Poliomyelitis: Splints for the Upper Extremity
|
|
|
- Caroline Flynn
- 6 years ago
- Views:
Transcription
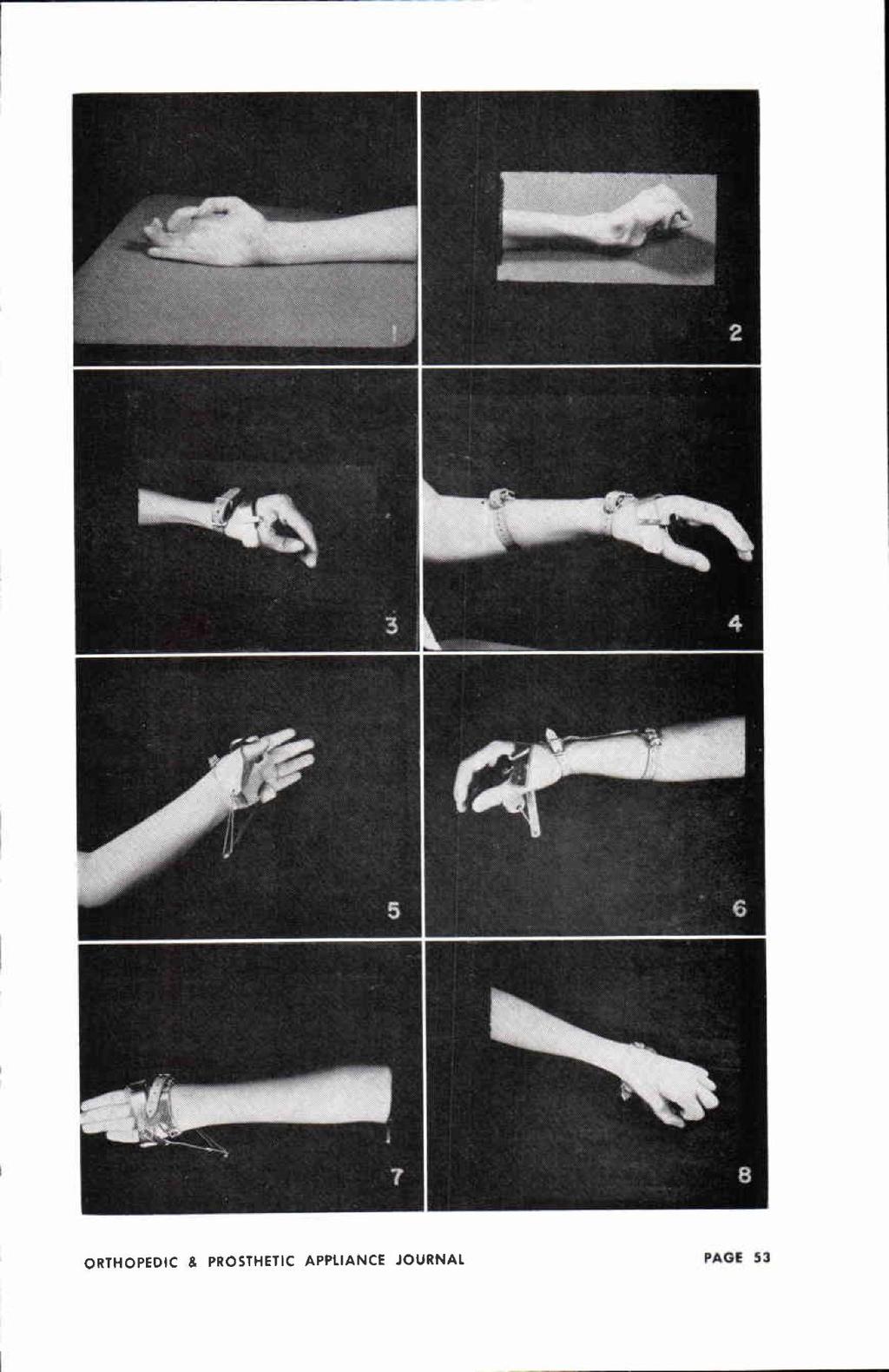
1 Poliomyelitis: Splints for the Upper Extremity By C.E. IRWIN, M.D. Atlanta, Ga. The splints to be discussed in this presentation are designed and used for therapeutic reasons only. They are in no sense recommended as permanent assistive or supportive equipment. The author through experience has learned that a patient with upper extremity involvement will develop ingenious substitution patterns and will of his own accord discard the equipment. It is conspicuous and often a hindrance rather than a help to him in carrying out the necessary every-day activities. We, as orthopedic surgeons, should thoroughly evaluate these individuals and carry out the necessary operative procedures to make them as independent and dextrous as possible without the need of any apparatus. A therapeutic splint may be classed as supportive, assistive and corrective. A single splint may fulfill one or a combination of two or more of these basic needs. A splint used preoperatively may be used for support and assistance postoperatively as the need for assistance and support remains the same as it was prior to surgery. Splints may be static or dynamic in use and design. Dynamic splinting should be used when possible. This principle provides both support and assistance for a weakened muscle or a weakened segment and allows motion and use of a weakened or transferred muscle in a manner approaching that for which it was normally intended. The splint should be simple in design, light in weight and constructed so that it can be easily applied and removed for necessary physical therapy. Rigid supports or plaster casts worn twenty-four hours a day are definitely contraindicated, particularly for the hand. This discussion will be concerned with splints for the thumb, for the intrinsics of the digits other than the thumb, the long finger extensors and flexors, the wrist, the elbow and the shoulder. The Thumb In the presence of weakness or paralysis of the thenar intrinsic musculature, the thumb will assume a position of adduction, hyperextension and external rotation or supination (fig. 1). Unless the thumb is properly splinted during convalescence, the following deformities will result: It will become contracted in adduction and external rotation or supination. Second, prolonged hyperextension of the thumb metacarpal will result in attenuation of the palmar portion of the capsule of the carpometacarpal joint. This important joint becomes unstable (fig. 2). Third, in the adducted and externally rotated thumb the long extensor will gradually migrate into the web space between the thumb and index metacarpal, resulting in ulnar deviation of the phalanges on the metacarpal. The patient uses the long extensor as an adductor and not as a true extensor of the distal phalanx (figs. 3, 4, 5, 6. 7 and 8). * The majority of this material and photographs was previously published in the American Academy of Orthopaedic Surgeons, Instructional Course Lectures, Vol. IX, Ann Arbor, J. W. Edwards, 1952, under the title "Apparatus for the Upper Extremity Disabled by Poliomyelitis," by C. E. Irwin, M.D. This is being reproduced with the permission of the American Academy of Orthopaedic Surgeons and J. W. Edwards, Inc.
