Obturator Hernia. Sara Kim Downstate Medical Center December 10, 2015
|
|
|
- Gordon Harvey
- 6 years ago
- Views:
Transcription

1 Obturator Hernia Sara Kim Downstate Medical Center December 10, 2015

2 Case presentation 87F with one week of midline abdominal pain radiating to RLQ, nausea and vomitting PMHx: HTN, hx of TB PSHx: s/p L pneumonectomy for TB ROS: recent weight loss, not intentional
3 Case presentation Vitals: T 98.3, P85, BP 163/90 PE: Abd: soft, mildly tender in RLQ, distended; no palpable hernias Hanington-Kiff Sign neg, howship-romberg sign neg Thigh: no palpable masses, no motor or sensory deficit Labs BUN/Creat: 44/1.76 CBC: 10.54>10.9/33<142, neut: 76.1% U/a: neg
4 What is the next step???
5 CT Abd/Pelvis
6 CT Abd/Pelvis

7 CT Abd/Pelvis
8 CT Abd/Pelvis
9 CT Abd/Pelvis
10 CT Abd/Pelvis
11 CT Abd/Pelvis
12 CT Abd/Pelvis

13 CT Abd/Pelvis
14 CT Abd/Pelvis
15 Plan: Foley, NGT placement IVF resuscitation OR for exploratory laparotomy, repair of obturator hernia
16 OR course Exploratory laparotomy Reduction of small bowel loop from R obturator canal Local perforation Small bowel resection with primary anastamosis Evaluation of remainder of small bowel Repair of obturator hernia Purse string suture around canal Re-enforced with broad ligament
17 Hospital Course Extubated on table POD 1-3 awaiting bowel function POD 4 2 bowel movements, tolerating PO intake Creatinine normalized (13/0.93) POD 5 Discharged home
18 Questions?

19 Obturator hernia little old lady hernia Usually 7 th or 8 th decade of life Recent weight loss Raised intra-abdominal pressure COPD Ascites Chronic cough Generally asymptomatic, unless Compression of obturator nerve Incarcerated bowel Account for 1% of all abdominal hernias
20 Obturator Hernia Female: male ratio 6:1 Broader pelvis Wide obturator canal Bilateral obturator hernias in 6% of cases


21 Clinical signs Howship-Romberg Sign Present in ~50% of cases, more commonly present in anterior type I hernias Pain along MEDIAL surface of thigh when leg is abducted and extended or internally rotated Internally rotate the leg PAIN Moritz Heinrich Romberg
22 Clinical signs Hanington-Kiff Sign Loss of the thigh adductor reflex Percuss over adductor muscle approximately 5 cm above the knee Intact patellar tendon reflex on same side
23 Clinical signs Howship-Romberg Sign Present in ~50% of cases, more commonly present in anterior type I hernias Pain along MEDIAL surface of thigh when leg is abducted and extended or internally rotated Intestinal obstruction Occurs in >80% of patients Hernia strangulation Repeated bowel obstructions that resolve quickly without intervention 30% Palpable mass in proximal medial aspect of thigh at origin of adductor muscles 20%
24 Clinical signs Howship-Romberg Sign Present in ~50% of cases, more commonly present in anterior type I hernias Pain along MEDIAL surface of thigh when leg is abducted and extended or internally rotated Intestinal obstruction Occurs in >80% of patients Hernia strangulation Repeated bowel obstructions that resolve quickly without intervention 30% Richter type hernia Palpable mass in proximal medial aspect of thigh at origin of adductor muscles 20%
25 Clinical signs Howship-Romberg Sign Present in ~50% of cases, more commonly present in anterior type I hernias Pain along MEDIAL surface of thigh when leg is abducted and extended or internally rotated Intestinal obstruction Occurs in >80% of patients Hernia strangulation Repeated bowel obstructions that resolve quickly without intervention 30% Palpable mass in proximal medial aspect of thigh at origin of adductor muscles 20%

26 3 types Type I anterior branch type **most common Type II posterior branch type Type III intermembranous type ** rare Sac enters space between the internal and external obturator membranes

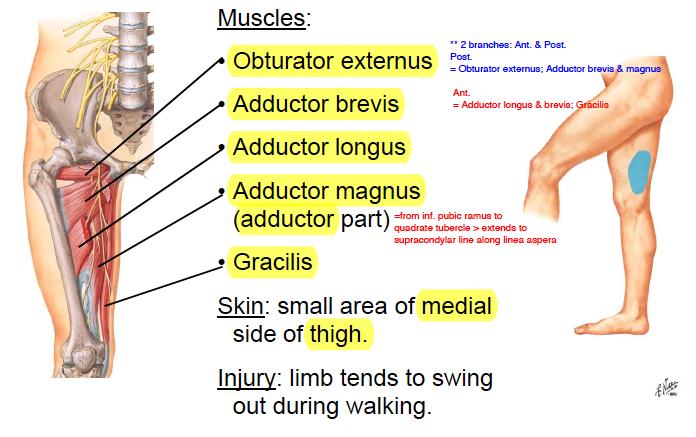
27 Anatomy

28 Anatomy Borders of obturator canal Superior: Obturator groove on superior pubic ramus Inferior: upper edge of the obturator membrane 3 cm in length Hernia lies deep to pectineus muscle difficult to palpate on exam

29 Anatomy Obturator foramen Ischial rami Pubic rami Obturator membrane covers the foramen except to allow the obturator vessels and nerves Neurovascular bundle usually lie posterolateral to hernia sac

30 Treatment Once diagnosis is made, SURGERY is the treatment High risk of incarceration and strangulation Three open approaches Lower midline transperitoneal approach Midline extraperitoneal approach Thigh approach Can consider laparoscopic TEP or TAPP repair
31 Lower midline transperitoneal approach 1. Laparotomy 2. Follow dilated small bowel to point of incarceration at obturator canal, reduce with gentle traction a. If unable to reduce, incise obturator membrane from anterior to posterior b. If unsuccessful, make counter-incision in medial groin -- attempt reduction from both sides of the canal 3. Assess viability of bowel, resect if needed 4. Close hernia opening around obturator neurovascular bundle a. Running suture, monofilament, encircling inner circumference of canal b. If no contamination, placement of mesh can be considered a. Consider attaching to cooper s ligament to prevent migration

