A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
|
|
|
- Blanche Singleton
- 6 years ago
- Views:
Transcription
1 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital

2 H&P 10 year old female presents as a trauma alert after being transferred via helicopter from an Level II adult trauma center s/p motor vehicle collision. She was the restrained rear seat passenger with a lap belt. On presentation was lethargic and complaining of severe abdominal pain. No LOC. Prior to arrival the patient had Foley placed at which revealed hematuria. She also received 1U prbc at the outside hospital for splenic injury and liver injury on outside CT scan.

3
4 Physical Exam VS: 97.5, HR 173, BP 78/50, RR 40, 95% RA Airway: patent Breathing: clear bilaterally Circulation: distal pulses intact Disability: GCS14 (3/5/6) Adjuncts: FAST: positive in all 4 quadrants CXR: negative PE: lethargic, abdominal seatbelt sign CT Head/Cspine: negative

5 Pediatric Vital Signs
6 Pediatric Glasgow Coma Score (GCS)

7 CT Chest Pericardial effusion Right middle lobe/right lower lobe contusion Right 11 th rib fracture
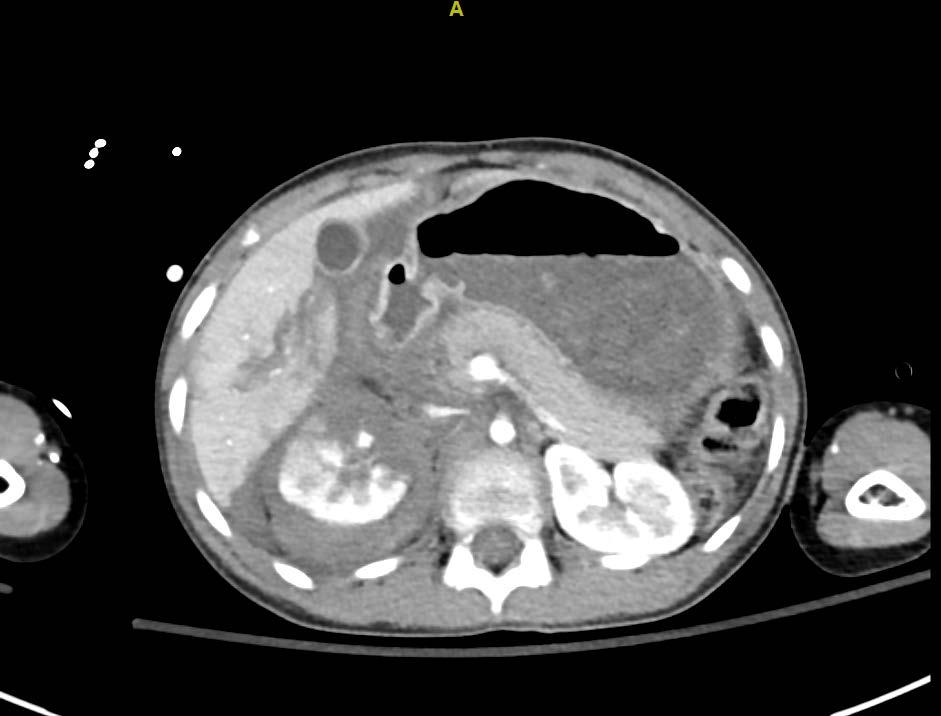
8 CT Abdomen/Pelvis
9 CT Abdomen/Pelvis Grade V liver injury Multiple lacerations to the right kidney with likely vascular compromise and possible renal vein laceration Partial tears of the spleen Decreased attenuation in uncinate process questionable for pancreatic injury Free air Jejunal hematoma Large amount of hemorrhagic ascites

10 Operative Findings Patient taken immediately to the operating room Exploratory laparotomy Trauma and pediatric surgery
11 Operative Findings Findings: Active bleeding from Grade 4 liver laceration Active bleeding from Grade 3 splenic laceration 1cm laceration to the first portion of the duodenum Serosal injury to 1 st and 2 nd portion of the duodenum Nonexpanding right Zone 2 retroperitoneal hematoma
12 What Would You Do Procedure: Exploratory laparotomy Packing of liver hemorrhage Splenectomy Primary repair of 1 st portion of duodenum. Repair of deserosalization injury to 1 st and 2 nd portion of the duodenum Pyloric exclusion Placement of Abthera vac
13 Post-Op Day 0 Patient intubated and taken to Pediatric ICU Pediatric Critical Care Service consulted for co-management Transfused 1 unit FFP Started on Zosyn

14 Post-op Day 1 Return to OR with pediatric surgery and hepatobiliary Reopening of recent laparotomy Removal of packs Gastrojejunostomy Intraoperative cholangiogram Exploration of common bile duct Gastropexy Placement of 10 Fr T-tube

15 Pyloric Exclusion Duodenal Repair Gastrojejunostomy
16 Post-Op Day 2-3 Patient extubated to nasal cannula Child life consulted Patient would benefit from therapeutic pet visitation, caring clown visit, music therapy, and art therapy

