the muscle itself appears entirely normal Histology may demonstrate an increase in interstitial fibrous tissue After SADS Idiopathic LV hypertrophy with or without fibrosis is the commonest cause of sudden unexplained cardiac death
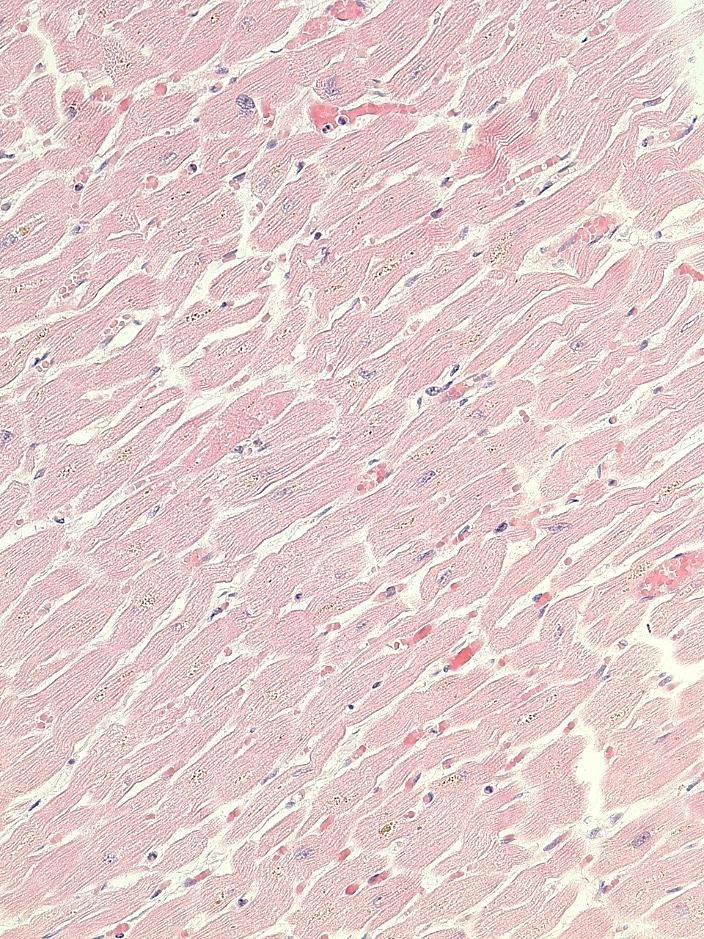
21 Normal Myocardium
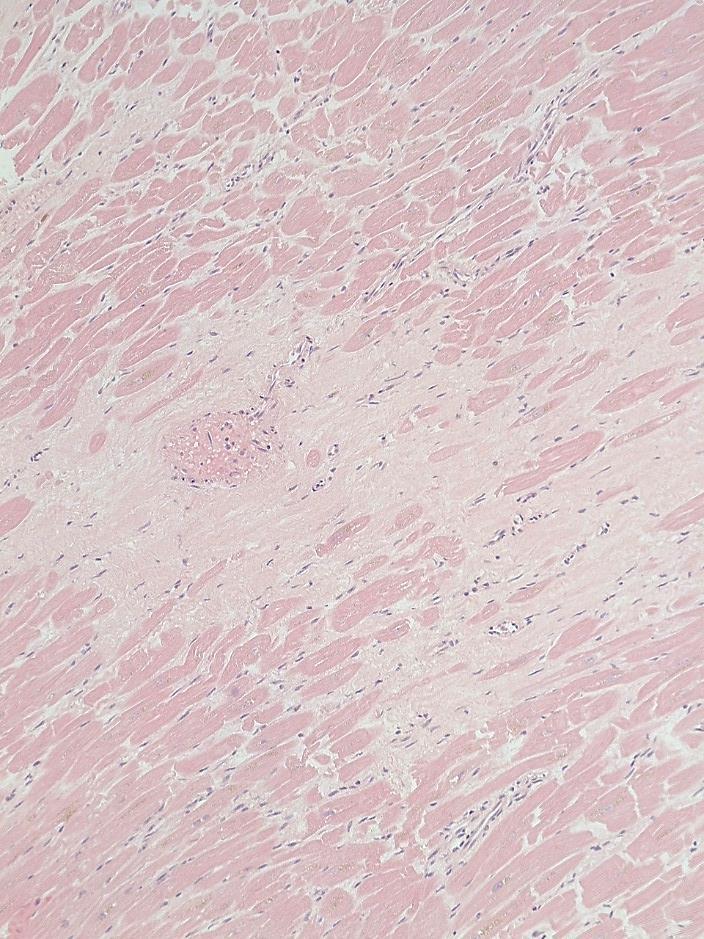
22 Unexplained Heart Failure

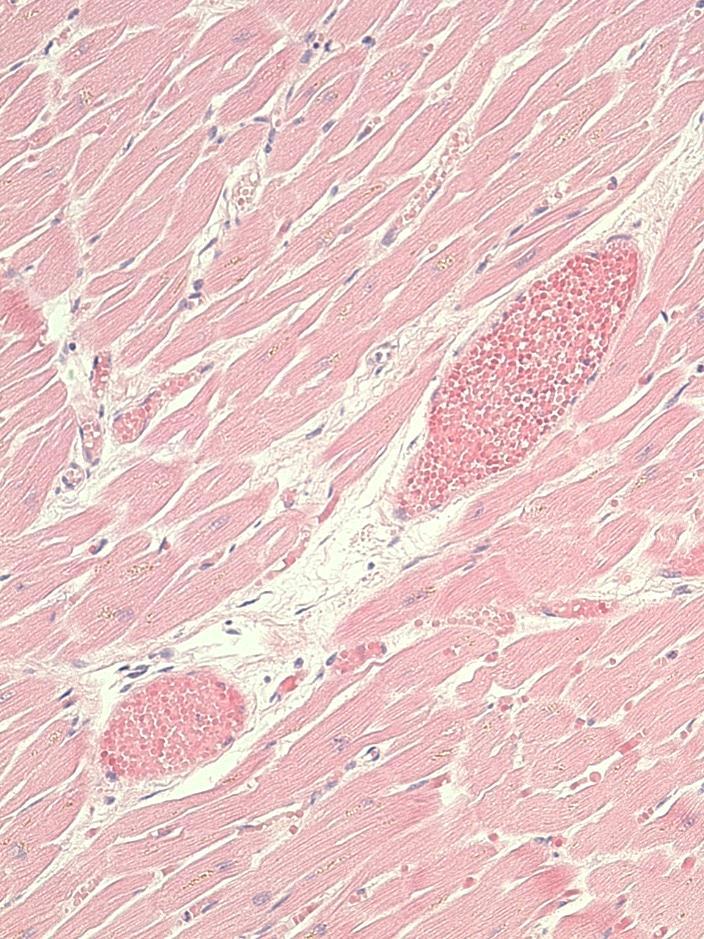
23 Diabetic Small Vessel Disease?
24 Non-cardiac abnormalities in chronic heart failure Fatigue and malaise are disabling symptoms in heart failure. Muscle bulk is lost and there may be structural abnormalities in muscle Many patients are anaemic In the majority of patients renal impairment is the result of the poor cardiac function ( pre renal renal failure )
25 Ischaemic Heart Disease Many patients with clear evidence of healed infarction do not have a critical coronary narrowing Critical narrowings may have been organised and coronary arteries may dilate as part of remodelling The appearance of the epicardial coronary arteries is no guide to the micro circulation Without histology you can miss fibrosis
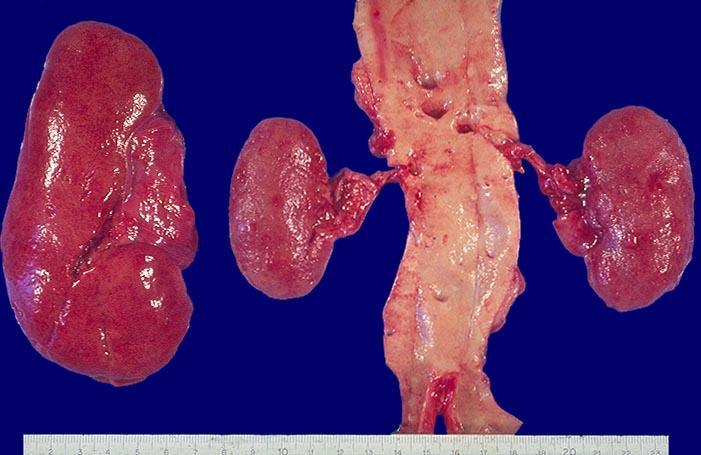
26 Hypertension Although Hospital and GP records are more and more accessible many patients do not have a documented BP There is no pattern of LVH that is diagnostic of hypertension Don t confuse ageing kidneys with hypertensive or end stage renal disease Think very carefully before diagnosing hypertensive heart disease
27

