Worldwide rheumatic fever is the most common cause of valve disease. In industrialized areas, valvular disease of old age predominates
|
|
|
- Martin Young
- 5 years ago
- Views:
Transcription




1 Michael Sumners DO
2 Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional Mitral Regurgitation
3 Epidemiology Valvular heart disease accounts for 10-20% of cardiac surgical procedures. Two-thirds of heart valve operations are for aortic valve replacement The most common reason for AVR is bicuspid aortic valve. 2/3 of <70yo. Mitral valve surgery is most often performed for MR
4 Valvular Disease is Under-detected Post-mortem studies show approximately 50% of aortic stenosis is identified before death. **** Perioperative and Maternal deaths
5
6 Major Changes to the Guideline Restructured to help determine timing of interventions Transcatheter therapies Recommendations for use of heart valve team More patients with asymptomatic severe valve disease can be considered for intervention
7 2008 Update 2014 ABCD Helps to determine Timing of intervention Assess risk Severity of Valve Lesion Symptoms Response of LV and RV Rhythm Changes
8
9
10 Aortic Stenosis Not a Passive Disease Process Active lipid deposition Inflammation Neo-angiogenesis Calcification Risk Factors Male, diabetes, dyslipidemia Metabolic syndrome, smoking

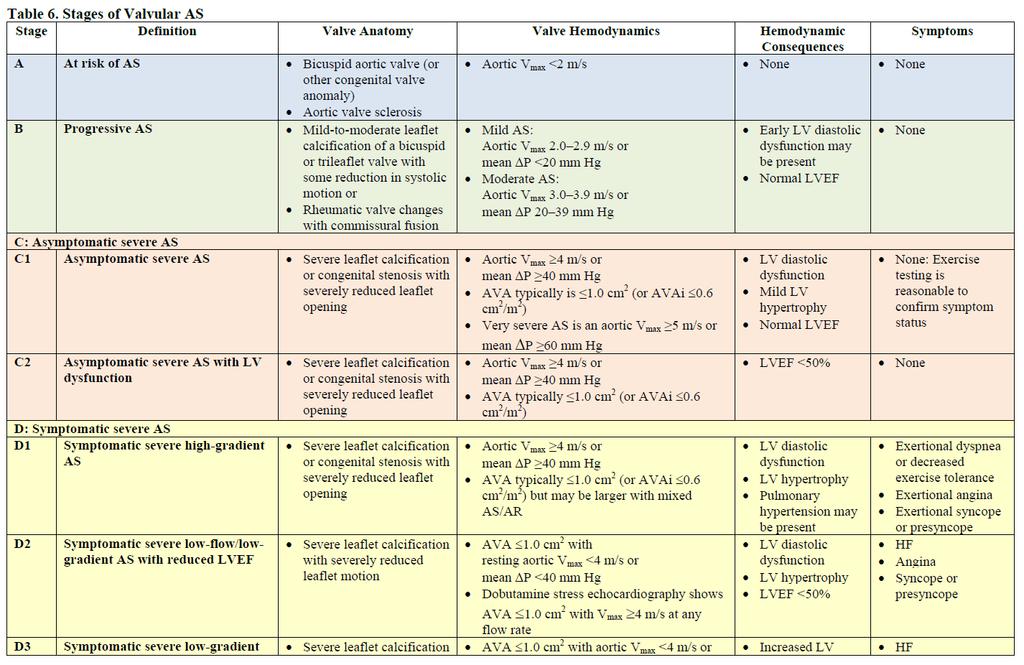
11 Natural History of Aortic Stenosis Sclerosis Valve calcification with velocity <2.5m/ sec Progression to severe AS 10% at 5 years. Once moderate disease is detected Increase in mean gradient 7 mmhg/yr Decrease in valve area of 0.1 cm^2/yr Increase velocity of 0.3 m/sec/yr

12 Aortic Stenosis



13 Aortic Stenosis Medical therapy Treat Hypertension Vasodilators Statins - Class 3
14 Aortic Stenosis Active Disease Process Lipid deposition Inflammation Neo-angiogenesis Calcification
15 The Simvastatin and Ezetemibe in Aortic Stenosis Trial (SEAS) Randomized double blind: 1873 pts Simvastatin + Zetia or Placebo Mild Moderate Aortic Stenosis Followed for average of 52 months No difference in rate of AVR or hemodynamic progression

