THE PATHOPHYSIOLOGY OF THE REFEEDING SYNDROME
|
|
|
- Jonah Fields
- 6 years ago
- Views:
Transcription








1 THE PATHOPHYSIOLOGY OF THE REFEEDING SYNDROME Zeno Stanga, MD Division of Endocrinology, Diabetes and Clinical Nutrition Division of General Internal Medicine
 approx.")
2 Minnesota Experiment Aim To guide the Allied assistance to famine victims in Europe at the end of the World War II impact of various rehabilitation strategies n = 36 men selected from over 200 volunteers of the Civilian Public Service Start February 12 th, 1945 Energy intake semi-starvation ca. 50% of the energy requirements 2 meals, at 8 a.m. and at 6 p.m. Objective 25% weight loss in 24 weeks (6 mts) approx. 1 kg per week Keys A et al. The Biology of Human Starvation.1950

3 The primary objective of the Minnesota Starvation Experiment was to study the physical and psychological effects of prolonged, famine-like semi-starvation on healthy men, as well as their subsequent rehabilitation from this condition. Psychological effects: most of the subjects experienced periods of severe emotional distress and depression. Sexual interest was drastically reduced, and the volunteers showed signs of social withdrawal and isolation. The participants reported a decline in concentration, comprehension & judgment capabilities. Keys A et al. The Biology of Human Starvation.1950

4 Physical effects: There were marked declines in physiological processes reflected in reduced body temperature, respiration and heart rate. Some of the subjects exhibited edema in their extremities, presumably due to decreased levels of plasma proteins like albumin. Keys A et al. The Biology of Human Starvation.1950


5 Keys A et al. The Biology of Human Starvation.1950

6 Keys A et al. The Biology of Human Starvation.1950

7 Keys A et al. The Biology of Human Starvation.1950

8 Keys A et al. The Biology of Human Starvation.1950

9 body composition ( % ) Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland body composition vs body weight fat mass body weight fat-free mass semi - starvation refeeding weeks Keys A et al. The Biology of Human Starvation.1950


10 body function ( % ) Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland body function vs body weight depression score body weight hand dynamometry fitness score semi - starvation refeeding weeks Keys A et al. The Biology of Human Starvation.1950
11 The five stages of metabolic adjustement during starvation GLUCOSE USED ( g / h ) : : Cahill GF et al. Annu Rev Nutr 2006
12 Brain substrate utilisation during starvation 100 % 80 % 1 / 3 60 % 40 % 2 / 3 20 % 0 % Owen OE et al. J Clin Invest 1967
13 Glycogen content ( % ) Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Fall in glycogen content during fasting muscle liver Time ( days ) Owen OE et al. Am J Clin Nutr 1998
14 Prootein consumption ( g ) Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Protein mobilisation during fasting Time ( days ) Owen OE et al. J Clin Invest 1969
15 Urea excretion ( g / 24 h ) Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Urinary urea excretion during fasting urea ammonia others urea ammonia others Cahill GF et al. NEJM 1970

16 Organ-weight and -energy requirements Weight % Energy % liver brain heart kidney muscle fat others
 Basal energy")


17 Overall scheme of starvation fuel metabolism (man 70 kg) Basal energy requirements 24 h ca kcal g/d 2/5 3/ g/d 80 g/d g/d g/d 20 g/d Triglycerides 140 g/d Proteines 20 g/d Cahill GF. NEJM 1970 & Annu Rev Nutr 2006
18 mmol / l Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Concentrations of ketone bodies and plasma free fatty acids during starvation 6 5 -OHB FFA days Cahill GF et al. Annu Rev Nutr 2006



19 mmol / l Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Concentrations of ketone bodies and plasma free fatty acids during starvation 6 5 -OHB FFA days Cahill GF et al. Annu Rev Nutr 2006


20 Definition of the refeeding syndrome ( RFS ) Life-threatening status with low-serum electrolyte and vitamin concentrations fluid imbalance sodium-retention disturbance of organ function resulting from over-rapid or unbalanced refeeding of a malnourished catabolic patient. NICE. Clin. Guidelines 2006 / Stanga Z. Eur J Clin Nutr 2008

 Kagansky et al.")

21 % patients Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Prevalence of RFS 10% pat. with gastrointestinal fistulae Fan et al. Nutrition % elderly patients (age 65 y) Kagansky et al. J Intern Med % cancer patients Gonzalez et al. Nutr Hosp % malnourished patients Hernandez-Aranda et al. Rev Gastroenterol Mex % pat. affected by anorexia nervosa (n = 69, mean BMI 15 kg/m²) Ornstein. J Adolesc Health 2003 HYPOPHOSPHATAEMIA (nadir) 55% 98% NOTE parenteral enteral oral Days after start refeeding
22 Serum PO 4 ( mmol/l ) Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Impact of parenteral nutrition on S-PO 4 in malnourished ICU-patients ( first 10 days ) 1,28 0,96 0,64 0,32 severe hypophosphataemia Time ( days ) Knochel JP et al. Arch Intern Med 1977
23 Pathophysiologic aspects of the RFS Starvation or malnutrition catabolic state insulin glucagon Gluconeogenesis, proteolysis loss of weight depletion of vitamin & mineral stores REFEEDING Glucose lipogenesis steatohepatitis thiamine Wernicke syn, met. acidosis hyperosmotic state neutrophil function Insulin Na ECV heart failure edema Transcellular shifts of Glucose, PO 4, K, Mg Mg, K, Ca spasms tetany arrhythmias Boateng AA et al. Nutrition 2010
24 Pathophysiologic aspects of the RFS PO 4 ATP RBC ATP, 2.3-DPG muscle weakness myalgia dyspnea rhabdomyolysis anemia hemolysis O 2 -delivery ischemia, hyperventilation central nervous, gastrontestinal system system respiratory alkalosis acute tubular necrosis weakness tremor ataxia paralysis delirium, coma anorexia constipation Boateng AA et al. Nutrition 2010


25 Pathophysiologic aspects of the RFS PO 4 ATP RBC ATP, 2.3-DPG muscle weakness myalgia dyspnea rhabdomyolysis anemia hemolysis O 2 -delivery ischemia, hyperventilation central nervous, gastrontestinal system system respiratory alkalosis acute tubular necrosis weakness tremor ataxia paralysis delirium, coma anorexia constipation Boateng AA et al. Nutrition 2010
 PO 4 -requirements pro mol glucose 2 mol (glycogen) resp.")
26 Pathophysiologie der Hypophosphatämie Starvation OR malnutrition Catabolism Muscle- and fat-mass PO 4 -loss NOTE: PO 4 -concentration normal, fat-oxidation without PO 4 -products Anabolism ( glucose supply ) PO 4 -requirements pro mol glucose 2 mol (glycogen) resp. 4 mol (Krebs cycle) Insulin glucose / PO 4 -transport in the cell
 PDH Thiamin (aerobic) 2 mol")

27 Glucose metabolism and thiamine use Glycogen 1 mol glucose LDH (anaerobic) PDH Thiamin (aerobic) 2 mol pyruvate oxidation 2 mol lactate pyruvate Krebs cycle acetyl-coa oxidation 38 mol ATP gluconeogenesis glucose Cori cycle


28 Glucose metabolism and thiamine use glukokinase hexokinase 3 glucose-1-p glucose-6-p Pentose phosphate cycle glucose-6-p ribulose-5-p fructose-6-p ribose-5-p fructose-6-p Transketolase Thiamin