28 End Stage Kidneys
29 Valvular Disease Clinical records are seldom helpful, murmurs vary and 3 rd and 4 th heart sounds rarely described. Even a consistent BP reading may be absent Echo report is invaluable Some degenerative change in all elderly patients Some murmurs have no structural basis

30 Heart sounds
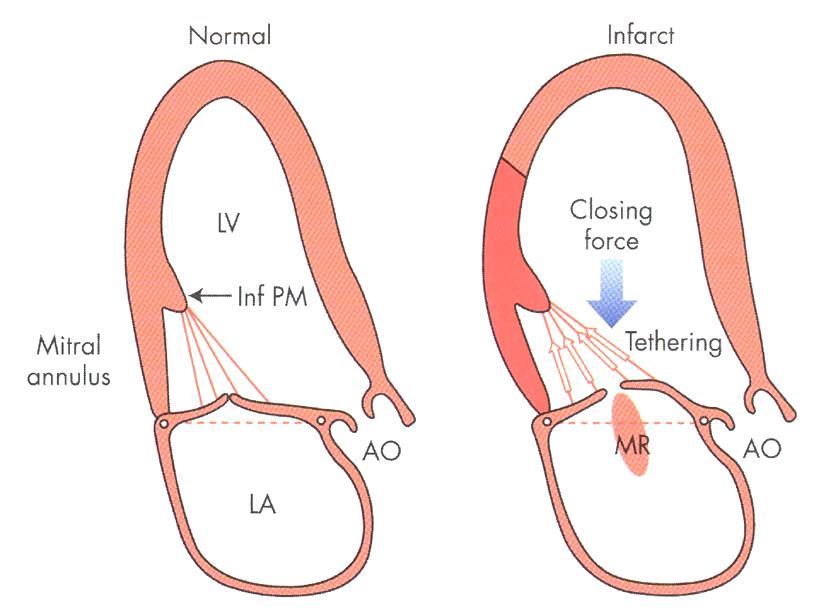
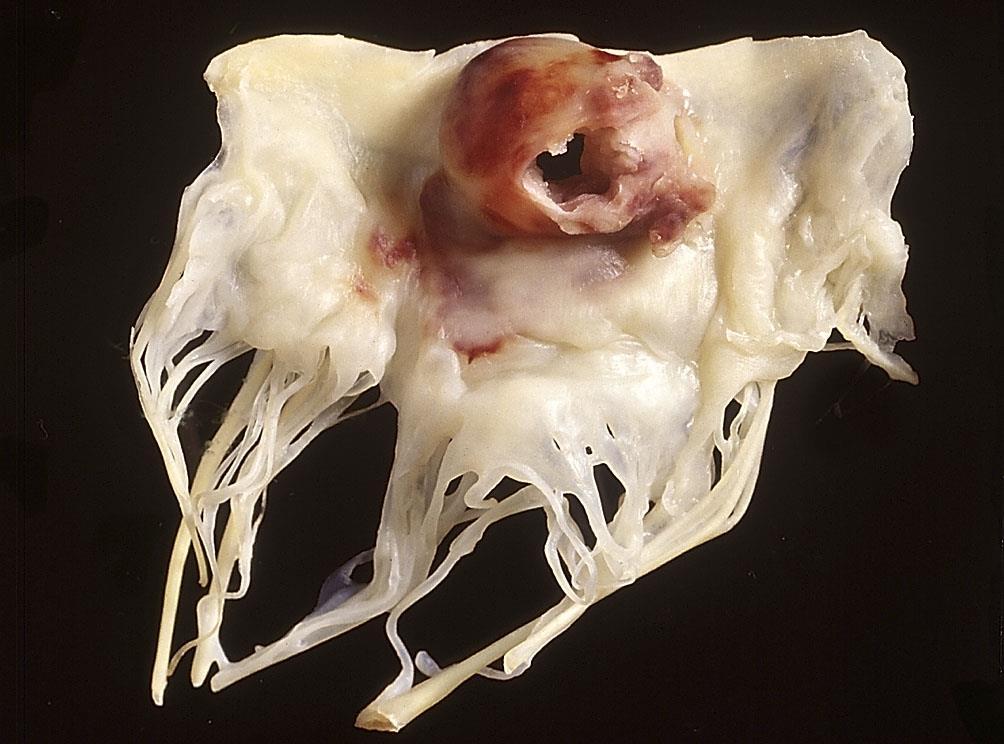
31 Mitral Incompetence Probably the commonest significant valvular abnormality It is often difficult to define a cause at post mortem examination In most cases there are no structural changes in the valve leaflets Limited ventricular dilatation or ischaemic fibrosis may impair mitral valve function An important cause of heart failure
32
33
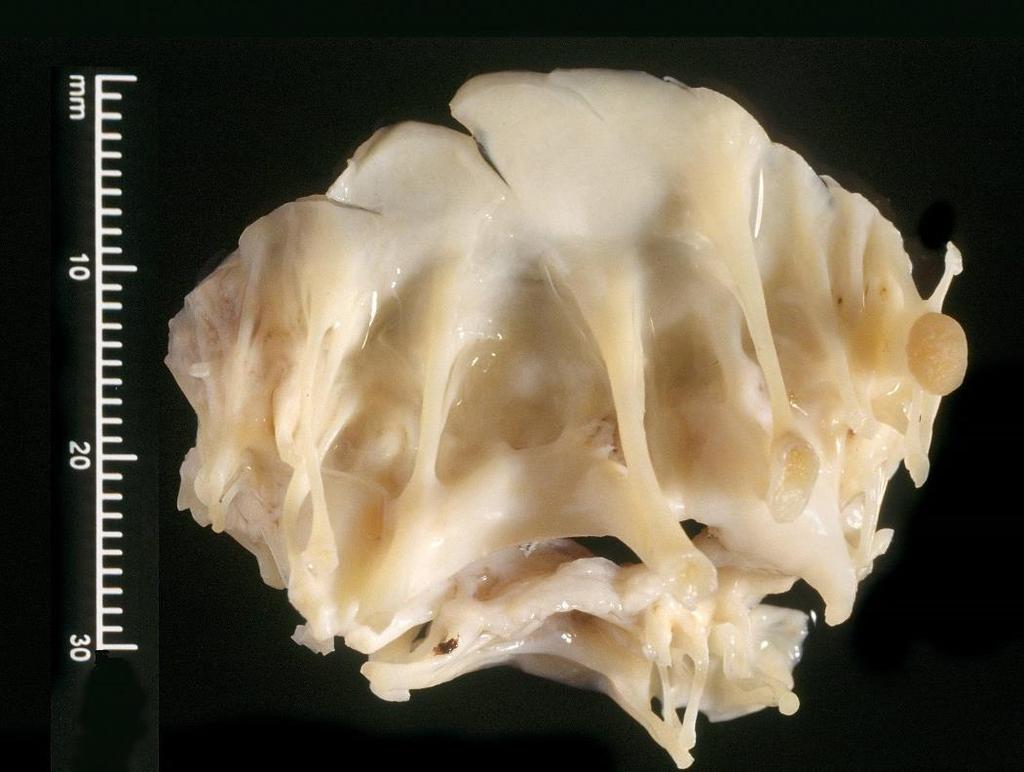
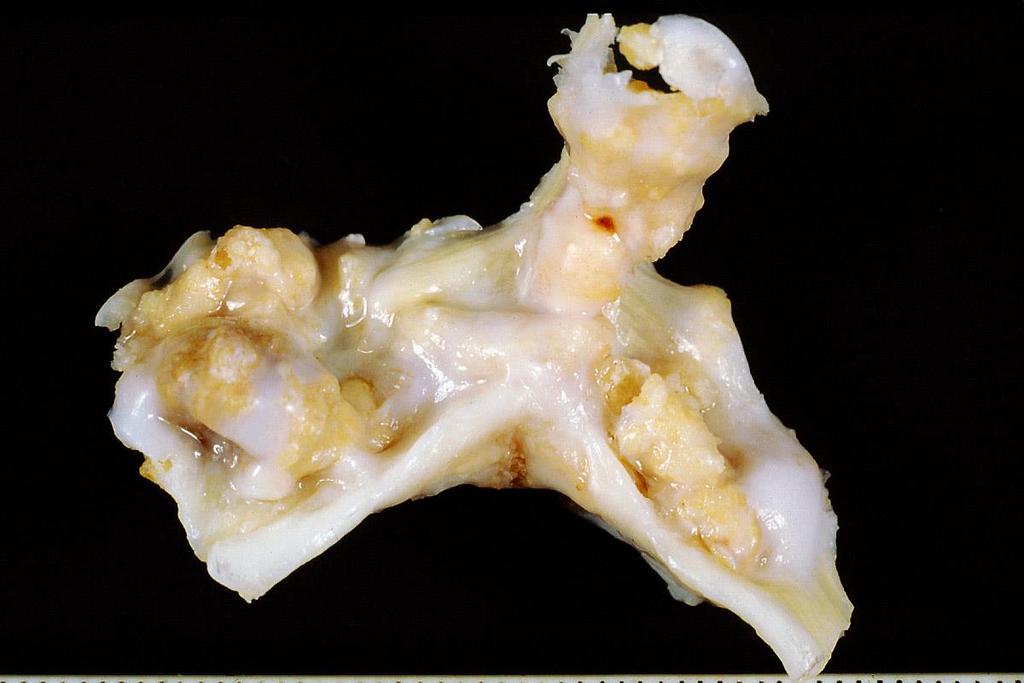
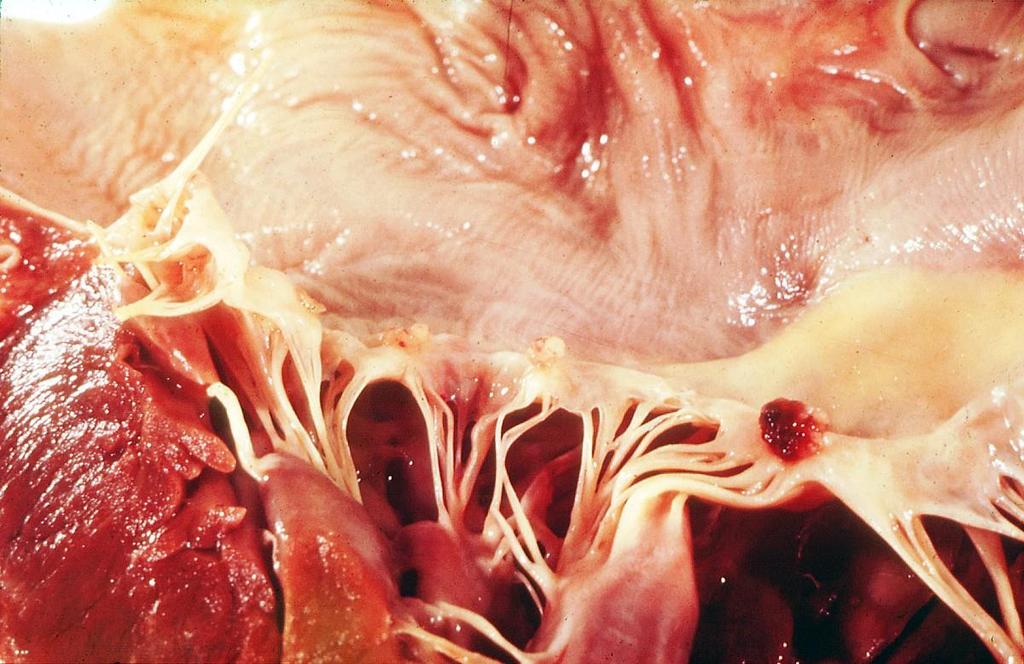
34 Mitral Valve Degeneration A common finding in elderly patients Some cases have marked valve thickening and prolapse. Variable histological changes Prolapse is associated with a mid systolic click and late systolic murmur Results of mitral valve repair are excellent A rare cause of unexpected sudden death

