Use of Aptus Heli-FX EndoAnchor implants with standard endografts to strengthen seal in hostile anatomies:
|
|
|
- Chloe Davidson
- 5 years ago
- Views:
Transcription
1 Use of Aptus Heli-FX EndoAnchor implants with standard endografts to strengthen seal in hostile anatomies: technical tips, case experience and clinical results CACVS Medtronic Symposium Paris, France January 20th, 2017 Jean M. Panneton, MD, FACS, FRCSC Professor of Surgery Chief and Program Director, Division of Vascular Surgery Eastern Virginia Medical School Norfolk, VA
2 DISCLOSURES: Consultant: Cook Medical Bolton Medical, Medtronic Inc, Volcano, WL Gore Speakers Bureau: Medtronic Inc. Grants / Research support: Bolton Medical Cook Medical Medtronic Inc. WL Gore Scientific Advisory Board: Medtronic Inc., Mellon Medical
3 Legacy studies continue to highlight need for lifelong surveillance in EVAR DREAM De Bruin et al. NEJM 2010 EVAR-1 Greenhalgh et al. NEJM 2010 ACE Becquemin et al. JVS 2011 Late ruptures in EVAR, none in open surgery With evar, predictors for rupture (endoleaks and migration) increase with time In ACE, 16% reinterventions in EVAR vs. 2.4% for open repair at 3 yr median f/u


4 OBJECTIVES The proximal neck is the Achilles heel of EVAR 1. To illustrate the technique for EndoAnchors implant in hostile anatomies during EVAR 2. To review the results of the ANCHOR Registry for prophylactic and therapeutic indications


5 These attributes qualify or disqualify a neck 1. Length 2. Diameter 3. Shape 4. Angulation 5. Wall ( thrombus or calcification ) The success of EVAR depends on fixation and seal at the proximal neck
6 IMPACT OF HOSTILE NECKS ON EVAR OUTCOMES Meta-Analysis of 7 major studies compared EVAR outcomes in hostile vs. friendly neck anatomies (total patients N = 1559) Study Sample Size Endografts Torsello et al, Endurant AbuRahma et al, AneuRx, Excluder, Zenith, Talent Hoshina et al, Excluder, Zenith Abbruzzese et al, AneuRx, Excluder, Zenith Choke et al, Talent, Zenith, Excluder, AneuRx Fulton et al, AneuRx Fairman et al, Talent Type I endoleaks 4.5x more likely at 1-year after endograft implantation in hostile proximal aortic neck anatomy (P =.010) Aneurysm-related mortality risk 9x greater in hostile neck anatomy (P=.013) 1 Antoniou GA et al. J Vasc Surg. 2013;57(2):



7 EVAR COMPLICATIONS Loss of fixation Loss of seal Ruptured AAA from migration with proximal type I endoleak Graft migration Type I endoleak






8 Displacement force in Newtons Tailored seal and fixation of endoanchors CREATE THE STABILITY OF A SURGICAL ANASTOMOSIS IN EVAR AND TEVAR Surgical Anastomosis EndoAnchoring Talent Endurant Excluder Zenith Mean Hand Sewn No EndoAnchors With EndoAnchors Chart from data published in Melas N, et al. J Vasc Surg 2012;55(6): Case images courtesy of John Aruny MD, Bart Edward Muhs, MD, PhD.



9 ENDOANCHORING: A NEW MODALITY TO IMPROVE PROXIMAL FIXATION AND SEALING Heli-FX Aortic Securement System Heli-FX Guide Heli-FX Applier Cassette with EndoAnchors EndoAnchor dimensions: 4.5mm length 3.0mm diameter EndoAnchors 10 for EVAR

10 EndoAnchor Deployment Controlled Tactile Intuitive Safe 2 steps process Recapture Release 11
11 Technique for EndoAnchors Deployment Minimum 4 EndoAnchors recommended 30º-45º RAO 30º-45º LAO Tips for EndoAnchor implantation: C-arm positioning critical for proper spacing, visualization & implantation Min 4 EndoAnchors recommended For prox neck dia. > 29mm, min 6 EndoAnchors recommended Strive for even spacing around neck circumference EndoAnchors should penetrate vessel wall Select positions lacking excessive thrombus/calcium EndoAnchors # of C-arm positions Recommended angular offset 4 EndoAnchors 2 ~90 Note: C-arm positions above show just one possible combination 6 EndoAnchors 3 ~60
12 Technique: C-Arm positioning for 6 EndoAnchors 30º RAO 30º LAO 90º Lateral Note: C-arm positions above show just one possible combination



13 PROPHYLACTIC ENDOANCHORS WITH INDEX EVAR 84 y.o female patient with rapidly expanding AAA CTA: short, conical angulated neck


14 PROPHYLACTIC ENDOANCHORS WITH INDEX EVAR CTA: Circumferential placement of endoanchors No endoleaks, AAA decreased to 4.5cm over 1yr



15 PROPHYLACTIC ENDOANCHORS WITH INDEX EVAR Patient information: 79 yr old female patient CTA: 7 cm AAA & 4.5 cm DTA Aortic neck: diameter 23 mm length 37 mm


16 PROPHYLACTIC ENDOANCHORS WITH INDEX EVAR 3 D CTA Should you place EndoAnchors?

17 PROPHYLACTIC ENDOANCHORS WITH INDEX EVAR Pre deployment angiogram


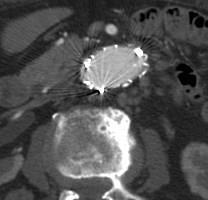
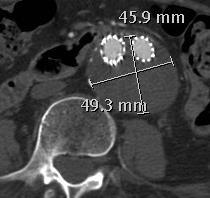
18 PROPHYLACTIC ENDOANCHORS WITH INDEX EVAR EndoAnchor deployment