2 Intrinsic Musculature of the Digits Other Than the Thumb The important intrinsic muscles provide both an extensor and a flexor component for the fingers. (The abduction component will be discussed with the index finger.) (fig. 9) For the purpose of discussing splints, one may say that the intrinsic muscles initiate and are the chief extensors of the distal two phalanges. The extrinsic flexor profundi and sublimi are the moderators of this component. For the same reason one may say that the intrinsic muscles initiate and are the chief flexors of the proximal phalanges. The extrinsic common extensors are the moderators of this component (fig. 10). The extrinsic extensors are not the primary extensors of the distal phalanges, nor are the extrinsic profundi and sublimi the primary flexors of the proximal phalanges. Skilled function of the fingers depends on proper balance between these two moderated groups of muscles. Appropriate dynamic splinting is important for these muscles both during the convalescent stage of the disease and for postoperative support and assistance following certain muscle transfers (figs , 13, 14 and 15). Instinsic Musculature of the Index Finger The function of the intrinsic muscles of the index finger differs from that of the other digits (figs. 16 and 17). The abductor function of the first dorsal interosseus muscle is highly developed and plays an important part in increasing the horizontal inter-tip space between the index and fifth fingers. Unlike the other intrinsics, it inserts chiefly into bone rather than into the lateral band. LEGENDS THUMB 1. Typical position assumed by the thumb in the presence of paralyzed or weak intrinsic musculature. The thumb assumes a position of external rotation, adduction and extension. Unless properly splinted, the thumb will become contracted in this position. 2. A typical long-standing thumb deformity due to paralysis of the thenar musculature. Note attenuation of the palmar portion of the capsule of the carpometacarpal joint and migration of the long extensor tendon into the web space. Patient has been using the long extensor as an adductor. There is ulnar deviation of the phalanges on the thumb metacarpal. Early proper splinting would have prevented this deformity. 3. A short opponens splint with a C spreader between the thumb and index metacarpal. This splint will prevent external rotation and adduction but will not fully restore pronation. The wrist musculature must be well balanced for the use of a short splint. 4. The same splint shown in figure 3 except it has an extension for support of the wrist. This is a basic opponens splint on which any other assistive or supportive apparatus may be attached. 5. Palmar view of an opponens splint with traction on the metacarpophalangeal joint. This is designed to stretch out contractures underlying the web space. Traction is motivated by rubber bands. 6. Radial view of an opponens splint with traction on the proximal phalanx. It is forcing the thumb in abduction and some flexion at the metacarpophalangeal joint. This is the splint routinely used following surgery as patients have a tendency to develop limitation of motion, particularly in flexion, of the metacarpophalangeal joint. The splint is applied seven days after surgery, at which time physical therapy is instituted. 7. Dorsal view of the same splint showing the method of attaching the traction bar. Note that the line of pull is in the direction of the pisiform bone parallel to the transferred tendon to the thumb. 8. A plastic splint used for postoperative immobilization of the metacarpophalangeal joint following arthrodesis. Motion in the carpometacarpal joint and in the interphalangeal joint may be instituted three weeks after surgery if the arthrodesis has been immobilized by a Kirschner wire.
3
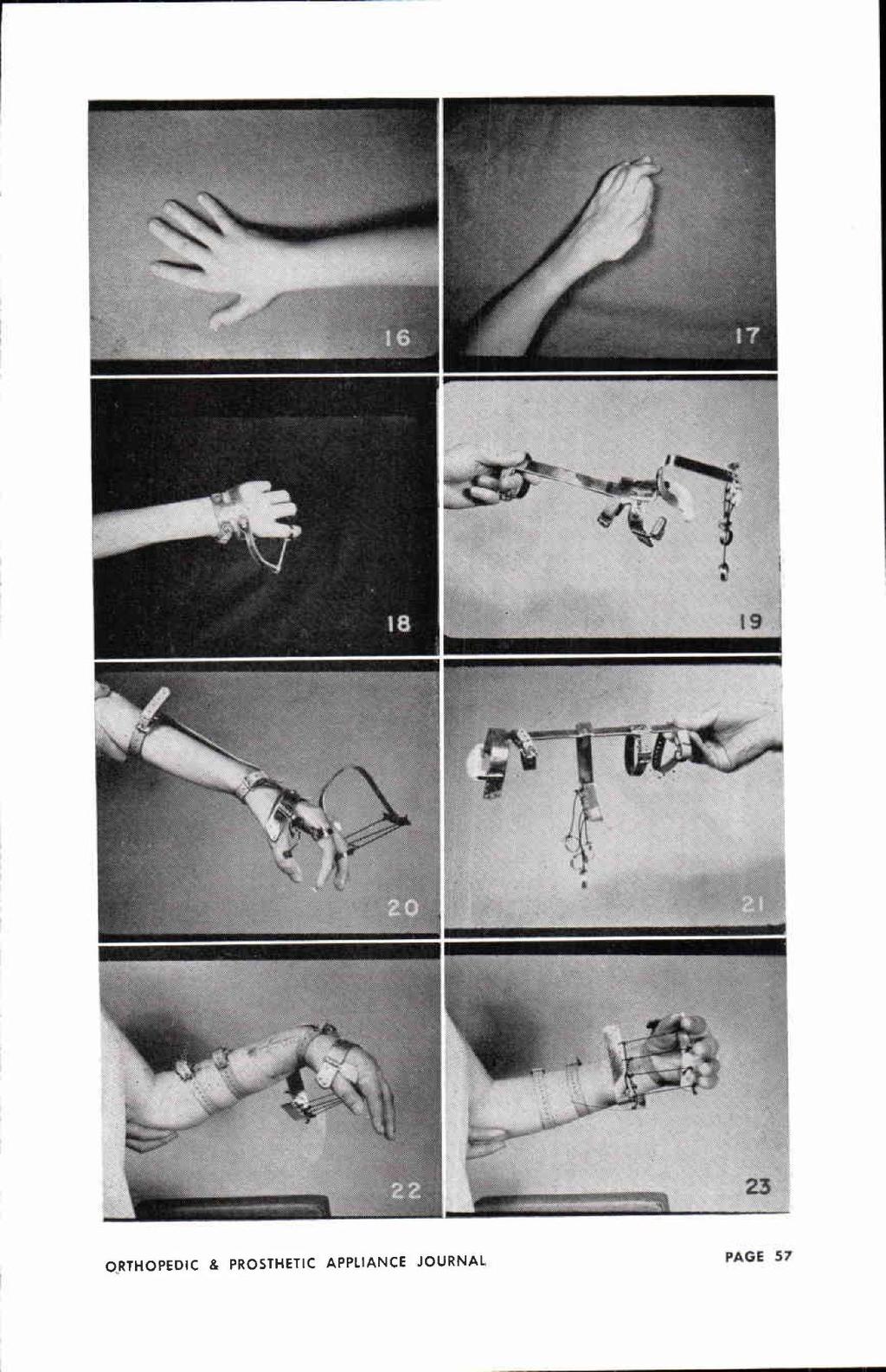
4 It does not ordinarily aid in extending the distal phalanges but is a strong abductor, a flexor, and an important stabilizer of the metacarpophalangeal joint, important for effective pinch. Supportive and assistive splinting for this finger should be dynamic (fig. 18). Long Finger Extensor When the wrist is extended 180 degrees or more, the common extensor extends only the proximal phaonstrate an effective corrective splint langes. The following figures demlanges (figs. 19 and 20). The distal attached to the basic opponens splint phalanges are extended by the intrinsics (figs. when 25, the 26 wrist and is in 27). this posi It can be tion. When the wrist is flexed or dropped, the long extensor can extend the distal phalanges by tenodesis action through the central slips. Long Finger Flexors The flexor profundi and sublimi are flexors of the distal phalanges and augment the flexor component of the intrinsics on the proximal phalanges (figs. 21, 22 and 23). Grasp is strongest when the wrist is extended or slightly hyperextended. Fixed Deformities of the Digits Weak intrinsic muscles which have been neglected as regards proper splinting will develop fixed flexion contractures of the distal phalanges and hyperextension contracture of the proximal phalanges fixed claw hand (fig. 24). These contractures must be overcome prior to intrinsic transfers. Continuous corrective force by a rigid plaster cast cannot be tolerated due to painful pressure on the palmar surfaces of the distal pha easily removed for periods of rest, manual stretching, and other physical therapy measures. The Wrist Splints for the wrist present no problem and nothing of particular interest (fig. 28). Dropped wrist is fairly common and may be associated with radial or ulnar deviation, depending on the distribution of muscle weakness. A static splint for support only is ordinarily used for convalescent care in our clinic and is shown in the following figures (figs. 29, 30, 31 and 32). LEGENDS INTRINSICS 9. This is the position the fingers assume at the end of forceful contraction of the intrinsic musculature. The long extensors and flexors, the moderators of the intrinsic function, are at their maximum resting length. 10. This is the position the fingers assume at the end of forceful contraction of the extrinsic musculature. The intrinsics, the moderators of the function of these muscles, are at their maximum resting length. 11. A basic opponens splint with wrist extension, the frame of which serves as the foundation on which one may attach an out-rigger for splinting the intrinsic musculature or for splinting the flexion or extension of the extrinsic musculature. 12. The intrinsic or extrinsic assembly which can easily be snapped into position on the dorsum of the basic opponens splint. The dynamic portion of the splint is motivated by rubber bands. Note the bar which prevents hyperextension at the metacarpophalangeal joint. 13. The apparatus in figures 11 and 12 assembled as one piece. The flexion component of the splint represented by the bar is static. The extension component motivated by the rubber bands is dynamic. 14. Dorsal view of an intrinsic splint in position on a patient. Notice the transverse bar maintaining the metacarpophalangeal joints in a flexed position and the traction on the extension component of the intrinsics distally. 15. Radial view of the splint just described. In addition, traction has been provided for the long thumb extensor, which is dynamic in character. This entire apparatus can be dissembled and reapplied very easily.

