AUTHOR(S): COUGHLIN, MICHAEL J., M.D., BOISE, IDAHO. An Instructional Course Lecture, The American Academy of Orthopaedic Surgeons
|
|
|
- Milo Hunt
- 6 years ago
- Views:
Transcription
1 JBJA Journal of Bone and Joint Surgery - American June 1996, Volume 78-A, Number Instructional Course Lectures, The American Academy of Orthopaedic Surgeons - Hallux Valgus* Instructional Course Lecture AUTHOR(S): COUGHLIN, MICHAEL J., M.D., BOISE, IDAHO An Instructional Course Lecture, The American Academy of Orthopaedic Surgeons J Bone Joint Surg [Am] 1996; 78-A; Hallux valgus occurs with lateral deviation of the great toe and medial deviation of the first metatarsal. Commonly, the deformity is characterized by progressive subluxation of the first metatarsophalangeal joint (Figs. 1-A, 1-B, and 1-C). Occasionally, there is a static deformity due to valgus angulation of the distal articular surface of the first metatarsal or the proximal phalangeal articular surface (Fig. 2). Hallux valgus occurs almost exclusively in shoewearing societies (17). Coughlin and Thompson (27), noting the extremely high prevalence of bunions in American women in the fourth, fifth, or sixth decade of life, implicated constricting footwear as a cause of hallux valgus. This notion is supported by a study from China, where the prevalence of hallux valgus was fifteen times higher in people who wore shoes than in those who did not (128). Likewise, in Japan, Kato and Watanabe (59) noted that the prevalence of hallux valgus in women increased dramatically following the introduction of high-fashion footwear after World War II. While constricting footwear appears to be the major extrinsic cause of hallux valgus, intrinsic factors play a role as well. Inman (52) and Hohmann (48) both suggested pronation of the hindfoot as a major cause of bunion formation, while Mann and Coughlin (87) as well as others (23,61) reported that pes planus plays a minor role in this process. An increased angle between the first and second metatarsals (metatarsus primus varus) is often associated with hallux valgus deformity. Hardy and Clapham (40) reported an association between the magnitude of the hallux valgus angle and the firstsecond intermetatarsal angle and stated that metatarsus primus varus is secondary to an increased hallux valgus angle. Other intrinsic causes of hallux valgus may include contracture of the Achilles tendon, generalized joint laxity, hypermobility of the first metatarsocuneiform joint, and neuromuscular disorders (including cerebral palsy and stroke) (89). Heredity is thought to influence the development of hallux valgus in many individuals. Hardy and Clapham noted that fifty-seven (63 per cent) of the ninety-one patients in their series had a parent who had hallux valgus, and I (23) reported that a bunion was identified in twenty-nine (94 per cent) of thirty-one mothers of children who had hallux valgus. Anatomy The metatarsophalangeal joint of the great toe is different from that of the lesser toes because it has a sesamoid mechanism and a set of intrinsic muscles that stabilize the joint and provide motor strength to the first ray (131). The muscles and tendons that control the great toe are divided into four groups that encircle the first metatarsophalangeal joint (Fig. 3-A). On the dorsal aspect of the great toe, the extensor hallucis longus and brevis pass centrally, inserting into the distal and proximal phalanges, respectively. The extensor hallucis longus is anchored by the hood ligaments (38), a fibrous band that interdigitates medially and laterally with the collateral and sesamoid ligaments, forming the capsule of the metatarsophalangeal joint. The short and long flexor tendons pass on the plantar surface, with the tendons of the medial and lateral heads of the flexor hallucis brevis inserting into the medial and lateral sesamoids (Fig. 3-B). Distally, the sesamoids are attached to the base of the proximal phalanx by the plantar plate (Fig. 3-C). The flexor hallucis longus tendon is located plantar to the sesamoid complex, passing within a tendon sheath to insert into the base of the distal phalanx. The abductor and adductor hallucis tendons are located on the plantar-medial and plantar-lateral aspects, respectively, of the metatarsophalangeal joint and insert into the base of the proximal phalanx and the adjacent sesamoids (Fig. 4). The plantar half of the metatarsophalangeal joint capsule is reinforced by the tendons of the abductor hallucis and adductor hallucis, while the dorsal half of the metatarsophalangeal capsule is comparatively thin, without tendinous constraints. With the development of hallux valgus (Figs. 5-A, 5-B, and 5-C), the abductor hallucis tendon is displaced plantarward, leaving only the thinner and weaker dorsal half of the capsule as the major restraining force on the medial aspect (76). In its normal position, the abductor hallucis provides major support to the well aligned great toe (131). On the lateral aspect, the adductor hallucis provides stability as well; however, its insertion into the plantar-aspect of the lateral base of the proximal phalanx and lateral sesamoid becomes a deforming force as the hallux valgus deformity increases. Because it arises from the shafts of the lesser metatarsals, the adductor hallucis tends to tether the sesamoids and proximal phalanx as the first metatarsal deviates medially. Because it inserts on the plantar aspect of the proximal phalanx, the adductor hallucis also exerts a rotational force on the great toe, pronating it as the phalanx deviates laterally (Figs. 6-A and 6-B). With continued lateral movement, the imbalance progresses and the intrinsic plantar cuff (the adductor hallucis, flexor hallucis brevis, and abductor hallucis) rotates in a lateral direction (in relation to the head of the first metatarsal), leaving the thin dorsal half of the capsule that is at risk for additional deformation (131). As the hallux valgus deformity progresses, the extensor hallucis longus displaces into the first interspace and
2 becomes an adduction force on the great toe. Continuing lateral rotation of the intrinsic plantar cuff leads to displacement or subluxation of the medial and lateral sesamoids in relation to the plantar surface of the first metatarsal (Figs. 7-A, 7-B and 7-C). While this phenomenon has been described as subluxation of the sesamoids, it is actually the first metatarsal that deviates medially away from the sesamoid complex. The plantar surface of the first metatarsal is characterized by a crista, or intersesamoidal ridge, that articulates with the medial and lateral sesamoids (Figs. 8-A, and 8-B). As displacement occurs, this ridge is gradually smoothed out until it offers no additional resistance to displacement of the sesamoid (26), as can be demonstrated on an axial radiograph (Fig. 8-D). On an anteroposterior radiograph of a joint with moderate subluxation, the lateral sesamoid is uncovered 50 to 75 per cent within the first intermetatarsal space and the medial sesamoid is located in a central position plantar to the first metatarsal head (Figs. 8-C and 8-D). With a severe hallux valgus deformity, the lateral sesamoid migrates to the lateral aspect of the first metatarsal head and lies vertically dorsal to the medial sesamoid (38) (Figs. 8-E and 8-F). It is important to recognize the magnitude of subluxation of the sesamoids because this will guide the choice of the method of operative reconstruction. An operation that does not reduce this subluxation by relocation of the first metatarsal head to a normal articulation with both the medial and the lateral sesamoid creates a risk for recurrent deformity. As the hallux valgus deformity increases in magnitude, there is a corresponding increase in both the subluxation of the sesamoids and the pronation of the great toe. The operative technique for correction may vary considerably, depending on the magnitude of both of these deformities. Angular measurements on radiographs made with the patient standing are helpful to define the magnitude of the hallux valgus deformity (Fig. 9). The hallux valgus angle is formed by the intersection of the longitudinal axes of the proximal phalanx and the first metatarsal. A hallux valgus angle of less than 15 degrees is considered normal (40). The first-second intermetatarsal angle is formed by the intersection of the longitudinal axes of the first and second metatarsals, and an angle of less than 9 degrees is considered normal (89). With the use of these two measurements, a general classification scheme for hallux valgus was developed. It is helpful to define mild, moderate, and severe deformities, both to standardize their description and to assist in preoperative planning (89). A mild hallux valgus deformity is characterized by a hallux valgus angle of less than 20 degrees and a first-second intermetatarsal angle of 11 degrees or less (Fig. 1-A). Subluxation of the lateral sesamoid, as measured on an anteroposterior radiograph, is less than 50 per cent. A moderate deformity is characterized by a hallux valgus angle of 20 to 40 degrees, a first-second intermetatarsal angle of less than 16 degrees, and 50 to 75 per cent subluxation of the lateral sesamoid (Figs. 1-B, 8-C, and 8-D). A severe deformity is characterized by a hallux valgus angle of more than 40 degrees, a first-second intermetatarsal angle of 16 degrees or more, and more than 75 per cent subluxation of the lateral sesamoid (Figs. 1-C, 8-E, and 8-F). There may be substantial variation in the shape of the distal articular surface of the first metatarsal. A rounded surface is most common (Fig. 10-A), and it is more prone to subluxation and to the development of a progressive hallux valgus deformity. A flattened or chevron-shaped metatarsophalangeal articulation is more stable and tends to resist subluxation (89) ( 10-B). The term congruity is used to describe the relationship of the metatarsal and phalangeal articular surfaces. When the surfaces are aligned, the joint is said to be congruous (108) (Figs. 10-C and 10-D). When they are not aligned, the articulation is noncongruous (subluxation of the metatarsophalangeal joint) (Figs. 1-A, 1 1-B, and 1-C). The distal metatarsal articular surface forms an angle with the longitudinal axis of the first metatarsal (the distal metatarsal articular angle). The proximal articular surface of the proximal phalanx forms an angle with the longitudinal axis of the proximal phalanx (the proximal phalangeal articular angle). These two angles reflect the basic inclination of the metatarsophalangeal joint. Normally, the great toe is in slight valgus angulation (0 to 15 degrees) as a result of the lateral inclination or sloping of the distal metatarsal articular surface (23,108,116). This angulation is also known as the metatarsal articular orientation or the proximal articular set angle; however, the term distal metatarsal articular angle describes more clearly the inclination of the metatarsal articular surface. The proximal phalangeal articular angle has also been called the phalangeal articular orientation and the distal articular set angle. Although substantial angulation of the phalangeal articular surface in relation to the shaft of the phalanx is uncommon (two of sixty-five feet in one series (23) ), when it is present a hallux valgus interphalangeus deformity is created (Figs. 11-A, 11-B, and 11-C). Angulation of the phalangeal articular surface can occur in the presence of an increased distal metatarsal articular angle or subluxation of the metatarsophalangeal joint, or both. A normal metatarsophalangeal articulation occurs with a hallux valgus angle of less than 15 degrees. Angulation of the metatorsophalangeal joint may be created by mild subluxation of that joint, by a lateral sloping of the distal metatarsal articular surface, by increased lateral sloping of the proximal phalangeal articular surface, or by a combination of these. Piggott (108), in an analysis of congruous and noncongruous metatarsophalangeal joints with hallux valgus, determined that a congruous joint was less likely to have progression of the hallux valgus deformity. A non-congruous joint was likely to subluxate further with time. Twenty (9 per cent) of 215 adult feet with hallux valgus in the series reviewed by Piggott had a congruous joint, and twenty-eight (47 per cent) of sixty juvenile feet with hallux valgus reported on by me (23) had a congruous joint. It is important to distinguish a congruous
3 metatarsophalangeal joint from a non-congruous one when treating hallux valgus, as the choice of a specific operative approach depends on the pathological elements present. An intra-articular realignment (such as a McBride procedure or another distal soft-tissue reconstruction) achieves correction by rotating the articular surface of the phalanx across the articular surface of the metatarsal to reduce the hallux valgus angle. In contrast, an extra-articular correction (an Akin, Reverdin, chevron, or Mitchell osteotomy; an osteotomy of the proximal end of the metatarsal; or an osteotomy of the cuneiform) achieves correction through periarticular osteotomies, which do not change the articular orientation or congruency of the metatarsophalangeal joint. Realignment of a congruous hallux valgus deformity with an intra-articular procedure may be complicated postoperatively by either recurrence of the deformity or restricted motion of the metatarsophalangeal joint (89). The medial eminence, or bunion, is often the most visible component of a hallux valgus deformity. Often preoperative pain is centered in this region because of irritation of the dorsal cutaneous nerve of the great toe or an inflamed or thickened bursa overlying the medial eminence. Occasionally the medial eminence is hypertrophied, but frequently it is not much enlarged. An increase in the first-second intermetatarsal angle with lateral deviation of the great toe leaves the medial eminence prominent and easily irritated by constricting footwear. As the proximal phalanx deviates laterally, the head of the metatarsal is pushed medially. The lateral soft-tissue structures contract as the medial soft-tissue constraints become attenuated. The medial deviation of the first metatarsal gradually uncovers the lateral sesamoid. The intrinsic muscles, which normally act to stabilize the metatarsophalangeal joint, become deforming forces. There are no muscle insertions into the first metatarsal head; thus, its position is influenced to a great extent by the position of the proximal phalanx. With progressive subluxation of the metatarsophalangeal joint, a groove (or sagittal sulcus) develops at the medial border of the metatarsal articular surface. The magnitude of the hallux valgus deformity determines the presence and location of the sagittal sulcus. While this groove delineates the border of the articular surface, it is an unreliable landmark for the planning of a medial exostectomy. The sagittal sulcus may be located in the center of the metatarsal head when the deformity is severe, and it may be located more medially when the deformity is mild or moderate (38). It is important not to rely on the sagittal sulcus as the guide for resection of the medial eminence because, with a severe deformity, doing so may lead to excessive resection of bone. The shape and orientation of the metatarsocuneiform joint are variable factors that influence the magnitude of medial inclination of the first metatarsal. Normally the first metatarsocuneiform joint is inclined medially, but occasionally there is marked medial obliquity, which is believed by some to result in instability of the metatarsocuneiform joint (7,64). Radiographically, the metatarsocuneiform joint may appear to be flat, curved, or oblique, and the appearance can vary dramatically depending on the plane of the weightbearing radiograph (7). Undoubtedly, there is a certain amount of flexibility in the metatarsocuneiform joint (143), and this is demonstrated by the decrease in the size of the first-second intermetatarsal angle following a distal soft-tissue reconstruction. Excessive flexibility at this joint may be inferred from a radiograph, but it is best ascertained by physical examination (7,64). History and Physical Examination The primary symptom of hallux valgus is pain over the medial eminence. Pressure from footwear is the most frequent cause of this discomfort. Bursal inflammation, irritation of the skin, and even breakdown of the skin may be noted. The physical examination of a hallux valgus deformity must be performed with the patient sitting and standing. The deformity is often accentuated with weight-bearing. The foot is examined for a pes planus deformity and for contracture of the Achilles tendon, both of which may affect the choice and success of the operation. The magnitude of the hallux valgus deformity is noted, as is any pronation of the great toe. The passive and active range of motion of the metatarsophalangeal joint is measured (130). Pain or crepitus, or both, with motion of the metatarsophalangeal joint is often indicative of degenerative osteoarthrosis and often alters the choice of operative procedure. To check the metatarsocuneiform joint for hypermobility, the examiner grasps the first metatarsal with the thumb and index finger and pushes it in a plantar lateral-todorsomedial direction (64). Mobility of more than nine millimeters represents hypermobility (64), which, according to Mann and Coughlin (89), is present in less than 5 per cent of patients. The neurovascular status of the foot must also be assessed. Doppler studies may be performed if there is a question regarding the adequacy of circulation. The foot is inspected for deformities of the lesser toes that may cause discomfort as well. Other frequent symptoms are hammer-toe deformities of the second toe or metatarsalgia of the lesser metatarsophalangeal joints. The plantar surface of the foot should be inspected for intractable plantar keratoses or callosities. An attempt should be made to reduce the first metatarsophalangeal joint by passive correction of the hallux valgus deformity. This may be difficult if there is a soft-tissue contracture. This maneuver helps the examiner to assess the congruency of the metatarsophalangeal joint. Passive attempts to alter the alignment of a congruous metatarsophalangeal joint frequently limit its passive range of motion. An interview with the patient is important not only to evaluate the major symptoms associated with the hallux valgus deformity but also to educate the patient with regard to the problem, the alternatives for treatment, and the risks and complications when an operation is indicated. A patient's preoperative expectations play a major role in his or her
4 postoperative satisfaction. Relief of pain is frequently the major objective, an improved appearance of the foot and the ability to wear smaller or narrower shoes are frequent (and often unstated) goals as well. Mann et al. (94) reported that, while forty-four (59 per cent) of seventy-five patients were able to wear their choice of shoes after repair of a hallux valgus deformity, thirty-one (41 per cent) were not. It is important to educate the patient regarding the likely result of operative reconstruction as well as its limitations. Radiographic Examination Anteroposterior, lateral, and axial (sesamoid) radiographs should be made with the patient bearing weight. Evaluation of the radiographs includes measurement of the hallux valgus angle and the firstsecond intermetatarsal angle. The first metatarsophalangeal joint is evaluated for osteoarthrosis and congruity, and the distal metatarsal articular angle and the proximal phalangeal articular angle are measured. The size of the medial eminence and the magnitude of sesamoid subluxation are assessed. The alignment of the forefoot is evaluated for metatarsus adductus, and the hindfoot is inspected for pes planus or pes cavus. Decision-Making for Treatment Non-operative care is always the first option for a patient who has hallux valgus deformity. Often, pain, blistering, and bursal inflammation can be relieved by elimination of friction over the medial eminence. Evaluation of the patient's footwear may prove helpful for making recommendations for modifications or a change in size or style of the shoes. A wider toe box may reduce symptoms substantially (27). Stretching of areas of the shoe that cause increased pressure can result in complete relief of the symptoms overlying a painful bunion. A patient who has pes planus can be managed with an orthosis. A contracture of the Achilles tendon may be treated with stretching exercises or, sometimes, with lengthening of the Achilles tendon. Severe pes planus not only may be a factor in the etiology of hallux valgus but also may lead to recurrent deformity. On rare occasions, stabilization or realignment of the hindfoot may be necessary in conjunction with a bunion operation. Despite non-operative measures, some patients eventually need operative management. The patient should be counseled regarding the risks, complications, and expectations of the operation. Various magnitudes of deformity, different pathological elements, and anatomical abnormalities make it important for the surgeon to have several techniques of hallux valgus repair available. The selection of the specific procedure is often based on the severity of the hallux valgus deformity and the magnitude of the first-second intermetatarsal angle but may vary from surgeon to surgeon. Angular measurements provide only some of the indications for a particular procedure. The chosen operative technique must correct all elements of the problem: prominence of the medial eminence, increased valgus angulation of the proximal phalanx, an increased firstsecond intermetatarsal angle, congruency of the metatarsophalangeal joint, subluxation of the sesamoids, and pronation of the great toe. When operative treatment is planned, association of the main symptom with the physical findings as well as the radiographic information helps the surgeon to select the best procedure for correction of a hallux valgus deformity. Operative Correction The goal of operative treatment of hallux valgus is to correct all pathological elements and yet maintain a biomechanically functional forefoot. The vast number of operative techniques that have been described indicates that no one procedure is universally applicable for all deformities and that many procedures have serious shortcomings. The history and physical examination provide information regarding postural deformities, tendon contractures, neurological and vascular abnormalities, and the alignment and range of motion of the first ray. Radiographic evaluation demonstrates the congruency of the metatarsophalangeal joint, the magnitudes of the hallux valgus and first-second intermetatarsal angles, and the degree of any osteoarthrosis of the joint. If correction is to be successful, the choice of the operative technique must depend on the anatomical and pathological abnormalities that are present. Options include metatarsophalangeal soft-tissue reconstruction, osteotomy of the distal or proximal end of the metatarsal, osteotomy of the cuneiform, arthrodesis of the metatarsophalangeal joint, and excisional arthroplasty. Joint implants are not considered in this discussion, as I believe that they are rarely indicated in the treatment of hallux valgus, although some surgeons may consider them when there is concomitant hallux rigidus. If a joint replacement is performed in a patient who has osteoarthrosis of the metatarsophalangeal joint as well as hallux valgus, the first-second intermetatarsal and hallux valgus angles must be corrected adequately at the time of the arthroplasty (85). I believe that any attempt to use an implant to achieve angular realignment is associated with a high risk of postoperative failure. A combination of procedures may occasionally be necessary to obtain a successful result. The surgeon should be aware that any of these procedures may fail and that a reasonable method of salvage should be possible after a failed hallux valgus reconstruction. It is not the purpose of this review to discuss the operative technique of every bunion procedure but rather to present an approach to operative intervention that involves several different techniques. A mild hallux valgus deformity (89), with or without a congruous metatarsophalangeal joint, can be satisfactorily corrected with a chevron or Mitchell osteotomy. A distal soft-tissue reconstruction may be considered, in addition to these procedures, for a mild hallux valgus deformity with subluxation of the metatarsophalangeal joint. However, a distal softtissue reconstruction cannot be used to correct a
5 hallux valgus deformity with a congruous metatarsophalangeal joint, as an intra-articular realignment may create a non-congruous joint that is at risk for recurrence of the deformity or the development of degenerative osteoarthrosis (21,26). For a moderate hallux valgus deformity (89) with subluxation of the metatarsophalangeal joint, a Mitchell osteotomy may be considered; however, a distal soft-tissue reconstruction combined with an osteotomy of the proximal end of the metatarsal is more commonly performed. For a moderate hallux valgus deformity with degenerative changes of the metatarsophalangeal joint, an excisional arthroplasty or arthrodesis should be done. A moderate hallux valgus deformity with a congruous metatarsophalangeal joint is not common; however, when one is present, satisfactory correction may necessitate a Mitchell osteotomy or a double or triple osteotomy (an Akin osteotomy of the proximal phalanx combined with an osteotomy of the metatarsal and, on occasion, an additional osteotomy of the cuneiform) (23). A severe hallux valgus deformity (89) most commonly includes subluxation of the metatarsophalangeal joint. A distal soft-tissue reconstruction with an osteotomy of the proximal end of the metatarsal is frequently used to achieve correction. In the presence of hypermobility of the metatarsocuneiform joint, which typically is associated with subluxation of the metatarsophalangeal joint, a distal soft-tissue reconstruction should be combined with arthrodesis of the metatarsocuneiform joint. With osteoarthrosis of the metatarsophalangeal joint, an arthrodesis may be considered. A severe hallux valgus deformity with a congruous metatarsophalangeal joint is uncommon; however, when one is present, a double or triple osteotomy is the procedure of choice. Proximal Phalangeal Osteotomy (Akin Procedure) With the Akin procedure (1,8,88,109,126), correction of a hallux valgus deformity is achieved by resection of the medial eminence, medial capsular reefing, and a medial closing-wedge osteotomy of the proximal phalanx. An increased first-second intermetatarsal angle is not corrected with this operation. The indications for the Akin procedure include hallux valgus interphalangeus, mild hallux valgus without metatarsus primus varus, and mild hallux valgus with an enlarged medial eminence. In the presence of a congruous metatarsophalangeal joint with hallux valgus, a phalangeal osteotomy can be combined with a metatarsal osteotomy (8,102) in order to create an extraarticular realignment. Technique With the Akin technique (1,8,88,109,126), a longitudinal incision is centered over the medial eminence and extends from the interphalangeal joint to just proximal to the distal metaphysis of the metatarsal. Care is taken to protect the plantar and dorsal digital nerves within the skin flap. An L-shaped capsular flap is developed by reflection of the capsule from the medial eminence (88) (Fig. 12-A). The weakest capsular attachments on the dorsal and proximal aspects are released, and the stout plantar and distal attachments are left intact to provide a secure flap that can later be reattached. The medial eminence is resected with an oscillating saw along a line parallel with the medial border of the first metatarsal (Fig. 12-B). Usually, the resection is carried out just medial to the sagittal sulcus. If any portion of the sagittal sulcus remains, it should be beveled with a rongeur. The capsule is then repaired with interrupted absorbable sutures. A drill-hole may be placed in the medial aspect of the metatarsal metaphysis to anchor the capsular flap. An osteotomy is performed in the proximal metaphyseal region of the proximal phalanx. Care must be taken to protect the distal insertion of the metatarsophalangeal capsular attachment and to avoid penetration of the interphalangeal or metatarsophalangeal joint with the saw blade (102). Subperiosteal dissection is used to reflect tissue in the metaphyseal region dorsally, medially, and plantarly, but extensive soft-tissue dissection is avoided. An oscillating saw is used to remove a medially based wedge of bone from the metaphysis. The lateral cortex is left intact. The size of the medial wedge depends on the magnitude of either the proximal phalangeal articular angle or the hallux valgus angle. An adequate wedge is removed to achieve correction of the deformity; typically, the wedge measures to inch (0.318 to centimeter) at its base. The osteotomy site is closed by cracking the remaining lateral cortex and is stabilized with two inch (0.157-centimeter) Kirschner wires placed in an oblique fashion (Figs. 12-C and 12-D). Pronation of the great toe may be corrected at the time of the osteotomy by derotation of the toe (8). Postoperative Care A compression dressing is applied in the operating room and is changed weekly for six weeks. The patient is allowed to walk while wearing a postoperative shoe. The fixation pins are removed after four to six weeks. Walking is encouraged, and range-of-motion exercises of the metatarsophalangeal and interphalangeal joints are initiated six weeks after the operation, after use of the compression dressing has been discontinued. Results and Complications The Akin procedure achieves slight, if any, correction of the first-second intermetatarsal angle (35, 109) (Fig. 13-A). Plattner and Van Manen (109), in a series of twenty-two patients, initially found an average correction of the hallux valgus angle of 13 degrees. However, after long-term follow-up, at four and a half years, the hallux valgus angle was decreased only 6 degrees compared with the preoperative measurement. Seelenfreund and Fried (123) reported recurrence in eight (16 per cent) of fifty patients, and Goldberg et al. (35) reported recurrence in seventy-five (21 per cent) of 351 patients (Fig. 13-B). The use of internal fixation to stabilize the site of the osteotomy usually prevents malunion. Non-union
6 is uncommon (123). Although Colloff and Weitz (15) recommended the use of a lateral metatarsophalangeal capsular and adductor release, I do not advise this because of the increased chance of devascularization of the proximal phalangeal fragment. Other complications that can occur when the Akin procedure is used as a primary procedure include poor cosmetic appearance (35) and a high rate of postoperative dissatisfaction (35,109). Goldberg et al. (35) concluded that isolated phalangeal osteotomy as treatment for a hallux valgus deformity does not have a sound biomechanical basis and should not be performed as an isolated... procedure. Plattner and Van Manen (109) concluded that the major indication for the Akin procedure is hallux valgus interphalangeus and that the technique is not indicated for hallux valgus with subluxation of the metatarsophalangeal joint. Colloff and Weitz (15) as well as Mitchell and Baxter (102) suggested that a phalangeal osteotomy may be used in combination with a more proximal osteotomy to align a congruous metatarsophalangeal joint in the presence of hallux valgus and an increased first-second intermetatarsal angle. Distal Soft-Tissue Reconstruction The technique of distal soft-tissue reconstruction for correction of a hallux valgus deformity has been advocated by many authors (29,76-78,87,99) ; however, it was Silver (127) who popularized it by performing a medial capsulorraphy, a medial exostectomy, and a lateral capsular and adductor release. This technique was later modified by McBride (76-78), who advocated removal of the lateral sesamoid and transfer of the adductor tendon to the lateral aspect of the first metatarsal head. DuVries (29) and others (21,26,87,88,92) have modified the procedure so that the eponym McBride is no longer appropriate. Mann and Coughlin (87) and later Mann and Pfeffinger (92) reviewed the results of this procedure and recommended preservation of the fibular sesamoid because of the high rate of postoperative hallux varus when it was excised. The indication for a distal soft-tissue reconstruction is a non-congruous hallux valgus deformity (a subluxated metatarsophalangeal joint) of less than 30 degrees and a first-second intermetatarsal angle of less than 15 degrees. A fixed intermetatarsal angle prevents the achievement of a long-lasting distal correction and, therefore, the first metatarsocuneiform joint must have adequate mobility so that the first-second intermetatarsal angle can decrease after the operation. Technique This technique (29,87,92) involves a three-centimeter dorsal longitudinal incision centered over the first intermetatarsal space to expose the conjoined adductor tendon. The tendon is dissected from the lateral sesamoid. The distal part of the tendon is left attached to its insertion on the base of the proximal phalanx and the tendon is severed approximately 1.5 centimeters proximal to the musculotendinous junction, allowing the adductor hallucis muscle to retract (Fig. 14). The distal stump of the tendon is later sutured into the lateral aspect of the metatarsal capsule. The lateral sesamoid is freed of any lateral soft-tissue attachments, and the transverse intermetatarsal ligament is released. Care must be taken not to injure the common digital nerve directly beneath this ligament. Several stab wounds are made in the lateral aspect of the capsule with a number-11 knife blade to release it, and the remaining lateral part of the capsule is torn by abduction of the great toe. The purpose of this tearing technique is to leave some lateral capsular tissue that will heal to stabilize the metatarsophalangeal joint and to minimize the chance of a postoperative hallux varus deformity. Three interrupted absorbable 2-0 sutures are placed in the lateral aspect of the capsule of the metatarsophalangeal joint and the medial aspect of the capsule of the second metatarsophalangeal joint within the first intermetatarsal space. They are tied later to approximate the first and second metatarsophalangeal capsules. A longitudinal incision is then centered over the medial eminence, and the dissection is deepened to the metatarsophalangeal joint capsule. Care is taken to protect the dorsal and plantar digital nerves, which are contained in the skin flaps. An L-shaped capsular release (Fig. 12-A detaches the dorsal and proximal attachments, exposing the medial eminence. The medial eminence is resected in a line parallel with the medial diaphyseal cortex of the first metatarsal (Fig. 15). The cut is made without reference to the sagittal sulcus, although frequently (with mild and moderate deformities) it is approximately one to two millimeters medial to the sulcus. A drill-hole is then made in the medial aspect of the metaphysis of the first metatarsal, and the medial aspect of the capsule is secured with an absorbable suture. The distal stump of the adductor tendon is sutured into the lateral aspect of the capsule, and the three sutures that were previously placed in the first web space are tied to approximate the first and second metatarsophalangeal heads. Several sutures are placed medially in the proximal aspect of the capsule, incorporating the abductor hallucis tendon. The dorsal capsular incision is repaired with interrupted suture as well, and the skin is closed in a routine fashion. Postoperative Care A gauze-and-tape compression dressing is applied in the operating room and is changed weekly for eight weeks. The patient is allowed to walk in a postoperative wooden-soled shoe, with weightbearing as tolerated. Passive and active range-ofmotion exercises are initiated six weeks after the operation. Results and Complications Although Silver (127) advocated resection of the medial eminence and lateral soft-tissue release, he did not report the results of this procedure. Kitaoka et al. (63), in a review of the results of simple bunionectomy and medial capsulorraphy with or without lateral capsulotomy in thirty-three patients (forty-nine feet), found that at 4.8 years the average
