UPDATES, 2018 NTDS PILOT (PROPOSED CHANGES TO 2020 NTDB DATA DICTIONARY) AND TQIP PROCESS MEASURES. Lita Holdeman, BS, CSTR AOTR Education Chair
|
|
|
- Conrad Griffin
- 5 years ago
- Views:
Transcription
 AND TQIP PROCESS MEASURES Lita Holdeman, BS, CSTR AOTR")
1 UPDATES, 2018 NTDS PILOT (PROPOSED CHANGES TO 2020 NTDB DATA DICTIONARY) AND TQIP PROCESS MEASURES Lita Holdeman, BS, CSTR AOTR Education Chair
2 Disclaimer Notice: All information provide to you at any specific time is as accurate as possible. The NTDS/TQIP change definitions and information frequently. If you have questions about the information provided, contact TQIP at You are encouraged to share corrected information with the AOTR group. Please remember to collect the information the way YOUR facility wants the information.
3 Did the patient report smoking cigarettes within the 12 months prior to injury YES NO Did the patient have a diagnosis of Tobacco Use disorder present prior to injury? Do not report Current Smoker Yes NO Report Current Smoker and Substance Abuse Disorder to NTDB Report Current Smoker to NTDB **Taken From TQIP
4 Alcohol Use Disorder Question: Are Alcohol Use Disorder and Alcohol Abuse the same? Answer from TQIP: No On page A3.1, the definition of Alcohol Use Disorder states Diagnosis of alcohol use disorder in the patient s medical record, present to prior to injury. On page A3.3, the definition of Substance Abuse Disorder states, Documentation of Substance Abuse Disorder documented in the patient medical record, present prior to injury. A diagnosis of Substance Abuse Disorder must be documented in the patient s medical record. The NTDB is collecting data on patients that has a diagnosis of alcohol use disorder.
5 Initial, Subsequent And Sequela Coding
6 Initial, Subsequent and Sequela Coding Seventh character A, initial encounter, is used while the patient is receiving active treatment for a condition. Examples of active treatment are surgical treatment, emergency department encounters, and evaluation and continuing treatment by the same or a different physician.
7 Initial, Subsequent and Sequela Coding Cont d A - Initial encounter for closed fracture B - Initial encounter for open fracture, type I or II C - Initial encounter for open fracture, type IIIA, IIIB or IIIC
8 Initial, Subsequent and Sequela Coding Seventh character D, subsequent encounter, is used for encounters after the patient has received active treatment of a condition and is receiving routine care for the condition during the healing or recovery phase. For fractures you can have additional seventh character of E, F, G, H, J, K, M, N, P, Q, R the meanings are on the next slides. Examples of subsequent care are cast change or removal, an X-ray to check healing status of fracture, removal of external or internal fixation device, medication adjustment, other aftercare, and follow-up visits following treatment of the injury or condition.
9 Initial, Subsequent and Sequela Coding Cont d D - Subsequent encounter for closed fracture with routine healing E - Subsequent encounter for open fracture, type I or II, with routine healing F - Subsequent encounter for open fracture, type IIIA, IIIB or IIIC, with routine healing G - Subsequent encounter for closed fracture with delayed healing
10 Initial, Subsequent and Sequela Coding Cont d H - Subsequent encounter for open fracture, type I or II, with delayed healing J - Subsequent encounter for open fracture, type IIIA, IIIB or IIIC, with delayed healing K - Subsequent encounter for closed fracture with nonunion M- Subsequent encounter for open fracture, type I or II, with nonunion N - Subsequent encounter for open fracture, type IIIA, IIIB or IIIC, with nonunion
11 Initial, Subsequent and Sequela Coding Cont d P - Subsequent encounter for closed fracture with malunion Q- Subsequent encounter for open fracture, type I or II, with malunion R- Subsequent encounter for open fracture, type IIIA, IIIB or IIIC, with malunion S -Sequela
12 Initial, Subsequent and Sequela Coding Seventh character S, sequela, is for use for complications or conditions that arise as a direct result of a condition, such as scar formation after a burn. The scars are sequelae of the burn. The S is added only to the injury code, not the sequela code. The seventh character S identifies the injury responsible for the sequela. The specific type of sequela (e.g. scar) is sequenced first, followed by the injury code.


