Metabolic Muscle Diseases
|
|
|
- Amice O’Neal’
- 5 years ago
- Views:
Transcription
1 Metabolic Muscle Diseases Dr Tim Hutchin, Birmingham Children s Hospital Jan 13, 2012

2 Metabolic myopathies are heterogeneous conditions with defects of muscle energy metabolism that result in predominantly skeletal muscle dysfunction but other muscles may be affected. Most are considered primary inborn errors of metabolism and are associated with enzymatic defects that affect the ability of muscle fibres to maintain adequate ATP supplies. Muscle contraction and relaxation require ATP
3 Liver glycogen Sources of ATP for muscle Phosphocreatine Glycogen Creatine Quick supply Contraction Glucose Glucose Glycolysis Myosin ATPase Lactic acid Pyruvate ATP Ca2 + ATPase Fatty acids Amino acids Oxidative phosphorylation Relaxation Protein Fat stores
4 Three types of muscle: Smooth muscle or "involuntary muscle" is found within the walls of organs and structures such as the oesophagus, stomach, intestines, uterus, bladder, blood vessels. No real energy stores. Cardiac muscle an "involuntary muscle" but more akin in structure to skeletal muscle. It contracts quite slowly, but it is used continuously and the total energy consumption is high. Totally specialized for energy production (30-40% of ventricular mass is made up of mitochondria). No real energy stores. Skeletal muscle or "voluntary muscle" is used to effect skeletal movement such as locomotion and in maintaining posture. Main energy stores are glycogen (3/4 of body s glycogen)
5 3 major pathways supply exercising muscle with ATP 1. Phosphocreatine stores provide rapid but very brief supply (~1-5 minutes) 2. Glycogen metabolism: anaerobic metabolism can then supply ATP but for more sustained activity aerobic metabolism is utilised as long as oxygen supplies meet demand. 3. Fatty acid metabolism is utilised for sustained submaximal exercise (ie >40 minutes).

6 Muscle Fibres for Different Jobs Type I fibres Type II a fibres Type II b fibres Contraction time Slow twitch Fast twitch Very fast twitch Resistance to fatigue Used for Mitochondrial density Oxidative capacity Glycolytic capacity High Fairly high Low Aerobic Marathon runners fibres Long-term anaerobic General purpose fibres Short-term anaerobic Sprinters fibres High High Low High High Low Low High High Myoglobin High High Low Glycogen content Major storage fuel Low Intermediate High Triglycerides Creatine phosphate, glycogen Creatine phosphate, glycogen
7 Inherited Disorders of Muscle Disease Structural Defects Defects in proteins involved in maintaining muscle tone and the contraction process (myopathies) e.g. muscular dystrophies, congenital myopathies. Membrane Transport Defects Defects in ion or neurotransmitter transport proteins or receptors (Channelopathies), e.g. myotonia congenita, hyper and hypokalemic periodic paralysis Metabolic Myopathies Defects in enzymes involved in muscle metabolism leading to energy depletion or structural damage.
8 Metabolic Muscle Disease Inherited disorders of metabolic pathways. Muscle is an ATP generating factory. Metabolic muscle disease causes either: Energy (ATP) depletion: Anaerobic (glycogenolysis, glycolysis) Aerobic (fatty acid oxidation, electron transport chain) Structural damage: Accumulation of abnormal glycogen (lysosomal or cytoplasmic) Free radical damage
9 Symptoms of Metabolic Metabolic myopathies have a wide range of symptom onset. Most present early in life (infancy to adolescence) Symptoms may be very mild (exercise intolerance) to fatal Generally, onset and severity depends on the disorder and degree of enzyme deficiency (complete or partial) Symptoms may be treatable Muscle Disease
10 Symptoms of Metabolic Muscle Disease Exercise intolerance Muscle pain (myalgia) after exercise Cramps Muscle damage Myoglobinuria Rhabdomyolysis ( CK) leading to renal failure Proximal muscle weakness Hypotonia Other organs may be affected
11 Further Symptoms of Metabolic Muscle Diseases Myoglobinuria: When overexertion triggers acute muscle breakdown (rhabdomyolysis), muscle proteins like creatine kinase and myoglobin are released into the blood and ultimately appear in the urine. Myoglobinuria can cause severe kidney damage if untreated. Malignant Hyperthermia: People with metabolic muscle disorders may be at higher risk for a potentially fatal reaction to certain common general anaesthetics. Cardiac Care: Some patients may develop significant heart problems. Respiratory Care: Some disorders may weaken the respiratory muscles that operate the lungs. These patients may require supplemental oxygen at some point.
12 Causes of metabolic muscle disease Glycogen storage disorders Chronic, progressive weakness with atrophy, cardiomegaly, hepatomegaly, macroglossia, respiratory dysfunction. Symptoms usually present after short period of exercise but may experience a second wind Lipid storage disorders Muscle weakness and pain, myoglobinuria, exercise intolerance. Symptoms usually present after prolonged period of exercise Purine recycling disorders Mitochondrial Enzyme deficiencies Multisystemic disorders. Very variable. Muscle weakness, exercise intolerance, hearing loss, seizures, ataxia, pigmentary retinopathy, cardiomyopathy
13 Carbohydrate Processing Disorders Glycogen synthase (GSD 0) (GSD IV) Brancher UDP-Glucose Glycogen GSD V (& VI) Glycogen debrancher Glucose-1P Glycogen Phosphorylase b inactive Phosphorylase b kinase Phosphorylase b active GSD IX GSD III GSD II Lysosome a-glucosidase Glucose GSD VII Phosphofructokinase Glucose-6-P Fructose-6-P Glucose 6- Phosphatase Glucose (GSD I) ER Glucose GSD XII Aldolase A Phosphoglycerate mutase GSD X GSD XIII b-enolase Fructose-1,6-P Lactate GSD XI Lactate dehydrogenase TCA cycle Pyruvate Acetyl CoA Fatty acids TGs
14 Glycogen Storage Disorders Predominantly muscle GSD II - acid a-glucosidase - Proximal muscle weakness More severe infantile form (cardiomegaly & hypotonia) GSD V - muscle phosphorylase - Exertional muscle weakness GSD VII - muscle phosphfoructokinase - Exertional muscle weakness GSD IXd - muscle phosphorylase b kinase - Exertional muscle weakness and cardiomyopathy Liver and Muscle GSD IIIa - debranching enzyme GSD IXb - phosphorylase b kinase Predominantly hepatic GSD 0 - glycogen synthase GSD I - glucose 6-phosphatatase or transport systems in ER GSD IIIb - debranching enzyme GSD IV - branching enzyme GSD VI - liver phosphorylase GSD IXa,c - liver phosphorylase b kinase
15 Glycogen storage disease II (Pompe) Clinical Infantile: Hypotonia, macroglossia, hepatomegaly, cardiomegaly and congestive heart failure, FTT. Death within 2 years due to cardiorespiratory failure. Incidence 1:130,000 Juvenile: Weakness, developmental delay, respiratory muscle affected but not cardiac. Adult: Slowly progressive myopathy after 20 years of age, symptoms of respiratory failure, diaphragm involvement leads to sleep apnea. Cardiac is normal. Incidence 1:57,000 Onset Defect Inheritance Laboratory findings Infantile to adulthood Acid a-glucosidase (Acid maltase). Lysosomal enzyme that breaks down glycogen Autosomal recessive Elevated CK, AST, LDH, particularly the infantile onset. Glycogen storage on histology.
16 Glycogen storage disease V (McArdle s) Clinical Onset Defect Inheritance Laboratory findings Muscle cramps/ pain after brief exercise Resting may lead to a second wind Rhabdomyolysis Myoglobinuria coke cola urine Most common GSD- 1:350,000 to 1:100,000. Susceptible to malignant hyperthermia. Phenotype modulated by myoadenylate deaminase gene Childhood to adulthood (usually diagnosed in adulthood) Muscle glycogen phosphorylase (PYGM). Removes glucose residues from a-(1,4)-linkages in glycogen Autosomal recessive (R50X mutation accounts for 60% of Caucasian mutations) Raised CK (up to 13,000), even at rest Raised ammonia, potassium and uric acid with exercise No increase in lactate in ischaemic forearm test
17 Glycogen storage disease III (Cori or Forbes) Clinical Type IIIa (85%) liver and muscle involvement Type IIIb (15%) liver only Onset Defect Inheritance Laboratory findings Hepatomegaly Muscle weakness Cardiomyopathy Growth retardation Hypoglycaemic seizures Childhood - adulthood Defect in amylo-1,6-glucosidase (AGL) gene- Debrancher Removes glucose from a-(1,6)-linkages in glycogen Autosomal recessive Hypoglycaemia Hyperlipidaemia Amino acids decreased- Ala, Leu, Ile, Val Transaminases Cholesterol CK may be raised
18 Glycogen storage disease VII (Tarui) Clinical Onset Defect Inheritance Laboratory findings Jaundice (due to haemolytic anaemia) Exercise intolerance Muscle weakness Muscle cramps with exertion Occasionally myoglobinuria Similar to McArdles but less likely to experience second wind Gout due to uric acid Childhood to adulthood Phosphofructokinase (Fructose-6-P Fructose-1,6-P) Autosomal recessive Myoglobinuria with extreme exertion Increased uric acid, CK, bilirubin, reticulocyte count Increased ammonia but not lactate with ischaemic exercise test
19 Glycogen phosphorylase b kinase Hexadecameric enzyme composed of 4 copies of 4 subunits. Activates glycogen phosphorylase in response to neuronal or hormonal stimuli Subunit Gene Expression Disorder Inheritance Affected tissues a PHKA1 Muscle GSD IXd X-linked Muscle PHKA2 Liver GSD IXa X-linked Liver b PHKB Muscle and liver GSD IXb Autosomal recessive g PHKG1 Muscle - Autosomal - PHFG2 Liver GSD IXc Autosomal recessive d CALM1 Ubiquitous - Autosomal - Muscle and liver Liver
20 Glycogen storage disease IX (Phosphorylase kinase) Clinical Onset Defect Inheritance Laboratory findings Variable, relatively mild Myalgia, cramps and weakness with exercise Myoglobinuria Some forms with hepatomegaly Childhood to adolescence Glycogen phosphorylase b kinase (activates glycogen phosphorylase). Autosomal recessive or X-linked Mild elevation of cholesterol, triglycerides, CK. Variable hypoglycaemia

21 Glycolytic Pathway Disorders GSD XII Aldolase A GSD X Phosphoglycerate mutase GSD XIII b-enolase GSD XI lactate Lactate dehydrogenase
22 Glycolytic Pathway Disorders Very rare, often only handful of cases reported. Usually present childhood to adolescence Autosomal recessive Multiple Isoforms of many enzymes Features may include: Exercise Intolerance Rhabdomyolysis Haemolytic Anaemias Increased CK
23 Glycolytic Pathway Disorders Phosphoglycerate Mutase deficiency (GSD X) Exercise intolerance, cramps, muscle pains. Sometimes myoglobinuria with intense exercise Lactate Dehydrogenase deficiency (GSD XI) Exercise intolerance, cramps, pains Rhabdomyolysis/ Myoglobinuria Skin rash Aldolase deficiency A (GSD XII) Exercise intolerance and proximal weakness Jaundice + anaemia Episodic myalgias and haemolysis b Enolase deficiency (GSD XIII) Myalgias
24 Fatty Acid Oxidation Defects Only defects affecting long chain fatty acid oxidation give muscle disease Paediatric forms usually have severe hypoglycaemia and may also have a hypertrophic cardiomyopathy and liver disease. Adult-onset forms often present without hypoglycaemia or cardiomyopathy. They usually have exercise intolerance and muscle weakness sometimes presenting with myoglobinuria or rhabdomyolysis. Metabolites are often normal even on fasting.