7 hallux valgus angle had increased 4.8 degrees from the preoperative deformity and the first-second intermetatarsal angle had increased 1.7 degrees. Twenty-nine per cent of the feet that had had the bunionectomy without the lateral capsulotomy had had a reoperation at five years. The rate of failure was 24 per cent (twelve) for the entire group of forty-nine feet (63). Bonney and Macnab (6) reported generally poor results after simple exostectomy (Figs. 16-A and 16-B). Twenty-five (37 per cent) of their sixty-eight patients needed additional treatment, and the authors concluded that the only indication for a simple exostectomy is a large medial eminence that is the sole cause of symptoms in a patient whose general medical condition contraindicates an extensive procedure and to whom postoperative appearance is not important. Johnson et al. (56) and Meyer et al. (99) reported a high degree of clinical success in the treatment of mild-to-moderate hallux valgus with the modified McBride procedure. Mann and Coughlin (87), in a review of the results of 100 McBride procedures, found an average correction of the hallux valgus angle of 14.8 degrees and an average correction of the first-second intermetatarsal angle of 5.2 degrees. However, they recommended that if more than 20 degrees of correction of the hallux valgus angle is needed, this procedure should be combined with an osteotomy of the first metatarsal (87). Hallux varus is a serious complication of the McBride procedure. Mann and Coughlin (87) reported this complication in eleven of their 100 patients, although it was severe in only four. Mann and Pfeffinger (92) noted that the prevalence of hallux varus is higher after attempted correction of more severe deformities. They also reported that forty-three (91 per cent) of their fortyseven patients were satisfied with the result of the modified McBride procedure and there was no postoperative progression of the hallux valgus deformity at an average of four years. The limitations of an isolated distal soft-tissue reconstruction are substantial. Mann and Pfeffinger (92) concluded that a severe hallux valgus deformity was not well corrected by a distal softtissue reconstruction, as only approximately 50 per cent of the hallux valgus angle was corrected in such deformities. Therefore, I believe that the indications for a distal soft-tissue reconstruction are a hallux valgus angle of less than 30 degrees (with subluxation of the metatarsophalangeal joint) and an intermetatarsal angle of less than 15 degrees (Figs. 17-A and 17-B). Chevron Osteotomy The chevron procedure (a distal metatarsal osteotomy) is indicated for mild and some moderate hallux valgus deformities (a hallux valgus angle of less than 30 degrees and a first-second intermetatarsal angle of less than 13 degrees) with subluxation of the metatarsophalangeal joint (20,47,97). Because the chevron osteotomy achieves an extra-articular correction, it may also be considered for the treatment of a hallux valgus deformity with a congruous metatarsophalangeal joint if the distal metatarsal articular angle is not severe (15 degrees or less). With this procedure, a resection of the medial eminence, a distal metatarsal osteotomy, and a medial capsulorrhaphy are used to realign the great toe. A chevron osteotomy does not correct pronation of the great toe and only partially corrects subluxation of the sesamoids. This procedure is contraindicated for a severe hallux valgus deformity, for hallux valgus associated with degenerative osteoarthrosis, in the presence of a congruous metatarsophalangeal joint with a distal metatarsal articular angle of more than 15 degrees, and for patients who are more than sixty years old (43). The indications for this procedure when it is combined with a phalangeal osteotomy (49) include a hallux valgus deformity with a congruous metatarsophalangeal joint (a distal metatarsal articular angle of less than 20 degrees) and with pronation of the great toe. If residual valgus angulation of the great toe remains after a chevron osteotomy, an additional phalangeal osteotomy may help to improve alignment. Technique This technique (20,57) is done through a longitudinal incision centered over the medial eminence that is extended from the mid-portion of the proximal phalanx to a point proximal to the metaphysis of the first metatarsal. Care is taken to protect the dorsal and plantar cutaneous nerves in the skin flaps. The incision is carried directly down to the metatarsophalangeal capsule. An inverted L-shaped plantar and distally based capsular flap is developed to expose the medial eminence (20) (Fig. 12-A). The medial eminence is resected with an oscillating saw at a point just medial to the sagittal sulcus, in line with the medial border of the foot (Fig. 15). A transverse medial-to-lateral drill-hole is made in the center of the metatarsal head to mark the apex of the chevron osteotomy. An oscillating saw blade with very fine inline teeth (number or ; Stryker, Kalamazoo, Michigan) to minimize shortening is used to create a V-shaped osteotomy in the coronal plane (Fig. 18). Excessive dorsal or lateral penetration of the saw blade or excessive soft-tissue dissection may disrupt critical soft-tissue attachments and devascularize the metatarsal head. For this reason, a lateral soft-tissue release is discouraged (34, 47,54,57,83,124,146) (Fig. 19), although Hetherington et al. (46) and others (3,69,70,110,113) have performed lateral releases without complications. The shaft of the metatarsal is then grasped with a bone clamp, and the capital fragment is translated approximately four to five millimeters in a lateral direction (47,54) (Fig. 20-A). If additional medial angulation of the osteotomy is desired (to accommodate an increased distal metatarsal articular angle), more metaphyseal bone is resected medially, allowing the capital fragment to incline medially. The metatarsal head is then impacted on the proximal fragment and stabilized with a inch (0.157-centimeter) Kirschner wire (Fig. 20-B). Care is taken to avoid penetration of the sesamoid mechanism plantarly by the Kirschner wire. The prominent metaphyseal flare created by
8 displacement at the site of the osteotomy is then beveled with the oscillating saw. A drill-hole is made in the metaphysis, and the medial aspect of the capsule is anchored through this hole. Several interrupted absorbable sutures are used to complete the capsulorrhaphy. The skin is approximated in a routine fashion. Postoperative Care A gauze-and-tape compression dressing is applied in the operating room and is changed weekly for six weeks. The Kirschner wire is removed three to four weeks after the operation, and passive range-ofmotion exercises are initiated at this time. Weightbearing is allowed on the heel and the lateral aspect of the foot. At four weeks, plantigrade walking is allowed while the patient is wearing a wooden-soled postoperative shoe. If the site of the osteotomy is unstable, a below-the-knee weight-bearing cast is applied for three weeks or until adequate bonehealing has been documented radiographically. Results and Complications Johnson et al. (57) and others (43,47,69,110) have reported excellent results with this procedure. After a chevron osteotomy, the average correction of the hallux valgus angle has been reported to be 12 to 13 degrees (43,46,47,57,69,70,110) and the average correction of the first-second intermetatarsal angle has been 4 to 5 degrees (43,46,47,57,69,70,110). Because of the limited correction of the hallux valgus, the chevron procedure is reserved for mild and some moderate deformities. Expansion of the indications for this procedure to more severe deformities appears to increase the risk of complications and patient dissatisfaction. Meier and Kenzora (97), in a series of fifty patients (seventy-two feet) who had had an osteotomy of the distal end of the metatarsal, noted a rate of satisfaction of 74 per cent when the preoperative first-second intermetatarsal angle had been more than 12 degrees and a rate of 94 per cent when the intermetatarsal angle had been 12 degrees or less. The most frequent complications associated with this procedure are recurrence or undercorrection of the deformity (four of twenty-nine feet, 14 per cent (70) ; eight of seventy-eight feet, 10 per cent (47) ; and thirty of 300 feet, 10 per cent (3) ). Hallux valgus may recur when the indications for the chevron procedure are expanded to include more severe deformities. Loss of correction (overcorrection or undercorrection) can be caused by slippage at the site of the osteotomy (47,97). While internal fixation was not advocated originally by Austin and Leventen (3) or by others (16,69,146), its use decreases the possibility of postoperative displacement of the capital fragment (57,110) (Figs. 21-A and 21-B). Shortening may occur as a result of excessive bone loss (3,47,83,97), and Klosok et al. (65) reported a postoperative transfer lesion in five (12 per cent) of forty-three feet and postoperative metatarsalgia in ten (43 per cent) of twenty-three patients. The most serious complication following this procedure is avascular necrosis of the first metatarsal head (Figs. 22-A and 22-B). Meier and Kenzora (97) reported that avascular necrosis developed in 20 per cent (twelve) of sixty feet after a chevron osteotomy, and this rate increased to four of ten feet when the osteotomy had been combined with an adductor tenotomy. Horne et al. (50) reported avascular necrosis in 12 per cent (nine) of seventy-six feet, and Mann (83) as well as others (53,145) reported several isolated cases of partial and whole-head avascular necrosis after osteotomy of the distal end of the metatarsal. In contrast, Johnson et al. (57) and others (3, 65,110) reported no evidence of avascular necrosis after osteotomy. Hattrup and Johnson (43) as well as Shereff et al. (124) cautioned that lateral release increases the risk of avascular necrosis. Release of the lateral structures may enable greater correction, but I believe that the risk of avascular necrosis is indeed increased (53,69,97,146). Distal Metatarsal Osteotomy (Mitchell or Wilson Osteotomy) Correction of a hallux valgus deformity through an osteotomy of the distal end of the first metatarsal was reported first by Reverdin (114), in 1881, and later by Hohmann (49) and by Peabody (106), who described variations in the technique. It was Mitchell (44,101) who popularized the technique of biplanar osteotomy of the distal end of the metatarsal, which achieves lateral and plantar displacement as well as shortening of the first metatarsal. Wilson (147) and others (37,103,121,138) have described an oblique metaphyseal osteotomy in this same region. Variations in the technique have included changes in the capsulorrhaphy (9,100,103,121), the metaphyseal osteotomy (100,103,121,138,147,150,151), the use of internal fixation (9,98,103,121,132,150,151), and the postoperative care (9,103,132). These many changes make the eponym Mitchell inadequate to describe the procedure as performed in many series. Indications for a transverse or oblique osteotomy of the distal end of the metatarsal include moderate hallux valgus with subluxation of the metatarsophalangeal joint; however, if the distal metatarsal articular angle is not severe (if it is less than 15 degrees), this distal metatarsal osteotomy is still indicated. The upper limits for deformity are a hallux valgus angle of 35 degrees and a first-second intermetatarsal angle of 15 degrees. Contraindications include a hallux valgus deformity with concurrent degenerative osteoarthrosis, a short first metatarsal, lateral metatarsalgia, and a congruous metatarsophalangeal joint with a distal metatarsal articular angle of more than 15 degrees. Technique A longitudinal skin incision is centered over the dorsomedial aspect of the first metatarsophalangeal joint and extends from the mid-portion of the proximal phalanx to the mid-portion of the first metatarsal. A distally based capsular flap (9) or a V-Y capsular flap (101) is created over the medial aspect of the metatarsophalangeal joint. The adductor tendon and lateral capsular attachments are not disturbed, in order to protect the vascularity of the metatarsal head (97). The medial eminence is exposed and
9 osteotomized in line with the shaft of the first metatarsal. Two dorsal-to-plantar drill-holes are made in the distal end of the metatarsal. The first hole, 1.5 centimeters proximal to the articular surface, is made near the medial cortex, and the second hole, 2.5 centimeters proximal to the articular surface, is made nearer to the lateral cortex. The drill-holes are positioned so that they will line up as the capital fragment is shifted laterally. An incomplete osteotomy is performed two centimeters proximal to the articular surface of the metatarsal, midway between the two drill-holes (Fig. 23-A). The distal cut is made partway through the shaft, with the depth depending on the desired width of the lateral shelf. The second osteotomy cut is made completely through the metatarsal, approximately two millimeters proximal to the initial cut and diverging plantarward, with removal of approximately one to two millimeters more bone on the plantar aspect (Fig. 23-B). The magnitude of the deformity (the first-second intermetatarsal angle) determines both the amount of longitudinal shortening to be achieved at the site of the osteotomy and the width of the incomplete osteotomy. With a moderate deformity, a lateral shelf one-sixth the width of the shaft is left on the distal fragment. With a severe deformity, a lateral shelf onethird the width of the shaft should remain. The capital fragment is then displaced four to five millimeters laterally until the lateral shelf locks over the lateral aspect of the proximal part of the shaft (Fig. 23-C). Care is taken to ensure that the capital fragment either is angulated plantarward approximately 10 degrees or is displaced plantarward two to three millimeters. With lateral sloping of the distal metatarsal articular angle, more bone can be resected medially (Fig. 23-D) to rotate the articular surface perpendicular to the long axis of the first metatarsal. The site of the osteotomy then is stabilized with a circumferential suture placed through the now-parallel drill-holes and tied dorsally (44,101,150,151) or is fixed with Kirschner wires (98,103,132), staples (9), or screws (150,151). The remaining medial metaphyseal flare created by lateral displacement of the capital fragment is removed with a power saw, and the metaphyseal capsule is plicated with interrupted sutures. The skin is closed in a routine fashion. Postoperative Care A gauze-and-tape compression dressing is applied in the operating room (9). A non-weight-bearing cast typically is applied a week after the operation. Most surgeons prefer a four-week course of non-weightbearing, after which walking is permitted with the foot immobilized in a below-the-knee cast until the site of the osteotomy has healed at eight to ten weeks postoperatively. Results and Complications Over-all, distal metatarsal osteotomies have resulted in satisfactory correction of the hallux valgus deformity in 82 to 97 per cent of feet (5,11,34,44,101,150, 151) (Figs. 24-A and 24-B). In the two larger series, 185 (91 per cent) of 204 patients (5) and 182 (97 per cent) of 188 patients (44) were satisfied with the result of the procedure. The average reported correction of the hallux valgus deformity has ranged from 10 to 25 degrees (5,9,34,62,150,151) and the average correction of the first-second intermetatarsal angle, from 5 to 10 degrees (5,9,34,44,62,150,151). These results are consistent with those of Jahss et al. (54), who estimated that an average of 4.3 degrees of correction of the intermetatarsal angle could be achieved with a distal metatarsal osteotomy. Shortening of the first metatarsal is an important part of this procedure as it helps to correct the deformity. However, excessive shortening is a frequent complication, which is undesirable as it may lead to transfer metatarsalgia (44). Merkel et al. (98) reported an average shortening of seven millimeters in their series; however, patients who had more than ten millimeters of shortening had a higher degree of dissatisfaction and an increased frequency of metatarsalgia. Lateral metatarsalgia and callus are the most frequently recognized complication and have been reported in almost all series in which distal osteotomy has been performed (11,34,44,62,100,101,121,147). Rates of 20 to 40 per cent have been reported (44,62, 101), with a 31 per cent rate (fifty-nine of 188 feet) in the largest series (44). While some calluses are asymptomatic, they may become painful in time. Plantar displacement, as advocated by Mitchell et al. (101) and by others (5,34,44), and plantar angulation, as recommended by Wu (150,151) and by Merkel et al. (98), have both been proposed to diminish the ill effects of shortening of the first metatarsal. Glynn et al. (34) stressed that failure to depress the capital fragment eventually predisposes to metatarsalgia. Dorsal angulation (9,98,150,151) is associated with patient dissatisfaction as it magnifies the effects of shortening of the first metatarsal. Undercorrection and recurrence of the deformity are also recognized as common complications following this osteotomy. Such complications have been reported in approximately 10 per cent of patients (5,34,44,100,101,150,151), with six of the series including at least 100 patients. The use of a distal metatarsal osteotomy for more severe deformities increases the risk of undercorrection or recurrence. Mitchell et al. (101) and others (11,37,53,83,97,121) have reported avascular necrosis after distal metatarsal osteotomy. Wu (150,151) mentioned the occasional use of lateral capsular and adductor release in combination with such an osteotomy, but Carr and Boyd (11) as well as others (44,101,138) recommended avoidance of a lateral capsular release to minimize this problem. The nature of this transverse osteotomy makes it relatively unstable, and loss of correction (62,76), malunion (9,150,151), delayed union (98,100,101), and nonunion (98) have all been reported. The technique is demanding (150,151) and this may be one reason for the high prevalence of complications, which has led to less frequent use of this procedure in favor of others. Distal Soft-Tissue Reconstruction with Osteotomy of the First Metatarsal
10 The primary indication for a distal soft-tissue reconstruction combined with a proximal osteotomy of the first metatarsal is a moderate or severe hallux valgus deformity (a hallux valgus angle of at least 35 degrees and an intermetatarsal angle of at least 15 degrees) with subluxation of the metatarsophalangeal joint (88,89). Techniques of proximal osteotomy of the first metatarsal include an opening-wedge (6,71,122,129), closing-wedge (112,122,142), proximal chevron (119), and crescentic osteotomy (22,23,72,85,89,94,135). Although an opening or closing-wedge osteotomy may be performed, substantial lengthening or shortening of the first ray is usually not necessary. In a study of more than 7000 feet, Harris and Beath (41) reported that, in most feet, the lengths of the first and second metatarsals were either equal or within a few millimeters of one another. Thus, I usually prefer a proximal crescentic osteotomy. Contraindications to this procedure include a congruous metatarsophalangeal joint (a distal metatarsal articular angle of more than 15 degrees) (22,71,135), degenerative osteoarthrosis of the first metatarsophalangeal joint (22,135), and severe metatarsus adductus (22). Technique With this technique (22,71,94), a three-centimeter dorsal longitudinal incision is centered over the proximal part of the first metatarsal medial to the extensor hallucis longus tendon and is deepened to the shaft of the first metatarsal. The metatarsocuneiform joint is identified. The crescentic osteotomy is performed 1.0 to 1.3 centimeters distal to the metatarsocuneiform joint with a curved saw blade (number ; Zimmer, Warsaw, Indiana, or number or ; Stryker). The osteotomy is directed in a dorsal-toplantar direction at a 120-degree angle with the shaft of the first metatarsal (Fig. 25). Care is taken to avoid either medial or lateral deviation of the saw blade as it may lead to plantar flexion or dorsiflexion at the site of the osteotomy (72). The orientation of the osteotomy may be concave distal (22,84) or concave proximal (94). The proximal fragment is rotated medially and the distal fragment is rotated laterally for approximately two to three millimeters, decreasing the first-second intermetatarsal angle. Care must be taken not to overcorrect the deformity. The osteotomy is fixed with both a inch ( centimeter) Kirschner wire and a small-fragment compression screw to provide compression as well as rotational stability (Fig. 26). A distal soft-tissue reconstruction is then performed as described previously. Intraoperative radiographs are made to evaluate the correction of the first-second intermetatarsal angle, the placement of the internal fixation, and the alignment of the metatarsophalangeal joint (Figs. 27-A and 27-B). Postoperative Care The foot is placed in a gauze-and-tape compression dressing in the operating room, and the dressing is changed weekly. Weight-bearing on the heel and lateral aspect of the foot is initially allowed with the patient wearing a wooden-soled postoperative shoe. The foot is rarely immobilized in a cast. Metatarsophalangeal range-of-motion exercises are initiated three to four weeks after the operation, while the foot is still maintained in the dressing. The internal fixation hardware is routinely removed six weeks after the operation in an outpatient or office setting with the patient under local anesthesia. An intensive walking program is begun at seven to eight weeks. Results and Complications The reported rate of patient satisfaction with this combined procedure (12,94,112,119,129,135) has ranged from 78 per cent (forty of fifty-one feet (119) ) to 93 per cent (forty-three of forty-six feet (135) ), with a 92 per cent rate (100 of 109 feet) in the largest series (94). The average correction of the hallux valgus angle has been consistently reported to be 23 or 24 degrees (23, 84,94,135). The degree of improvement is directly proportional to the severity of the preoperative deformity, and Mann (85) noted that, for more severe deformities (a hallux valgus angle of more than 40 degrees), the average correction was 30 degrees. The correction of the first-second intermetatarsal angle has averaged 8 to 11 degrees (23,84,94,135) after a crescentic osteotomy, 3 to 6 degrees (112,122,142) after a closing-wedge osteotomy of the proximal end of the metatarsal, and 7 degrees (71,129) after an openingwedge osteotomy. Wanivenhaus and Feldner-Busztin (142) reported an average shortening of the first metatarsal of 3.6 millimeters after a closingwedge osteotomy, and shortening of the first metatarsal has been reported by other authors as well (12,112,122,142). Shortening or dorsiflexion as the site of the osteotomy is closed predisposes to the development of lateral metatarsalgia (85,112). I prefer a crescentic osteotomy because it results in minimum shortening (84,89). Lengthening of the first metatarsal through an opening-wedge osteotomy (6,71, 122,128) may lead to instability as well as malunion at the site of the osteotomy. An opening-wedge osteotomy also lengthens the adjacent soft tissues, which may increase tension on an already tight metatarsophalangeal joint and lead to recurrence (85, 122) Ċomplications with this procedure include recurrence or undercorrection of the deformity (22,23, 119,122,129), overcorrection (hallux varus) (22,23,94,135), inadequate or failure of the internal fixation (22,94), shortening (94,112), metatarsalgia (94,135), delayed union (22,119), and malunion (72,119,135) (Fig. 28). Overcorrection frequently has been associated with lateral sesamoidectomy. Simmonds and Menelaus (129) and later Mann and Coughlin (87) cautioned that the sesamoid should rarely, if ever, be removed. Retention of the sesamoid when possible decreased the prevalence of hallux varus in one series from eleven (11 per cent) of 100 patients (87) to six (8 per cent) of seventy-two patients (94). Many postoperative hallux varus deformities of less than 10 degrees are asymptomatic and do not preclude a satisfactory result (135). The deformity may recur for a variety of reasons. A
11 distal soft-tissue reconstruction should be avoided in the presence of a congruous metatarsophalangeal joint because it will probably lead to recurrence. Meticulous attention to operative technique may reduce the prevalence of malunion. Lippert and McDermott (72) stressed the importance of correct positioning of the saw blade to avoid a dorsiflexion malunion (with medial rotation of the saw blade) or a plantar-flexion and supination malunion (with lateral rotation of the saw blade). Thordarson and Leventen (135) emphasized that adequate internal fixation is the most important factor in the avoidance of a dorsiflexion malunion and the lateral metatarsalgia that accompanies it. Mann et al. (94) noted dorsiflexion at the site of the osteotomy in 28 per cent (thirty) of 109 feet, but they had used a single Steinmann pin for internal fixation. The use of screws (135) or screws and Kirschner wires (22) appears to increase the stability of the osteotomy site, and Thordarson and Leventen documented less shortening with a more stable construct. Malunion can be extremely difficult to treat and may necessitate a complex and extensive salvage procedure that involves a osteotomy down and a distal soft-tissue realignment. Use of intraoperative radiographs may help to diminish malalignment. A proximal metatarsal osteotomy combined with a distal soft-tissue reconstruction is technically demanding. In the treatment of moderate and severe hallux valgus deformities with subluxation of the metatarsophalangeal joint, meticulous attention to operative technique coupled with careful preoperative planning can minimize postoperative complications Arthrodesis of the Metatarsocuneiform Joint (Modified Lapidus Procedure) Arthrodesis of the first metatarsocuneiform joint can be combined with a distal soft-tissue realignment at the metatarsophalangeal joint to correct a hallux valgus deformity. On occasion, with a congruous metatarsophalangeal joint, a phalangeal osteotomy may be combined with the arthrodesis to achieve an extra-articular correction (105). The major indication for this procedure is a moderate or severe hallux valgus deformity (a hallux valgus angle of at least 30 degrees and an intermetatarsal angle of at least 16 degrees (105) ) with subluxation of the metatarsophalangeal joint associated with hypermobility of the metatarsocuneiform joint (120) or generalized ligamentous laxity (105). It is also used as a salvage procedure after a failed repair of hallux valgus (105,120). Contraindications include a short first ray, juvenile hallux valgus with an open epiphysis, a moderate hallux valgus deformity without excessive hypermobility of the metatarsocuneiform joint, and degenerative osteoarthrosis of the metatarsophalangeal joint (80). Technique A distal soft-tissue reconstruction, as described earlier, is routinely performed in conjunction with the arthrodesis of the metatarsocuneiform joint. The joint is then exposed through a three-centimeter dorsal longitudinal incision just medial to the extensor hallucis longus tendon. A biplanar joint resection is performed to lateralize the first metatarsal, decrease the first-second intermetatarsal angle, and flex the first ray plantarly to diminish the prevalence of lateral metatarsalgia (Figs. 29-A and 29-B). Meticulous preparation is necessary to ensure a successful arthrodesis. Excessive resection of bone is avoided as it may destabilize the metatarsocuneiform joint, increasing the chance of malunion. The metatarsal should be aligned in neutral rotation in relation to the first cuneiform. A cancellous-bone graft (120) obtained from the distal tibial metaphysis, the iliac crest, or the calcaneus is added to the site of the arthrodesis to promote healing. Internal fixation is an important aspect of the arthrodesis. Lapidus (67) recommended a heavy suture to secure the site of the arthrodesis; however, compression of the arthrodesis site with 3.5- millimeter fully threaded lag screws or 4.0-millimeter cancellous-bone screws is preferred. The first screw is introduced from the dorsal aspect of the base of the first metatarsal, 1.5 centimeters distal to the site of the arthrodesis, and is directed at a 45-degree angle into the first cuneiform. Care must be taken not to fracture the dorsal medial cortex or to depress the shaft of the first metatarsal excessively as the screw is tightened. A second screw is directed from the dorsal aspect of the first cuneiform distally into the first metatarsal. An optional third screw may be placed from the base of the first metatarsal into the second metatarsal. After adequate stabilization and alignment of the metatarsocuneiform joint is confirmed with intraoperative radiographs or fluoroscopy, the wound is closed in a routine fashion. Postoperative Care A gauze-and-tape compression dressing is applied in the operating room and is changed twenty-four hours after the operation, at which point a below-theknee non-weight-bearing cast is applied. At four weeks, the cast is changed and weight-bearing is permitted (120). Immobilization in a cast is continued until radiographic confirmation of fusion has been obtained. The hardware may be removed at twelve to sixteen weeks after the arthrodesis, when radiographs show that fusion has occurred (Figs. 30-A and 30-B). Results and Complications In 1934, Lapidus (67) described arthrodesis of the first and second metatarsocuneiform joints combined with a distal soft-tissue reconstruction for the treatment of hallux valgus. Neither that report nor a follow-up report (68) contained any analysis of the results of the procedure. Mauldin et al. (96) as well as others (105,120) modified this procedure so that the second metatarsal is no longer included in the arthrodesis. Mauldin et al. (96), Myerson (105), and Sangeorzan and Hansen (120) reported rates of patient satisfaction with the result of this procedure ranging from 75 per cent (twenty-one of twenty-eight feet (120) ) to 90 per cent (forty-six of fifty-one feet (96) ). These authors reported an average correction of the hallux valgus angle of 18 degrees (96,105) and an average correction of the first-
12 second intermetatarsal angle of 6 to 8 degrees (96,105, 120) Ṡangeorzan and Hansen (120) as well as Myerson (105) observed prolonged swelling and a lengthy convalescent period after this procedure, compared with the findings after other bunion operations. Sangeorzan and Hansen also reported that only twelve (43 per cent) of twenty-eight feet were pain-free at the time of long-term follow-up. High rates of non-union (10 and 12 per cent) at the site of the arthrodesis have been reported (105,120), and Mauldin et al. (96) confirmed fusion radiographically in only thirteen (25 per cent) of fifty-one feet. Rigid internal fixation and bone-grafting appear to reduce the prevalence of complications. Fixation with screws, as observed by Sangeorzan and Hansen, maintains position but is quite unforgiving [and the] metatarsal must be positioned exactly at the time of surgery. Inadequate preparation of the joint surfaces or inadequate internal fixation may lead to malposition at the site of the arthrodesis. Sangeorzan and Hansen (120) reported that five (13 per cent) of forty feet needed operative revision. The over-all rate of failure in their study was eight (20 per cent) of forty feet. Excessive plantar flexion may lead to an intractable plantar keratosis beneath the first metatarsal, and excessive dorsiflexion may lead to lateral metatarsalgia. If a hallux valgus deformity is associated with shortening of the first ray or if the arthrodesis creates shortening without compensatory plantar flexion of the first ray, lateral metatarsalgia may be a serious problem. Myerson (105) noted that six (10 per cent) of sixty-two metatarsals were fused in dorsiflexion, and three of these resulted in a transfer lesion or lateral metatarsalgia. Undercorrection may lead to recurrent hallux valgus, while overcorrection may actually create a negative intermetatarsal angle with subsequent hallux varus (10). Postoperative hallux varus was reported in eight (16 per cent) of fifty-one feet by Mauldin et al. (96), a rate similar to that reported by Mann and Coughlin (87) after distal softtissue reconstruction alone. Sangeorzan and Hansen (120) believed that the frequent failures of this procedure can be attributed to its technical complexity, and they concluded that the procedure should be reserved for hallux valgus deformities with hypermobility of the first ray (64,89, 105,143) and recurrent deformity in young adults or adolescents. Arthrodesis of the First Metatarsophalangeal Joint Arthrodesis of the first metatarsophalangeal joint is recommended as a salvage procedure for various conditions, including severe hallux valgus (73,90,91), recurrent hallux valgus (90,136), rheumatoid arthritis (73, 86,91,93,140,144), hallux rigidus (31,42,55,90,134,136,140), previous infection (134), traumatic osteoarthrosis (55), and hallux valgus associated with a neuromuscular disorder (90,91,136). This arthrodesis was initially described by Clutton (14), various approaches, techniques for preparing the joint, and methods of internal fixation have been described in an effort to improve the success rate of the procedure. Flat surfaces have been advocated because of the simplicity of preparation (42,86,91,93,104,137) ; however, creation of a flat surface requires precision to achieve the desired alignment in all planes. Attempts to vary alignment in one plane intraoperatively may simultaneously affect alignment in another, creating an undesirable effect. The difficulty in achieving acceptable triplanar alignment at the site of the arthrodesis led Lipscomb (73) and others (4,33,79,104,111, 112,134,140,144,148) to curve and contour the surfaces of the bone to enable adjustment of the alignment before placement of the internal fixation device. Later, cannulated cup-shaped power reamers were introduced to create congruous arthrodesis surfaces (18,19,24). Both flat (42,86,91,93,104,137) and curved surfaces (4,79,111,112,117,144) have yielded relatively high rates of fusion. Various internal fixation devices have been used, including compression screws (4,55,73,79,104, 111,144), Steinmann pins (25,90,91,93), Kirschner wires (33), staples (86), and compression plates (18,19,24,140). Contraindications to arthrodesis of the first metatarsophalangeal joint include active infection, substantial osteoarthrosis of the interphalangeal joint (4,55,95,140), and severe osteoporosis (112). Technique With this technique (18,19,24,79), a dorsal longitudinal incision is centered over the first metatarsophalangeal joint on the medial aspect of the extensor hallucis longus tendon. When necessary, the tendon is divided to aid exposure. The dissection is deepened to the metatarsophalangeal joint, and the capsular structures are released. An oscillating saw is used to resect the medial eminence and the articular surfaces of the base of the proximal phalanx and the first metatarsal head (Fig. 31). The amount of bone resected determines the eventual length of the ray. Preparation of the joint surfaces for arthrodesis is critical to achieve proper alignment (18). I prefer to use cup-shaped power reamers for this purpose. The concave female reamer shapes the metatarsal head into a convex hemisphere (Fig. 32-A), and the phalangeal reamer is used to excavate the base of the proximal phalanx (Fig. 32-B). (Numbers , , and reamers [Howmedica, East Rutherford, New Jersey] are used.) After preparation, the surfaces are coapted (Fig. 32-C) in the desired alignment (15 to 20 degrees of valgus, 20 to 30 degrees of dorsiflexion, and neutral rotation) and are temporarily stabilized with a Kirschner wire. A small or minifragment plate is bent to the desired angle of dorsiflexion, positioned on the dorsal aspect of the phalanx and metatarsal, and secured with bicortical screws (Figs. 33-A and 33-B). The Kirschner wire is then removed, an oblique screw is introduced at the base of the proximal phalanx, and the screw is driven in a proximal-lateral direction across the site of the arthrodesis. The position of the arthrodesis should be confirmed with intraoperative radiographs. The extensor hallucis longus is repaired if necessary, and a routine capsular and skin closure is performed. Postoperative Care