13 2018 NTDS Pilot NTDS Proposed changes for 2020

14 Inclusion Criteria
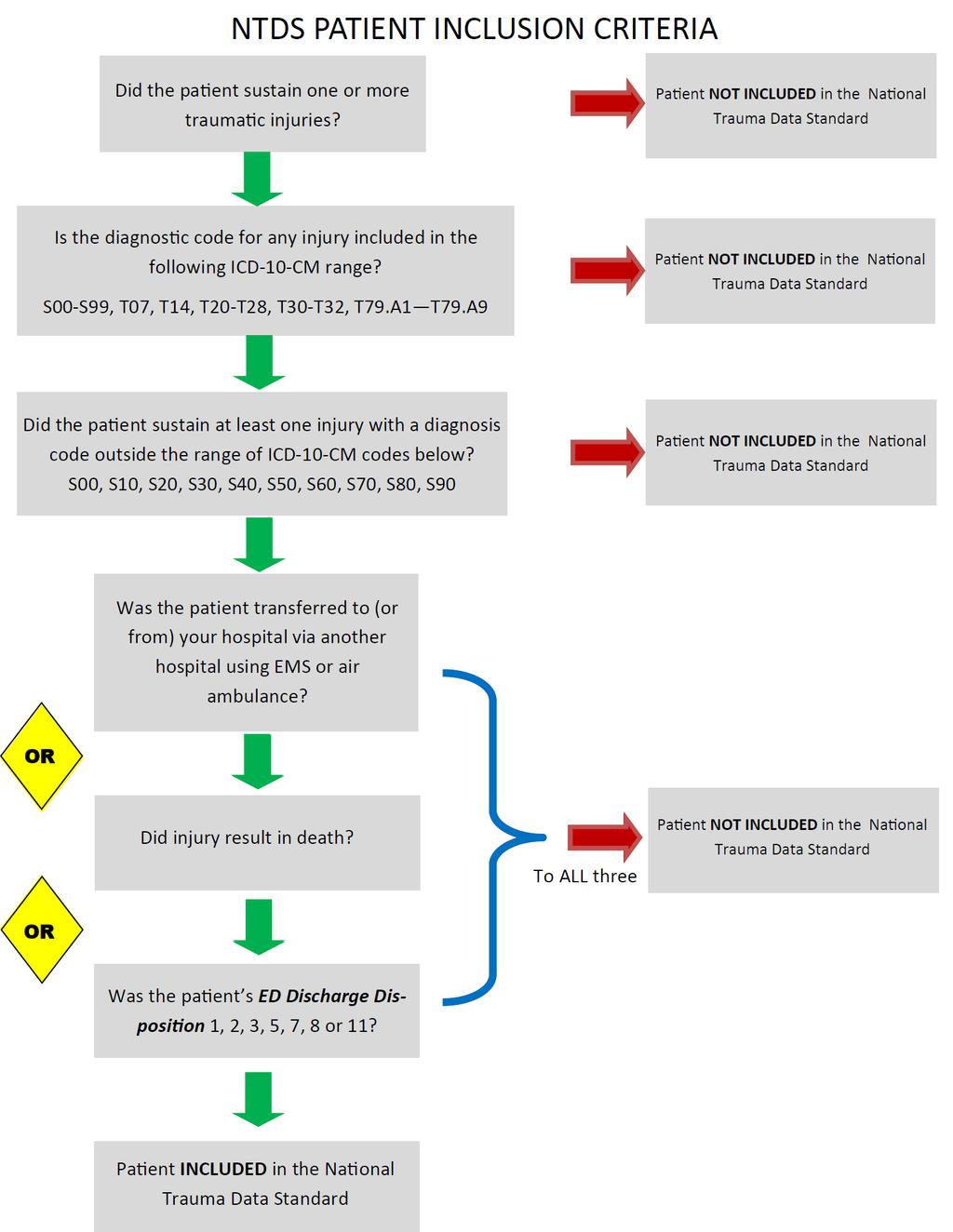
15
16 Topics of proposed changes ED Discharge Disposition-updated definition Alcohol Use Disorder- updated definition Mental/Personality Disorder-updated definition Physicians Orders for Life-sustaining treatment (POLST)-new field Pregnancy-new field Substance abuse disorder-updated definition Delirium-new field
17 Topics of proposed changes cont d Myocardial Infarction (MI)-updated information Unplanned visit to the operating room-updated definition Unplanned Visit to OR-if it is stated in the OR note they are planning to return to OR this by NTDS standard is still considered an unplanned visit to OR. Packed Red Blood Cells-updated collection to CCs instead of CCs or units- doing away with conversion Whole Blood-New Field Plasma, Platelets, Cryo- Collection Criterion update

18 Topics of proposed changes cont d Lowest ED/Hospital Systolic BP-collection criterion change. Angiography-collection criterion change and definition change. Embolization Site-collection criterion change. Angiography Date/Time-Collection Criterion Change Surgery for Hemorrhage Control Type, Date &Timecollection criterion change.
19

20 TQIP Process Measures (From TQIP Online Course)
21 TQIP Process Measures These are specific steps in a process that lead to either positively or negatively to a particular outcome metric. TBI Hemorrhage Control Venous Thromboembolism Prophylaxis Withdrawal of Care * These Process Measure are collected at Level 1 & 2 Trauma Centers

22 First TQIP Process Measures (Criterion) Collect on all patients with at least one injury in the AIS region of the Head- excluding superficial injuries such as, scalp lacerations, contusion and /or avulsions. Bing.com
23 TQIP Collection Criteria for Head Injury Cont d Highest GCS total within 24 hours of ED/Hospital Arrival to index hospital * Highest Motor GCS with 24 hours of ED/Hospital Arrival GCS Assessment Qualifier Component of Highest GCS total Initial ED/Hospital Pupillary Response *Note this refers to the hospital abstracting the data
 if there is no other contradicting documentation.")
24 Collection Criteria for Head Cont d Midline Shift > 5mm within 24 hours after time of INJURY *Note If the injury time is unknown, but there is supporting documentation that the injury occurred with 24-hours of any CT measuring a > 5 mm shift, report the field value 1 (Yes) if there is no other contradicting documentation. Cerebral Monitor- Indicate all cerebral monitors that were placed Cerebral Monitor Date and Time- The date and time of the first cerebral monitor

25 2 nd TQIP Process Measure Criterion Collect on ALL patients
.")
26 Venous Thromboembolism Prophylaxis Type (VTE) The type of data to be collected here is Medications only. Collect the first dose given. If other forms of prophylaxis is used i.e. SCDs you will capture it as 5 (none).
27 VTE Date/Time Date and Time the prophylaxis is administered at YOUR hospital. If a patient is given the dose after D/C order is written you will not collect the information. You will get a Level 1 Edit.

28 Withdrawal of Life Supporting Treatment Treatment was withdrawn based on a decision to either remove or withhold further life sustaining intervention. Must be documented in the Medical Record Is often, but not always associated with a discussion with the legal guardian or next of kin. They do NOT have to have a DNR in place.
.")
29 Withdrawal Cont d Interventions are: Ventilator support (with or without extubation). Dialysis or other forms of renal support. Medications to support cardiac function or blood pressure. Specific surgical, interventional or radiological procedure (angio, craniectomy, hemorrhage control). This includes withdrawal of intervention in place or a decision not to proceed with a lifesupporting measure such as extubation or intubation.
30 Withdrawal of Life Support Treatment Date/Time Date and time of withdrawal of treatment. If no withdrawal of treatment is placed use the date and time the decision is made not to proceed with life sustaining treatment i.e. intubation.

