Cardiology. the Sounds: #7 HCM. LV Outflow Obstruction: Aortic Stenosis. (Coming Soon - HCM)
|
|
|
- Annabelle Powers
- 5 years ago
- Views:
Transcription

1 A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD Howard@12daysinmarch.com
2 Aortic Valve Disorders Stenosis Regurgitation
3 Aortic Valve Disorders Stenosis Location: RUSB (base) carotids Systolic Quality: crescendo-decrescendo Key points: Associated with congenital bicusp (TS) Obstructive physiology LVH Afterload (prototypical) Do Not Confuse: HCM Very noisy when ventricle contracts
4 LV Outflow Obstruction AS RUSB Base of Heart Ao LSB Chronic AI HCM VSD
5 AS RUSB Base of Heart Ao LSB Apex
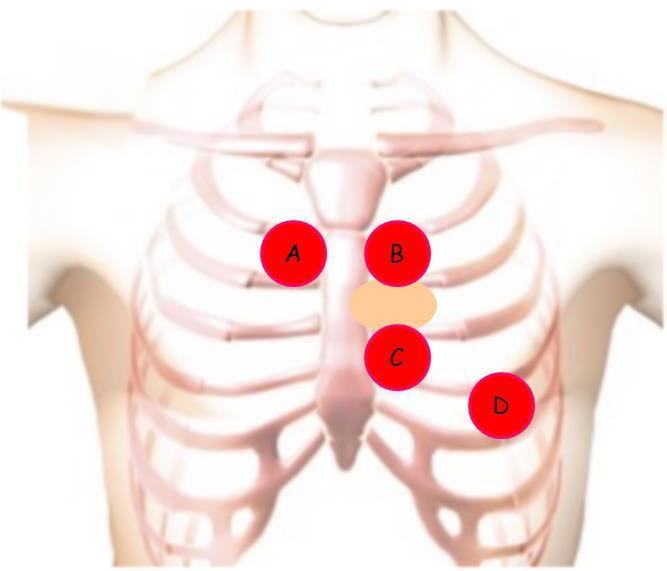

6 Ao LSB
7 Aortic Valve Disorders Stenosis Location: RUSB (base) carotids Systolic Quality: crescendo-decrescendo Key points: Associated with congenital bicusp (TS) Rapid Ejection Obstructive physiology LVH Afterload (prototypical) Do Not Confuse: HCM
8 Aortic Valve Disorders Stenosis Location: RUSB (base) carotids Systolic Quality: crescendo-decrescendo Key points: Associated with congenital bicusp (TS) Rapid Ejection Obstructive physiology LVH Afterload (prototypical) Do Not Confuse: HCM
 Normal intensity of S2 Obstructive physiology LVH Afterload (prototypical) Do Not Confuse: HCM Non-Critical")
9 Aortic Valve Disorders Stenosis Location: RUSB (base) carotids Systolic Quality: crescendo-decrescendo Failure to radiate to the carotids Key points: AND Associated with congenital bicusp (TS) Normal intensity of S2 Obstructive physiology LVH Afterload (prototypical) Do Not Confuse: HCM Non-Critical AS
10 Aortic Valve Disorders Stenosis Location: RUSB (base) carotids Systolic Quality: crescendo-decrescendo Key points: Associated with congenital bicusp (TS) Obstructive Black Box physiology Warning: LVH Afterload (prototypical) The NBME assumes you can Do identify Not Confuse: the murmur. HCM It is a rare question that asks you to name the murmur. They present the abnormal physical exam and then launch derivatives.
