TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury
|
|
|
- Juliana Owens
- 5 years ago
- Views:
Transcription
1 TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley Shock Trauma Center Division of Vascular Surgery, University of Maryland School of Medicine


2 Blunt Thoracic Aortic Injury: 2 nd leading cause of death Majority - MVC Rapid deceleration

3 Deceleration Mobile Fixed
4 Diagnosis H&P - Mechanism CXR Hematoma Anomalies Equivocal CT Angiogram IVUS / Angiogram
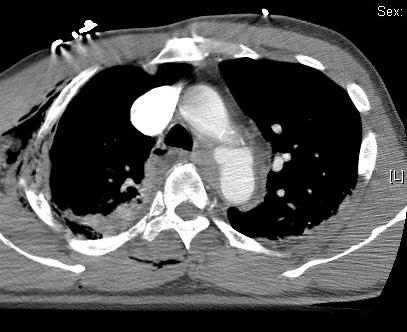

5 CT Scan

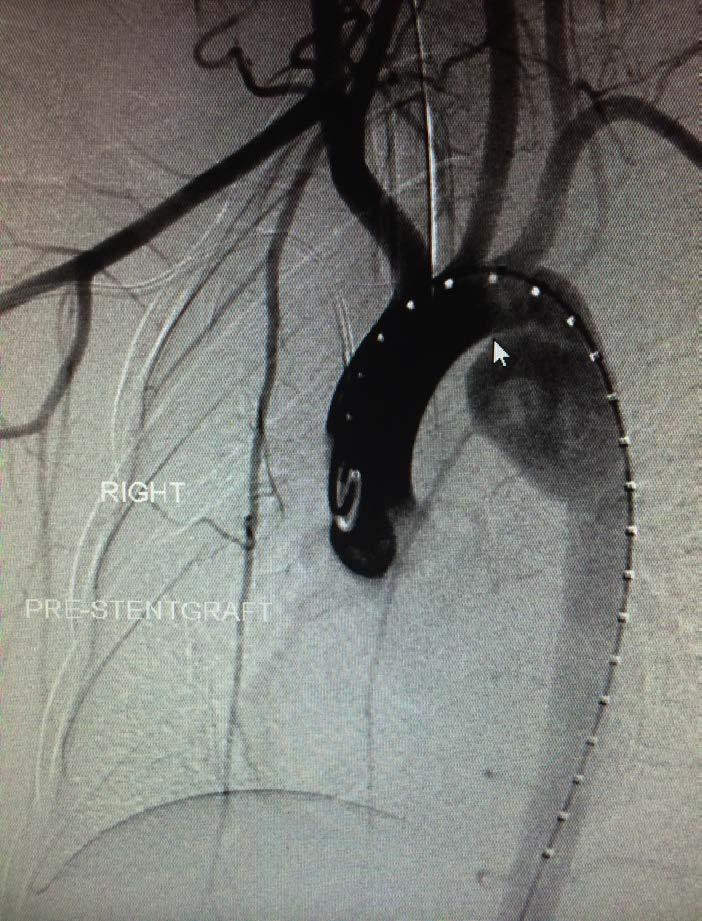
6 Aortogram

7 IVUS No contrast No radiation Real time accurate measurement Morphology (plaque, thrombus, ca++)

8 The Utility of Intravascular Ultrasound Compared to Angiography in the Diagnosis of Blunt Traumatic Aortic Injury A Azizzadeh, J Valdes, CC Miller, LL Nguyen, AL Estrera, K Charlton-Ouw, SM Coogan, JB Holcomb, and HJ Safi CTA widely used as screening for BTAI After equivocal CTA, additional imaging required IVUS more sensitive than angiogram JVS March 2011


9 AAST I and II Demetriades et al
10 AAST I & AAST II Transition in diagnosis Angiogram / echocardiogram >>> CTA Improved outcomes with transition to TEVAR Mortality decreased from 22.0% to 13.0% Paraplegia decreased from 8.7% to 1.6% Delayed repair > Immediate repair


11 AAST I & II Studies Prospective, Multicenter Study N = 193 pts TEVAR - related complications = 20%

12 TEVAR the whole answer for BTAI? Need a common nomenclature to guide: Type of treatment provided Timing of intervention Must work across a spectrum of injuries

13 IV Thoracic aorta, descending

14 Layers of the aortic wall
15 2011


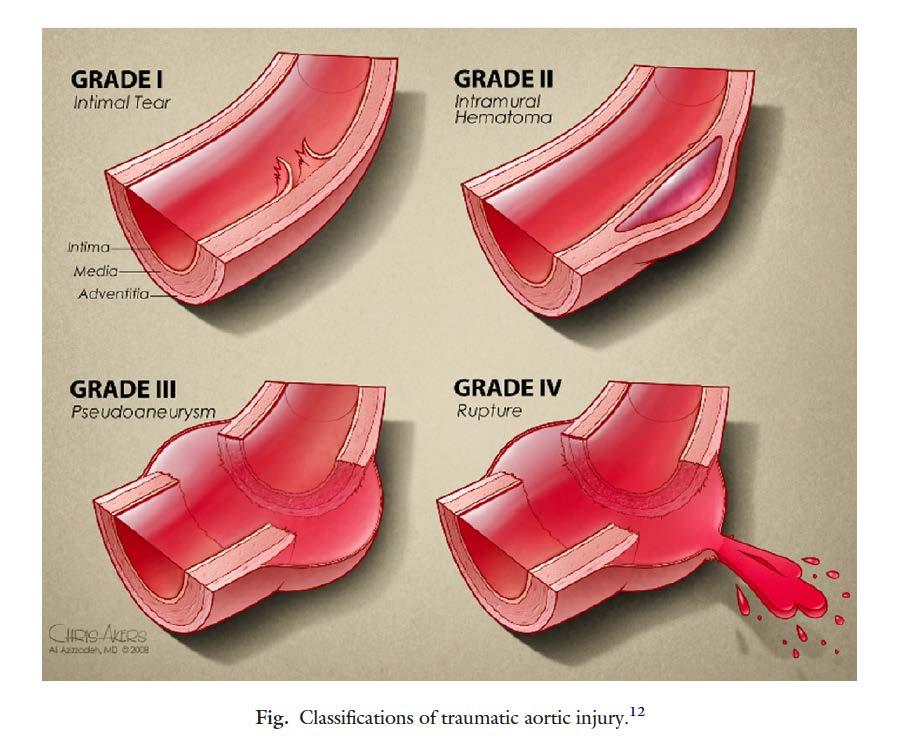
16 Treatment Algorithm GRADE I Intimal Tear IVUS / Med TX GRADE II Intramural Hematoma TEVAR / OR GRADE III Pseudoaneurysm TEVAR / OR GRADE IV Rupture TEVAR / OR (Emergent)