31 Transfusion Blood (4 Hours) Patients who had blood transfused at YOUR hospital within the first 4 hours of ED/Hospital arrival. If no blood is given then it should be reported as 0 not NA. Make sure to report if CCs OR Units If using CCs then in the conversion field should be NA. Conversion field is used ONLY is submitting if collecting blood in UNITS This is for all BLOOD fields.

32 3 rd TQIP Process Measure Criterion Collect on ALL patients with transfused packed red blood cells within first 4 hours after ED/Hospital arrival.
33 Transfusion Blood Products (4 & 24 Hours) If a patient receives PRBCs within 4 hours of ED/Hospital arrival then you will collect other blood products: PRBC (24 hours) Plasma (4 &24 hours) Platelets (4 & 24 Hours) Cryoprecipitate (4 &24 Hours) ONLY COLLECT these products if patient received PRBC in the first 4 hours You will also collect the blood measurements and blood conversion on these.

34 Lowest ED/Hospital Systolic Blood Pressure Collect on all patients who had PRBCs transfused in the first 4 hours after arrival to ED/Hospital. This is at YOUR hospital not the referring hospital.

35 Angiography Collect on all patients who received PRBCs in the first 4 hours. This is the first interventional angiogram with or without embolization in the first 24 hours of ED/Hospital Arrival. If patient did not have PRBCs in the first 4 hours then fill the field is NA. Exclude CTA
36 Angiography Date/Time The date and time of the first angiogram was performed
 5. Retroperitoneum (lumbar, sacral) 6. Peripheral vascular (neck, extremities) 7. Aorta (thoracic or abdominal) 8.")
37 Embolization Site Collect on all patients with transfused PRBCs in first 4 hours What organ/site had embolization for hemorrhage control: 1. Liver 2. Spleen 3. Kidneys 4. Pelvic(iliac, gluteal, obturator) 5. Retroperitoneum (lumbar, sacral) 6. Peripheral vascular (neck, extremities) 7. Aorta (thoracic or abdominal) 8. Other Note: The null value NA is used it the data field Angiography is 1 NONE or 2 Angiogram only The null value Na is used for patients who do not meet the collection criterion. Use all that apply.

38 Surgery for Hemorrhage Control Type First type of hemorrhage control within 24 hours of hospital arrival. These procedures do not necessarily mean they were done in OR 1. None 2. Laparotomy 3. Thoracotomy 4. Sternotomy 5. Extremity 6. Neck 7. Mangle extremity/traumatic amputation 8. Other skin/soft tissue Note:Procedures can be done in ED such as thoracotomy, but because you think procedure it doesn t mean that they were done in OR only, some can be done in other locations.

39 Surgery Date/Time The date and time the surgery for hemorrhage control was performed.

40 Conclusion Make sure to follow how your institute wants you to collect the data. Refer to the data dictionary for further information. Ask TQIP for further clarification or your Clinical team. If you get further clarification from TQIP share with the group so that we all can be on the same page.
41 References TQIP online Course ViewClass.aspx?ClassID=189&View=Syllabus Initial, Sequela & Subsequent Coding NTDS Data Dictionary HIPAA Cartoons