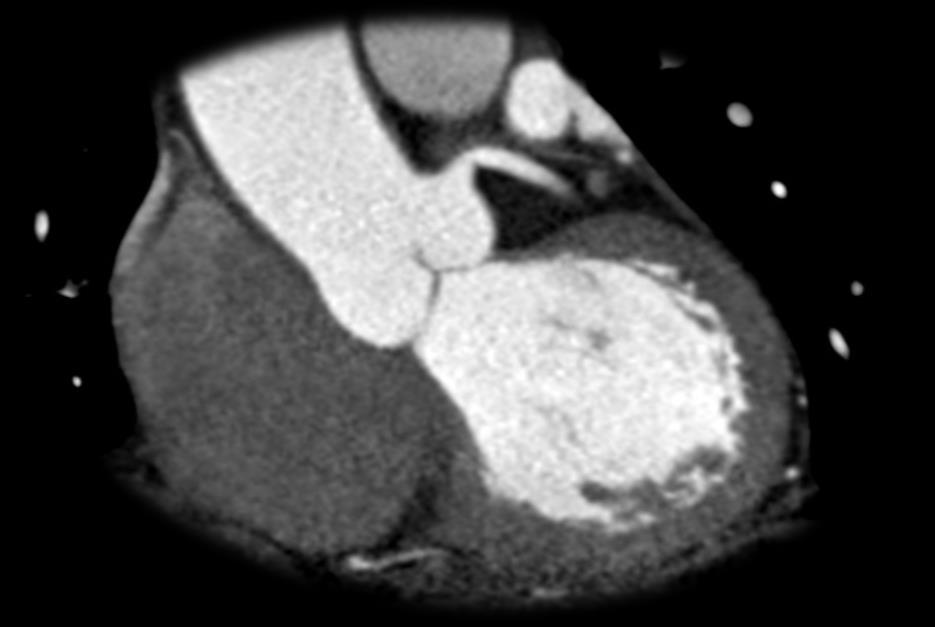
11 Aortic Valve Disorders Stenosis Location: RUSB (base) carotids Systolic Quality: crescendo-decrescendo Key points: Associated with congenital bicusp (TS) Obstructive physiology LVH Afterload (prototypical) Do Not Confuse: HCM Concentric Hypertrophy
12 Aortic Valve Disorders Stenosis Location: RUSB (base) carotids Systolic Quality: crescendo-decrescendo Key points: Associated with congenital bicusp (TS) Obstructive physiology LVH Afterload (prototypical) Do Not Confuse: HCM
13 ~ Aortic Stenosis Hemodynamics I ~ Pressure Ao Close ESV Increased Afterload Isovolumetric Relaxation Isovolumetric Contraction Stroke Volume MV Open Rapid Filling MV Close Low Hg, Hi Vol EDV SV = EDV - ESV Volume
14 Pressure Pressure Volume Volume
15 ~ Aortic Stenosis Hemodynamics I ~ Pressure Ao Close ESV Increased Afterload Increased LV pressure to overcome valve R (not Ao mm Hg) Isovolumetric Relaxation Stroke Volume MV Open Rapid Filling MV Close SV = EDV - ESV Volume
16 ~ Aortic Stenosis Hemodynamics I ~ Ao Close ESV Increased Afterload Pressure Isovolumetric Relaxation Stroke Volume SV 2 to: Decreased velocity of sarcomere shortening Decreased distance shortened MV Open Rapid Filling MV Close SV = EDV - ESV Volume
17 ~ Aortic Stenosis Hemodynamics I ~ Ao Close ESV Increased Afterload Pressure Stroke Volume Cardiac work = SV x afterload Cardiac work = SV x mm Hg BP major determinant of cardiac work MV Open Rapid Filling MV Close Volume
18 ~ Aortic Stenosis Hemodynamics I ~ Ao Close ESV Increased Afterload Pressure Stroke Volume In spite of SV, the cardiac work and myocardial oxygen demand increases Cardiac work = SV x afterload Cardiac work = SV x mm Hg BP major determinant of cardiac work MV Open Rapid Filling MV Close Volume
19 Increased Afterload (AS) Decreased velocity of shortening Decreased distance shortened Decreased SV Increased cardiac work Increased myocardial oxygen consumption Aortic Stenosis Malignant HTN
20 Compare and Contrast Increased Afterload (AS) Decreased velocity of shortening Decreased distance shortened Decreased SV Increased cardiac work Increased myocardial oxygen consumption Decreased Afterload (Nitroprusside) Treatment of Choice for Malignant HTN (on Step One)

21 Compare and Contrast Decreased Afterload (Nitroprusside) Increased Afterload (AS) Decreased velocity of shortening Decreased distance shortened Decreased SV Increased cardiac work Increased myocardial oxygen consumption
22 Compare and Contrast Increased Afterload (AS) Decreased velocity of shortening Decreased distance shortened Decreased SV Increased cardiac work Increased myocardial oxygen consumption Decreased Afterload (Nitroprusside)
23 Aortic Stenosis Hemodynamics II 120 AV Open AV Close 80 Isovol Cont Rapid eject Isovol Relax LV Pressure Rapid filling 10 MV Close MV Open What happens to the LV mm Hg curve with aortic stenosis? LV pressure has to surpass resistance of the stenotic valve.