29 Criteria for determination of patients at risk of RFS ONE OF THE FOLLOWING BMI < 16 kg/m2 Unintentional weight loss > 15% in the preceding 3-6 months Very little or no nutritional intake for more than 10 days Low levels of serum potassium, phosphate or magnesium prior to feed TWO OF THE FOLLOWING BMI < 18.5 kg/m2 Unintentional weight loss > 10% in the preceding 3-6 months Very little or no nutritional intake for more than 5 days History of alcool or drug abuse FURTHER PATIENTS AT RISK hungerstrikers, anorexia nervosa After bariatric surgery, short bowel syndrome Oncology patients, elderly, chronic alcool or drug abuse NICE. Clinical Guidelines 2006 / Stanga Z et al. EJCN 2007







30 Criteria for confirmation RFS Severly low electrolytes PO 4 < 0.32 mmol/l K < 2.5 mmol/l Mg < 0.5 mmol/l Fluid overload Peripheral oedema or acute circulatory fluid overload REFEEDING SYNDROME Disturbance to organ function respiratory failure, cardiac failure or pulmonary oedema Rio A et al. BMJ Open 2013 / Crook MA et al. Nutrition 2001

31
32 Mr. HA, Tunisian, 27 years old Asylum seeker, in detention pending deportation FH PH AP unremarkable thalassemia minor hunger strike since 4 months (political reason) he drinks only tea and coffee with sugar 20 kg weight loss
33 Status at admission ( prison at our university hospital ) reduced general state, cachectic state 183 cm, 49.5 kg BMI: 15 kg/m² BP 80/55 mmhg, P 56/min, T axilla 35.4 C adynamic, dysphoric, orientated dry mucosae, skin turgor Heart, chest and abdomen control normal Neurostatus: reflexes weak, otherwise normal

34
35 Chronological follow-up kg refuses any nutrition, drinks only tea & coffee with sugar further worsening of the general state, tired, aphatic kg from day 20 after admission forced feeding insertion of a CVC ( v. jugularis ) isocaloric EN (naso-gastral): 750 ml/day PN : standard AIO-solution: ml/day NaCl 0.9%: ml/d Additional i.v./day: KCl 20 mmol, 1 amp. water-soluble vitamins, 1 amp. fat-soluble vitamins, 1 amp. trace elements, 1 amp. zinc of 5 mg
36
37 Refeeding Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Laboratory parameters Date Hb g/dl Proteins g/l 80 Albumin g/l Glucose mmol/l K mmol/l Na mmol/l PO4 mmol/l Ca mmol/l Mg mmol/l Urea mmol/l TSH mu/l ft4 pmol/l Zinc mol/l Vit B1 nmol/l Vit B12 pmol/l Folate nmol/l 10.5 forced feeding



38 Chronological follow-up kg refuses any nutrition, drinks only tea & coffee with sugar further worsening of the general state, tired, aphatic kg from day 20 after admission forced feeding insertion of a CVC ( v. jugularis ) isocaloric EN (naso-gastral): 750 ml/day PN : standard AIO-solution: ml/day NaCl 0.9%: ml/d Additional i.v./day: KCl 20 mmol, 1 amp. water-soluble vitamins, 1 amp. fat-soluble vitamins, 1 amp. trace elements, 1 amp. zinc of 5 mg


39 Refeeding Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Laboratory parameters Date Hb g/dl Proteins g/l 80 Albumin Glucose K Na PO4 Ca Mg Urea g/l mmol/l mmol/l mmol/l mmol/l mmol/l mmol/l mmol/l ? 4.3? 3.6? 137??????? TSH mu/l ft4 pmol/l 8 Zinc Vit B1 Vit B12 mol/l nmol/l pmol/l ??? Folate nmol/l forced feeding 15.5 vertical nystagmus phosphate
40 Chronological follow-up kg tired, apathic, suffer from vertigo clinically: vertical rotating nystagmus PN with unchanged additives KPO4 40 mmol/day stop EN ON (menu) + snacks between kg vertical rot. Nystagmus Wernicke encephalopathy
41 serum parameters Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Serum parameters: starvation refeeding Kalium K (mmol/l) ( mmol/l ) Phosphat PO 4 (mmol/l) ( mmol/l ) Hämoglobin Hb (g/dl) ( g/dl ) Intervals of 1 day time ( dates )
 Kalzium ( mmol/l ) Mg (mmol/l) Magnesium ( mmol/l ) PO 4 (mmol/l) Phosphat ( mmol/l ) 0 20.4 10.5 15.5 18.5 28.5 5.6 15.")
42 serum parameters Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Serum parameters: starvation refeeding Ca (mmol/l) Kalzium ( mmol/l ) Mg (mmol/l) Magnesium ( mmol/l ) PO 4 (mmol/l) Phosphat ( mmol/l ) time ( dates )



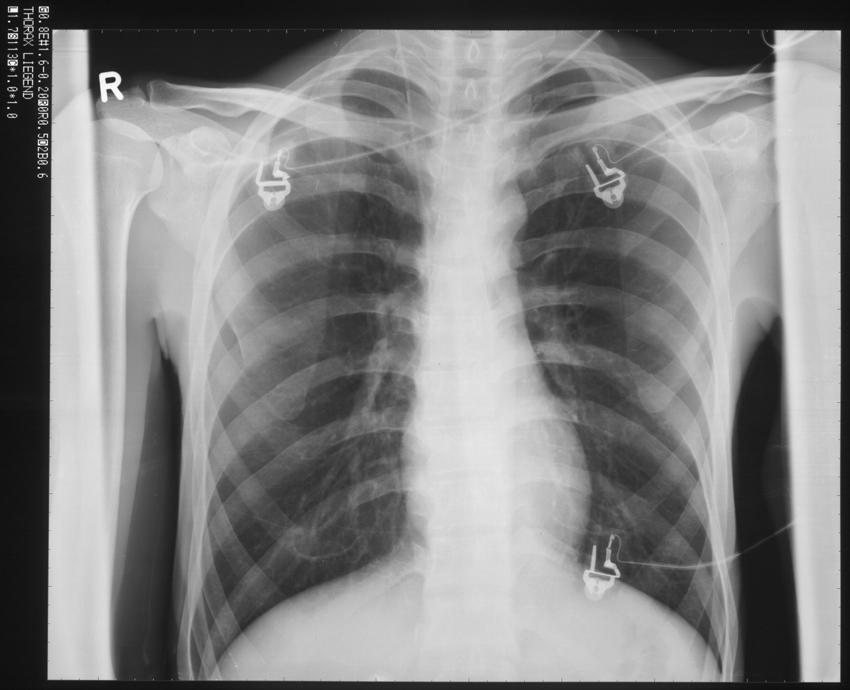
43 horizontal nystagmus vertical nystagmus rotating nystagmus