17 Post-Op Day 4 R Femoral line removed PICC line placed TPN started Echo: Normal appearing anatomy. No effusion CT Urogram Fractured right kidney with extravasation of excreted urinary contrast into large right perinephric collection without visualization of the right ureter or evidence of vascular extravasation
18 Post-Op Day 5 Transferred to Pediatric Stepdown Unit NG-tube removed Care transitioned from Pediatric Critical Care Team to General Pediatrics Zosyn stopped
19 Post-Op Day 6-7 Foley and JP drains removed Pediatric infectious disease consulted for vaccination timing recommendations and need for prophylactic antibiotics Two weeks after her splenectomy give a dose of PCV-13 and HIB vaccines Four weeks after her PCV-13 and HIB, give a dose of conjugate Meningococcal vaccine Four weeks after receiving the conjugate Meningococcal vaccine, give pneumovax 4 weeks after pneumovax, give Meningococcal B vaccination Penicillin 250 mg BID prophylaxis

20 Post-Op Day 8-10 Regular diet started TPN stopped T-tube clamped after study showed anterograde flow Renal ultrasound: Healing renal laceration, small residual hematoma, uroma

21 Multidisciplinary Approach Trauma surgery Pediatric surgery Pediatric critical care General pediatrics Subspecialists that provide pediatric care Nursing Social work Child life
22 There is a golden hour between life and death. If you are critically injured you have less than 60 minutes to survive. You might not die right then; it may be three days or two weeks later but something has happened in your body that is irreparable. -R Adams Cowley (1975)