24 Aortic Stenosis Hemodynamics II AV Open 120 AV Close 80 Isovol Cont Isovol Relax 10 MV Close MV Open Rapid filling What happens to the LV mm Hg curve with aortic stenosis? LV pressure has to surpass resistance of the stenotic valve.
25 Aortic Stenosis Hemodynamics II Rapid ejection Crescendo Decrescendo 120 AV Close 80 Isovol Cont Isovol Relax 10 MV Close MV Open Rapid filling
26 Aortic Stenosis Hemodynamics II Rapid ejection Crescendo Decrescendo 120 AV Close 80 Isovol Cont Isovol Relax 10 MV Close MV Open Rapid filling What happens to the LV mm Hg curve with aortic stenosis? LV pressure has to increase (surpassing Ao Hg) to open stenotic valve. Peak murmur intensity?
27 Symptoms SCD Angina Syncope CHF Symptoms Angina Where are the coronary ostia located?

28 Symptoms SCD Angina Syncope CHF Symptoms Angina Where are the coronary ostia located?: Above aortic valve
29 Symptoms Angina Where are the coronary ostia?: Above aortic valve Symptoms SCD Angina Syncope CHF Symptoms Syncope* Obstructive basis. If they describe a patient with systolic murmur and syncope* how will you * distinguish may be described between by AS LH and or dizziness HCM?
30 Symptoms Angina Where are the coronary ostia?: Above aortic valve Symptoms SCD Angina Syncope CHF Symptoms Syncope Obstructive basis. If they describe a patient with systolic murmur and syncope how will you distinguish between AS and HCM?
31 Symptoms SCD Angina Syncope CHF Symptoms Syncope Obstructive basis. If they describe a patient with systolic murmur and syncope, how will you distinguish between AS and HCM? HCM: FH SCD, young age/athlete, dysrhythmia, maneuvers (PE and cath lab), pathology AS: older (unless bicusp), maneuvers not reliable, quality/location of murmur What They Tell You, What They Don t Tell You
32 Symptoms SCD Angina Syncope CHF CHF Increased afterload Eventual Cardiac Decompensation

33 CHF Increased afterload Eventual Cardiac Decompensation Atrial Fibrillation and Aortic Stenosis Symptoms SCD Angina Syncope CHF Complications: CHF Ischemia Preload Pulmonary Venous Congestion Fast heart rate less time in diastole Diastolic Filling of Coronary Vessels
34 Aortic Stenosis Symptoms SCD Angina Syncope CHF They use the signs and symptoms of aortic stenosis as a gateway condition to a number of loosely associated derivatives



35 Black Box Warning: The NBME assumes you can identify the murmur. They present the abnormal physical exam and then launch derivatives.
36 Aortic Stenosis: Pathology XO Raphe Dystrophic calcification Who gets AS (demographic description on Step One)? Aged degenerative; dystrophic calcification ~ Young or Turner syndrome with congenital bicusp ~ ~ Rheumatic Fever, late manifestation ~
?")