16 Aortic Stenosis Timing of Intervention
17

18 Aortic Stenosis AVR

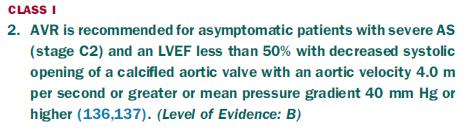
19 Asymptomatic Severe Aortic Stenosis Which patients with asymptomatic severe aortic stenosis should be considered for intervention. EF < 50 Already undergoing cardiac surgery Velocity >5m/sec, Mean gradient >60, low risk Abnormal Exercise Treadmill Fast progression on echo >0.3m/s/yr

20 Bicuspid Aortic Valve Prevalence of 0.5-2% 70-80% of cases are male Should be considered a general thoracic aortopathy.


21 Bicuspid Aortic Valve Aortopathy No medical therapy has proven to reduce the rate of progression of aortopathy associated with a bicuspid valve.


22 Bicuspid Aortic Valve Aortopathy >4.5 cm: cm: >5.5cm:



23 TAVR >50% risk of death or major morbidity at 1 year with surgery Disease affecting 3 major organ systems Anatomic factors that increase risk of surgery

24 How is risk determined?



25 Extreme Risk High Risk Higher rate of survival with TAVR at 2 years
26 Ongoing Intermediate Risk Trials PARTNER 2A SURTAVI Moderate risk Corevalve trial


27 : 3815 Consecutive patients from registry data with severe AS 300 Initial surgical Conservative 5 yr All cause death and HF hospitalization 15% - Initial surgical 26% - Conservative
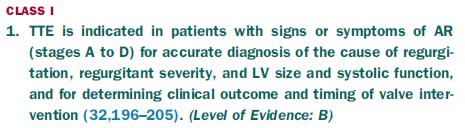
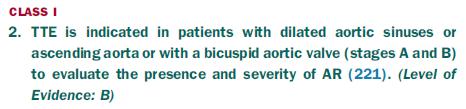
28 Aortic Insufficiency Testing
29 Aortic Insufficiency Medical Treatment

30 Aortic Insufficiency: AVR Symptomatic LV Dysfunction Undergoing surgery LV Dilation



31 Mitral Stenosis Left Atrium Natural history: Rate of progression is highly variable. Avg rate of decrease in area of 0.1cm
32
 Mitral Prolapse")
 LV")
33 Mitral Regurgitation Primary (Degenerative) Mitral Prolapse Correction of MR curative Secondary (Functional) LV dysfunction
34 Mitral Regurgitation Intervention Benefits of Mitral Repair vs. Replacement Lower operative mortality LV Function is better preserved Risks with anticoagulation Valve degeneration




35 Mitraclip EVEREST II Reduced MR Improved symptoms LV remodeling
36 Mixed Valve Disease 64yo M presents to establish care after not having a physician for the past 10 years. Reports slowly progressive exertional fatigue for the past 10 years. Echo Moderate mitral regurgitation. Moderate mitral stenosis.
37 Mixed Valve Disease Symptoms and routine treatment follow the predominant lesion Require more frequent evaluation than isolated disease of the same severity May require intervention despite the lack of severe quantification
38 Prosthetic Valves Mechanical or Bio-prosthetic How long will a bio-prosthetic valve last Inversely related to age. Deterioration rate at years 10% if age 70 90% if age 20 Individualized decision.