32 Midline extraperitoneal approach Midline incision: umbilicus to pubis Enter pre-peritoneal plane deep to rectus muscle free bladder from peritoneum Open space to reveal superior pubic ramus and obturator internus muscle Hernia sac: projection of peritoneum passing inferiorly into obturator canal Incise sac at its base, reduce contents, transect the neck of the sac Close internal opening of obturator canal with a continuous suture as described previously Include periosteum of sup pubic rami, fascia of internal obturator muscle **avoid injury to obturator vessels Can also use mesh to cover defect
33 Thigh approach Vertical incision in upper medial thigh Made along adductor longus muscle Retract muscle medially Exposes pectineus muscle cut this to expose hernia sac Open sac, examine contents CAREFULLY, and reduce if viable Resect sac If contents not viable, will need midline laparotomy to address this Close hernia opening with continuous suture layer

34 Thigh Approach

35 Use of Broad ligament

36 Obturator hernias: A review of the laparoscopic approach Samer Deeba, Sanjay Purkayastha, Ara Darzi, Emmanouil Zacharakis J Minim Access Surg Oct-Dec; 7(4): Cases reviewed in literature from Total of 28 cases, data pooled Laparoscopic approach to obturator hernia is SAFE and EFFECTIVE 2 of the emergent cases required conversion to resect necrotic bowel 1 mesh repair 1 direct repair In acute presentations, rec TAPP repair to assess viability of incarcerated bowel


37 Obturator hernias: A review of the laparoscopic approach Samer Deeba, Sanjay Purkayastha, Ara Darzi, Emmanouil Zacharakis J Minim Access Surg Oct-Dec; 7(4): Direct repair 14% Elective repair: 20/28 cases Avg age: 53.2 years Avg weight: 55.3 kg Avg OR time: 50.6 min TAPP 29% Plug repair 4% TEP 53%
38 104 consecutive repairs of obturator hernia Mesh repair (n=24) vs nonmesh repair 24 mesh repair with via polypropylene patches with a memory recoil ring (Kugel repair) 5 plug mesh repairs Non mesh repair Simple reduction n=9 Simple closure of sac n=15 Fascial closure (suture of pectineus muscle to periosteum of bone) n=4 Covering of defect using an adjacent organ n=47 Laparotomy for 78% of operations Inguinal approach 22% No laparoscopic repairs
39
40 Mesh repair n=24 (30%) Bowel resection n=35 (44%) Intestinal perforation n=17 (21%) Five patients with bowel resection without perforation were repaired with mesh (6%) Post op complications N=31 (39%) In hospital mortality n=4 (5%) None had mesh repair, all underwent bowel resection Surgical site infection n=16 (20%) 13 underwent bowel resection (9 with perforation) 2/5 year survival: 74/55% No obturator neuralgia post op
41 Recurrences n=17 (16%) Simple reduction n=1 Simple closure of sac n=2 Covering defect with adj organ viscera n=14 Recs: If no contra-indication, mesh repair preferred
42 Summary Obturator hernia extremely rare skinny old lady hernia Treatment is SURGERY Four approaches Midline laparotomy Extraperitoneal approach Thigh approach Laparoscopic TEP or TAPP If no contamination, mesh repair is preferred