44 MR brain Contrast enrichment peri-aqueductal (medulla oblungata) TYPICAL LESION OF THIAMINE DEFICIENCY manifestation as Wernicke encephalopathy diplopia, nystagmus, ataxia, consciousness troubles, apathy, confusion, somnolence, dysarthria, dysphagia, etc.
45 Chronological follow-up kg tired, apathic, suffer from vertigo clinically: vertical rotating nystagmus PN with unchanged additives KPO4 40 mmol/day stop EN ON (menu) + snacks between kg vertical rot. Nystagmus Wernicke encephalopathy Start thiamine substitution: 1 amp. 200 mg/day i.v.
46 Refeeding Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland Laboratory parameters Date Hb g/dl Proteins g/l 80 Albumin Glucose K Na PO4 Ca Mg Urea g/l mmol/l mmol/l mmol/l mmol/l mmol/l mmol/l mmol/l ? 4.3? 3.6? 137??????? ? 3.4? 1.14??? 1.52???? TSH mu/l ft4 pmol/l 8 11 Zinc Vit B1 Vit B12 mol/l nmol/l pmol/l ????? Folate nmol/l forced feeding 15.5 vertical nystagmus phosphate 17.5 Wernicke encephalopathy Vit B1
47 anthropometrics Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland anthropometrics: starvation refeeding BW Körpergewicht (kg) ( kg ) BMI ( kg/m2 ) BMI (kg/m 2 ) Intervals of 2 days Zeit (Daten)
 ( kg ) BMI ( kg/m2 ) BMI (kg/m 2 ) 20 10 7.12 23.1 22.4 11.5 14.5 16.5 18.5 20.5 22.5 24.5 26.5 30.5 6.6 13.6 16.")
48 anthropometrics Division of Endocrinology, Diabetes and Clinical Nutrition & Division of General Internal Medicine, University Hospital, Bern, Switzerland anthropometrics: starvation refeeding BW Körpergewicht (kg) ( kg ) BMI ( kg/m2 ) BMI (kg/m 2 ) Intervals of 2 days Zeit (Daten)


49 Chronological follow-up kg tired, apathic, suffer from vertigo clinically: vertical rotating nystagmus PN with unchanged additives KPO4 40 mmol/day stop EN ON (menu) + snacks between kg vertical rot. Nystagmus Wernicke encephalopathy stop PN, stop thiamine i.v kg build up strength, improvement of the general state rotating nystagmus only enhanced by fixation stop i.v. additives, vitamins tabl. orally till hospital discharge kg discharge, rotating nystagmus unchanged!
50 Prevention and treatment of the RFS DAY 1 10 Identification of patients at risk check PO 4, K, Mg Energy: day 1-3 day 4-6 day 7-10 by all routes kcal / kg / day kcal / kg /day kcal / kg /day Electrolytes: baseline, 6 h later, and daily till day 3 of refeeding supplementation according to the plasma levels Trace elements (100% DRI) / vitamins (200% DRI) Give mg thiamine i.v. or p.o. 30 min. before feeding Stanga Z. Eur J Clin Nutr 2008
51 Prevention and treatment of the RFS DAY 1 10 Salt: restrict sodium to <1 mmol / kg / day Fluids: day 1-3 day 4-6 day ml / kg / day ml / kg / day ml / kg / day Body weight: 1x / day, after day 6 2x / week Biochemistry: PO 4, Mg, K, Na, Ca, glucose, creatinie, urea day 1-3 1x / day, after day 4 2x / week Clinical examination: 1x / day (hydration state? Objective: zero fluid balance) Preferably ECG-monitoring in severe cases ( ~24 h ) Stanga Z. Eur J Clin Nutr 2008


52 Hypokalaemia Hypomagnesaemia Hypophosphataemia Thiamine deficiency Salt & water retention Starvation or malnutrition Gluconeogenesis, glycogenolysis & protein catabolism K + Mg 2+ PO 4 2- REFEEDING SYNDROME Depletion of mineral and vitamin stores glucose uptake utilization of thiamine Glucose major energy source protein synthesis Na + retention ECV Insulin secretion Stanga Z. Eur J Clin Nutr 2008


53 Hypokalaemia Hypomagnesaemia Hypophosphataemia Thiamine deficiency Salt & water retention Starvation or malnutrition Gluconeogenesis, glycogenolysis & protein catabolism K + Mg 2+ PO 4 2- REFEEDING SYNDROME Depletion of mineral and vitamin stores glucose uptake utilization of thiamine Glucose major energy source protein synthesis Na + retention ECV Insulin secretion Stanga Z. Eur J Clin Nutr 2008