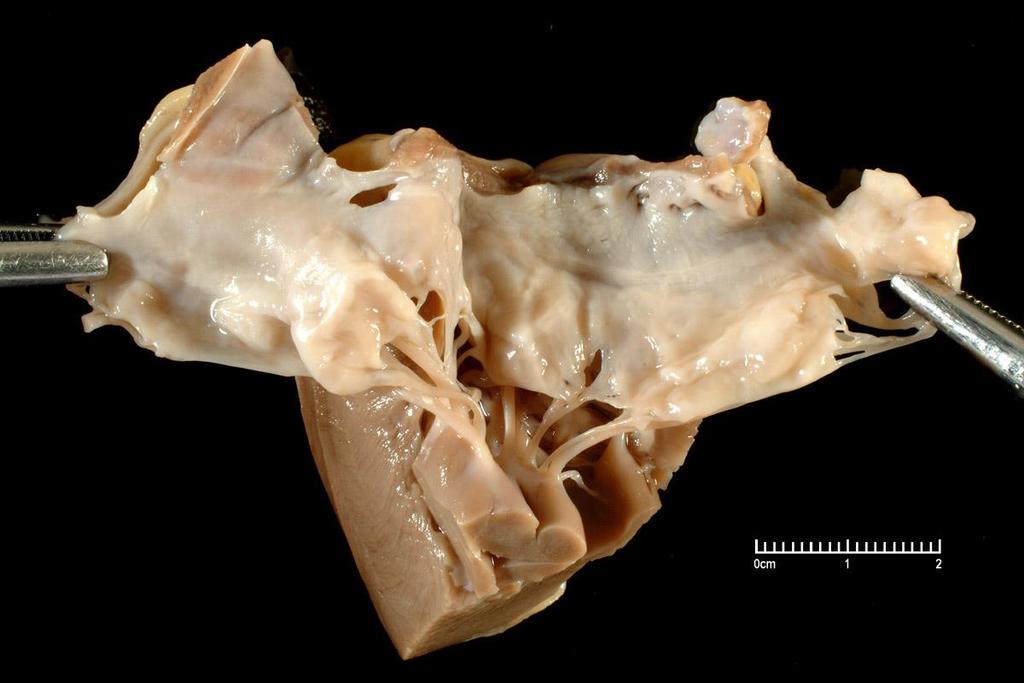
35 Mitral valve prolapse
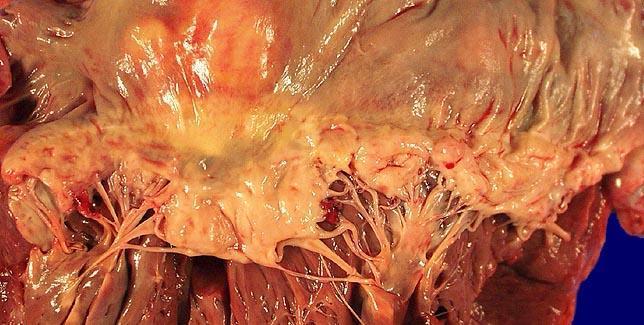
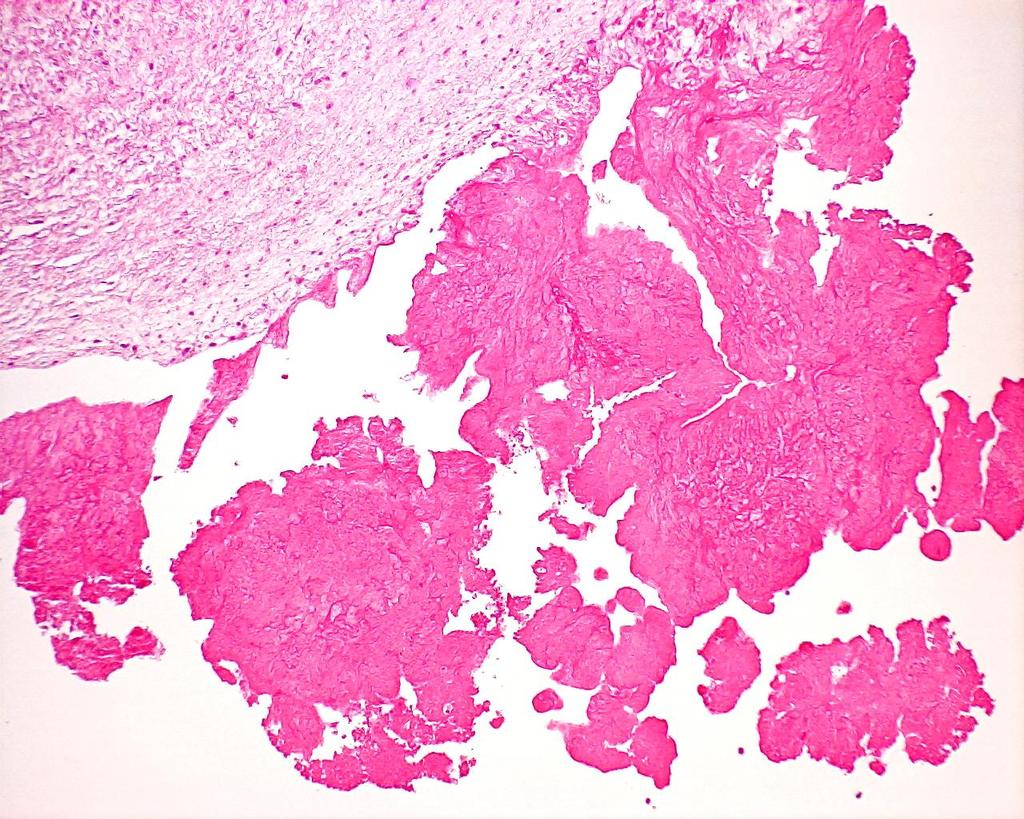