37 Aortic Stenosis: Pathology XO Raphe Dystrophic calcification Who gets AS (demographic description on Step One)? Aged degenerative; dystrophic calcification ~ Young or Turner syndrome with congenital bicusp ~ ~ Rheumatic Fever, late manifestation ~
 Normal")


38 LVH: complication of pressure overload (AS, HTN) Normal myocardium Wall Stress = P x r/2h h wall thickness Thick wall, Low stress Thicker Concentric Hypertrophy (adaptive: wall stress)


39 Carotids Ao Loud and systolic: ventricular contraction RUSB Stethoscope placed here is likely AS They will ask derivatives (pathology, hemodynamics, etc)
40 Aortic Stenosis Demographic Elderly Young patient with congenital bicusp (and/or Turner s) Late complication of rheumatic fever Physical Exam RUSB/base Crescendo-Decrescendo systolic murmur Radiating to carotids Severity affects intensity of S 2 Hemodynamics Increased afterload: derivatives and the pressure-volume curve Compare and contrast with the decreased afterload curve Cardiac cycle curve: peak murmur intensity Pathology Dystrophic calcification of the elderly Fusion of the commissure in the congenital bicusp Complications/Presentation Concentric LVH SCD, Angina, Syncope, CHF
41 A Cardiology HCM LV OutFlow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD Howard@12daysinmarch.com
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Cardiac Output MCQ. Professor of Cardiovascular Physiology. Cairo University 2007
 Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
Cardiac Cycle MCQ. Professor of Cardiovascular Physiology. Cairo University 2007
 Cardiac Cycle MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 1- Regarding the length of systole and diastole: a- At heart rate 75 b/min, the duration of
Cardiac Cycle MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 1- Regarding the length of systole and diastole: a- At heart rate 75 b/min, the duration of
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Physical Exam Part II
 Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
BUSINESS. Articles? Grades Midterm Review session
 BUSINESS Articles? Grades Midterm Review session REVIEW Cardiac cells Myogenic cells Properties of contractile cells CONDUCTION SYSTEM OF THE HEART Conduction pathway SA node (pacemaker) atrial depolarization
BUSINESS Articles? Grades Midterm Review session REVIEW Cardiac cells Myogenic cells Properties of contractile cells CONDUCTION SYSTEM OF THE HEART Conduction pathway SA node (pacemaker) atrial depolarization
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload Cardiac output (CO) represents the volume of blood that is delivered
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #12 Understanding Preload and Afterload Cardiac output (CO) represents the volume of blood that is delivered
Cardiac Issues in the Adolescent Athlete. Sean Levchuck, M.D. St. Francis Hospital- The Heart Center
 Cardiac Issues in the Adolescent Athlete Sean Levchuck, M.D. St. Francis Hospital- The Heart Center Sudden Cardiac Death Incidence is.6-6.2 % per 100,000 children in the US 20-25 % of the deaths occur
Cardiac Issues in the Adolescent Athlete Sean Levchuck, M.D. St. Francis Hospital- The Heart Center Sudden Cardiac Death Incidence is.6-6.2 % per 100,000 children in the US 20-25 % of the deaths occur
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Pulmonary-Vascular Disease. Howard J. Sachs, MD.
 Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
IP: Regulation of Cardiac Output
 ANP 1105D Winter 2013 Assignment 9: The Heart, part 2: Chap... Assignment 9: The Heart, part 2: Chapter 18 Signed in as Alex Sokolowski Help Close Resources Due: 11:59pm on Monday, March 25, 2013 Note:
ANP 1105D Winter 2013 Assignment 9: The Heart, part 2: Chap... Assignment 9: The Heart, part 2: Chapter 18 Signed in as Alex Sokolowski Help Close Resources Due: 11:59pm on Monday, March 25, 2013 Note:
Cardiovascular Structure & Function
 Cardiovascular Structure & Function Cardiovascular system: The heart Arteries Veins Capillaries Lymphatic vessels Weighting of the heart ceremony: Ancient Egyptians William Harvey and Blood Flow April
Cardiovascular Structure & Function Cardiovascular system: The heart Arteries Veins Capillaries Lymphatic vessels Weighting of the heart ceremony: Ancient Egyptians William Harvey and Blood Flow April
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Cardiovascular Physiology. Heart Physiology. Introduction. The heart. Electrophysiology of the heart
 Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
Cardiovascular Physiology Heart Physiology Introduction The cardiovascular system consists of the heart and two vascular systems, the systemic and pulmonary circulations. The heart pumps blood through
Heart sounds and murmurs. Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct
 Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Heart Pump and Cardiac Cycle. Faisal I. Mohammed, MD, PhD
 Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
Mitral Valve Disease. Prof. Sirchak Yelizaveta Stepanovna
 Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
SymBioSys Exercise 2 Cardiac Function Revised and reformatted by C. S. Tritt, Ph.D. Last updated March 20, 2006
 SymBioSys Exercise 2 Cardiac Function Revised and reformatted by C. S. Tritt, Ph.D. Last updated March 20, 2006 The goal of this exercise to explore the behavior of the heart as a mechanical pump. For
SymBioSys Exercise 2 Cardiac Function Revised and reformatted by C. S. Tritt, Ph.D. Last updated March 20, 2006 The goal of this exercise to explore the behavior of the heart as a mechanical pump. For