54
MANAGEMENT AND PREVENTION OF REFEEDING SYNDROME IN INPATIENTS: A PRACTICAL APPROACH
 MANAGEMENT AND PREVENTION OF REFEEDING SYNDROME IN INPATIENTS: A PRACTICAL APPROACH Prof. Zeno Stanga, MD Nutritional Medicine Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism
MANAGEMENT AND PREVENTION OF REFEEDING SYNDROME IN INPATIENTS: A PRACTICAL APPROACH Prof. Zeno Stanga, MD Nutritional Medicine Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism
Refeeding syndrome a practical approach
 Refeeding syndrome a practical approach PENG pre-bapen Conference Teaching Day Birmingham Monday 20 th November 2017 Rhys White Acting Clinical and Operational Lead Dietitian Guys and St Thomas NHS Foundation
Refeeding syndrome a practical approach PENG pre-bapen Conference Teaching Day Birmingham Monday 20 th November 2017 Rhys White Acting Clinical and Operational Lead Dietitian Guys and St Thomas NHS Foundation
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ
 Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
Prevention of Electrolyte Disorders Refeeding Syndrome พญ.น นทพร เต มพรเล ศ Outline Refeeding Syndrome What is refeeding syndrome? What Electrolytes and minerals are involved? Who is at risk? How to manage
Refeeding Syndrom: Ein Update. Prof. Philipp Schuetz, Leitender Arzt Medizinische Uniklinik, Kantonsspital Aarau GESKES Kurs Aarau, April 14 th 2016
 Refeeding Syndrom: Ein Update Prof. Philipp Schuetz, Leitender Arzt Medizinische Uniklinik, Kantonsspital Aarau GESKES Kurs Aarau, April 14 th 2016 Email: Schuetzph@gmail.com Historical perspective First
Refeeding Syndrom: Ein Update Prof. Philipp Schuetz, Leitender Arzt Medizinische Uniklinik, Kantonsspital Aarau GESKES Kurs Aarau, April 14 th 2016 Email: Schuetzph@gmail.com Historical perspective First
Acute management of severe malnutrition. Dr Simon Gabe St Mark s Hospital, London
 Acute management of severe malnutrition Dr Simon Gabe St Mark s Hospital, London Malnutrition definition A state resulting from lack of uptake or intake of nutrition leading to altered body composition
Acute management of severe malnutrition Dr Simon Gabe St Mark s Hospital, London Malnutrition definition A state resulting from lack of uptake or intake of nutrition leading to altered body composition
Dutch consensus statement on Refeeding syndrome
 Dutch consensus statement on Refeeding syndrome Introduction Disease related malnutrition is a common problem in health care. The refeeding syndrome is defined as the severe and potentially fatal shifts
Dutch consensus statement on Refeeding syndrome Introduction Disease related malnutrition is a common problem in health care. The refeeding syndrome is defined as the severe and potentially fatal shifts
Refeeding Low Weight Adolescents with AN
 RCPsych ED 2013 Refeeding Low Weight Adolescents with AN Graeme O Connor RD PhD Research Student -UCL Specialist paediatric Dietitian Great Ormond Street Hospital Foundation Trust Pathophysiology of starvation
RCPsych ED 2013 Refeeding Low Weight Adolescents with AN Graeme O Connor RD PhD Research Student -UCL Specialist paediatric Dietitian Great Ormond Street Hospital Foundation Trust Pathophysiology of starvation
Adaptation and re-feeding Hypokalemia Bone complications
 Adaptation and re-feeding Hypokalemia Bone complications René Klinkby Støving Odense University Hospital Denmark 10% 20% 30% 40% BMI 18.5 BMI 16.5 BMI 14.5 BMI 12.5 Willmore DW, The Metabolic Management
Adaptation and re-feeding Hypokalemia Bone complications René Klinkby Støving Odense University Hospital Denmark 10% 20% 30% 40% BMI 18.5 BMI 16.5 BMI 14.5 BMI 12.5 Willmore DW, The Metabolic Management
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION
 ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
Energy metabolism - the overview
 Energy metabolism - the overview Josef Fontana EC - 40 Overview of the lecture Important terms of the energy metabolism The overview of the energy metabolism The main pathways of the energy metabolism
Energy metabolism - the overview Josef Fontana EC - 40 Overview of the lecture Important terms of the energy metabolism The overview of the energy metabolism The main pathways of the energy metabolism
Acid Base Balance. Professor Dr. Raid M. H. Al-Salih. Clinical Chemistry Professor Dr. Raid M. H. Al-Salih
 Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Case Study: Nutritional management of a patient at high risk of developing refeeding syndrome
 Case Study: Nutritional management of a patient at high risk of developing refeeding syndrome Dolman RC, PhD, Senior Lecturer; Conradie C, MSc, Lecturer Lombard MJ, PhD, Senior Lecturer; Nienaber A, MSc,
Case Study: Nutritional management of a patient at high risk of developing refeeding syndrome Dolman RC, PhD, Senior Lecturer; Conradie C, MSc, Lecturer Lombard MJ, PhD, Senior Lecturer; Nienaber A, MSc,
Formulary and Prescribing Guidelines
 Formulary and Prescribing Guidelines SECTION 15: TREATMENT OF EATING DISORDERS 15.1 Introduction Please review the Trust document Guidelines for the assessment and treatment of eating disorders in the
Formulary and Prescribing Guidelines SECTION 15: TREATMENT OF EATING DISORDERS 15.1 Introduction Please review the Trust document Guidelines for the assessment and treatment of eating disorders in the
Refeeding Syndrome Guideline
 Refeeding Syndrome Guideline Author: Responsible Lead Executive Director: Endorsing Body: Governance or Assurance Committee Pamela Miller Biochemistry Implementation Date: January 2017 Version Number:
Refeeding Syndrome Guideline Author: Responsible Lead Executive Director: Endorsing Body: Governance or Assurance Committee Pamela Miller Biochemistry Implementation Date: January 2017 Version Number:
anabolic pathways- Catabolic Amphibolic
 METABOLISM Introduction The fate of dietary components after digestion and absorption constitute metabolism regulated by metabolic pathway 3 types: anabolic pathways- Synthesis of compound e.g. synthesis
METABOLISM Introduction The fate of dietary components after digestion and absorption constitute metabolism regulated by metabolic pathway 3 types: anabolic pathways- Synthesis of compound e.g. synthesis
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter
 Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Long term monitoring. Dr Alison Culkin Research Dietitian St Mark s Hospital
 Long term monitoring Dr Alison Culkin Research Dietitian St Mark s Hospital Patient 23 year old lady 1/4/14 Colectomy for UC 3-7/4/14 Ischaemic bowel 4 laparotomies Jejunostomy at 35 cm 23/5/14 Weight
Long term monitoring Dr Alison Culkin Research Dietitian St Mark s Hospital Patient 23 year old lady 1/4/14 Colectomy for UC 3-7/4/14 Ischaemic bowel 4 laparotomies Jejunostomy at 35 cm 23/5/14 Weight
Chapter 7- Metabolism: Transformations and Interactions Thomson - Wadsworth
 Chapter 7- Metabolism: Transformations and Interactions 2008 Thomson - Wadsworth Simple Overview of Energy Metabolism The sum of all chemical reactions that go on in living cells Introduction Energy Heat-
Chapter 7- Metabolism: Transformations and Interactions 2008 Thomson - Wadsworth Simple Overview of Energy Metabolism The sum of all chemical reactions that go on in living cells Introduction Energy Heat-
Intensive Care Nutrition. Dr Alan Race BSc(Hons) PhD FRCA
 PhD FRCA") Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Refeeding syndrome: An overlooked condition?
 Focused Review Refeeding syndrome: An overlooked condition? Yuttiwat Vorakunthada MD, Passisd Laoveeravat MD, Wasawat Vutthikraivit MD, Weerapong Lilitwat MD, FAAP, Ariwan Rakvit MD, FACG Abstract Refeeding
Focused Review Refeeding syndrome: An overlooked condition? Yuttiwat Vorakunthada MD, Passisd Laoveeravat MD, Wasawat Vutthikraivit MD, Weerapong Lilitwat MD, FAAP, Ariwan Rakvit MD, FACG Abstract Refeeding
Introduction to Carbohydrate metabolism
 Introduction to Carbohydrate metabolism Some metabolic pathways of carbohydrates 1- Glycolysis 2- Krebs cycle 3- Glycogenesis 4- Glycogenolysis 5- Glyconeogenesis - Pentose Phosphate Pathway (PPP) - Curi