42 Questions/Discussions
Process Measures Toolkit for 2016 Admissions
 Process Measures Toolkit for 2016 Admissions Collection Criterion #1 Collect on all patients The following data fields should be reported using the listed field value option(s), or relevant value, as indicated
Process Measures Toolkit for 2016 Admissions Collection Criterion #1 Collect on all patients The following data fields should be reported using the listed field value option(s), or relevant value, as indicated
Datapoint Description On Tab On Report Data Element Name Type Values Default
 CUSTOM DATA ELEMENTS FOR 2017 MTQIP TAB Datapoint Description On Tab On Report Data Element Name Type Values Default Intubation status X X MTQIP_INT_STAT Number with pick list 1=Never, 2=Field/Scene/En
CUSTOM DATA ELEMENTS FOR 2017 MTQIP TAB Datapoint Description On Tab On Report Data Element Name Type Values Default Intubation status X X MTQIP_INT_STAT Number with pick list 1=Never, 2=Field/Scene/En
4. Which survey program does your facility use to get your program designated by the state?
 TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
ACUTE KIDNEY INJURY (AKI) ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) ADVANCED DIRECTIVE LIMITING CARE...91 AGE...9 AGE UNITS...
 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) ADVANCED DIRECTIVE LIMITING CARE...91 AGE...9 AGE UNITS...") ACUTE KIDNEY INJURY (AKI)...122 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS)...124 ADVANCED DIRECTIVE LIMITING CARE...91 AGE...9 AGE UNITS...10 AIRBAG DEPLOYMENT...30 AIS PREDOT CODE...118 AIS SEVERITY...119
ACUTE KIDNEY INJURY (AKI)...122 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS)...124 ADVANCED DIRECTIVE LIMITING CARE...91 AGE...9 AGE UNITS...10 AIRBAG DEPLOYMENT...30 AIS PREDOT CODE...118 AIS SEVERITY...119
Datapoint Description On Tab On Report Data Element Name Type Values Default Validation
 Datapoint Description On Tab On Report Data Element Name Type Values Default Validation 1=Never, 2=Field/Scene/ En Route, 3=ED, 4=OR, 5=ICU, 6=Other (Floor, Number with Radiology, Intubation status X X
Datapoint Description On Tab On Report Data Element Name Type Values Default Validation 1=Never, 2=Field/Scene/ En Route, 3=ED, 4=OR, 5=ICU, 6=Other (Floor, Number with Radiology, Intubation status X X
Number with pick list. 5/6/2011 Michigan TQIP
 Datapoint Description On Tab On Report Data Element Name Type Values Default Validation Intubation status X X MTQIP_INT_STAT list 1=Never, 2=Field/Scene/En Route, 3=ED, 4=OR, 5=ICU, 6=Other (Floor, Radiology,
Datapoint Description On Tab On Report Data Element Name Type Values Default Validation Intubation status X X MTQIP_INT_STAT list 1=Never, 2=Field/Scene/En Route, 3=ED, 4=OR, 5=ICU, 6=Other (Floor, Radiology,
Q1 Contact Information
 Q1 Contact Information Answered: 7 Skipped: 0 ANSWER CHOICES Hospital Name of Person Completing Survey Email RESPONSES 100.00% 7 100.00% 7 100.00% 7 # HOSPITAL DATE 1 Saint Luke's Hospital of Kansas City
Q1 Contact Information Answered: 7 Skipped: 0 ANSWER CHOICES Hospital Name of Person Completing Survey Email RESPONSES 100.00% 7 100.00% 7 100.00% 7 # HOSPITAL DATE 1 Saint Luke's Hospital of Kansas City
Who is Using ICD-10-CM?
 Conventions and Guidelines You Need to Know Presented by Brenda Edwards, CPC, CPMA, CPB, CPC-I, CEMC, CRC Who is Using ICD-10-CM? 1 Objectives of Presentation Review new conventions and chapter specific
Conventions and Guidelines You Need to Know Presented by Brenda Edwards, CPC, CPMA, CPB, CPC-I, CEMC, CRC Who is Using ICD-10-CM? 1 Objectives of Presentation Review new conventions and chapter specific
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
2019 Collector Update. Lyndsey Diehl, RHIA, CHDA, CSTR Manager of Trauma Data Quality Stephanie Radzevick, CPC Trauma Data Analyst
 2019 Collector Update Lyndsey Diehl, RHIA, CHDA, CSTR Manager of Trauma Data Quality Stephanie Radzevick, CPC Trauma Data Analyst Stephanie Breakdown 2019 PTOS/Collector Changes 2019 Miscellaneous PTOS/Collector
2019 Collector Update Lyndsey Diehl, RHIA, CHDA, CSTR Manager of Trauma Data Quality Stephanie Radzevick, CPC Trauma Data Analyst Stephanie Breakdown 2019 PTOS/Collector Changes 2019 Miscellaneous PTOS/Collector
ICD 10 CM. What does it mean to YOU? It s all about specificity
 ICD 10 CM What does it mean to YOU? It s all about specificity ICD TIMELINE ICD-9 Published by WHO in 1978 ICD-10 Endorsed by WHO in 1990 ICD-10-CM draft released in 1995 ICD-10 Used for mortality in the
ICD 10 CM What does it mean to YOU? It s all about specificity ICD TIMELINE ICD-9 Published by WHO in 1978 ICD-10 Endorsed by WHO in 1990 ICD-10-CM draft released in 1995 ICD-10 Used for mortality in the
ICD-10 Service Line Overview Musculoskeletal
 ICD-10 Service Line Overview Musculoskeletal ICD-10 incorporates much greater clinical detail and specificity as well as updated terminology to be consistent with current clinical practices. ICD-10-CM
ICD-10 Service Line Overview Musculoskeletal ICD-10 incorporates much greater clinical detail and specificity as well as updated terminology to be consistent with current clinical practices. ICD-10-CM
ICD-10 CM Training. Orthopaedic
 ICD-10 CM Training Orthopaedic ICD-10-CM Compliance Dates ICD-10-CM will be valid for dates of service on or after October 1, 2015 Outpatient dates of service of October 1, 2015 and beyond. Inpatient hospital
ICD-10 CM Training Orthopaedic ICD-10-CM Compliance Dates ICD-10-CM will be valid for dates of service on or after October 1, 2015 Outpatient dates of service of October 1, 2015 and beyond. Inpatient hospital
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