25 Carnitine and Fatty Acid Oxidation Carnitine OCTN2 Long chain Fatty Acid Carnitine Outer Mitochondrial membrane CoASH AcylCoA synth Acyl CoA Carnitine CPT 1 Acylcarnitine CoASH Carnitine Inner Mitochondrial membrane Acyl CoA CPT 2 CoASH CACT Carnitine Acylcarnitine Carnitine b-oxidation spiral
26 Carnitine Essential for the transport of fatty acids into the mitochondrion for oxidation. Deficient patients present with severe progressive cardiomyopathy and/or recurrent episodes of encephalopathy associated with hypoketotic hypoglycaemia and liver dysfunction. Skeletal muscle involvement may manifest as motor delay, hypotonia, or proximal limb weakness. Symptoms may be corrected when carnitine levels are raised with L-carnitine replacement Primary deficiency Defect in transport of carnitine into the cell. Can be systemic due to OCTN2 defect or restricted to muscle (? muscle carnitine transporter) Secondary Carnitine levels may be reduced by other disorders (fatty acid oxidation, organic acidurias, mitochondrial), malnutrition, renal failure (eg valproate therapy)
27 OCTN2 Clinical Onset Defect Inheritance Laboratory findings Cardiomyopathy Hepatomegaly Fatigability/ Muscle weakness Vomiting Abdominal pain Hypoglyaemia Episodic encephalomyopathy Infancy to first decade Organic Cation Transporter (OCTN2)- Na 2+ -dependent carnitine transporter- transports carnitine across cell membranes Autosomal recessive Plasma carnitine (total and free) low or absent Hyperammonaemia Hypoglycaemia
28 CACT Deficiency Clinical Onset Defect Inheritance Laboratory findings Encephalopathy Cardiomyopathy Muscle weakness Episodic neonatal apnoea Neonatal- usually fatal within months Carnitine-acylcarnitine translocase (SLC25A20) deficiency. Shuttles substrates between cytosol and intramitochondrial matrix space Autosomal recessive Hypoketosis (low ketones) Hypoglycaemia Hyperammonaemia Increase in plasma acylcarnitines (C16, C18) and low carnitine
29 Carnitine Palmitoyltransferase II- Late onset Clinical Onset Defect Muscle weakness, stiffness, cramps, pain following prolonged exercise or other stress (heat, cold, illness, fasting) Rhabdomyolysis (most common inherited cause) Adolescence or adulthood. Triggered by prolonged exercise or metabolic stresses, illness, cold Carnitine palmitoyl transferase II Inheritance Autosomal recessive Laboratory findings Raised CK after an attack Low free carnitine, normal total Increased phosphates, uric acid, AST. Increased ratio (C16+C18)/C2
30 Fatty Acid Oxidation Defects VLCADD MADD MTP
31 VLCAD Deficiency Clinical i) Severe early onset form with cardiomyopathy and hepatopathy ii) Hepatic phenotype manifests in infancy with recurrent episodes of hypoketotic hyperglycinaemia iii) Milder later onset myopathic form with episodic muscle weakness, myalgia and myoglobinuria with prolonged exercise Defect Very long chain Acyl-CoA dehydrogenase Inheritance Autosomal recessive Laboratory findings Increased acylcarnitines C14, ratio C14:1/C12:1 Dicarboxylic aciduria
32 Mild mitochondrial Tri-functional protein/ LCHAD Clinical i) Rapidly progressive neonatal onset, early death ii) Infantile onset with hepatic involvement iii) Childhood/ adolescent onset with myopathy and neuropathy Most patients die from heart failure Defect Inheritance a and b subunits of mitochondrial trifunctional proteincatalyses 3 reactions in fatty acid oxidation inc LCHAD Autosomal recessive Laboratory findings Increased acylcarnitines C14- C18
33 Riboflavin responsive MADD (Glutaric Aciduria 2) Clinical Onset Defect Inheritance Laboratory findings Recurrent vomiting Encephalopathy Muscle weakness proximal limbs, respiratory, dysphagia Infant to adulthood Multiple Acyl CoA Dehydrogenase (Electron Transfer Flavoprotein ETFDH). May be precipitated by poor diet of riboflavin Autosomal recessive Low plasma carnitine Ketosis MADD specific organic acid when symptomatic- Increased lactic, glutaric, ethylmalonic, dicarboxylic acids MADD specific carnitines (C4-C18) even when asymptomatic
34 Lipin 1 - a phosphatidate phosphatase in triglyceride and phospholipid synthesis and transcriptional co-activator for fatty acid oxidation HAT Lipin PPARa PCG1a Lipin Fatty acid oxidation genes GPAT = glycerol-3-phosphate acyltransferase AGPAT = 1-acylglycerol-3-phosphate acyltransferase DGAT = diacylglycerol acyltransferase
35 LPIN1 Deficiency Clinical Onset Defect Inheritance Laboratory findings Repeated attacks of rhabdomyolysis with myoglobinuria. Often precipitated by febrile illness, anaesthetic or fasting. Early childhood Lipin 1(LPIN1)- a phosphatidate phosphatase in triglyceride and phospholipid synthesis and a transcriptional co-activator for fatty acid oxidation Autosomal recessive. A moderately common gene deletion Increased CK

36 The Purine Nucleotide Cycle Myoadenylate deaminase
37 Disorders of Purine Nucleotide Metabolism The purine nucleotide cycle serves to replenish TCA and glycolytic intermediates when energy demand is high. Reaction occurs mainly during aerobic exercise to replenish ATP. Supply of aspartate is high and is constantly replenished from blood or internal muscle protein stores.
38 Myoadenylate Deaminase Deficiency Clinical Onset Defect Inheritance Laboratory findings Most patients asymptomatic (1-2% of Europeans are homozygous for a mutation giving <10% activity) Exercise induced myopathy Post-exertional muscle weakness or cramping Prolonged fatigue after exercise Adulthood Myoadenylate deaminase (adenosine monophosphate deaminase) Autosomal recessive. Common mutation (can also modulate disease severity in McArdle s disease) Increased CK. No increase in ammonia in ischaemic forearm test

39 Symptoms of Respiratory Chain Disorders Exercise Intolerance Cardiomyopathy Neurological Symptoms Ophthalmoplegia Endocrine Abnormalities Failure to thrive Impaired gut motility Dysmorphic Features
40 Electron Transport Chain Mitochondrial inner membrane Matrix I CoQ II III CytC IV (COX) IV NADH FADH2 O 2 H 2 0 ATP Succinate Pyruvate Fatty Acids TCA Cycle Acetyl CoA
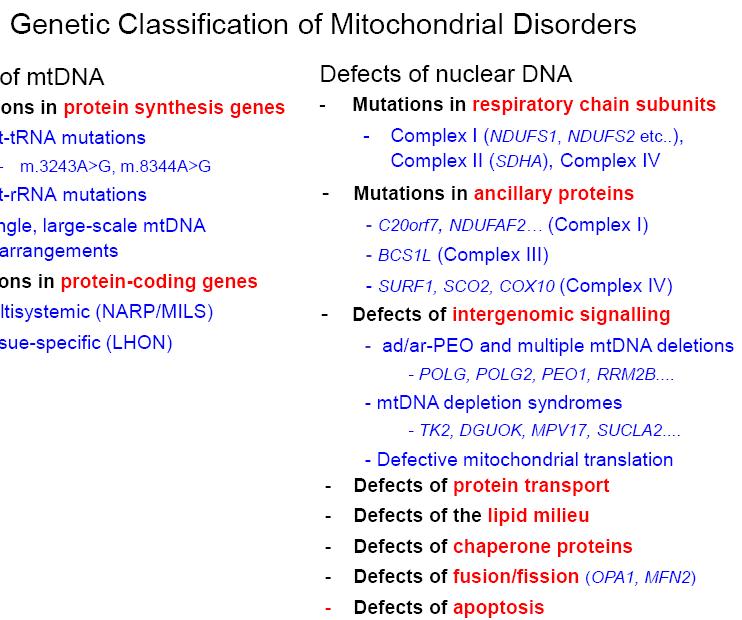

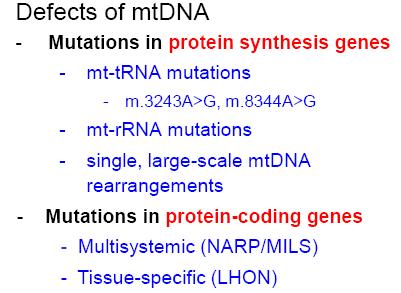
41 Genetic Classification of Mitochondrial Diseases
42 Mutations of mtdna can cause muscle disease MELAS: mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes Inheritance pattern: maternal Onset: childhood to early adulthood Features: Recurrent stroke-like episodes, migraine-like headaches, vomiting and seizures. Other symptoms include PEO, general muscle weakness, exercise intolerance, hearing loss, diabetes and short stature. MERRF: myoclonus epilepsy with ragged red fibres Inheritance pattern: maternal Onset: late childhood to adolescence Features: myoclonus (muscle jerks), seizures, ataxia and muscle weakness. Can cause hearing impairment and short stature. KSS: Kearns-Sayre syndrome Inheritance pattern: sporadic (deletions in mtdna) Onset: before age 20 Features: Defined by PEO and pigmentary retinopathy. Other symptoms include cardiac conduction block, ataxia and proximal muscle weakness.