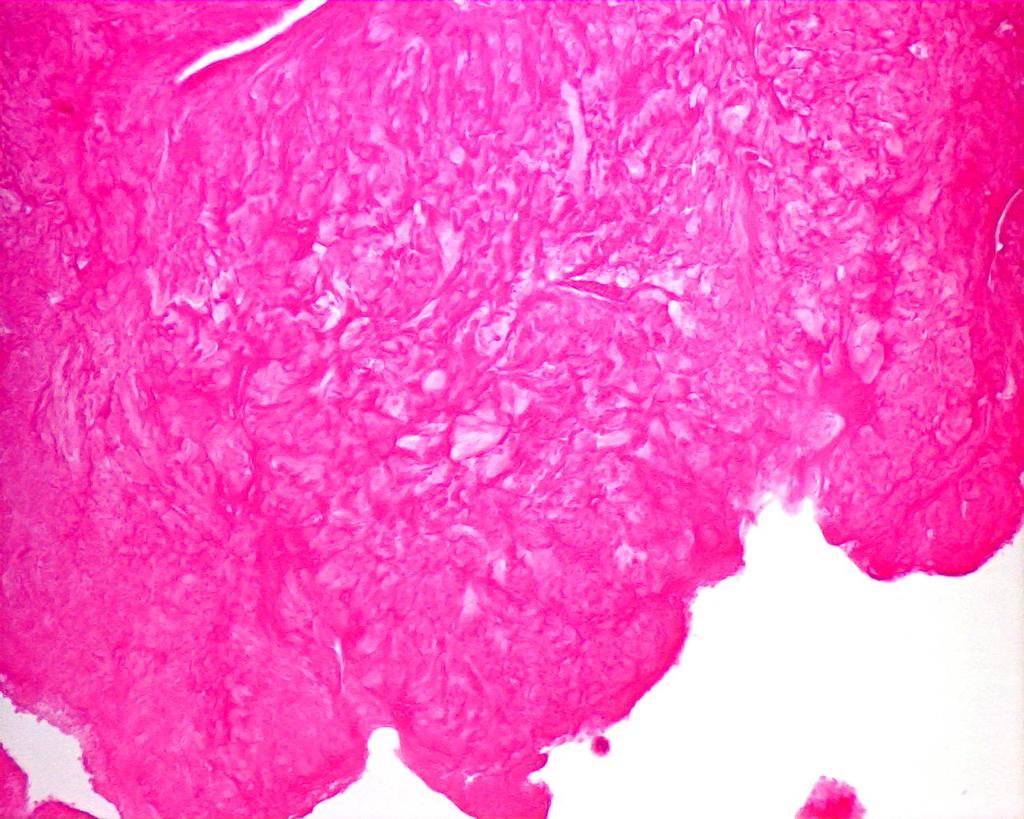
36 Mucoid Degeneration
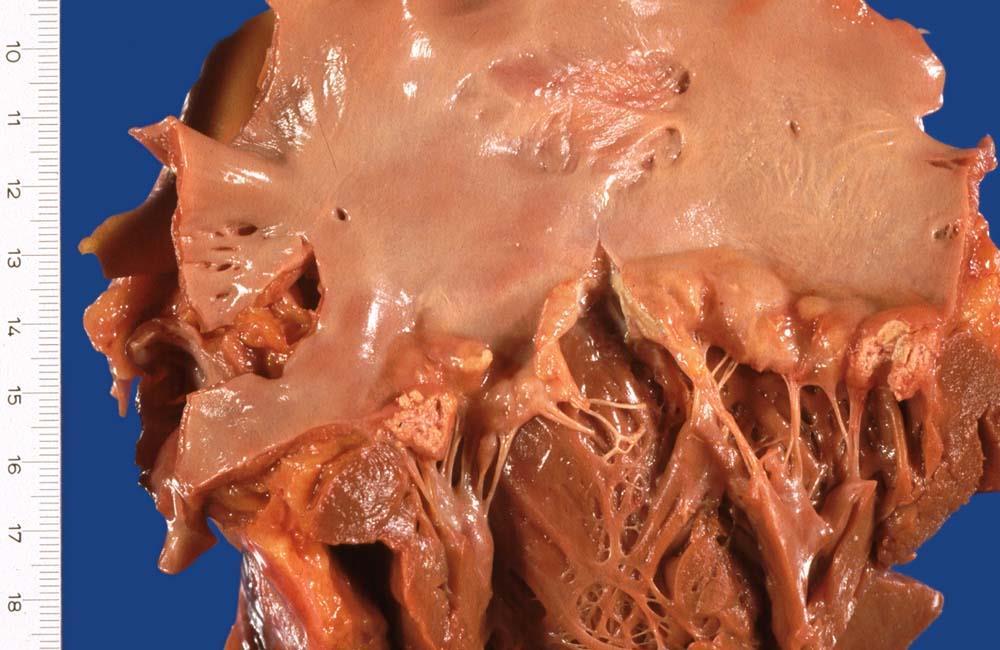
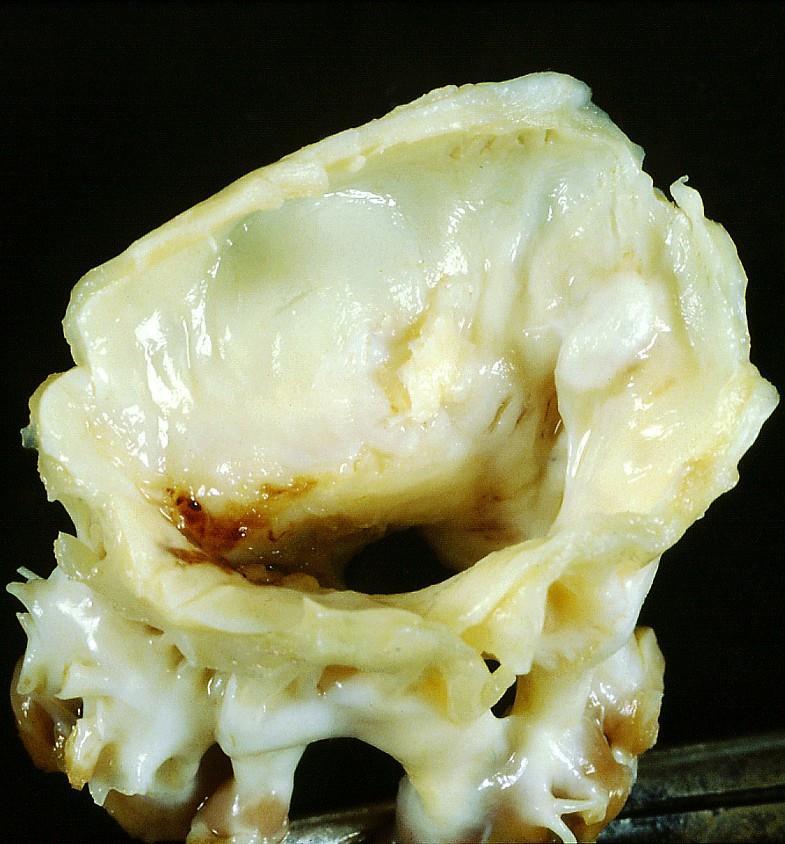
37 Calcification MV Annulus
38