23 Acknowledgments

24 Questions?
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
10/27/2014. An experience that causes physical, emotional, or psychological distress or harm.
 Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
JUNCTIONAL STAB WOUND SAVING THE UN-SAVABLE
 JUNCTIONAL STAB WOUND SAVING THE UN-SAVABLE MARVIN WAYNE, MD, FACEP, FAAEM, FAHA ASSOCIATE CLINICAL PROF. DEPT. OF EM, UNIVERISTY OF WASHINGTON EMS MEDICAL DIRECTOR WHATCOM COUNTY WA EMERGENCY DEPT. PEACEHEALTH
JUNCTIONAL STAB WOUND SAVING THE UN-SAVABLE MARVIN WAYNE, MD, FACEP, FAAEM, FAHA ASSOCIATE CLINICAL PROF. DEPT. OF EM, UNIVERISTY OF WASHINGTON EMS MEDICAL DIRECTOR WHATCOM COUNTY WA EMERGENCY DEPT. PEACEHEALTH
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center
 ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center Disclosures Speaking Consultant with Prytime Medical Outline Mechanism
ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center Disclosures Speaking Consultant with Prytime Medical Outline Mechanism
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application
 Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury
 TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
PEDIATRIC PENETRATING TRAUMA. Laura Boomer 11/18/15
 PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY
 NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
Pediatric Trauma. July 27 th, Suzana Buac, PGY4. Dr. Neil Merritt
 Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Cases from the Streets. Kelly Buchanan MD, ATC/L EMS Fellow December, 2011
 Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
CLINICAL MANAGEMENT GUIDELINE PAGE 1 NO REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12
 CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Trauma Workshop! Skills Centre, St George Hospital! Saturday 15 March 2014!
 Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Pediatric Trauma. Sept 2nd, Patrick Murphy Neil Merritt
 Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Uroradiology For Medical Students
 Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital
 Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Question 2. What percentage of abdominal trauma involve the kidney? a) 5 % b) 10% c) 15 % d) 20 %
 5 % b) 10% c) 15 % d) 20 %") Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
History Data Panel. Case 030 Preg Trauma. Presenting Complaint Altered mental status s/p MVC. Person Giving Information EMS
 History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die
 account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Exam. On call that evening
 On call that evening 27 y/o M, law student, GSW R. chest x 2 Breathing comfortably, phonating BP 118/p, 83, 22, GCS=15 A&A&O one GSW, R. axilla one GSW, R. lateral chest, ~ 3 rd intersp. One bullet palpable,
On call that evening 27 y/o M, law student, GSW R. chest x 2 Breathing comfortably, phonating BP 118/p, 83, 22, GCS=15 A&A&O one GSW, R. axilla one GSW, R. lateral chest, ~ 3 rd intersp. One bullet palpable,
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology
 Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD
 Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
17. Imaging and interventional radiology
 17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Pediatric Solid Organ Injuries: Waiting/Watching and Beyond
 Pediatric Solid Organ Injuries: Waiting/Watching and Beyond Ellen Reynolds, MSN, CRNP, CPNP AC/PC PNP, Trauma Clinical Services Children s Hospital of Pittsburgh of UPMC ABDOMINAL INJURIES The Cutting
Pediatric Solid Organ Injuries: Waiting/Watching and Beyond Ellen Reynolds, MSN, CRNP, CPNP AC/PC PNP, Trauma Clinical Services Children s Hospital of Pittsburgh of UPMC ABDOMINAL INJURIES The Cutting
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
Data Collection Tool. Standard Study Questions: Admission Date: Admission Time: Age: Gender:
 Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Discussion of Complex Clinical Scenarios and Variable Review ACS NSQIP Clinical Support Team
 Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Normal Recovery or Complication: The Risks of Post-Operative Care
 Normal Recovery or Complication: The Risks of Post-Operative Care Darrell Ranum, JD, CPHRM Vice President Patient Safety and Risk Management Department Ohio Hospital Association Convention June 14, 2016
Normal Recovery or Complication: The Risks of Post-Operative Care Darrell Ranum, JD, CPHRM Vice President Patient Safety and Risk Management Department Ohio Hospital Association Convention June 14, 2016
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015
![Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015](/thumbs/83/87309292.jpg "Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015") Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Geriatric Trauma Care Pre-Conference Society of Trauma Nurses
 Geriatric Trauma Care Pre-Conference Society of Trauma Nurses March 21, 2018 1 2 About My Center 1. North Shore University Hospital-Northwell Health: A quaternary care facility located in Manhasset New
Geriatric Trauma Care Pre-Conference Society of Trauma Nurses March 21, 2018 1 2 About My Center 1. North Shore University Hospital-Northwell Health: A quaternary care facility located in Manhasset New
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Trauma Activation 7/18/17
 Blunt Rupture of the Thoracic Duct after Severe Thoracic Trauma Samuel Brown, MD Trauma Activation 7/18/17 53 year old male, rear end MVC, exited vehicle and was struck by a semi truck. Denies LOC, complaints
Blunt Rupture of the Thoracic Duct after Severe Thoracic Trauma Samuel Brown, MD Trauma Activation 7/18/17 53 year old male, rear end MVC, exited vehicle and was struck by a semi truck. Denies LOC, complaints
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
Date of Admission: [DATE]. Date of Discharge:
![Date of Admission: [DATE]. Date of Discharge:](/thumbs/74/71277118.jpg "Date of Admission: [DATE]. Date of Discharge:") Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Laparotomy for Abdominal Injury in Traffic Accidents
 Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Child as a victim of injury. Maciej Dudkiewicz M.D. Ph.D. Dpt of Anaesthesia and Intensive Care Medical University of Lodz
 Child as a victim of injury Maciej Dudkiewicz M.D. Ph.D. Dpt of Anaesthesia and Intensive Care Medical University of Lodz Epidemiology Trauma is most common cause of mortality and morbidity in the US pediatric
Child as a victim of injury Maciej Dudkiewicz M.D. Ph.D. Dpt of Anaesthesia and Intensive Care Medical University of Lodz Epidemiology Trauma is most common cause of mortality and morbidity in the US pediatric
Evaluation of Children with Blunt Abdominal Trauma. James F. Holmes, MD, MPH UC Davis School of Medicine
 Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
A regional perspective, to improve patient outcomes. Mr Peter F. Burke. Senior Consultant General Surgeon: LRH
 A regional perspective, to improve patient outcomes. Mr Peter F. Burke. Senior Consultant General Surgeon: LRH What is its role? *VASM involves the clinical review of all cases, where patients have died
A regional perspective, to improve patient outcomes. Mr Peter F. Burke. Senior Consultant General Surgeon: LRH What is its role? *VASM involves the clinical review of all cases, where patients have died
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma
: Penetrating Cardiac Trauma") Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY
 SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Liver lacerations in abdominal trauma management based on anatomical knowledge: A Case report
 American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
UPDATES, 2018 NTDS PILOT (PROPOSED CHANGES TO 2020 NTDB DATA DICTIONARY) AND TQIP PROCESS MEASURES. Lita Holdeman, BS, CSTR AOTR Education Chair
 AND TQIP PROCESS MEASURES. Lita Holdeman, BS, CSTR AOTR Education Chair") UPDATES, 2018 NTDS PILOT (PROPOSED CHANGES TO 2020 NTDB DATA DICTIONARY) AND TQIP PROCESS MEASURES Lita Holdeman, BS, CSTR AOTR Education Chair Disclaimer Notice: All information provide to you at any
UPDATES, 2018 NTDS PILOT (PROPOSED CHANGES TO 2020 NTDB DATA DICTIONARY) AND TQIP PROCESS MEASURES Lita Holdeman, BS, CSTR AOTR Education Chair Disclaimer Notice: All information provide to you at any
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Frostbite. Jessica Cardona PGY1 Jackson Memorial Hospital Pediatrics Department
 Frostbite Jessica Cardona PGY1 Jackson Memorial Hospital Pediatrics Department Question 1 An 8 year old male is brought in by EMS from an icy mountain. He was with his family skiing but was separated from
Frostbite Jessica Cardona PGY1 Jackson Memorial Hospital Pediatrics Department Question 1 An 8 year old male is brought in by EMS from an icy mountain. He was with his family skiing but was separated from
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT
 The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)