19 PROPHYLACTIC ENDOANCHORS WITH INDEX EVAR EndoAnchor deployment


20 PROPHYLACTIC ENDOANCHORS WITH INDEX EVAR Completion angiogram



21 PROPHYLACTIC ENDOANCHORS WITH INDEX EVAR 3 years AAA diameter Down to 4.9 cm
22 TOP TEN TIPS FOR ENDOANCHORS IN PRIMARY EVAR 1. Take the time for preoperative planning 2. Wishful thinking does not create a neck 3. Deliver the endograft accurately at the lowest renal artery 4. Do the aortic balloon molding first 5. Size the Aptus guide according to endograft size 6. Place the gantry at 90 o angle to the applier 7. Make sure you make contact and penetrate the aortic wall 8. Anchor at the proximal fabric edge of the endograft 9. Deploy 2 rows of EndoAnchors in the neck 10.Space the EndoAnchors circumferentially
23 ANCHOR REGISTRY CAPTURING REAL-WORLD USAGE Registry Design Registry Principal Investigators Treatment Arms Prospective & Observational, International & Multi-Center, Dual-arm Registry with Core Lab Analysis Europe: Dr Jean-Paul de Vries Chief of Vascular Surgery, St. Antonius Hospital US: Dr William Jordan Chief of Vascular Surgery/Endovascular Therapy, Emory University Primary Up to 1000 pts, Prophylactic Revision Up to 1000 pts, Therapeutic Enrollment & Duration Enrollment began 2012 and patients will be followed for 5 years Follow-up Per Standard of Care at each center & discretion of Investigator Over 680 Patients Enrolled as of November 2016
24 ANCHOR REGISTRY * PRIMARY ARM REPRESENTS 72.4% OF PTS 604 ANCHOR REGISTRY Arm Stent Grafts - Primary Medtronic Endurant Gore Excluder * Cook Zenith * Jotec * Other 437 PRIMARY ARM 167 REVISION ARM 1 *Data cut June 15, Despite Endurant being 1 in 2 grafts in the primary arm, it is only a subset of what's being presented with complications in the revision arm 2 No longer commercially available in the US Arm Stent Grafts - Revision Metronic Endurant Medtronic Talent 2 Medtronic AneuRx 2 Gore Excluder * Cook Zenith * Jotec * Other/Unknown
25 ANCHOR REGISTRY PRIMARY ARM (N=437) Prophylactic Use: Application of EndoAnchor implants without evidence of type 1a endoleak, but concern for late failure and/or prevention of neck dilatation ANCHOR REGISTRY PRIMARY ARM REVISION ARM PROPHYLACTIC USE (72%, N=314) INTRA-OP TYPE IA ENDOLEAKS (28%, N=123)
26 ANCHOR REGISTRY PROPHYLACTIC SUBJECTS Baseline characteristics & aneurysm measurements* Male: 78% Infrarenal Diameter: 25.6 mm Avg Neck Calcium Thickness: 1.2 mm Infrarenal Angulation: 24.6 * Mean Core Lab measurements based on 251 patients with baseline CTs Neck Length (median): 11.5 mm Conical Neck (>10%/10mm): 41.4% Max Aneurysm Diameter: 55.7 mm Female: 22% Mean Age: 72.4 Years HOSTILE NECKS: 91.2% (229/251) Diameter at renals >28mm Proximal Neck Length <15mm Neck Angulation >60 Conical (>10%/10mm) Thrombus/Calcium >2mm OR Thrombus/Calcium >1mm / 180
27 ANCHOR REGISTRY PROPHYLACTIC SUBJECTS TECHNICAL SUCCESS* 94.9% PROCEDURAL SUCCESS* 94.6% Successful deployment of EndoAnchor implants with adequate penetration into aortic wall Technical success without type Ia endoleak at completion arteriography Avg. duration of Procedure (minutes) 15.8 Avg. time to EndoAnchor implants (minutes) 5.5 Avg. Number of EndoAnchor implants * Site-reported data
28 ANCHOR REGISTRY PROPHYLACTIC SUBJECTS Proximal Endoleaks and Migration Core Lab 12 months 24 months Type Ia Endoleak 0.6% (1/181) 0.0% (0/86) Migration 0.0% (0/129) 0.0% (0/43) Migration was assessed in comparison to the 1-month CT scan
29 ANCHOR REGISTRY PROPHYLACTIC SUBJECTS All-Cause Mortality, Aneurysm-Related Mortality, 2 nd Procedures Kaplan-Meier Estimates 1 Year (N=301) 1 2 Year (N=214) 1 Freedom from ACM 94.5% 90.6% Freedom from ARM 98.4% 98.4% Freedom from 2 nd Procedures 95.9% 92.1% 1 Number of subjects at risk at the beginning of interval
30 USE ENDOANCHOR IMPLANTS PROPHYLACTICALLY TO Prevent/Mitigate Risk for Type Ia Endoleaks Improve the Durability of EVAR for Hostile AAA Necks Short, Wide, Angled, Conical Thrombus and Calcium
31 Technique: C-Arm Positioning for Type 1 EL Treatment Move C-Arm in degree increments Identify leak channel and then create a suture line along wall. Circumferential anchoring before/after T1 EL treatment is recommended: address concerns of long-term neck morphology changes



32 THERAPEUTIC ENDOANCHORS WITH INDEX EVAR 82 y.o male patient; CTA: short, conical angulated neck

33 THERAPEUTIC ENDOANCHORS WITH INDEX EVAR Post deployment angiogram: Type Ia endoleak

34 THERAPEUTIC ENDOANCHORS WITH INDEX EVAR Post EndoAnchors completion angiogram: resolved endoleak AAA sac regression of 11 mm at 1 year Thrombosed sac No endoleak