43 mtdna Depletion Syndromes Characterized by a reduction in mtdna copy number (15-20% of normal). May be relatively common neurogenetic disorder of infancy (up to 10% of referrals for weakness, hypotonia and developmental delay) Phenotypically heterogeneous: Hepatocerebral form Myopathic form Benign later onset myopathic form Cardiomyopathic form Muscle weakness, and/or liver failure, and more rarely, brain abnormalities. Lactic acidosis, hypotonia, feeding difficulties, and developmental delays are common; PEO and seizures are less common. Typically early onset and death
44 mtdna Depletion Syndromes Primarily due to enzymes involved in maintenance of mtdna copy number, e.g. nucleotide synthesis or mtdna replication. Inheritance: Many causes, usually recessive, can be dominant or sporadic. Biochemical features may include: olactic acidosis in more severe cases. omethylmalonic aciduria in some forms oserum CK: Mildly, or Prominently elevated to > 1,000 omitochondrial changes in muscle Low activity: Complex I, III, IV Normal activity: Complex II
45 mtdna Depletion Syndromes Disorder Gene Product Function Phenotype MTDPS1 TYMP Thymidine phosphorylase dntp pools MTDPS2 TK2 Thymidine kinase dntp pools Myopathic MTDPS3 DGUOK Deoxyguanosine kinase dntp pools MNGIE (mitochondrial neurogastrointestinal encephalomyopathy) Hepatocerebral MTDPS4 POLG Polymerase gamma mtdna replication Hepatocerebral/ Alpers MTDPS5 SUCLA2 Succinyl-CoA synthase dntp pools Encephalomyopathic with MMA MTDPS6 MPV17 -? Hepatocerebral MTDPS7 PEO1 (Twinkle) MTDPS8 RRM2B Ribonucleotide reductase M2B MTDPS9 SUCLG1 Succinate-CoA ligase a subunit? DNA Helicase mtdna replication Hepatocerebral dntp pools dntp pools Encephalomyopathic with renal tubulopathy Fatal infantile lactic acidosis with MMA
46 Mitochondrial neurogastrointestinal encephalomyopathy (MNGIE) Clinical PEO Ptosis Limb weakness Gastrointestinal (digestive) problems, including pseudo-obstruction, chronic diarrhoea and abdominal pain. Peripheral neuropathy. Onset Defect Inheritance Laboratory findings Childhood to adulthood Thymidine phosphorylase (TYMP) Autosomal recessive Increased serum thymidine and deoxyuridine
47 Clinical Diagnosis of Muscle Disease A multi-disciplinary approach Physiology / Electrophysiology (can rule out other disorders) Magnetic Resonance Imaging & Spectroscopy Histopathology (histology & immunocytochemistry) Biochemistry (metabolites and enzymes) Genetics (can allow genetic counselling and testing in family members) Haematology
48 Biochemical Abnormalities Elevated creatine kinase (intermittent) Elevated troponin (Heart or Muscle?) Hypoglycaemia Abnormal LFTs (sometimes due to muscle damage!) Myoglobinuria (cola- coloured urine) Increased plasma lactate Increased cholesterol & triglycerides Increased plasma urate. Abnormal acylcarnitines Abnormalities may be present only during an attack
49 Clinical Investigations Family history Neurological Cardiac *Gastrointestinal *Ophthalmology *Audiology 1 st line Biochemical Investigations Plasma Urine CSF* Lactate Amino acids Lactate Creatine kinase Organic acids Amino Acids Acylcarnitines Free carnitine *esp for mitochondrial Consider additional testing (non invasive) Exercise testing Forearm exercise test EMG, ECG, MRS
50 Glycogenoses Early exercise intolerance (e.g. cramps/ pain/ myoglobinuria) CK usually chronically raised Other first line tests normal Respiratory muscles may be involved, e.g. late onset Pompe Biochemistry Glucose Urate LFTs Lipids FBC Blood Mutation analysis for GSD V GSD enzymes Muscle biopsy Histology and enzyme assay where indicated
51 Fatty Acid Oxidation defects Exercise intolerance (e.g. pain/stiffness/ myoglobinuria)- typically on prolonged/ sustained exercise. Exacerbated by poor food intake/ stress/ illness CK usually normal between episodes Plasma acylcarnitines may be abnormal Urine organic acids may be abnormal Blood Common mutation in CPT2 Skin biopsy Fatty acid oxidation flux assays Specific CPT2 enzyme assay
52 Purine cycle defects Exercise intolerance (e.g. cramps/pain) CK usually normal between episodes Other first line tests normal Blood Mutation analysis for myoadenylate deaminase (AMPD1) Muscle biopsy Need to exclude other causes as this is common
53 Mitochondrial Respiratory Chain defects Exercise intolerance, occasionally myoglobinuria Often more than one organ affected Normal or raised lactate (plasma and CSF) and CK May have abnormal organic acids (e.g. TCA intermediates, MMA) Normal or raised plasma alanine, reflecting lactic acidaemia May have generalised amino aciduria Blood Mutation analysis for common mtdna mutations Muscle Biopsy Respiratory chain complexes assay May include ubiquinone and mtdna depletion studies Histology may have ragged red fibres or show decreased staining for some complexes


54 Ragged Red Fibres Gomori trichrome stain Muscle fibres with mitochondrial proliferation stain as red



55 Cytochrome Oxidase staining Normal COX deficient Type I fibres stain more darkly than type II. COX negative muscle fibres may have increased staining of SDH
56 The Ischaemic Exercise Test Test for glycolytic defects, esp McArdles Restrict blood flow to arm muscle Ask patient to exercise arm Collect blood samples pre and at specified intervals post exercise. Measure lactate, creatine kinase, ammonia: Normal response: 3-5 fold rise in lactate and ammonia. Glycolytic defect: No increase in lactate MAD defect: No increase in ammonia Fatty Acid defect: Normal response
57 Treatment of Metabolic Myopathies Dietary/ supplements Glucose Medium Chain Triglycerides Carnitine supplements CoQ10 Creatine Enzyme replacement therapy, e.g. Pompe Disease Exercise training to stimulate anaerobic or aerobic pathways
58 Other factors to note Lipid lowering drugs (e.g. statins) can induce myopathy/ rhabdomyolysis in some muscle disorders such as MAD, GSD V and CPT2. Patients with muscle disorders such as McArdles and CPT2 may be at risk of malignant hyperthermia (causes a fast rise in body temperature and severe muscle contractions when the affected person gets general anaesthesia). The common MAD mutation can worsen the phenotype of some muscle disease patients.