Introduction to Carbohydrate metabolism Some metabolic pathways of carbohydrates 1- Glycolysis 2- Krebs cycle 3- Glycogenesis 4- Glycogenolysis 5- Glyconeogenesis - Pentose Phosphate Pathway (PPP) - Curi
Metabolism. Chapter 5. Catabolism Drives Anabolism 8/29/11. Complete Catabolism of Glucose
 8/29/11 Metabolism Chapter 5 All of the reactions in the body that require energy transfer. Can be divided into: Cell Respiration and Metabolism Anabolism: requires the input of energy to synthesize large
8/29/11 Metabolism Chapter 5 All of the reactions in the body that require energy transfer. Can be divided into: Cell Respiration and Metabolism Anabolism: requires the input of energy to synthesize large
Nutrition in Pancreatic Cancer. Edmond Sung Consultant Gastroenterologist Lead Clinician for Clinical Nutrition and Endoscopy
 Nutrition in Pancreatic Cancer Edmond Sung Consultant Gastroenterologist Lead Clinician for Clinical Nutrition and Endoscopy Overview The pancreas and nutrition Nutrition screening - can we do this well?
Nutrition in Pancreatic Cancer Edmond Sung Consultant Gastroenterologist Lead Clinician for Clinical Nutrition and Endoscopy Overview The pancreas and nutrition Nutrition screening - can we do this well?
6-7 JULY 2015, BIRMINGHAM CONGRESS
 6-7 JULY 2015, BIRMINGHAM CONGRESS Keywords: /Malnutrition/ Enteral feeding/critical illness This article has been double-blind peer reviewed Patients who are critically ill are at greater risk of malnutrition
6-7 JULY 2015, BIRMINGHAM CONGRESS Keywords: /Malnutrition/ Enteral feeding/critical illness This article has been double-blind peer reviewed Patients who are critically ill are at greater risk of malnutrition
Class 3: Refeeding Syndrome. Liz Hudson MPH, RD
 Class 3: Refeeding Syndrome Liz Hudson MPH, RD Case Study #1 NUTRITION ASSESSMENT: Consult PATIENT MEDICAL/HEALTH HISTORY: 49 y/o male with significant history of HTN, DM, and stage V CKD currently on
Class 3: Refeeding Syndrome Liz Hudson MPH, RD Case Study #1 NUTRITION ASSESSMENT: Consult PATIENT MEDICAL/HEALTH HISTORY: 49 y/o male with significant history of HTN, DM, and stage V CKD currently on
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives
 Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
Integration of Metabolism 1. made by: Noor M. ALnairat. Sheet No. 18
 Integration of Metabolism 1 made by: Noor M. ALnairat Sheet No. 18 Data :24/11/2016 SLIDE 2: Metabolism Consist of Highly Interconnected Pathways The basic strategy of catabolic metabolism is to form ATP,
Integration of Metabolism 1 made by: Noor M. ALnairat Sheet No. 18 Data :24/11/2016 SLIDE 2: Metabolism Consist of Highly Interconnected Pathways The basic strategy of catabolic metabolism is to form ATP,
Nutritional Demands of Disease and Trauma
 Nutritional Demands of Disease and Trauma Lecture 89 2000 Northwestern University Medical School Nutritional Requirements Based on needs to support optimal physiological function Are changed by disease
Nutritional Demands of Disease and Trauma Lecture 89 2000 Northwestern University Medical School Nutritional Requirements Based on needs to support optimal physiological function Are changed by disease
Chemistry 1120 Exam 4 Study Guide
 Chemistry 1120 Exam 4 Study Guide Chapter 12 12.1 Identify and differentiate between macronutrients (lipids, amino acids and saccharides) and micronutrients (vitamins and minerals). Master Tutor Section
Chemistry 1120 Exam 4 Study Guide Chapter 12 12.1 Identify and differentiate between macronutrients (lipids, amino acids and saccharides) and micronutrients (vitamins and minerals). Master Tutor Section
Nutrition in Liver Disease An overview of the EASL Clinical Practice Guidelines
 Nutrition in Liver Disease An overview of the EASL Clinical Practice Guidelines Marike Bauermeister Registered Dietitian Wits Donald Gordon Medical Centre Malnutrition Malnutrition is a complication in
Nutrition in Liver Disease An overview of the EASL Clinical Practice Guidelines Marike Bauermeister Registered Dietitian Wits Donald Gordon Medical Centre Malnutrition Malnutrition is a complication in
Nutritional Demands of Disease and Trauma
 al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
al Demands of Disease and Trauma Lecture 89 Medical School al Requirements Based on needs to support optimal physiological function Are changed by disease or injury metabolism is altered to prevent further
Integrative Metabolism: Significance
 Integrative Metabolism: Significance Energy Containing Nutrients Carbohydrates Fats Proteins Catabolism Energy Depleted End Products H 2 O NH 3 ADP + Pi NAD + NADP + FAD + Pi NADH+H + NADPH+H + FADH2 Cell
Integrative Metabolism: Significance Energy Containing Nutrients Carbohydrates Fats Proteins Catabolism Energy Depleted End Products H 2 O NH 3 ADP + Pi NAD + NADP + FAD + Pi NADH+H + NADPH+H + FADH2 Cell
Protein & Amino Acid Metabolism
 Pathophysiology 101-823 Unit 4 Metabolism & Metabolic Disease Protein & Amino Acid Metabolism Paul Anderson FALL 2008 Learning Objectives 1. List the metabolic functions of proteins & amino acids. 2. Explain
Pathophysiology 101-823 Unit 4 Metabolism & Metabolic Disease Protein & Amino Acid Metabolism Paul Anderson FALL 2008 Learning Objectives 1. List the metabolic functions of proteins & amino acids. 2. Explain
GUIDANCE NOTES. DIETETIC RISK ASSESSMENT FOR REFEEDING RECOMMENDED MEAL PLANS When commencing re-feeding: NICE (2006)
") When commencing re-feeding: NICE (2006) NICE (2006) Clinical Guideline 32 Nutrition support in adults: oral nutrition support, enteral tube feeding and parenteral nutrition (The following is based on www.nice.org.uk/cg032
When commencing re-feeding: NICE (2006) NICE (2006) Clinical Guideline 32 Nutrition support in adults: oral nutrition support, enteral tube feeding and parenteral nutrition (The following is based on www.nice.org.uk/cg032
CHY2026: General Biochemistry UNIT 7& 8: CARBOHYDRATE METABOLISM
 CHY2026: General Biochemistry UNIT 7& 8: CARBOHYDRATE METABOLISM Metabolism Bioenergetics is the transfer and utilization of energy in biological systems The direction and extent to which a chemical reaction
CHY2026: General Biochemistry UNIT 7& 8: CARBOHYDRATE METABOLISM Metabolism Bioenergetics is the transfer and utilization of energy in biological systems The direction and extent to which a chemical reaction
Cellular Respiration Other Metabolites & Control of Respiration. AP Biology
 Cellular Respiration Other Metabolites & Control of Respiration Cellular respiration: Beyond glucose: Other carbohydrates: Glycolysis accepts a wide range of carbohydrates fuels. polysaccharides glucose
Cellular Respiration Other Metabolites & Control of Respiration Cellular respiration: Beyond glucose: Other carbohydrates: Glycolysis accepts a wide range of carbohydrates fuels. polysaccharides glucose
ESPEN Congress Florence 2008
 ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in pancreas diseases L. Gianotti (Italy) ESPEN Guidelines on Parenteral Nutrition: Pancreas L.Gianotti, R.Meier, D.N.Lobo, C.Bassi,
ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in pancreas diseases L. Gianotti (Italy) ESPEN Guidelines on Parenteral Nutrition: Pancreas L.Gianotti, R.Meier, D.N.Lobo, C.Bassi,
HISTORY OF THE KETOGENIC DIET
 Laura Roche RD Horizon Health Authority May 29, 2018 AGENDA History of the Ketogenic Diet Diet Pathophysiology Side Effects Pros and Cons How and Why the Diet works Ketogenic Diet for Type 2 Diabetes Ketogenic
Laura Roche RD Horizon Health Authority May 29, 2018 AGENDA History of the Ketogenic Diet Diet Pathophysiology Side Effects Pros and Cons How and Why the Diet works Ketogenic Diet for Type 2 Diabetes Ketogenic
BIOCHEMISTRY. Glycolysis. by Dr Jaya Vejayan Faculty of Industrial Sciences & Technology
 BIOCHEMISTRY Glycolysis by Dr Jaya Vejayan Faculty of Industrial Sciences & Technology email: jayavejayan@ump.edu.my Chapter Description Overview This chapter is related to carbohydrate catabolism. It