35 THERAPEUTIC ENDOANCHORS WITH INDEX ChEVAR 85 y.o. male patient with ruptured juxtarenal AAA


36 THERAPEUTIC ENDOANCHORS WITH INDEX ChEVAR Intraop angio: Type Ia endoleak Corrected by EndoAnchors



37 THERAPEUTIC ENDOANCHORS WITH INDEX ChEVAR EA EndoAnchor below the left renal chimney EA EA
38 ANCHOR REGISTRY THERAPEUTIC USE (N=290) Therapeutic Use cohort consists of patients receiving EndoAnchor implants to treat complications (type 1a EL, migration, neck dilatation) in the Primary and Revision Arms. ANCHOR REGISTRY PRIMARY ARM REVISION ARM PROPHYLACTIC USE INTRA-OP TYPE Ia ELs (42.4%, N=123) PROXIMAL NECK RE-INTERVENTION (57.6%, N=167)
39 ANCHOR REGISTRY THERAPEUTIC USE Indications for EndoAnchor Implants Intra-Op T1 EL Pts within index procedure N= % Urgent Cases 100% Type 1a Endoleak Revision Pts post-evar follow-up N= % Urgent Cases 12% Migration 59% Type 1a Endoleak 18% Migration and Type 1a Endoleak 11.8% Urgent Cases 9.2% Urgent Cases 14.8% Urgent Cases Male: 73% Female: 27% Male: 81% Female: 19% Mean Age: 74.5 Years Mean Age: 77.6 Years
40 ANCHOR REGISTRY THERAPEUTIC USE IN INTRA-OP T1 EL Baseline characteristics & aneurysm measurements* Male: 73% Female: 27% Mean Age: 74.5 Years Infrarenal Diameter: 26.2 mm Infrarenal Angulation: 26.6 Conical Neck (>10%/10mm): 40.2% * Mean Core Lab measurements based on 107 patients with baseline CTs Neck Length (median): 12.1 mm Aneurysm Diameter: 57.0 mm Avg Neck Calcium Thickness: 1.2 mm HOSTILE NECKS: 82.2% (88/107) Diameter at renals >28mm Proximal Neck Length <15mm Neck Angulation >60 Conical (>10%/10mm) Thrombus/Calcium >2mm OR Thrombus/Calcium >1mm / 180
41 ANCHOR REGISTRY THERAPEUTIC USE IN REVISION SETTING Baseline characteristics & aneurysm measurements* Infrarenal Diameter: 29.3 mm Infrarenal Angulation: 21.3 Conical Neck (>10%/10mm): 50.7% * Mean Core Lab measurements based on 146 patients with baseline CTs Neck Length (median): 10.2 mm Aneurysm Diameter: 69.6 mm Avg Neck Calcium Thickness: 0.27 mm Male: 81% Female: 19% Mean Age: 77.6 Years HOSTILE NECKS: 88.4% (129/146) Diameter at renals >28mm Proximal Neck Length <15mm Neck Angulation >60 Conical (>10%/10mm) Thrombus/Calcium >2mm OR Thrombus/Calcium >1mm / 180
42 ANCHOR REGISTRY THERAPEUTIC USE TECHNICAL SUCCESS Successful deployment of EndoAnchor implants with adequate penetration into aortic wall PROCEDURAL SUCCESS Technical success without type Ia endoleak at completion arteriography 94.3% Intra-op T1 EL 87.0% Intra-op T1 EL 90.2% Revision 89.0% Revision Avg. duration of Procedure (min) Avg. time to EndoAnchor implants (min) Avg. number of EndoAnchor implants Intra-op T1 EL * Site-reported data Revision Intra-op Revision Intra-op Revision T1 EL T1 EL
43 ANCHOR REGISTRY THERAPEUTIC USE Proximal Endoleaks and Migration Core Lab Intra-Op Type 1 EL 12 months 24 months Type 1a Endoleak 1.4% (1/70) 2.9% (1/35) Migration 0.0% (0/44) 0.0% (0/17) Revision Setting 12 months 24 months Type 1a Endoleak 19.2% (15/78) 11.1% (3/27) Migration 0.0% (0/55) 0.0% (0/16) Migration was assessed in comparison to the 1-month CT scan
44 ANCHOR REGISTRY THERAPEUTIC USE All-Cause Mortality, Aneurysm-Related Mortality, 2 nd Procedures Intra-Op Type 1 EL 1 Year 2 Year Freedom from ACM 95.5% (117)1 89.9% (79)1 Freedom from ARM 98.4% (117)1 98.4% (79)1 Freedom from 2 nd Procedures 97.9% (117)1 92.9% (78)1 Revision Setting 1 Year 2 Year Freedom from ACM 88.2% (158)1 75.6% (94)1 Freedom from ARM 96.5% (158)1 92.9% (94)1 Freedom from 2 nd Procedures 84.8% (156)1 79.9% (81)1 1 Number of subjects at risk at the beginning of interval
45 THERAPEUTIC USE SUMMARY EndoAnchor implants to treat index procedure Type Ia endoleaks associated with excellent results through 2-Year follow-up EndoAnchor implants used in a revision setting are successful in majority of cases 97.1 % 97.1% of patients treated for Intra-op T1 EL had decreasing or stable AAA sacs at 2-years 89.7% 89.7% of patients treated in the Revision Arm had decreasing or stable AAA sacs at 2-years 92.9 % 92.9% of patients treated for Intra-op T1 EL were free from 2 nd procedures through 2-years 79.9% 79.9% of patients treated in the Revision Arm were free from 2 nd procedures through 2-years

46 THERAPEUTIC ENDOANCHORS WITH ChEVAR EL 87 y.o. female patient PMHx: HTN, CAD, CKD II PSHx: PCI x 3, EVAR Presenting with acute back pain Contained ruptured AAA with a type Ia & right Ib endoleaks Redo EVAR with Endurant cuff & triple chimneys Right hypogastric embolization and iliac extension



47 THERAPEUTIC ENDOANCHORS WITH ChEVAR Placement of EndoAnchors above and below the left renal chimney


48 THERAPEUTIC ENDOANCHORS WITH ChEVAR Posterior Placement of EndoAnchors


49 THERAPEUTIC ENDOANCHORS WITH ChEVAR Completion angiogram in RAO




50 THERAPEUTIC ENDOANCHORS WITH ChEVAR POST OP CTA All 3 chimneys patent CTA at 3 years: no endoleak EndoAnchor EndoAnchor

51 CONCLUSIONS EVAR in difficult aortic necks leads to poorer outcome and open repair should be considered in properly selected patients and in experienced hands The deployment of EndoAnchors during EVAR is simple, intuitive, safe and effective. The learning curve is relatively short and experience allows deployment in more challenging anatomy