59 SUMMARY Muscle function requires ATP. Sources of ATP are creatine kinase, carbohydrates (aerobic and anaerobic) and fatty acids. Defects in supply of ATP can cause muscle disease. Symptoms and onset vary widely and may include: Exercise intolerance (after brief exercise in carbohydrate disorders or sustained exercise in fatty acid disorders) Cramps/ pains Rhabdomyolysis Diagnosis requires a multidisciplinary approach: Physiology Biochemistry/ enzymology Histology DNA
Non-Lysosomal Glycogen Storage Disorders Biochemical Diagnosis
 Non-Lysosomal Glycogen Storage Disorders Biochemical Diagnosis Katie Bainbridge Enzyme Laboratory Great Ormond Street Hospital Glycogen Metabolism Glycogen Glycogen -glucosidase Lysosome Brancher Glycogen
Non-Lysosomal Glycogen Storage Disorders Biochemical Diagnosis Katie Bainbridge Enzyme Laboratory Great Ormond Street Hospital Glycogen Metabolism Glycogen Glycogen -glucosidase Lysosome Brancher Glycogen
Muscle Metabolism. Dr. Nabil Bashir
 Muscle Metabolism Dr. Nabil Bashir Learning objectives Understand how skeletal muscles derive energy at rest, moderate exercise, and strong exercise. Recognize the difference between aerobic and anaerobic
Muscle Metabolism Dr. Nabil Bashir Learning objectives Understand how skeletal muscles derive energy at rest, moderate exercise, and strong exercise. Recognize the difference between aerobic and anaerobic
Presentation and investigation of mitochondrial disease in children
 Presentation and investigation of mitochondrial disease in children Andrew Morris Willink Unit, Manchester Mitochondrial function Carbohydrate Fat Respiratory chain Energy Mitochondria are the product
Presentation and investigation of mitochondrial disease in children Andrew Morris Willink Unit, Manchester Mitochondrial function Carbohydrate Fat Respiratory chain Energy Mitochondria are the product
REQUISITION FORM NOTE: ALL FORMS MUST BE FILLED OUT COMPLETELY FOR SAMPLE TO BE PROCESSED. Last First Last First
 #: DEPARTMENT OF NEUROLOGY COLUMBIA COLLEGE OF PHYSICIANS & SURGEONS Room 4-420 630 West 168th Street, New York, NY 10032 Telephone #: 212-305-3947 Fax#: 212-305-3986 REQUISITION FORM NOTE: ALL FORMS MUST
#: DEPARTMENT OF NEUROLOGY COLUMBIA COLLEGE OF PHYSICIANS & SURGEONS Room 4-420 630 West 168th Street, New York, NY 10032 Telephone #: 212-305-3947 Fax#: 212-305-3986 REQUISITION FORM NOTE: ALL FORMS MUST
e-learning Fatty Acid Oxidation Defects Camilla Reed and Dr Simon Olpin Sheffield Children s Hospital
 e-learning Fatty Acid Oxidation Defects Camilla Reed and Dr Simon Olpin Sheffield Children s Hospital Fatty Acids Fatty acids are a major source of energy and body fat is an energy dense material. They
e-learning Fatty Acid Oxidation Defects Camilla Reed and Dr Simon Olpin Sheffield Children s Hospital Fatty Acids Fatty acids are a major source of energy and body fat is an energy dense material. They
Nutritional Interventions in Primary Mitochondrial Disorders
 Nutritional Interventions in Primary Mitochondrial Disorders Carolyn J Ellaway MBBS PhD FRACP CGHGSA Genetic Metabolic Disorders Service Sydney Children s Hospital Network Disciplines of Child and Adolescent
Nutritional Interventions in Primary Mitochondrial Disorders Carolyn J Ellaway MBBS PhD FRACP CGHGSA Genetic Metabolic Disorders Service Sydney Children s Hospital Network Disciplines of Child and Adolescent
Robert Barski. Biochemical Genetics St James s University Hospital, Leeds. MetBioNet IEM Introductory Training
 Robert Barski Biochemical Genetics St James s University Hospital, Leeds Lactate is produced as the fate of anaerobic metabolism of pyruvate. It is an important intermediary metabolite especially with
Robert Barski Biochemical Genetics St James s University Hospital, Leeds Lactate is produced as the fate of anaerobic metabolism of pyruvate. It is an important intermediary metabolite especially with
CHY2026: General Biochemistry UNIT 7& 8: CARBOHYDRATE METABOLISM
 CHY2026: General Biochemistry UNIT 7& 8: CARBOHYDRATE METABOLISM Metabolism Bioenergetics is the transfer and utilization of energy in biological systems The direction and extent to which a chemical reaction
CHY2026: General Biochemistry UNIT 7& 8: CARBOHYDRATE METABOLISM Metabolism Bioenergetics is the transfer and utilization of energy in biological systems The direction and extent to which a chemical reaction
Biochemistry #02. The biochemical basis of skeletal muscle and bone disorders Dr. Nabil Bashir Bara Sami. 0 P a g e
 ]Type text[ ]Type text[ ]Type text[ Biochemistry #02 The biochemical basis of skeletal muscle and bone disorders Dr. Nabil Bashir Bara Sami 0 P a g e Greetings everyone, ladies and gentlemen The biochemical
]Type text[ ]Type text[ ]Type text[ Biochemistry #02 The biochemical basis of skeletal muscle and bone disorders Dr. Nabil Bashir Bara Sami 0 P a g e Greetings everyone, ladies and gentlemen The biochemical
Metabolic Muscle Disease
 Metabolic Muscle Disease Dr. Simon Olpin Consultant Clinical Scientist in Inherited Metabolic Disease Department of Clinical Chemistry Sheffield Children s Hospital Clinical Diagnosis of Muscle Disease
Metabolic Muscle Disease Dr. Simon Olpin Consultant Clinical Scientist in Inherited Metabolic Disease Department of Clinical Chemistry Sheffield Children s Hospital Clinical Diagnosis of Muscle Disease
Metabolism of pentoses, glycogen, fructose and galactose. Jana Novotna
 Metabolism of pentoses, glycogen, fructose and galactose Jana Novotna 1. The Pentose Phosphate Pathway The pentose phosphate pathway (PPP): (hexose monophosphate or 6-phosphogluconate patway) Process that
Metabolism of pentoses, glycogen, fructose and galactose Jana Novotna 1. The Pentose Phosphate Pathway The pentose phosphate pathway (PPP): (hexose monophosphate or 6-phosphogluconate patway) Process that
Fatty Acid Oxidation Disorders- an update. Fiona Carragher Biochemical Sciences, GSTS Pathology St Thomas Hospital, London
 Fatty Acid Oxidation Disorders- an update Fiona Carragher Biochemical Sciences, GSTS Pathology St Thomas Hospital, London An update. Overview of metabolism Clinical presentation and outcome Diagnostic
Fatty Acid Oxidation Disorders- an update Fiona Carragher Biochemical Sciences, GSTS Pathology St Thomas Hospital, London An update. Overview of metabolism Clinical presentation and outcome Diagnostic
Oxidation of Long Chain Fatty Acids
 Oxidation of Long Chain Fatty Acids Dr NC Bird Oxidation of long chain fatty acids is the primary source of energy supply in man and animals. Hibernating animals utilise fat stores to maintain body heat,
Oxidation of Long Chain Fatty Acids Dr NC Bird Oxidation of long chain fatty acids is the primary source of energy supply in man and animals. Hibernating animals utilise fat stores to maintain body heat,
g) Cellular Respiration Higher Human Biology
 Cellular Respiration Higher Human Biology") g) Cellular Respiration Higher Human Biology What can you remember about respiration? 1. What is respiration? 2. What are the raw materials? 3. What are the products? 4. Where does it occur? 5. Why does
g) Cellular Respiration Higher Human Biology What can you remember about respiration? 1. What is respiration? 2. What are the raw materials? 3. What are the products? 4. Where does it occur? 5. Why does
Newborn Screen & Development Facts about the genetic diseases new since March 2006 (Excluding Cystic Fibrosis)
") Newborn Screen & Development Facts about the genetic diseases new since March 2006 (Excluding Cystic Fibrosis) 1) Argininosuccinic acidemia (ASA) a) Incidence: ~1 in 70,000 b) Deficiency in an enzyme of
Newborn Screen & Development Facts about the genetic diseases new since March 2006 (Excluding Cystic Fibrosis) 1) Argininosuccinic acidemia (ASA) a) Incidence: ~1 in 70,000 b) Deficiency in an enzyme of
UNIVERSITY OF BOLTON SPORT AND BIOLOGICAL SCIENCES SPORT AND EXERCISE SCIENCE PATHWAY SEMESTER TWO EXAMINATIONS 2016/2017
 LH14 UNIVERSITY OF BOLTON SPORT AND BIOLOGICAL SCIENCES SPORT AND EXERCISE SCIENCE PATHWAY SEMESTER TWO EXAMINATIONS 2016/2017 INTRODUCTION TO SPORT AND EXERCISE PHYSIOLOGY MODULE NO: SPS4002 Date: Thursday
LH14 UNIVERSITY OF BOLTON SPORT AND BIOLOGICAL SCIENCES SPORT AND EXERCISE SCIENCE PATHWAY SEMESTER TWO EXAMINATIONS 2016/2017 INTRODUCTION TO SPORT AND EXERCISE PHYSIOLOGY MODULE NO: SPS4002 Date: Thursday
Fatty acid oxidation. Naomi Rankin
 Fatty acid oxidation Naomi Rankin Fatty acid oxidation Provides energy to muscles from lipid stores, spares glucose for the brain Lipolysis of triglycerides results in FFA, mainly C16 and C18 FA oxidation
Fatty acid oxidation Naomi Rankin Fatty acid oxidation Provides energy to muscles from lipid stores, spares glucose for the brain Lipolysis of triglycerides results in FFA, mainly C16 and C18 FA oxidation
Diseases Associated with Glycogen Synthesis
 Paper : 04 Metabolism of carbohydrates Module: 29 Principal Investigator, Dr. S.K.Khare, Professor IIT Delhi. Paper Coordinator Content Writer Dr. Ramesh Kothari, Professor Dr. Vijaya Khader UGC-CAS Dr.
Paper : 04 Metabolism of carbohydrates Module: 29 Principal Investigator, Dr. S.K.Khare, Professor IIT Delhi. Paper Coordinator Content Writer Dr. Ramesh Kothari, Professor Dr. Vijaya Khader UGC-CAS Dr.
Carnitine palmitoyl transferase 2 deficiency (CPT2) is a rare inherited disorder that occurs when
 is a rare inherited disorder that occurs when") CPT2 Deficiency Carnitine palmitoyl transferase 2 deficiency (CPT2) is a rare inherited disorder that occurs when the last step in the entry of fats into sac-like bodies called mitochondria is blocked.
CPT2 Deficiency Carnitine palmitoyl transferase 2 deficiency (CPT2) is a rare inherited disorder that occurs when the last step in the entry of fats into sac-like bodies called mitochondria is blocked.
Disorders of Muscle. Disorders of Muscle. Muscle Groups Involved in Myopathy. Needle Examination of EMG. History. Muscle Biopsy
 Disorders of Muscle Disorders of Muscle Zakia Bell, M.D. Associate Professor of Neurology and Physical Medicine & Rehabilitation Virginia Commonwealth University Cardinal symptom of diseases of the muscle
Disorders of Muscle Disorders of Muscle Zakia Bell, M.D. Associate Professor of Neurology and Physical Medicine & Rehabilitation Virginia Commonwealth University Cardinal symptom of diseases of the muscle
Glycogen function. Cellular glucose store. Local emergency store Local short term use
 Glycogen function Cellular glucose store Liver Brain Muscle Body sump Local emergency store Local short term use Glycogen storage diseases Accumulation abnormal amount/type glycogen Hypoglycaemia, lactic
Glycogen function Cellular glucose store Liver Brain Muscle Body sump Local emergency store Local short term use Glycogen storage diseases Accumulation abnormal amount/type glycogen Hypoglycaemia, lactic
There are four different forms of Tarui disease, which are classed by their signs and symptoms and age of presentation.
 Tarui Disease Tarui disease (also known as phosphofructokinase deficiency, or glycogen storage disease type VII) was first described in 1965 by the Japanese physician Seiichiro Tarui and his co-workers.
Tarui Disease Tarui disease (also known as phosphofructokinase deficiency, or glycogen storage disease type VII) was first described in 1965 by the Japanese physician Seiichiro Tarui and his co-workers.