17 TEVAR mandated?

18 Same Risk for Early Rupture?
19 Vancouver Simplified System
20 Harborview Minimal Aortic Injuries

21 Parameters for successful non-operative management of traumatic aortic injury Joseph Rabin, MD, Joe DuBose, MD, Clint W. Sliker, MD, James V. O Connor, MD, Thomas M. Scalea, MD, and Bartley P. Griffith, MD The Journal of Thoracic and Cardiovascular Surgery, Volume 147, Issue 1, January 2014, Pages Grade III with SSI Suggest urgent repair Grade III with out SSI Consider delayed repair during hospitalization after initial medical management Grade I and II with SSI consider repair if risk of rupture increased.
22
23 What Optimal Grading Should Do: Determine treatment Medical vs. TEVAR vs. Open repair Guide timing of treatment Emergent vs. Urgent vs. Delayed Guide prediction of natural history and optimal follow-up

24 aortictrauma.org 2014
25 Mission Statement To improve outcomes of patients with traumatic aortic injury (TAI) through education and research. Structure: Non-profit 501(c)(3) organization Board of Directors Multispecialty Medical Advisory Board

26 ATF Multispecialty Scientific Advisory Board (SAB) International leaders in TAI Vascular surgeons CT surgeons Trauma surgeons Radiologists
27 Aortic Trauma Foundation BTAI Study Retrospective study (Jan 2008 Dec 2013) Nine ACS Level 1 Trauma Centers 453 BTAI patients Exclusion if death before imaging (58) or transfer (13) N = 382 BTAI patients
28 Demographics Total (N =382) Age (Mean ± SD) 41.8 ± 17.8 Male, n (%) 278 (72.8%) Mechanism MVC, n (%) 249 (72.8%) MCC, n (%) 55 (14.4%) Fall, n (%) 28 (7.3%) Auto vs. Ped, n (%) 36 (9.4%) Other blunt, n (%) 14 (3.7%) Hypotension (SBP < 90) on arrival, n (%) 56 (14.7%) Admission GCS 8, n (%) 112 (29.3%) ISS (Mean ± SD) 37.5 ± 12.5 AIS Head 3, n (%) 139 (36.4%) AIS Chest 3, n (%) 375 (98.2%) AIS Abdomen 3, n (%) 132 (34.6%) AIS Extremity 3, n (%) 157 (41.1%)
 Grade II, n (%) 68 (17.8%) Grade III, n (%) 192 (50.")
29 Injuries Identified SVS Injury Grade Grade I, n (%) 94 (24.6%) Grade II, n (%) 68 (17.8%) Grade III, n (%) 192 (50.3%) Grade IV, n (%) 28 (7.3%)
30 Imaging and Associated Findings Imaging Modality utilized for diagnosis CTA alone, n (%) 361 (94.5%) CTA + Angiography, n (%) 9 (2.4%) Angiography Alone, n (%) 2 (0.5%) CTA + Angiography + IVUS, n (%) 10 (2.6%) Pseudocarctation, n (%) 13 (3.4%) Mediastinal Hematoma with evidence of compression, n (%) 103 (27.0%) Associated Hemothorax, n (%) 110 (28.8%) Hemothorax > 300 cc, n (%) 40 (10.5%) Hemothorax > 500 cc, n (%) 18 (4.7%) Hemothorax > 1000 cc, n (%) 5 (1.3%)
31 Non-BTAI Specific Treatment Requirements Craniotomy / Craniectomy, n (%) 4 (1.0%) Laparotomy, n (%) 87 (22.8%) Thoracotomy / Sternotomy (not for TAI), n (%) 16 (4.2%) ICU LOS (Mean ± SD) 11.3 ± 12.6 Hospital LOS (Mean ± SD) 19.0 ± 19.5 Ventilator Days (Mean ± SD) 8.2 ± 11.0 PRBC 24 hrs (Mean ± SD) 3.6 ± 6.0 FFP 24 hrs (Mean ± SD) 2.4 ± 4.6
32 Complications Stroke, n (%) 6 (1.6%) Acute Renal Failure, n (%) 26 (6.8%) DVT, n (%) 23 (6.0%) Pulmonary Embolism, n (%) 25 (6.5%) Catheter-related UTI, n (%) 30 (7.9%) Blood Stream Infection, n (%) 46 (12.0%) Hospital-acquired pneumonia, n (%) 36 (9.4%) Ventilator-associated pneumonia, n (%) 50 (13.1%) ALI / ARDS, n (%) 45 (11.8%) Sepsis, n (%) 56 (14.7%)
33 Overall BTAI Mortality (N = 382) In-hospital mortality, n (%) 72 (18.8%) Aortic-related mortality, n (%) 25 (6.5%)
34 Nonoperative Management 123 patients; 31.9% N = 123 patients (31.9% overall) NOM (vs. Open Repair or TEVAR) Older (Mean 44.7 vs. 40.4%, p = 0.028) 76.5% of all Grade I BTAI Less likely to have mediastinal hematoma on CTA Higher overall mortality (35.0% vs. 11.2%, p < 0.001)
35 Nonoperative Management 2 failures (Grade I, IV) => TEVAR Aortic-related mortality = 9.8% vs. 5.0% for repair (Open or TEVAR)
36 Repair (Open / TEVAR) Open Repair (OR) = 61 (16%) TEVAR = 198 (51.8%) TEVAR patients (compared to OR) Older (Mean 41.7 vs. 35.8, p = ) Lower ISS (Mean 35.6 vs. 42.4, p < 0.001) Less mediastinal hematoma (25.8% vs. 50.8%, p < 0.001) Less PRBC required (Mean 3.1 vs. 5.9, p = 0.002) Less FFP required (Mean 3.3 vs. 1.9, p = 0.021)