52 CONCLUSIONS Data from the ANCHOR Registry suggest that with careful patient selection and case planning, some patients with hostile necks can be treated both safely and effectively with standard EVAR combined with EndoAnchors and without more advanced endograft technology
53 THANK YOU
Improving Endograft Durability with EndoAnchors
 Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
EVAR Revision Setting - How can Heli-FX EndoAnchors improve the outcomes?
 D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg EVAR Revision Setting - How can Heli-FX EndoAnchors improve the outcomes? Disclosures Speaker name: Dittmar Böckler
D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg EVAR Revision Setting - How can Heli-FX EndoAnchors improve the outcomes? Disclosures Speaker name: Dittmar Böckler
Mid-term results from ANCHOR: How does this data influence the treatment algorithm for hostile EVAR anatomies
 Mid-term results from ANCHOR: How does this data influence the treatment algorithm for hostile EVAR anatomies Jean-Paul P.M. de Vries Head Department of Surgery, University Medical Centre Groningen The
Mid-term results from ANCHOR: How does this data influence the treatment algorithm for hostile EVAR anatomies Jean-Paul P.M. de Vries Head Department of Surgery, University Medical Centre Groningen The
Hostile Neck During EVAR, The Role Of Endoanchores
 Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany
 Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
Treating very short necks ( 4mm <10mm) using the Endurant stent graft + EndoAnchors: 1-year results and current insights
 using the Endurant stent graft + EndoAnchors: 1-year results and current insights") Treating very short necks ( 4mm
Treating very short necks ( 4mm
Jean M. Panneton, MD, FRCSC, FACS. Professor of Surgery, Chief & Program Director Division of Vascular Surgery. Norfolk, VA
 Jean M. Panneton, MD, FRCSC, FACS Professor of Surgery, Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School Norfolk, VA The Houston Aortic Symposium Houston TX, February
Jean M. Panneton, MD, FRCSC, FACS Professor of Surgery, Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School Norfolk, VA The Houston Aortic Symposium Houston TX, February
When to use standard EVAR with EndoAnchors or CHEVAR in short-neck AAAs LINC ASIA 18
 When to use standard EVAR with EndoAnchors or CHEVAR in short-neck AAAs JEAN-PAUL P.M. DE VRIES, DIRECTOR OF VASCULAR SURGERY ST.ANTONIUS HOSPITAL NIEUWEGEIN, THE NETHERLANDS. LINC ASIA-PACIFIC HongKong,
When to use standard EVAR with EndoAnchors or CHEVAR in short-neck AAAs JEAN-PAUL P.M. DE VRIES, DIRECTOR OF VASCULAR SURGERY ST.ANTONIUS HOSPITAL NIEUWEGEIN, THE NETHERLANDS. LINC ASIA-PACIFIC HongKong,
Ralf R. Kolvenbach. Verbund Katholischer Kliniken Gefäßzentrum Augusta Krankenhaus Düsseldorf
 Ralf R. Kolvenbach Verbund Katholischer Kliniken Gefäßzentrum Augusta Krankenhaus Düsseldorf Endograft migration Stent no longer above renal artery 15 mm migration 6 Mos Do we really need any adjuncts
Ralf R. Kolvenbach Verbund Katholischer Kliniken Gefäßzentrum Augusta Krankenhaus Düsseldorf Endograft migration Stent no longer above renal artery 15 mm migration 6 Mos Do we really need any adjuncts
Technique and Tips for Complicated AAA Cases with Stent Graft
 Technique and Tips for Complicated AAA Cases with Stent Graft Seung-Woon Rha, MD, PhD FACC, FAHA, FESC, FSCAI, FAPSIC Cardiovascular Center, Korea University Guro Hospital Mar 15, 2018 LINC AP 2018 Endoleak;
Technique and Tips for Complicated AAA Cases with Stent Graft Seung-Woon Rha, MD, PhD FACC, FAHA, FESC, FSCAI, FAPSIC Cardiovascular Center, Korea University Guro Hospital Mar 15, 2018 LINC AP 2018 Endoleak;
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs
 How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
Patient selection in Hostile Necks and how. to prevent endoleaks a word of caution
 Patient selection in Hostile Necks and how to prevent endoleaks a word of caution P M Kasprzak, K. Pfister Department of Vascular Surgery Endovascular Surgery University Hospital Regensburg, Germany Conflict
Patient selection in Hostile Necks and how to prevent endoleaks a word of caution P M Kasprzak, K. Pfister Department of Vascular Surgery Endovascular Surgery University Hospital Regensburg, Germany Conflict
Anatomy-Driven Endograft Selection for Abdominal Aortic Aneurysm Repair S. Jay Mathews, MD, MS, FACC
 Anatomy-Driven Endograft Selection for Abdominal Aortic Aneurysm Repair S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton, FL, USA Disclosures
Anatomy-Driven Endograft Selection for Abdominal Aortic Aneurysm Repair S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton, FL, USA Disclosures
Endoanchor-assisted TEVAR
 Endoanchor-assisted TEVAR May 29, 2015 NCVH2015 Grayson H. Wheatley III, MD Director of Aortic and Endovascular Surgery Associate Professor of Surgery Temple University School of Medicine Disclosures Consultant
Endoanchor-assisted TEVAR May 29, 2015 NCVH2015 Grayson H. Wheatley III, MD Director of Aortic and Endovascular Surgery Associate Professor of Surgery Temple University School of Medicine Disclosures Consultant
Now that Endoanchors are Approved (and paid for) We have a Durable Solution to Short Necks That s so Easy!
 We have a Durable Solution to Short Necks That s so Easy!") Now that Endoanchors are Approved (and paid for) We have a Durable Solution to Short Necks That s so Easy! David H. Deaton, MD Vascular Surgery / University of South Carolina / Palmetto Health Chief Medical
Now that Endoanchors are Approved (and paid for) We have a Durable Solution to Short Necks That s so Easy! David H. Deaton, MD Vascular Surgery / University of South Carolina / Palmetto Health Chief Medical
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice
 Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Technique and Outcome of Laser Fenestration For Arch Vessels
 Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Considerations for a Durable Repair
 Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
The Auckland Experience with the Nellix EVAS System. Andrew Holden, MBChB, FRANZCR