7 Medical Genetics. Hemoglobinopathies. Hemoglobinopathies. Protein and Gene Structure. and Biochemical Genetics
 SESSION 7 Medical Genetics Hemoglobinopathies and Biochemical Genetics J a v a d F a s a J a m s h i d i U n i v e r s i t y o f M e d i c a l S c i e n c e s, N o v e m b e r 2 0 1 7 Hemoglobinopathies
SESSION 7 Medical Genetics Hemoglobinopathies and Biochemical Genetics J a v a d F a s a J a m s h i d i U n i v e r s i t y o f M e d i c a l S c i e n c e s, N o v e m b e r 2 0 1 7 Hemoglobinopathies
number Done by Corrected by Doctor Nayef Karadsheh
 number 14 Done by Dergam Al-Tarawneh Corrected by Maya Attarakih Doctor Nayef Karadsheh 1 P a g e Glycogen metabolism Note: Everything written in orange is from the book not mentioned by the doctor. In
number 14 Done by Dergam Al-Tarawneh Corrected by Maya Attarakih Doctor Nayef Karadsheh 1 P a g e Glycogen metabolism Note: Everything written in orange is from the book not mentioned by the doctor. In
Biol 219 Lec 7 Fall 2016
 Cellular Respiration: Harvesting Energy to form ATP Cellular Respiration and Metabolism Glucose ATP Pyruvate Lactate Acetyl CoA NAD + Introducing The Players primary substrate for cellular respiration
Cellular Respiration: Harvesting Energy to form ATP Cellular Respiration and Metabolism Glucose ATP Pyruvate Lactate Acetyl CoA NAD + Introducing The Players primary substrate for cellular respiration
2. What is molecular oxygen directly converted into? a. Carbon Dioxide b. Water c. Glucose d. None of the Above
 Biochem 1 Mock Exam 3 Chapter 11: 1. What is glucose completely oxidized into? a. Carbon Dioxide and Water b. Carbon Dioxide and Oxygen c. Oxygen and Water d. Water and Glycogen 2. What is molecular oxygen
Biochem 1 Mock Exam 3 Chapter 11: 1. What is glucose completely oxidized into? a. Carbon Dioxide and Water b. Carbon Dioxide and Oxygen c. Oxygen and Water d. Water and Glycogen 2. What is molecular oxygen
How Did Energy-Releasing Pathways Evolve? (cont d.)
") How Did Energy-Releasing Pathways Evolve? (cont d.) 7.1 How Do Cells Access the Chemical Energy in Sugars? In order to use the energy stored in sugars, cells must first transfer it to ATP The energy transfer
How Did Energy-Releasing Pathways Evolve? (cont d.) 7.1 How Do Cells Access the Chemical Energy in Sugars? In order to use the energy stored in sugars, cells must first transfer it to ATP The energy transfer
Chemistry 1120 Exam 4 Study Guide
 Chemistry 1120 Exam 4 Study Guide Chapter 12 12.1 Identify and differentiate between macronutrients (lipids, amino acids and saccharides) and micronutrients (vitamins and minerals). Master Tutor Section
Chemistry 1120 Exam 4 Study Guide Chapter 12 12.1 Identify and differentiate between macronutrients (lipids, amino acids and saccharides) and micronutrients (vitamins and minerals). Master Tutor Section
How Cells Release Chemical Energy. Chapter 8
 How Cells Release Chemical Energy Chapter 8 Impacts, Issues: When Mitochondria Spin Their Wheels More than forty disorders related to defective mitochondria are known (such as Friedreich s ataxia); many
How Cells Release Chemical Energy Chapter 8 Impacts, Issues: When Mitochondria Spin Their Wheels More than forty disorders related to defective mitochondria are known (such as Friedreich s ataxia); many
Recent Advances in Neurology 2014: Neuromuscular Case Presentations
 Recent Advances in Neurology 2014: Neuromuscular Case Presentations Jeffrey W. Ralph, MD Associate Clinical Professor Patient #1: Young woman with severe polyneuropathy 25 year-old woman Normal motor and
Recent Advances in Neurology 2014: Neuromuscular Case Presentations Jeffrey W. Ralph, MD Associate Clinical Professor Patient #1: Young woman with severe polyneuropathy 25 year-old woman Normal motor and
Chapter 7 How Cells Release Chemical Energy
 Chapter 7 How Cells Release Chemical Energy 7.1 Mighty Mitochondria More than forty disorders related to defective mitochondria are known (such as Friedreich s ataxia); many of those afflicted die young
Chapter 7 How Cells Release Chemical Energy 7.1 Mighty Mitochondria More than forty disorders related to defective mitochondria are known (such as Friedreich s ataxia); many of those afflicted die young
How Cells Harvest Chemical Energy
 How Cells Harvest Chemical Energy Global Athlete Outreach Program US CytoThesis Systems Medicine Center www.cytothesis.us US OncoTherapy Systems BioMedicine Group CytoThesis Bioengineering Research Group
How Cells Harvest Chemical Energy Global Athlete Outreach Program US CytoThesis Systems Medicine Center www.cytothesis.us US OncoTherapy Systems BioMedicine Group CytoThesis Bioengineering Research Group
Medical Biochemistry and Molecular Biology department
 Medical Biochemistry and Molecular Biology department Cardiac Fuels [Sources of energy for the Cardiac muscle] Intended learning outcomes of the lecture: By the end of this lecture you would be able to:-
Medical Biochemistry and Molecular Biology department Cardiac Fuels [Sources of energy for the Cardiac muscle] Intended learning outcomes of the lecture: By the end of this lecture you would be able to:-
Metabolism of cardiac muscle. Dr. Mamoun Ahram Cardiovascular system, 2013
 Metabolism of cardiac muscle Dr. Mamoun Ahram Cardiovascular system, 2013 References This lecture Mark s Basic Medical Biochemistry, 4 th ed., p. 890-891 Hand-out Why is this topic important? Heart failure
Metabolism of cardiac muscle Dr. Mamoun Ahram Cardiovascular system, 2013 References This lecture Mark s Basic Medical Biochemistry, 4 th ed., p. 890-891 Hand-out Why is this topic important? Heart failure
Metabolism. Chapter 5. Catabolism Drives Anabolism 8/29/11. Complete Catabolism of Glucose
 8/29/11 Metabolism Chapter 5 All of the reactions in the body that require energy transfer. Can be divided into: Cell Respiration and Metabolism Anabolism: requires the input of energy to synthesize large
8/29/11 Metabolism Chapter 5 All of the reactions in the body that require energy transfer. Can be divided into: Cell Respiration and Metabolism Anabolism: requires the input of energy to synthesize large
NCG Diagnostic and Management Service for McArdle Disease and Related Disorders Lead clinician: Dr Ros Quinlivan
 Queen Square Centre for Neuromuscular Diseases NCG Diagnostic and Management Service for McArdle Disease and Related Disorders Lead clinician: Dr Ros Quinlivan Described 1951 Autosomal recessive McArdle
Queen Square Centre for Neuromuscular Diseases NCG Diagnostic and Management Service for McArdle Disease and Related Disorders Lead clinician: Dr Ros Quinlivan Described 1951 Autosomal recessive McArdle
Integrative Metabolism: Significance
 Integrative Metabolism: Significance Energy Containing Nutrients Carbohydrates Fats Proteins Catabolism Energy Depleted End Products H 2 O NH 3 ADP + Pi NAD + NADP + FAD + Pi NADH+H + NADPH+H + FADH2 Cell
Integrative Metabolism: Significance Energy Containing Nutrients Carbohydrates Fats Proteins Catabolism Energy Depleted End Products H 2 O NH 3 ADP + Pi NAD + NADP + FAD + Pi NADH+H + NADPH+H + FADH2 Cell
Lipid Metabolism. Remember fats?? Triacylglycerols - major form of energy storage in animals
 Remember fats?? Triacylglycerols - major form of energy storage in animals Your energy reserves: ~0.5% carbs (glycogen + glucose) ~15% protein (muscle, last resort) ~85% fat Why use fat for energy? 1 gram
Remember fats?? Triacylglycerols - major form of energy storage in animals Your energy reserves: ~0.5% carbs (glycogen + glucose) ~15% protein (muscle, last resort) ~85% fat Why use fat for energy? 1 gram
Glycogen Storage Disease Type III also known as Cori or Forbe s Disease/Debrancher Enzyme Deficiency
 Glycogen Storage Disease Type III also known as Cori or Forbe s Disease/Debrancher Enzyme Deficiency What is GSDIII? Glycogen Storage Disease type 3 is an inherited condition caused by a defect in a gene
Glycogen Storage Disease Type III also known as Cori or Forbe s Disease/Debrancher Enzyme Deficiency What is GSDIII? Glycogen Storage Disease type 3 is an inherited condition caused by a defect in a gene
Glucose is the only source of energy in red blood cells. Under starvation conditions ketone bodies become a source of energy for the brain
 Glycolysis 4 / The Text :- Some Points About Glucose Glucose is very soluble source of quick and ready energy. It is a relatively stable and easily transported. In mammals, the brain uses only glucose
Glycolysis 4 / The Text :- Some Points About Glucose Glucose is very soluble source of quick and ready energy. It is a relatively stable and easily transported. In mammals, the brain uses only glucose
Metabolic diseases of the liver
 Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
Review Article Inborn Errors of Energy Metabolism Associated with Myopathies
 Journal of Biomedicine and Biotechnology Volume 2010, Article ID 340849, 19 pages doi:10.1155/2010/340849 Review Article Inborn Errors of Energy Metabolism Associated with Myopathies AnibhM.Das, 1 Ulrike
Journal of Biomedicine and Biotechnology Volume 2010, Article ID 340849, 19 pages doi:10.1155/2010/340849 Review Article Inborn Errors of Energy Metabolism Associated with Myopathies AnibhM.Das, 1 Ulrike
5.0 HORMONAL CONTROL OF CARBOHYDRATE METABOLISM
 5.0 HORMONAL CONTROL OF CARBOHYDRATE METABOLISM Introduction: Variety of hormones and other molecules regulate the carbohydrates metabolism. Some of these have already been cited in previous sections.