37 Repair (Open / TEVAR) TEVAR (vs. OR) Lower overall mortality (8.6% vs. 19.7%, p = 0.021) Lower aortic-related mortality (2.5% vs. 13.1%, p = 0.003)
38 TEVAR Devices Characteristics of TEVAR devices utilized (n =198) (4 not recorded; 194 known) Manufacturers Cook % Gore % Medtronic %
39 TEVAR Devices Diameter of Devices (4 not recorded; 194 known) N % Less than 26 mm % mm % mm % Device Lengths (8 not recorded known) Less than or equal 10 cm % Greater than 10 cm % Minimum 6.0 cm Maximum 20.2 cm
40 TEVAR Outcomes Endovascular repair, n (%) 198/382 (51.8%) Subclavian coverage, n (%) 82/198 (41.4%) Endograft malposition at initial TEVAR, n (%) 6/198 (3.0%) Endoleak, n (%) 5/198 (2.5%) Early Stent Fracture, n (%) 0/198 (0%) Early stent migration, n (%) 1/198 (0.5%) Access site pseudoaneurysm, n (%) 1/198 (0.5%) Access site persistent or delayed bleeding requiring intervention, n (%) 1/198 (0.5%) Treatment failure TEVAR, n (%) 6/198 (3.0%) TEVAR salvage, n (%) 2/198 (1.0%) OPEN salvage, n (%) 4/198 (2.0%)
41 TEVAR Outcomes Paralysis after TEVAR = 1 34 mm diameter device; 20 cm coverage No subclavian coverage 81 yo Stroke = 2 Diameters 26, 32 mm; Length 10,15 cm Both underwent L SCA coverage Ages 62, 85
42 SVS Grade I - II Nonoperative management (N = 91) TEVAR (N = 61) p - vlaue No difference in outcomes for patients Age (Mean ± SD) 42.3 ± ± Male, n (%) 64 (66.7%) 41 (67.2%) ISS (Mean ± SD) 34.9 ± ,1 ± Hypotension treated (SBP < 90) on arrival, n (%) with NOM vs. TEVAR 12 (13.0%) for Minimal 8 (13.1%) Admission GCS 8, n (%) 23 (24.7%) 17 (28.3%) AIS Head 3, n (%) 33 (35.1%) 19 (31.1%) AIS Abdomen 3, n (%) 33 (35.1%) 24 (39.3%) BTAI (SVS Grade I II injuries) AIS Extremity 3, n (%) 40 (42.6%) 27 (44.3%) Mediastinal Hematoma with evidence of compression, n (%) 5 (5.2%) 12 (19.7%) Associated Hemothorax, n (%) 15 (15.6%) 15 (24.6%) Goal Blood Pressure achieved with medical adjuncts, n (%) 51 (91.1%) 15 (93.8%) Craniotomy / Craniectomy, n (%) 3 (3.1%) 1 (1.6%) Laportomy, n (%) 17 (17.7%) 17 (27.9%) Thoracotomy / Sternotomy (not for TAI), n (%) 2 (2.1%) 1 (1.6%) SVS presently recommends treatment for ICU LOS (Mean ± SD) 9.8 ± ± Hospital LOS (Mean ± SD) 16.4 ± ± Ventilator Days (Mean ± SD) 6.3 ± ± PRBC 24 hrs (Mean SVS ± SD) Grade II injuries 2.2 ± ± FFP 24 hrs (Mean ± SD) 1.8 ± ± Paralysiss, n (%) 0 (0%) 1 (1.6%) Stroke, n (%) 4 (4.2%) 1 (1.6%) Acute Renal Failure, n (%) 8 (8.3%) 3 (4.9%) DVT, n (%) 4 (4.2%) 6 (9.8%) Pulmonary Embolism, n (%) 4 (4.2%) 6 (9.8%) More investigation needed in this subgroup Catheter-related UTI, n (%) 6 (6.3%) 5 (8.2%) Blood Stream Infection, n (%) 12 (12.5%) 6 (9.8%) Hospital-acquired pneumonia, n (%) 4 (4.2%) 5 (8.2%) Ventilator-associated pneumonia, n (%) 8 (8.3%) 7 (11.5%) ALI / ARDS, n (%) 11 (11.5%) 9 (14.8%) Sepsis, n (%) 9 (9.4%) 11 (18.0%) In-hospital mortality, n (%) 19 (19.8%) 6 (9.8%) Aortic-related mortality, n (%) 0 (0%) 2 (3.3%) 0.149
43 Aortic-related mortality 25 aortic-related mortalities overall All but 7 occurred prior to opportunity for repair All dying before repair attempt ISS > 25 7 deaths occurred after opportunity for repair
44 Deaths after attempt at BTAI repair (N = 7) 2 Grade II; 2 Grade 3; 4 Grade 4 All severely injured 3 GCS 3 on arrival with head AIS > 3 4 abdominal AIS > 3 3 required laparotomy 2 massive transfusions
45 Deaths after attempt at BTAI repair (N = 7) 4 open surgical repairs; 3 TEVAR 5 died within 24 hours of admission one between 24 and 48 hours one at 36 days in ICU with VAP and MOF
46 Independent Predictors of all-cause and aortic-related mortality among BTAI patients Variable Adjusted Odds Ratio (95% CI) p -value All-cause mortality ISS (continuous) 1.06 [ ] Nonoperative Management [ ] < SVS Grade (linear continuous) 2.45 [ ] < Admission Glasgow Coma Score 0.88 [ ] PRBC's required over 1st 24 hours 1.10 [ ] Aortic-related mortality ISS (continuous) 1.07 [ ] SVS Grade (linear continuous) [ ] < TEVAR (dichotomous) 0.21 [ ] AIS Chest (continuous) 6.41 [ ]
47 ATF Survey