43
44 References 1. Javid Patrick J, Brooks David C, "Chapter 5. Hernias" (Chapter). Zinner MJ, Ashley SW: Maingot's Abdominal Operations, 11th Edition. 2. Gene L. Colborn, Robert M. Rogers Jr., John E. Skandalakis, Chapter 28. Pelvis and Perineum (Chapter). Skandalakis' Surgical Anatomy 3. Obturator hernias: A review of the laparoscopic approach. Samer Deeba, Sanjay Purkayastha, Ara Darzi, and Emmanouil Zacharakis; J Minim Access Surg Oct-Dec; 7(4): Obturator Hernia: Laparoscopic Diagnosis and Repair. Linwood R. Haith, Mark R Simeone, Kathleen J Reilly, Mary Lou Patton, Brian E. Moss, Barbara A Shotwell; JSLS Apr-Jun; 2(2): The Obturator hernia: Difficult to Diagnose, Easy To Repair. C.D. Shipkov, A.P. Uchikov, E. Grigoriadis; Hernia. 2004; 8: Strangulated Intestinal Obstruction Secondary to a Typical Obturator Hernia: A Case Report with Literature Review. Xiaoyan Cai, Xiangyang Song, and Xiujun Cai, Int J Med Sci. 2012; 9(3): Laparoscopic Management of Incarcerated Obturator Hernia. Kwok, Kay Yau, Wing Tai Siu, Chun Han Chau, Pei Cheung Yang and Michael Ka Wah Li; Can J Surg Feb; 48(1): Long-term Outcomes Afte Obturator Hernia Repair: Retrpsepctive Analysis of 80 Operations at a Single Institution. Karasaki, T., Y. Nomura, N. Tanaka; Hernia Jun 1; 18(3).
Consecutive, Bilateral Obturator Hernia in a Single Case HO Aydın¹, EHA Soy¹, T Avcı¹, T Tezcaner¹, S Yıldırım ABSTRACT
 Consecutive, Bilateral Obturator Hernia in a Single Case HO Aydın¹, EHA Soy¹, T Avcı¹, T Tezcaner¹, S Yıldırım ABSTRACT Obturator hernia (OH) is a rare pelvic hernia. It is diffucult to make an early diagnosis
Consecutive, Bilateral Obturator Hernia in a Single Case HO Aydın¹, EHA Soy¹, T Avcı¹, T Tezcaner¹, S Yıldırım ABSTRACT Obturator hernia (OH) is a rare pelvic hernia. It is diffucult to make an early diagnosis
Kay Barrera MD. September 4, 2014 SUNY Downstate
 Kay Barrera MD September 4, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations Case Presentation Symptoms Indications for repair Anatomy Operative management #TBT Throwback Thursday
Kay Barrera MD September 4, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations Case Presentation Symptoms Indications for repair Anatomy Operative management #TBT Throwback Thursday
34 yo M presented in ER of KCH at 7/06/10 Painful lump lt groin + vomiting Pain started 2 hrs before presentation. PMH known left inguinal hernia PSH
 Case Presentation 34 yo M presented in ER of KCH at 7/06/10 Painful lump lt groin + vomiting Pain started 2 hrs before presentation. PMH known left inguinal hernia PSH negative NKDA Case Presentation VS:
Case Presentation 34 yo M presented in ER of KCH at 7/06/10 Painful lump lt groin + vomiting Pain started 2 hrs before presentation. PMH known left inguinal hernia PSH negative NKDA Case Presentation VS:
Inguinal Hernia. Dr. Budi Irwan, SpB-KBD. Department of Surgery Faculty of Medicine University of North Sumatera Adam Malik National Hospital
 Inguinal Hernia Dr. Budi Irwan, SpB-KBD Division of Digestive Surgery Department of Surgery Faculty of Medicine University of North Sumatera Adam Malik National Hospital Definition Abnormal protrusion
Inguinal Hernia Dr. Budi Irwan, SpB-KBD Division of Digestive Surgery Department of Surgery Faculty of Medicine University of North Sumatera Adam Malik National Hospital Definition Abnormal protrusion
Inguinal and Femoral Hernias. August 10, 2016 Basic Science Lecture Department of Surgery University of Tennessee Health Science Center
 Inguinal and Femoral Hernias August 10, 2016 Basic Science Lecture Department of Surgery University of Tennessee Health Science Center Background Approximately 20 million groin hernias are repaired each
Inguinal and Femoral Hernias August 10, 2016 Basic Science Lecture Department of Surgery University of Tennessee Health Science Center Background Approximately 20 million groin hernias are repaired each
Femoral Triangle and Adductor Canal. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Femoral Triangle and Adductor Canal Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Femoral Triangle and Adductor Canal Femoral triangle Is a triangular depressed area located in the upper
Femoral Triangle and Adductor Canal Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Femoral Triangle and Adductor Canal Femoral triangle Is a triangular depressed area located in the upper
The front of the thigh. Dr.Amjad shatarat
 The front of the thigh Femoral triangle (Scarpa s triangle) Is a triangular depressed area located in the upper part of the medial aspect of the thigh immediately below the inguinal ligament. Superiorly:
The front of the thigh Femoral triangle (Scarpa s triangle) Is a triangular depressed area located in the upper part of the medial aspect of the thigh immediately below the inguinal ligament. Superiorly:
HERNIAS .(A) .(B) 5. .(A) 7..( (Lumbar hernia),
 .(B) 5. .(A) 7..( (Lumbar hernia),") HERNIAS ysms91@wonju.yonsei.ac.kr 1..(B) 2..(B) 3..(A) 4. (Hesselbach's striangle).(b) 5.,.(A) 6. (Sliding hernia).(a) 7..( (Lumbar hernia), (Obturator hernia), (Sciatica hernia)).(b) Hernia = rupture
HERNIAS ysms91@wonju.yonsei.ac.kr 1..(B) 2..(B) 3..(A) 4. (Hesselbach's striangle).(b) 5.,.(A) 6. (Sliding hernia).(a) 7..( (Lumbar hernia), (Obturator hernia), (Sciatica hernia)).(b) Hernia = rupture
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
Technique Guide. Bard MK Hernia Repair. Featuring Modified Onflex Mesh SOFT TISSUE REPAIR. Anterior Approach to a Preperitoneal Inguinal Hernia Repair
 Bard MK Hernia Repair Featuring Modified Onflex Mesh Technique Guide Anterior Approach to a Preperitoneal Inguinal Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. The opinions
Bard MK Hernia Repair Featuring Modified Onflex Mesh Technique Guide Anterior Approach to a Preperitoneal Inguinal Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. The opinions
Hernias Umbilical Hernia When to See a Surgeon? What Are Symptoms of an Umbilical Hernia? How is Repair Performed?
 Hernias Umbilical Hernia An umbilical hernia occurs when part of the intestine protrudes through the umbilical opening in the abdominal muscles. Umbilical hernias are common and typically harmless. They
Hernias Umbilical Hernia An umbilical hernia occurs when part of the intestine protrudes through the umbilical opening in the abdominal muscles. Umbilical hernias are common and typically harmless. They