39 Prosthetic Valves Anticoagulation Mechanical: Thrombogenicity and alteration of flow. Aortic Valve goal INR 2.5 if low risk. Mitral Valve or AVR with higher risk goal INR 3.0. ASA 81mg for all.
40 Prosthetic Valve Bridging Anticoagulation Atrial Fibrillation Prior VTE Hypercoagulable Older Mechanical Valve EF < 30 >1 Mechanical Valve ADD Class 1 indications***
41 Mild: 3-5 years Moderate: 1-2 years Severe: 6mo to 1 year
42 Review Treatment for valve disease is becoming progressively more complex with increasing treatment options and a heart team approach is recommended for complex decisions.
43 Review Trans-catheter treatments for valve disease with TAVR or Mitra-clip are becoming more common and ongoing trials assessing utility in lower risk patients are ongoing.
44 Review Patients with moderate mixed valve disease require closer follow-up and may require intervention despite lack of severe quantification.
45 Review Bicuspid Aortic Valve should be considered a global thoracic aortopathy and imaged in its entirety with routine follow up.
46 References****pending 2008 update 2014 guideline Braunwalds Hemodynamic rounds Partner* Mitra clip trials**
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Aortic Stenosis: Background
 Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative
 Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis.
 Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
In Process, Unpublished STS/ACC TVT Registry Manuscripts
 In Process, Unpublished STS/ACC TVT Registry Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript
In Process, Unpublished STS/ACC TVT Registry Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Update on Percutaneous Therapies for Structural Heart Disease. William Thomas MD Director of Structural Heart Program Tucson Medical Center
 Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
In Process, Unpublished STS/ACC TVT Registry Manuscripts
 In Process, Unpublished STS/ACC TVT Registry Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript
In Process, Unpublished STS/ACC TVT Registry Manuscripts The following pages list current research and publications proposals that have been recently approved, are under analysis, are under manuscript
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Valvular Heart Disease Transcatheter Valve Therapies. October 2016 Brian Whisenant MD
 Valvular Heart Disease Transcatheter Valve Therapies October 2016 Brian Whisenant MD Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Valvular Heart Disease Transcatheter Valve Therapies October 2016 Brian Whisenant MD Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Prognostic Impact of FMR
 Secondary Mitral Valve Regurgitation in Heart Failure, Age 60 Years From Medical Therapy to Surgical Repair to Transcatheter Intervention The Interventionalist s View Samin K Sharma, MD, FACC, FSCAI Director
Secondary Mitral Valve Regurgitation in Heart Failure, Age 60 Years From Medical Therapy to Surgical Repair to Transcatheter Intervention The Interventionalist s View Samin K Sharma, MD, FACC, FSCAI Director
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC
 TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Transcatheter Valve Replacement: Current State in 2017
 Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD
 2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute
 Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Cardiac Valve/Structural Therapies
 Property of Dr. Chad Rammohan Cardiac Valve/Structural Therapies Chad Rammohan, MD FACC Medical Director, El Camino Hospital Cardiac Catheterization Lab Director, Interventional and Structural Cardiology,
Property of Dr. Chad Rammohan Cardiac Valve/Structural Therapies Chad Rammohan, MD FACC Medical Director, El Camino Hospital Cardiac Catheterization Lab Director, Interventional and Structural Cardiology,
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
New Imaging for Aortic Valve Disease. Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego
 New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Gender Differences in Valvular Heart Disease. Linda D. Gillam, MD FESC Disclosure: Core Lab services Edwards Lifesciences
 Gender Differences in Valvular Heart Disease Linda D. Gillam, MD FESC Disclosure: Core Lab services Edwards Lifesciences Obstacles Interest in gender differences is a relatively new phenomenon Registries/RCT
Gender Differences in Valvular Heart Disease Linda D. Gillam, MD FESC Disclosure: Core Lab services Edwards Lifesciences Obstacles Interest in gender differences is a relatively new phenomenon Registries/RCT
Welcome 17 Michigan TAVR Participating Hospitals!
 Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Cardiac catheterisation in AS
 AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Watchman and Structural update..the next frontier. Ari Chanda, MD Cardiology Associates of Fredericksburg
 Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
Watchman and Structural update..the next frontier Ari Chanda, MD Cardiology Associates of Fredericksburg Different Left Atrial Appendage (LAA) morphologies Watchman (the device) Fabric Anchors Device structure