13 A gauze-and-tape compression dressing is applied in the operating room and is changed weekly. Walking is initiated with the patient wearing a postoperative shoe, with weight-bearing on the heel and lateral aspect of the foot. Alternatively, the foot may be immobilized in a cast. The first ray is protected until adequate union is demonstrated radiographically, usually at eight to twelve weeks postoperatively. Results and Complications The rate of fusion varies substantially depending on the operative technique, the method of internal fixation, and the preoperative diagnosis. Reported rates of success have ranged from 77 to 100 per cent (4,25,30,33,42,51,55,79,91,93,111,117,136,137,140,144,148), with an average rate of 90 per cent (18). The rate of success in the largest series (117) was 91 per cent (281 of 309 procedures). With use of a dorsal compression plate, the reported rate of successful fusion (19,24 82,140) has ranged from 92 per cent (forty-seven of fifty-one procedures (82) ) to 100 per cent (thirty-five of thirtyfive procedures (19) ). Coughlin and Abdo (24) reported a subjective good or excellent result in 93 per cent (fifty-four) of fifty-eight feet. While inadequate fixation is the most frequent cause of non-union (33, 112,137), failure of the internal fixation is uncommon (117) and an unsuccessful arthrodesis or a pseudarthrosis may still lead to a painless and acceptable result (79) (Figs. 34-A and 34-B). The achievement of good alignment at the site of the arthrodesis is critically important for ultimate patient satisfaction. Recommendations for alignment in the frontal plane have ranged from 5 to 30 degrees of valgus (10,25,30,31,93,95,111,117), with an average of 15 degrees (18,19,24,91). After arthrodesis of the metatarsophalangeal joint, a widened first-second intermetatarsal angle associated with severe hallux valgus deformity is usually reduced (51,73,79,90,104,111, 117) (Figs. 35-A and 35-B), and only rarely is an additional metatarsal osteotomy necessary (42,51,90). Fitzgerald (30) cautioned that arthrodesis in less than 20 degrees of valgus is associated with a threefold increase in the prevalence of osteoarthrosis of the interphalangeal joint. Recommendations for alignment in the sagittal plane have ranged from 10 to 40 degrees of dorsiflexion (24,25,55,91,93,95,104,111,117,134, 137,140) (in relation to the shaft of the first metatarsal), with 20 to 25 degrees being the most commonly recommended position (18). Excessive plantar flexion leads to pressure beneath the tip of the toe while excessive dorsiflexion frequently leads to an intractable plantar keratosis beneath the sesamoids. Malunion in any plane, however, is poorly tolerated and underscores the necessity of meticulous attention to the final position of the arthrodesis. No bunion procedure requires a technique that is more exacting and unforgiving than that required in arthrodesis of the first metatarsophalangeal joint. When an arthrodesis is combined with resection arthroplasties of the metatarsophalangeal joints of the lesser toes, shortening of the first ray is not a problem. When only the first ray is operated on, slight shortening is of little consequence; however, marked shortening may be unacceptable, particularly from a cosmetic standpoint (24,91). The use of a dorsal compression plate is relatively easy and is associated with high rates of fusion and patient satisfaction. One major concern is that the plate, from a mechanical standpoint, is on the compression surface rather than the tension surface. I have not found this to be a problem. While bulky mini-fragment stainless-steel plates usually have to be removed (19,82,140), the low-profile Vitallium plate that I currently use usually does not (24). Alternatively, others have found that fixation with compression screws also offers a reliable means of internal fixation with a high degree of patient satisfaction (55). The operative technique should be easy to perform and should achieve a predictable result. The shaping of congruous cancellous surfaces that allow easy adjustment to the desired position (varus and valgus angulation, dorsiflexion and plantar flexion, and rotation) and the use of rigid internal fixation are both important factors in achieving and maintaining position while attaining a high rate of osseous fusion. However, as McKeever (79) stated: It is the [fusion] and its position that is important and not the method by which it is produced. Excisional Arthroplasty The Keller excisional arthroplasty is indicated for moderate hallux valgus deformities (a hallux valgus angle of less than 30 degrees) associated with degenerative osteoarthrosis of the metatarsophalangeal joint in older, more sedentary patients who have limited expectations with regard to walking (139). The procedure is contraindicated in young, active individuals (75) ; older patients in whom function of the first metatarsophalangeal joint should be preserved; and patients who have a severe deformity and who consider subtotal correction unacceptable. With this technique, a resection of the medial eminence, partial proximal phalangectomy, and medial capsular plication are used to realign the great toe (58,88,115,141). Often considered a salvage procedure, the technique involves resection of as much as one-third of the proximal aspect of the proximal phalanx to decompress the metatarsophalangeal joint (139,149). Technique With this technique (60,88,115,141), a medial longitudinal skin incision is centered over the metatarsophalangeal joint and extends from the interphalangeal joint to a point proximal to the medial eminence. A proximally based capsular flap is developed by detaching it from the base of the proximal phalanx, exposing the medial eminence. The base of the proximal phalanx is exposed by a subperiosteal dissection. The medial eminence is excised with a power saw in line with the medial border of the foot. Any remaining osteophytes in the area of the sagittal sulcus are removed with a rongeur. The proximal fourth of the proximal phalanx is then osteotomized at the level of the metaphyseal flare with an oscillating saw, is carefully released from the plantar plate, and is removed (115) (Figs. 36-A and
14 36-B). Two drill-holes are made plantarly in the diaphyseal portion of the remaining proximal phalangeal segment, and the plantar plate with the attached sesamoids and intrinsic muscles is sutured to the base of the phalanx with interrupted nonabsorbable sutures (141) (Fig. 36-C). The joint is then stabilized with one or two inch ( centimeter) Kirschner wires (115,133,139) introduced at the joint, drilled distally, and then drilled in a retrograde direction into the metatarsal head. The pins are bent at the tip of the toe to prevent proximal migration. The medial part of the capsule is then reattached to the proximal phalanx with interrupted absorbable sutures. The wound is closed in a routine fashion. Postoperative Care The foot is placed in a gauze-and-tape compression dressing in the operating room. The dressing is changed weekly for six weeks. Walking with weightbearing is permitted with the patient wearing a wooden-soled shoe. The Kirschner wires are removed four weeks after the operation, at which point metatarsophalangeal range-of-motion and plantarflexion exercises are initiated (115). Results and Complications After excisional arthroplasty, the hallux valgus angle is usually reduced approximately 50 per cent or less (81,138,139), and the intermetatarsal angle is not changed much at all (118,138) (Figs. 37-A, 37-B, and 37-C). Satisfactory results occur more often when the hallux valgus angle is less than 30 degrees because correction can be obtained with removal of less than one-third of the proximal phalanx. Pain is reduced with decompression of the osteoarthrotic joint. Pain from a prominent medial eminence is reduced as well, and frequently this allows the patient to wear more comfortable shoes. Reported rates of subjective satisfaction (13,75,139,149), as judged mainly on the basis of relief of bunion-related pain and not on the basis of the absence of metatarsalgia, have ranged from 72 per cent (thirty-nine of fifty-four feet (149) ) to 96 per cent (157 of 163 feet (13) ). Bonney and Macnab (6) observed that functional results may deteriorate with time. Rogers and Joplin (118) reported generally poor results with this procedure, noting marked objective improvement in five (9 per cent) of fifty-five feet, no change in thirty-nine feet (71 per cent), and postoperative deterioration in eleven feet (20 per cent). Henry and Waugh (45) documented that the inability of the great toe to bear weight postoperatively is associated with metatarsalgia. Coughlin and Mann (25) as well as others (13,45,58,115,118,138,149) reported postoperative metatarsalgia as a frequent complication following a Keller procedure. While excision of at least one-half of the phalanx has been recommended (6,13,58), Vallier et al. (139) and Wrighton (149) reported that limited phalangeal resection is associated with a higher rate of postoperative satisfaction. Henry and Waugh noted an association between an increased phalangeal resection and increased weight-bearing on the lateral part of the forefoot as well as increased lateral metatarsalgia. Weight-bearing on the great toe was noted in twenty-four (73 per cent) of the thirty-three feet from which one-third or less of the proximal phalanx had been resected, while it was noted in only nine (19 per cent) of the forty-seven feet from which more than one-third of the proximal phalanx had been resected (45). With more severe deformities, there is a tendency to resect a larger amount of the proximal phalanx in order to correct the hallux valgus. Vallier et al. stressed that this tendency may lead to a short, flail, functionless great toe. Besides postoperative metatarsalgia, which has been reported in almost all series (13,35,43,115,118,125,139, 149), other complications include a cock-up deformity of the great toe (25,75,81,118,138) (Figs. 38-A and 38-B); stiffness of the interphalangeal joint (25,45) ; and marked shortening (25,45), impaired control and function (25,45, 149), and diminished flexor strength (25,81,125,138,139) of the great toe. Because of the high frequency of incomplete correction and associated postoperative metatarsalgia, excisional arthroplasty of the first metatarsophalangeal joint is recommended for elderly, low-demand patients who have osteoarthrotic changes of that joint in the absence of lateral metatarsalgia (81). As Henry and Waugh (45) observed: Any operation for hallux valgus should attempt to restore (or at least not destroy) the ability of the big toe to bear weight. Multiple Osteotomies An intra-articular or soft-tissue reconstruction is contraindicated for the operative treatment of hallux valgus in the presence of a congruous metatarsophalangeal joint (a distal metatarsal articular angle of greater than 15 degrees) (23). In this situation, an extra-articular correction may be achieved with either a double or a triple osteotomy. An Akin phalangeal osteotomy (2,21,23,36) can decrease phalangeal angulation due to an increased proximal phalangeal articular angle; a proximal osteotomy of the first metatarsal (28,107) or a cuneiform osteotomy (21, 39) can diminish an increased intermetatarsal angle; and, in some cases, an increase in the distal metatarsal articular angle necessitates a medial closing-wedge osteotomy of the distal end of the metatarsal (32,49,106,114). Mitchell and Baxter (102) recommended combining a chevron osteotomy with a phalangeal osteotomy. In general, the magnitude of the distal metatarsal articular angle determines the need for multiple osteotomies of the first ray. Richardson et al. (116) found that, on anatomical and radiographic analysis, the average distal metatarsal articular angle in 100 normal feet was 6 or 7 degrees. As this angle increases, the magnitude of the hallux valgus angle increases (23). As previously mentioned, Piggott (108) noted that 9 per cent of adults who have hallux valgus have congruous metatarsophalangeal joints, and I (23) found congruous joints in twentyeight (47 per cent) of sixty children who had hallux valgus. It is in these patients who have a congruous joint and a large distal metatarsal articular angle that a double or triple osteotomy has the best capacity to
15 correct a hallux valgus deformity. Technique Distal metatarsal osteotomy: With the use of this technique (28,32,106,107,114), a medial longitudinal incision is centered over the metatarsophalangeal joint. The dissection is deepened to the capsule. The medial part of the capsule is released on the dorsal and proximal aspect with an L-shaped distally based capsular flap. At a point approximately 1.5 centimeters proximal to the surface of the metatarsophalangeal joint, a medial closing-wedge osteotomy of the proximal metatarsal metaphysis is performed (Figs. 39-A, 39-B, and 39-C). The magnitude of the medial closing wedge depends on the magnitude of the lateral slope of the distal metatarsal articular angle. Usually, the wedge is six to ten millimeters wide at its base. Care must be taken to avoid injury of the sesamoid complex on the plantar aspect with this closing-wedge osteotomy. Loretz et al. (74) and Kramer et al. (66) both described a z-shaped osteotomy of the distal end of the metatarsal that protects the sesamoid mechanism. Once the wedge has been removed, the osteotomy is closed and fixed with two oblique inch (0.157-centimeter) Kirschner wires. The medial eminence is then resected with an oscillating saw. The medial part of the capsule is approximated and secured to the first metatarsal with a suture placed through a metaphyseal drill-hole. The capsular repair is completed with interrupted absorbable sutures. After completion of this osteotomy, the great toe may appear to be in slight varus because the toe now more closely parallels the long axis of the shaft of the metatarsal. This situation creates the need for a proximal osteotomy of the first ray to diminish the first-second intermetatarsal angle. A proximal osteotomy of the first metatarsal may be considered but should be approached with caution as extensive soft-tissue stripping of the first metatarsal may devascularize it. An alternative osteotomy, therefore, is an opening-wedge osteotomy of the first cuneiform (21). Osteotomy of the first cuneiform: This technique (21) involves a medial longitudinal incision centered over the first cuneiform. Care is taken to identity the naviculocuneiform and metatarsocuneiform joints, exposing the entire medial aspect of the first cuneiform, which is approximately three centimeters high and two centimeters long (Figs. 39-A, 39-B, and 39-C). A vertical osteotomy is made in the center of the bone, and the osteotomy site is opened medially. Once the osteotomy site had been distracted, a triangular bicortical iliac-crest bone graft is impacted into place and stabilized with two inch (0.157-centimeter) Kirschner wires. Bone removed from the metatarsal head or the medial eminence usually is insufficient to serve as a graft. The incision is closed in a routine fashion. Postoperative Care The foot is placed in a gauze-and-tape compression dressing in the operating room, and a non-weightbearing below-the-knee cast is applied. At four weeks, the cast is changed and weight-bearing is allowed. Usually, the sites of the osteotomies heal in six to eight weeks. The cast is removed after radiographic confirmation of healing, and range-ofmotion exercises are initiated. Results and Complications While Funk and Wells (32), Peabody (106), Hohmann (49), and Reverdin (114) reported success with distal osteotomies of the first metatarsal, and Durman (28) as well as Goldner and Gaines (36) reported success with double osteotomies, very few investigators have reported quantitative results of these procedures. Kramer et al. (66) reported an average 15-degree correction of the distal metatarsal articular angle with a distal z-type rotational osteotomy, and Loretz et al. (74) reported a similar improvement in this angle. Funk and Wells (32) reported an average 7.2-degree correction of the intermetatarsal angle with a distal closing-wedge osteotomy of the metatarsal. A variety of double osteotomies have been advocated, including phalangeal with metatarsal osteotomy (2,23, 36), double metatarsal osteotomies (23,28), phalangeal with chevron osteotomy (102), and phalangeal with cuneiform osteotomy (21,39) (Figs. 40-A, 40=B, and 40-C). Reporting on the use of double and triple osteotomies for the treatment of adolescent hallux valgus with congruous metatarsophalangeal joints, I (23) noted an average hallux valgus correction of 22.9 degrees and an average correction of the first-second intermetatarsal angle of 8.3 degrees in seven patients. This correction was in the presence of an average distal metatarsal articular angle of 18.9 degrees. These results are similar to those obtained by Peterson and Newman (107), who reported on ten adolescent patients who had an average correction of the hallux valgus angle of 24 degrees and an average correction of the first-second intermetatarsal angle of 8.2 degrees after double osteotomies. A high rate of subjective satisfaction was reported in both series. Complications with multiple metatarsal osteotomies include loss of fixation, loss of correction (21), malunion (21), avascular necrosis (53), intra-articular extension of the osteotomy (102), and degenerative osteoarthrosis of the interphalangeal or metatarsophalangeal joint. These techniques are difficult and should be reserved for the occasional case of a hallux valgus deformity with a congruous joint associated with an increased distal metatarsal articular angle of more than 15 degrees. Overview The process of deciding which procedure to perform for a patient who has a bunion or bunions requires a careful preoperative physical evaluation and radiographic assessment to determine the specific pathological elements that need operative correction. All elements of the deformity, including an increased hallux valgus angle, increased first-second intermetatarsal angle, pronation of the great toe, increased distal metatarsal articular angle, enlarged medial eminence, and subluxation of the sesamoids,
16 must be corrected. Failure to correct any of these components places the foot at substantial risk for recurrent deformity. The large number of procedures that are available testifies to the fact that no one method sufficiently corrects all bunion deformities. While it is not uncommon for a surgeon to be comfortable with one specific procedure and to use it to correct most hallux valgus deformities, different deformities have various pathological components and magnitudes and may necessitate distinctly different operative approaches if consistently good results are to be achieved. Likewise, the upper limits of deformities that can be corrected successfully on a routine basis vary from surgeon to surgeon and may depend in part on the familiarity with the procedure, the operative technique used, and the frequency with which it is used. Operative versatility is important, and several types of operations should be at the disposal of the surgeon in order to address the different anatomical abnormalities. Some operative procedures have very limited indications. Choosing a procedure that has the capacity to correct a hallux valgus deformity easily is preferable to stretching the indications of a less intensive procedure, as doing so invites postoperative complications. In selecting a specific operative technique, the surgeon must attempt to maintain a flexible first metatarsophalangeal joint, preserve the normal weight-bearing pattern of the forefoot, and retain a reasonable means of salvage should a complication occur. References: (1-151) 1. Akin, O.: The treatment of hallux valgus a new operative procedure and its results. Med. Sentinel 1925; 33: Amarnek, D. L.; Jacobs, A. M.; and Oloff, L. M.: Adolescent hallux valgus: its etiology and surgical management. J. Foot Surg. 1985; 24: Austin, D. W.; and Leventen, E. O.: A new osteotomy for hallux valgus: a horizontally directed V displacement osteotomy of the metatarsal head for hallux valgus and primus varus. Clin. Orthop. 1981; 157: Bingold, A. C.: Arthrodesis of the great toe. Proc. Roy. Soc. Med. 1958; 51: Blum, J. L.: The modified Mitchell osteotomybunionectomy: indications and technical considerations. Foot and Ankle Internat. 1994; 15: Bonney, G.; and Macnab, I.: Hallux valgus and hallux rigidus. A critical survey of operative results. J. Bone and Joint Surg. 1952; 34-B(3): Brage, M. E.; Holmes, J. R.; and Sangeorzan, B. J.: The influence of x-ray orientation on the first metatarsocuneiform joint angle. Foot and Ankle Internat. 1994; 15: Brahms, M. A.: Hallux valgus the Akin procedure. Clin. Orthop. 1981; 157: Briggs, T. W. R.; Smith, P.; and McAuliffe, T. B.: Mitchell's osteotomy using internal fixation and early mobilisation. J. Bone and Joint Surg. 1992; 74-B(1): Butson, A. R. C.: A modification of the Lapidus operation for hallux valgus. J. Bone and Joint Surg. 1980; 62-B(3): Carr, C. R.; and Boyd, B. M.: Correctional osteotomy for metatarsus primus varus and hallux valgus. J. Bone and Joint Surg. Oct. 1968; 50-A: Cedell, C. A.; and Astrom, M.: Proximal metatarsal osteotomy in hallux valgus. Acta Orthop. Scandinavica 1982; 53: Cleveland, M.; and Winant, E. M.: An endresult study of the Keller operation. J. Bone and Joint Surg. Jan. 1950; 32-A: Clutton, H. H.: The treatment of hallux valgus. St. Thomas Hosp. Rep ; 22: Colloff, B.; and Weitz, E. M.: Proximal phalangeal osteotomy in hallux valgus. Clin. Orthop. 1967; 54: Corless, J.: A modification of the Mitchell procedure. In Proceedings of the Canadian Orthopaedic Association. J. Bone and Joint Surg. 1976; 58-B(1): Coughlin, M. J.: Hallux valgus. Causes, evaluation, and treatment. Postgrad. Med. 1984; 75: Coughlin, M. J.: Arthrodesis of the first metatarsophalangeal joint. Orthop. Rev. 1990; 19: Coughlin, M. J.: Arthrodesis of the first metatarsophalangeal joint with mini-fragment plate fixation. Orthopedics 1990; 13: Coughlin, M. J.: Chevron procedure. Contemp. Orthop. 1991; 23: Coughlin, M. J.: The juvenile bunion. In Surgery of the Foot and Ankle, edited by R. A. Mann and M. J. Coughlin. Ed. 6, pp St. Louis, Mosby-Year Book, Coughlin, M.: Proximal first metatarsal osteotomy. In The Foot and Ankle. Master Techniques in Orthopaedic Surgery, pp Edited by K. A. Johnson. New York, Raven Press, Coughlin, M. J.: Juvenile hallux valgus: etiology and treatment. Foot and Ankle Internat. 1995; 16: Coughlin, M. J.; and Abdo, R. V.: Arthrodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot and Ankle Internat. 1994; 15: Coughlin, M. J.; and Mann, R. A.: Arthrodesis of the first metatarsophalangeal joint as salvage for the failed Keller procedure. J. Bone and Joint Surg. Jan. 1987; 69-A: Coughlin, M. J., and Mann, R. A.: The pathophysiology of the juvenile bunion. In Instructional Course Lectures, The American Academy of Orthopaedic Surgeons. Vol. 36,
17 pp Park Ridge, Illinois, The American Academy of Orthopaedic Surgeons, Coughlin, M. J., and Thompson, F. M.: The high price of high-fashion footwear. In Instructional Course Lectures, The American Academy of Orthopaedic Surgeons. Vol. 44, pp Rosemont, Illinois, The American Academy of Orthopaedic Surgeons, Durman, D. C.: Metatarsus primus varus and hallux valgus. Arch. Surg. 1957; 74: DuVries, H. L.: Surgery of the Foot, pp St. Louis, C. V. Mosby, Fitzgerald, J. A. W.: A review of long-term results of arthrodesis of the first metatarsophalangeal joint. J. Bone and Joint Surg. 1969; 51-B(3): Fitzgerald, J. A. W.; and Wilkinson, J. M.: Arthrodesis of the metatarsophalangeal joint of the great toe. Clin. Orthop. 1981; 157: Funk, F. J., Jr.; and Wells, R. E.: Bunionectomy with distal osteotomy. Clin. Orthop. 1972; 85: Gimple, K.; Amspacher, J. C.; and Kopta, J. A.: Metatarsophalangeal joint fusion of the great toe. Orthopedics 1978; 1: Glynn, M. K.; Dunlop, J. B.; and FitzPatrick, D.: The Mitchell distal metatarsal osteotomy for hallux valgus. J. Bone and Joint Surg. 1980; 62-B(2): Goldberg, I.; Bahar, A.; and Yosipovitch, Z.: Late results after correction of hallux valgus deformity by basilar phalangeal osteotomy. J. Bone and Joint Surg. Jan. 1987; 69-A: Goldner, J. L.; and Gaines, R. W.: Adult and juvenile hallux valgus: analysis and treatment. Orthop. Clin. North America 1976; 7: Grace, D.; Hughes, J.; and Klenerman, L.: A comparison of Wilson and Hohmann osteotomies in the treatment of hallux valgus. J. Bone and Joint Surg. 1988; 70-B(2): Haines, R. W.; and McDougall, A.: The anatomy of hallux valgus. J. Bone and Joint Surg. 1954; 36-B(2): Hara, B.; Beck, J. C.; and Woo, R. A.: First cuneiform closing abductory osteotomy for reduction of metatarsus primus adductus. J. Foot Surg. 1992; 31: Hardy, R. H.; and Clapham, J. C. R.: Observations on hallux valgus. Based on a controlled series. J. Bone and Joint Surg. 1951; 33-B(3): Harris, R. I.; and Beath, T.: The short first metatarsal. Its incidence and clinical significance. J. Bone and Joint Surg. July 1949; 31-A: Harrison, M. H. M.; and Harvey, F. J.: Arthrodesis of the first metatarsophalangeal joint for hallux valgus and rigidus. J. Bone and Joint Surg. April 1963; 45-A: Hattrup, S. J.; and Johnson, K. A.: Chevron osteotomy: analysis of factors in patients' dissatisfaction. Foot and Ankle 1985; 5: Hawkins, F. B.; Mitchell, C. L.; and Hedrick, D. W.: Correction of hallux valgus by metatarsal osteotomy. J. Bone and Joint Surg. July 1945; 27: Henry, A. P. J.; and Waugh, W.: The use of footprints in assessing the results of operations for hallux valgus~ A comparison of Keller's operation and arthrodesis. J. Bone and Joint Surg. 1975; 57-B(4): Hetherington, V. J.; Steinbock, G.; LaPorta, D.; and Gardner, C.: The Austin bunionectomy: a follow-up study. J. Foot and Ankle Surg. 1993; 32: Hirvensalo, E.; Böstman, O.; Törmälä, P.; Vainionpä, S.; and Rokkanen, P.: Chevron osteotomy fixed with absorbable polyglycolide pins. Foot and Ankle 1991; 11: Hohmann, G.: Der Hallux valgus und die ubrigen Zehenverkrummungen. Ergeb. Chir. Orthop. 1925; 18: Hohmann, G.: Fuss und Bein. Ed. 4, p Munich, J. F. Bergmann, Horne, G.; Tanzer, T.; and Ford, M.: Chevron osteotomy for the treatment of hallux valgus. Clin. Orthop. 1984; 183: Humbert, J. L.; Bourbonniere, C.; and Laurin, C. A.: Metatarsophalangeal fusion for hallux valgus: indications and effect on the first metatarsal ray. Canadian Med. Assn. J. 1979; 120: Inman, V. T.: Hallux valgus: a review of etiologic factors. Orthop. Clin. North America 1974; 5: Jahss, M. H.: Hallux valgus: further considerations of the first metatarsal head [editorial] Foot and Ankle 1981; 2: Jahss, M. H.; Troy, A. I.; and Kummer, F.: Roentgenographic and mathematical analysis of first metatarsal osteotomies for metatarsus primus varus: a comparative study. Foot and Ankle 1985; 5: Johansson, J. E.; and Barrington, T. W.: Cone arthrodesis of the first metatarsophalangeal joint. Foot and Ankle 1984; 4: Johnson, J. E.; Clanton, T. O.; Baxter, D. E.; and Gottlieb, M. S.: Comparison of chevron osteotomy and modified McBride bunionectomy for correction of mild to moderate hallux valgus deformity. Foot and Ankle 1991; 12: Johnson, K. A.; Cofield, R. H.; and Morrey, B. F.: Chevron osteotomy for hallux valgus. Clin. Orthop. 1979; 142: Jordan, H. H.; and Brodsky, A. E.: Keller operation for hallux valgus and hallux rigidus. An end result study. Arch. Surg. 1951; 62: Kato, T.; and Watanabe, S.: The etiology of hallux valgus in Japan. Clin. Orthop. 1981;
18 157: Keller, W. L.: The surgical treatment of bunions and hallux valgus. New York Med. J. 1904; 80: Kilmartin, T. E.; and Wallace, W. A.: The significance of pes planus in juvenile hallux valgus. Foot and Ankle 1992; 13: Kinnard, P.; and Gordon, D.: A comparison between chevron and Mitchell osteotomies for hallux valgus. Foot and Ankle 1984; 4: Kitaoka, H. B.; Franco, M. G.; Weaver, A. L.; and Ilstrup, D. M.: Simple bunionectomy with medial capsulorrhaphy. Foot and Ankle 1991; 12: Klaue, K.; Hansen, S. T.; and Masquelet, A. C.: Clinical, quantitative assessment of first tarsometatarsal mobility in the sagittal plane and its relation to hallux valgus deformity. Foot and Ankle Internat. 1994; 15: Klosok, J. K.; Pring, D. J.; Jessop, J. H.; and Maffulli, N.: Chevron or Wilson metatarsal osteotomy for hallux valgus. A prospective randomised trial. J. Bone and Joint Surg. 1993; 75-B(5): Kramer, J.; Barry, L. D.; Helfman, D. N.; Mehnert, J. A.; and Pokrifcak, V. M.: The modified Scarf bunionectomy. J. Foot Surg. 1992; 31: Lapidus, P. W.: Operative correction of the metatarsus varus primus in hallux valgus. Surg., Gynec. and Obstet. 1934; 58: Lapidus, P. W.: The author's bunion operation from 1931 to Clin. Orthop. 1960; 16: Leventen, E. O.: The chevron procedure. Orthopedics 1990; 13: Lewis, R. J.; and Feffer, H. L.: Modified chevron osteotomy of the first metatarsal. Clin. Orthop. 1981; 157: Limbird, T. J.; DaSilva, R. M.; and Green, N. E.: Osteotomy of the first metatarsal base for metatarsus primus varus. Foot and Ankle 1989; 9: Lippert, F. G., III; and McDermott, J. E.: Crescentic osteotomy for hallux valgus: a biomechanical study of variables affecting the final position of the first metatarsal. Foot and Ankle 1991; 11: Lipscomb, P. R.: Arthrodesis of the first metatarsophalangeal joint for severe bunions and hallux rigidus. Clin. Orthop. 1979; 142: Loretz, L.; DeValentine, S.; and Yamaguchi, K.: The first metatarsal bicorrectional head osteotomy (distal L /Reverdin-Laird procedure) for correction of hallux abducto valgus: a retrospective study. J. Foot and Ankle Surg. 1993; 32: Love, T. R.; Whynot, A. S.; Farine, I.; Lavoie, M.; Hunt, L.; and Gross, A.: Keller arthroplasty: a prospective review. Foot and Ankle 1987; 8: McBride, E. D.: A conservative operation for bunions. J. Bone and Joint Surg. Oct. 1928; 10: McBride, E. D.: The conservative operation for bunions. End results and refinements of technic. J. Am. Med. Assn. 1935; 105: McBride, E. D.: The McBride bunion hallux valgus operation. Refinements in the successive surgical steps of the operation. J. Bone and Joint Surg. Dec. 1967; 49-A: McKeever, D. C.: Arthrodesis of the first metatarsophalangeal joint for hallux valgus, hallux rigidus, and metatarsus primus varus. J. Bone and Joint Surg. Jan. 1952; 34-A: Maguire, W. B.: The Lapidus procedure for hallux valgus. In Proceedings of the Australian Orthopaedic Association. J. Bone and Joint Surg. 1973; 55-B(1): Majkowski, R. S.; and Galloway, S.: Excision arthroplasty for hallux valgus in the elderly: a comparison between the Keller and modified Mayo operations. Foot and Ankle 1992; 13: Mankey, M. G.; and Mann, R. A.: Arthrodesis of the first metatarso-phalangeal joint utilizing a dorsal plate. Orthop. Trans ; 16: Mann, R. A.: Letter to the editor. Foot and Ankle 1982; 3: Mann, R. A.: Hallux valgus. In Instructional Course Lectures, The American Academy of Orthopaedic Surgeons. Vol. 35, pp St. Louis, C. V. Mosby, Mann, R. A.: Decision-making in bunion surgery. In Instructional Course Lectures, The American Academy of Orthopaedic Surgeons. Vol. 39, pp Park Ridge, Illinois, The American Academy of Orthopaedic Surgeons, Mann, R. A.; and Coughlin, M. J.: The rheumatoid foot. Review of literature and method of treatment. Orthop. Rev. 1979; 8: Mann, R. A.; and Coughlin, M. J.: Hallux valgus etiology, anatomy, treatment and surgical considerations. Clin. Orthop. 1981; 157: Mann, R. A., and Coughlin, M. J.: Video Textbook of Foot and Ankle Surgery, pp St. Louis, Medical Video Productions, Mann, R. and Coughlin, M. J.: Adult hallux valgus. In Surgery of the Foot and Ankle, edited by R. A. Mann and M. J. Coughlin. Ed. 6, pp St. Louis, Mosby-Year Book, Mann, R. A.; and Katcherian, D. A.: Relationship of metatarsophalangeal joint fusion on the intermetatarsal angle. Foot and Ankle 1989; 10: Mann, R. A.; and Oates, J. C.: Arthrodesis of the first metatarsophalangeal joint. Foot and
19 Ankle 1980; 1: Mann, R. A.; and Pfeffinger, L.: Hallux valgus repair. DuVries modified McBride procedure. Clin. Orthop. 1991; 272: Mann, R. A.; and Thompson, F. M.: Arthrodesis of the first metatarsophalangeal joint for hallux valgus in rheumatoid arthritis. J. Bone and Joint Surg. June 1984; 66-A: Mann, R. A.; Rudicel, S.; and Graves, S. C.: Repair of hallux valgus with a distal softtissue procedure and proximal metatarsal osteotomy. A long-term follow-up. J. Bone and Joint Surg. Jan. 1992; 74-A: Marin, G. A.: Arthrodesis of the metatarsophalangeal joint of the big toe for hallux valgus and hallux rigidus. A new method. Internat. Surg. 1968; 50: Mauldin, D. M.; Sanders, M.; and Whitmer, W. W.: Correction of hallux valgus with metatarsocuneiform stabilization. Foot and Ankle 1990; 11: Meier, P. J.; and Kenzora, J. E.: The risks and benefits of distal first metatarsal osteotomies. Foot and Ankle 1985; 6: Merkel, K. D.; Katoh, Y.; Johnson, E. W., Jr.; and Chao, E. Y. S.: Mitchell osteotomy for hallux valgus: long-term follow-up and gait analysis. Foot and Ankle 1983; 3: Meyer, J. M.; Hoffmeyer, P.; and Borst, F.: The treatment of hallux valgus in runners using a modified McBride procedure. Internat. Orthop. 1987; 11: Miller, J. W.: Distal first metatarsal displacement osteotomy. Its place in the schema of bunion surgery. J. Bone and Joint Surg. July 1974; 56-A: Mitchell, C. L.; Fleming, J. L.; Allen, R.; Glenney, C.; and Sanford, G. A.: Osteotomybunionectomy for hallux valgus. J. Bone and Joint Surg. Jan. 1958; 40-A: Mitchell, L. A.; and Baxter, D. E.: The chevron-akin double osteotomy for correction of hallux valgus. Foot and Ankle 1991; 12: Mizuno, K.; Hashimura, M.; Kimura, M.; and Hirohata, K.: Treatment of hallux valgus by oblique osteotomy of the first metatarsal. Foot and Ankle 1992; 13: Moynihan, F. J.: Arthrodesis of the metatarsophalangeal joint of the great toe. J. Bone and Joint Surg. 1967; 49-B(3): Myerson, M.: Metatarsocuneiform arthrodesis for treatment of hallux valgus and metatarsus primus varus. Orthopedics 1990; 13: Peabody, C. W.: The surgical cure of hallux valgus. J. Bone and Joint Surg. April 1931; 13: Peterson, H. A.; and Newman, S. R.: Adolescent bunion deformity treated with double osteotomy and longitudinal pin fixation of the first ray. J. Pediat. Orthop. 1993; 13: Piggott, H.: The natural history of hallux valgus in adolescence and early adult life. J. Bone and Joint Surg. 1960; 42-B(4): Plattner, P. F.; and Van Manen, J. W.: Results of Akin type proximal phalangeal osteotomy for correction of hallux valgus deformity. Orthopedics 1990; 13: Pochatko, D. J.; Schlehr, F. J.; Murphey, M. D.; and Hamilton, J. J.: Distal chevron osteotomy with lateral release for treatment of hallux valgus deformity. Foot and Ankle Internat. 1994; 15: Raymakers, R.; and Waugh, W.: The treatment of metatarsalgia with hallux valgus. J. Bone and Joint Surg. 1971; 53-B(4): Resch, S.; Stenström, A.; and Egund, N.: Proximal closing wedge osteotomy and adductor tenotomy for treatment of hallux valgus. Foot and Ankle 1989; 9: Resch, S.; Stenström, A.; and Gustafson, T.: Circulatory disturbance of the first metatarsal head after chevron osteotomy as shown by bone scintigraphy. Foot and Ankle 1992; 13: Reverdin, J.: De la déviation en dehors du gros orteil et de son traitement chirurgical. Trans. Internat. Med. Congress 1881; 2: Richardson, E. G.: Keller resection arthroplasty. Orthopedics 1990; 13: Richardson, E. G.; Graves, S. C.; McClure, J. T.; and Boone, R. T.: First metatarsal headshaft angle: a method of determination. Foot and Ankle 1993; 14: Riggs, S. A., Jr.; and Johnson, E. W., Jr.: McKeever arthrodesis for the painful hallux. Foot and Ankle 1983; 3: Rogers, W. A.; and Joplin, R. J.: Hallux valgus, weak foot, and the Keller operation: an end-result study. Surg. Clin. North America 1947; 27: Sammarco, G. J.; Brainard, B. J.; and Sammarco, V. J.: Bunion correction using proximal chevron osteotomy. Foot and Ankle 1993; 14: Sangeorzan, B. J.; and Hansen, S. T., Jr.: Modified Lapidus procedure for hallux valgus. Foot and Ankle 1989; 9: Schemitsch, E.; and Horne, G.: Wilson's osteotomy for the treatment of hallux valgus. Clin. Orthop. 1989; 240: Scranton, P. E., Jr.; and Zuckerman, J. D.: Bunion surgery in adolescents: results of surgical treatment. J. Pediat. Orthop. 1984; 4: Seelenfreund, M.; and Fried, A.: Correction of hallux valgus deformity by basal phalanx osteotomy of the big toe. J. Bone and Joint Surg. Oct. 1973; 55-A: Shereff, M. J.; Yang, Q. M.; and Kummer, F. J.: Extraosseous and intraosseous arterial supply to the first metatarsal and
20 metatarsophalangeal joint. Foot and Ankle 1987; 8: Sherman, K. P.; Douglas, D. L.; and Benson, M. K. D'A.: Keller's arthroplasty: is distraction useful? A prospective trial. J. Bone and Joint Surg. 1984; 66-B(5): Silberman, F. S.: Proximal phalangeal osteotomy for the correction of hallux valgus. Clin. Orthop. 1972; 85: Silver, D.: The operative treatment of hallux valgus. J. Bone and Joint Surg. April 1923; 5: Sim-Fook, L.; and Hodgson, A. R.: A comparison of foot forms among the non-shoe and shoe-wearing Chinese population. J. Bone and Joint Surg. Oct. 1958; 40-A: Simmonds, F. A.; and Menelaus, M. B.: Hallux valgus in adolescents. J. Bone and Joint Surg. 1960; 42-B(4): Smith, R. W.; Reynolds, J. C.; and Stewart, M. J.: Hallux valgus assessment: report of research committee of American Orthopaedic Foot and Ankle Society. Foot and Ankle 1984; 5: Stein, H. C.: Hallux valgus. Surg., Gynec. and Obstet. 1938; 66: Szaboky, G. T.; and Raghaven, V. C.: Modification of Mitchell's lateral displacement angulation osteotomy. J. Bone and Joint Surg. Oct. 1969; 51-A: Thomas, F. B.: Keller's arthroplasty modified. A technique to ensure post-operative distraction of the toe. J. Bone and Joint Surg. 1962; 44-B(2): Thompson, F. R.; and McElvenny, R. T.: Arthrodesis of the first metatarsophalangeal joint. J. Bone and Joint Surg. July 1940; 22: Thordarson, D. B.; and Leventen, E. O.: Hallux valgus correction with proximal metatarsal osteotomy: two year follow-up. Foot and Ankle 1992; 13: Tupman, S.: Arthrodesis of first metatarsophalangeal joint. In Proceedings of the Regional Orthopaedic Clubs. J. Bone and Joint Surg. 1958; 40-B(4): Turan, I.; and Lindgren, U.: Compressionscrew arthrodesis of the first metatarsophalangeal joint of the foot. Clin. Orthop. 1987; 221: Turnbull, T.; and Grange, W.: A comparison of Keller's arthroplasty and distal metatarsal osteotomy in the treatment of adult hallux valgus. J. Bone and Joint Surg. 1986; 68- B(1): Vallier, G. T.; Petersen, S. A.; and LaGrone, M. O.: The Keller resection arthroplasty: a 13- year experience. Foot and Ankle 1991; 11: von Salis-Soglio, G.; and Thomas, W.: Arthrodesis of the metatarsophalangeal joint of the great toe. Arch. Orthop. and Trauma Surg. 1979; 95: Wagner, F. W., Jr.: Technique & rationale:

 subluxation of the sesamoids. Fig.")
21 Figs. 1-A, 1-B, and 1-C: Radiographs demonstrating the different degrees of a hallux valgus deformity. The arrow indicate the direction of the subluxation, and the arrowheads indicate the extent of the joint surface. Fig. 1-A: A mild hallux valgus deformity with subluxation of the first metatarsophalangeal joint. The hallux valgus angle is 19 degrees, the firstsecond intermetatarsal angle is 10 degrees, and there is less than 50 per cent (mild) subluxation of the sesamoids. Fig. 1-B: Moderate hallux valgus deformity with subluxation of the first metatarsophalangeal joint. The hallux valgus angle is 30 degrees, the firstsecond intermetatarsal angle is 14 degrees, and there is 50 to 75 per cent (moderate) subluxation of the sesamoids.
 subluxation of the sesamoids.")
 has developed medial to the articular surface.")
22 Fig. 1-C: A severe, recurrent hallux valgus deformity with severe subluxation of the first metatarsophalangeal joint. The hallux valgus angle is 50 degrees, the intermetatarsal angle is 17 degrees, and there is more than 75 per cent (severe) subluxation of the sesamoids. The second metatarsophalangeal joint is dislocated. Radiograph of a foot with moderate hallux valgus deformity without subluxation of the first metatarsophalangeal joint. The hallux valgus is due mainly to 25 degrees of valgus angulation of the distal articular surface of the metatarsal. A sagittal groove (or sulcus) has developed medial to the articular surface. There is a prominent medial eminence. The dotted line indicates the medial and lateral extent of the distal articular surface of the metatarsal.