HERNIA. Jacek Szeliga MD, PhD
 HERNIA Jacek Szeliga MD, PhD Hernia: The protrusion of tissue through a defect in fascial and/or muscular layer(s) that normally contain it. The sine qua non of a hernia is a bulge. 16th century illustration
HERNIA Jacek Szeliga MD, PhD Hernia: The protrusion of tissue through a defect in fascial and/or muscular layer(s) that normally contain it. The sine qua non of a hernia is a bulge. 16th century illustration
Internal supravesical hernia - a rare cause of intestinal obstruction: report of two cases
 Case report Open Access Internal supravesical hernia - a rare cause of intestinal obstruction: report of two cases Mahdi Bouassida 1,&, Selim Sassi 1, Hassen Touinsi 1, Helmi Kallel 1, Mohamed Mongi Mighri
Case report Open Access Internal supravesical hernia - a rare cause of intestinal obstruction: report of two cases Mahdi Bouassida 1,&, Selim Sassi 1, Hassen Touinsi 1, Helmi Kallel 1, Mohamed Mongi Mighri
Follow this and additional works at: Part of the Other Medical Specialties Commons, and the Surgery Commons
 Lehigh Valley Health Network LVHN Scholarly Works Department of Surgery Hernias Lauren Dudas MD Lehigh Valley Health Network, Lauren.Dudas@lvhn.org Follow this and additional works at: http://scholarlyworks.lvhn.org/surgery
Lehigh Valley Health Network LVHN Scholarly Works Department of Surgery Hernias Lauren Dudas MD Lehigh Valley Health Network, Lauren.Dudas@lvhn.org Follow this and additional works at: http://scholarlyworks.lvhn.org/surgery
ABSITE Review: Hernias
 ABSITE Review: Inguinal and Femoral Hernias Sybile Val M.D. SUNY Downstate Medical Center Department of Surgery June 27, 2008 Objectives www.downstatesurgery.org Correctly identify anatomical landmarks
ABSITE Review: Inguinal and Femoral Hernias Sybile Val M.D. SUNY Downstate Medical Center Department of Surgery June 27, 2008 Objectives www.downstatesurgery.org Correctly identify anatomical landmarks
rotation of the hip Flexion of the knee Iliac fossa of iliac Lesser trochanter Femoral nerve Flexion of the thigh at the hip shaft of tibia
 Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
Obturator hernia: diagnosis and treatment in the modern era
 866 Original Article Obturator hernia: diagnosis and treatment in the modern era Mantoo S K, Mak K, Tan T J ABSTRACT Introduction: Obturator hernia is a rare variety of abdominal hernia that nonetheless
866 Original Article Obturator hernia: diagnosis and treatment in the modern era Mantoo S K, Mak K, Tan T J ABSTRACT Introduction: Obturator hernia is a rare variety of abdominal hernia that nonetheless
ABDOMINAL WALL & RECTUS SHEATH
 ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
Incarcerated obturator hernia: pitfalls in the application of ultrasound
 Crit Ultrasound J (2009) 1:59 63 DOI 10.1007/s13089-009-0017-4 ORIGINAL ARTICLE Incarcerated : pitfalls in the application of ultrasound Masaaki Ogata Published online: 18 November 2009 Springer-Verlag
Crit Ultrasound J (2009) 1:59 63 DOI 10.1007/s13089-009-0017-4 ORIGINAL ARTICLE Incarcerated : pitfalls in the application of ultrasound Masaaki Ogata Published online: 18 November 2009 Springer-Verlag
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
Dr Sanjay Pandanaboyana
 Dr Sanjay Pandanaboyana General and Laparoscopic Surgeon Specialist General Hepatobiliary and Pancreatic Surgeon Auckland 16:30-16:50 It's Just a Hernia! Its just a hernia! Mr. Sanjay Pandanaboyana MS,
Dr Sanjay Pandanaboyana General and Laparoscopic Surgeon Specialist General Hepatobiliary and Pancreatic Surgeon Auckland 16:30-16:50 It's Just a Hernia! Its just a hernia! Mr. Sanjay Pandanaboyana MS,
Clinical Study Bilateral Obturator Hernia Diagnosed by Computed Tomography: A Case Report with Review of the Literature
 Radiology Research and Practice, Article ID 625873, 4 pages http://dx.doi.org/10.1155/2014/625873 Clinical Study Bilateral Obturator Hernia Diagnosed by Computed Tomography: A Case Report with Review of
Radiology Research and Practice, Article ID 625873, 4 pages http://dx.doi.org/10.1155/2014/625873 Clinical Study Bilateral Obturator Hernia Diagnosed by Computed Tomography: A Case Report with Review of
The thigh. Prof. Oluwadiya KS
 The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011
 Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Obturator Hernia: diagnosis and management under conditions of limited resources
 ORIGINAL ARTICLE Obturator Hernia: diagnosis and management under conditions of limited resources James I UMUNNA Department of Anatomy College of Medicine and Health Sciences Imo State University Owerri;
ORIGINAL ARTICLE Obturator Hernia: diagnosis and management under conditions of limited resources James I UMUNNA Department of Anatomy College of Medicine and Health Sciences Imo State University Owerri;
INGUINAL HERNIA REPAIR PROCEDURE GUIDE
 ROOM CONFIGURATION The following figure shows an overhead view of the recommended OR configuration for a da Vinci Inguinal Hernia Repair (Figure 1). NOTE: Configuration of the operating room suite is dependent
ROOM CONFIGURATION The following figure shows an overhead view of the recommended OR configuration for a da Vinci Inguinal Hernia Repair (Figure 1). NOTE: Configuration of the operating room suite is dependent
The Hip (Iliofemoral) Joint. Presented by: Rob, Rachel, Alina and Lisa
 Joint. Presented by: Rob, Rachel, Alina and Lisa") The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
Abdominal Hernia Omar alnoubani MD,MRCS
 Abdominal Hernia Omar alnoubani MD,MRCS Definition of hernia Anatomical landmarks Overview of types of hernia Presentation and Management of common types of hernia What is the definition of a hernia? An
Abdominal Hernia Omar alnoubani MD,MRCS Definition of hernia Anatomical landmarks Overview of types of hernia Presentation and Management of common types of hernia What is the definition of a hernia? An
COMPLICATIONS OF HERNIA REPAIR
 COMPLICATIONS OF HERNIA REPAIR Stanley Rogers, MD Associate Clinical Professor of Surgery University of Califronia, San Francisco Paré was respected as a hernia specialist, and was known to have elevated
COMPLICATIONS OF HERNIA REPAIR Stanley Rogers, MD Associate Clinical Professor of Surgery University of Califronia, San Francisco Paré was respected as a hernia specialist, and was known to have elevated