5.0 HORMONAL CONTROL OF CARBOHYDRATE METABOLISM Introduction: Variety of hormones and other molecules regulate the carbohydrates metabolism. Some of these have already been cited in previous sections.
Structure. Lysosomes are membrane-enclosed organelles. Hydrolytic enzymes. Variable in size & shape need
 Lysosomes Structure Lysosomes are membrane-enclosed organelles Hydrolytic enzymes Variable in size & shape need Degrade material taken up from outside and inside the cell Variable in size and shape Lysosomal
Lysosomes Structure Lysosomes are membrane-enclosed organelles Hydrolytic enzymes Variable in size & shape need Degrade material taken up from outside and inside the cell Variable in size and shape Lysosomal
Cellular Respiration
 Cellular Respiration 1. To perform cell work, cells require energy. a. A cell does three main kinds of work: i. Mechanical work, such as the beating of cilia, contraction of muscle cells, and movement
Cellular Respiration 1. To perform cell work, cells require energy. a. A cell does three main kinds of work: i. Mechanical work, such as the beating of cilia, contraction of muscle cells, and movement
Metabolic Myopathies. Review Article. Alejandro Tobon, MD ABSTRACT
 Review Article Metabolic Myopathies Alejandro Tobon, MD ABSTRACT Purpose of Review: The metabolic myopathies result from inborn errors of metabolism affecting intracellular energy production due to defects
Review Article Metabolic Myopathies Alejandro Tobon, MD ABSTRACT Purpose of Review: The metabolic myopathies result from inborn errors of metabolism affecting intracellular energy production due to defects
MetBioNet Best Practice Guidelines. Investigation of an inherited metabolic cause of cardiomyopathy
 Introduction MetBioNet Best Practice Guidelines Investigation of an inherited metabolic cause of Inborn errors of metabolism (IEM) account for at least 5% of cases of. In some disorders, is the major cause
Introduction MetBioNet Best Practice Guidelines Investigation of an inherited metabolic cause of Inborn errors of metabolism (IEM) account for at least 5% of cases of. In some disorders, is the major cause
Transfer of food energy to chemical energy. Includes anabolic and catabolic reactions. The cell is the metabolic processing center
 Metabolism There are a lot of diagrams here. DO NOT, I repeat, DO NOT get overly anxious or excited about them. We will go through them again slowly!! Read the slides, read the book, DO NOT TAKE NOTES.
Metabolism There are a lot of diagrams here. DO NOT, I repeat, DO NOT get overly anxious or excited about them. We will go through them again slowly!! Read the slides, read the book, DO NOT TAKE NOTES.
The laboratory investigation of lactic acidaemia. J Bonham/T Laing
 The laboratory investigation of lactic acidaemia J Bonham/T Laing Reference range Typical ranges for blood lactate are: Newborn 0.3-2.2 mmol/l Nielsen J et al1 1994 1-12mo 0.9-1.8 mmol/l Bonnefont et al
The laboratory investigation of lactic acidaemia J Bonham/T Laing Reference range Typical ranges for blood lactate are: Newborn 0.3-2.2 mmol/l Nielsen J et al1 1994 1-12mo 0.9-1.8 mmol/l Bonnefont et al
Metabolism. Metabolic pathways. BIO 5099: Molecular Biology for Computer Scientists (et al) Lecture 11: Metabolic Pathways
 Lecture 11: Metabolic Pathways") BIO 5099: Molecular Biology for Computer Scientists (et al) Lecture 11: Metabolic Pathways http://compbio.uchsc.edu/hunter/bio5099 Larry.Hunter@uchsc.edu Metabolism Metabolism is the chemical change of
BIO 5099: Molecular Biology for Computer Scientists (et al) Lecture 11: Metabolic Pathways http://compbio.uchsc.edu/hunter/bio5099 Larry.Hunter@uchsc.edu Metabolism Metabolism is the chemical change of
Biochemistry Team 437. Glycogen metabolism. Color index: Doctors slides Notes and explanations Extra information Highlights. Musculoskeletal block
 Glycogen metabolism Color index: Doctors slides Notes and explanations Extra information Highlights Biochemistry Team 437 ﺑ ﺳ م ﷲ اﻟرﺣﻣن اﻟرﺣﯾم Musculoskeletal block Objectives: By the end of this lecture,
Glycogen metabolism Color index: Doctors slides Notes and explanations Extra information Highlights Biochemistry Team 437 ﺑ ﺳ م ﷲ اﻟرﺣﻣن اﻟرﺣﯾم Musculoskeletal block Objectives: By the end of this lecture,
NAME KEY ID # EXAM 3a BIOC 460. Wednesday April 10, Please include your name and ID# on each page. Limit your answers to the space provided!
 EXAM 3a BIOC 460 Wednesday April 10, 2002 Please include your name and ID# on each page. Limit your answers to the space provided! 1 1. (5 pts.) Define the term energy charge: Energy charge refers to the
EXAM 3a BIOC 460 Wednesday April 10, 2002 Please include your name and ID# on each page. Limit your answers to the space provided! 1 1. (5 pts.) Define the term energy charge: Energy charge refers to the
CHY2026: General Biochemistry. Lipid Metabolism
 CHY2026: General Biochemistry Lipid Metabolism Lipid Digestion Lipid Metabolism Fats (triglycerides) are high metabolic energy molecules Fats yield 9.3 kcal of energy (carbohydrates and proteins 4.1 kcal)
CHY2026: General Biochemistry Lipid Metabolism Lipid Digestion Lipid Metabolism Fats (triglycerides) are high metabolic energy molecules Fats yield 9.3 kcal of energy (carbohydrates and proteins 4.1 kcal)
National Metabolic Biochemistry Network Guidelines for the investigation of hypoglycaemia in infants and children
 National Metabolic Biochemistry Network Guidelines for the investigation of hypoglycaemia in infants and children Aim To provide guidance on the biochemical investigation of hypoglycaemia in infants and
National Metabolic Biochemistry Network Guidelines for the investigation of hypoglycaemia in infants and children Aim To provide guidance on the biochemical investigation of hypoglycaemia in infants and
BIOCHEMISTRY. Glycolysis. by Dr Jaya Vejayan Faculty of Industrial Sciences & Technology
 BIOCHEMISTRY Glycolysis by Dr Jaya Vejayan Faculty of Industrial Sciences & Technology email: jayavejayan@ump.edu.my Chapter Description Overview This chapter is related to carbohydrate catabolism. It
BIOCHEMISTRY Glycolysis by Dr Jaya Vejayan Faculty of Industrial Sciences & Technology email: jayavejayan@ump.edu.my Chapter Description Overview This chapter is related to carbohydrate catabolism. It
Mitochondrial Diseases
 Mitochondrial Diseases Simon Heales SWIM Conference Taunton, November 29 th 2018 Respiratory Failure Cardiomyopathy Optic Atrophy / Retinitis Pigmentosa Seizures / Developmental delay Liver Failure Deafness
Mitochondrial Diseases Simon Heales SWIM Conference Taunton, November 29 th 2018 Respiratory Failure Cardiomyopathy Optic Atrophy / Retinitis Pigmentosa Seizures / Developmental delay Liver Failure Deafness
Bioenergetics: Energy for Exercise. Chapter 3 pp 28-47
 Bioenergetics: Energy for Exercise Chapter 3 pp 28-47 ATP ATP Adenosine Ribose 3 Phosphates ATP ATP ATP ATP ATP ATP ATP ATP ATP Energy Out ADP + P ATP ATP Energy Out ADP + P ATP ATP Energy Out Energy In
Bioenergetics: Energy for Exercise Chapter 3 pp 28-47 ATP ATP Adenosine Ribose 3 Phosphates ATP ATP ATP ATP ATP ATP ATP ATP ATP Energy Out ADP + P ATP ATP Energy Out ADP + P ATP ATP Energy Out Energy In
Pompe. Lysosomal Disorders. Introduction
 Introduction disease is an inherited, genetic disorder which results in the lack of an enzyme 'acid alpha-glucosidase. disease is also known as acid maltase deficiency or glycogen storage disease type
Introduction disease is an inherited, genetic disorder which results in the lack of an enzyme 'acid alpha-glucosidase. disease is also known as acid maltase deficiency or glycogen storage disease type
Intermediary metabolism. Eva Samcová
 Intermediary metabolism Eva Samcová Metabolic roles of tissues Four major tissues play a dominant role in fuel metabolism : liver, adipose, muscle, and brain. These tissues do not function in isolation.
Intermediary metabolism Eva Samcová Metabolic roles of tissues Four major tissues play a dominant role in fuel metabolism : liver, adipose, muscle, and brain. These tissues do not function in isolation.