See below for descriptions of the waveform
 The internal jugular vein (IJV) connects to the right atrium without any intervening valves. The pulsation of the right atrium therefore causes the column of blood in the IJV to rise and fall this is called
The internal jugular vein (IJV) connects to the right atrium without any intervening valves. The pulsation of the right atrium therefore causes the column of blood in the IJV to rise and fall this is called
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center
 Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Collin County Community College
 Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 5 The Heart 1 The Heart Beat and the EKG 2 1 The Heart Beat and the EKG P-wave = Atrial depolarization QRS-wave = Ventricular depolarization
Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 5 The Heart 1 The Heart Beat and the EKG 2 1 The Heart Beat and the EKG P-wave = Atrial depolarization QRS-wave = Ventricular depolarization
Cardiac Ausculation in the Elderly
 Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
THE CARDIOVASCULAR SYSTEM
 THE CARDIOVASCULAR SYSTEM AND RESPONSES TO EXERCISE Mr. S. Kelly PSK 4U North Grenville DHS THE HEART: A REVIEW Cardiac muscle = myocardium Heart divided into two sides, 4 chambers (L & R) RS: pulmonary
THE CARDIOVASCULAR SYSTEM AND RESPONSES TO EXERCISE Mr. S. Kelly PSK 4U North Grenville DHS THE HEART: A REVIEW Cardiac muscle = myocardium Heart divided into two sides, 4 chambers (L & R) RS: pulmonary
The Cardiovascular System
 The Cardiovascular System The Cardiovascular System A closed system of the heart and blood vessels The heart pumps blood Blood vessels allow blood to circulate to all parts of the body The function of
The Cardiovascular System The Cardiovascular System A closed system of the heart and blood vessels The heart pumps blood Blood vessels allow blood to circulate to all parts of the body The function of
THE CARDIOVASCULAR SYSTEM. Heart 2
 THE CARDIOVASCULAR SYSTEM Heart 2 PROPERTIES OF CARDIAC MUSCLE Cardiac muscle Striated Short Wide Branched Interconnected Skeletal muscle Striated Long Narrow Cylindrical PROPERTIES OF CARDIAC MUSCLE Intercalated
THE CARDIOVASCULAR SYSTEM Heart 2 PROPERTIES OF CARDIAC MUSCLE Cardiac muscle Striated Short Wide Branched Interconnected Skeletal muscle Striated Long Narrow Cylindrical PROPERTIES OF CARDIAC MUSCLE Intercalated
Chapter 13 The Cardiovascular System: Cardiac Function
 Chapter 13 The Cardiovascular System: Cardiac Function Overview of the Cardiovascular System The Path of Blood Flow through the Heart and Vasculature Anatomy of the Heart Electrical Activity of the Heart
Chapter 13 The Cardiovascular System: Cardiac Function Overview of the Cardiovascular System The Path of Blood Flow through the Heart and Vasculature Anatomy of the Heart Electrical Activity of the Heart
SIKLUS JANTUNG. Rahmatina B. Herman
 SIKLUS JANTUNG Rahmatina B. Herman The Cardiac Cycle Definition: The cardiac events that occur from the beginning of one heartbeat to the beginning of the next The cardiac cycle consists of: - Diastole
SIKLUS JANTUNG Rahmatina B. Herman The Cardiac Cycle Definition: The cardiac events that occur from the beginning of one heartbeat to the beginning of the next The cardiac cycle consists of: - Diastole
Hemodynamics of Exercise
 Hemodynamics of Exercise Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH, STVAHCS Exercise Physiology - Acute Effects Cardiac Output (Stroke volume, Heart Rate ) Oxygen Extraction (Arteriovenous O 2 difference,
Hemodynamics of Exercise Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH, STVAHCS Exercise Physiology - Acute Effects Cardiac Output (Stroke volume, Heart Rate ) Oxygen Extraction (Arteriovenous O 2 difference,
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
For more information about how to cite these materials visit
 Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Managing Hypertrophic Cardiomyopathy with Imaging. Gisela C. Mueller University of Michigan Department of Radiology
 Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery
 Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Practice Exercises for the Cardiovascular System
 Practice Exercises for the Cardiovascular System On the diagram below, color the oxygen-rich blood red and the oxygen-poor blood blue. Label the parts: Continued on the next page... Label the parts on
Practice Exercises for the Cardiovascular System On the diagram below, color the oxygen-rich blood red and the oxygen-poor blood blue. Label the parts: Continued on the next page... Label the parts on
-12. -Ensherah Mokheemer - ABDULLAH ZREQAT. -Faisal Mohammad. 1 P a g e
 -12 -Ensherah Mokheemer - ABDULLAH ZREQAT -Faisal Mohammad 1 P a g e In the previous lecture we talked about: - cardiac index: we use the cardiac index to compare the cardiac output between different individuals,
-12 -Ensherah Mokheemer - ABDULLAH ZREQAT -Faisal Mohammad 1 P a g e In the previous lecture we talked about: - cardiac index: we use the cardiac index to compare the cardiac output between different individuals,
By the end of this session, the student should be able to:
 Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
The Heart. Happy Friday! #takeoutyournotes #testnotgradedyet
 The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
Coronary Anomalies & Hemodynamic Identification
 Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.
Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.
Age-related changes in cardiovascular system. Dr. Rehab Gwada
 Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results
Age-related changes in cardiovascular system Dr. Rehab Gwada Objectives explain the main structural and functional changes in cardiovascular system associated with normal aging Introduction aging results
Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009
 www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers MANAGEMENT
www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers MANAGEMENT
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
CARDIOVASCULAR PHYSIOLOGY
 CARDIOVASCULAR PHYSIOLOGY LECTURE 4 Cardiac cycle Polygram - analysis of cardiac activity Ana-Maria Zagrean MD, PhD The Cardiac Cycle - definitions: the sequence of electrical and mechanical events that
CARDIOVASCULAR PHYSIOLOGY LECTURE 4 Cardiac cycle Polygram - analysis of cardiac activity Ana-Maria Zagrean MD, PhD The Cardiac Cycle - definitions: the sequence of electrical and mechanical events that
Hemodynamics: Cardiac and Vascular Jeff Davis, RRT, RCIS
 Hemodynamics: Cardiac and Vascular Jeff Davis, RRT, RCIS Program Director, Cardiovascular Technology Florida SouthWestern State College Fort Myers, FL Disclosures Speaker s Bureau: None Stockholder: None
Hemodynamics: Cardiac and Vascular Jeff Davis, RRT, RCIS Program Director, Cardiovascular Technology Florida SouthWestern State College Fort Myers, FL Disclosures Speaker s Bureau: None Stockholder: None
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE. Karen Stout, MD University of Washington Seattle Children s Seattle, WA
 EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
EVALUATION OF PREGNANT PATIENTS WITH HEART DISEASE Karen Stout, MD University of Washington Seattle Children s Seattle, WA CASE PRESENTATION 24 year old woman with aortic regurgitation referred for evaluation
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Lab 16. The Cardiovascular System Heart and Blood Vessels. Laboratory Objectives
 Lab 16 The Cardiovascular System Heart and Blood Vessels Laboratory Objectives Describe the anatomical structures of the heart to include the pericardium, chambers, valves, and major vessels. Describe
Lab 16 The Cardiovascular System Heart and Blood Vessels Laboratory Objectives Describe the anatomical structures of the heart to include the pericardium, chambers, valves, and major vessels. Describe
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
CONGENITAL AORTIC STENOSIS PRODUCED BY A UNICOMMISSURAL VALVE
 Brit. Heart J., 1965, 27, 505. CONGENITAL AORTIC STENOSIS PRODUCED BY A UNICOMMISSURAL VALVE WILLIAM C. BY ROBERTS AND ANDREW G. MORROW From the Clinic of Surgery, National Heart Institute, National Institutes
Brit. Heart J., 1965, 27, 505. CONGENITAL AORTIC STENOSIS PRODUCED BY A UNICOMMISSURAL VALVE WILLIAM C. BY ROBERTS AND ANDREW G. MORROW From the Clinic of Surgery, National Heart Institute, National Institutes
Etiology, Classification & Management. Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London
 Etiology, Classification & Management Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London Introduction World Health Organization (1995): Diseases of myocardium (heart
Etiology, Classification & Management Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London Introduction World Health Organization (1995): Diseases of myocardium (heart
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Section V VALVULAR HEART T DISEASE. Chapter 27 Aortic Stenosis Chapter 28 Aortic Insufficiency Chapter 29 Mitral Valve Disease...