EAST MULTICENTER STUDY DATA DICTIONARY
 EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
M TQIP Data Dictionary
 M TQIP 2019 Data Dictionary Table of Contents PATIENT INCLUSION CRITERIA... 1 CASE NUMBER... 1 TRAUMA CENTER... 2 DEMOGRAPHIC INFORMATION... 2 PATIENT'S HOME ZIP/POSTAL CODE... 2 PATIENT'S HOME COUNTRY...
M TQIP 2019 Data Dictionary Table of Contents PATIENT INCLUSION CRITERIA... 1 CASE NUMBER... 1 TRAUMA CENTER... 2 DEMOGRAPHIC INFORMATION... 2 PATIENT'S HOME ZIP/POSTAL CODE... 2 PATIENT'S HOME COUNTRY...
ICD-10-CM & ICD-10-PCS CODING ROUNDTABLES. Emergency Room Scenarios
 ICD-10-CM & ICD-10-PCS CODING ROUNDTABLES Emergency Room Scenarios THANK YOU TO OUR CODING ROUNDTABLE SPONSOR CHANNEL PUBLISHING! ICD-10-CM: Diagnosis Coding Chapter 19 Injury, poisoning and certain other
ICD-10-CM & ICD-10-PCS CODING ROUNDTABLES Emergency Room Scenarios THANK YOU TO OUR CODING ROUNDTABLE SPONSOR CHANNEL PUBLISHING! ICD-10-CM: Diagnosis Coding Chapter 19 Injury, poisoning and certain other
This way to ICD 10 1
 This way to ICD 10 1 Quick Review We currently report diagnoses with ICD 9 codes Effective with date of service 10 1 14 we must report services using ICD 10 diagnosis codes Many more codes to choose from
This way to ICD 10 1 Quick Review We currently report diagnoses with ICD 9 codes Effective with date of service 10 1 14 we must report services using ICD 10 diagnosis codes Many more codes to choose from
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
ICD 10 CM Coding and Documentation
 ICD 10 CM Coding and Documentation Adult Day Health Care Council Karen L. Fabrizio, RHIA, CHTS CP, CPRA April 10, 2014 Presented by: Karen Fabrizio, RHIA CHTS CP CPRA is an AHIMA Approved ICD 10 CM/PCS
ICD 10 CM Coding and Documentation Adult Day Health Care Council Karen L. Fabrizio, RHIA, CHTS CP, CPRA April 10, 2014 Presented by: Karen Fabrizio, RHIA CHTS CP CPRA is an AHIMA Approved ICD 10 CM/PCS
Institution Subject number. Demographics Age (yrs) Male (0/1) Race (0/1) Hispanic Non-hispanic AA Asian
 Male (0/1) Race (0/1) Hispanic Non-hispanic AA Asian") Institution Subject number Demographics Age (yrs) Male (0/1) Race (0/1) Hispanic Non-hispanic AA Asian Co-morbidities (0/1) Hypertension Coronary artery disease If 1: Coronary stents History of cardiac
Institution Subject number Demographics Age (yrs) Male (0/1) Race (0/1) Hispanic Non-hispanic AA Asian Co-morbidities (0/1) Hypertension Coronary artery disease If 1: Coronary stents History of cardiac
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Clinical Quality Measures for PQRS. Last Updated: June 4, 2014
 Clinical Quality Measures for PQRS Last Updated: June 4, 2014 The Michigan Bariatric Surgery Collaborative (MBSC) Quality Clinical Data Registry will submit the following measures outlined below on behalf
Clinical Quality Measures for PQRS Last Updated: June 4, 2014 The Michigan Bariatric Surgery Collaborative (MBSC) Quality Clinical Data Registry will submit the following measures outlined below on behalf
M TQIP Data Dictionary
 M TQIP 2018 Data Dictionary Table of Contents PATIENT INCLUSION CRITERIA... 1 CASE NUMBER... 1 TRAUMA CENTER... 2 DEMOGRAPHIC INFORMATION... 2 PATIENT'S HOME ZIP/POSTAL CODE... 2 PATIENT'S HOME COUNTRY...
M TQIP 2018 Data Dictionary Table of Contents PATIENT INCLUSION CRITERIA... 1 CASE NUMBER... 1 TRAUMA CENTER... 2 DEMOGRAPHIC INFORMATION... 2 PATIENT'S HOME ZIP/POSTAL CODE... 2 PATIENT'S HOME COUNTRY...
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #358: Patient-Centered Surgical Risk Assessment and Communication National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #358: Patient-Centered Surgical Risk Assessment and Communication National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL MEASURES:
The Michigan Trauma Quality Improvement Program. Ann Arbor, MI June 7, 2011
 The Michigan Trauma Quality Improvement Program Ann Arbor, MI June 7, 2011 Information Current centers 14 New centers (July 1) Botsford Covenant Spectrum St. Johns Future centers (January 1) 23 Total Information
The Michigan Trauma Quality Improvement Program Ann Arbor, MI June 7, 2011 Information Current centers 14 New centers (July 1) Botsford Covenant Spectrum St. Johns Future centers (January 1) 23 Total Information
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury
 TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
"ICD-10 For Clinical Staff" February 21, 2014 by Paula Digby, CPC, CCS, CPCI, AHIMA Approved ICD-10-CM/PCS Instructor. Disclaimer
 Slide 1 1 Slide 2 Disclaimer The information contained in this presentation is provided to assist the attendee in understanding the reimbursement process. It is intended to assist healthcare providers
Slide 1 1 Slide 2 Disclaimer The information contained in this presentation is provided to assist the attendee in understanding the reimbursement process. It is intended to assist healthcare providers
9/1/2015. Studies (AHIMA)
") 9/1/2015 IC CD 10 Coding Supplemental Case Studies Amy Franklin, RN, RAC MT, ICD 10 CM/PCS Trainer (AHIMA) 1. DM Case Study 62 y.o. Mr. X has DM with insulin in use, DM Neuropathy and DM Renal insufficiency.
9/1/2015 IC CD 10 Coding Supplemental Case Studies Amy Franklin, RN, RAC MT, ICD 10 CM/PCS Trainer (AHIMA) 1. DM Case Study 62 y.o. Mr. X has DM with insulin in use, DM Neuropathy and DM Renal insufficiency.
Appropriate Use of 7 th Character in ICD 10 CM
 Appropriate Use of 7 th Character in ICD 10 CM Jameel Ahmed RHIA,CCS Corporate, Group HIM Manager SEHA - Abu Dhabi Health Services Co SEHA: Abu Dhabi Healthservices 18,000 Employees 12 Hospitals 57 Ambulatory