Lecture 01 Internal surface of anterolateral abdominal wall. BY Dr Farooq Khan Aurakzai
 Lecture 01 Internal surface of anterolateral abdominal wall BY Dr Farooq Khan Aurakzai Dated: 21.12.2017 Internal surface of the anterolateral abdominal wall The internal ( posterior ) surface of the anterolateral
Lecture 01 Internal surface of anterolateral abdominal wall BY Dr Farooq Khan Aurakzai Dated: 21.12.2017 Internal surface of the anterolateral abdominal wall The internal ( posterior ) surface of the anterolateral
Gross Anatomy ABDOMEN/SESSION 1 Dr. Firas M. Ghazi
 Anterior Abdominal Wall Structure, muscles and surface anatomy Curricular Objectives By the end of this session students are expected to: Practical 1. Identify the hip and distinguish the three bones forming
Anterior Abdominal Wall Structure, muscles and surface anatomy Curricular Objectives By the end of this session students are expected to: Practical 1. Identify the hip and distinguish the three bones forming
The Emergency Hernia or The call you don t want at 2:00 a.m.*
 or The call you don t want at 2:00 a.m.* *Or even at 8:00 a.m. Michael G. Sarr, MD Professor of Surgery Mayo Clinic South Canada WEST CANADA EAST CANADA Clinical talk Hernias Inguinal Umbilical Incisional
or The call you don t want at 2:00 a.m.* *Or even at 8:00 a.m. Michael G. Sarr, MD Professor of Surgery Mayo Clinic South Canada WEST CANADA EAST CANADA Clinical talk Hernias Inguinal Umbilical Incisional
2015 General Surgery Survival Guide
 2015 General Surgery Survival Guide Chapter 10: Hernia Repair Know What to Look for When Coding Hernia Repair Reporting hernia repair can be tricky. But if you know what to look for then half the work
2015 General Surgery Survival Guide Chapter 10: Hernia Repair Know What to Look for When Coding Hernia Repair Reporting hernia repair can be tricky. But if you know what to look for then half the work
2. List the 8 pelvic spaces: list one procedure or dissection which involves entering that space.
 Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Introduction Facts you should know:
 Introduction Facts you should know: - Mid inguinal point = ASIS to pubis symphysis (femoral artery) - Midpoint of inguinal ligament = ASIS to pubic tubercle (deep inguinal ring: 1 to 2cm above femoral
Introduction Facts you should know: - Mid inguinal point = ASIS to pubis symphysis (femoral artery) - Midpoint of inguinal ligament = ASIS to pubic tubercle (deep inguinal ring: 1 to 2cm above femoral
This presentation will discuss the anatomy of the anterior abdominal wall as it pertains to gynaecological and obstetric surgery.
 This presentation will discuss the anatomy of the anterior abdominal wall as it pertains to gynaecological and obstetric surgery. 1 The border of the anterior abdominal wall is defined superiorly by the
This presentation will discuss the anatomy of the anterior abdominal wall as it pertains to gynaecological and obstetric surgery. 1 The border of the anterior abdominal wall is defined superiorly by the
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT. Dr Farooq Khan Aurakzai. Dated:
 Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
A COMPARATIVE STUDY OF LAPROSCOPIC (TOTAL EXTRA PERITONEAL) AND OPEN LICHENSTEIN REPAIR OF INGUINAL HERNIA
 AND OPEN LICHENSTEIN REPAIR OF INGUINAL HERNIA") A COMPARATIVE STUDY OF LAPROSCOPIC (TOTAL EXTRA PERITONEAL) AND OPEN LICHENSTEIN REPAIR OF INGUINAL HERNIA Nishant Khurana, *Raghav Tantia, Devansh Arora, Sanjay Singhal, Dheeraj Aggarwal and Shireesh
A COMPARATIVE STUDY OF LAPROSCOPIC (TOTAL EXTRA PERITONEAL) AND OPEN LICHENSTEIN REPAIR OF INGUINAL HERNIA Nishant Khurana, *Raghav Tantia, Devansh Arora, Sanjay Singhal, Dheeraj Aggarwal and Shireesh
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery doi: To be assigned Early view version published: November
: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery doi: To be assigned Early view version published: November
The Lower Limb. Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa
 The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
Tier 2 MSK Clinic GP Message of the Month June Sportsman s groin (inguinal disruption).
.") Tier 2 MSK Clinic GP Message of the Month June 2014 Sportsman s groin (inguinal disruption). This month s MoM presents a case of bilateral inguinal disruption (ID) presenting as chronic (right) groin pain.
Tier 2 MSK Clinic GP Message of the Month June 2014 Sportsman s groin (inguinal disruption). This month s MoM presents a case of bilateral inguinal disruption (ID) presenting as chronic (right) groin pain.
Lower Limb Nerves. Clinical Anatomy
 Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
lower limb Anterior Compartment: lecture 3 The deep fascia ( fascia lata) divides the thigh into 3 compartments:
 divides the thigh into 3 compartments:") lower limb lecture 3 The deep fascia ( fascia lata) divides the thigh into 3 compartments: 1. Anterior Extensor compartment 2. Medial Adductor compartment 3. Posterior Flexor compartment Anterior Compartment:
lower limb lecture 3 The deep fascia ( fascia lata) divides the thigh into 3 compartments: 1. Anterior Extensor compartment 2. Medial Adductor compartment 3. Posterior Flexor compartment Anterior Compartment:
Inferior Pelvic Border
 Pelvis + Perineum Pelvic Cavity Enclosed by bony, ligamentous and muscular wall Contains the urinary bladder, ureters, pelvic genital organs, rectum, blood vessels, lymphatics and nerves Pelvic inlet (superior
Pelvis + Perineum Pelvic Cavity Enclosed by bony, ligamentous and muscular wall Contains the urinary bladder, ureters, pelvic genital organs, rectum, blood vessels, lymphatics and nerves Pelvic inlet (superior
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
LAPAROSCOPIC HERNIA REPAIR
 LAPAROSCOPIC HERNIA REPAIR Treating Your Hernia with Laparoscopy When You Have a Hernia Anyone can have a hernia. This is a weakness or tear in the wall of the abdomen. It often results from years of wear
LAPAROSCOPIC HERNIA REPAIR Treating Your Hernia with Laparoscopy When You Have a Hernia Anyone can have a hernia. This is a weakness or tear in the wall of the abdomen. It often results from years of wear
Technical points of the laparoscopic transabdominal preperitoneal (TAPP) approach in inguinal hernia repair