48 ATF Survey SVS AAST EAST STS SIR

49

50

51

52

53

54
55 Methods TEVAR for BTAI from December 2004-October 2015 Age, gender, mechanism of injury, admission physiologic data, ISS, TRISS, and hospital/icu length of stay Grade of aortic injury based on the SVS aortic injury scale
 grade II 79 (90%) grade III 7 (8%)")
56 Results 88 patients Aortic injury grade 2 (2%) grade II 79 (90%) grade III 7 (8%) grade IV
57 Major In-Hospital Complications Major in hospital complication rate was 57% (50) TEVAR related mortality was 0 Overall mortality 6 (6.8%) Intra-abdominal sepsis 1 (1.1%) Cardiac arrest 2 (2.3%) Grade 5 liver injury 1 (1.1%) TBI 2 (2.3%)
58 Paraplegia/Stroke Paraplegia and stroke rate of 0% Decreasing rates since 2008 AAST (0.8% paraplegia and 1.6% stroke) Consistent with recent reports Likely secondary to short treatment zones and compensatory nature of younger patients
 Approach Patient # (%) Complication Rate Open Femoral 87% 0% Percutaneous Femoral 10 (11.")
59 Percutaneous TEVAR (ptevar) First description of 6Fr Perclose ProGlide systems exclusively in trauma patients Final 10 consecutive patients in the series treated percutaneously No significant access complications with any approach (1 seroma, observed) Approach Patient # (%) Complication Rate Open Femoral 87% 0% Percutaneous Femoral 10 (11.4%) 0% Retroperitoneal Conduit 1 (1%) 0%
60 Heparin SVS recommends heparinization in smaller doses in trauma 23 patients with a TBI were given heparin 10 patients without heparin No adverse events from its use or lack thereof Decision to heparinize should be individualized
 partially in 7 patients (8%) 2 Carotid LSCA bypasses")

61 Upper Extremity Ischemia LSCA covered in 19 patients (21.6%) partially in 7 patients (8%) 2 Carotid LSCA bypasses performed prophylactically No post operative ischemia was identified Revascularization only if necessary CABG, cerebrovascular disease
62 TEVAR-related Complications TEVAR-related complication in 8 patients (9.1%) 4 (4.5%) type 1a 2 (2.3%) type 2 2 (2.3%) type 3 No late endoleaks All type 2 and 3 endoleaks resolved spontaneously Overall TEVAR re-intervention rate was 4.5% Open conversion required in only 2 (2.3%)
63 TEVAR-related Complications Reduction in endoleaks and major vascular injuries Higher rate of endoleak observation and resolution No re interventions necessary after 2009

64 TEVAR-related Complications AAST 2008 Current Review Endoleak 14.4% 9.1% Endoleak Reintervention Conversion to open Major Vascular Injury 12% 4.5% 4.8% 2.3% 4% 0%
65 Follow-Up Post discharge surveillance continues to be a problem No delayed device complications were identified on CT No patients returned with complications Mid to late term device complications are rarely identified in the literature
66 BTAI: Ongoing Areas of Controversy Management of intramural hematoma (G 2) Timing of repair Urgent vs. emergent Prioritizing repair of associated injuries (TBI) Optimal follow-up imaging regimen

67 Future Research ATF-AAST Prospective Registry Optimal Management of Minimal Aortic Injuries Predictors of early rupture Multispecialty consensus on diagnosis and treatment Long-term outcomes Establish natural history