 The Auckland Experience with the Nellix EVAS System Andrew Holden, MBChB, FRANZCR Disclosure Speaker name: Associate Professor Andrew Holden I have the following potential conflicts of interest to report:
The Auckland Experience with the Nellix EVAS System Andrew Holden, MBChB, FRANZCR Disclosure Speaker name: Associate Professor Andrew Holden I have the following potential conflicts of interest to report:
How to Categorize the Infrarenal Neck Properly? I Van Herzeele Dept. Thoracic and Vascular Surgery, Ghent University, Belgium
 How to Categorize the Infrarenal Neck Properly? I Van Herzeele Dept. Thoracic and Vascular Surgery, Ghent University, Belgium Disclosure Speaker name: Isabelle Van Herzeele I have the following potential
How to Categorize the Infrarenal Neck Properly? I Van Herzeele Dept. Thoracic and Vascular Surgery, Ghent University, Belgium Disclosure Speaker name: Isabelle Van Herzeele I have the following potential
EndoVascular Aneurysm Sealing (EVAS) with Nellix
 with Nellix") 1 2 EndoVascular Aneurysm Sealing (EVAS) with Nellix Designed to seal entire aneurysm with contained biostable polymer Non-modular design with complete fixation Expands endovascular patient eligibility
1 2 EndoVascular Aneurysm Sealing (EVAS) with Nellix Designed to seal entire aneurysm with contained biostable polymer Non-modular design with complete fixation Expands endovascular patient eligibility
Standardization of the CHEVAR procedure: How a standard approach has improved outcomes. Prof Peter Holt St George s, London
 Standardization of the CHEVAR procedure: How a standard approach has improved outcomes Prof Peter Holt St George s, London Disclosure Speaker name: Prof Peter Holt I have the following potential conflicts
Standardization of the CHEVAR procedure: How a standard approach has improved outcomes Prof Peter Holt St George s, London Disclosure Speaker name: Prof Peter Holt I have the following potential conflicts
CASE BOOK: ENDOANCHOR TM FIXATION UC EN
 CASE BOOK: ENDOANCHOR TM FIXATION UC201700368 EN PURPOSE OF THIS MATERIAL The Aptus TM Heli-FX TM EndoAnchor TM systems have been used in over 5,000 patients worldwide, with over 30,000 EndoAnchor implants
CASE BOOK: ENDOANCHOR TM FIXATION UC201700368 EN PURPOSE OF THIS MATERIAL The Aptus TM Heli-FX TM EndoAnchor TM systems have been used in over 5,000 patients worldwide, with over 30,000 EndoAnchor implants
Anatomical challenges in EVAR
 Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Management of Endoleaks
 Management of Endoleaks Murray Shames, MD Professor and Chief, Director Tampa General Hospital Aortic Program Vice Chair of Research, Dept. of Surgery Conflict of Interests: Speaker: Gore, Medtronic, Cook
Management of Endoleaks Murray Shames, MD Professor and Chief, Director Tampa General Hospital Aortic Program Vice Chair of Research, Dept. of Surgery Conflict of Interests: Speaker: Gore, Medtronic, Cook
Disclosures. EVAR follow-up: actual recommendation. EVAR follow-up: critical issues
 Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
Durability of The Endurant Stent-Graft through 5 Years
 Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
Aorfix Pythagoras US Clinical Trial:
 Overall 1 Year Results from the Aorfix Pythagoras US Clinical Trial: 1 st IDE Study in Highly Angulated 60 133 Aortic Necks Mark Fillinger MD for the PYTHAGORAS Investigators Disclosure Speaker name: Mark
Overall 1 Year Results from the Aorfix Pythagoras US Clinical Trial: 1 st IDE Study in Highly Angulated 60 133 Aortic Necks Mark Fillinger MD for the PYTHAGORAS Investigators Disclosure Speaker name: Mark
Taming The Aorta. David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA
 Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Current Status of EVAR for Infrarenal AAA. 31 st Annual Florida Vascular Society. PENN Surgery
 Current Status of EVAR for Infrarenal AAA 31 st Annual Florida Vascular Society PENN Surgery No Disclosures Stent Grafts Design Related Differences What really matters? Modular Unibody Supported Unsupported
Current Status of EVAR for Infrarenal AAA 31 st Annual Florida Vascular Society PENN Surgery No Disclosures Stent Grafts Design Related Differences What really matters? Modular Unibody Supported Unsupported
Conflicts of Interest. When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Summary. Infrarenal EVAR for short necks 2y postop
 When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Tim Resch MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau, IP, Research support Medtronic
When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Tim Resch MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau, IP, Research support Medtronic
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment
 Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
From 1996 to 1999, a total of 1,193 patients with
 THE ANEURX CLINICAL TRIAL AT 8 YEARS Lessons learned following the US AneuRx clinical trial from 1996 to 2004. BY CHRISTOPHER K. ZARINS, MD From 1996 to 1999, a total of 1,193 patients with infrarenal
THE ANEURX CLINICAL TRIAL AT 8 YEARS Lessons learned following the US AneuRx clinical trial from 1996 to 2004. BY CHRISTOPHER K. ZARINS, MD From 1996 to 1999, a total of 1,193 patients with infrarenal
Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS)
") Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS) Jean-Paul P.M. de Vries Dept Vascular Surgery St. Antonius Hospital, Nieuwegein,The Netherlands On behalf of the DEVASS study
Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS) Jean-Paul P.M. de Vries Dept Vascular Surgery St. Antonius Hospital, Nieuwegein,The Netherlands On behalf of the DEVASS study
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
My personal experience with INCRAFT in standard and challenging cases
 My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
Optimizing Accuracy of Aortic Stent Grafts in Short Necks
 Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
 Young-Guk Ko, M.D., Dangas G, J Am Coll Cardiol Intv 2012;5:1071 All-cause Mortality Dangas Severance G, J Am Coll Cardiovascular Cardiol Intv Hospital, 2012;5:1071 Yonsei University Health System Aneurysm-related