23 Figs. 6-A and 6-B: Photographs of a foot with severe hallux valgus with pronation of the great toe. Axial view, demonstrating pronation of the great toe.
 and axial (Fig.")
. Figs. 8-A and 8-B: Anteroposterior (Fig.")
24 Figs. 8-A through 8-F: Radiographs showing normal alignment and subluxation of the sesamoids. Figs. 8- A and 8-B: Anteroposterior (Fig. 8-A) and axial (Fig. 8-B) radiographs made with the patient standing, demonstrating the normal alignment of the sesamoids with a straight great toe. Note the crista (double chevrons). Figs. 8-A and 8-B: Anteroposterior (Fig. 8-A) and axial (Fig. 8-B) radiographs, made with the patient standing, demonstrating the normal alignment of the sesamoids with a straight great toe. Note the crista (double chevrons).
. Figs. 8-C and 8-D: Anteroposterior (Fig. 8-C) and axial (Fig.")
25 Figs. 8-C and 8-D: Anteroposterior (Fig. 8-C) and axial (Fig. 8-D) radiographs, made with the patient standing, showing moderate hallux valgus deformity. The hallux valgus angle is 32 degrees, and there is 75 per cent subluxation of the sesamoids (dotted outlines). Figs. 8-C and 8-D: Anteroposterior (Fig. 8-C) and axial (Fig. 8-D) radiographs, made with the patient standing, showing a moderate hallux valgus deformity. The hallux valgus angle is 32 degrees, and there is 75 per cent subluxation of the sesamoids (dotted outlines).