68 Thank you
How Did We Get To The? CT Scan Granularity & Development of TAVER. Multi & Single Center Reports Getting Us Closer to Answer
 How Did We Get To The? CT Scan Granularity & Development of TAVER Multi & Single Center Reports Getting Us Closer to Answer # Patients Dying That anyone survives complete transection of this artery is
How Did We Get To The? CT Scan Granularity & Development of TAVER Multi & Single Center Reports Getting Us Closer to Answer # Patients Dying That anyone survives complete transection of this artery is
TEVAR FOR! THORACIC AORTIC TRAUMA"
 10th HKL Vascular Surgery Conference and Workshop" TEVAR FOR! THORACIC AORTIC TRAUMA" Dr Hanif Hussein" Vascular and General Surgeon" Department of Surgery" Hospital Kuala Lumpur" Source: MIROS! Thoracic
10th HKL Vascular Surgery Conference and Workshop" TEVAR FOR! THORACIC AORTIC TRAUMA" Dr Hanif Hussein" Vascular and General Surgeon" Department of Surgery" Hospital Kuala Lumpur" Source: MIROS! Thoracic
Advances in Treatment of Traumatic Aortic Transection
 Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die
 account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
Contemporary Management of Blunt Thoracic Aortic Injury: Results of an EAST, AAST and SVS Survey by the Aortic Trauma Foundation
 Original Article Vol. 1, No. 1; 2017; pp 4 8 DOI: 10.26676/jevtm.v1i1.8 Contemporary Management of Blunt Thoracic Aortic Injury: Results of an EAST, AAST and SVS Survey by the Aortic Trauma Foundation
Original Article Vol. 1, No. 1; 2017; pp 4 8 DOI: 10.26676/jevtm.v1i1.8 Contemporary Management of Blunt Thoracic Aortic Injury: Results of an EAST, AAST and SVS Survey by the Aortic Trauma Foundation
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury. Conflict of Interest. Hypotensive shock 5/5/2014. none
 EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan
 The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
Four-year Surgical Results for Traumatic Aortic Injury in China Medical University Hospital, Mid-Taiwan
 Four-year Surgical Results for Traumatic Aortic Injury in China Medical University Hospital, Mid-Taiwan Yi-Chun Lin 林怡均 (5 th grade medical student), MingLi Li 李明禮, Chih-Hsiang Hsu, Ching-Feng Wu, Hui-Han
Four-year Surgical Results for Traumatic Aortic Injury in China Medical University Hospital, Mid-Taiwan Yi-Chun Lin 林怡均 (5 th grade medical student), MingLi Li 李明禮, Chih-Hsiang Hsu, Ching-Feng Wu, Hui-Han
Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry
 University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Haemodynamically unstable patient with chest trauma
 HR J Clinical Case - Test Yourself Interventional Haemodynamically unstable patient with chest trauma Dimitrios Tomais, Theodoros Kratimenos, Dimosthenis Farsaris Interventional Radiology Unit, Radiology
HR J Clinical Case - Test Yourself Interventional Haemodynamically unstable patient with chest trauma Dimitrios Tomais, Theodoros Kratimenos, Dimosthenis Farsaris Interventional Radiology Unit, Radiology
Development of a Branched LSA Endograft & Ascending Aorta Endograft
 Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Thoracic aortic trauma A.T.O.ABDOOL-CARRIM ACADEMIC HEAD VASCULAR SURGERY DEPARTMENT OF SURGERY UNIVERSITY OF WITWATERSRAND
 Thoracic aortic trauma A.T.O.ABDOOL-CARRIM ACADEMIC HEAD VASCULAR SURGERY DEPARTMENT OF SURGERY UNIVERSITY OF WITWATERSRAND Thoracic Aortic Trauma In USA and CANADA 7500-8000 die of blunt thoracic aortic
Thoracic aortic trauma A.T.O.ABDOOL-CARRIM ACADEMIC HEAD VASCULAR SURGERY DEPARTMENT OF SURGERY UNIVERSITY OF WITWATERSRAND Thoracic Aortic Trauma In USA and CANADA 7500-8000 die of blunt thoracic aortic
An outcome analysis of endovascular versus open repair of blunt traumatic aortic injuries
 From the Southern Association for Vascular Surgery An outcome analysis of endovascular versus open repair of blunt traumatic aortic injuries Ali Azizzadeh, MD, a Kristofer M. Charlton-Ouw, MD, a Zhongxue
From the Southern Association for Vascular Surgery An outcome analysis of endovascular versus open repair of blunt traumatic aortic injuries Ali Azizzadeh, MD, a Kristofer M. Charlton-Ouw, MD, a Zhongxue
I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical Department National Taiwan University Hospital
 Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Neurological Complications of TEVAR. Frank J Criado, MD. Union Memorial-MedStar Health Baltimore, MD USA
 ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
Blunt traumatic aortic injury: Initial experience with endovascular repair
 Blunt traumatic aortic injury: Initial experience with endovascular repair Ali Azizzadeh, MD, Kourosh Keyhani, DO, Charles C. Miller III, PhD, Sheila M. Coogan, MD, Hazim J. Safi, MD, and Anthony L. Estrera,
Blunt traumatic aortic injury: Initial experience with endovascular repair Ali Azizzadeh, MD, Kourosh Keyhani, DO, Charles C. Miller III, PhD, Sheila M. Coogan, MD, Hazim J. Safi, MD, and Anthony L. Estrera,
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Technique and Outcome of Laser Fenestration For Arch Vessels
 Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
I have the following financial relationships to disclose:
 Novel Approaches to Endovascular Management of Aortic Aneurysms Rodney A White, MD Medical Director, Vascular Services MemorialCare Heart & Vascular Institute Long Beach Memorial Hospital Long Beach, California
Novel Approaches to Endovascular Management of Aortic Aneurysms Rodney A White, MD Medical Director, Vascular Services MemorialCare Heart & Vascular Institute Long Beach Memorial Hospital Long Beach, California
High Risk Uncomplicated Type B Dissection
 High Risk Uncomplicated Type B Dissection Ali Azizzadeh, MD, FACS Director, Vascular Surgery Vice Chair, Department of Surgery Associate Director, Heart Institute Cedars-Sinai Medical Center Los Angeles,