BIOCHEMISTRY Glycolysis by Dr Jaya Vejayan Faculty of Industrial Sciences & Technology email: jayavejayan@ump.edu.my Chapter Description Overview This chapter is related to carbohydrate catabolism. It
CARBOHYDRATE METABOLISM
 Note (Study Glycolysis, fermentation and their regulation, Gluconeogenesis and glycogenolysis, Metabolism of galactose, TCA cycle and Amphibolic role of the cycle, and Glyoxalic acid cycle, HMP shunt in
Note (Study Glycolysis, fermentation and their regulation, Gluconeogenesis and glycogenolysis, Metabolism of galactose, TCA cycle and Amphibolic role of the cycle, and Glyoxalic acid cycle, HMP shunt in
ESPEN Congress Vienna Neglected deficiencies in severe malnutrition: Commentary - Thiamine. E. Doberer (Austria)
") ESPEN Congress Vienna 2009 Neglected deficiencies in severe malnutrition: Commentary - Thiamine E. Doberer (Austria) Neglected deficiencies in severe malnutrition: Commentary - Thiamine Edith Doberer Department
ESPEN Congress Vienna 2009 Neglected deficiencies in severe malnutrition: Commentary - Thiamine E. Doberer (Austria) Neglected deficiencies in severe malnutrition: Commentary - Thiamine Edith Doberer Department
Financial Interest Disclosure (over the past 24 months)
") : Across the Spectrum of Primary care Jan Greenwood, R.D. Nutrition Support Consultant The Basic Five Programs The opinions expressed in this presentation are that of the presenter and do not necessarily
: Across the Spectrum of Primary care Jan Greenwood, R.D. Nutrition Support Consultant The Basic Five Programs The opinions expressed in this presentation are that of the presenter and do not necessarily
METABOLISM Sri Widia A Jusman Department of Biochemistry & Molecular Biology FMUI
 METABOLISM Sri Widia A Jusman Department of Biochemistry & Molecular Biology FMUI 1 METABOLISM Process of how cells acquire, transform, store and use energy Study of the chemistry, regulation and energetics
METABOLISM Sri Widia A Jusman Department of Biochemistry & Molecular Biology FMUI 1 METABOLISM Process of how cells acquire, transform, store and use energy Study of the chemistry, regulation and energetics
Alterations in Fluids and Electrolytes During Refeeding Syndrome. Objectives. Refeeding Syndrome (RS) 4/26/2013. Barbara Magnuson, PharmD, BCNSP
 4/26/2013. Barbara Magnuson, PharmD, BCNSP") Alterations in Fluids and Electrolytes During Refeeding Syndrome Barbara Magnuson, PharmD, BCNSP Objectives Define refeeding syndrome including its signs and symptoms Identify fluid and electrolyte disturbances
Alterations in Fluids and Electrolytes During Refeeding Syndrome Barbara Magnuson, PharmD, BCNSP Objectives Define refeeding syndrome including its signs and symptoms Identify fluid and electrolyte disturbances
ESPEN LLL Programme in Clinical Nutrition and Metabolism. List of Topics and Modules 2014
 ESPEN LLL Programme in Clinical Nutrition and Metabolism List of Topics and Modules 204 Code Title Credits for Live course Credits for on-line course Credits for Grading Quiz Topic 0 Introduction in Nutrition
ESPEN LLL Programme in Clinical Nutrition and Metabolism List of Topics and Modules 204 Code Title Credits for Live course Credits for on-line course Credits for Grading Quiz Topic 0 Introduction in Nutrition
, 吳文傑. Refeeding syndrome (RFS) is a well described but often forgotten condition,
 is a well described but often forgotten condition,") 中文題目 : 再餵食症候群 - 病例報告 英文題目 : Refeeding syndrome in a patient with suspected MEN-I syndrome: a case report 作者 : 楊光祖 1, 沈曉津 2, 廖麗瑛 3 3*, 吳文傑 1 服務單位 : 臺北市立聯合醫院仁愛院區內科部臺北市立聯合醫院仁愛院區教學 2 研究部臺北市立聯合醫院仁愛院區消化內科 Introduction
中文題目 : 再餵食症候群 - 病例報告 英文題目 : Refeeding syndrome in a patient with suspected MEN-I syndrome: a case report 作者 : 楊光祖 1, 沈曉津 2, 廖麗瑛 3 3*, 吳文傑 1 服務單位 : 臺北市立聯合醫院仁愛院區內科部臺北市立聯合醫院仁愛院區教學 2 研究部臺北市立聯合醫院仁愛院區消化內科 Introduction
Intermediary metabolism. Eva Samcová
 Intermediary metabolism Eva Samcová Metabolic roles of tissues Four major tissues play a dominant role in fuel metabolism : liver, adipose, muscle, and brain. These tissues do not function in isolation.
Intermediary metabolism Eva Samcová Metabolic roles of tissues Four major tissues play a dominant role in fuel metabolism : liver, adipose, muscle, and brain. These tissues do not function in isolation.
EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion , version 1.1
 Nutriflex Omega peri emulsion for infusion , version 1.1") EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion 13.7.2015, version 1.1 III.1. Elements for a Public Summary III.1.1. Overview of disease epidemiology Patients may need parenteral
EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion 13.7.2015, version 1.1 III.1. Elements for a Public Summary III.1.1. Overview of disease epidemiology Patients may need parenteral
Integration Of Metabolism
 Integration Of Metabolism Metabolism Consist of Highly Interconnected Pathways The basic strategy of catabolic metabolism is to form ATP, NADPH, and building blocks for biosyntheses. 1. ATP is the universal
Integration Of Metabolism Metabolism Consist of Highly Interconnected Pathways The basic strategy of catabolic metabolism is to form ATP, NADPH, and building blocks for biosyntheses. 1. ATP is the universal
Dr. Mohnen s notes on GLUCONEOGENESIS
 Dr. Mohnen s notes on GLUCONEOGENESIS Note: Even though we did not get through all of these slides during lecture, I advise you to look them all through because they will be helpful to you as you learn
Dr. Mohnen s notes on GLUCONEOGENESIS Note: Even though we did not get through all of these slides during lecture, I advise you to look them all through because they will be helpful to you as you learn
Metabolism of cardiac muscle. Dr. Mamoun Ahram Cardiovascular system, 2013
 Metabolism of cardiac muscle Dr. Mamoun Ahram Cardiovascular system, 2013 References This lecture Mark s Basic Medical Biochemistry, 4 th ed., p. 890-891 Hand-out Why is this topic important? Heart failure
Metabolism of cardiac muscle Dr. Mamoun Ahram Cardiovascular system, 2013 References This lecture Mark s Basic Medical Biochemistry, 4 th ed., p. 890-891 Hand-out Why is this topic important? Heart failure
Energy Metabolism. Chapter Cengage Learning. All Rights Reserved.
 Energy Metabolism Chapter 7 Introduction Energy Heat, mechanical, electrical, and chemical Metabolism How the body uses foods to meet its needs Chemical Reactions in the Body Energy metabolism How body
Energy Metabolism Chapter 7 Introduction Energy Heat, mechanical, electrical, and chemical Metabolism How the body uses foods to meet its needs Chemical Reactions in the Body Energy metabolism How body
Transfer of food energy to chemical energy. Includes anabolic and catabolic reactions. The cell is the metabolic processing center
 Metabolism There are a lot of diagrams here. DO NOT, I repeat, DO NOT get overly anxious or excited about them. We will go through them again slowly!! Read the slides, read the book, DO NOT TAKE NOTES.
Metabolism There are a lot of diagrams here. DO NOT, I repeat, DO NOT get overly anxious or excited about them. We will go through them again slowly!! Read the slides, read the book, DO NOT TAKE NOTES.
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY
 1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS An Overview WHAT IS HOMEOSTASIS? Homeostasis
1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS An Overview WHAT IS HOMEOSTASIS? Homeostasis
Biol 219 Lec 7 Fall 2016
 Cellular Respiration: Harvesting Energy to form ATP Cellular Respiration and Metabolism Glucose ATP Pyruvate Lactate Acetyl CoA NAD + Introducing The Players primary substrate for cellular respiration
Cellular Respiration: Harvesting Energy to form ATP Cellular Respiration and Metabolism Glucose ATP Pyruvate Lactate Acetyl CoA NAD + Introducing The Players primary substrate for cellular respiration
Hormonal regulation of. Physiology Department Medical School, University of Sumatera Utara