Appropriate Use of 7 th Character in ICD 10 CM Jameel Ahmed RHIA,CCS Corporate, Group HIM Manager SEHA - Abu Dhabi Health Services Co SEHA: Abu Dhabi Healthservices 18,000 Employees 12 Hospitals 57 Ambulatory
ICD-10 Physician Education. Palliative Care SIP
 ICD-10 Physician Education Palliative Care SIP 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
ICD-10 Physician Education Palliative Care SIP 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
More of Chapter 19 ICD 10 CM Injuries 7 th Characters, Aftercare, Follow up and Sequelae. Wednesday, December 2, :00 pm CST
 More of Chapter 19 ICD 10 CM Injuries 7 th Characters, Aftercare, Follow up and Sequelae Wednesday, December 2, 2015 12:00 pm CST 1 Disclaimer This audio conference is designed to provide accurate and
More of Chapter 19 ICD 10 CM Injuries 7 th Characters, Aftercare, Follow up and Sequelae Wednesday, December 2, 2015 12:00 pm CST 1 Disclaimer This audio conference is designed to provide accurate and
VENOUS THROMBOEMBOLISM (VTE) PREVENTION MEDICAL PROVIDER EDUCATION JUNE 2017
 PREVENTION MEDICAL PROVIDER EDUCATION JUNE 2017") VENOUS THROMBOEMBOLISM (VTE) PREVENTION MEDICAL PROVIDER EDUCATION JUNE 2017 VTE IS THE 2 ND MOST COMMON HOSPITAL ACQUIRED CONDITION RISK FACTORS DECREASED ACTIVITY = VTE RISK (NURSES MEASURE WITH BRADEN
VENOUS THROMBOEMBOLISM (VTE) PREVENTION MEDICAL PROVIDER EDUCATION JUNE 2017 VTE IS THE 2 ND MOST COMMON HOSPITAL ACQUIRED CONDITION RISK FACTORS DECREASED ACTIVITY = VTE RISK (NURSES MEASURE WITH BRADEN
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Registry Documentation December 16, 2014
 Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Presented at 2015 TQIP conference. Developed by a panel of experts. Evidence based with expert opinion as needed
 Presented at 2015 TQIP conference Developed by a panel of experts Evidence based with expert opinion as needed Orthopaedic Trauma Best Practice Guidelines (BPG) Goals Offer guidance on what is practical
Presented at 2015 TQIP conference Developed by a panel of experts Evidence based with expert opinion as needed Orthopaedic Trauma Best Practice Guidelines (BPG) Goals Offer guidance on what is practical
Initial Management of Pelvic Injuries
 Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
APR-DRG and the Trauma Registry. Jodi Hackworth, MPH Johanna Askegard-Giesmann, MD Thomas Rouse, MD Brian Benneyworth, MD, MS
 APR-DRG and the Trauma Registry Jodi Hackworth, MPH Johanna Askegard-Giesmann, MD Thomas Rouse, MD Brian Benneyworth, MD, MS November 2015 Conflict of Interests Disclosures Jodi Hackworth and her co-authors
APR-DRG and the Trauma Registry Jodi Hackworth, MPH Johanna Askegard-Giesmann, MD Thomas Rouse, MD Brian Benneyworth, MD, MS November 2015 Conflict of Interests Disclosures Jodi Hackworth and her co-authors
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
EMS System for Metropolitan Oklahoma City and Tulsa 2018 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
CEU Final Exam for Code It! Sixth Edition
 CEU Final Exam for 3-2-1 Code It! Sixth Edition Note to CEU applicant In order to receive CEU credit for taking this exam, the following criteria must be met: You must be certified by AAPC prior to purchasing
CEU Final Exam for 3-2-1 Code It! Sixth Edition Note to CEU applicant In order to receive CEU credit for taking this exam, the following criteria must be met: You must be certified by AAPC prior to purchasing
ICD-10-CM Coding and Documentation for Long Term Care
 ICD-10-CM Coding and Documentation for Long Term Care June 3, 2014 Chris Hoskins, MA, RHIA, CTR, CHC Karen Fabrizio, RHIA CHTS-CP AHIMA Approved ICD-10-CM/PCS Trainers Objectives Review 2014 Coding Guidelines
ICD-10-CM Coding and Documentation for Long Term Care June 3, 2014 Chris Hoskins, MA, RHIA, CTR, CHC Karen Fabrizio, RHIA CHTS-CP AHIMA Approved ICD-10-CM/PCS Trainers Objectives Review 2014 Coding Guidelines
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Get With the Guidelines Stroke PMT. Quality Measure Descriptions
 Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
ICD-10 for Beginners Four-Part Series
 ICD-10 for Beginners Four-Part Series www.jluhealth.com 1 ICD-10-CM: Introduction to Coding Fundamentals PRESENTER: Joan L. Usher, BS, RHIA, ACE AHIMA Approved ICD-10-CM Trainer JLU HEALTH RECORD SYSTEMS
ICD-10 for Beginners Four-Part Series www.jluhealth.com 1 ICD-10-CM: Introduction to Coding Fundamentals PRESENTER: Joan L. Usher, BS, RHIA, ACE AHIMA Approved ICD-10-CM Trainer JLU HEALTH RECORD SYSTEMS
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
A Comparative Analysisof Male versus Female Breast Cancer in the ACS NSQIP Database
 A Comparative Analysisof Male versus Female Breast Cancer in the ACS NSQIP Database Lindsay Petersen, MD Rush University Medical Center Chicago, IL I would like to recognize my coauthors: Andrea Madrigrano,
A Comparative Analysisof Male versus Female Breast Cancer in the ACS NSQIP Database Lindsay Petersen, MD Rush University Medical Center Chicago, IL I would like to recognize my coauthors: Andrea Madrigrano,
EAST MULTICENTER STUDY DATA COLLECTION TOOL
 EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Effect of Regional Anesthesia on Delirium in Geriatric Trauma Patients with Multiple Rib Fractures Enrolling Center: Enrolling Co-investigators:
EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Effect of Regional Anesthesia on Delirium in Geriatric Trauma Patients with Multiple Rib Fractures Enrolling Center: Enrolling Co-investigators:
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Documentation Tips for Pulmonary/Critical Care