 approach in inguinal hernia repair") Surgical Technique Page 1 of 5 Technical points of the laparoscopic transabdominal preperitoneal (TAPP) approach in inguinal hernia repair Qiwei Shen, Qiyuan Yao Department of General Surgery, Huashan
Surgical Technique Page 1 of 5 Technical points of the laparoscopic transabdominal preperitoneal (TAPP) approach in inguinal hernia repair Qiwei Shen, Qiyuan Yao Department of General Surgery, Huashan
Professional Baseball Chiropractic Society Workshop. January 18-20, 2018
 Professional Baseball Chiropractic Society Workshop January 18-20, 2018 Dr. Craig Couillard Team Chiropractor and Soft Tissue Specialist for the St. Paul Saints What is a Sport s Hernia? What is the current
Professional Baseball Chiropractic Society Workshop January 18-20, 2018 Dr. Craig Couillard Team Chiropractor and Soft Tissue Specialist for the St. Paul Saints What is a Sport s Hernia? What is the current
Robot Assisted Rectopexy
 1. Abdominal cavity approach 1A Trocars Introduce Introduce five trocars to gain access to the abdominal cavity (in da Vinci Si type; In Xi type the trocar placement may differ slightly). First the camera
1. Abdominal cavity approach 1A Trocars Introduce Introduce five trocars to gain access to the abdominal cavity (in da Vinci Si type; In Xi type the trocar placement may differ slightly). First the camera
Borders of the Abdomen
 Abdominal wall Borders of the Abdomen Abdomen is the region of the trunk that lies between the diaphragm above and the inlet of the pelvis below Borders Superior: Costal cartilages 7-12. Xiphoid process:
Abdominal wall Borders of the Abdomen Abdomen is the region of the trunk that lies between the diaphragm above and the inlet of the pelvis below Borders Superior: Costal cartilages 7-12. Xiphoid process:
Anterior and Medial compartments of the thigh. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT
 STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
THIEME. Anterior and Medial Compartments of the Thigh
 CHAPTER Anterior and Medial Compartments of the Thigh Learning Objectives 2 At the end of the dissection, you should be able to identify the following: Cutaneous nerves innervating the skin of the anterior
CHAPTER Anterior and Medial Compartments of the Thigh Learning Objectives 2 At the end of the dissection, you should be able to identify the following: Cutaneous nerves innervating the skin of the anterior
REPRODUCTIVE SYSTEM By Dr.Ahmed Salman
 The University Of Jordan Faculty Of Medicine Anatomy Department REPRODUCTIVE SYSTEM By Dr.Ahmed Salman Assistant Professor of Anatomy &embryology Perineum It is the diamond-shaped lower end of the trunk
The University Of Jordan Faculty Of Medicine Anatomy Department REPRODUCTIVE SYSTEM By Dr.Ahmed Salman Assistant Professor of Anatomy &embryology Perineum It is the diamond-shaped lower end of the trunk
Ali Yaghi. Omar Eyad. Ahmad Salman. 1 P a g e
 5 Ali Yaghi Omar Eyad Ahmad Salman 1 P a g e **There are two types of groin hernia; the femoral hernia and the inguinal hernia. But how can we differentiate between the inguinal hernia and the femoral
5 Ali Yaghi Omar Eyad Ahmad Salman 1 P a g e **There are two types of groin hernia; the femoral hernia and the inguinal hernia. But how can we differentiate between the inguinal hernia and the femoral
Lectures of Human Anatomy
 Lectures of Human Anatomy Lower Limb Gluteal Region and Hip Joint By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D.
Lectures of Human Anatomy Lower Limb Gluteal Region and Hip Joint By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D.
Identify the muscles associated with the medial compartment of the thigh. Identify the attachment points of the medial thigh muscles.
 L 8 A B O R A T O R Y Thigh MEDIAL THIGH Identify the muscles associated with the medial compartment of the thigh. Identify the attachment points of the medial thigh muscles. Identify the actions of these
L 8 A B O R A T O R Y Thigh MEDIAL THIGH Identify the muscles associated with the medial compartment of the thigh. Identify the attachment points of the medial thigh muscles. Identify the actions of these
Cover Page. The following handle holds various files of this Leiden University dissertation:
 Cover Page The following handle holds various files of this Leiden University dissertation: http://hdl.handle.net/1887/6119 Author: Spruit, E.N. Title: Increasing the efficiency of laparoscopic surgical
Cover Page The following handle holds various files of this Leiden University dissertation: http://hdl.handle.net/1887/6119 Author: Spruit, E.N. Title: Increasing the efficiency of laparoscopic surgical
Abdominal muscles. Subinguinal hiatus and ingiunal canal. Femoral and adductor canals. Neurovascular system of the lower limb. Sándor Katz M.D.,Ph.D.
 Abdominal muscles. Subinguinal hiatus and ingiunal canal. Femoral and adductor canals. Neurovascular system of the lower limb. Sándor Katz M.D.,Ph.D. External oblique muscle Origin: outer surface of the
Abdominal muscles. Subinguinal hiatus and ingiunal canal. Femoral and adductor canals. Neurovascular system of the lower limb. Sándor Katz M.D.,Ph.D. External oblique muscle Origin: outer surface of the
2) Department of Surgery, Showa-inan General Hospital, Komagane, Japan. First Department of Surgery, Shinshu University School of Medicine,
 Department of Surgery, Showa-inan General Hospital, Komagane, Japan. First Department of Surgery, Shinshu University School of Medicine,") Transabdominal preperitoneal repair for obturator hernia A short running head: TAPP for obturator hernia Takahide Yokoyama MD 1), 2), Akira Kobayashi MD, PhD 1), Toshiki Kikuchi MD, PhD 2), Ken Hayashi
Transabdominal preperitoneal repair for obturator hernia A short running head: TAPP for obturator hernia Takahide Yokoyama MD 1), 2), Akira Kobayashi MD, PhD 1), Toshiki Kikuchi MD, PhD 2), Ken Hayashi
Baraa Ayed حسام أبو عوض. Ahmad Salman. 1 P a g e
 4 Baraa Ayed حسام أبو عوض Ahmad Salman 1 P a g e Today we are going to cover these concepts: Iliotibial tract Anterior compartment of the thigh and the hip Medial compartment of the thigh Femoral triangle
4 Baraa Ayed حسام أبو عوض Ahmad Salman 1 P a g e Today we are going to cover these concepts: Iliotibial tract Anterior compartment of the thigh and the hip Medial compartment of the thigh Femoral triangle