High Risk Uncomplicated Type B Dissection Ali Azizzadeh, MD, FACS Director, Vascular Surgery Vice Chair, Department of Surgery Associate Director, Heart Institute Cedars-Sinai Medical Center Los Angeles,
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011
 Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation
 Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Endovascular Trauma Management. Thomas Larzon, MD, PhD Dep of Cardiothoracic and Vascular Surgery Örebro University Hospital, Sweden
 Endovascular Trauma Management Thomas Larzon, MD, PhD Dep of Cardiothoracic and Vascular Surgery Örebro University Hospital, Sweden Medtronic Symposium, LINC 2016 Disclosures I have the following potential
Endovascular Trauma Management Thomas Larzon, MD, PhD Dep of Cardiothoracic and Vascular Surgery Örebro University Hospital, Sweden Medtronic Symposium, LINC 2016 Disclosures I have the following potential
Animesh Rathore, MD 4/21/17. Penetrating atherosclerotic ulcers of aorta
 Animesh Rathore, MD 4/21/17 Penetrating atherosclerotic ulcers of aorta Disclosures No financial disclosures Thank You Dr. Panneton for giving this lecture for me. I am stuck at Norfolk with an emergency
Animesh Rathore, MD 4/21/17 Penetrating atherosclerotic ulcers of aorta Disclosures No financial disclosures Thank You Dr. Panneton for giving this lecture for me. I am stuck at Norfolk with an emergency
Role of the Radiologist
 Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
TEVAR for the Ascending Aorta
 TEVAR for the Ascending Aorta Himanshu J. Patel MD Joe D. Morris Collegiate Professor Section Head, Adult Cardiac Surgery University of Michigan Frankel Cardiovascular Center Disclosures Himanshu J. Patel
TEVAR for the Ascending Aorta Himanshu J. Patel MD Joe D. Morris Collegiate Professor Section Head, Adult Cardiac Surgery University of Michigan Frankel Cardiovascular Center Disclosures Himanshu J. Patel
Thoracic Endovascular Aortic Repair (TEVAR) Indications and Basic Procedure
 Indications and Basic Procedure") Thoracic Endovascular Aortic Repair (TEVAR) Indications and Basic Procedure Tilo Kölbel, MD, PhD University Heart Center Hamburg University Hospital Eppendorf Disclosure Speaker name: Tilo Kölbel, MD I
Thoracic Endovascular Aortic Repair (TEVAR) Indications and Basic Procedure Tilo Kölbel, MD, PhD University Heart Center Hamburg University Hospital Eppendorf Disclosure Speaker name: Tilo Kölbel, MD I
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
Total Endovascular Repair Type A Dissection. Eric Herget Interventional Radiology
 Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm
 Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic
 Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies. Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018
 Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Current treatment of Aortic Aneurysms and Dissections. Adam Keefer, MD, FACS Sean Hislop, MD, FACS
 Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
A 14-year experience with blunt thoracic aortic injury
 From the New England Society for Vascular Surgery A 14-year experience with blunt thoracic aortic injury Jennifer Watson, MD, Jeffrey Slaiby, MD, Manuel Garcia Toca, MD, Edward J. Marcaccio Jr, MD, and
From the New England Society for Vascular Surgery A 14-year experience with blunt thoracic aortic injury Jennifer Watson, MD, Jeffrey Slaiby, MD, Manuel Garcia Toca, MD, Edward J. Marcaccio Jr, MD, and
Endovascular Treatment of Symptomatic Abdominal Aortic Aneurysms
 춘계심장학회, April 2013 Endovascular Treatment of Symptomatic Abdominal Aortic Aneurysms Seung-Hyuk Choi Division of Cardiology Samsung Medical Center SungKyunKwan Univ. Contents Introduction EVAR vs. Open
춘계심장학회, April 2013 Endovascular Treatment of Symptomatic Abdominal Aortic Aneurysms Seung-Hyuk Choi Division of Cardiology Samsung Medical Center SungKyunKwan Univ. Contents Introduction EVAR vs. Open
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
IMH/Penetrating Aortic Ulcers/ Saccular Aneurysms: How to manage and when to intervene
 IMH/Penetrating Aortic Ulcers/ Saccular Aneurysms: How to manage and when to intervene UCSF Vascular Surgery Symposium 2018 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery Co-director, Comprehensive
IMH/Penetrating Aortic Ulcers/ Saccular Aneurysms: How to manage and when to intervene UCSF Vascular Surgery Symposium 2018 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery Co-director, Comprehensive
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA)
") The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Disclosures: Acute Aortic Syndrome. A. Michael Borkon, M.D. Director of CV Surgery Mid America Heart Institute Saint Luke s Hospital Kansas City, MO
 Acute Aortic Syndrome Disclosures: A. Michael Borkon, M.D. Director of CV Surgery Mid America Heart Institute Saint Luke s Hospital Kansas City, MO No financial relationships to disclose 1 Acute Aortic
Acute Aortic Syndrome Disclosures: A. Michael Borkon, M.D. Director of CV Surgery Mid America Heart Institute Saint Luke s Hospital Kansas City, MO No financial relationships to disclose 1 Acute Aortic
UC SF. Disclosures. Thoracic Endovascular Aortic Repair 4/24/2009. Management of Acute Dissections: Is There Still a Role for Open Surgery?
 UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
Approaches to type II Endoleaks: Transcaval, transarterial, translumbar. Saher Sabri,MD University of Virginia
 Approaches to type II Endoleaks: Transcaval, transarterial, translumbar Saher Sabri,MD University of Virginia Saher Sabri, M.D. Speakers Bureau: W.L.Gore & Associates, Abbott Type 2 Endoleaks after EVAR
Approaches to type II Endoleaks: Transcaval, transarterial, translumbar Saher Sabri,MD University of Virginia Saher Sabri, M.D. Speakers Bureau: W.L.Gore & Associates, Abbott Type 2 Endoleaks after EVAR
Role of Gender in TEVAR and EVAR results from the GREAT registry