39 Papillary muscle rupture

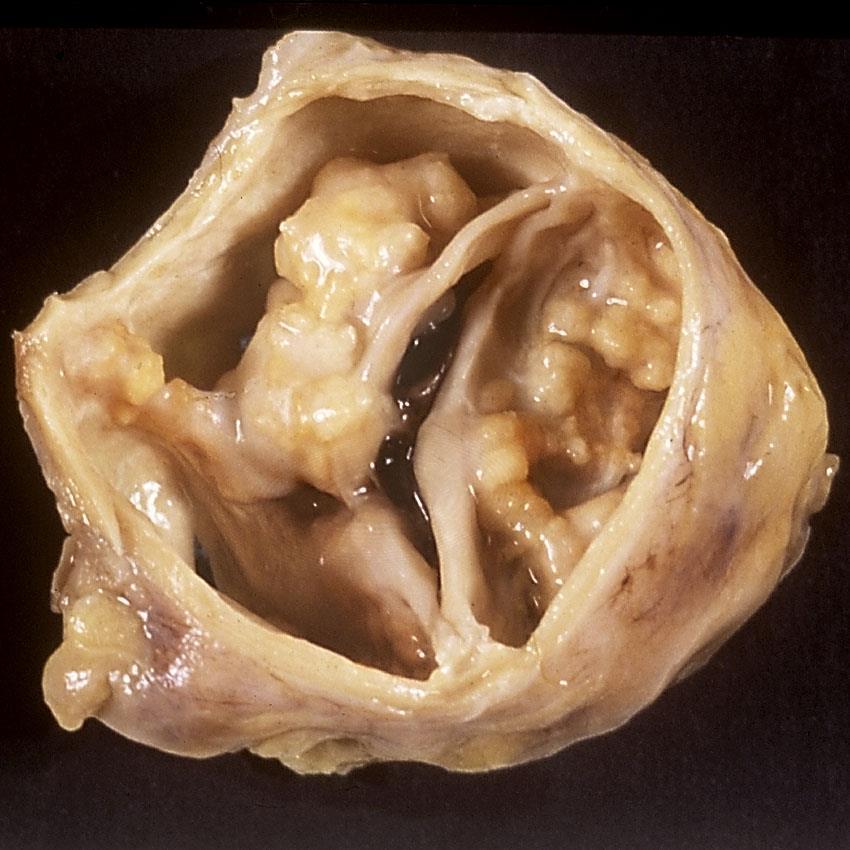
40 Mitral Stenosis
41
42 Mitral Stenosis A small number of cases in white British patients with previous rheumatic fever No progress in understanding of pathogenesis over 40 years Symptoms develop when mitral valve area reduced to 1 cm 2 Significant mortality associated with MVR. Balloon valvuloplasty possible

43 Mitral stenosis with incompetence Atrial dilatation
44 Atrial Fibrillation Suspect AF when there is a history of digitalis or amiodarone treatment There is no established method of estimating ventricular or atrial size Look carefully at the atrial appendages Don t forget to examine the thyroid. Very few thyroids in elderly patients are completely normal

45 Normal aortic valve M66

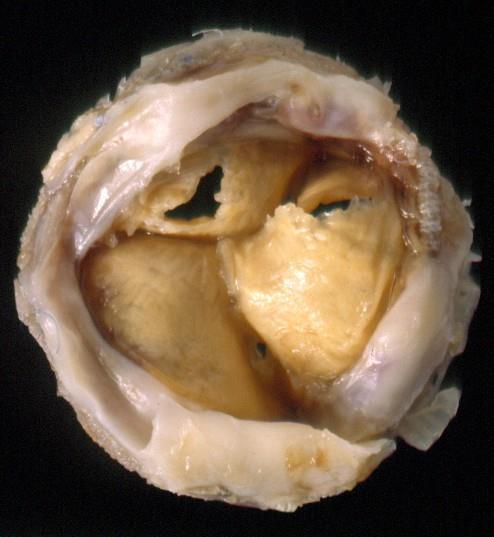
46 Aortic Stenosis
47
48 Aortic Stenosis An important cause of sudden unexpected death. Risk factors similar to those for atheroma. Emerging evidence that there is low grade chronic inflammation in the cusps Previous rheumatic fever is now a rare cause of aortic stenosis. Gradient is related to valve area, e.g. 2cm 2, 26 1cm 2 but 0.5 cm 2
49
50
51

52 Diagnosis
53 Infective Endocarditis Native valve Prosthetic valve Drug abuse Hospital acquired infections After interventions, e.g. haemodialysis, pacemakers etc

54
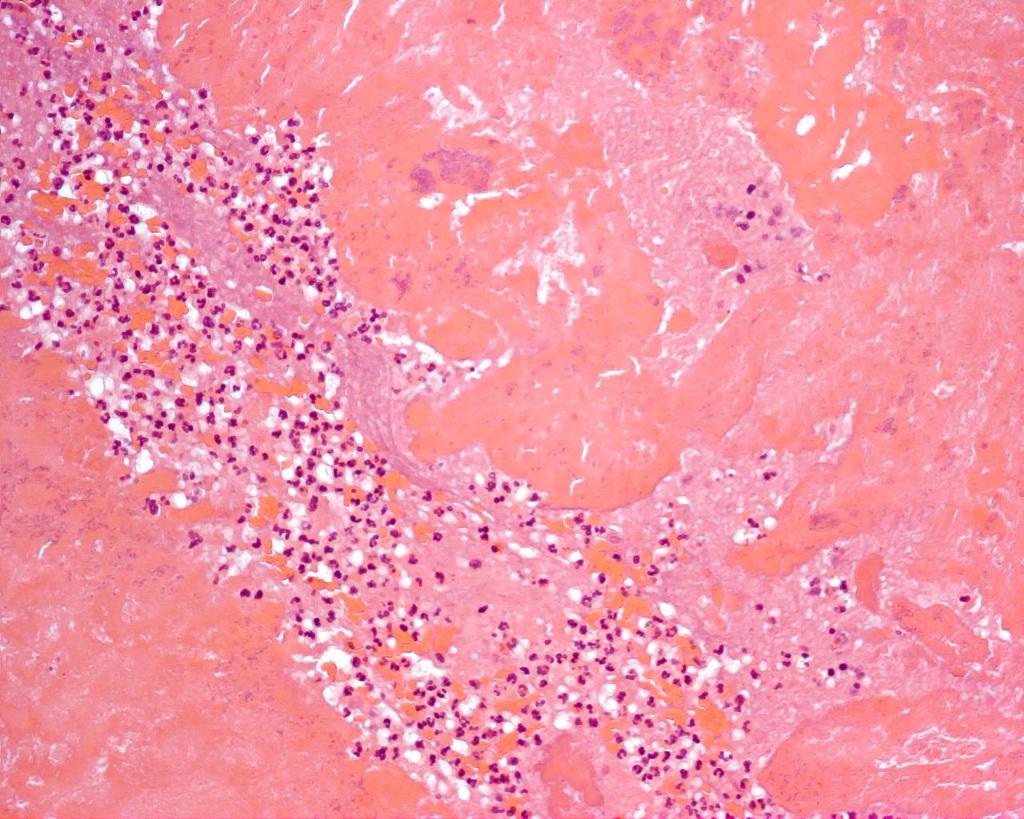
55 Infective Endocarditis The full range of signs and symptoms described in classical texts are now rarely present For various reasons about 15% of genuine cases with echo changes are culture negative S. aureus is now a common causative organism Cases that do not respond rapidly to antibiotic therapy are considered for valve replacement
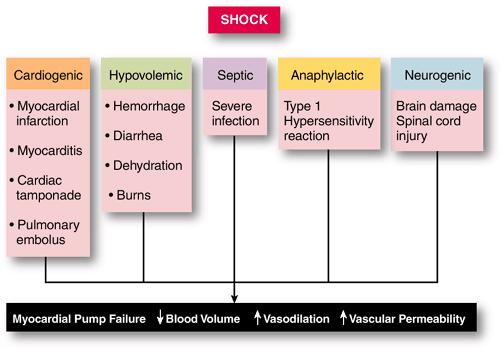
56 Bacteraemia & Septicaemia Bacteria can enter the blood stream from the mouth, gastrointestinal tract, the skin and any source of infection Normally rapidly opsonised and phagocytosed and cleared by the spleen In septicaemia larger numbers of bacteria set up a chain of reactions which generate cytokines and may cause shock
57
58 Septic (Endotoxic) Shock LPS-LPB complexes bind to specific pattern recognition receptors on the surface of monocytes/macrophages. This causes cytokine secretion, especially tumour necrosis factor α (TNFα)
59
60 Septic (Endotoxic) Shock TNF-α stimulates release of other cytokine molecules, such as IL-1 and IL-6 and may directly injure tissues TNF-α also increases the expression of adhesion molecules (e.g.icams) which increase leucocyte adhesion to endothelium Tissue factor release promotes coagulation
61