Muscles of the Thigh. 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group
 Muscles of the Thigh 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Sartorius: This is a long strap like muscle with flattened tendons at each
Muscles of the Thigh 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Sartorius: This is a long strap like muscle with flattened tendons at each
CODING AND PRACTICE MANAGEMENT CORNER
 Hernia repair and complex abdominal wall reconstruction by Christopher Senkowski, MD, FACS; Mark Savarise, MD, FACS; John S. Roth, MD, FACS; and Jan Nagle, MS, RPh 52 The American College of Surgeons (ACS)
Hernia repair and complex abdominal wall reconstruction by Christopher Senkowski, MD, FACS; Mark Savarise, MD, FACS; John S. Roth, MD, FACS; and Jan Nagle, MS, RPh 52 The American College of Surgeons (ACS)
THE INS AND OUTS OF HERNIAS WHERE TO START? WHAT IS A HERNIA? CLINICAL INDICATIONS THE INGUINAL CANAL THE CLINICAL QUESTION 18/09/2018
 THE INS AND OUTS OF HERNIAS Cassandra Harrison BA/BSc, MMRU, AMS WHERE TO START? The Clinical Question Essential anatomy Inguinal hernia Scanning technique Variations WHAT IS A HERNIA? CLINICAL INDICATIONS
THE INS AND OUTS OF HERNIAS Cassandra Harrison BA/BSc, MMRU, AMS WHERE TO START? The Clinical Question Essential anatomy Inguinal hernia Scanning technique Variations WHAT IS A HERNIA? CLINICAL INDICATIONS
Sports Hernias. Matthew Gimre, MD ATC Conference, June 20, 2015
 Sports Hernias Matthew Gimre, MD ATC Conference, June 20, 2015 Sports hernia: So what is it? An injury to the rectus abdominis-common adductor aponeurosis, at the anterior/inferior aspect of the pubic
Sports Hernias Matthew Gimre, MD ATC Conference, June 20, 2015 Sports hernia: So what is it? An injury to the rectus abdominis-common adductor aponeurosis, at the anterior/inferior aspect of the pubic
Posterior Rectus Sheath Hernia Causing Intermittent Small Bowel Obstruction
 Posterior Rectus Sheath Hernia Causing Intermittent Small Bowel Obstruction Scott Lenobel 1*, Robert Lenobel 2, Joseph Yu 1 1. Department of Radiology, The Ohio State University Wexner Medical Center,
Posterior Rectus Sheath Hernia Causing Intermittent Small Bowel Obstruction Scott Lenobel 1*, Robert Lenobel 2, Joseph Yu 1 1. Department of Radiology, The Ohio State University Wexner Medical Center,
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Introduction Compartment Syndromes of the Leg Related to Athletic Activity Mark M. Casillas, M.D. Consequences of a misdiagnosis persistence of a performance limitation loss of function/compartment loss
Introduction Compartment Syndromes of the Leg Related to Athletic Activity Mark M. Casillas, M.D. Consequences of a misdiagnosis persistence of a performance limitation loss of function/compartment loss
Inguinal Hernia. Incarcerated hernia
 Inguinal Hernia An inguinal hernia occurs when soft tissue usually part of the membrane lining the abdominal cavity (omentum) or part of the intestine protrudes through a weak point in the abdominal muscles.
Inguinal Hernia An inguinal hernia occurs when soft tissue usually part of the membrane lining the abdominal cavity (omentum) or part of the intestine protrudes through a weak point in the abdominal muscles.
ORIENTING TO BISECTED SPECIMENS ON THE PELVIS PRACTICAL
 ORIENTING TO BISECTED SPECIMENS ON THE PELVIS PRACTICAL The Pelvis is just about as complicated as head and neck and considerably more mysterious. You have to be able to visualize (imagine) the underlying
ORIENTING TO BISECTED SPECIMENS ON THE PELVIS PRACTICAL The Pelvis is just about as complicated as head and neck and considerably more mysterious. You have to be able to visualize (imagine) the underlying
The Preperitoneal Inguinal Hernia Prosthetic Repair: Indications and Technical Notes
 Article ID: WMC002622 2046-1690 The Preperitoneal Inguinal Hernia Prosthetic Repair: Indications and Technical Notes Corresponding Author: Dr. Antonio Manenti, Associate Professor, Department Surgery -
Article ID: WMC002622 2046-1690 The Preperitoneal Inguinal Hernia Prosthetic Repair: Indications and Technical Notes Corresponding Author: Dr. Antonio Manenti, Associate Professor, Department Surgery -
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015
 ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
Muscles of the lower extremities. Dr. Nabil khouri MD, MSc, Ph.D
 Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
GI anatomy Lecture: 2 د. عصام طارق
 GI anatomy Lecture: 2 د. عصام طارق Objectives: To define rectus sheath. To describe anatomy of inguinal canal. To relates types of inguinal hernia to the region. To explore spermatic cord. Rectus Abdominis
GI anatomy Lecture: 2 د. عصام طارق Objectives: To define rectus sheath. To describe anatomy of inguinal canal. To relates types of inguinal hernia to the region. To explore spermatic cord. Rectus Abdominis
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty
 CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty Augustine Reid Wilson, MS, Justin Daggett, MD, Michael Harrington, MD, MPH, and Deniz
CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty Augustine Reid Wilson, MS, Justin Daggett, MD, Michael Harrington, MD, MPH, and Deniz
Emergency presentation of hernias of the torso: What your surgeon wants to know.
 Emergency presentation of hernias of the torso: What your surgeon wants to know. Ken F Linnau, MD, MS Emergency Radiology UW Medicine Harborview Medical Center klinnau@uw.edu Nordic Forum 2017 Helsinki,
Emergency presentation of hernias of the torso: What your surgeon wants to know. Ken F Linnau, MD, MS Emergency Radiology UW Medicine Harborview Medical Center klinnau@uw.edu Nordic Forum 2017 Helsinki,
Tor Chiu. Deep Inferior Epigastric Artery Perforator Flap 161
 18 Deep Inferior Epigastric Artery Perforator Flap Tor Chiu Deep Inferior Epigastric Artery Perforator Flap 161 Deep Inferior Epigastric Artery Perforator Flap FLAP TERRITORY The deep inferior epigastric
18 Deep Inferior Epigastric Artery Perforator Flap Tor Chiu Deep Inferior Epigastric Artery Perforator Flap 161 Deep Inferior Epigastric Artery Perforator Flap FLAP TERRITORY The deep inferior epigastric
Lumbar Plexus. Ventral rami L1 L4 Supplies: Major nerves.. Abdominal wall External genitalia Anteromedial thigh
 Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Perhaps the most controversial of new laparoscopic operations is the repair of the inguinal hernia. The
 JOURNAL OF LAPAROENDOSCOPIC SURGERY Volume 2, Number 6, 1992 Mary Ann Liebert, Inc., Publishers Extraperitoneal Endoscopie Inguinal Hernia Repair GEORGE S. FERZLI, M.D., F.A.C.S., AZIZ MASSAD, M.D., and
JOURNAL OF LAPAROENDOSCOPIC SURGERY Volume 2, Number 6, 1992 Mary Ann Liebert, Inc., Publishers Extraperitoneal Endoscopie Inguinal Hernia Repair GEORGE S. FERZLI, M.D., F.A.C.S., AZIZ MASSAD, M.D., and
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH
 FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
Obstructed direct inguinal hernia: A rare encounter
 www.edoriumjournals.com CASE REPORT PEER REVIEWED OPEN ACCESS Obstructed direct inguinal hernia: A rare encounter Sudhir Kumar Mohanty, Kumarmani Jena, Tanmaya Mahapatra, Jyoti Ranjan Dash, Ajax John,
www.edoriumjournals.com CASE REPORT PEER REVIEWED OPEN ACCESS Obstructed direct inguinal hernia: A rare encounter Sudhir Kumar Mohanty, Kumarmani Jena, Tanmaya Mahapatra, Jyoti Ranjan Dash, Ajax John,
THE LOWER LIMB NERVES VESSELS
 THE LOWER LIMB NERVES VESSELS LOWER LIMB: FEMORAL TRIANGLE FEMORAL TRIANGLE LOWER LIMB: FEMORAL TRIANGLE FEMORAL TRIANGLE is a triangular landmark useful in dissection and in understanding relationships
THE LOWER LIMB NERVES VESSELS LOWER LIMB: FEMORAL TRIANGLE FEMORAL TRIANGLE LOWER LIMB: FEMORAL TRIANGLE FEMORAL TRIANGLE is a triangular landmark useful in dissection and in understanding relationships
Hernia. emoryhealthcare.org
 Hernia Have you noticed a bulge or pain in your abdominal wall or groin? If so you may have a hernia. You may be in the process of confirming this diagnosis with your Primary Care Physician or already
Hernia Have you noticed a bulge or pain in your abdominal wall or groin? If so you may have a hernia. You may be in the process of confirming this diagnosis with your Primary Care Physician or already
Doc, I've done my groin. Groin Pain. Peter Brukner. Doc, I've done my groin 1. acute chronic
 Doc, I've done my groin Peter Brukner Associate Professor in Sports Medicine Centre for Sports Medicine Research and Education School of Physiotherapy 9/22/2006 The University of Melbourne Groin Pain acute
Doc, I've done my groin Peter Brukner Associate Professor in Sports Medicine Centre for Sports Medicine Research and Education School of Physiotherapy 9/22/2006 The University of Melbourne Groin Pain acute
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Table 2. First Generated List of Expert Responses. Likert-Type Scale. Category or Criterion. Rationale or Comments (1) (2) (3) (4)
 (2) (3) (4)") Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Lesson 24. A & P Hip
 Lesson 24 A & P Hip 1 Aims of the Session This session will allow candidates to have an understanding of the bony prominences and soft tissues of the hip 2 Learning Outcomes By the end of the lesson the
Lesson 24 A & P Hip 1 Aims of the Session This session will allow candidates to have an understanding of the bony prominences and soft tissues of the hip 2 Learning Outcomes By the end of the lesson the
Prevention and Surgical management of Parastomal hernias; When to treat?
 Prevention and Surgical management of Parastomal hernias; When to treat? Sabry A. Mahmoud (MD) Prof of General & Colorectal Surgery Mansoura University It is an incisional hernia that develops at the site
Prevention and Surgical management of Parastomal hernias; When to treat? Sabry A. Mahmoud (MD) Prof of General & Colorectal Surgery Mansoura University It is an incisional hernia that develops at the site
The Hip Joint. Shenequia Howard David Rivera
 The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
MUSCULOSKELETAL LOWER LIMB
 MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
Gluteal region DR. GITANJALI KHORWAL
 Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Prevention of Surgical Injuries in Gynecology
 in Gynecology John K. Chan, M.D. Division of Gynecologic Oncology Overview Review anatomy, etiology, intraoperative, postoperative management, prevention of injuries to: 1. Urinary tract 2. Gastrointestinal
in Gynecology John K. Chan, M.D. Division of Gynecologic Oncology Overview Review anatomy, etiology, intraoperative, postoperative management, prevention of injuries to: 1. Urinary tract 2. Gastrointestinal
Mr John Groom The Complete Guide to Hernia
 Mr John Groom The Complete Guide to Hernia What Do They Have in Common? AA Both Subjects Controversial! Debate 1. Laparoscopic verses Open Hernia Repair Beautiful Big splash Debate 2. Use of Mesh in Hernia
Mr John Groom The Complete Guide to Hernia What Do They Have in Common? AA Both Subjects Controversial! Debate 1. Laparoscopic verses Open Hernia Repair Beautiful Big splash Debate 2. Use of Mesh in Hernia
Bones of Lower Limb. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Bones of Lower Limb Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Bones of the lower limb Hip Bone Made up of 3 bones: 1) Ilium (flat), superior in position 2) Ischium (L), postero-inferior
Bones of Lower Limb Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Bones of the lower limb Hip Bone Made up of 3 bones: 1) Ilium (flat), superior in position 2) Ischium (L), postero-inferior
Comparison of Laparoscopic vs Open Modified Shouldice Technique in Inguinal Hernia Repair. Thomas Nicholson, MD, V. Tiruchelvam, MD METHODS
 Comparison of vs Modified Shouldice Technique in Inguinal Hernia Repair JSLS Thomas Nicholson, MD, V. Tiruchelvam, MD ABSTRACT Inguinal hernia repair has been a common procedure performed by general surgeo.
Comparison of vs Modified Shouldice Technique in Inguinal Hernia Repair JSLS Thomas Nicholson, MD, V. Tiruchelvam, MD ABSTRACT Inguinal hernia repair has been a common procedure performed by general surgeo.
DISSECTION 8: URINARY AND REPRODUCTIVE SYSTEMS
 8546d_c01_1-42 6/25/02 4:32 PM Page 38 mac48 Mac 48: 420_kec: 38 Cat Dissection DISSECTION 8: URINARY AND REPRODUCTIVE SYSTEMS Typically, the urinary and reproductive systems are studied together, because
8546d_c01_1-42 6/25/02 4:32 PM Page 38 mac48 Mac 48: 420_kec: 38 Cat Dissection DISSECTION 8: URINARY AND REPRODUCTIVE SYSTEMS Typically, the urinary and reproductive systems are studied together, because