5 Figs. 9-15, Intrinsics. See captions, bottom poge 54.
6 The Elbow Inability to flex the forearm on the arm constitutes a real handicap, particularly for the patients with bilateral involvement (fig. 33). These individuals may be able to use the hands on flat table surfaces for most anything they wish, but, being unable to get their bands to their face level, they cannot feed themselves, brush their teeth, shave, and comb their hair, and are deprived of many other functions ordinarily taken for granted. The following figures show a very efficient assistive piece of apparatus which enables the patient to get his hand to the face level although he has no muscles to flex the forearm on the arm. With the apparatus the forearm can be flexed by depressing the shoulder or shifting the body weight toward the involved side. The principle may be used on a flat table surface or as a part of an assistive overhead sling (figs. 34 and 25). Some of these patients may be freed of apparatus by a Bunnell modification of the Steindler flexorplasty. The Shoulder Splinting of the shoulder weakened by poliomyelitis is a controversial subject. Three possible component disabilities of a weakened shoulder must be considered. These components are: (1) the abductors, (2) the rotator cuff, and (3) the shoulder depressors. If one keeps in mind the above three possible component disabilities and will accept the premise that a weakened muscle is done no harm if it is supported at a point of its maximum resting length, then the time-honored use of abduction or airplane splints for all weakened shoulders is not always applicable (figs 36 and 37). LEGENDS INDEX FINGER 16. The position assumed by the index finger due to loss of power in the first dorsal interosseus muscle. Note the ulnar deviation of the phalanges on the index metacarpal. 17. Ineffective pinch in the presence of weakness of the first dorsal interosseus. Here again, note the ulnar deviation of the proximal phalanx on the metacarpal. The index finger also lacks the flexion component of the intrinsic musculature. There is also loss of opposition. 18. A dynamic splint or support for first dorsal interosseus weakness or following transfer to restore function of the first dorsal interosseus muscle. The flexion component of the intrinsics is weak. The splint can be made to pull in radial adduction and flexion. LEGENDS EXTRINSIC EXTENSION 19. A basic opponens splint with an out-rigger for support of weak common extension, or for stretching out contractures of the profundi or sublimi. 20. The apparatus in position on the patient. Note the cross bar to prevent hyperextension of the metacarpophalangeal joints. The line of pull is from a point to stretch the sublimi. EXTRINSIC FLEXION 21. The foundation that fits on the dorsum of the forearm, wrist and hand for support of weak finger flexion, or for overcoming contractures of the long extensors. 22. A patient in the splint just described following transfer of the brachioradialis into the profundi. 23. Palmar view of the same splint. Note the curved bar under the metacarpal heads.
7

8 CONTRACTURE OF LONG FLEXORS 24. Contracture of the long finger extensors and the long finger flexors in the presence of paralysis of the intrinsic musculature. 25. Finger portion of a corrective splint to overcome contractures of the sublimi and profundi. 26. Dorsal view of the splint in position. The counter-thrust bar on the proximal phalanges fits the contour of the fingers. Note the residual flexion contracture in the profoundi. 27. Radial side view of the same splint in position on the patient. This splint can be easily removed and reapplied for the necessary daily physical therapy.

9 LEGENDS WRIST DROP 28. A typical drop wrist due to absence or weakness of all musculature on the extensor aspect of the forearm and hand. 29. A simple cock-up spint with palmar support that fits the contour of the normal palm. 30. Palmar view of the cock-up splint in position on the patient. 31. A supportive drop wrist splint with transverse bar, which can be molded to fit the contour of the palm and turned up into either the radial or the ulnar side to prevent radial or ulnar deviation. 32. Splint in position on the patient.

10 STAND FEEDERS 33. Patient with insufficient musculature to flex the forearm on the arm. She can use her hand very well on the flat surface of a raised lap board, but is completely helpless for functions at face level. 34. A stand feeder. The forearm rests in a trough portion of the apparatus, the flexed elbow projects backward. The hinge at the upright allows the apparatus to tilt upward or downward. Free movement between the rod and tubing allows inward and outward motion. 35. Patient shown in figure 34 using the stand feeder. The apparatus is operated by elevating or depressing the shoulder or shifting the upper trunk away from or toward the apparatus. OVER-HEAD SLINGS 36. A side view of the raised lap board, bilateral over-head slings, suspension feeder all assembled on an ordinary wheel chair. This apparatus makes it possible for a patient with weak forearm flexors to carry out many functions otherwise impossible. 37. Over-head slings in position on the patient. For weak anterior shoulder the forearm is suspended at a point distal to the upright. For posterior shoulder weakness it is suspended at a point more proximal to the upright.
Intrinsic muscles palsies of the hand Management of Thumb Opposition with BURKHALTER s Procedure
 Intrinsic muscles palsies of the hand Management of Thumb Opposition with BURKHALTER s Procedure TRUONG LE DAO, MD, IFAAD 1 Burkhalter W.E, Cristhensen R.C, Brown P.W, Extensor Indicis Proprius opponensplasty
Intrinsic muscles palsies of the hand Management of Thumb Opposition with BURKHALTER s Procedure TRUONG LE DAO, MD, IFAAD 1 Burkhalter W.E, Cristhensen R.C, Brown P.W, Extensor Indicis Proprius opponensplasty
Main Menu. Wrist and Hand Joints click here. The Power is in Your Hands
 1 The Wrist and Hand Joints click here Main Menu K.5 http://www.handsonlineeducation.com/classes/k5/k5entry.htm[3/23/18, 1:40:40 PM] Bones 29 bones, including radius and ulna 8 carpal bones in 2 rows of
1 The Wrist and Hand Joints click here Main Menu K.5 http://www.handsonlineeducation.com/classes/k5/k5entry.htm[3/23/18, 1:40:40 PM] Bones 29 bones, including radius and ulna 8 carpal bones in 2 rows of
Muscles of the hand Prof. Abdulameer Al-Nuaimi
 Muscles of the hand Prof. Abdulameer Al-Nuaimi a.alnuaimi@sheffield.ac.uk abdulameerh@yahoo.com Thenar Muscles Thenar muscles are three short muscles located at base of the thumb. All are innervated by
Muscles of the hand Prof. Abdulameer Al-Nuaimi a.alnuaimi@sheffield.ac.uk abdulameerh@yahoo.com Thenar Muscles Thenar muscles are three short muscles located at base of the thumb. All are innervated by
GENERAL EXERCISES THUMB, WRIST, HAND BMW MANUFACTURING CO. PZ-AM-G-US I July 2017
 GENERAL EXERCISES THUMB, WRIST, HAND BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only
GENERAL EXERCISES THUMB, WRIST, HAND BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only
Nerves of Upper limb. Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh
 Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Metacarpophalangeal Joint Implant Arthroplasty REHABILITATION PROTOCOL
 Andrew McNamara, MD The Orthopaedic and Fracture Clinic 1431 Premier Drive Mankato, MN 56001 507-386-6600 Metacarpophalangeal Joint Implant Arthroplasty REHABILITATION PROTOCOL Patient Name: Date: Diagnosis:
Andrew McNamara, MD The Orthopaedic and Fracture Clinic 1431 Premier Drive Mankato, MN 56001 507-386-6600 Metacarpophalangeal Joint Implant Arthroplasty REHABILITATION PROTOCOL Patient Name: Date: Diagnosis:
10/10/2014. Structure and Function of the Hand. The Hand. Osteology of the Hand
 Structure and Function of the Hand 19 bones and 19 joints are necessary to produce all the motions of the hand The Hand Dorsal aspect Palmar aspect The digits are numbered 1-5 Thumb = #1 Little finger
Structure and Function of the Hand 19 bones and 19 joints are necessary to produce all the motions of the hand The Hand Dorsal aspect Palmar aspect The digits are numbered 1-5 Thumb = #1 Little finger
Hand Anatomy A Patient's Guide to Hand Anatomy
 Hand Anatomy A Patient's Guide to Hand Anatomy Introduction Few structures of the human anatomy are as unique as the hand. The hand needs to be mobile in order to position the fingers and thumb. Adequate
Hand Anatomy A Patient's Guide to Hand Anatomy Introduction Few structures of the human anatomy are as unique as the hand. The hand needs to be mobile in order to position the fingers and thumb. Adequate
Clinical examination of the wrist, thumb and hand
 Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.
 Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.") MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
Nerve Injury. 1) Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.
 Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.") Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Elbow Exercise Program
 Elbow Exercise Program Name: Date: Diagnosis: Date of Surgery: 1. Deep Friction Massage deep transverse friction across area of elbow that is sore. 5 minutes, several times daily. 2. Grip grip apparatus,
Elbow Exercise Program Name: Date: Diagnosis: Date of Surgery: 1. Deep Friction Massage deep transverse friction across area of elbow that is sore. 5 minutes, several times daily. 2. Grip grip apparatus,
Classification of Established Volkmann s Ischemic Contracture and the Program for Its Treatment
 10 Classification of Established Volkmann s Ischemic Contracture and the Program for Its Treatment In spite of the advances made in preventive treatment of muscular ischemia at the forearm and hand, there
10 Classification of Established Volkmann s Ischemic Contracture and the Program for Its Treatment In spite of the advances made in preventive treatment of muscular ischemia at the forearm and hand, there
Physical therapy of the wrist and hand
 Physical therapy of the wrist and hand Functional anatomy wrist and hand The wrist includes distal radius, scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, and hamate. The hand includes
Physical therapy of the wrist and hand Functional anatomy wrist and hand The wrist includes distal radius, scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, and hamate. The hand includes
ARM Brachium Musculature
 ARM Brachium Musculature Coracobrachialis coracoid process of the scapula medial shaft of the humerus at about its middle 1. flexes the humerus 2. assists to adduct the humerus Blood: muscular branches
ARM Brachium Musculature Coracobrachialis coracoid process of the scapula medial shaft of the humerus at about its middle 1. flexes the humerus 2. assists to adduct the humerus Blood: muscular branches
Reversing PIP Joint Contractures:
 Reversing PIP Joint Contractures: Applicability of the Digit Widget External Fixation System John M. Agee M.D. Reversing PIP Joint Contractures: Applicability of the Digit Widget External Fixation System
Reversing PIP Joint Contractures: Applicability of the Digit Widget External Fixation System John M. Agee M.D. Reversing PIP Joint Contractures: Applicability of the Digit Widget External Fixation System
The hand is full with sweat glands, activated at times of stress. In Slide #2 there was a mistake where the doctor mentioned lateral septum twice.
 We should only know: Name, action & nerve supply Layers - Skin - Superficial fascia - Deep fascia The hand is full with sweat glands, activated at times of stress. Deep fascia In Slide #2 there was a mistake
We should only know: Name, action & nerve supply Layers - Skin - Superficial fascia - Deep fascia The hand is full with sweat glands, activated at times of stress. Deep fascia In Slide #2 there was a mistake
SUSPECTS THE UNUSUAL. Often-Overlooked Muscles. Sternohyoid, longus colli, and longus capitis. Flexor pollicis longus.
 THE UNUSUAL SUSPECTS Often-Overlooked Muscles By Joseph E. Muscolino, DC Sternohyoid, longus colli, and longus capitis Flexor pollicis longus Quadratus femoris 52 massage & bodywork november/december 2016
THE UNUSUAL SUSPECTS Often-Overlooked Muscles By Joseph E. Muscolino, DC Sternohyoid, longus colli, and longus capitis Flexor pollicis longus Quadratus femoris 52 massage & bodywork november/december 2016
THROWERS TEN EXERCISE PROGRAM
 THROWERS TEN EXERCISE PROGRAM The Thrower s Ten Program is designed to exercise the major muscles necessary for throwing. The Program s goal is to be an organized and concise exercise program. In addition,
THROWERS TEN EXERCISE PROGRAM The Thrower s Ten Program is designed to exercise the major muscles necessary for throwing. The Program s goal is to be an organized and concise exercise program. In addition,
Kinesiology of The Wrist and Hand. Cuneyt Mirzanli Istanbul Gelisim University
 Kinesiology of The Wrist and Hand Cuneyt Mirzanli Istanbul Gelisim University Bones The wrist and hand contain 29 bones including the radius and ulna. There are eight carpal bones in two rows of four to
Kinesiology of The Wrist and Hand Cuneyt Mirzanli Istanbul Gelisim University Bones The wrist and hand contain 29 bones including the radius and ulna. There are eight carpal bones in two rows of four to
Body Planes & Positions
 Learning Objectives Objective 1: Identify and utilize anatomical positions, planes, and directional terms. Demonstrate what anatomical position is and how it is used to reference the body. Distinguish
Learning Objectives Objective 1: Identify and utilize anatomical positions, planes, and directional terms. Demonstrate what anatomical position is and how it is used to reference the body. Distinguish
Wrist and Hand Anatomy
 Wrist and Hand Anatomy Bone Anatomy Scapoid Lunate Triquetrium Pisiform Trapeziod Trapezium Capitate Hamate Wrist Articulations Radiocarpal Joint Proximal portion Distal portion Most surface contact found
Wrist and Hand Anatomy Bone Anatomy Scapoid Lunate Triquetrium Pisiform Trapeziod Trapezium Capitate Hamate Wrist Articulations Radiocarpal Joint Proximal portion Distal portion Most surface contact found
Small muscles of the hand
 By the name of Allah Small muscles of the hand Revision: The palmar aponeurosis is triangular in shape with apex and base. It is divided into 4 bands that radiate to the medial four fingers. Dupuytren
By the name of Allah Small muscles of the hand Revision: The palmar aponeurosis is triangular in shape with apex and base. It is divided into 4 bands that radiate to the medial four fingers. Dupuytren
Key Points for Success:
 SELF WRIST & HAND 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Sit comfortably in a position where you can straighten or fully extend
SELF WRIST & HAND 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Sit comfortably in a position where you can straighten or fully extend
Hands PA; Obl. Lat.; Norgaard s Thumb AP; Lat. PA. PA; Lat.: Obls.; Elongated PA with ulnar deviation
 Projections Region Basic projections Additional / Modified projections Upper Limbs Hands PA; Obl. Lat.; Norgaard s Thumb ; Lat. PA Fingers PA; Lat. Wrist PA; Lat. Obls. Scaphoid Lunate Trapezium Triquetral
Projections Region Basic projections Additional / Modified projections Upper Limbs Hands PA; Obl. Lat.; Norgaard s Thumb ; Lat. PA Fingers PA; Lat. Wrist PA; Lat. Obls. Scaphoid Lunate Trapezium Triquetral
The Muscular System. Chapter 10 Part C. PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College
 Chapter 10 Part C The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.9: Muscles Crossing the Shoulder
Chapter 10 Part C The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.9: Muscles Crossing the Shoulder
THROWER S TEN EXERCISE PROGRAM David Andrew Parker, MD
 THROWER S TEN EXERCISE PROGRAM David Andrew Parker, MD The thrower s ten exercise program has been designed to exercise the major muscles necessary to return to throwing. The program s goal is to be an
THROWER S TEN EXERCISE PROGRAM David Andrew Parker, MD The thrower s ten exercise program has been designed to exercise the major muscles necessary to return to throwing. The program s goal is to be an
TALLGRASS ORTHOPEDIC & SPORTS MEDICINE THROWING ATHLETE EXERCISE PROGRAM TALLGRASSORTHOPEDICS.COM
 TALLGRASS ORTHOPEDIC & SPORTS MEDICINE THROWING ATHLETE EXERCISE PROGRAM TALLGRASSORTHOPEDICS.COM Patient Name: Date of Surgery: General Principles: The Throwing Athlete Exercise Program is designed to
TALLGRASS ORTHOPEDIC & SPORTS MEDICINE THROWING ATHLETE EXERCISE PROGRAM TALLGRASSORTHOPEDICS.COM Patient Name: Date of Surgery: General Principles: The Throwing Athlete Exercise Program is designed to
Ligaments of Elbow hinge: sagittal plane so need lateral and medial ligaments
 Ligaments of Elbow hinge: sagittal plane so need lateral and medial ligaments Ulnar Collateral ligament on medial side; arising from medial epicondyle and stops excess valgus movement (lateral movement)
Ligaments of Elbow hinge: sagittal plane so need lateral and medial ligaments Ulnar Collateral ligament on medial side; arising from medial epicondyle and stops excess valgus movement (lateral movement)
Throwers Ten Exercise Program
 The Thrower s Ten Program is designed to exercise the major muscles necessary for throwing. The Program s goal is to be an organized and concise exercise program. In addition, all exercises included are
The Thrower s Ten Program is designed to exercise the major muscles necessary for throwing. The Program s goal is to be an organized and concise exercise program. In addition, all exercises included are
Fractures of the Hand in Children Which are simple? And Which have pitfalls??
 Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
D: Doorway Stretch E: Towel Stretch for Pectoralis Minor Blackburn Exercises: 6 Positions A: Prone Horizontal Abduction (Neutral)
") D: Doorway Stretch Bring your shoulder into a horizontal position out to your side (abduction) and flex your elbow 90û Place your elbow against the edge of a doorway Lead forward and downwards with your
D: Doorway Stretch Bring your shoulder into a horizontal position out to your side (abduction) and flex your elbow 90û Place your elbow against the edge of a doorway Lead forward and downwards with your
Lab Activity 11: Group II
 Lab Activity 11: Group II Muscles Martini Chapter 11 Portland Community College BI 231 Origin and Insertion Origin: The place where the fixed end attaches to a bone, cartilage, or connective tissue. Insertion:
Lab Activity 11: Group II Muscles Martini Chapter 11 Portland Community College BI 231 Origin and Insertion Origin: The place where the fixed end attaches to a bone, cartilage, or connective tissue. Insertion:
Institute of Reconstructive Surgery, Sofia, Bulgaria
 TRANSPOSITION OF THE LATERAL SLIPS OF THE APONEUROSIS IN TREATMENT OF LONG-STANDING " BOUTONNIERE DEFORMITY " OF THE FINGERS By IVAN MATEV Institute of Reconstructive Surgery, Sofia, Bulgaria RUPTURE of
TRANSPOSITION OF THE LATERAL SLIPS OF THE APONEUROSIS IN TREATMENT OF LONG-STANDING " BOUTONNIERE DEFORMITY " OF THE FINGERS By IVAN MATEV Institute of Reconstructive Surgery, Sofia, Bulgaria RUPTURE of
A Clinicians Guide To The Active Movement Scale (AMS) An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy
 An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy") A Clinicians Guide To The Active Movement Scale (AMS) An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy Table of Contents Introduction.. 3 Active Movement Scale 4 AMS Evaluation Form.
A Clinicians Guide To The Active Movement Scale (AMS) An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy Table of Contents Introduction.. 3 Active Movement Scale 4 AMS Evaluation Form.
"Zero-Position" Functional Shoulder Orthosis for Postoperative. management of rotator cuff injuries.
 "Zero-Position" Functional Shoulder Orthosis for Postoperative Management of Rotator Cuff Injuries Jiro Ozaki, M.D. Ichiro Kawamura INTRODUCTION Many shoulder orthoses such as the airplane splint, the
"Zero-Position" Functional Shoulder Orthosis for Postoperative Management of Rotator Cuff Injuries Jiro Ozaki, M.D. Ichiro Kawamura INTRODUCTION Many shoulder orthoses such as the airplane splint, the
S that will permit necessary functional use but prevent most of the persistent
 CURRENT COMMENT Orthetic Devices to Prevent Deformities of the Hand in Rheumatoid Arthritis By ROBERT L. BENNETT IMPLE ORTHETIC DEVICES can be made for the fingers and thumb S that will permit necessary
CURRENT COMMENT Orthetic Devices to Prevent Deformities of the Hand in Rheumatoid Arthritis By ROBERT L. BENNETT IMPLE ORTHETIC DEVICES can be made for the fingers and thumb S that will permit necessary
GENERAL EXERCISES ELBOW BMW MANUFACTURING CO. PZ-AM-G-US I July 2017
 GENERAL EXERCISES ELBOW BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to be
GENERAL EXERCISES ELBOW BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to be
WRIST SPRAIN. Description
 WRIST SPRAIN Description Other sports, such as skiing, bowling, pole vaulting Wrist sprain is a violent overstretching and tearing of one Poor physical conditioning (strength and flexibility) or more ligaments
WRIST SPRAIN Description Other sports, such as skiing, bowling, pole vaulting Wrist sprain is a violent overstretching and tearing of one Poor physical conditioning (strength and flexibility) or more ligaments
ELBOW - 1 FLEXION: ROM (Supine / Sitting)
") ELBOW - 1 FLEXION: ROM (Supine / Sitting) Position (A) Patient: Place arm against side of trunk. Helper: Hold elbow to stabilize. (B) - Lift hand toward shoulder, palm up. - Keep wrist straight. Do sessions
ELBOW - 1 FLEXION: ROM (Supine / Sitting) Position (A) Patient: Place arm against side of trunk. Helper: Hold elbow to stabilize. (B) - Lift hand toward shoulder, palm up. - Keep wrist straight. Do sessions
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 The Stiff Hand: Boutonniere & Sylvia Dávila, PT, CHT San Antonio, Texas Extensor Mechanism Central slip inserts into base of the middle phalanx Lateral bands lie dorsal to the PIP joint center of rotation
The Stiff Hand: Boutonniere & Sylvia Dávila, PT, CHT San Antonio, Texas Extensor Mechanism Central slip inserts into base of the middle phalanx Lateral bands lie dorsal to the PIP joint center of rotation
Location Terms. Anterior and posterior. Proximal and Distal The term proximal (Latin proximus; nearest) describes where the appendage joins the body.
 describes where the appendage joins the body.") HUMAN ANAT OMY Location Terms Anterior and posterior In human anatomical usage, anterior refers to the front of the individual. Similarly, posterior refers to the back of the subject. In standard anatomical
HUMAN ANAT OMY Location Terms Anterior and posterior In human anatomical usage, anterior refers to the front of the individual. Similarly, posterior refers to the back of the subject. In standard anatomical
GOLFERS TEN PROGRAM 1. SELF STRETCHING OF THE SHOULDER CAPSULE
 GOLFERS TEN PROGRAM 1. SELF STRETCHING OF THE SHOULDER CAPSULE POSTERIOR CAPSULAR STRETCH Bring your arm across your chest toward the opposite shoulder. With the opposite arm grasp your arm at your elbow.