 Role of Gender in TEVAR and EVAR results from the GREAT registry Mauro Gargiulo Vascular Surgery University of Bologna - DIMES Policlinico S.Orsola-Malpighi Bologna, Italy mauro.gargiulo2@unibo.it Disclosure
Role of Gender in TEVAR and EVAR results from the GREAT registry Mauro Gargiulo Vascular Surgery University of Bologna - DIMES Policlinico S.Orsola-Malpighi Bologna, Italy mauro.gargiulo2@unibo.it Disclosure
Endoanchor-assisted TEVAR
 Endoanchor-assisted TEVAR May 29, 2015 NCVH2015 Grayson H. Wheatley III, MD Director of Aortic and Endovascular Surgery Associate Professor of Surgery Temple University School of Medicine Disclosures Consultant
Endoanchor-assisted TEVAR May 29, 2015 NCVH2015 Grayson H. Wheatley III, MD Director of Aortic and Endovascular Surgery Associate Professor of Surgery Temple University School of Medicine Disclosures Consultant
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Improving Endograft Durability with EndoAnchors
 Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Effect of post-intubation hypotension on outcomes in major trauma patients
 Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Experience of endovascular procedures on abdominal and thoracic aorta in CA region
 Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
VALIANT THORACIC STENT GRAFT WITH THE CAPTIVIA DELIVERY SYSTEM 2016 ANNUAL PHYSICIAN CLINICAL UPDATE
 VALIANT THORACIC STENT GRAFT WITH THE CAPTIVIA DELIVERY SYSTEM 2016 ANNUAL PHYSICIAN CLINICAL UPDATE MARCH 27, 2016 2016 ANNUAL PHYSICIAN CLINICAL UPDATE VALIANT THORACIC STENT GRAFT WITH THE CAPTIVIA
VALIANT THORACIC STENT GRAFT WITH THE CAPTIVIA DELIVERY SYSTEM 2016 ANNUAL PHYSICIAN CLINICAL UPDATE MARCH 27, 2016 2016 ANNUAL PHYSICIAN CLINICAL UPDATE VALIANT THORACIC STENT GRAFT WITH THE CAPTIVIA
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations
 The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
TEVAR. (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection. Bruce Tjaden MD Vascular Surgery Fellow
 for Aneurysm and Dissection. Bruce Tjaden MD Vascular Surgery Fellow") Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston TEVAR (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston TEVAR (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection
Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft
 MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
AAA Management: A Review of Current Therapy, Techniques, Outcomes and Best Practices
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians Frank R. Arko, III, MD Professor, Cardiovascular Surgery Co Director, Aortic Institute Director, Endovascular
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians Frank R. Arko, III, MD Professor, Cardiovascular Surgery Co Director, Aortic Institute Director, Endovascular
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Disclosures. Harborview Medical Center. Ruptured Aortic Aneurysms. April 6, Copyright UPM-Kymmene Group 1. Co-Founder: AORTICA Corporation
 EVAR for Ruptured Abdominal Aortic Aneurysm How I Do It and What Are the Results? Disclosures Co-Founder: AORTICA Corporation Benjamin W. Starnes MD, FACS The Alexander Whitehill Clowes Endowed Chair of
EVAR for Ruptured Abdominal Aortic Aneurysm How I Do It and What Are the Results? Disclosures Co-Founder: AORTICA Corporation Benjamin W. Starnes MD, FACS The Alexander Whitehill Clowes Endowed Chair of
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Aortic CT: Intramural Hematoma. Leslie E. Quint, M.D.
 Aortic CT: Intramural Hematoma Leslie E. Quint, M.D. 43 M Mid back pain X several months What type of aortic disease? A. Aneurysm with intraluminal thrombus B. Chronic dissection with thrombosed false
Aortic CT: Intramural Hematoma Leslie E. Quint, M.D. 43 M Mid back pain X several months What type of aortic disease? A. Aneurysm with intraluminal thrombus B. Chronic dissection with thrombosed false
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy. Johannes Lammer Medical University Vienna, Austria
 Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
Fri., 10/17/14 Polytrauma, PAPER #74, 4:00 pm OTA 2014
 Fri., 10/17/14 Polytrauma, PAPER #74, 4:00 pm OTA 2014 Clinical Indications for CT Angiography in Lower Extremity Trauma Joseph T. Patterson, MD 1 ; Thomas Fishler, MD 2 ; Daniel D. Bohl, MPH 3 ; Michael
Fri., 10/17/14 Polytrauma, PAPER #74, 4:00 pm OTA 2014 Clinical Indications for CT Angiography in Lower Extremity Trauma Joseph T. Patterson, MD 1 ; Thomas Fishler, MD 2 ; Daniel D. Bohl, MPH 3 ; Michael
Taming The Aorta. David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA
 Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Subclavian Artery Plug Embolization (SAPE study): a real experience about endovascular subclavian occlusion prior to thoracic vascular repair
: a real experience about endovascular subclavian occlusion prior to thoracic vascular repair") Subclavian Artery Plug Embolization (SAPE study): a real experience about endovascular subclavian occlusion prior to thoracic vascular repair Simone Salvati, Luca Bertoglio, Alessandra Fittipaldi, Andrea
Subclavian Artery Plug Embolization (SAPE study): a real experience about endovascular subclavian occlusion prior to thoracic vascular repair Simone Salvati, Luca Bertoglio, Alessandra Fittipaldi, Andrea
Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries
 Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries 4 th Nordic Trauma Course 2006 Stuart E. Mirvis, M.D., FACR Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland
Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries 4 th Nordic Trauma Course 2006 Stuart E. Mirvis, M.D., FACR Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland
6. Endovascular aneurysm repair
 Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
3 : 37. Kirit Patel, USA CLASSIFICATION DIAGNOSIS
 3 : 37 Management of Aortic Aneurysms Clinical features and diagnosis of thoracic aortic aneurysm An aneurysm is currently defined as a localized dilatation of the aorta, 50 percent over the normal diameter,