62
63 Pathophysiology of IE In theory opsoninisation and phagocytosis should kill Gram positive organisms and lead to resolution In IE bacteria grow on the surface of valves, capped by a layer of fibrin. Easy access to nutrients, protected from phagocytes In this privileged site organisms proliferate slowly and form masses called vegetations
64 Infective endocarditis
65
66 Changing Patterns of IE Although the overall incidence may be falling it is rising in elderly patients Improved dental hygiene has reduced streptococcal endocarditis Staphylococci are now the leading cause. Especially associated with haemodialysis, diabetes and iv drugs The advantages of intravascular devices must be weighed against the risk of IE
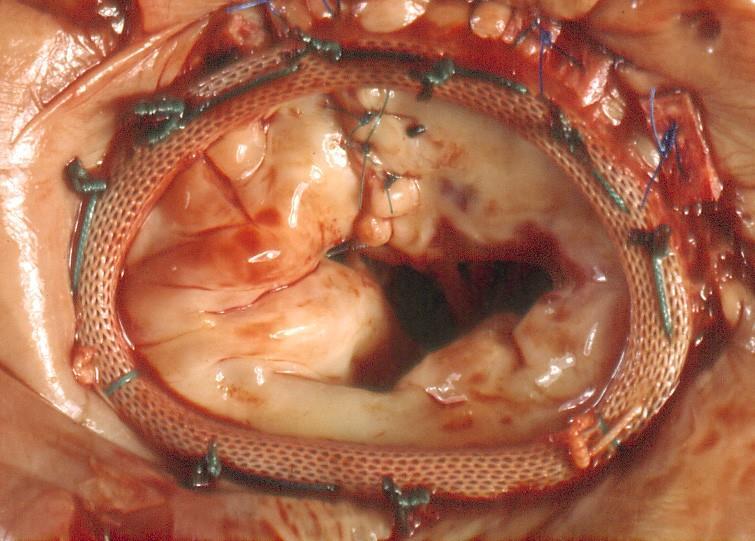
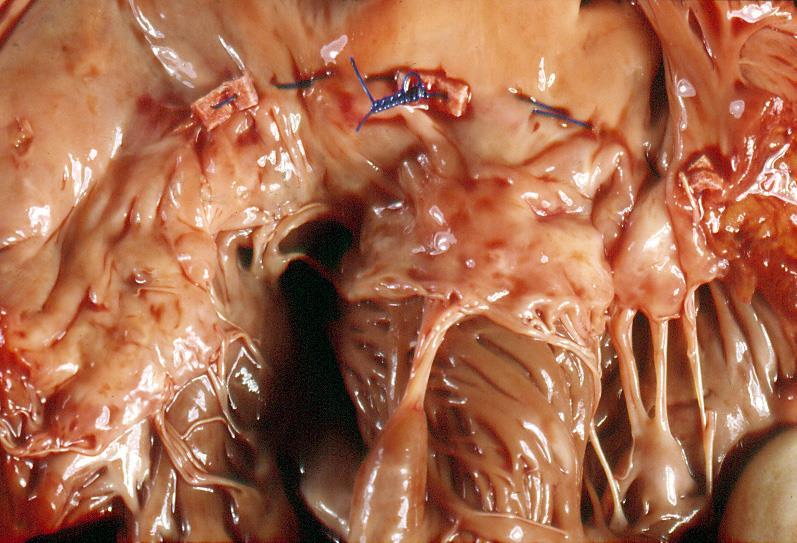
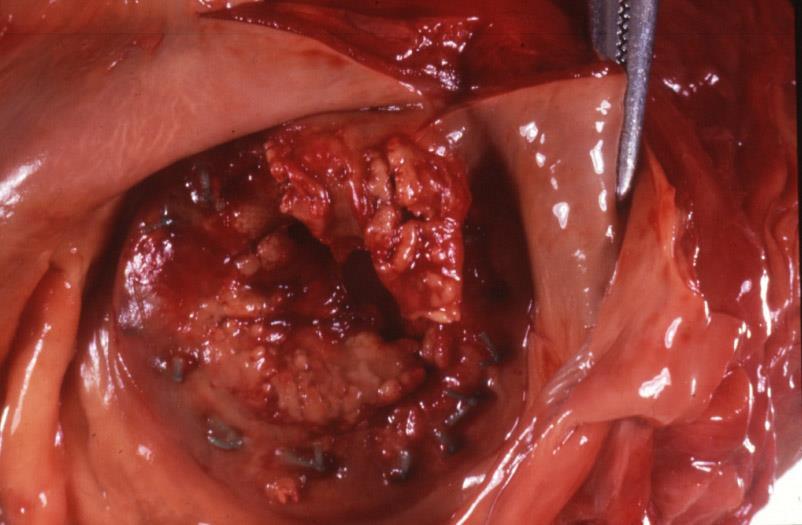
67 Complications of Valve Replacement Perioperative ventricular rupture Infective endocarditis Valvular thrombosis Periprosthetic leak Structural failure Calcification of homografts