 Documentation Tips for Pulmonary/Critical Care ICD-10 classifications: The HARD WAY! J44 Other chronic obstructive pulmonary disease Includes: asthma with chronic obstructive pulmonary disease chronic
Documentation Tips for Pulmonary/Critical Care ICD-10 classifications: The HARD WAY! J44 Other chronic obstructive pulmonary disease Includes: asthma with chronic obstructive pulmonary disease chronic
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
ESCOME Pre-Course Outline (v1.09)
") ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
PATIENT: DOB: TODAY S DATE:
 1. I have been strongly advised to carefully read and consider this operative permit. I realize that it is important that I understand this material. I also understand that if certain sections are not
1. I have been strongly advised to carefully read and consider this operative permit. I realize that it is important that I understand this material. I also understand that if certain sections are not
Assessment and Scoring Tools
 Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition)
") 2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
NTDS DATA & TACR DICTIONARY COMPARISON. CO-MORBID CONDITIONS Lita Holdeman, BS, CSTR, Education Chair, AOTR Education Committee
 NTDS DATA & TACR DICTIONARY COMPARISON CO-MORBID CONDITIONS Lita Holdeman, BS, CSTR, Education Chair, AOTR Education Committee Co-Morbid Conditions(Risks) Co-morbid conditions are pre-existing health factors
NTDS DATA & TACR DICTIONARY COMPARISON CO-MORBID CONDITIONS Lita Holdeman, BS, CSTR, Education Chair, AOTR Education Committee Co-Morbid Conditions(Risks) Co-morbid conditions are pre-existing health factors
Institutional Priorities and the Impact on Mortality Rates
 Institutional Priorities and the Impact on Mortality Rates John M. McGregor, MD Ciarán Powers, MD, PhD Associate Professor, Clinical Neurosurgery Associate Professor, Neurological Surgery Co-Chair Neurosciences
Institutional Priorities and the Impact on Mortality Rates John M. McGregor, MD Ciarán Powers, MD, PhD Associate Professor, Clinical Neurosurgery Associate Professor, Neurological Surgery Co-Chair Neurosciences
FY 2017 ICD-10-CM Guideline Updates. Melanie Endicott, MBA/HCM, RHIA, CHDA, CDIP, CCS, CCS-P, FAHIMA, AHIMA-Approved ICD-10-CM/PCS Trainer
 FY 2017 ICD-10-CM Guideline Updates Melanie Endicott, MBA/HCM, RHIA, CHDA, CDIP, CCS, CCS-P, FAHIMA, AHIMA-Approved ICD-10-CM/PCS Trainer How to Review Guideline Changes 1. Download the FY 2017 ICD-10-CM
FY 2017 ICD-10-CM Guideline Updates Melanie Endicott, MBA/HCM, RHIA, CHDA, CDIP, CCS, CCS-P, FAHIMA, AHIMA-Approved ICD-10-CM/PCS Trainer How to Review Guideline Changes 1. Download the FY 2017 ICD-10-CM
ECLS Registry Form Extracorporeal Life Support Organization (ELSO)
") ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
IMPLEMENTING THE EXTERNAL CAUSE MATRIX FOR INJURY MORBIDITY NORTH CAROLINA EMERGENCY DEPARTMENT DATA JANUARY 2015 MAY 2015/JANUARY 2016 MAY 2016
 IMPLEMENTING THE EXTERNAL CAUSE MATRIX FOR INJURY MORBIDITY NORTH CAROLINA EMERGENCY DEPARTMENT DATA JANUARY 2015 MAY 2015/JANUARY 2016 MAY 2016 A Report on the Transition to ICD-10-CM Prepared by Katherine
IMPLEMENTING THE EXTERNAL CAUSE MATRIX FOR INJURY MORBIDITY NORTH CAROLINA EMERGENCY DEPARTMENT DATA JANUARY 2015 MAY 2015/JANUARY 2016 MAY 2016 A Report on the Transition to ICD-10-CM Prepared by Katherine
Trauma Workshop! Skills Centre, St George Hospital! Saturday 15 March 2014!
 Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Trauma Registry Training. Exercises. Dee Vernberg Dan Robinson Digital Innovation (800) ex 4.
 ex 4.") Trauma Registry Training Exercises Dee Vernberg 785-296-0613 Dan Robinson 785-296-3180 Digital Innovation (800) 344-3668 ex 4 www.kstrauma.org For a copy of the Data Dictionary, please follow the below
Trauma Registry Training Exercises Dee Vernberg 785-296-0613 Dan Robinson 785-296-3180 Digital Innovation (800) 344-3668 ex 4 www.kstrauma.org For a copy of the Data Dictionary, please follow the below
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/30/2012 Radiology Quiz of the Week # 79 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/30/2012 Radiology Quiz of the Week # 79 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
PIPS Committee Meeting Clinical Congress October 2017
 PIPS Committee Meeting Clinical Congress October 2017 Don Jenkins, MD, FACS Performance Improvement and Patient Safety Committee Chair Agenda Work Group Updates Optimal PI Plan/Chapter 16 Best Practice
PIPS Committee Meeting Clinical Congress October 2017 Don Jenkins, MD, FACS Performance Improvement and Patient Safety Committee Chair Agenda Work Group Updates Optimal PI Plan/Chapter 16 Best Practice
SAMPLE Data Entry Manual for the veds Project
 The data entry manual is designed to provide a clear definition for each variable collected and the options for each variable SAMPLE Data Entry Manual for the veds Project Subject ID Each study participant
The data entry manual is designed to provide a clear definition for each variable collected and the options for each variable SAMPLE Data Entry Manual for the veds Project Subject ID Each study participant
Proprietary Acute Care Indicators
 Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1).
.") PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PEDIATRIC PENETRATING TRAUMA. Laura Boomer 11/18/15
 PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
Where Are You on the ICD-10-CM Radar Screen? Presented to the Indiana Medical Group Management Association
 Where Are You on the ICD-10-CM Radar Screen? Presented to the Indiana Medical Group Management Association ICD-10 Final Rule On January 16, 2009, the U.S. Department of Health and Human Services (HHS)