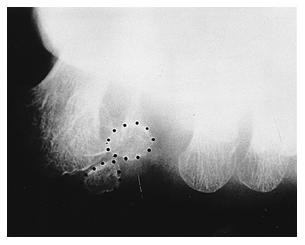
26 Anteroposterior (Fig. 8-E) and axial (Fig. 8-F) radiographs, made with the patient standing, showing a severe hallux valgus deformity. The hallux valgus angle is 55 degrees, with vertical orientation of the lateral sesamoid dorsal to the medial sesamoid (dotted outlines in Fig. 8-F). Anteroposterior (Fig. 8-E) and axial (Fig. 8-F) radiographs, made with the patient standing, showing a severe hallux valgus deformity. The hallux valgus angle is 55 degrees, with vertical orientation of the lateral sesamoid dorsal to the medial sesamoid (dotted outlines in Fig. 8-F).


27 Figs. 10-A, 10-B, and 10-C: Anteroposterior radiographs demonstrating the shapes of the metatarsophalangeal articular surfaces. Fig. 10-A: A rounded articular surface (dotted line) is more prone to subluxation of the metatarsophalangeal joint. Fig. 10-B: The joint is congruous without subluxation. A flat or chevron-shaped metatarsophalangeal joint to tends resist subluxation.
.")
28 Fig. 10-C: A hallux valgus deformity with a congruous metatarsophalangeal joint (dotted lines). Photograph and radiograph of a foot with hallux valgus interphalangeus.


29 Photograph and radiograph of a foot with hallux valgus interphalangeus. Radiograph of the foot shown in Figs. 11-A and 11- B, after correction of the hallux valgus interphalangeus deformity with the Akin procedure (1,8,88,109,126).

30 Figs. 13-A and 13-B: Radiographs made after the performance of an Akin procedure (1,8,88,109,126) in a foot with a moderate hallux valgus deformity. Fig. 13- A: Postoperatively, there is no correction of the firstsecond intermetatarsal angle and little correction of the hallux valgus angle. Fig. 13-B: Fourteen years postoperatively, there is recurrent deformity with increased subluxation of the sesamoids.
31 Figs. 16-A and 16-B: Radiographs made before and after exostectomy in a foot with moderate hallux valgus deformity. Fig. 16-A: Preoperatively, the lateral sesamoid is displaced 50 per cent. The fifth toe had been amputated previously as a result of trauma. Fig. 16-B: After the operation, the hallux valgus recurred, with progression of the deformity. The hallux valgus is now characterized by severe subluxation of the metatarsophalangeal joint and progression of the sesamoid displacement.
32 Figs. 17-A and 17-B: Radiographs made before and after a distal soft-tissue reconstruction in a foot with mild hallux valgus deformity, subluxation of the metatarsophalangeal joint, and 50 per cent subluxation of the lateral sesamoid. Fig. 17-A: Preoperatively, the hallux valgus angle is 17 degrees, and the first-second intermetatarsal angle is 10 degrees. Fig. 17-B: Postoperatively, the hallux valgus and firstsecond intermetatarsal angles have been corrected. The hallux valgus angle is 9 degrees, and the firstsecond intermetatarsal angle is 5 degrees.
33 Figs. 21-A and 21-B: Radiographs made before and after a chevron osteotomy in a foot with a moderate hallux valgus deformity and subluxation of the metatarsophalangeal joint. Fig. 21-A: Preoperative appearance. Fig. 21-B: Postoperatively, satisfactory correction has been achieved. Note the internal fixation with a Kirschner wire.
 radiographs showing avascular necrosis after a chevron osteotomy combined")
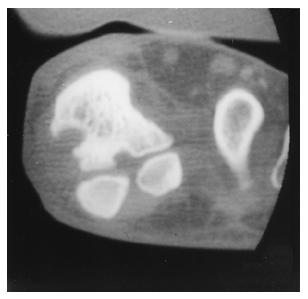
34 Anteroposterior (Fig. 22-A) and axial (sesamoid) (Fig. 22-B) radiographs showing avascular necrosis after a chevron osteotomy combined with a lateral release. Anteroposterior (Fig. 22-A) and axial (sesamoid) (Fig. 22-B) radiographs showing avascular necrosis after a chevron osteotomy combined with a lateral release.