GOLFERS TEN PROGRAM 1. SELF STRETCHING OF THE SHOULDER CAPSULE POSTERIOR CAPSULAR STRETCH Bring your arm across your chest toward the opposite shoulder. With the opposite arm grasp your arm at your elbow.
medial half of clavicle; Sternum; upper six costal cartilages External surfaces of ribs 3-5
 MUSCLE ORIGIN INSERTION ACTION NERVE Pectoralis Major medial half of clavicle; Sternum; upper six costal cartilages Lateral lip of intertubercular groove of horizontal adduction Medial and lateral pectoral
MUSCLE ORIGIN INSERTION ACTION NERVE Pectoralis Major medial half of clavicle; Sternum; upper six costal cartilages Lateral lip of intertubercular groove of horizontal adduction Medial and lateral pectoral
Wrist & Hand Assessment and General View
 Wrist & Hand Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The hand can be divided
Wrist & Hand Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The hand can be divided
Biceps Brachii. Muscles of the Arm and Hand 4/4/2017 MR. S. KELLY
 Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
Terms of Movements by Prof. Dr. Muhammad Imran Qureshi
 Terms of Movements by Prof. Dr. Muhammad Imran Qureshi Three systems of the body work in coordination to perform various movements of the body. These are: A System of Bones (Osteology), A System of Muscles
Terms of Movements by Prof. Dr. Muhammad Imran Qureshi Three systems of the body work in coordination to perform various movements of the body. These are: A System of Bones (Osteology), A System of Muscles
THROWERS TEN EXERCISE PROGRAM
 Throwers Shoulder Home Exercise Program Clayton W. Nuelle, MD THROWERS TEN EXERCISE PROGRAM The throwers ten exercise program has been designed to exercise the major muscles necessary to return to throwing.
Throwers Shoulder Home Exercise Program Clayton W. Nuelle, MD THROWERS TEN EXERCISE PROGRAM The throwers ten exercise program has been designed to exercise the major muscles necessary to return to throwing.
BUNNELL. Expanded product line Customer service Please visit BunnellSplints.com Sizing information on back page WRIST HAND FINGER ORTHOSIS
 Established 1907 WENIGER Exclusive Manufacturer of BUNNELL WRIST HAND FINGER ORTHOSIS STATIC DYNAMIC STATIC PROGRESSIVE POSITIONING LATEX FREE SOFT STRAPS ORTHOSIS FITS RIGHT OR LEFT HAND Expanded product
Established 1907 WENIGER Exclusive Manufacturer of BUNNELL WRIST HAND FINGER ORTHOSIS STATIC DYNAMIC STATIC PROGRESSIVE POSITIONING LATEX FREE SOFT STRAPS ORTHOSIS FITS RIGHT OR LEFT HAND Expanded product
Medical Terminology. Unit 2
 Medical Terminology Unit 2 Students will apply medical terminology. Objective 1: Identify and utilize anatomical positions, planes, and directional terms. Demonstrate what anatomical position is and how
Medical Terminology Unit 2 Students will apply medical terminology. Objective 1: Identify and utilize anatomical positions, planes, and directional terms. Demonstrate what anatomical position is and how
Medical Terminology. Anatomical Position, Directional Terms and Movements
 Medical Terminology Anatomical Position, Directional Terms and Movements What we will cover... Content Objectives Students will be able to gain a better understanding and application of medical terminology
Medical Terminology Anatomical Position, Directional Terms and Movements What we will cover... Content Objectives Students will be able to gain a better understanding and application of medical terminology
Ascension. Silicone MCP surgical technique. surgical technique Ascension Silicone MCP
 Ascension Silicone MCP surgical technique WW 2 Introduction This manual describes the sequence of techniques and instruments used to implant the Ascension Silicone MCP (FIGURE 1A). Successful use of this
Ascension Silicone MCP surgical technique WW 2 Introduction This manual describes the sequence of techniques and instruments used to implant the Ascension Silicone MCP (FIGURE 1A). Successful use of this
Hand and Wrist Editing file. Color Code Important Doctors Notes Notes/Extra explanation
 Hand and Wrist Editing file Color Code Important Doctors Notes Notes/Extra explanation Objectives Describe the anatomy of the deep fascia of the wrist & hand (flexor & extensor retinacula & palmar aponeurosis).
Hand and Wrist Editing file Color Code Important Doctors Notes Notes/Extra explanation Objectives Describe the anatomy of the deep fascia of the wrist & hand (flexor & extensor retinacula & palmar aponeurosis).
NEWBORN NURSES POLICY AND PROCEDURES. PURPOSE: Varying positions helps to stimulate physiological functioning and provides rest.
 NEWBORN NURSES POLICY AND PROCEDURES SUBJECT: POSITIONING EFFECTIVE DATE: 6/91 PURPOSE: Varying positions helps to stimulate physiological functioning and provides rest. POLICY: 1. The nurse will vary
NEWBORN NURSES POLICY AND PROCEDURES SUBJECT: POSITIONING EFFECTIVE DATE: 6/91 PURPOSE: Varying positions helps to stimulate physiological functioning and provides rest. POLICY: 1. The nurse will vary
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/36343 holds various files of this Leiden University dissertation Author: Jong, Staas de Title: Computed fingertip touch for the instrumental control of
Cover Page The handle http://hdl.handle.net/1887/36343 holds various files of this Leiden University dissertation Author: Jong, Staas de Title: Computed fingertip touch for the instrumental control of
The Language of Anatomy. (Anatomical Terminology)
") The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
Sports Medicine Unit 16 Elbow
 Sports Medicine Unit 16 Elbow I. Bones a. b. c. II. What movements does the elbow perform? a. Flexion b. c. Pronation d. III. Muscles in motion a. FLEXION (supinated) i Brachialis (pronated) ii (neutral)
Sports Medicine Unit 16 Elbow I. Bones a. b. c. II. What movements does the elbow perform? a. Flexion b. c. Pronation d. III. Muscles in motion a. FLEXION (supinated) i Brachialis (pronated) ii (neutral)
The Golfers Ten Program. 1. Self Stretching of the Shoulder Capsule
 The Golfers Ten Program 1. Self Stretching of the Shoulder Capsule A. Posterior capsular stretch Bring your arm across your chest toward the opposite shoulder. With the opposite arm grasp your arm at your
The Golfers Ten Program 1. Self Stretching of the Shoulder Capsule A. Posterior capsular stretch Bring your arm across your chest toward the opposite shoulder. With the opposite arm grasp your arm at your
HAND SURGERY- GUIDELINES for POST-OP TREATMENT and REFERRAL to HAND THERAPY
 HAND SURGERY- GUIDELINES for POST-OP TREATMENT and REFERRAL to HAND THERAPY Please use the specific hand therapy referral form. Always give at least one telephone number for the patient so that there is
HAND SURGERY- GUIDELINES for POST-OP TREATMENT and REFERRAL to HAND THERAPY Please use the specific hand therapy referral form. Always give at least one telephone number for the patient so that there is
CHAPTER 6: THE UPPER EXTREMITY: THE ELBOW, FOREARM, WRIST, AND HAND
 CHAPTER 6: THE UPPER EXTREMITY: THE ELBOW, FOREARM, WRIST, AND HAND KINESIOLOGY Scientific Basis of Human Motion, 12 th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D.,
CHAPTER 6: THE UPPER EXTREMITY: THE ELBOW, FOREARM, WRIST, AND HAND KINESIOLOGY Scientific Basis of Human Motion, 12 th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D.,
Anatomy of the Upper Limb
 Anatomy of the Upper Limb Figure 53: The thenar & midpalmar spaces. The synovial (tendon) sheaths of the long flexors [Figure.54] These sheaths surround the tendons of the long flexors; flexor digitorum
Anatomy of the Upper Limb Figure 53: The thenar & midpalmar spaces. The synovial (tendon) sheaths of the long flexors [Figure.54] These sheaths surround the tendons of the long flexors; flexor digitorum
SaeboMAS (Patent Pending)
") SaeboMAS (Patent Pending) Product Manual Maximizing Function While Improving Proximal Strength No Plateau In Sight Introduction SaeboMAS dynamic mobile arm support system is a zero gravity upper extremity
SaeboMAS (Patent Pending) Product Manual Maximizing Function While Improving Proximal Strength No Plateau In Sight Introduction SaeboMAS dynamic mobile arm support system is a zero gravity upper extremity
Monster Walk Stand with your feet slightly closer than shoulder-width apart in an athletic stance. Loop an elastic band around your ankles.