Young-Guk Ko, M.D., Dangas G, J Am Coll Cardiol Intv 2012;5:1071 All-cause Mortality Dangas Severance G, J Am Coll Cardiovascular Cardiol Intv Hospital, 2012;5:1071 Yonsei University Health System Aneurysm-related
symptomatic aneurysms or aneurysms that grow >1cm/yr
 1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
COMBINED TECHNIQUE CHIMNEY + FENESTRATED ENDOGRAFT FOR COMPLEX ANEURYSMS ERIC DUCASSE - MD PHD FEVBS CHU BORDEAUX
 COMBINED TECHNIQUE CHIMNEY + FENESTRATED ENDOGRAFT FOR COMPLEX ANEURYSMS ERIC DUCASSE - MD PHD FEVBS CHU BORDEAUX DISCLOSURE SPEAKER NAME: PR. E. DUCASSE I HAVE THE FOLLOWING POTENTIAL CONFLICTS OF INTEREST
COMBINED TECHNIQUE CHIMNEY + FENESTRATED ENDOGRAFT FOR COMPLEX ANEURYSMS ERIC DUCASSE - MD PHD FEVBS CHU BORDEAUX DISCLOSURE SPEAKER NAME: PR. E. DUCASSE I HAVE THE FOLLOWING POTENTIAL CONFLICTS OF INTEREST
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients
 ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability. Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands
 GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
Insights from the PROTAGORAS/PERICLES Registries: impact on ChEVAR results
 Insights from the PROTAGORAS/PERICLES Registries: impact on ChEVAR results Konstantinos P. Donas, Giovanni Torsello Department of Vascular Surgery St. Franziskus Hospital Münster, Germany Disclosure Speaker
Insights from the PROTAGORAS/PERICLES Registries: impact on ChEVAR results Konstantinos P. Donas, Giovanni Torsello Department of Vascular Surgery St. Franziskus Hospital Münster, Germany Disclosure Speaker
No Neck Is Needed! Treat the Aneurysm Instead! Andrew Holden, MD Associate Professor of Radiology Auckland City Hospital
 No Neck Is Needed! Treat the Aneurysm Instead! Andrew Holden, MD Associate Professor of Radiology Auckland City Hospital Disclosures Andrew Holden, MBChB, FRANZCR No financial investment to disclose Investigator
No Neck Is Needed! Treat the Aneurysm Instead! Andrew Holden, MD Associate Professor of Radiology Auckland City Hospital Disclosures Andrew Holden, MBChB, FRANZCR No financial investment to disclose Investigator
A New EVAR Device for Infrarenal AAAs
 A New EVAR Device for Infrarenal AAAs Peter Nelson, MD, MS Assistant Professor of Surgery MM0203 Rev. 01 Current U.S. EVAR Devices Anatomical Fixation Proximal Fixation Powerlink - Endologix Excluder WL
A New EVAR Device for Infrarenal AAAs Peter Nelson, MD, MS Assistant Professor of Surgery MM0203 Rev. 01 Current U.S. EVAR Devices Anatomical Fixation Proximal Fixation Powerlink - Endologix Excluder WL
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts
 Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
Treatment options of late failures of EVAS. Michel Reijnen Rijnstate Arnhem The Netherlands
 Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
EVAS How does this Impact EVAR Therapy
 EVAS How does this Impact EVAR Therapy John S. Lane III, MD, FACS Professor and Acting Chief of Vascular Surgery University of California, San Diego PNEC, 2017 Endologix products and associated components
EVAS How does this Impact EVAR Therapy John S. Lane III, MD, FACS Professor and Acting Chief of Vascular Surgery University of California, San Diego PNEC, 2017 Endologix products and associated components
Influence of patient selection and IFU compliance on outcomes following EVAS
 Influence of patient selection and IFU compliance on outcomes following EVAS LUNCH SYMPOSIUM LINC 2017 Jan MM Heyligers, MD, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg,
Influence of patient selection and IFU compliance on outcomes following EVAS LUNCH SYMPOSIUM LINC 2017 Jan MM Heyligers, MD, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg,
Ovation. Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic
 Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Degeneration of the Neck Post Implementation - a New Era of AAA Stent
 Degeneration of the Neck Post Implementation - a New Era of AAA Stent New Mexico Heart Institute Albuquerque, New Mexico USA - Gore Current FDA-Approved EVAR Devices Sealing Mechanism Endologix Lombard
Degeneration of the Neck Post Implementation - a New Era of AAA Stent New Mexico Heart Institute Albuquerque, New Mexico USA - Gore Current FDA-Approved EVAR Devices Sealing Mechanism Endologix Lombard
EndoAnchors: Endovascular Stitching During EVAR and TEVAR
 EndoAnchors: Endovascular Stitching During EVAR and TEVAR BY JEAN-PAUL P. M. de VRIES, MD, PhD THE EVOLUTION OF ENDOVAS- CULAR REPAIR IS CHARACTER- IZED BY INNOVATION Endovascular aneurysm repair (EVAR)
EndoAnchors: Endovascular Stitching During EVAR and TEVAR BY JEAN-PAUL P. M. de VRIES, MD, PhD THE EVOLUTION OF ENDOVAS- CULAR REPAIR IS CHARACTER- IZED BY INNOVATION Endovascular aneurysm repair (EVAR)
EVAR replaced standard repair in most cases. Why?
 EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
14F OD Ovation Abdominal Stent Graft System
 14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
TriVascular Ovation Prime Abdominal Stent Graft System
 TriVascular Ovation Prime Abdominal Stent Graft System Science of the Seal O-Ring Sealing Technology O-Ring Sealing in Proven Engineering Solutions O-rings are designed to seal by blocking the flow of
TriVascular Ovation Prime Abdominal Stent Graft System Science of the Seal O-Ring Sealing Technology O-Ring Sealing in Proven Engineering Solutions O-rings are designed to seal by blocking the flow of
Lessons learned from Ch-EVAR for the treatment of. Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly
 Lessons learned from Ch-EVAR for the treatment of pararenal AAAs Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly Ch-EVAR Ch-EVAR = Chimney-EVAR Placement of single
Lessons learned from Ch-EVAR for the treatment of pararenal AAAs Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly Ch-EVAR Ch-EVAR = Chimney-EVAR Placement of single
Predictors of abdominal aortic aneurysm sac enlargement after EVAR Longterm results from the ENGAGE Registry
 Predictors of abdominal aortic aneurysm sac enlargement after EVAR Longterm results from the ENGAGE Registry D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg Disclosure