 Fig.")
35 Figs. 24-A and 24-B: Radiographs made before and after a distal metatarsal osteotomy in a foot with a moderate hallux valgus deformity and subluxation of the metatarsophalangeal joint. (Radiographs courtesy of Kent K. Wu, M.D.) Fig. 24-B: Postoperatively, there is satisfactory correction.


36 Figs. 27-A and 27-B: Radiographs made before and after a proximal osteotomy of the first metatarsal in a foot with a hallux valgus deformity. Fig. 27-A: Preoperatively, the hallux valgus angle is 45 degrees and the first-second intermetatarsal angle is 13 degrees. Fig. 27-B: Eight years after the operation, the hallux valgus angle is 15 degrees and the first-second intermetatarsal angle is 6 degrees.
37 Radiograph of a foot with overcorrection (negative first-second intermetatarsal angle) and malunion at the site of the proximal osteotomy, which leads to an increased risk of hallux varus. Figs. 30-A and 30-B: Radiographs made before and after a distal soft-tissue repair and arthrodesis of the metatarsocuneiform joint in a foot with a moderate hallux valgus deformity and subluxation of the metatarsophalangeal joint. On preoperative examination, the patient had hypermobility of the metatarsocuneiform joint. Fig. 30-A: Preoperative appearance.

38 Fig. 30-B: Postoperatively, correction has been achieved. Internal fixation is routinely removed at twelve to sixteen weeks after a successful arthrodesis, to avoid breakage of the intermetatarsal screw. Figs. 32-A, 32-B, and 32-C: Photographs of the cannulated reaming technique. Fig. 32-A: The metatarsal head is reamed to a convex surface.



39 Fig. 32-B: The base of the proximal phalanx is reamed with a cannulated reamer. The cup-shaped congruous surfaces are prepared for arthrodesis. Lateral radiograph and illustration demonstrating the Vitallium mini-fragment screw-and-plate construct.


40 Dorsal photograph and illustration of the Vitallium mini-fragment screw-and-plate construct. Figs. 34-A and 34-B: Radiographs made before and after arthrodesis of the first metatarsophalangeal joint in a patient who had rheumatoid arthritis and severe hallux valgus deformity. Fig. 34-A: Preoperative appearance.

41 Fig. 34-B: Six months postoperatively, there is a painless fibrous union and the deformity is much less severe. Figs. 35-A and 35-B: Radiographs made before and after arthrodesis of the metatarsophalangeal joint in a foot with a severe hallux valgus deformity and widening of the first-second intermetatarsal angle to 25 degrees. Fig. 35-A: Preoperative appearance.
42 Fig. 35-B: Postoperatively, the first-second intermetatarsal angle decreased to 10 degrees as the hallux valgus angle was corrected. Figs. 37-A, 37-B, and 37-C: Radiographs made before and after excisional arthroplasty in an eightyyear-old woman who had a moderate hallux valgus deformity as well as osteoarthrosis of the metatarsophalangeal joint. Fig. 37-A: Preoperative appearance.

43 Fig. 37-B: Postoperatively, the intramedullary fixation with one Kirschner wire is seen. Fig. 37-C: One year after the operation, there is continued good alignment. Photograph and radiograph of a cock-up deformity of the great toe after an excisional arthroplasty.

44 Photograph and radiograph of a cock-up deformity of the great toe after an excisional arthroplasty. Figs. 40-A, 40-B, and 40-C: Radiographs made before and after a closing-wedge phalangeal osteotomy, a crescentic osteotomy of the proximal end of the metatarsal, and a closing-wedge osteotomy of the distal end of the metatarsal in a foot that had recurrent hallux valgus after a McBride procedure. Fig. 40-A: Preoperatively, the hallux valgus angle is 40 degrees and the distal metatarsal articular angle is 30 degrees.
45 Fig. 40-B: Immediate postoperative appearance. Fig. 40-C: Six months postoperatively, there has been excellent correction. The hallux valgus angle is 11 degrees, and the distal metatarsal articular angle is 2 degrees.
.")
46 Figs. 3-A, 3-B, and 3-C: Drawings illustrating the anatomy of the foot. Fig. 3-A: A transverse section through the first ray at the level of the first metatarsal head. The long and short extensors are the major tendinous structures on the dorsal aspect of the first metatarsophalangeal joint. The hood ligament interdigitates with the extensor hallucis longus (EHL). The flexors pass on the plantar aspect, with the flexor hallucis brevis (FHB) inserting into the sesamoids. EHB = extensor hallucis brevis, FHL = flexor hallucis longus, Ses. Lig. = sesamoid ligament, Col. Lig. = collateral ligament, and Medial Ses. = medial sesamoid. The plantar aspect of the first metatarsophalangeal joint. The sesamoid complex has been reflected distally to reveal the plantar plate. The plantar plate connects the sesamoids and the flexor hallucis brevis to the base of the proximal phalanx plantarly.
 and intrinsic muscles stabilize the plantar aspect of the first metatarsal head. The hood ligaments make up much of the dorsal aspect of the capsule.")

47 Illustration of the anatomy of a foot with the great toe in normal alignment. The sesamoids (Ses.) and intrinsic muscles stabilize the plantar aspect of the first metatarsal head. The hood ligaments make up much of the dorsal aspect of the capsule. EHL = extensor hallucis longus, EHB = extensor hallucis brevis, ADH = adductor hallucis, FHL = flexor hallucis longus, and ABH = abductor hallucis. Figs. 5-A, and 5-B: Drawings of the plantar aspect of a foot with hallux valgus. Fig. 5-A: The great toe deviates laterally. The great toe pronates (arrow) as it rotates on the axis of the conjoined adductor hallucis tendon.
 is diminished in height as the sesamoids (Ses.")


48 Drawing of the dorsal aspect of the toes of a foot with hallux valgus and a cross section through the first metatarsal head. The crista (intersesamoid ridge) is diminished in height as the sesamoids (Ses.) assume a more lateral orientation and the abductor hallucis (ABH) tendon migrates plantarward (arrows), leaving the thin extensor hood ligament as the major softtissue constraint against progressive hallux valgus. EHL = extensor hallucis longus, EHB = extensor hallucis brevis, ADH = adductor hallucis, and FHL = flexor hallucis longus. Figs. 7-A, 7-B, and 7-C: Illustrations demonstrating normal alignment and subluxation of the sesamoids. Fig. 7-A: Normal alignment of the sesamoids. As the first metatarsal migrates medially, the crista is eroded and the medial sesamoid assumes a more central location (arrow). With a severe deformity, the lateral sesamoid comes to lie vertically dorsal to the medial sesamoid (arrow), and a lateral soft-tissue contracture occurs.

49 Illustration demonstrating the radiographic measurements in the assessment of hallux valgus. The hallux valgus angle is formed by the intersection of the longitudinal axes of the first metatarsal and the proximal phalanx. A normal angle is less than 15 degrees. The first-second intermetatarsal angle is formed by the intersection of the longitudinal axes of the first and second metatarsals. A normal angle is less than 9 degrees. Illustration demonstrating how the distal metatarsal articular angle measures the lateral slope of the articular surface of the metatarsal. The distal metatarsal articular angle is the angle subtended by a line drawn perpendicular to the metatarsal articular surface and the longitudinal axis of the first metatarsal. With increasing lateral angulation of the articular surface, the angle increases. Illustration demonstrating how the proximal phalangeal articular angle increases with hallux valgus interphalangeus. The proximal phalangeal articular angle is the angle subtended by a line drawn perpendicular to the phalangeal articular surface and the longitudinal axis of the proximal phalanx.

.")
50 Figs. 12-A through 12-D: The proximal phalangeal osteotomy (Akin procedure (1,8,88,109,126) ). Fig. 12-A: Illustration demonstrating how an L-shaped capsulotomy releases the dorsal and proximal attachments of the metatarsophalangeal capsule. a = dorsal neurovascular bundle and b = capsular incision. Fig. 12-B: Illustration demonstrating how the medial eminence is excised in line with the medial aspect of the first metatarsal (lower shaded area). The medialbased osteotomy is located in the proximal phalangeal metaphysis (upper shaded area). Fig. 12-C: Illustration demonstrating how the osteotomy is approximated and fixed internally with Kirschner wires. The capsule is secured through a drill-hole in the metaphysis.

 is in line with the medial diaphyseal cortex of the first metatarsal.")
51 Illustration of a distal soft-tissue reconstruction. The conjoined adductor tendon is released, leaving a 1.5- centimeter stump of tendon, which is secured to the lateral aspect of the metatarsal capsule at the conclusion of the procedure. Illustration comparing resection of the medial eminence for the distal soft-tissue reconstruction with that for the chevron osteotomy. For the distal softtissue reconstruction, the excision of the medial eminence (line b) is in line with the medial diaphyseal cortex of the first metatarsal. However, for the chevron osteotomy, the osteotomy (line a) is in line with the medial border of the foot. Illustration of the chevron osteotomy. A drill-hole in the center of the metatarsal head marks the apex of the osteotomy. The angle of the osteotomy cut is 60 to 90 degrees, providing a large, stable surface area.


52 A dorsal view of the first metatarsal. The vascular supply to the head of the first metatarsal is through the medial and lateral soft-tissue structures and medullary vessels. A proximal metatarsal osteotomy does not interrupt the intramedullary supply. A distal metatarsal osteotomy, when combined with an extensive lateral soft-tissue release, may compromise the vascularity of the capital fragment. Figs. 20-A and 20-B: Illustrations of the chevron osteotomy. Fig. 20-A: The capital fragment is translated laterally (arrow). Fig. 20-B: The osteotomy is stabilized with a Kirschner wire, and the capsule is anchored with a suture through the metaphysis.
53 Figs. 23-A through 23-D: Illustrations of a distal metatarsal osteotomy. Fig. 23-A: The proposed osteotomy for a moderate hallux valgus deformity. The width of the lateral shelf determines the amount of displacement of the capital fragment (the wider the shelf, the greater the displacement). Fig. 23-B: More plantar bone is resected at the site of the osteotomy to allow plantar flexion. This diminishes the prevalence of postoperative transfer lesions. Fig. 23-C: After shortening and displacement, the capital fragment is translated laterally (arrow). The medial metatarsal flare is resected.

54 Fig. 23-D: With an increased distal metatarsal articular angle, a trapezoidal resection allows realignment of a congruous metatarsophalangeal joint. Illustration of the orientation of the saw blade at a 120-degree angle to the shaft of the first metatarsal during a distal soft-tissue reconstruction with a proximal osteotomy of the first metatarsal. Illustration of a foot after distal soft-tissue reconstruction with a proximal osteotomy of the first metatarsal and internal fixation with a compression screw and a Kirschner wire.
55 Figs. 29-A and 29-B: Illustrations of an arthrodesis of the first metatarsocuneiform joint. Fig. 29-A: Minimum resection of the articular surface and subchondral bone decreases the first-second intermetatarsal angle. Fig. 29-B: Slightly more bone is resected on the plantar surface to achieve plantar flexion at the site of the arthrodesis. Illustration demonstrating the two articular surfaces are resected in preparation for arthrodesis of the first metatarsophalangeal joint. Figs. 36-A, 36-B, and 36-C: Illustrations of an excisional arthroplasty. Fig. 36-A: Proposed resection of the medial eminence and the proximal quarter of the proximal phalanx.
56 Fig. 36-B: After resection of the bone. Fig. 36-C: The plantar plate is reapproximated to the residual proximal phalanx. Figs. 39-A, 39-B, and 39-C: Illustrations demonstrating how multiple osteotomies can be performed to achieve extra-articular correction of a hallux valgus deformity, especially when the distal metatarsal articular angle is increased. Fig. 39-A: A closing-wedge phalangeal osteotomy (a), a closingwedge osteotomy of the distal end of the metatarsal with exostectomy of the medial eminence (b), and an opening-wedge osteotomy of the first cuneiform (c). Lateral view showing the locations of the osteotomies.