 Off-season Lower-Body Tennis Exercises Research conducted on elite tennis players shows that lower-body strength is the same on both the left and right sides. Therefore, lower-body training for tennis
Off-season Lower-Body Tennis Exercises Research conducted on elite tennis players shows that lower-body strength is the same on both the left and right sides. Therefore, lower-body training for tennis
What is Kinesiology? Basic Biomechanics. Mechanics
 What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
The Elbow and Radioulnar Joints Kinesiology. Dr Cüneyt Mirzanli Istanbul Gelisim University
 The Elbow and Radioulnar Joints Kinesiology Dr Cüneyt Mirzanli Istanbul Gelisim University 1 The Elbow & Radioulnar Joints Most upper extremity movements involve the elbow & radioulnar joints. Usually
The Elbow and Radioulnar Joints Kinesiology Dr Cüneyt Mirzanli Istanbul Gelisim University 1 The Elbow & Radioulnar Joints Most upper extremity movements involve the elbow & radioulnar joints. Usually
Connects arm to thorax 3 joints. Glenohumeral joint Acromioclavicular joint Sternoclavicular joint
 Connects arm to thorax 3 joints Glenohumeral joint Acromioclavicular joint Sternoclavicular joint Scapula Elevation Depression Protraction (abduction) Retraction (adduction) Downward Rotation Upward Rotation
Connects arm to thorax 3 joints Glenohumeral joint Acromioclavicular joint Sternoclavicular joint Scapula Elevation Depression Protraction (abduction) Retraction (adduction) Downward Rotation Upward Rotation
An Improved Tenodesis Splint
 An Improved Tenodesis Splint By ARTHUR J. HEATHER, M.D. Medical Director, Eugene du Pont Memorial Hospital and Rehabilitation Center, Wilmington, Delaware and THOMAS A. SMITH Project Engineer, All American
An Improved Tenodesis Splint By ARTHUR J. HEATHER, M.D. Medical Director, Eugene du Pont Memorial Hospital and Rehabilitation Center, Wilmington, Delaware and THOMAS A. SMITH Project Engineer, All American
8 Recovering From HAND FRACTURE SURGERY
 8 Recovering From HAND FRACTURE SURGERY Hand fractures are caused by trauma and result in breaking (fracturing) the phalanges or metacarpals. Surgery involves achieving acceptable alignment and providing
8 Recovering From HAND FRACTURE SURGERY Hand fractures are caused by trauma and result in breaking (fracturing) the phalanges or metacarpals. Surgery involves achieving acceptable alignment and providing
9/26/2012. Osteokinematics (how the bones move) & Arthrokinematics (how the joints move) Planes & Axes. Planes & Axes continued
 & Arthrokinematics (how the joints move) Planes & Axes. Planes & Axes continued") Osteokinematics (how the bones move) & (how the joints move) Planes & Axes Planes of Action = Three fixed lines of reference along which the body is divided. Each plane is at right angles (or perpendicular)
Osteokinematics (how the bones move) & (how the joints move) Planes & Axes Planes of Action = Three fixed lines of reference along which the body is divided. Each plane is at right angles (or perpendicular)
A Dynalllic Splint for U se After Total Wrist Arthroplasty
 A Dynalllic Splint for U se After Total Wrist Arthroplasty (active-assistive therapy, post-operative splinting, rheumatoid arthritis) Barbara M. Johnson Mary Jean Gregory Flynn Robert D. Beckenbaugh Total
A Dynalllic Splint for U se After Total Wrist Arthroplasty (active-assistive therapy, post-operative splinting, rheumatoid arthritis) Barbara M. Johnson Mary Jean Gregory Flynn Robert D. Beckenbaugh Total
Hand injuries. The metacarpal bones may fracture through the base, shaft or the neck.
 Hand injuries Metacarpal injuries The metacarpal bones may fracture through the base, shaft or the neck. Shaft fractures; these are caused by direct trauma which may cause transverse # of one or more metacarpal
Hand injuries Metacarpal injuries The metacarpal bones may fracture through the base, shaft or the neck. Shaft fractures; these are caused by direct trauma which may cause transverse # of one or more metacarpal
Structure and Function of the Hand
 Structure and Function of the Hand Some say it takes a village to raise a child, but it takes 19 bones and 19 joints in the hand for it to function smoothly. The Hand Dorsal aspect 2 3 4 The digits are
Structure and Function of the Hand Some say it takes a village to raise a child, but it takes 19 bones and 19 joints in the hand for it to function smoothly. The Hand Dorsal aspect 2 3 4 The digits are
POSTERIOR 1. situated behind: situated at or toward the hind part of the body :
 ANATOMICAL LOCATION Anatomy is a difficult subject with a large component of memorization. There is just no way around that, but we have made every effort to make this course diverse and fun. The first
ANATOMICAL LOCATION Anatomy is a difficult subject with a large component of memorization. There is just no way around that, but we have made every effort to make this course diverse and fun. The first
SaeboGlove. Saebo INSTRUCTION MANUAL. New Era in Hand Rehabilitation
 SaeboGlove New Era in Hand Rehabilitation Saebo INSTRUCTION MANUAL Introduction Saebo is pleased to provide you with the latest innovation for hand rehabilitation. The SaeboGlove is a low profile functional
SaeboGlove New Era in Hand Rehabilitation Saebo INSTRUCTION MANUAL Introduction Saebo is pleased to provide you with the latest innovation for hand rehabilitation. The SaeboGlove is a low profile functional
Elbow, Wrist & Hand Evaluation.
 Elbow, Wrist & Hand Evaluation www.fisiokinesiterapia.biz Common Injuries to the Elbow, Wrist, Hand & Fingers Lateral epicondylitis tennis elbow Medial epicondylitis golfer s s elbow, little league elbow
Elbow, Wrist & Hand Evaluation www.fisiokinesiterapia.biz Common Injuries to the Elbow, Wrist, Hand & Fingers Lateral epicondylitis tennis elbow Medial epicondylitis golfer s s elbow, little league elbow
Phase 1 Maximum Protection 0-4 Weeks
 Dr. Schmidt CMC Arthroplasty When conservative treatment of thumb osteoarthritis fails to control pain surgical treatment may be indicated. The most common surgical technique involves complete resection
Dr. Schmidt CMC Arthroplasty When conservative treatment of thumb osteoarthritis fails to control pain surgical treatment may be indicated. The most common surgical technique involves complete resection
PIP Joint Injuries of the Finger A Patient's Guide to PIP Joint Injuries of the Finger
 PIP Joint Injuries of the Finger A Patient's Guide to PIP Joint Injuries of the Finger Introduction We use our hands constantly, placing them in harm's way continuously. Injuries to the finger joints are
PIP Joint Injuries of the Finger A Patient's Guide to PIP Joint Injuries of the Finger Introduction We use our hands constantly, placing them in harm's way continuously. Injuries to the finger joints are
The Rheumatoid Hand Deformities & Management. Dr. Anirudh Sharma Resident Department of Orthopedics
 + The Rheumatoid Hand Deformities & Management Dr. Anirudh Sharma Resident Department of Orthopedics + Why is Rheumatoid Arthritis important? + RA is a very debilitating disease median life expectancy
+ The Rheumatoid Hand Deformities & Management Dr. Anirudh Sharma Resident Department of Orthopedics + Why is Rheumatoid Arthritis important? + RA is a very debilitating disease median life expectancy
GENERAL EXERCISES SHOULDER BMW MANUFACTURING CO. PZ-AM-G-US I July 2017
 GENERAL EXERCISES SHOULDER BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to
GENERAL EXERCISES SHOULDER BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to
AROM of DIP flex/ext, 10 reps hourly.