 Section V VALVULAR HEART T DISEASE Chapter 27 Aortic Stenosis........................... 256 Chapter 28 Aortic Insufficiency....................... 265 Chapter 29 Mitral Valve Disease......................
Section V VALVULAR HEART T DISEASE Chapter 27 Aortic Stenosis........................... 256 Chapter 28 Aortic Insufficiency....................... 265 Chapter 29 Mitral Valve Disease......................
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to:
 The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
COLIC AND MURMURS: AN OVERVIEW
 COLIC AND MURMURS: AN OVERVIEW Gunther van Loon, DVM, PhD, Department of Large Animal Internal Medicine, Ghent University, Merelbeke, Belgium Introduction Many horses with colic present with a cardiac
COLIC AND MURMURS: AN OVERVIEW Gunther van Loon, DVM, PhD, Department of Large Animal Internal Medicine, Ghent University, Merelbeke, Belgium Introduction Many horses with colic present with a cardiac
For more information about how to cite these materials visit
 Author(s): Louis D Alecy, D.M.D., Ph.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License:
Author(s): Louis D Alecy, D.M.D., Ph.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License:
TOP 10 TAKEAWAYS. Jane A. Linderbaum MS, APRN, CNP, AACC Assistant Professor of Medicine Department of cardiovascular disease
 TOP 10 TAKEAWAYS Jane A. Linderbaum MS, APRN, CNP, AACC Assistant Professor of Medicine Department of cardiovascular disease No Disclosures No off-label discussions 73% of survey respondents identified
TOP 10 TAKEAWAYS Jane A. Linderbaum MS, APRN, CNP, AACC Assistant Professor of Medicine Department of cardiovascular disease No Disclosures No off-label discussions 73% of survey respondents identified
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
A Health Care Professional s Guide Aortic Stenosis in Seniors
 A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
The Cardiac Cycle Clive M. Baumgarten, Ph.D.
 The Cardiac Cycle Clive M. Baumgarten, Ph.D. OBJECTIVES: 1. Describe periods comprising cardiac cycle and events within each period 2. Describe the temporal relationships between pressure, blood flow,
The Cardiac Cycle Clive M. Baumgarten, Ph.D. OBJECTIVES: 1. Describe periods comprising cardiac cycle and events within each period 2. Describe the temporal relationships between pressure, blood flow,
Cardiac output and Venous Return. Faisal I. Mohammed, MD, PhD
 Cardiac output and Venous Return Faisal I. Mohammed, MD, PhD 1 Objectives Define cardiac output and venous return Describe the methods of measurement of CO Outline the factors that regulate cardiac output
Cardiac output and Venous Return Faisal I. Mohammed, MD, PhD 1 Objectives Define cardiac output and venous return Describe the methods of measurement of CO Outline the factors that regulate cardiac output
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY
 OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
Valvular Stenosis and Regurgitation: Barriers to Flow
 Valvular Stenosis and Regurgitation: Barriers to Flow Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com CNEA 2009 1 Cardiac Valves Prevent Backward Flow Permit Forward Flow 2 www.cardionursing.com
Valvular Stenosis and Regurgitation: Barriers to Flow Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com CNEA 2009 1 Cardiac Valves Prevent Backward Flow Permit Forward Flow 2 www.cardionursing.com
Electrical Conduction
 Sinoatrial (SA) node Electrical Conduction Sets the pace of the heartbeat at 70 bpm AV node (50 bpm) and Purkinje fibers (25 40 bpm) can act as pacemakers under some conditions Internodal pathway from
Sinoatrial (SA) node Electrical Conduction Sets the pace of the heartbeat at 70 bpm AV node (50 bpm) and Purkinje fibers (25 40 bpm) can act as pacemakers under some conditions Internodal pathway from
The circulatory system
 Introduction to Physiology (Course # 72336) 1 הלב עקרונות בסיסיים (הכנה למעבדת לב) Adi Mizrahi mizrahia@cc.huji.ac.il Textbook Chapter 12 2 The circulatory system To the heart Away from the heart 3 L 2.5