Where Are You on the ICD-10-CM Radar Screen? Presented to the Indiana Medical Group Management Association ICD-10 Final Rule On January 16, 2009, the U.S. Department of Health and Human Services (HHS)
The determination of eligible population for this measure requires administrative claims data.
 Overuse of Imaging Measure 6: Ratio of Magnetic Resonance Imaging Scans to Computed Tomography Scans for the Evaluation of Children with Atraumatic Headache Description This measure assesses the ratio
Overuse of Imaging Measure 6: Ratio of Magnetic Resonance Imaging Scans to Computed Tomography Scans for the Evaluation of Children with Atraumatic Headache Description This measure assesses the ratio
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations
 50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
Rules of Engagement: Adapting to Change
 Rules of Engagement: Adapting to Change Stephanie Johnson, CCS Coding Supervisor, Education, Training, and Consultation Uniform Data System for Medical Rehabilitation Carol Harper, COTA/L Manager, Education,
Rules of Engagement: Adapting to Change Stephanie Johnson, CCS Coding Supervisor, Education, Training, and Consultation Uniform Data System for Medical Rehabilitation Carol Harper, COTA/L Manager, Education,
9/18/16. Setting: Community ED, 30k admissions per year Time: Friday night, 11pm. CC: Syncope
 William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Caution!!! Copyright 2014, Lynn Thornton My Coding Coach, All Rights Reserved 2
 My Coding Coach Caution!!! You are entering the knowledge portal. Only proceed if you are prepared to expand your clinical knowledge and grasp of complex scenarios. No coding books are required for the
My Coding Coach Caution!!! You are entering the knowledge portal. Only proceed if you are prepared to expand your clinical knowledge and grasp of complex scenarios. No coding books are required for the
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Data Collection Tool. Standard Study Questions: Admission Date: Admission Time: Age: Gender:
 Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD
 HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
Appendix. Potentially Preventable Complications (PPCs) identify. complications that can occur during an admission. There are 64
 identify. complications that can occur during an admission. There are 64") Calikoglu S, Murray R, Feeney D. Hospital pay-for-performance programs in Maryland produced strong results, including reduced hospital-acquired infections. Health Aff (Millwood). 2012;31(12). Appendix
Calikoglu S, Murray R, Feeney D. Hospital pay-for-performance programs in Maryland produced strong results, including reduced hospital-acquired infections. Health Aff (Millwood). 2012;31(12). Appendix
ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP: #204. Ischemic Vascular Disease (IVD):
ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP: #204. Ischemic Vascular Disease (IVD):
Injury, poisoning and certain other consequences of external causes (S00-T88)
") Injury, poisoning and certain other consequences of external causes (S00-T88) Presented by Andy Bhatia, DPM Webinar 6: Thursday, April 17, 2014 1 APMA Educational Information: ICD-10 Webinars Register
Injury, poisoning and certain other consequences of external causes (S00-T88) Presented by Andy Bhatia, DPM Webinar 6: Thursday, April 17, 2014 1 APMA Educational Information: ICD-10 Webinars Register
LIMB COMPRESSION DEVICES FOR VENOUS THROMBOEMBOLISM PROPHYLAXIS
 PROPHYLAXIS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are dependent
PROPHYLAXIS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are dependent
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
ISPUB.COM. Rare Cases: Tracheal/bronchial Obstruction. O Wenker, L Moehn, C Portera, G Walsh HISTORY ADMISSION
 ISPUB.COM The Internet Journal of Radiology Volume 1 Number 1 O Wenker, L Moehn, C Portera, G Walsh Citation O Wenker, L Moehn, C Portera, G Walsh.. The Internet Journal of Radiology. 1999 Volume 1 Number
ISPUB.COM The Internet Journal of Radiology Volume 1 Number 1 O Wenker, L Moehn, C Portera, G Walsh Citation O Wenker, L Moehn, C Portera, G Walsh.. The Internet Journal of Radiology. 1999 Volume 1 Number
What You Need To Know Now. Background
 What You Need To Know Now ICD 10 Background You have heard the news. Right? 5010 is January 1, 2012 ICD 10 CM/PCS is October 1, 2013 CM for outpatient PCS for inpatient 1 It s not all about us Code Sets
What You Need To Know Now ICD 10 Background You have heard the news. Right? 5010 is January 1, 2012 ICD 10 CM/PCS is October 1, 2013 CM for outpatient PCS for inpatient 1 It s not all about us Code Sets
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Contents. Version 1.0: 01/02/2010 Protocol# ISRCTN Page 1 of 7
 Contents 1. INTRODUCTION... 2 2. STUDY SYNOPSIS... 2 3. STUDY OBJECTIVES... 2 3.1. Primary Objective... 2 3.2. Secondary Objectives... 2 3.3. Assessment of Objectives... 3 3.4. Change the Primary Objective
Contents 1. INTRODUCTION... 2 2. STUDY SYNOPSIS... 2 3. STUDY OBJECTIVES... 2 3.1. Primary Objective... 2 3.2. Secondary Objectives... 2 3.3. Assessment of Objectives... 3 3.4. Change the Primary Objective
Orthopedic Admission Hip Fracture Version 2 1/25/2017
 Patient Name: Initial each page and Sign/Date/Time last page Diagnosis: Allergies with reaction type: Orthopedic Admission Hip Fracture Version 2 1/25/2017 Patient Placement Patient Status If the physician
Patient Name: Initial each page and Sign/Date/Time last page Diagnosis: Allergies with reaction type: Orthopedic Admission Hip Fracture Version 2 1/25/2017 Patient Placement Patient Status If the physician