4. Which step shows a split of one molecule into two smaller molecules? a. 2. d. 5
 1. Which of the following statements about NAD + is false? a. NAD + is reduced to NADH during both glycolysis and the citric acid cycle. b. NAD + has more chemical energy than NADH. c. NAD + is reduced
1. Which of the following statements about NAD + is false? a. NAD + is reduced to NADH during both glycolysis and the citric acid cycle. b. NAD + has more chemical energy than NADH. c. NAD + is reduced
Integration of Metabolism
 Integration of Metabolism Metabolism is a continuous process. Thousands of reactions occur simultaneously in order to maintain homeostasis. It ensures a supply of fuel, to tissues at all times, in fed
Integration of Metabolism Metabolism is a continuous process. Thousands of reactions occur simultaneously in order to maintain homeostasis. It ensures a supply of fuel, to tissues at all times, in fed
Metabolic Myopathies Mark A. Tarnopolsky, MD, PhD
 Review Article Downloaded from https://journals.lww.com/continuum by maxwo3znzwrcfjddvmduzvysskax4mzb8eymgwvspgpjoz9l+mqfwgfuplwvy+jmyqlpqmifewtrhxj7jpeo+505hdqh14pdzv4lwky42mcrzqckilw0d1o4yvrwmuvvhuyo4rrbviuuwr5dqytbtk/icsrdbt0hfryk7+zagvaltkgnudxdohhaxffu/7kno26hifzu/+bcy16w7w1bdw==
Review Article Downloaded from https://journals.lww.com/continuum by maxwo3znzwrcfjddvmduzvysskax4mzb8eymgwvspgpjoz9l+mqfwgfuplwvy+jmyqlpqmifewtrhxj7jpeo+505hdqh14pdzv4lwky42mcrzqckilw0d1o4yvrwmuvvhuyo4rrbviuuwr5dqytbtk/icsrdbt0hfryk7+zagvaltkgnudxdohhaxffu/7kno26hifzu/+bcy16w7w1bdw==
CLINICAL SIGNS SUGGESTIVE OF A NEUROMETABOLIC DISEASE. Bwee Tien Poll-The Amsterdam UMC The Netherlands
 CLINICAL SIGNS SUGGESTIVE OF A NEUROMETABOLIC DISEASE Bwee Tien Poll-The Amsterdam UMC The Netherlands FRAMEWORK OF PRINCIPALS 1. Problem-oriented clinical approach 2. Biomarkers in plasma, urine, CSF
CLINICAL SIGNS SUGGESTIVE OF A NEUROMETABOLIC DISEASE Bwee Tien Poll-The Amsterdam UMC The Netherlands FRAMEWORK OF PRINCIPALS 1. Problem-oriented clinical approach 2. Biomarkers in plasma, urine, CSF
How Cells Release Chemical Energy. Chapter 7
 How Cells Release Chemical Energy Chapter 7 7.1 Overview of Carbohydrate Breakdown Pathways All organisms (including photoautotrophs) convert chemical energy of organic compounds to chemical energy of
How Cells Release Chemical Energy Chapter 7 7.1 Overview of Carbohydrate Breakdown Pathways All organisms (including photoautotrophs) convert chemical energy of organic compounds to chemical energy of
Class XI Chapter 14 Respiration in Plants Biology. 1. It is a biochemical process. 1. It is a physiochemical process.
 Question 1: Differentiate between (a) Respiration and Combustion (b) Glycolysis and Krebs cycle (c) Aerobic respiration and Fermentation (a) Respiration and combustion Respiration Combustion 1. It is a
Question 1: Differentiate between (a) Respiration and Combustion (b) Glycolysis and Krebs cycle (c) Aerobic respiration and Fermentation (a) Respiration and combustion Respiration Combustion 1. It is a
Integration & Hormone Regulation
 Integration Branchpoints in metabolism where metabolites can go several directions 1. Glucose 6-phosphate Energy needed (low energy charge): glycolysis Low blood sugar: high [glucagon], low [insulin] glycogen
Integration Branchpoints in metabolism where metabolites can go several directions 1. Glucose 6-phosphate Energy needed (low energy charge): glycolysis Low blood sugar: high [glucagon], low [insulin] glycogen
Energy metabolism - the overview
 Energy metabolism - the overview Josef Fontana EC - 40 Overview of the lecture Important terms of the energy metabolism The overview of the energy metabolism The main pathways of the energy metabolism
Energy metabolism - the overview Josef Fontana EC - 40 Overview of the lecture Important terms of the energy metabolism The overview of the energy metabolism The main pathways of the energy metabolism
BIOCHEMICAL AND MOLECULAR HETEROGENEITY IN CARNITINE PALMITOYLTRANSFERASE II DEFICIENCY
 BIOCHEMICAL AND MOLECULAR HETEROGENEITY IN CARNITINE PALMITOYLTRANSFERASE II DEFICIENCY Carmen Sousa, Helena Fonseca, Hugo Rocha, Ana Marcão, Laura Vilarinho, Luísa Diogo, Sílvia Sequeira, Cristina Costa,
BIOCHEMICAL AND MOLECULAR HETEROGENEITY IN CARNITINE PALMITOYLTRANSFERASE II DEFICIENCY Carmen Sousa, Helena Fonseca, Hugo Rocha, Ana Marcão, Laura Vilarinho, Luísa Diogo, Sílvia Sequeira, Cristina Costa,
Glycolysis. Intracellular location Rate limiting steps
 Glycolysis Definition Fx Fate Site Intracellular location Rate limiting steps Regulation Consume ATP Subs level phosphoryla tion Key reactions control points Nb Oxidation of glucose to give pyruvate (
Glycolysis Definition Fx Fate Site Intracellular location Rate limiting steps Regulation Consume ATP Subs level phosphoryla tion Key reactions control points Nb Oxidation of glucose to give pyruvate (
Roles of Lipids. principal form of stored energy major constituents of cell membranes vitamins messengers intra and extracellular
 Roles of Lipids principal form of stored energy major constituents of cell membranes vitamins messengers intra and extracellular = Oxidation of fatty acids Central energy-yielding pathway in animals. O
Roles of Lipids principal form of stored energy major constituents of cell membranes vitamins messengers intra and extracellular = Oxidation of fatty acids Central energy-yielding pathway in animals. O
Inborn errors of metabolism
 ESPEN Congress Nice 2010 From child to adult nutrition Inborn errors of metabolism Pascal Crenn Inborn errors of metabolism: from child to adult Pascal Crenn Hôpital Raymond Poincaré 92380 Garches. France
ESPEN Congress Nice 2010 From child to adult nutrition Inborn errors of metabolism Pascal Crenn Inborn errors of metabolism: from child to adult Pascal Crenn Hôpital Raymond Poincaré 92380 Garches. France
Transport. Oxidation. Electron. which the en the ETC and. of NADH an. nd FADH 2 by ation. Both, Phosphorylation. Glycolysis Glucose.
 Electron Transport Chain and Oxidation Phosphorylation When one glucose molecule is oxidized to six CO 2 molecules by way of glycolysiss and TCA cycle, considerable amount of energy (ATP) is generated.
Electron Transport Chain and Oxidation Phosphorylation When one glucose molecule is oxidized to six CO 2 molecules by way of glycolysiss and TCA cycle, considerable amount of energy (ATP) is generated.
respiration mitochondria mitochondria metabolic pathways reproduction can fuse or split DRP1 interacts with ER tubules chapter DRP1 ER tubule
 mitochondria respiration chapter 3-4 shape highly variable can fuse or split structure outer membrane inner membrane cristae intermembrane space mitochondrial matrix free ribosomes respiratory enzymes
mitochondria respiration chapter 3-4 shape highly variable can fuse or split structure outer membrane inner membrane cristae intermembrane space mitochondrial matrix free ribosomes respiratory enzymes
Energy Production In A Cell (Chapter 25 Metabolism)
") Energy Production In A Cell (Chapter 25 Metabolism) Large food molecules contain a lot of potential energy in the form of chemical bonds but it requires a lot of work to liberate the energy. Cells need
Energy Production In A Cell (Chapter 25 Metabolism) Large food molecules contain a lot of potential energy in the form of chemical bonds but it requires a lot of work to liberate the energy. Cells need
Referring Physician Information Name: (Last, First, Middle):
:") Page 1 of 5 Patient Information Clinical Indication: Patient Name: (Last, First, Middle): DOB (M/D/Y): Sex: M F Guardian Name (for minor patients only): Address: City: State: ZIP: Phone: Ethnic Background
Page 1 of 5 Patient Information Clinical Indication: Patient Name: (Last, First, Middle): DOB (M/D/Y): Sex: M F Guardian Name (for minor patients only): Address: City: State: ZIP: Phone: Ethnic Background
What s the point? The point is to make ATP! ATP
 2006-2007 What s the point? The point is to make ATP! ATP Glycolysis 2 ATP Kreb s cycle 2 ATP Life takes a lot of energy to run, need to extract more energy than 4 ATP! There s got to be a better way!
2006-2007 What s the point? The point is to make ATP! ATP Glycolysis 2 ATP Kreb s cycle 2 ATP Life takes a lot of energy to run, need to extract more energy than 4 ATP! There s got to be a better way!