Introduction to Physiology (Course # 72336) 1 הלב עקרונות בסיסיים (הכנה למעבדת לב) Adi Mizrahi mizrahia@cc.huji.ac.il Textbook Chapter 12 2 The circulatory system To the heart Away from the heart 3 L 2.5
RV dysfunction and failure PATHOPHYSIOLOGY. Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland
 RV dysfunction and failure PATHOPHYSIOLOGY Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland Normal Right Ventricle (RV) Thinner wall Weaker myocytes Differences
RV dysfunction and failure PATHOPHYSIOLOGY Adam Torbicki MD, Dept Chest Medicine Institute of Tuberculosis and Lung Diseases Warszawa, Poland Normal Right Ventricle (RV) Thinner wall Weaker myocytes Differences
Cath Lab Essentials: Basic Hemodynamics for the Cath Lab and ICU
 Cath Lab Essentials: Basic Hemodynamics for the Cath Lab and ICU Ailin Barseghian El-Farra, MD, FACC Assistant Professor, Interventional Cardiology University of California, Irvine Department of Cardiology
Cath Lab Essentials: Basic Hemodynamics for the Cath Lab and ICU Ailin Barseghian El-Farra, MD, FACC Assistant Professor, Interventional Cardiology University of California, Irvine Department of Cardiology
Clinical significance of cardiac murmurs: Get the sound and rhythm!
 Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
*Generating blood pressure *Routing blood: separates. *Ensuring one-way blood. *Regulating blood supply *Changes in contraction
 *Generating blood pressure *Routing blood: separates pulmonary and systemic circulations *Ensuring one-way blood flow: valves *Regulating blood supply *Changes in contraction rate and force match blood
*Generating blood pressure *Routing blood: separates pulmonary and systemic circulations *Ensuring one-way blood flow: valves *Regulating blood supply *Changes in contraction rate and force match blood
Heart. Structure Physiology of blood pressure and heartbeat
 Heart Structure Physiology of blood pressure and heartbeat Location and Anatomy Location and Anatomy Pericardial cavity: surrounds, isolates, and anchors heart Parietal pericardium lined with serous membrane
Heart Structure Physiology of blood pressure and heartbeat Location and Anatomy Location and Anatomy Pericardial cavity: surrounds, isolates, and anchors heart Parietal pericardium lined with serous membrane
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
During exercise the heart rate is 190 bpm and the stroke volume is 115 ml/beat. What is the cardiac output?
 The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
Introduction to Physiology (Course # 72336) 1. Adi Mizrahi Textbook Chapter 12
 1. Adi Mizrahi Textbook Chapter 12") Introduction to Physiology (Course # 72336) 1 עקרונות בסיסיים (הכנה למעבדת לב) הלב Adi Mizrahi mizrahia@cc.huji.ac.il Textbook Chapter 12 2 The circulatory system To the heart Away from the heart 3 L 2.5
Introduction to Physiology (Course # 72336) 1 עקרונות בסיסיים (הכנה למעבדת לב) הלב Adi Mizrahi mizrahia@cc.huji.ac.il Textbook Chapter 12 2 The circulatory system To the heart Away from the heart 3 L 2.5
Valvular Heart Disease
 Valvular Heart Disease Roman M. Sniecinski, MD, FASE Associate Professor of Anesthesiology Emory University School of Medicine Learning Objectives Review the major pathophysiology of the most common heart
Valvular Heart Disease Roman M. Sniecinski, MD, FASE Associate Professor of Anesthesiology Emory University School of Medicine Learning Objectives Review the major pathophysiology of the most common heart
Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing. 5. Intensity 2. Shape. 6. Pitch 3. Location of maximum intensity
 Definition Items in description of Timing Shape Location of maximum intensity Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing 5. Intensity 2. Shape 6. Pitch 3. Location of maximum
Definition Items in description of Timing Shape Location of maximum intensity Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing 5. Intensity 2. Shape 6. Pitch 3. Location of maximum
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
TGA atrial vs arterial switch what do we need to look for and how to react
 TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up