57 Appearance of a foot after a triple osteotomy. There is over-all improved alignment of the first ray and the first metatarsophalangeal joint.
Proximal metatarsal osteotomy and distal soft tissue reconstruction as treatment for hallux valgus deformity
 REVIEW Proximal metatarsal osteotomy and distal soft tissue reconstruction as treatment for hallux valgus deformity Michael J. Coughlin and J. Speight Grimes Boise, Idaho, USA (Received for publication
REVIEW Proximal metatarsal osteotomy and distal soft tissue reconstruction as treatment for hallux valgus deformity Michael J. Coughlin and J. Speight Grimes Boise, Idaho, USA (Received for publication
JUVENILE AND ADOLESCENT HALLUX VALGUS. George E. Quill, Jr., M.D.
 JUVENILE AND ADOLESCENT HALLUX VALGUS George E. Quill, Jr., M.D. The development of a hallux valgus deformity in children and adolescents is actually an uncommon entity. Most of these occurrences can be
JUVENILE AND ADOLESCENT HALLUX VALGUS George E. Quill, Jr., M.D. The development of a hallux valgus deformity in children and adolescents is actually an uncommon entity. Most of these occurrences can be
Hallux Valgus Deformity: Preoperative Radiologic Assessment
 119 Pictorial Essay H............ - Hallux Valgus Deformity: Preoperative Radiologic Assessment David Karasick1 and Keith L. Wapner An estimated 40% of the American adult population experiences foot problems,
119 Pictorial Essay H............ - Hallux Valgus Deformity: Preoperative Radiologic Assessment David Karasick1 and Keith L. Wapner An estimated 40% of the American adult population experiences foot problems,
Soft Tissue Rebalancing Procedures for the Treatment of Hallux Valgus Deformities
 Soft Tissue Rebalancing Procedures for the Treatment of Hallux Valgus Deformities NO DISCLOSURES Objectives The main objectives of any procedure in hallux abducto valgus surgery are to correct the deformity,
Soft Tissue Rebalancing Procedures for the Treatment of Hallux Valgus Deformities NO DISCLOSURES Objectives The main objectives of any procedure in hallux abducto valgus surgery are to correct the deformity,
Merete PlantarMAX Lapidus Plate Surgical Technique. Description of Plate
 Merete PlantarMAX Lapidus Plate Surgical Technique Description of Plate Merete Medical has designed the PlantarMax; a special Plantar/Medial Locking Lapidus plate which places the plate in the most biomechanically
Merete PlantarMAX Lapidus Plate Surgical Technique Description of Plate Merete Medical has designed the PlantarMax; a special Plantar/Medial Locking Lapidus plate which places the plate in the most biomechanically
THE FIBULAR SESAMOID ELEVATOR: A New Instrument to Aid the Lateral Release in Hallux Valgus Surgery
 C H A P T E R 1 4 THE FIBULAR SESAMOID ELEVATOR: A New Instrument to Aid the Lateral Release in Hallux Valgus Surgery Thomas F. Smith, DPM Lopa Dalmia, DPM INTRODUCTION Hallux valgus surgery is a complex
C H A P T E R 1 4 THE FIBULAR SESAMOID ELEVATOR: A New Instrument to Aid the Lateral Release in Hallux Valgus Surgery Thomas F. Smith, DPM Lopa Dalmia, DPM INTRODUCTION Hallux valgus surgery is a complex
Re+Line Bunion Correction System for Correction of Hallux Abducto Valgus Deformity
 Re+Line Bunion Correction System for Correction of Hallux Abducto Valgus Deformity Amber M. Shane, DPM, FACFAS 1, Christopher L. Reeves, DPM, FACFAS 1 1. Orlando Foot & Ankle Clinic, Orlando, FL Abstract
Re+Line Bunion Correction System for Correction of Hallux Abducto Valgus Deformity Amber M. Shane, DPM, FACFAS 1, Christopher L. Reeves, DPM, FACFAS 1 1. Orlando Foot & Ankle Clinic, Orlando, FL Abstract
Clinical results of modified Mitchell s osteotomy for hallux valgus augmented with oblique lesser metatarsal osteotomy
 Journal of Orthopaedic Surgery 2005:13(3):245-252 Clinical results of modified Mitchell s osteotomy for hallux valgus augmented with oblique lesser metatarsal osteotomy K Yamamoto, A Imakiire, Y Katori,
Journal of Orthopaedic Surgery 2005:13(3):245-252 Clinical results of modified Mitchell s osteotomy for hallux valgus augmented with oblique lesser metatarsal osteotomy K Yamamoto, A Imakiire, Y Katori,
QUICK REFERENCE GUIDE. MiniRail System. Part B: Foot Applications. By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ALWAYS INNOVATING
 14 MiniRail System Part B: Foot Applications By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ALWAYS INNOVATING ORDERING INFORMATION Sterilization box, empty M190 Can accommodate: M101 Standard MiniRail
14 MiniRail System Part B: Foot Applications By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ALWAYS INNOVATING ORDERING INFORMATION Sterilization box, empty M190 Can accommodate: M101 Standard MiniRail
Introduction Basics MIS Screw 2 System Characteristics 2 Indication 2
 Clinical Advisor M. Walther. M.D., Ph.D. Professor of Orthopedic Surgery Head of Department Centre for Foot and Ankle Surgery Schön Klinik München Harlaching FIFA Medical Centre Table of Contents Introduction
Clinical Advisor M. Walther. M.D., Ph.D. Professor of Orthopedic Surgery Head of Department Centre for Foot and Ankle Surgery Schön Klinik München Harlaching FIFA Medical Centre Table of Contents Introduction
Index. Clin Podiatr Med Surg 22 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Clin Podiatr Med Surg 22 (2005) 309 314 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, myectomy of, for tailor s bunionette, 243 Achilles tendon, lengthening
Clin Podiatr Med Surg 22 (2005) 309 314 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, myectomy of, for tailor s bunionette, 243 Achilles tendon, lengthening
REVISIONAT HAttUX VATGUS SURGERY
 REVISIONAT HAttUX VATGUS SURGERY Bradley Castellano, D.P.M. Recurrence of deformity is one of the more common complications in hallux valgus surgery (1-3). The deformity may have been undercorrected with
REVISIONAT HAttUX VATGUS SURGERY Bradley Castellano, D.P.M. Recurrence of deformity is one of the more common complications in hallux valgus surgery (1-3). The deformity may have been undercorrected with
Moderate to severe hallux valgus deformity: correction with proximal crescentic osteotomy and distal soft-tissue release
 Arch Orthop Trauma Surg (2000) 120 : 397 402 Springer-Verlag 2000 ORIGINAL ARTICLE R. Zettl H.-J. Trnka M. Easley M. Salzer P. Ritschl Moderate to severe hallux valgus deformity: correction with proximal
Arch Orthop Trauma Surg (2000) 120 : 397 402 Springer-Verlag 2000 ORIGINAL ARTICLE R. Zettl H.-J. Trnka M. Easley M. Salzer P. Ritschl Moderate to severe hallux valgus deformity: correction with proximal
Diagnosing and treating hallux valgus: A conservative approach for a common problem
 REVIEW BRIAN G. DONLEY, MD Orthopaedic surgeon, Cleveland Clinic, specializing in foot and ankle disorders. CHRISTOPHER L. TISDEL, MD Orthopaedic surgeon. Cleveland Clinic. JAMES J. SFERRA, MD Orthopaedic
REVIEW BRIAN G. DONLEY, MD Orthopaedic surgeon, Cleveland Clinic, specializing in foot and ankle disorders. CHRISTOPHER L. TISDEL, MD Orthopaedic surgeon. Cleveland Clinic. JAMES J. SFERRA, MD Orthopaedic
PAINFUL SESAMOID OF THE GREAT TOE Dr Vasu Pai ANATOMICAL CONSIDERATION. At the big toe MTP joint: Tibial sesamoid (medial) & fibular (lateral)
 & fibular (lateral)") PAINFUL SESAMOID OF THE GREAT TOE Dr Vasu Pai ANATOMICAL CONSIDERATION At the big toe MTP joint: Tibial sesamoid (medial) & fibular (lateral) They are contained within the tendons of Flexor Hallucis Brevis
PAINFUL SESAMOID OF THE GREAT TOE Dr Vasu Pai ANATOMICAL CONSIDERATION At the big toe MTP joint: Tibial sesamoid (medial) & fibular (lateral) They are contained within the tendons of Flexor Hallucis Brevis
The effectiveness of distal soft tissue procedures in hallux valgus
 J Orthopaed Traumatol (2008) 9:117 121 DOI 10.1007/s10195-008-0017-3 ORIGINAL ARTICLE The effectiveness of distal soft tissue procedures in hallux valgus Cemil Kayali Æ Hasan Ozturk Æ Haluk Agus Æ Taskin
J Orthopaed Traumatol (2008) 9:117 121 DOI 10.1007/s10195-008-0017-3 ORIGINAL ARTICLE The effectiveness of distal soft tissue procedures in hallux valgus Cemil Kayali Æ Hasan Ozturk Æ Haluk Agus Æ Taskin
MiniRail System. Part B: Foot Applications. By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito
 Q U I C K R E F E R E N C E G U I D E 14 MiniRail System Part B: Foot Applications By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ORDERING INFORMATION MiniRail System Kit, M190C Contents: M 101 Standard
Q U I C K R E F E R E N C E G U I D E 14 MiniRail System Part B: Foot Applications By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ORDERING INFORMATION MiniRail System Kit, M190C Contents: M 101 Standard
Chevron Osteotomy With Lateral Soft Tissue Release
 5(4):250 256, 2006 T E C H N I Q U E Chevron Osteotomy With Lateral Soft Tissue Release Hans-Jörg Trnka, MD, PhD and Stefan Gerhard Hofstaetter, MD Foot and Ankle Center Vienna Vienna, Austria Ó 2006 Lippincott
5(4):250 256, 2006 T E C H N I Q U E Chevron Osteotomy With Lateral Soft Tissue Release Hans-Jörg Trnka, MD, PhD and Stefan Gerhard Hofstaetter, MD Foot and Ankle Center Vienna Vienna, Austria Ó 2006 Lippincott
19 Arthrodesis of the First Metatarsocuneiform Joint
 19 Arthrodesis of the First Metatarsocuneiform Joint CHARLES GUDAS Abduction of the first metatarsal to correct metatarsus primus varus and hallux valgus was first described by Albrecht in 1911. 1 Lapidus
19 Arthrodesis of the First Metatarsocuneiform Joint CHARLES GUDAS Abduction of the first metatarsal to correct metatarsus primus varus and hallux valgus was first described by Albrecht in 1911. 1 Lapidus
Distal First Metatarsal Displacement Osteotomy
 Distal First Metatarsal Displacement Osteotomy ITS PLACE IN THE SCHEMA OF BUNION SURGERY* From the Section of Orthopedic Surgerv, The Mason Clinic. Seattle ABSTRACT: In a review of 401 operations for symptomatic
Distal First Metatarsal Displacement Osteotomy ITS PLACE IN THE SCHEMA OF BUNION SURGERY* From the Section of Orthopedic Surgerv, The Mason Clinic. Seattle ABSTRACT: In a review of 401 operations for symptomatic
HemiEDGE. Patent No. 8,845,750. Surgical Technique
 HemiEDGE Patent No. 8,845,750 Surgical Technique Contents Product Based on the clinical success of our First MPJ Hemi Implant, the HemiEDGE, incorporates an overlapping edge extending around the medial,
HemiEDGE Patent No. 8,845,750 Surgical Technique Contents Product Based on the clinical success of our First MPJ Hemi Implant, the HemiEDGE, incorporates an overlapping edge extending around the medial,
PEDUS-L. Locking Plantar Lapidus Plate
 PEDUS-L Locking Plantar Lapidus Plate Page 1 PEDUS-L - Locking Plantar Lapidus Plate Table of Contents Implants 3 System 4 Operation manual 5 Approach 5 Identification of the TMT 1 joint with a cannula
PEDUS-L Locking Plantar Lapidus Plate Page 1 PEDUS-L - Locking Plantar Lapidus Plate Table of Contents Implants 3 System 4 Operation manual 5 Approach 5 Identification of the TMT 1 joint with a cannula
Case 57 What is the diagnosis? Insidious onset forefoot pain in a 50 year old female for last 3 months.
 Case 57 What is the diagnosis? Insidious onset forefoot pain in a 50 year old female for last 3 months. Diagnosis: II MTP instability Demographics of MT instability Lesser MTP joint instability occurs
Case 57 What is the diagnosis? Insidious onset forefoot pain in a 50 year old female for last 3 months. Diagnosis: II MTP instability Demographics of MT instability Lesser MTP joint instability occurs
Complications associated with Mitchell s Osteotomy for Hallux Valgus Correction: A retrospective hospital review
 The Foot and Ankle Online Journal Official publication of the International Foot & Ankle Foundation Complications associated with Mitchell s Osteotomy for Hallux Valgus Correction: A retrospective hospital
The Foot and Ankle Online Journal Official publication of the International Foot & Ankle Foundation Complications associated with Mitchell s Osteotomy for Hallux Valgus Correction: A retrospective hospital
The Ludloff Osteotomy
 Techniques in Foot and Ankle Surgery 4(4):263 268, 2005 Ó 2005 Lippincott Williams & Wilkins, Philadelphia The Ludloff Osteotomy T E C H N I Q U E Hans-Jörg Trnka, MD, PhD and Stefan Hofstätter, MD Foot
Techniques in Foot and Ankle Surgery 4(4):263 268, 2005 Ó 2005 Lippincott Williams & Wilkins, Philadelphia The Ludloff Osteotomy T E C H N I Q U E Hans-Jörg Trnka, MD, PhD and Stefan Hofstätter, MD Foot
First MPJ Hemi Implant
 First MPJ Hemi Implant Surgical Technique Contents Product The BioPro First MPJ Hemi Implant is a simple, durable, metallic hemiarthroplasty resurfacing prosthesis for the hallux metatarsophalangeal joint
First MPJ Hemi Implant Surgical Technique Contents Product The BioPro First MPJ Hemi Implant is a simple, durable, metallic hemiarthroplasty resurfacing prosthesis for the hallux metatarsophalangeal joint
Minimally Invasive Bunionectomy: The Lam Modification of the Traditional Distal First Metatarsal Osteotomy Bunionectomy
 CHAPTER 2 Minimally Invasive Bunionectomy: The Lam Modification of the Traditional Distal First Metatarsal Osteotomy Bunionectomy Kevin Lam, DPM Rikhil Patel, DPM Thomas Merrill, DPM Hallux abducto valgus
CHAPTER 2 Minimally Invasive Bunionectomy: The Lam Modification of the Traditional Distal First Metatarsal Osteotomy Bunionectomy Kevin Lam, DPM Rikhil Patel, DPM Thomas Merrill, DPM Hallux abducto valgus
Use of the 20 Memory Staple in Osteotomies of Fusions of the Forefoot
 168 Forefoot Reconstruction Use of the 20 Memory Staple in Osteotomies of Fusions of the Forefoot Definition, History, Generalities This staple first provides a permanent compression both in the prongs
168 Forefoot Reconstruction Use of the 20 Memory Staple in Osteotomies of Fusions of the Forefoot Definition, History, Generalities This staple first provides a permanent compression both in the prongs
MICA. Minimally Invasive Foot Surgery CHEVRON OSTEOTOMY SURGIC AL TECHNIQUE
 MICA Minimally Invasive Foot Surgery CHEVRON OSTEOTOMY SURGIC AL TECHNIQUE Contents Chapter 1 4 Introduction Chapter 2 5 Indications and Warnings Chapter 3 6 Patient Positioning and Set Up Chapter 4 7
MICA Minimally Invasive Foot Surgery CHEVRON OSTEOTOMY SURGIC AL TECHNIQUE Contents Chapter 1 4 Introduction Chapter 2 5 Indications and Warnings Chapter 3 6 Patient Positioning and Set Up Chapter 4 7
Medincenter GlavUpDK by the Ministry of Foreign Affairs of Russia, Moscow.
 Medincenter GlavUpDK by the Ministry of Foreign Affairs of Russia, Moscow. Berezhnoy Sergey. Percutaneous First Metatarsocuneiform Joint Arthrodesis in a Treatment of Metatarsus Primus Varus: a Prospective
Medincenter GlavUpDK by the Ministry of Foreign Affairs of Russia, Moscow. Berezhnoy Sergey. Percutaneous First Metatarsocuneiform Joint Arthrodesis in a Treatment of Metatarsus Primus Varus: a Prospective
A Patient s Guide to Bunions. Foot and Ankle Center of Massachusetts, P.C.
 A Patient s Guide to Bunions Welcome to Foot and Ankle Center of Massachusetts, where we believe in accelerating your learning curve with educational materials that are clearly written and professionally
A Patient s Guide to Bunions Welcome to Foot and Ankle Center of Massachusetts, where we believe in accelerating your learning curve with educational materials that are clearly written and professionally
Index. Note: Page numbers of article titles are in bold face type.
 Index Note: Page numbers of article titles are in bold face type. A Achilles tendon, Zadek osteotomy effects on, 430 Adult acquired flatfoot disorder, 387 403 calcaneal Z osteotomy for, 397 399 historical
Index Note: Page numbers of article titles are in bold face type. A Achilles tendon, Zadek osteotomy effects on, 430 Adult acquired flatfoot disorder, 387 403 calcaneal Z osteotomy for, 397 399 historical
SURGICAL TECHNIQUE GUIDE
 DANGER indicates an imminently hazardous situation which, if not avoided, will result in death or serious injury. WARNING indicates a potentially hazardous situation which, if not avoided, could result
DANGER indicates an imminently hazardous situation which, if not avoided, will result in death or serious injury. WARNING indicates a potentially hazardous situation which, if not avoided, could result
6/5/2018. Forefoot Disorders. Highgate Private Hospital (Royal Free London NHS Foundation Trust (Barnet & Chase Farm Hospitals) Hallux Rigidus
 Hallux Rigidus") Forefoot Disorders Mr Pinak Ray (MS, MCh(Orth), FRCS, FRCS(Tr&Orth)) Highgate Private Hospital (Royal Free London NHS Foundation Trust (Barnet & Chase Farm Hospitals) E: ray.secretary@uk-conslutants Our
Forefoot Disorders Mr Pinak Ray (MS, MCh(Orth), FRCS, FRCS(Tr&Orth)) Highgate Private Hospital (Royal Free London NHS Foundation Trust (Barnet & Chase Farm Hospitals) E: ray.secretary@uk-conslutants Our
Distal metatarsal osteotomy for hallux varus following surgery for hallux valgus
 FOOT AND ANKLE Distal metatarsal osteotomy for hallux varus following surgery for hallux valgus K. J. Choi, H. S. Lee, Y. S. Yoon, S. S. Park, J. S. Kim, J. J. Jeong, Y. R. Choi From the Asan Medical Center,
FOOT AND ANKLE Distal metatarsal osteotomy for hallux varus following surgery for hallux valgus K. J. Choi, H. S. Lee, Y. S. Yoon, S. S. Park, J. S. Kim, J. J. Jeong, Y. R. Choi From the Asan Medical Center,
REPAIR OF THE DISPLACED AUSTIN OSTEOTOMY
 C H A P T E R 2 1 REPAIR OF THE DISPLACED AUSTIN OSTEOTOMY John V. Vanore, DPM INTRODUCTION Bunion surgery is frequently performed by foot and ankle surgeons. Generally, bunion surgery is quite predictable,
C H A P T E R 2 1 REPAIR OF THE DISPLACED AUSTIN OSTEOTOMY John V. Vanore, DPM INTRODUCTION Bunion surgery is frequently performed by foot and ankle surgeons. Generally, bunion surgery is quite predictable,
The Effect of Hallux Abducto Valgus Surgery on the Sesamoid Apparatus Position
 1999 WILLIAM J. STICKEL GOLD AWARD The Effect of Hallux Abducto Valgus Surgery on the Sesamoid Apparatus Position MOLLY S. JUDGE, DPM* STEPHAN LAPOINTE, DPM, PhD GERARD V. YU, DPM JEFFREY E. SHOOK, DPM
1999 WILLIAM J. STICKEL GOLD AWARD The Effect of Hallux Abducto Valgus Surgery on the Sesamoid Apparatus Position MOLLY S. JUDGE, DPM* STEPHAN LAPOINTE, DPM, PhD GERARD V. YU, DPM JEFFREY E. SHOOK, DPM
Lesser MPJ Hemi Implant
 Lesser MPJ Hemi Implant Surgical Technique Contents Product The BioPro Lesser MPJ Hemi Implant is a simple, durable, metallic hemiarthroplasty resurfacing prosthesis for the treatment of arthritis, Freiberg
Lesser MPJ Hemi Implant Surgical Technique Contents Product The BioPro Lesser MPJ Hemi Implant is a simple, durable, metallic hemiarthroplasty resurfacing prosthesis for the treatment of arthritis, Freiberg
Modified Proximal Scarf Osteotomy for Hallux Valgus
 Original Article Clinics in Orthopedic Surgery 2018;10:479-483 https://doi.org/10.4055/cios.2018.10.4.479 Modified Proximal Scarf Osteotomy for Hallux Valgus Ki Won Young, MD, Hong Seop Lee, MD, Seong
Original Article Clinics in Orthopedic Surgery 2018;10:479-483 https://doi.org/10.4055/cios.2018.10.4.479 Modified Proximal Scarf Osteotomy for Hallux Valgus Ki Won Young, MD, Hong Seop Lee, MD, Seong
Bunions. Compliments of: Institute of Sports Medicine & Orthopaedics
 A Patient s Guide to Bunions 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Bunions 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in this booklet is compiled
Increased pressures at
 Surgical Off-loading of Plantar Hallux Ulcerations These approaches can be used to treat DFUs. By Adam R. Johnson, DPM Increased pressures at the plantar aspect of the hallux leading to chronic hyperkeratosis
Surgical Off-loading of Plantar Hallux Ulcerations These approaches can be used to treat DFUs. By Adam R. Johnson, DPM Increased pressures at the plantar aspect of the hallux leading to chronic hyperkeratosis
PROstep Minimally Invasive Surgery HALLUX VALGUS CORRECTION USING PROSTEP MICA MINIMALLY INVASIVE FOOT SURGERY: TWO CASE STUDIES
 PROstep Minimally Invasive Surgery HALLUX VALGUS CORRECTION USING PROSTEP MICA MINIMALLY INVASIVE FOOT SURGERY: TWO CASE STUDIES AS PRESENTED BY: JOEL VERNOIS M.D. 016798A Case Study 1 PROstep Minimally
PROstep Minimally Invasive Surgery HALLUX VALGUS CORRECTION USING PROSTEP MICA MINIMALLY INVASIVE FOOT SURGERY: TWO CASE STUDIES AS PRESENTED BY: JOEL VERNOIS M.D. 016798A Case Study 1 PROstep Minimally
How to avoid complications of distraction osteogenesis for first brachymetatarsia
 220 Acta Orthopaedica 2009; 80 (2): 220 225 How to avoid complications of distraction osteogenesis for first brachymetatarsia Keun-Bae Lee, Hyun-Kee Yang, Jae-Yoon Chung, Eun-Sun Moon, and Sung-Taek Jung
220 Acta Orthopaedica 2009; 80 (2): 220 225 How to avoid complications of distraction osteogenesis for first brachymetatarsia Keun-Bae Lee, Hyun-Kee Yang, Jae-Yoon Chung, Eun-Sun Moon, and Sung-Taek Jung
Comparison of Postoperative Outcomes between Modified Mann Procedure and Modified Lapidus Procedure for Hallux Valgus
 Comparison of Postoperative Outcomes between Modified Mann Procedure and Modified Lapidus Procedure for Hallux Valgus Yui Akiyama, Takaaki Hirano, Hiroyuki Mitsui Shingo Maeda, Hisateru Niki Department
Comparison of Postoperative Outcomes between Modified Mann Procedure and Modified Lapidus Procedure for Hallux Valgus Yui Akiyama, Takaaki Hirano, Hiroyuki Mitsui Shingo Maeda, Hisateru Niki Department
Hallux Malleus develops after Flexible Hallux Varus correction with Tensioned Suture Device: A Case Report
 The Foot and nkle Online Journal Official publication of the International Foot & nkle Foundation Hallux Malleus develops after Flexible Hallux Varus correction with Tensioned Suture Device: Case Report
The Foot and nkle Online Journal Official publication of the International Foot & nkle Foundation Hallux Malleus develops after Flexible Hallux Varus correction with Tensioned Suture Device: Case Report
Surgical technique. Angular Stable X-Plate and 2-Hole Plate. For osteotomies, arthrodeses and fractures of the foot.
 Surgical technique Angular Stable X-Plate and 2-Hole Plate. For osteotomies, arthrodeses and fractures of the foot. Table of Contents Indications 4 Implants 5 X-plate: Crescentic osteotomy 6 X-plate:
Surgical technique Angular Stable X-Plate and 2-Hole Plate. For osteotomies, arthrodeses and fractures of the foot. Table of Contents Indications 4 Implants 5 X-plate: Crescentic osteotomy 6 X-plate:
Six Surgical Techniques
 Comprehensive Solutions for Forefoot and Midfoot Surgery using the Mini TightRope System : Mini TightRope FT Repair Kit 2.7 mm Drill Hole Technique Mini TightRope 1.1 mm Disposables Kit Metal Mini TightRope
Comprehensive Solutions for Forefoot and Midfoot Surgery using the Mini TightRope System : Mini TightRope FT Repair Kit 2.7 mm Drill Hole Technique Mini TightRope 1.1 mm Disposables Kit Metal Mini TightRope
20 Cuneiform Osteotomy
 20 Cuneiform Osteotomy FRANCIS LYNCH While the use of the cuneiform osteotomy for surgical repair of hallux abducto valgus has never gained significant notoriety, there has been a recent heightened interest
20 Cuneiform Osteotomy FRANCIS LYNCH While the use of the cuneiform osteotomy for surgical repair of hallux abducto valgus has never gained significant notoriety, there has been a recent heightened interest
RETROSPECTIVE ANALYSIS OF END-TO-END DIGITAL ARTHRODESIS
 C H A P T E R 1 7 RETROSPECTIVE ANALYSIS OF END-TO-END DIGITAL ARTHRODESIS Michelle L. Butterworth, DPM Michael S. Downey, DPM Digital deformities are one of the most common entities we face as foot and
C H A P T E R 1 7 RETROSPECTIVE ANALYSIS OF END-TO-END DIGITAL ARTHRODESIS Michelle L. Butterworth, DPM Michael S. Downey, DPM Digital deformities are one of the most common entities we face as foot and
The Lapidus Procedure as Salvage After Failed Surgical Treatment of Hallux Valgus A PROSPECTIVE COHORT STUDY
 60 COPYRIGHT 2003 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED The Lapidus Procedure as Salvage After Failed Surgical Treatment of Hallux Valgus A PROSPECTIVE COHORT STUDY BY J. CHRIS COETZEE,
60 COPYRIGHT 2003 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED The Lapidus Procedure as Salvage After Failed Surgical Treatment of Hallux Valgus A PROSPECTIVE COHORT STUDY BY J. CHRIS COETZEE,
Ascension. Silicone MCP surgical technique. surgical technique Ascension Silicone MCP
 Ascension Silicone MCP surgical technique WW 2 Introduction This manual describes the sequence of techniques and instruments used to implant the Ascension Silicone MCP (FIGURE 1A). Successful use of this
Ascension Silicone MCP surgical technique WW 2 Introduction This manual describes the sequence of techniques and instruments used to implant the Ascension Silicone MCP (FIGURE 1A). Successful use of this
IN HAttUX VALGUS SURGERY
 INTRA.OPERATIVE DECISION MAKING IN HAttUX VALGUS SURGERY Dennis E. Martin, D.P.M. Alfred f. Phillips, D.P.M. fohn A. Ruch, D.P.M. PURPOSE The techniques of anatomic dissection in hallux valgus surgery
INTRA.OPERATIVE DECISION MAKING IN HAttUX VALGUS SURGERY Dennis E. Martin, D.P.M. Alfred f. Phillips, D.P.M. fohn A. Ruch, D.P.M. PURPOSE The techniques of anatomic dissection in hallux valgus surgery
Merete BLP. Surgical Technique. - Bunion Locking Plate - Low Profile Locking Bone Plate System
 Merete BLP - Bunion Locking Plate - Low Profile Locking Bone Plate System Surgical Technique Merete Medical, Inc. 49 Purchase Street Rye, N.Y. 10580 Phone: 914 967-1532 www.merete-medical.com - Surgical
Merete BLP - Bunion Locking Plate - Low Profile Locking Bone Plate System Surgical Technique Merete Medical, Inc. 49 Purchase Street Rye, N.Y. 10580 Phone: 914 967-1532 www.merete-medical.com - Surgical
Long Oblique Distal Osteotomy of the Fifth Metatarsal for Correction of Tailor s Bunion: A Retrospective Review
 Long Oblique Distal Osteotomy of the Fifth Metatarsal for Correction of Tailor s Bunion: A Retrospective Review Barry P. London, DPM, 1 Stephen F. Stern, DPM, 2 Mark A. Quist, DPM, 3 Robert K. Lee, DPM,
Long Oblique Distal Osteotomy of the Fifth Metatarsal for Correction of Tailor s Bunion: A Retrospective Review Barry P. London, DPM, 1 Stephen F. Stern, DPM, 2 Mark A. Quist, DPM, 3 Robert K. Lee, DPM,
Investigation performed at Orthopaedic Hospital Gersthof, Vienna, Austria
 1131 COPYRIGHT 2004 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED Salvage of a Failed Keller Resection Arthroplasty BY FELIX MACHACEK JR., MD, MARK E. EASLEY, MD, FLORIAN GRUBER, MD, PETER RITSCHL,
1131 COPYRIGHT 2004 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED Salvage of a Failed Keller Resection Arthroplasty BY FELIX MACHACEK JR., MD, MARK E. EASLEY, MD, FLORIAN GRUBER, MD, PETER RITSCHL,
with regard to our presentation.
 Rotated Insertion Metatarsal Osteotomy with Distal Soft Tissue Procedure for Severe Hallux Valgus Deformity Novel Procedure of the 1 st metatarsal osteotomy Norihiro Samoto MD, Ph.D. Director of Department
Rotated Insertion Metatarsal Osteotomy with Distal Soft Tissue Procedure for Severe Hallux Valgus Deformity Novel Procedure of the 1 st metatarsal osteotomy Norihiro Samoto MD, Ph.D. Director of Department
DARCO. Bow 2 Plate SURGIC AL TECHNIQUE
 DARCO Bow 2 Plate SURGIC AL TECHNIQUE Contents 2 Preface 3 Chapter 1 4 Chapter 2 5 6 7 8 9 Appendix 10 10 11 Intended Use Indications/Contraindications Design Rationale Preoperative Planning Surgical Technique
DARCO Bow 2 Plate SURGIC AL TECHNIQUE Contents 2 Preface 3 Chapter 1 4 Chapter 2 5 6 7 8 9 Appendix 10 10 11 Intended Use Indications/Contraindications Design Rationale Preoperative Planning Surgical Technique
Mr. Siva Chandrasekaran Orthopaedic Surgeon MBBS MSpMed MPhil (surg) FRACS
 FRACS") Bunion Surgery Most people with bunions find pain relief with simple treatments to reduce pressure on the big toe, such as wearing wider shoes or using pads in their shoes. However, if these measures do
Bunion Surgery Most people with bunions find pain relief with simple treatments to reduce pressure on the big toe, such as wearing wider shoes or using pads in their shoes. However, if these measures do
LAPIDUS What is Old is New
 LAPIDUS What is Old is New Alan Jay Block, DPM, MS, FASPS, FACFAS Fellowship trained in Advanced Ankle Techniques Adjunct Professor Dept Of Orthopeadics The Ohio State University Board Member The Ohio
LAPIDUS What is Old is New Alan Jay Block, DPM, MS, FASPS, FACFAS Fellowship trained in Advanced Ankle Techniques Adjunct Professor Dept Of Orthopeadics The Ohio State University Board Member The Ohio
Endolog Implant for Correction of Hallux Valgus
 Endolog Implant for Correction of Hallux Valgus Surgical Technique Distributed by: Simple and precise Mini-invasive For mild, moderate and severe HV Surgical Indications Endolog implant is proposed for
Endolog Implant for Correction of Hallux Valgus Surgical Technique Distributed by: Simple and precise Mini-invasive For mild, moderate and severe HV Surgical Indications Endolog implant is proposed for
Other Congenital and Developmental Diseases of the Foot. Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University
 Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
Surgical Technique. Surgical Technique
 Surgical Technique Surgical Technique Chevron Osteotomy Akin Osteotomy Basal Osteotomy 1st Mtpj Cheilectomy Distal Metatarsal Osteotomy Calcaneal Osteotomy Minimally Invasive Foot Surgery 1 Introduction
Surgical Technique Surgical Technique Chevron Osteotomy Akin Osteotomy Basal Osteotomy 1st Mtpj Cheilectomy Distal Metatarsal Osteotomy Calcaneal Osteotomy Minimally Invasive Foot Surgery 1 Introduction
4/22/2017 ADVENTURES IN FOREFOOT RECONSTRUCTIVE SURGERY WHAT IS FOREFOOT RECONSTRUCTION? HALLUX VALGUS CORRECTION
 4/22/217 ADVENTURES IN FOREFOOT RECONSTRUCTIVE SURGERY ERIN E. KLEIN, DPM, MS Associate Director of Research, Weil Foot & Ankle Institute Clinical Instructor, Dr William M Scholl College of Podiatric Medicine
4/22/217 ADVENTURES IN FOREFOOT RECONSTRUCTIVE SURGERY ERIN E. KLEIN, DPM, MS Associate Director of Research, Weil Foot & Ankle Institute Clinical Instructor, Dr William M Scholl College of Podiatric Medicine
Accu-Cut Osteotomy Guide System
 Accu-Cut Osteotomy Guide System Surgical Technique Contents Product The BioPro Accu-Cut Osteotomy Guide System provides precise and repeatable osteotomies for many types of bunion correction surgery. Table
Accu-Cut Osteotomy Guide System Surgical Technique Contents Product The BioPro Accu-Cut Osteotomy Guide System provides precise and repeatable osteotomies for many types of bunion correction surgery. Table
Essential Insights On Tendon Transfers For Digital Dysfunction
 Essential Insights On Tendon Transfers For Digital Dysfunction VOLUME: 23 PUBLICATION DATE: Apr 01 2010 Issue Number: 4 April 2010 Author(s): Lawrence DiDomenico, DPM, FACFAS While tendon transfers have
Essential Insights On Tendon Transfers For Digital Dysfunction VOLUME: 23 PUBLICATION DATE: Apr 01 2010 Issue Number: 4 April 2010 Author(s): Lawrence DiDomenico, DPM, FACFAS While tendon transfers have
Reliability of the radiographic measurement of the hallux interphalangeal angle. Mohammadali Khademi
 Reliability of the radiographic measurement of the hallux interphalangeal angle Mohammadali Khademi A research report submitted to the Faculty of Health Sciences, University of the Witwatersrand, in partial
Reliability of the radiographic measurement of the hallux interphalangeal angle Mohammadali Khademi A research report submitted to the Faculty of Health Sciences, University of the Witwatersrand, in partial
Question: You trained as a general orthopaedic and trauma surgeon and became a Consultant in Newcastle in 1968.
 Question: You trained as a general orthopaedic and trauma surgeon and became a Consultant in Newcastle in 1968. How did you become so interested in conditions of the foot? As an Orthopaedic trainee in
Question: You trained as a general orthopaedic and trauma surgeon and became a Consultant in Newcastle in 1968. How did you become so interested in conditions of the foot? As an Orthopaedic trainee in
Digital Surgery Complications
 Annual Surgical Conference 2018 Digital Surgery Complications Zeeshan S. Husain, DPM, FACFAS, FASPS Great Lakes Foot and Ankle Institute September 21, 2018 None Disclosures Presentation Outline Differentials
Annual Surgical Conference 2018 Digital Surgery Complications Zeeshan S. Husain, DPM, FACFAS, FASPS Great Lakes Foot and Ankle Institute September 21, 2018 None Disclosures Presentation Outline Differentials
Combination of First Metatarsophalangeal Joint Arthrodesis and Proximal Correction for Severe Hallux Valgus Deformity
 FOOT &ANKLE INTERNATIONAL DOI: 10.3113/FAI.2012.0400 Combination of First Metatarsophalangeal Joint Arthrodesis and Proximal Correction for Severe Hallux Valgus Deformity Pascal F. Rippstein, MD; Young-Uk
FOOT &ANKLE INTERNATIONAL DOI: 10.3113/FAI.2012.0400 Combination of First Metatarsophalangeal Joint Arthrodesis and Proximal Correction for Severe Hallux Valgus Deformity Pascal F. Rippstein, MD; Young-Uk
5 COMMON CONDITIONS IN THE FOOT & ANKLE
 5 COMMON CONDITIONS IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA IN A NUTSHELL ~ ALL ANATOMY & BIOMECHANICS >90% OF CONDITIONS IN FOOT & ANKLE DIAGNISED FROM GOOD
5 COMMON CONDITIONS IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA IN A NUTSHELL ~ ALL ANATOMY & BIOMECHANICS >90% OF CONDITIONS IN FOOT & ANKLE DIAGNISED FROM GOOD
ToeMobile. Surgical Technique. Great Toe Endoprosthesis
 Great Toe Endoprosthesis Surgical Technique Merete Medical, Inc. 99 Purchase Street Rye, N.Y. 10580 Phone: 914 967-1532 Fax: 914-967-1542 E-Mail: service@merete-medical.com www.merete-medical.com - Description
Great Toe Endoprosthesis Surgical Technique Merete Medical, Inc. 99 Purchase Street Rye, N.Y. 10580 Phone: 914 967-1532 Fax: 914-967-1542 E-Mail: service@merete-medical.com www.merete-medical.com - Description
A New Incisional Approach to the Rheumatoid Foot
 A New Incisional Approach to the Rheumatoid Foot The authors introduce a new incisional approach to surgery of the rheumatoid foot. Advantages and disadvantages are presented. Historical comparisons are
A New Incisional Approach to the Rheumatoid Foot The authors introduce a new incisional approach to surgery of the rheumatoid foot. Advantages and disadvantages are presented. Historical comparisons are
Effect of metatarsal osteotomy and open lateral soft tissue procedure on sesamoid position: radiological assessment
 Choi et al. Journal of Orthopaedic Surgery and Research (2018) 13:11 DOI 10.1186/s13018-017-0712-y RESEARCH ARTICLE Effect of metatarsal osteotomy and open lateral soft tissue procedure on sesamoid position:
Choi et al. Journal of Orthopaedic Surgery and Research (2018) 13:11 DOI 10.1186/s13018-017-0712-y RESEARCH ARTICLE Effect of metatarsal osteotomy and open lateral soft tissue procedure on sesamoid position:
Foot and Ankle Technique Guide Proximal Inter-Phalangeal (PIP) Fusion
 Fusion") Surgical Technique Foot and Ankle Technique Guide Proximal Inter-Phalangeal (PIP) Fusion Prepared in consultation with: Phinit Phisitkul, MD Department of Orthopedics and Rehabilitation University of Iowa
Surgical Technique Foot and Ankle Technique Guide Proximal Inter-Phalangeal (PIP) Fusion Prepared in consultation with: Phinit Phisitkul, MD Department of Orthopedics and Rehabilitation University of Iowa
Bunion Correction System
 Bunion Correction System Easy insertion and medial placement accuracy using Landmark Guide technology Maximized and repeatable uniform compression across osteotomy site Stable Fixation of the Metatarsal
Bunion Correction System Easy insertion and medial placement accuracy using Landmark Guide technology Maximized and repeatable uniform compression across osteotomy site Stable Fixation of the Metatarsal
SWANSON. Flexible Hinge Toe Implant SURGIC AL TECHNIQUE
 SWANSON Flexible Hinge Toe Implant SURGIC AL TECHNIQUE SWANSON flexible HINGE TOE IMPLANT with SWANSON Flexible Hinge Grommet surgical technique presented by ALFRED B. SWANSON, MD, FACS, GRAND RAPIDS,
SWANSON Flexible Hinge Toe Implant SURGIC AL TECHNIQUE SWANSON flexible HINGE TOE IMPLANT with SWANSON Flexible Hinge Grommet surgical technique presented by ALFRED B. SWANSON, MD, FACS, GRAND RAPIDS,
Foot and Ankle Technique Guide Metatarsal Shortening Osteotomy
 Surgical Technique Foot and Ankle Technique Guide Metatarsal Shortening Osteotomy Prepared in consultation with: Phinit Phisitkul, MD Department of Orthopedics and Rehabilitation University of Iowa Iowa
Surgical Technique Foot and Ankle Technique Guide Metatarsal Shortening Osteotomy Prepared in consultation with: Phinit Phisitkul, MD Department of Orthopedics and Rehabilitation University of Iowa Iowa
Integra. Silicone Toe System SURGICAL TECHNIQUE
 Silicone Toe System SURGICAL TECHNIQUE Silicone Toe System Table of Contents Indications...2 Contraindications...2 Warnings...2 Precautions...2 Adverse Events...2 Flexible Great Toe (FGT)...3 Surgical
Silicone Toe System SURGICAL TECHNIQUE Silicone Toe System Table of Contents Indications...2 Contraindications...2 Warnings...2 Precautions...2 Adverse Events...2 Flexible Great Toe (FGT)...3 Surgical
Technique Guide. 2.4 mm Variable Angle LCP Distal Radius System. For fragment-specific fracture fixation with variable angle locking technology.
 Technique Guide 2.4 mm Variable Angle LCP Distal Radius System. For fragment-specific fracture fixation with variable angle locking technology. Table of Contents Introduction 2.4 mm Variable Angle LCP
Technique Guide 2.4 mm Variable Angle LCP Distal Radius System. For fragment-specific fracture fixation with variable angle locking technology. Table of Contents Introduction 2.4 mm Variable Angle LCP
Crossover Second Toe: Demographics, Etiology, and Radiographic Assessment
 FOOT &ANKLE INTERNATIONAL Copyright 2007 by the American Orthopaedic Foot & Ankle Society, Inc. DOI: 10.3113/FAI.2007.1223 Crossover Second Toe: Demographics, Etiology, and Radiographic Assessment Ari
FOOT &ANKLE INTERNATIONAL Copyright 2007 by the American Orthopaedic Foot & Ankle Society, Inc. DOI: 10.3113/FAI.2007.1223 Crossover Second Toe: Demographics, Etiology, and Radiographic Assessment Ari
Aetiology: Pressure of Distal intermetatarsal ligament against common digital nerve. Lumbar radiculopathy Instability MTPJ joint or inflammatory MPJ
 MORTON S NEUROMA 80% III web space (next common is II). Never occurs in III or IV Common in females in fifties Aetiology: Pressure of Distal intermetatarsal ligament against common digital nerve Rule out
MORTON S NEUROMA 80% III web space (next common is II). Never occurs in III or IV Common in females in fifties Aetiology: Pressure of Distal intermetatarsal ligament against common digital nerve Rule out
Symptomatic Medial Exostosis of the Great Toe Distal Phalanx: A Complication Due to Over-correction Following Akin Osteotomy for Hallux Valgus Repair
 Symptomatic Medial Exostosis of the Great Toe Distal Phalanx: A Complication Due to Over-correction Following Akin Osteotomy for Hallux Valgus Repair Carlos Villas, MD, PhD, 1 Javier Del Río, MD, 3 Andres
Symptomatic Medial Exostosis of the Great Toe Distal Phalanx: A Complication Due to Over-correction Following Akin Osteotomy for Hallux Valgus Repair Carlos Villas, MD, PhD, 1 Javier Del Río, MD, 3 Andres
A Patient s Guide to Hallux Rigidus
 A Patient s Guide to Hallux Rigidus Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 DISCLAIMER: The information in this booklet
A Patient s Guide to Hallux Rigidus Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 DISCLAIMER: The information in this booklet
1 st MP Arthrodesis. - Unraveling The Myths - Craig A. Camasta, DPM Atlanta, Georgia, USA
 1 st MP Arthrodesis - Unraveling The Myths - Craig A. Camasta, DPM Atlanta, Georgia, USA Hallux Limitus Dorsal Bunion Spasm of Short Flexor Immobility of Sesamoids DJD of 1 st MPJ Hallus Limitus Plantar
1 st MP Arthrodesis - Unraveling The Myths - Craig A. Camasta, DPM Atlanta, Georgia, USA Hallux Limitus Dorsal Bunion Spasm of Short Flexor Immobility of Sesamoids DJD of 1 st MPJ Hallus Limitus Plantar
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
ANATOMIC APPROACH TO PREPARATION AND FUSION OF THE INTERPHALANGEAL JOINT
 C H A P T E R 1 2 ANATOMIC APPROACH TO PREPARATION AND FUSION OF THE INTERPHALANGEAL JOINT Robert B. Weinstein, DPM INTRODUCTION The complex combination of deformities grouped under the umbrella hammertoes
C H A P T E R 1 2 ANATOMIC APPROACH TO PREPARATION AND FUSION OF THE INTERPHALANGEAL JOINT Robert B. Weinstein, DPM INTRODUCTION The complex combination of deformities grouped under the umbrella hammertoes
Clarification of Terms
 Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
SURGICAL TECHNIQUE CHI. Cannulated Hemi Implants 1 ST MPJ ARTHROPLASTY
 CHI Cannulated Hemi Implants 1 ST MPJ ARTHROPLASTY SURGICAL TECHNIQUE CHI Cannulated Hemi Implants Design Rationale Pain of the great toe joint often leads to altered lifestyles. The goal of MPJ implant
CHI Cannulated Hemi Implants 1 ST MPJ ARTHROPLASTY SURGICAL TECHNIQUE CHI Cannulated Hemi Implants Design Rationale Pain of the great toe joint often leads to altered lifestyles. The goal of MPJ implant
A COMPARISON OF KELLER S ARTHROPLASTY AND DISTAL METATARSAL OSTEOTOMY IN THE TREATMENT OF ADULT HALLUX VALGUS
 A COMPARISON OF KELLER S ARTHROPLASTY AND DISTAL METATARSAL OSTEOTOMY IN THE TREATMENT OF ADULT HALLUX VALGUS TIMOTHY TURNBULL, WILLIAM GRANGE From the North East Thames Regional Orthopaedic Centre, Black
A COMPARISON OF KELLER S ARTHROPLASTY AND DISTAL METATARSAL OSTEOTOMY IN THE TREATMENT OF ADULT HALLUX VALGUS TIMOTHY TURNBULL, WILLIAM GRANGE From the North East Thames Regional Orthopaedic Centre, Black
A PROSPECTIVE RANDOMISED CONTROLLED TRIAL
 K. B. Lee, N. Y. Cho, H. W. Park, J. K. Seon, S. H. Lee From Chonnam National University Medical School and Hospital, Gwangju, Korea K. B. Lee, MD, PhD, Professor, Department of J. K. Seon, MD, PhD, Associate
K. B. Lee, N. Y. Cho, H. W. Park, J. K. Seon, S. H. Lee From Chonnam National University Medical School and Hospital, Gwangju, Korea K. B. Lee, MD, PhD, Professor, Department of J. K. Seon, MD, PhD, Associate
Alberta Health Care Insurance Plan. Schedule Of Anaesthetic Rates Applicable To Podiatry. Procedure List. As Of. 01 April Government of Alberta
 Alberta Health Care Insurance Plan Procedure List As Of 01 April 2017 Alberta Health Care Insurance Plan Page i Generated 2017/03/14 TABLE OF CONTENTS As of 2017/04/01 II. OPERATIONS ON THE NERVOUS SYSTEM.......................
Alberta Health Care Insurance Plan Procedure List As Of 01 April 2017 Alberta Health Care Insurance Plan Page i Generated 2017/03/14 TABLE OF CONTENTS As of 2017/04/01 II. OPERATIONS ON THE NERVOUS SYSTEM.......................
Midfoot - Reduction & Fixation - ORIF - screw fixation - AO Surgery Reference. ORIF - screw fixation
 Midfoot - TMT (Lisfranc) injury 1. Diagnosis ORIF - screw fixation Authors Mechanism of the injury Tarso-metatarsal (Lisfranc) injuries may be caused by direct or indirect forces. Direct forces include
Midfoot - TMT (Lisfranc) injury 1. Diagnosis ORIF - screw fixation Authors Mechanism of the injury Tarso-metatarsal (Lisfranc) injuries may be caused by direct or indirect forces. Direct forces include
METATARSUS ADDUCTUS/SOFT TISSU E
 METATARSUS ADDUCTUS/SOFT TISSU E RETEASE PROCEDURES Thomas F. Smith, D.P.M. Dennis Martin, D.P.M. INTRODUCTION lf caught early enough, a large majority of pediatric metatarsus adductus deformities are
METATARSUS ADDUCTUS/SOFT TISSU E RETEASE PROCEDURES Thomas F. Smith, D.P.M. Dennis Martin, D.P.M. INTRODUCTION lf caught early enough, a large majority of pediatric metatarsus adductus deformities are
A Patient s Guide to Hallux Rigidus
 A Patient s Guide to Hallux Rigidus Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Hallux Rigidus Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled from a variety
Correction System. Surgical Technique
 Re+Line Bunion Correction System Surgical Technique Bunion Correction System Easy insertion and medial placement accuracy using Landmark Guide technology 1 mm compression slot and fixed tines to encourage
Re+Line Bunion Correction System Surgical Technique Bunion Correction System Easy insertion and medial placement accuracy using Landmark Guide technology 1 mm compression slot and fixed tines to encourage
Fixation of first metatarsal basal osteotomy using Acutrak screw
 Available online at www.sciencedirect.com Foot and Ankle Surgery 14 (2008) 21 25 www.elsevier.com/locate/fas Fixation of first metatarsal basal osteotomy using Acutrak screw G.E. Fadel MD FRCS Tr & Orth*,
Available online at www.sciencedirect.com Foot and Ankle Surgery 14 (2008) 21 25 www.elsevier.com/locate/fas Fixation of first metatarsal basal osteotomy using Acutrak screw G.E. Fadel MD FRCS Tr & Orth*,
in the treatment of hallux valgus
 original ARTICLE Our experience with double metatarsal osteotomy in the treatment of hallux valgus Pradeep George Mathew, Pavel Šponer, Jaroslav Pavlata, Haroun Hassan Shaikh Charles University in Prague,
original ARTICLE Our experience with double metatarsal osteotomy in the treatment of hallux valgus Pradeep George Mathew, Pavel Šponer, Jaroslav Pavlata, Haroun Hassan Shaikh Charles University in Prague,
The Flower Medial Column Fusion Plate
 The Flower Medial Column Fusion Plate PROCEDURE GUIDE www.flowerortho.com The Flower Foot & Ankle Application NC FUSION PLATE 2-HOLE COMPRESSION PLATE TMT FUSION PLATE LAPIDUS FUSION PLATE COMPRESSION
The Flower Medial Column Fusion Plate PROCEDURE GUIDE www.flowerortho.com The Flower Foot & Ankle Application NC FUSION PLATE 2-HOLE COMPRESSION PLATE TMT FUSION PLATE LAPIDUS FUSION PLATE COMPRESSION
Surgical Strategies: Ludloff First Metatarsal Osteotomy
 FOOT &ANKLE INTERNATIONAL Copyright 2007 by the American Orthopaedic Foot & Ankle Society, Inc. DOI: 10.3113/FAI.2007.0025 Surgical Strategies: Ludloff First Metatarsal Osteotomy Su-Young Bae, M.D.; Lew
FOOT &ANKLE INTERNATIONAL Copyright 2007 by the American Orthopaedic Foot & Ankle Society, Inc. DOI: 10.3113/FAI.2007.0025 Surgical Strategies: Ludloff First Metatarsal Osteotomy Su-Young Bae, M.D.; Lew