3 : 37 Management of Aortic Aneurysms Clinical features and diagnosis of thoracic aortic aneurysm An aneurysm is currently defined as a localized dilatation of the aorta, 50 percent over the normal diameter,
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D.
 CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
Vascular Emergencies. Scott M Surowiec, MD Assistant Professor of Surgery Upstate Vascular and Crouse Hospital September 29, 2015
 Vascular Emergencies Scott M Surowiec, MD Assistant Professor of Surgery Upstate Vascular and Crouse Hospital September 29, 2015 Introduction Main vascular emergencies include Ruptured Abdominal Aortic
Vascular Emergencies Scott M Surowiec, MD Assistant Professor of Surgery Upstate Vascular and Crouse Hospital September 29, 2015 Introduction Main vascular emergencies include Ruptured Abdominal Aortic
Arch Repair with the Bolton Medical RelayBranch Thoracic Stent-graft system: Multicenter experience
 Arch Repair with the Bolton Medical RelayBranch Thoracic Stent-graft system: Multicenter experience Joost van Herwaarden, MD, PhD University Medical Center, Utrecht Disclosure I have the following potential
Arch Repair with the Bolton Medical RelayBranch Thoracic Stent-graft system: Multicenter experience Joost van Herwaarden, MD, PhD University Medical Center, Utrecht Disclosure I have the following potential
Endovascular Stent Grafts for Disorders of the Thoracic Aorta
 Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2018 Origination: 5/2006 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Endovascular Stent Grafts for Disorders of the Thoracic Aorta Policy Number: 7.01.86 Last Review: 9/2018 Origination: 5/2006 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Animesh Rathore, MD 4/22/17. The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management
 Animesh Rathore, MD 4/22/17 The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management Disclosures Just a young vascular surgeon who would like to keep his job My opponent
Animesh Rathore, MD 4/22/17 The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management Disclosures Just a young vascular surgeon who would like to keep his job My opponent
GORE TAG Thoracic Endoprosthesis ANNUAL CLINICAL UPDATE SEPTEMBER 2018 Abstract. Section I GORE TAG Device Clinical experience. Section II Conformable
 GORE TAG Thoracic Endoprosthesis ANNUAL CLINICAL UPDATE SEPTEMBER 08 Abstract This annual clinical update provides a review of the ongoing experience with the GORE TAG Thoracic Endoprosthesis There have
GORE TAG Thoracic Endoprosthesis ANNUAL CLINICAL UPDATE SEPTEMBER 08 Abstract This annual clinical update provides a review of the ongoing experience with the GORE TAG Thoracic Endoprosthesis There have
OHSU. Blunt cerebrovascular injuries: anatomic and pathologic heterogeneity produce management uncertainties.
 Kohler Pavilion With tram station Center for Health and Healing Top ten trauma papers published in the past year Presented at St Charles Medical Center, Bend, Oregon March 13, 2015 OHSU Richard J Mullins,
Kohler Pavilion With tram station Center for Health and Healing Top ten trauma papers published in the past year Presented at St Charles Medical Center, Bend, Oregon March 13, 2015 OHSU Richard J Mullins,
Clinical Trials of Acute and Chronic Dissections. Gregory Landry MD
 Clinical Trials of Acute and Chronic Dissections Gregory Landry MD No disclosures Acute vs chronic dissection: Definitions 1950s: Acute < 2 weeks, Chronic > 2 weeks 2013: European Interdisciplinary Consensus
Clinical Trials of Acute and Chronic Dissections Gregory Landry MD No disclosures Acute vs chronic dissection: Definitions 1950s: Acute < 2 weeks, Chronic > 2 weeks 2013: European Interdisciplinary Consensus
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
MANAGEMENT OF RETAINED HAEMOTHORAX DR AG JACOBS PRINCIPAL SPECIALIST DEPARTMENT OF CARDIO THORACIC SURGERY UNIVERSITY OF PRETORIA
 MANAGEMENT OF RETAINED HAEMOTHORAX DR AG JACOBS PRINCIPAL SPECIALIST DEPARTMENT OF CARDIO THORACIC SURGERY UNIVERSITY OF PRETORIA MANAGEMENT OF RETAINED HAEMOTHORAX Retained Haemothorax Definition: Failure
MANAGEMENT OF RETAINED HAEMOTHORAX DR AG JACOBS PRINCIPAL SPECIALIST DEPARTMENT OF CARDIO THORACIC SURGERY UNIVERSITY OF PRETORIA MANAGEMENT OF RETAINED HAEMOTHORAX Retained Haemothorax Definition: Failure
Version 4.4. Institutional Outcomes Report 2014Q3. National Outcomes Report Aggregation Date: Jan 12, :59:59 PM
 Version 4.4 Institutional Outcomes Report 2014Q3 National Outcomes Report 999997 Aggregation Date: Jan 12, 2015 11:59:59 PM Publish Date: Jan 29, 2015 If User desires to publish or otherwise distribute
Version 4.4 Institutional Outcomes Report 2014Q3 National Outcomes Report 999997 Aggregation Date: Jan 12, 2015 11:59:59 PM Publish Date: Jan 29, 2015 If User desires to publish or otherwise distribute
Re-interventions after TEVAR:
 Re-interventions after TEVAR: How often does it occur and what are procedures most commonly utilized to treat these issues? Pacific Northwest Endovascular Conference Seattle, WA June 15, 2018 PENN Surgery
Re-interventions after TEVAR: How often does it occur and what are procedures most commonly utilized to treat these issues? Pacific Northwest Endovascular Conference Seattle, WA June 15, 2018 PENN Surgery
Importance of changes in thoracic and abdominal aortic stiffness following stent graft implantation
 14/9/2018 Importance of changes in thoracic and abdominal aortic stiffness following stent graft implantation Christos D. Liapis, MD, FACS, FRCS, FEBVS Professor (Em) of Vascular Surgery National & Kapodistrian
14/9/2018 Importance of changes in thoracic and abdominal aortic stiffness following stent graft implantation Christos D. Liapis, MD, FACS, FRCS, FEBVS Professor (Em) of Vascular Surgery National & Kapodistrian
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18