 Hormonal regulation of nutrient metabolism Physiology Department Medical School, University of Sumatera Utara Homeostasis & Controls Successful compensation Homeostasis reestablished Failure to compensate
Hormonal regulation of nutrient metabolism Physiology Department Medical School, University of Sumatera Utara Homeostasis & Controls Successful compensation Homeostasis reestablished Failure to compensate
Refeeding Syndrome: An Important Complication Following Obesity Surgery
 Received: July 27, 2015 Accepted: October 28, 2015 Published online: January 9, 2016 2016 The Author(s) Published by S. Karger GmbH, Freiburg 1662 4033/15/0091 0012$39.50/0 This article is licensed under
Received: July 27, 2015 Accepted: October 28, 2015 Published online: January 9, 2016 2016 The Author(s) Published by S. Karger GmbH, Freiburg 1662 4033/15/0091 0012$39.50/0 This article is licensed under
Major Pathways in Carbohydrate Metabolism
 Major Pathways in Carbohydrate Metabolism 70 Stage 1: Digestion of Carbohydrates In Stage 1, the digestion of carbohydrates Begins in the mouth where salivary amylase breaks down polysaccharides to smaller
Major Pathways in Carbohydrate Metabolism 70 Stage 1: Digestion of Carbohydrates In Stage 1, the digestion of carbohydrates Begins in the mouth where salivary amylase breaks down polysaccharides to smaller
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology
 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
Intradialytic Parenteral Nutrition in Hemodialysis Patients. Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia
 Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Disclaimer. Chapter 3 Disorder of Water, Electrolyte and Acid-base Professor A. S. Alhomida. Disorder of Water and Electrolyte
 Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS
 NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
List of Topics and Modules (2012)
") List of Topics and Modules (202) Code Title Credits for Live course Topic 0 Introduction to Clinical Nutrition EDU T0 M 0. Introduction to clinical nutrition support Topic Metabolism of Metabolism of Macronutrients,
List of Topics and Modules (202) Code Title Credits for Live course Topic 0 Introduction to Clinical Nutrition EDU T0 M 0. Introduction to clinical nutrition support Topic Metabolism of Metabolism of Macronutrients,
Ketones: A barrier to treatment
 KCL Division of Women s Health Ketones: A barrier to treatment Professor Cathy Nelson-Piercy Consultant Obstetric Physician Ketones / ketonuria Page 1 The presence and quantity of ketones in the urine
KCL Division of Women s Health Ketones: A barrier to treatment Professor Cathy Nelson-Piercy Consultant Obstetric Physician Ketones / ketonuria Page 1 The presence and quantity of ketones in the urine
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 25 Metabolism and Nutrition Metabolic Reactions Metabolism refers to all of the chemical reactions taking place in the body. Reactions that break
Principles of Anatomy and Physiology 14 th Edition CHAPTER 25 Metabolism and Nutrition Metabolic Reactions Metabolism refers to all of the chemical reactions taking place in the body. Reactions that break
Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + )
") Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration in body fluids Precise regulation of ph at
Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration in body fluids Precise regulation of ph at
Chapter 8. Chapter 8: Protein-energy Malnutrition
 Chapter 8 Introduction to Nutrition and Metabolism, 3 rd edition David A Bender Taylor & Francis Ltd, London 2002 Chapter 8: Protein-energy Malnutrition Press the space bar or click the mouse to build
Chapter 8 Introduction to Nutrition and Metabolism, 3 rd edition David A Bender Taylor & Francis Ltd, London 2002 Chapter 8: Protein-energy Malnutrition Press the space bar or click the mouse to build
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
Lecture 5: Cell Metabolism. Biology 219 Dr. Adam Ross
 Lecture 5: Cell Metabolism Biology 219 Dr. Adam Ross Cellular Respiration Set of reactions that take place during the conversion of nutrients into ATP Intricate regulatory relationship between several
Lecture 5: Cell Metabolism Biology 219 Dr. Adam Ross Cellular Respiration Set of reactions that take place during the conversion of nutrients into ATP Intricate regulatory relationship between several
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Acid-Base Balance Dr. Gary Mumaugh
 Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
INTEGRATION OF METABOLISM
 SIBC511- INTEGRATION OF METABOLISM Assistant Professor Dr. Chatchawan Srisawat INTEGRATION OF METABOLISM INTEGRATION OF METABOLISM Dietary intake Fed state Fasting state The metabolism of carbohydrate,
SIBC511- INTEGRATION OF METABOLISM Assistant Professor Dr. Chatchawan Srisawat INTEGRATION OF METABOLISM INTEGRATION OF METABOLISM Dietary intake Fed state Fasting state The metabolism of carbohydrate,
Nutrition Competency Framework (NCF) March 2016
 March 2016") K1 SCIENCES understanding of the basic sciences in relation to nutrition Framework (NCF) March 2016 1. Describe the functions of essential nutrients, and the basis for the biochemical demand for energy
K1 SCIENCES understanding of the basic sciences in relation to nutrition Framework (NCF) March 2016 1. Describe the functions of essential nutrients, and the basis for the biochemical demand for energy
Final Review Sessions. 3/16 (FRI) 126 Wellman (4-6 6 pm) 3/19 (MON) 1309 Surge 3 (4-6 6 pm) Office Hours
 126 Wellman (4-6 6 pm) 3/19 (MON) 1309 Surge 3 (4-6 6 pm) Office Hours") Final Review Sessions 3/16 (FRI) 126 Wellman (4-6 6 pm) 3/19 (MON) 1309 Surge 3 (4-6 6 pm) Office ours 3/14 (WED) 9:30 11:30 am (Rebecca) 3/16 (FRI) 9-11 am (Abel) Final ESSENTIALS Posted Lecture 20 ormonal
Final Review Sessions 3/16 (FRI) 126 Wellman (4-6 6 pm) 3/19 (MON) 1309 Surge 3 (4-6 6 pm) Office ours 3/14 (WED) 9:30 11:30 am (Rebecca) 3/16 (FRI) 9-11 am (Abel) Final ESSENTIALS Posted Lecture 20 ormonal
Metabolic integration and Regulation
 Metabolic integration and Regulation 109700: Graduate Biochemistry Trimester 2/2016 Assistant Prof. Dr. Panida Khunkaewla kpanida@sut.ac.th School of Chemistry Suranaree University of Technology 1 Overview
Metabolic integration and Regulation 109700: Graduate Biochemistry Trimester 2/2016 Assistant Prof. Dr. Panida Khunkaewla kpanida@sut.ac.th School of Chemistry Suranaree University of Technology 1 Overview
NUTRITION. Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017
 NUTRITION Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017 Step One Competency 1.19 Factors contributing to nutritional impairment in critical illness. Nutritional
NUTRITION Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017 Step One Competency 1.19 Factors contributing to nutritional impairment in critical illness. Nutritional
Acid Base Balance. Chapter 26 Balance. ph Imbalances. Acid Base Balance. CO 2 and ph. Carbonic Acid. Part 2. Acid/Base Balance
 Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Glucose is the only source of energy in red blood cells. Under starvation conditions ketone bodies become a source of energy for the brain
 Glycolysis 4 / The Text :- Some Points About Glucose Glucose is very soluble source of quick and ready energy. It is a relatively stable and easily transported. In mammals, the brain uses only glucose
Glycolysis 4 / The Text :- Some Points About Glucose Glucose is very soluble source of quick and ready energy. It is a relatively stable and easily transported. In mammals, the brain uses only glucose
ESPEN Congress Gothenburg Combined parenteral and enteral nutrition. Crohn s disease. Željko Krznarić
 ESPEN Congress Gothenburg 2011 Combined parenteral and enteral nutrition Crohn s disease Željko Krznarić ŽELJKO KRZNARIĆ, FEBGH U N I V E R S I T Y OF Z A G R E B C R O A T I A EDUCATIONAL SESSION COMBINED