Childhood epilepsy: the biochemical epilepsies. Dr Colin D Ferrie Consultant Paediatric Neurologist Leeds General Infirmary
 Childhood epilepsy: the biochemical epilepsies Dr Colin D Ferrie Consultant Paediatric Neurologist Leeds General Infirmary Definitions Epileptic Seizure Manifestation(s) of epileptic (excessive and/or
Childhood epilepsy: the biochemical epilepsies Dr Colin D Ferrie Consultant Paediatric Neurologist Leeds General Infirmary Definitions Epileptic Seizure Manifestation(s) of epileptic (excessive and/or
 Question 1: Differentiate between (a) Respiration and Combustion (b) Glycolysis and Krebs cycle (c) Aerobic respiration and Fermentation (a) Respiration and combustion Respiration Combustion 1. It is a
Question 1: Differentiate between (a) Respiration and Combustion (b) Glycolysis and Krebs cycle (c) Aerobic respiration and Fermentation (a) Respiration and combustion Respiration Combustion 1. It is a
Training Syllabus CLINICAL SYLLABUS
 Training Syllabus CLINICAL SYLLABUS SYLLABUS FOR TRAINING IN CLINICAL PAEDIATRIC METABOLIC MEDICINE Updated July 2006 This syllabus is intended as a guide. Whilst the training should be comprehensive,
Training Syllabus CLINICAL SYLLABUS SYLLABUS FOR TRAINING IN CLINICAL PAEDIATRIC METABOLIC MEDICINE Updated July 2006 This syllabus is intended as a guide. Whilst the training should be comprehensive,
CARBOHYDRATE METABOLISM
 Note (Study Glycolysis, fermentation and their regulation, Gluconeogenesis and glycogenolysis, Metabolism of galactose, TCA cycle and Amphibolic role of the cycle, and Glyoxalic acid cycle, HMP shunt in
Note (Study Glycolysis, fermentation and their regulation, Gluconeogenesis and glycogenolysis, Metabolism of galactose, TCA cycle and Amphibolic role of the cycle, and Glyoxalic acid cycle, HMP shunt in
Chapter 7- Metabolism: Transformations and Interactions Thomson - Wadsworth
 Chapter 7- Metabolism: Transformations and Interactions 2008 Thomson - Wadsworth Simple Overview of Energy Metabolism The sum of all chemical reactions that go on in living cells Introduction Energy Heat-
Chapter 7- Metabolism: Transformations and Interactions 2008 Thomson - Wadsworth Simple Overview of Energy Metabolism The sum of all chemical reactions that go on in living cells Introduction Energy Heat-
Mitochondria and ATP Synthesis
 Mitochondria and ATP Synthesis Mitochondria and ATP Synthesis 1. Mitochondria are sites of ATP synthesis in cells. 2. ATP is used to do work; i.e. ATP is an energy source. 3. ATP hydrolysis releases energy
Mitochondria and ATP Synthesis Mitochondria and ATP Synthesis 1. Mitochondria are sites of ATP synthesis in cells. 2. ATP is used to do work; i.e. ATP is an energy source. 3. ATP hydrolysis releases energy
Test next Thursday, the 24 th will only cover the lecture
 Test next Thursday, the 24 th will only cover the lecture material, not lab stuff! Objectives Understand how muscles differ Fiber types Understand how we fuel muscle Glycogen Fats How many ATP from each
Test next Thursday, the 24 th will only cover the lecture material, not lab stuff! Objectives Understand how muscles differ Fiber types Understand how we fuel muscle Glycogen Fats How many ATP from each
Cell Injury MECHANISMS OF CELL INJURY
 Cell Injury MECHANISMS OF CELL INJURY The cellular response to injurious stimuli depends on the following factors: Type of injury, Its duration, and Its severity. Thus, low doses of toxins or a brief duration
Cell Injury MECHANISMS OF CELL INJURY The cellular response to injurious stimuli depends on the following factors: Type of injury, Its duration, and Its severity. Thus, low doses of toxins or a brief duration
Development of LCHF in Muscle GSDs. S.L. Reason RN MScN EdD
 Development of LCHF in Muscle GSDs S.L. Reason RN MScN EdD McArdle Disease is a rare disease of muscle metabolism, which is caused by a deficiency of the enzyme myophosphorylase. It is equally represented
Development of LCHF in Muscle GSDs S.L. Reason RN MScN EdD McArdle Disease is a rare disease of muscle metabolism, which is caused by a deficiency of the enzyme myophosphorylase. It is equally represented
THE GLUCOSE-FATTY ACID-KETONE BODY CYCLE Role of ketone bodies as respiratory substrates and metabolic signals
 Br. J. Anaesth. (1981), 53, 131 THE GLUCOSE-FATTY ACID-KETONE BODY CYCLE Role of ketone bodies as respiratory substrates and metabolic signals J. C. STANLEY In this paper, the glucose-fatty acid cycle
Br. J. Anaesth. (1981), 53, 131 THE GLUCOSE-FATTY ACID-KETONE BODY CYCLE Role of ketone bodies as respiratory substrates and metabolic signals J. C. STANLEY In this paper, the glucose-fatty acid cycle
CHE 242 Exam 3 Practice Questions
 CHE 242 Exam 3 Practice Questions Glucose metabolism 1. Below is depicted glucose catabolism. Indicate on the pathways the following: A) which reaction(s) of glycolysis are irreversible B) where energy
CHE 242 Exam 3 Practice Questions Glucose metabolism 1. Below is depicted glucose catabolism. Indicate on the pathways the following: A) which reaction(s) of glycolysis are irreversible B) where energy
Glycogen Storage Disease
 Glycogen Storage Disease 1 Introduction The food we eat is usually used for growth, tissue repair and energy. The body stores what it does not use. Excess sugar, or glucose, is stored as glycogen in the
Glycogen Storage Disease 1 Introduction The food we eat is usually used for growth, tissue repair and energy. The body stores what it does not use. Excess sugar, or glucose, is stored as glycogen in the
In glycolysis, glucose is converted to pyruvate. If the pyruvate is reduced to lactate, the pathway does not require O 2 and is called anaerobic
 Glycolysis 1 In glycolysis, glucose is converted to pyruvate. If the pyruvate is reduced to lactate, the pathway does not require O 2 and is called anaerobic glycolysis. If this pyruvate is converted instead
Glycolysis 1 In glycolysis, glucose is converted to pyruvate. If the pyruvate is reduced to lactate, the pathway does not require O 2 and is called anaerobic glycolysis. If this pyruvate is converted instead
This is an example outline of 3 lectures in BSC (Thanks to Dr. Ellington for sharing this information.)
") This is an example outline of 3 lectures in BSC 2010. (Thanks to Dr. Ellington for sharing this information.) Topic 10: CELLULAR RESPIRATION (lectures 14-16) OBJECTIVES: 1. Know the basic reactions that
This is an example outline of 3 lectures in BSC 2010. (Thanks to Dr. Ellington for sharing this information.) Topic 10: CELLULAR RESPIRATION (lectures 14-16) OBJECTIVES: 1. Know the basic reactions that
ANSC 619 PHYSIOLOGICAL CHEMISTRY OF LIVESTOCK SPECIES. Carbohydrate Metabolism
 ANSC 619 PHYSIOLOGICAL CHEMISTRY OF LIVESTOCK SPECIES I. Glycolysis A. Pathway Regulation of glycolysis Hexokinase: Activated by glucose. Inhibited by G6P. 6-Phosphofructokinase: Inhibited by ATP, especially
ANSC 619 PHYSIOLOGICAL CHEMISTRY OF LIVESTOCK SPECIES I. Glycolysis A. Pathway Regulation of glycolysis Hexokinase: Activated by glucose. Inhibited by G6P. 6-Phosphofructokinase: Inhibited by ATP, especially
Energy Metabolism. Chapter Cengage Learning. All Rights Reserved.
 Energy Metabolism Chapter 7 Introduction Energy Heat, mechanical, electrical, and chemical Metabolism How the body uses foods to meet its needs Chemical Reactions in the Body Energy metabolism How body
Energy Metabolism Chapter 7 Introduction Energy Heat, mechanical, electrical, and chemical Metabolism How the body uses foods to meet its needs Chemical Reactions in the Body Energy metabolism How body
Chapter 9. Cellular Respiration and Fermentation
 Chapter 9 Cellular Respiration and Fermentation Energy flows into an ecosystem as sunlight and leaves as heat Photosynthesis generates O 2 and organic molecules, which are used in cellular respiration
Chapter 9 Cellular Respiration and Fermentation Energy flows into an ecosystem as sunlight and leaves as heat Photosynthesis generates O 2 and organic molecules, which are used in cellular respiration
NBCE Mock Board Questions Biochemistry
 1. Fluid mosaic describes. A. Tertiary structure of proteins B. Ribosomal subunits C. DNA structure D. Plasma membrane structure NBCE Mock Board Questions Biochemistry 2. Where in the cell does beta oxidation
1. Fluid mosaic describes. A. Tertiary structure of proteins B. Ribosomal subunits C. DNA structure D. Plasma membrane structure NBCE Mock Board Questions Biochemistry 2. Where in the cell does beta oxidation
Fatty acid breakdown
 Fatty acids contain a long hydrocarbon chain and a terminal carboxylate group. Most contain between 14 and 24 carbon atoms. The chains may be saturated or contain double bonds. The complete oxidation of
Fatty acids contain a long hydrocarbon chain and a terminal carboxylate group. Most contain between 14 and 24 carbon atoms. The chains may be saturated or contain double bonds. The complete oxidation of
Oxidative phosphorylation
 OXIDATIVE PHOSPHORYLATION Oxidative phosphorylation Oxidative reaction Coupled by phosphorylation to the generation of high energy intermediate (ATP or other high phosphagen) Oxidative phosphorylation
OXIDATIVE PHOSPHORYLATION Oxidative phosphorylation Oxidative reaction Coupled by phosphorylation to the generation of high energy intermediate (ATP or other high phosphagen) Oxidative phosphorylation
Glycolysis Part 2. BCH 340 lecture 4
 Glycolysis Part 2 BCH 340 lecture 4 Regulation of Glycolysis There are three steps in glycolysis that have enzymes which regulate the flux of glycolysis These enzymes catalyzes irreversible reactions of
Glycolysis Part 2 BCH 340 lecture 4 Regulation of Glycolysis There are three steps in glycolysis that have enzymes which regulate the flux of glycolysis These enzymes catalyzes irreversible reactions of
Pathway overview. Glucose + 2NAD + + 2ADP +2Pi 2NADH + 2pyruvate + 2ATP + 2H 2 O + 4H +
 Glycolysis Glycolysis The conversion of glucose to pyruvate to yield 2ATP molecules 10 enzymatic steps Chemical interconversion steps Mechanisms of enzyme conversion and intermediates Energetics of conversions
Glycolysis Glycolysis The conversion of glucose to pyruvate to yield 2ATP molecules 10 enzymatic steps Chemical interconversion steps Mechanisms of enzyme conversion and intermediates Energetics of conversions
Mitochondrial Fatty Acid Oxidation Deficiencies Prof. Niels Gregersen
 Mitochondrial Fatty Acid Oxidation Deficiencies Research Unit for Molecular Medicine Clinical Institute Aarhus University Hospital and Faculty of Health Sciences Aarhus University, Aarhus, Denmark 1 Menu
Mitochondrial Fatty Acid Oxidation Deficiencies Research Unit for Molecular Medicine Clinical Institute Aarhus University Hospital and Faculty of Health Sciences Aarhus University, Aarhus, Denmark 1 Menu
Link download full of Test Bank for Fundamentals of Biochemistry 4th Edition by Voet
 Link download full of Test Bank for Fundamentals of Biochemistry 4th Edition by Voet http://testbankair.com/download/test-bank-for-fundamentals-ofbiochemistry-4th-edition-by-voet/ Chapter 16: Glycogen
Link download full of Test Bank for Fundamentals of Biochemistry 4th Edition by Voet http://testbankair.com/download/test-bank-for-fundamentals-ofbiochemistry-4th-edition-by-voet/ Chapter 16: Glycogen