68 Carpentier Ring
69
70


71

72 Prosthetic valve endocarditis

73

74 Acute prosthetic valve thrombosis

75 Organising thrombosis of prosthetic valve
76 Periprosthetic leak

77 Structural failure of bioprosthetic valves
78 Summary Hepatic congestion, pleural effusions, LV dilatation & hypertrophy, limb oedema Overlap between CCF and DCM, especially in the elderly Aortic stenosis is an undoubted cause of sudden death. Look out for bicuspids and refer relatives to Drs Curtis/Stuart Ischaemic mitral incompetence is difficult to assess at PM
HEART FAILURE. Study day November 2018 Sarah Briggs
 HEART FAILURE Study day November 2018 Sarah Briggs Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology of heart failure
HEART FAILURE Study day November 2018 Sarah Briggs Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology of heart failure
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Infective Endocarditis عبد المهيمن أحمد
 Infective Endocarditis إعداد : عبد المهيمن أحمد أحمد علي Infective endocarditis Inflammation of the heart valve or endocardium of the heart. The agents are usually bacterial, but other organisms can also
Infective Endocarditis إعداد : عبد المهيمن أحمد أحمد علي Infective endocarditis Inflammation of the heart valve or endocardium of the heart. The agents are usually bacterial, but other organisms can also
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should.
 What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
Means failure of heart to pump enough blood to satisfy the need of the body.
 Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased
Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased
By the end of this session, the student should be able to:
 Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
results in stenosis or insufficiency (regurgitation or incompetence), or both.
, or both.") results in stenosis or insufficiency (regurgitation or incompetence), or both. The outcome of valvular disease depends on : 1-the valve involved 2-the degree of impairment 3-the cause of its development
results in stenosis or insufficiency (regurgitation or incompetence), or both. The outcome of valvular disease depends on : 1-the valve involved 2-the degree of impairment 3-the cause of its development
MI Acute occlusion of the proximal left anterior descending (LAD) artery is the cause of 40% to 50% of all MIs. *
 artery is the cause of 40% to 50% of all MIs. *") MI *33% -50% die before hospital lethal arrhythmia Sudden Cardiac Death. * Arrhythmias are caused by electrical abnormalities of the ischemic myocardium and conduction system. *Acute occlusion of the proximal
MI *33% -50% die before hospital lethal arrhythmia Sudden Cardiac Death. * Arrhythmias are caused by electrical abnormalities of the ischemic myocardium and conduction system. *Acute occlusion of the proximal
Myocardial Infarction
 Myocardial Infarction MI = heart attack Defined as necrosis of heart muscle resulting from ischemia. A very significant cause of death worldwide. of these deaths, 33% -50% die before they can reach the
Myocardial Infarction MI = heart attack Defined as necrosis of heart muscle resulting from ischemia. A very significant cause of death worldwide. of these deaths, 33% -50% die before they can reach the
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Shock, Hemorrhage and Thrombosis
 Shock, Hemorrhage and Thrombosis 1 Shock Systemic hypoperfusion due to: Reduction in cardiac output Reduction in effective circulating blood volume Hypotension Impaired tissue perfusion Cellular hypoxia
Shock, Hemorrhage and Thrombosis 1 Shock Systemic hypoperfusion due to: Reduction in cardiac output Reduction in effective circulating blood volume Hypotension Impaired tissue perfusion Cellular hypoxia
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to:
 The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
DOWNLOAD PDF ABC OF HEART FAILURE
 Chapter 1 : The ABCs of managing systolic heart failure: Past, present, and future Heart failure is a multisystem disorder which is characterised by abnormalities of cardiac, skeletal muscle, and renal
Chapter 1 : The ABCs of managing systolic heart failure: Past, present, and future Heart failure is a multisystem disorder which is characterised by abnormalities of cardiac, skeletal muscle, and renal
VALVULAR HEART DISEASE
 VALVULAR HEART DISEASE Stenosis: failure of a valve to open completely, obstructing forward flow. - almost always due to a chronic process (e.g., calcification or valve scarring). Insufficiency : failure
VALVULAR HEART DISEASE Stenosis: failure of a valve to open completely, obstructing forward flow. - almost always due to a chronic process (e.g., calcification or valve scarring). Insufficiency : failure
Clinical Indications for Echocardiography
 Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart on Fire: Infective Endocarditis. Objectives. Disclosure 8/27/2018. Mary McGreal DNP, RN, ANP-c, CCRN
 Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
The Causes of Heart Failure
 The Causes of Heart Failure Andy Birchall HFSN Right heart failure LVSD - HFREF Valve regurgitation or stenosis Dropsy CCF congestive cardiac failure Cor pulmonale Pulmonary hypertension HFPEF LVF Definitions
The Causes of Heart Failure Andy Birchall HFSN Right heart failure LVSD - HFREF Valve regurgitation or stenosis Dropsy CCF congestive cardiac failure Cor pulmonale Pulmonary hypertension HFPEF LVF Definitions
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
ATHEROSCLEROSIS. Secondary changes are found in other coats of the vessel wall.
 ATHEROSCLEROSIS Atherosclerosis Atherosclerosis is a disease process affecting the intima of the aorta and large and medium arteries, taking the form of focal thickening or plaques of fibrous tissue and
ATHEROSCLEROSIS Atherosclerosis Atherosclerosis is a disease process affecting the intima of the aorta and large and medium arteries, taking the form of focal thickening or plaques of fibrous tissue and
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Structure and organization of blood vessels
 The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
Saluki heart pathology study
 Heart conditions by MaryDee Sist, DVM Originally published in Baraka Book, Autumn-Winter 2001 For the last decade I have been involved in Saluki heart research. Ouroriginalgoalwastoexaminethe incidence
Heart conditions by MaryDee Sist, DVM Originally published in Baraka Book, Autumn-Winter 2001 For the last decade I have been involved in Saluki heart research. Ouroriginalgoalwastoexaminethe incidence
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
HEART FAILURE. Study day November 2017 Sarah Briggs and Janet Laing
 HEART FAILURE Study day November 2017 Sarah Briggs and Janet Laing Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology
HEART FAILURE Study day November 2017 Sarah Briggs and Janet Laing Overview and Introduction This course is an introduction and overview of heart failure. Normal heart function and basic pathophysiology
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
1) Severe, crushing substernal chest pain 2) radiate to the neck, jaw, epigastrium, or left arm. 3- rapid and weak pulse 4- nausea (posterior MI).
 Severe, crushing substernal chest pain 2) radiate to the neck, jaw, epigastrium, or left arm. 3- rapid and weak pulse 4- nausea (posterior MI).") 1) Severe, crushing substernal chest pain 2) radiate to the neck, jaw, epigastrium, or left arm. 3- rapid and weak pulse 4- nausea (posterior MI). 5- cardiogenic shock (massive MIs >40% of the left ventricle)
1) Severe, crushing substernal chest pain 2) radiate to the neck, jaw, epigastrium, or left arm. 3- rapid and weak pulse 4- nausea (posterior MI). 5- cardiogenic shock (massive MIs >40% of the left ventricle)
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Charles Spencer MD, FRCP Consultant Cardiologist Mid Staffs NHSFT
 Charles Spencer MD, FRCP Consultant Cardiologist Mid Staffs NHSFT Key Messages Heart Failure is Common Heart failure is complex Heart Failure is a major issue for the NHS Heart Failure has a worse prognosis
Charles Spencer MD, FRCP Consultant Cardiologist Mid Staffs NHSFT Key Messages Heart Failure is Common Heart failure is complex Heart Failure is a major issue for the NHS Heart Failure has a worse prognosis
Valvular defects. Lectures from Pathological Physiology. Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková
 Valvular defects Lectures from Pathological Physiology Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková 1 2 3 1 Valvular dysfunction - introduction Stenosis block of flow;
Valvular defects Lectures from Pathological Physiology Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková 1 2 3 1 Valvular dysfunction - introduction Stenosis block of flow;
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
Mitral Valve Disease. Prof. Sirchak Yelizaveta Stepanovna
 Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
3. Results of study. Causes of death
 3. Results of study Causes of death Towards the end of an autopsy report is the pathologist's opinion as to the cause of death, which should be presented in the standard manner prescribed by the Office
3. Results of study Causes of death Towards the end of an autopsy report is the pathologist's opinion as to the cause of death, which should be presented in the standard manner prescribed by the Office
Ischemic heart disease
 Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Cardiovascular manifestations of HIV
 Cardiovascular manifestations of HIV Prabhakar Rajiah, MBBS, MD, FRCR Associate Professor of Radiology Associate Director, Cardiac CT and MRI University of Texas Southwestern Medical Center, Dallas, USA
Cardiovascular manifestations of HIV Prabhakar Rajiah, MBBS, MD, FRCR Associate Professor of Radiology Associate Director, Cardiac CT and MRI University of Texas Southwestern Medical Center, Dallas, USA
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Worldwide rheumatic fever is the most common cause of valve disease. In industrialized areas, valvular disease of old age predominates
 Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Cardiac Pathology & Rehabilitation
 Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload Cardiac output (CO) represents the volume of blood that is delivered
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload Cardiac output (CO) represents the volume of blood that is delivered
Diastolic Heart Failure. Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012
 Diastolic Heart Failure Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012 Disclosures Have spoken for Merck, Sharpe and Dohme Sat on a physician advisory