ESPEN Congress Gothenburg 2011 Combined parenteral and enteral nutrition Crohn s disease Željko Krznarić ŽELJKO KRZNARIĆ, FEBGH U N I V E R S I T Y OF Z A G R E B C R O A T I A EDUCATIONAL SESSION COMBINED
Case Study: Carbohydrate Metabolism. eating an early dinner the night before and skipping breakfast that morning, Sid goes to the
 Student Name Biochemistry 4320 Case Study Part I 4 November 2013 Case Study: Carbohydrate Metabolism Sid is a high school student who has decided to start exercising before school. After eating an early
Student Name Biochemistry 4320 Case Study Part I 4 November 2013 Case Study: Carbohydrate Metabolism Sid is a high school student who has decided to start exercising before school. After eating an early
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Metformin Hydrochloride
 Metformin Hydrochloride 500 mg, 850 mg, 500 mg LA and 750 mg LA Tablet Description Informet is a preparation of metformin hydrochloride that belongs to a biguanide class of oral antidiabetic drugs. Metformin
Metformin Hydrochloride 500 mg, 850 mg, 500 mg LA and 750 mg LA Tablet Description Informet is a preparation of metformin hydrochloride that belongs to a biguanide class of oral antidiabetic drugs. Metformin
Glucose. Glucose. Insulin Action. Introduction to Hormonal Regulation of Fuel Metabolism
 Glucose Introduction to Hormonal Regulation of Fuel Metabolism Fasting level 3.5-5 mmol (1 mmol = 18 mg/dl) Postprandial 6-10 mmol Amount of glucose in circulation is dependent on: Absorption from the
Glucose Introduction to Hormonal Regulation of Fuel Metabolism Fasting level 3.5-5 mmol (1 mmol = 18 mg/dl) Postprandial 6-10 mmol Amount of glucose in circulation is dependent on: Absorption from the
TOTAL PARENTERAL NUTRITION
 TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
BUFFERING OF HYDROGEN LOAD
 BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
Amino Acids and Sorbitol injection with/without Electrolytes NIRMIN *
 For the use of a registered medical practitioner or a Hospital or a Laboratory only Amino Acids and Sorbitol injection with/without Electrolytes NIRMIN * DESCRIPTION: NIRMIN * is a clear, colourless injection
For the use of a registered medical practitioner or a Hospital or a Laboratory only Amino Acids and Sorbitol injection with/without Electrolytes NIRMIN * DESCRIPTION: NIRMIN * is a clear, colourless injection
Glycolysis Introduction to Metabolism Regulation of Metabolism Overview of Glycolysis Reactions of Glycolysis
 Glycolysis Introduction to Metabolism Regulation of Metabolism Overview of Glycolysis Reactions of Glycolysis Suggested Reading: Lippincot s Ilustrated reviews: Biochemistry Glycolysis, an example of metabolic
Glycolysis Introduction to Metabolism Regulation of Metabolism Overview of Glycolysis Reactions of Glycolysis Suggested Reading: Lippincot s Ilustrated reviews: Biochemistry Glycolysis, an example of metabolic
What systems are involved in homeostatic regulation (give an example)?
?") 1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS (Diabetes Mellitus Part 1): An Overview
1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS (Diabetes Mellitus Part 1): An Overview
Biochemistry 7/11/ Bio-Energetics & ATP. 5.1) ADP, ATP and Cellular Respiration OVERVIEW OF ENERGY AND METABOLISM
 ADP, ATP and Cellular Respiration OVERVIEW OF ENERGY AND METABOLISM") Biochemistry 5. Bio-Energetics & ATP 5.1) ADP, ATP and Cellular Respiration Prof. Dr. Klaus Heese OVERVIEW OF ENERGY AND METABOLISM 1. The food we eat, (carbohydrates/ glucose /sugar, lipids/fat, proteins),
Biochemistry 5. Bio-Energetics & ATP 5.1) ADP, ATP and Cellular Respiration Prof. Dr. Klaus Heese OVERVIEW OF ENERGY AND METABOLISM 1. The food we eat, (carbohydrates/ glucose /sugar, lipids/fat, proteins),
Nutrients. Chapter 25 Nutrition, Metabolism, Temperature Regulation
 Chapter 25 Nutrition, Metabolism, Temperature Regulation 25-1 Nutrients Chemicals used by body to produce energy, provide building blocks or function in other chemical reactions Classes Carbohydrates,
Chapter 25 Nutrition, Metabolism, Temperature Regulation 25-1 Nutrients Chemicals used by body to produce energy, provide building blocks or function in other chemical reactions Classes Carbohydrates,
Hyperglycaemic Emergencies GRI EDUCATION
 Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Glossary. acute PEM protein-energy malnutrition caused by recent severe food restriction; characterized in children by thinness for height (wasting).
.") Glossary Protein acidosis above-normal acidity in the blood and body fluids. acids compounds that release hydrogen ions in a solution. acute PEM protein-energy malnutrition caused by recent severe food
Glossary Protein acidosis above-normal acidity in the blood and body fluids. acids compounds that release hydrogen ions in a solution. acute PEM protein-energy malnutrition caused by recent severe food
Accepted Article. Celiac crisis in adults: a case report and review of the literature focusing in the prevention of refeeding syndrome
 Accepted Article Celiac crisis in adults: a case report and review of the literature focusing in the prevention of refeeding syndrome Marcela de Almeida Menezes, Vírginia Cabral, Sônia Letícia Silva Lorena
Accepted Article Celiac crisis in adults: a case report and review of the literature focusing in the prevention of refeeding syndrome Marcela de Almeida Menezes, Vírginia Cabral, Sônia Letícia Silva Lorena
Regulation of Metabolism
 Regulation of Metabolism Pratt and Cornely Chapter 19 Regulation by Compartmentalization Form of reciprocal regulation Degradation vs biosynthesis Requires transporters 1 Specialization of organs Fuel
Regulation of Metabolism Pratt and Cornely Chapter 19 Regulation by Compartmentalization Form of reciprocal regulation Degradation vs biosynthesis Requires transporters 1 Specialization of organs Fuel
Medical Biochemistry and Molecular Biology department
 Medical Biochemistry and Molecular Biology department Cardiac Fuels [Sources of energy for the Cardiac muscle] Intended learning outcomes of the lecture: By the end of this lecture you would be able to:-
Medical Biochemistry and Molecular Biology department Cardiac Fuels [Sources of energy for the Cardiac muscle] Intended learning outcomes of the lecture: By the end of this lecture you would be able to:-
Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015
 Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015 Protein-calorie malnutrition (PCM) is extremely common
Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015 Protein-calorie malnutrition (PCM) is extremely common
Macro- and Micronutrient Homeostasis in the Setting of Chronic Kidney Disease. T. Alp Ikizler, MD Vanderbilt University Medical Center
 Macro- and Micronutrient Homeostasis in the Setting of Chronic Kidney Disease T. Alp Ikizler, MD Vanderbilt University Medical Center Nutrition and Chronic Kidney Disease What is the disease itself and
Macro- and Micronutrient Homeostasis in the Setting of Chronic Kidney Disease T. Alp Ikizler, MD Vanderbilt University Medical Center Nutrition and Chronic Kidney Disease What is the disease itself and
ENERGY FROM INGESTED NUTREINTS MAY BE USED IMMEDIATELY OR STORED
 QUIZ/TEST REVIEW NOTES SECTION 1 SHORT TERM METABOLISM [METABOLISM] Learning Objectives: Identify primary energy stores of the body Differentiate the metabolic processes of the fed and fasted states Explain
QUIZ/TEST REVIEW NOTES SECTION 1 SHORT TERM METABOLISM [METABOLISM] Learning Objectives: Identify primary energy stores of the body Differentiate the metabolic processes of the fed and fasted states Explain
OVERVIEW OF ENERGY AND METABOLISM
 Biochemistry 5. Bio-Energetics & ATP 5.1) ADP, ATP and Cellular Respiration OVERVIEW OF ENERGY AND METABOLISM 1. The food we eat, (carbohydrates/ glucose /sugar, lipids/fat, proteins), are our only source
Biochemistry 5. Bio-Energetics & ATP 5.1) ADP, ATP and Cellular Respiration OVERVIEW OF ENERGY AND METABOLISM 1. The food we eat, (carbohydrates/ glucose /sugar, lipids/fat, proteins), are our only source