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Mitral Regurgitation:
 Mitral Regurgitation: Diagnosis and Treatment 2018 Annual Chattanooga Cardiology Symposium 10 February, 2018 Allen E. Atchley, MD Disclosures None Objectives: 1. Understand functional vs. degenerative
Mitral Regurgitation: Diagnosis and Treatment 2018 Annual Chattanooga Cardiology Symposium 10 February, 2018 Allen E. Atchley, MD Disclosures None Objectives: 1. Understand functional vs. degenerative
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
2/4/2019. Nursing Perspective of TAVR. Disclosure. Learning Outcomes
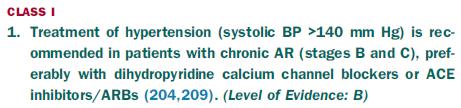
 Nursing Perspective of TAVR Tara Whitmire, DNP, APRN-NP, NP-C, CHFN Nebraska Methodist Hospital Cardiothoracic Surgery Nurse Practitioner Danelle Homeyer, RN Methodist Physicians Clinic Director, Structural
Nursing Perspective of TAVR Tara Whitmire, DNP, APRN-NP, NP-C, CHFN Nebraska Methodist Hospital Cardiothoracic Surgery Nurse Practitioner Danelle Homeyer, RN Methodist Physicians Clinic Director, Structural
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL
 PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives. Bernard Iung Bichat Hospital, Paris
 Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
TAVR: Intermediate Risk Patients
 TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
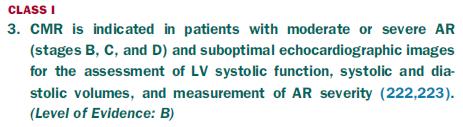
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
I (312) Mitral Regurgitation What Should You Know?
 Mitral Regurgitation What Should You Know?") Mitral Regurgitation What Should You Know? Table of Contents What is Mitral Regurgitation? 3 What are the Symptoms? 4 What are the risks? 5 Who Gets Mitral Regurgitation? 6 Diagnosing Mitral Regurgitation
Mitral Regurgitation What Should You Know? Table of Contents What is Mitral Regurgitation? 3 What are the Symptoms? 4 What are the risks? 5 Who Gets Mitral Regurgitation? 6 Diagnosing Mitral Regurgitation
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification. Rheumatic Mitral Stenosis 76yo male
 MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
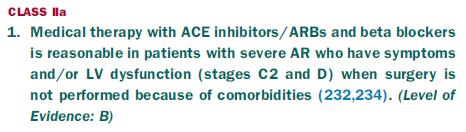
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
 Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Percutaneous Management of Severe AS in Octagenarians. Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington
 Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease
 2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
Next Generation Therapies: Aortic, Mitral and Beyond
 Next Generation Therapies: Aortic, Mitral and Beyond Scott M Lilly, MD PhD Medical (Interventional) Director, Structural Heart Program Heart Summit, Lima OH August 26 th, 2017 Next Generation Therapies:
Next Generation Therapies: Aortic, Mitral and Beyond Scott M Lilly, MD PhD Medical (Interventional) Director, Structural Heart Program Heart Summit, Lima OH August 26 th, 2017 Next Generation Therapies:
Etiology of Valvular Heart Disease in the 21 st Century
 Etiology of Valvular Heart Disease in the 21 st Century Genetic and Molecular Mechanisms Harisios Boudoulas, MD, Dr, Dr Hon. Professor, Academician (ant. mem.) The Ohio State University, USA Biomedical
Etiology of Valvular Heart Disease in the 21 st Century Genetic and Molecular Mechanisms Harisios Boudoulas, MD, Dr, Dr Hon. Professor, Academician (ant. mem.) The Ohio State University, USA Biomedical
Menachem M. Weiner Assistant Professor of Anesthesiology Icahn School of Medicine at Mount Sinai
 Menachem M. Weiner Assistant Professor of Anesthesiology Icahn School of Medicine at Mount Sinai Anesthetic care and considerations Intraoperative events TEE Perioperative complications Most common valvular
Menachem M. Weiner Assistant Professor of Anesthesiology Icahn School of Medicine at Mount Sinai Anesthetic care and considerations Intraoperative events TEE Perioperative complications Most common valvular
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
Integrating Innovative Technologies into the Care of Cardiac Patients
 Integrating Innovative Technologies into the Care of Cardiac Patients Marc J. Semigran MD Medical Director, Heart Failure & Cardiac Transplantation MGH Associate Professor Harvard Medical School Presenter
Integrating Innovative Technologies into the Care of Cardiac Patients Marc J. Semigran MD Medical Director, Heart Failure & Cardiac Transplantation MGH Associate Professor Harvard Medical School Presenter
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Unusual Causes of Aortic Regurgitation. Case 1
 Unusual Causes of Aortic Regurgitation Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA No Disclosures Case 1 54 year old female with h/o cerebral aneurysm and vascular malformation
Unusual Causes of Aortic Regurgitation Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA No Disclosures Case 1 54 year old female with h/o cerebral aneurysm and vascular malformation
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine
 Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Aortic stenosis and regurgitation
 1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