 BRIGHAM AND WOMEN S HOSPITAL A Teaching Affiliate of Harvard Medical School 75 Francis St. Boston, Massachusetts 02115 Department of Rehabilitation Services Physical Therapy The intent of this protocol
BRIGHAM AND WOMEN S HOSPITAL A Teaching Affiliate of Harvard Medical School 75 Francis St. Boston, Massachusetts 02115 Department of Rehabilitation Services Physical Therapy The intent of this protocol
The Elbow and the cubital fossa. Prof Oluwadiya Kehinde
 The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
Definition of Anatomy. Anatomy is the science of the structure of the body and the relation of its parts.
 Definition of Anatomy Anatomy is the science of the structure of the body and the relation of its parts. Basic Anatomical Terms Anatomical terms for describing positions: Anatomical position: Supine position:
Definition of Anatomy Anatomy is the science of the structure of the body and the relation of its parts. Basic Anatomical Terms Anatomical terms for describing positions: Anatomical position: Supine position:
Module 7 - The Muscular System Muscles of the Arm and Trunk
 Module 7 - The Muscular System Muscles of the Arm and Trunk This Module will cover the muscle anatomy of the arms and trunk. We have already seen the muscles that move the humerus, so this module will
Module 7 - The Muscular System Muscles of the Arm and Trunk This Module will cover the muscle anatomy of the arms and trunk. We have already seen the muscles that move the humerus, so this module will
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Trapezium is by the thumb, Trapezoid is inside
 Trapezium is by the thumb, Trapezoid is inside Intercarpal Jt Radiocarpal Jt Distal Middle Proximal DIP PIP Interphalangeal Jts Metacarpalphalangeal (MCP) Jt Metacarpal Carpometacarpal (CMC) Jt Trapezium
Trapezium is by the thumb, Trapezoid is inside Intercarpal Jt Radiocarpal Jt Distal Middle Proximal DIP PIP Interphalangeal Jts Metacarpalphalangeal (MCP) Jt Metacarpal Carpometacarpal (CMC) Jt Trapezium
Chapter 6 part 2. Skeletal Muscles of the Body
 Chapter 6 part 2 Skeletal Muscles of the Body Basic Principles 600 + muscles in the human body (you are required to learn 45, lucky kids)! Skeletal Muscles pull on bones Origin of a muscle = point of attachment
Chapter 6 part 2 Skeletal Muscles of the Body Basic Principles 600 + muscles in the human body (you are required to learn 45, lucky kids)! Skeletal Muscles pull on bones Origin of a muscle = point of attachment
Interesting Case Series. Swan-Neck Deformity in Cerebral Palsy
 Interesting Case Series Swan-Neck Deformity in Cerebral Palsy Leyu Chiu, BA, a Nicholas S. Adams, MD, a,b and Paul A. Luce, MD, a,b,c a Michigan State University College of Human Medicine, Grand Rapids,
Interesting Case Series Swan-Neck Deformity in Cerebral Palsy Leyu Chiu, BA, a Nicholas S. Adams, MD, a,b and Paul A. Luce, MD, a,b,c a Michigan State University College of Human Medicine, Grand Rapids,
forearm posterior compartment
 Quick revision: The anterior compartment of the forearm contains of 8 muscles... -4 superficial -1 intermediate -3 deep *All supplied by median nerve except 1 and 1/2 muscle (by ulnar N.) forearm posterior
Quick revision: The anterior compartment of the forearm contains of 8 muscles... -4 superficial -1 intermediate -3 deep *All supplied by median nerve except 1 and 1/2 muscle (by ulnar N.) forearm posterior
Elbow Anatomy, Growth and Physical Exam. Donna M. Pacicca, MD Section of Sports Medicine Division of Orthopaedic Surgery Children s Mercy Hospital
 Elbow Anatomy, Growth and Physical Exam Donna M. Pacicca, MD Section of Sports Medicine Division of Orthopaedic Surgery Children s Mercy Hospital Contributing Factors to Elbow Injury The elbow is affected
Elbow Anatomy, Growth and Physical Exam Donna M. Pacicca, MD Section of Sports Medicine Division of Orthopaedic Surgery Children s Mercy Hospital Contributing Factors to Elbow Injury The elbow is affected
Sick Call Screener Course
 Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
2452 Lincolnway East Goshen, IN Toll Free: Phone:
 2452 Lincolnway East Goshen, IN 46526 Toll Free: 800.252.4909 Phone: 574.534.3418 Fax: 574.642.4546 E-mail: sales@darenind.com Orthopedic Products Catalog TABLE OF CONTENTS 1 Wrist and Forearm Splints
2452 Lincolnway East Goshen, IN 46526 Toll Free: 800.252.4909 Phone: 574.534.3418 Fax: 574.642.4546 E-mail: sales@darenind.com Orthopedic Products Catalog TABLE OF CONTENTS 1 Wrist and Forearm Splints
Wrist and Hand Anatomy/Biomechanics
 Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Orthopaedic Manual Physical Therapy Series 2017-2018 Anatomy -
Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Orthopaedic Manual Physical Therapy Series 2017-2018 Anatomy -
Anatomy - Hand. Wrist and Hand Anatomy/Biomechanics. Osteology. Carpal Arch. Property of VOMPTI, LLC
 Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT The wrist The metacarpals The Phalanges Digit 1 thumb Digit 5 digiti minimi Anatomy - Hand Orthopaedic Manual Physical Therapy Series
Wrist and Hand Anatomy/Biomechanics Kristin Kelley, DPT, OCS, FAAOMPT The wrist The metacarpals The Phalanges Digit 1 thumb Digit 5 digiti minimi Anatomy - Hand Orthopaedic Manual Physical Therapy Series
CASE ONE CASE ONE. RADIAL HEAD FRACTURE Mason Classification. RADIAL HEAD FRACTURE Mechanism of Injury. RADIAL HEAD FRACTURE Imaging
 CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
EPICONDYLITIS, LATERAL (Tennis Elbow)
") EPICONDYLITIS, LATERAL (Tennis Elbow) Description Expected Outcome Lateral epicondylitis (tennis elbow) is the most common painful condition of the elbow. Inflammation and pain occur on the outer side
EPICONDYLITIS, LATERAL (Tennis Elbow) Description Expected Outcome Lateral epicondylitis (tennis elbow) is the most common painful condition of the elbow. Inflammation and pain occur on the outer side
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint
 / Shoulder Joint") INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
Essential intervention No. 3 Oedema control KEY OBJECTIVES. Danger
 Essential intervention No. 3 Oedema control KEY OBJECTIVES To know what causes oedema. To know which kind of oedema needs to be referred for emergency surgery and why. To know the effects of oedema on
Essential intervention No. 3 Oedema control KEY OBJECTIVES To know what causes oedema. To know which kind of oedema needs to be referred for emergency surgery and why. To know the effects of oedema on
THROWERS' TEN EXERCISE PROGRAM
 _9~------------------------------------------------ THROWERS' TEN EXERCISE PROGRAM Kevin E. Wilk, P. T. The Throwers' Ten Exercise Program' is designed to exercise the major muscles necessary for throwing.
_9~------------------------------------------------ THROWERS' TEN EXERCISE PROGRAM Kevin E. Wilk, P. T. The Throwers' Ten Exercise Program' is designed to exercise the major muscles necessary for throwing.