Diastolic Heart Failure Edwin Tulloch-Reid MBBS FACC Consultant Cardiologist Heart Institute of the Caribbean December 2012 Disclosures Have spoken for Merck, Sharpe and Dohme Sat on a physician advisory
Sarah J. Miller, DVM, Diplomate ACVIM (Cardiology) Degenerative Valvular Disease What s New?
 Degenerative Valvular Disease What s New?") Sarah J. Miller, DVM, Diplomate ACVIM (Cardiology) Degenerative Valvular Disease What s New? Chronic degenerative valvular disease is the most common cardiovascular disease in small animals, and is also
Sarah J. Miller, DVM, Diplomate ACVIM (Cardiology) Degenerative Valvular Disease What s New? Chronic degenerative valvular disease is the most common cardiovascular disease in small animals, and is also
Valvular Heart Disease in Clinical Practice
 Valvular Heart Disease in Clinical Practice Michael Y. Henein Editor Valvular Heart Disease in Clinical Practice 123 Editor Michael Y. Henein Consultant Cardiologist Umea Heart Centre Umea University
Valvular Heart Disease in Clinical Practice Michael Y. Henein Editor Valvular Heart Disease in Clinical Practice 123 Editor Michael Y. Henein Consultant Cardiologist Umea Heart Centre Umea University
Valvular Heart Disease
 Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
10/8/2018. Lecture 9. Cardiovascular Health. Lecture Heart 2. Cardiovascular Health 3. Stroke 4. Contributing Factor
 Lecture 9 Cardiovascular Health 1 Lecture 9 1. Heart 2. Cardiovascular Health 3. Stroke 4. Contributing Factor 1 The Heart Muscular Pump The Heart Receives blood low pressure then increases the pressure
Lecture 9 Cardiovascular Health 1 Lecture 9 1. Heart 2. Cardiovascular Health 3. Stroke 4. Contributing Factor 1 The Heart Muscular Pump The Heart Receives blood low pressure then increases the pressure
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
In Vivo Animal Models of Heart Disease. Why Animal Models of Disease? Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison
 In Vivo Animal Models of Heart Disease Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison Why Animal Models of Disease? Heart Failure (HF) Leading cause of morbidity and mortality
In Vivo Animal Models of Heart Disease Timothy A Hacker, PhD Department of Medicine University of Wisconsin-Madison Why Animal Models of Disease? Heart Failure (HF) Leading cause of morbidity and mortality
Do Now. Get out work from last class to be checked
 Do Now Get out work from last class to be checked Heart Actions Cardiac Cycle: One complete heartbeat. The contraction of a heart chamber is called systole and the relaxation of a chamber is called diastole.
Do Now Get out work from last class to be checked Heart Actions Cardiac Cycle: One complete heartbeat. The contraction of a heart chamber is called systole and the relaxation of a chamber is called diastole.
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Rheumatic heart disease
 Rheumatic heart disease What will we discuss today? Etiology and epidemiology of rheumatic heart disease Pathogenesis of rheumatic heart disease Morphological changes in rheumatic heart disease Clinical
Rheumatic heart disease What will we discuss today? Etiology and epidemiology of rheumatic heart disease Pathogenesis of rheumatic heart disease Morphological changes in rheumatic heart disease Clinical
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
10. Thick deposits of lipids on the walls of blood vessels, called, can lead to serious circulatory issues. A. aneurysm B. atherosclerosis C.
 Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
Heart Student: 1. carry blood away from the heart. A. Arteries B. Veins C. Capillaries 2. What is the leading cause of heart attack and stroke in North America? A. alcohol B. smoking C. arteriosclerosis
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Year 1 Peer Based Learning 2018 Cardiovascular System
 Please note this learning resource has been produced by the GUMS Academic Team. It is possible that there are some minor errors in the questions/answers, and other possible answers that are not included
Please note this learning resource has been produced by the GUMS Academic Team. It is possible that there are some minor errors in the questions/answers, and other possible answers that are not included
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide
 Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
In the name of GOD. Animal models of cardiovascular diseases: myocardial infarction & hypertension
 In the name of GOD Animal models of cardiovascular diseases: myocardial infarction & hypertension 44 Presentation outline: Cardiovascular diseases Acute myocardial infarction Animal models for myocardial
In the name of GOD Animal models of cardiovascular diseases: myocardial infarction & hypertension 44 Presentation outline: Cardiovascular diseases Acute myocardial infarction Animal models for myocardial
Anatomy and Physiology, Spring 2015 Exam II: Form A April 9, Name Student Number
 Anatomy and Physiology, Spring 2015 Exam II: Form A April 9, 2015 Name Student Number For Questions 1 2 refer to the following table. 1 Ventricular pressure is greater than aortic 6 AV valve is open 2
Anatomy and Physiology, Spring 2015 Exam II: Form A April 9, 2015 Name Student Number For Questions 1 2 refer to the following table. 1 Ventricular pressure is greater than aortic 6 AV valve is open 2
ACUTE CENTRAL PERIFERALEMBOLISM
 EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC
 Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC Overview ACS continued Heart Failure Valvular Disorders and Endocarditis Diagnosis Nuclear stress test- stable angina
Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC Overview ACS continued Heart Failure Valvular Disorders and Endocarditis Diagnosis Nuclear stress test- stable angina
Hemodynamic Disorders, Thrombosis, and Shock. Richard A. McPherson, M.D.
 Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Aortic Valve Lesions
 Version 1.0 Valvular Heart Disease 25/03/2012 Aortic Stenosis Aortic Valve Lesions General Most common isolated affected valve, esp elderly 4M:1F Unrecognised can be important cause of anaesthetic & obstetric
Version 1.0 Valvular Heart Disease 25/03/2012 Aortic Stenosis Aortic Valve Lesions General Most common isolated affected valve, esp elderly 4M:1F Unrecognised can be important cause of anaesthetic & obstetric
The Cardiovascular System
 The Cardiovascular System The Cardiovascular System A closed system of the heart and blood vessels The heart pumps blood Blood vessels allow blood to circulate to all parts of the body The function of
The Cardiovascular System The Cardiovascular System A closed system of the heart and blood vessels The heart pumps blood Blood vessels allow blood to circulate to all parts of the body The function of
Aortic stenosis and regurgitation
 1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
Section 5.1 The heart and heart disease
 Section 5.1 The heart and heart disease Mammals are too large to rely on diffusion. They need a circulatory system to move substances around the body. Blood moves down pressure gradients, from high to
Section 5.1 The heart and heart disease Mammals are too large to rely on diffusion. They need a circulatory system to move substances around the body. Blood moves down pressure gradients, from high to
Pathophysiology of Cardiovascular System. Dr. Hemn Hassan Othman, PhD
 Pathophysiology of Cardiovascular System Dr. Hemn Hassan Othman, PhD hemn.othman@univsul.edu.iq What is the circulatory system? The circulatory system carries blood and dissolved substances to and from
Pathophysiology of Cardiovascular System Dr. Hemn Hassan Othman, PhD hemn.othman@univsul.edu.iq What is the circulatory system? The circulatory system carries blood and dissolved substances to and from
Therefore MAP=CO x TPR = HR x SV x TPR
 Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
The Cardiovascular System
 The Cardiovascular System https://www.youtube.com/watch?v=ohmmtqkgs50 Human Anatomy & Physiology P. Wilson 1 Introduction The functions of the cardiovascular system are: to bring oxygen & nutrients to
The Cardiovascular System https://www.youtube.com/watch?v=ohmmtqkgs50 Human Anatomy & Physiology P. Wilson 1 Introduction The functions of the cardiovascular system are: to bring oxygen & nutrients to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
ADVANCES IN MITRAL VALVE DISEASE
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk ADVANCES IN MITRAL VALVE DISEASE Author : Gemma Hopkins Categories : Vets Date : June 1, 2009 Gemma Hopkins relates an informative
Vet Times The website for the veterinary profession https://www.vettimes.co.uk ADVANCES IN MITRAL VALVE DISEASE Author : Gemma Hopkins Categories : Vets Date : June 1, 2009 Gemma Hopkins relates an informative
Cardiovascular Disorders. Heart Disorders. Diagnostic Tests for CV Function. Bio 375. Pathophysiology
 Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Outcomes: By the end of this session the student will be able to:
 Outcomes: By the end of this session the student will be able to: Discuss the cardiovascular system Identify the normal changes that occur with ageing Explain the nurses role in the care of residents with
Outcomes: By the end of this session the student will be able to: Discuss the cardiovascular system Identify the normal changes that occur with ageing Explain the nurses role in the care of residents with
Cardiology. the Sounds: #7 HCM. LV Outflow Obstruction: Aortic Stenosis. (Coming Soon - HCM)
") A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
Cardiomyopathy Consequences. function of the myocardium for any reason. This is a serious disease in which the heart muscle
 Becki Simmons Cardiomyopathy Consequences Cardiomyopathy, which literally means "heart muscle disease," is the deterioration of the function of the myocardium for any reason. This is a serious disease
Becki Simmons Cardiomyopathy Consequences Cardiomyopathy, which literally means "heart muscle disease," is the deterioration of the function of the myocardium for any reason. This is a serious disease
Mitral Valve Disease. Chapter 29
 Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
Pregnancy and Heart Disease. Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital
 Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
4/11/2017. Cardiomyopathy. John Steuter, MD Bryan Heart. Disclosures. No Conflicts. Cardiomyopathy. WHO Classification
 Cardiomyopathy John Steuter, MD Bryan Heart Disclosures No Conflicts Cardiomyopathy WHO Classification Anatomy & physiology of the LV 1. Dilated Enlarged Systolic dysfunction 2. Hypertrophic Thickened
Cardiomyopathy John Steuter, MD Bryan Heart Disclosures No Conflicts Cardiomyopathy WHO Classification Anatomy & physiology of the LV 1. Dilated Enlarged Systolic dysfunction 2. Hypertrophic Thickened