Predictors of abdominal aortic aneurysm sac enlargement after EVAR Longterm results from the ENGAGE Registry D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg Disclosure
History of the Powerlink System Design and Clinical Results. Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ
 History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
The Ventana Off-the-Shelf Graft for Pararenal AAA. Andrew Holden Associate Professor of Radiology Auckland Hospital
 The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
EXPERIENCE AFTER 500 ENDOLUMINAL STENT GRAFTS. DEVICES SPECIFIC OUTCOME AND LESSONS LEARNED.
 EXPERIENCE AFTER 500 ENDOLUMINAL STENT GRAFTS. DEVICES SPECIFIC OUTCOME AND LESSONS LEARNED. A/Prof. B. Patrice Mwipatayi MD, MMed (Surg), MClinEd (Melb), FCS, FRACS Department of Vascular Surgery, Royal
EXPERIENCE AFTER 500 ENDOLUMINAL STENT GRAFTS. DEVICES SPECIFIC OUTCOME AND LESSONS LEARNED. A/Prof. B. Patrice Mwipatayi MD, MMed (Surg), MClinEd (Melb), FCS, FRACS Department of Vascular Surgery, Royal
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
AAA: DEBATE THERE ARE NO LIMITS USING EVAR FOR AAA. 2 nd -3 rd June 2016.
 AAA: DEBATE THERE ARE NO LIMITS USING EVAR FOR AAA JORGE FERNÁNDEZ NOYA ANGIOLOGY AND VASCULAR SURGERY DEPARTMENT UNIVERSITARY CLINICAL HOSPITAL SANTIAGO DE COMPOSTELA 2 nd -3 rd June 2016. 1888 ENDOANEURYSMORRHAPHY
AAA: DEBATE THERE ARE NO LIMITS USING EVAR FOR AAA JORGE FERNÁNDEZ NOYA ANGIOLOGY AND VASCULAR SURGERY DEPARTMENT UNIVERSITARY CLINICAL HOSPITAL SANTIAGO DE COMPOSTELA 2 nd -3 rd June 2016. 1888 ENDOANEURYSMORRHAPHY
NEW INNOVATIONS IN ENDOLEAK MANAGEMENT
 DISCLOSURES NEW INNOVATIONS IN ENDOLEAK MANAGEMENT Kelley HodgkissHarlow, MD, RPVI, FACS Vascular and Endovascular Surgery Kaiser Permanente, San Diego Nothing to disclose GOALS BACKGROUND Background Surveillance
DISCLOSURES NEW INNOVATIONS IN ENDOLEAK MANAGEMENT Kelley HodgkissHarlow, MD, RPVI, FACS Vascular and Endovascular Surgery Kaiser Permanente, San Diego Nothing to disclose GOALS BACKGROUND Background Surveillance
Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully
 Full thickness woven polyester graft material Fully") Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Trattamento Endovascolare degli Aneurismi dell Aorta Addominale con Colletto Prossimale Ostile:
 Trattamento Endovascolare degli Aneurismi dell Aorta Addominale con Colletto Prossimale Ostile: Risultati Precoci e a Medio Termine in Esperienza Monocentrica A.Lauricella - R.Silingardi Chirurgia Vascolare,
Trattamento Endovascolare degli Aneurismi dell Aorta Addominale con Colletto Prossimale Ostile: Risultati Precoci e a Medio Termine in Esperienza Monocentrica A.Lauricella - R.Silingardi Chirurgia Vascolare,
Hostile Proximal Neck: A New Conformable EVAR Device
 Hostile Proximal Neck: A New Conformable EVAR Device Young-Guk Ko, M.D., Seoul, Korea Currently Available Devices for EVAR in Korea, 2018 Zenith Flex, Cook Endurant IIs, Medtronic INCRAFT, Cordis AFX2,
Hostile Proximal Neck: A New Conformable EVAR Device Young-Guk Ko, M.D., Seoul, Korea Currently Available Devices for EVAR in Korea, 2018 Zenith Flex, Cook Endurant IIs, Medtronic INCRAFT, Cordis AFX2,
Faculty Disclosure. Glue, Particulates, Thrombin, Coils and the Kitchen Sink for Type II Endoleak Management. Background.
 Glue, Particulates, Thrombin, Coils and the Kitchen Sink for Type II Endoleak Management Faculty Disclosure I disclose the following financial relationships: UCSF Vascular Symposium 2013 Receive grant/research
Glue, Particulates, Thrombin, Coils and the Kitchen Sink for Type II Endoleak Management Faculty Disclosure I disclose the following financial relationships: UCSF Vascular Symposium 2013 Receive grant/research
What does the data tell us about outcomes of EVAR in challenging anatomy?
 What does the data tell us about outcomes of EVAR in challenging anatomy? UCSF Vascular Surgery Symposium 2018 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery Co-director, Comprehensive Aortic
What does the data tell us about outcomes of EVAR in challenging anatomy? UCSF Vascular Surgery Symposium 2018 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery Co-director, Comprehensive Aortic
Management of Endoleaks
 Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Endovascular Treatment of the Aorta with Fenestrated and Branched Grafts
 Endovascular Treatment of the Aorta with Fenestrated and Branched Grafts Eric LG Verhoeven,MD, PhD, A. Katsargyris, MD Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany
Endovascular Treatment of the Aorta with Fenestrated and Branched Grafts Eric LG Verhoeven,MD, PhD, A. Katsargyris, MD Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany
Access More Patients. Customize Each Seal.
 Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
Durable outcomes. Proven performance.
 Durable outcomes. Proven performance. GORE EXCLUDER AAA Endoprosthesis GORE EXCLUDER Iliac Branch Endoprosthesis GORE EXCLUDER AAA Endoprosthesis The most-studied* EVAR stent graft designed for durable
Durable outcomes. Proven performance. GORE EXCLUDER AAA Endoprosthesis GORE EXCLUDER Iliac Branch Endoprosthesis GORE EXCLUDER AAA Endoprosthesis The most-studied* EVAR stent graft designed for durable
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry
 University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
INCRAFT system: Update from the Pivotal INSPIRATION Study
 INCRAFT system: Update from the Pivotal INSPIRATION Study Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh
INCRAFT system: Update from the Pivotal INSPIRATION Study Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh
Overcoming Challenging Aortic Anatomy: from Hostile Necks to Tortuous Iliac arteries
 Overcoming Challenging Aortic Anatomy: from Hostile Necks to Tortuous Iliac arteries Robert Fisher Royal Liverpool University Hospital, UK Liverpool Vascular and Endovascular Service Introduction Late
Overcoming Challenging Aortic Anatomy: from Hostile Necks to Tortuous Iliac arteries Robert Fisher Royal Liverpool University Hospital, UK Liverpool Vascular and Endovascular Service Introduction Late
Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type 1b Endoleak following an EVAR for Ruptured AAA
 Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
LOWERING THE PROFILE RAISING THE BAR
 LOWERING THE PROFILE RAISING THE BAR INNOVATIVE LOW PROFILE. ADVANCED CLINICAL PERFORMANCE. The AFX TM Endovascular AAA System integrates anatomical fixation with an advanced delivery system and graft
LOWERING THE PROFILE RAISING THE BAR INNOVATIVE LOW PROFILE. ADVANCED CLINICAL PERFORMANCE. The AFX TM Endovascular AAA System integrates anatomical fixation with an advanced delivery system and graft
Low profile TEVAR: is it an added value? Michel Bosiers, G. Torsello Münster
 Low profile TEVAR: is it an added value? Michel Bosiers, G. Torsello Münster Disclosure Speaker name:...michel Bosiers... I have the following potential conflicts of interest to report: Consulting Employment
Low profile TEVAR: is it an added value? Michel Bosiers, G. Torsello Münster Disclosure Speaker name:...michel Bosiers... I have the following potential conflicts of interest to report: Consulting Employment
Approaches to type II Endoleaks: Transcaval, transarterial, translumbar. Saher Sabri,MD University of Virginia
 Approaches to type II Endoleaks: Transcaval, transarterial, translumbar Saher Sabri,MD University of Virginia Saher Sabri, M.D. Speakers Bureau: W.L.Gore & Associates, Abbott Type 2 Endoleaks after EVAR
Approaches to type II Endoleaks: Transcaval, transarterial, translumbar Saher Sabri,MD University of Virginia Saher Sabri, M.D. Speakers Bureau: W.L.Gore & Associates, Abbott Type 2 Endoleaks after EVAR
EVAS using Nellix in my practice Where are we today?
 EVAS using Nellix in my practice Where are we today? Prof. dr. Michel MPJ Reijnen Department of Vascular Surgery, Rijnstate Hospital Arnhem Faculty of Science and Technology, University of Twente The Netherlands
EVAS using Nellix in my practice Where are we today? Prof. dr. Michel MPJ Reijnen Department of Vascular Surgery, Rijnstate Hospital Arnhem Faculty of Science and Technology, University of Twente The Netherlands
Why Nellix? Treating Concomitant Common Iliac Aneurysms
 INDICATIONS FOR USE The Nellix EndoVascular Aneurysm Sealing System can be used in patients who have an infrarenal abdominal aortic (AAA) or aortoiliac aneurysm with suitable anatomy as indicated below:
INDICATIONS FOR USE The Nellix EndoVascular Aneurysm Sealing System can be used in patients who have an infrarenal abdominal aortic (AAA) or aortoiliac aneurysm with suitable anatomy as indicated below:
ChEVAR Vs. fevar for juxtarenal Aneurysm. E.Ducasse MD PhD FEVBS Unit of vascular surgery CHU bordeaux
 ChEVAR Vs. fevar for juxtarenal Aneurysm E.Ducasse MD PhD FEVBS Unit of vascular surgery CHU bordeaux CH-EVAR VS. F-EVAR IN JAAAs Meta-analysis, 2001-2012 5 CH-EVAR studies (94 patients, 151 target vessels)
ChEVAR Vs. fevar for juxtarenal Aneurysm E.Ducasse MD PhD FEVBS Unit of vascular surgery CHU bordeaux CH-EVAR VS. F-EVAR IN JAAAs Meta-analysis, 2001-2012 5 CH-EVAR studies (94 patients, 151 target vessels)
Accessi Iliaci Ostili
 Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery Accessi Iliaci Ostili nel trattamento della patologia aortica E. Gallitto Iliac Navigations Alma Mater Studiorum
Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery Accessi Iliaci Ostili nel trattamento della patologia aortica E. Gallitto Iliac Navigations Alma Mater Studiorum
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry
 Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan
 The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
Is EVAS a proper choice in women?
 Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
Zenith Renu AAA Converter Graft. Device Description Planning and Sizing Deployment Sequence Patient Follow-Up
 Zenith Renu AAA Converter Graft Device Description Planning and Sizing Deployment Sequence Patient Follow-Up Device description: Device indications The Zenith Renu AAA Converter Graft with Z-Trak Introduction
Zenith Renu AAA Converter Graft Device Description Planning and Sizing Deployment Sequence Patient Follow-Up Device description: Device indications The Zenith Renu AAA Converter Graft with Z-Trak Introduction
When and where EVAR patients should be discharged?
 When and where EVAR patients should be discharged? Joost A. van Herwaarden University Medical Center Utrecht The Netherlands Disclosure of Interest I have the following potential conflicts of interest
When and where EVAR patients should be discharged? Joost A. van Herwaarden University Medical Center Utrecht The Netherlands Disclosure of Interest I have the following potential conflicts of interest
NASDAQ: ELGX December Innovation that Empowers
 NASDAQ: ELGX www.endologix.com December 2014 Innovation that Empowers Safe Harbor This presentation contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act
NASDAQ: ELGX www.endologix.com December 2014 Innovation that Empowers Safe Harbor This presentation contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act
Case Report A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after Endovascular Aneurysm Repair with the Chimney Technique
 Case Reports in Vascular Medicine Volume 2016, Article ID 5307416, 4 pages http://dx.doi.org/10.1155/2016/5307416 Case Report A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after
Case Reports in Vascular Medicine Volume 2016, Article ID 5307416, 4 pages http://dx.doi.org/10.1155/2016/5307416 Case Report A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after
Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair
 583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
EVAS is Associated with Lower All-Cause Mortality
 EVAS is Associated with Lower All-Cause Mortality Marc L Schermerhorn, MD Chief, Division of Vascular and Endovascular Surgery Beth Israel Deaconess Medical Center Professor of Surgery Harvard Medical
EVAS is Associated with Lower All-Cause Mortality Marc L Schermerhorn, MD Chief, Division of Vascular and Endovascular Surgery Beth Israel Deaconess Medical Center Professor of Surgery Harvard Medical