The Tricuspid Valve: The Not So Forgotten Valve. Manuel J Antunes Cardiothoracic Surgery Coimbra, Portugal
 The Tricuspid Valve: The Not So Forgotten Valve Manuel J Antunes Cardiothoracic Surgery Coimbra, Portugal No Conflicts of Interest to declare with regards to this subject 2 INCIDENCE OF TRICUSPID REGURGITATION
The Tricuspid Valve: The Not So Forgotten Valve Manuel J Antunes Cardiothoracic Surgery Coimbra, Portugal No Conflicts of Interest to declare with regards to this subject 2 INCIDENCE OF TRICUSPID REGURGITATION
Transcatheter Valve Therapies Update
 Providence Heart and Vascular Institute Transcatheter Valve Therapies Update Where In The H*@# Is All This Going??? Robert Hodson MD Medical Director, Providence Valve Center October 24, 2015 DISCLOSURES
Providence Heart and Vascular Institute Transcatheter Valve Therapies Update Where In The H*@# Is All This Going??? Robert Hodson MD Medical Director, Providence Valve Center October 24, 2015 DISCLOSURES
Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications
 24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
24th Annual Advances in Heart Disease 16 December 2007 Long-Term Outcome of Patients With Aortic Regurgitation: Medical Management and Surgical Indications Melvin D. Cheitlin, M.D. Emeritus Professor of
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
Alec Vahanian,FESC, FRCP (Edin.) Bichat Hospital University Paris VII, Paris, France
 Bichat Hospital University Paris VII, Paris, France") Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI
 Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
Prof. Dr. Thomas Walther. TAVI in ascending aorta / aortic root dilatation
 Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Policy Specific Section: March 30, 2012 March 7, 2013
 Medical Policy Transcatheter Aortic Valve Replacement for Aortic Stenosis Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date:
Medical Policy Transcatheter Aortic Valve Replacement for Aortic Stenosis Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date:
Culprit vs Multivalve Transcatheter Intervention
 Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
Valvular Heart Disease and Adult Congenital Intervention. A Pichard, MD. Director Cath Labs, Washington Hospital Center. Georgetown University.
 Valvular Heart Disease and Adult Congenital Intervention. A Pichard, MD Director Cath Labs, Washington Hospital Center. ProfessorofMedicine (Cardiology), Georgetown University. Conflict of Interest Proctor
Valvular Heart Disease and Adult Congenital Intervention. A Pichard, MD Director Cath Labs, Washington Hospital Center. ProfessorofMedicine (Cardiology), Georgetown University. Conflict of Interest Proctor
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong
 Pol.Col.Dr.Kasem Ratanasumawong") Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
DISCLOSURE. Mitral ViV: why? Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? UW Medicine NONE.
 Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Valvular heart disease (VHD) is present in 2.5% of the
 is present in 2.5% of the") 2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
TAVI and Valve Replacement Thromboprophylaxis. Warren Prokopiw Pharmacy Resident
 TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
Mitral Regurgitation
 Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
Percutaneous Mitral Valve Repair
 Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F.
 Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Transcatheter Mitral Valve Replacement How Close Are We?
 Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S.
 ACC 2015 LBCT Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S. A report from the STS/ACC TVT Registry Paul Sorajja, MD, Saibal Kar, MD, Amanda Stebbins,
ACC 2015 LBCT Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S. A report from the STS/ACC TVT Registry Paul Sorajja, MD, Saibal Kar, MD, Amanda Stebbins,
The Worshipful Company of Barbers. Mr. John Hunter. History of cardiac surgery. PDA ligation. Blalock-Taussig Shunt
 The Worshipful Company of Barbers Puneet Dhawan M.D Assistant Health Sciences Clinical Professor David Geffen School of Medicine at UCLA Assistant Chief Division of Cardiothoracic Surgery Harbor-UCLA Medical
The Worshipful Company of Barbers Puneet Dhawan M.D Assistant Health Sciences Clinical Professor David Geffen School of Medicine at UCLA Assistant Chief Division of Cardiothoracic Surgery Harbor-UCLA Medical
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center
Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center") The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
Valvular defects. Lectures from Pathological Physiology. Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková
 Valvular defects Lectures from Pathological Physiology Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková 1 2 3 1 Valvular dysfunction - introduction Stenosis block of flow;
Valvular defects Lectures from Pathological Physiology Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková 1 2 3 1 Valvular dysfunction - introduction Stenosis block of flow;