Is inhalational induction justifiable in paediatric emergencies? Richard Craig Alder Hey Children s Hospital
|
|
|
- Amos Dickerson
- 5 years ago
- Views:
Transcription
1 Is inhalational induction justifiable in paediatric emergencies? Richard Craig Alder Hey Children s Hospital

2 The beginning of wisdom is the definition of terms. Socrates


3 If you wish to converse with me, said Voltaire, define your terms. Will Durant The story of philosophy Chapter 2 part 3: the foundation of logic, page 59

4 Emergencies A B C Intervention required within 24 hours
5 Anatomical Airway Obstruction Principle: maintain spontaneous ventilation until the airway is secure Rationale: to retain some muscle tone in the upper airway and allow time for laryngoscopy and intubation Why not give a muscle relaxant? - to avoid the scenario where a muscle relaxant has been given, bag-mask ventilation proves difficult or impossible, the child becomes hypoxaemic, and cannot be intubated - CICO The management of difficult intubation in children. Paediatric Anesthesia 2009; 19 (Suppl. 1): RM Walker and J Ellwood.
6 Anatomical Airway Obstruction Inhalational induction still popular in paediatrics NAP 4 census report - management of the predicted difficult airway in children: Inhalational induction - 63% Intravenous induction - 37% Awake intubation - 0%
7 Anatomical Airway Obstruction Canadian paediatric anesthesiologists prefer inhalational anesthesia to manage difficult airways: a survey Canadian Journal of Anesthesia 2005; 52:3 pp Peter Brooks et al. 6 scenarios - web-based survey 63 responses from 136 invitations- experienced paediatric anaesthetists 2 scenarios - emergencies with a compromised airway 2 year old child with potential epiglottis needing emergency endotracheal intubation - 95% of respondents chose to keep the patient breathing spontaneously and 97% would use an inhalational agent to do this.
8 Anatomical Airway Obstruction Rigid bronchoscopy for foreign body removal: anaesthesia and ventilation Pediatric Anesthesia : pp84-89 PT Farrell in an emergency situation or with a distressed infant, establishing iv access immediately after inhalation induction is acceptable spontaneous ventilation must be maintained until it is certain that the child can still be ventilated under anaesthesia most experienced anaesthesiologists prefer inhalational rather than intravenous induction
9 Anatomical Airway Obstruction A child with a difficult airway: what do I do next? Current Opinion in Anesthesiology 2012; 25(3): T Engelhardt and M Weiss the recent NAP 4 audit suggests that spontaneously breathing adult patients who lost the airway do not recover rapidly. Full recovery of a child with lower oxygen reserves is even more unlikely and as yet not reported in the literature.

10 Anatomical Airway Obstruction NAP 4 report: Chapter 13 management of the CICV situation, page 113
11 Anatomical Airway Obstruction DAS 2015 guidelines for the management of the unanticipated difficult intubation in adults Plan C - the final attempt at face-mask ventilation If face-mask ventilation is impossible - paralyze ensuring full paralysis offers a final chance of rescuing the airway without recourse to Plan D airway rescue via the front of neck should not be attempted without complete neuromuscular block
12 Anatomical Airway Obstruction Cannot ventilate - paralyze! Pediatric Anesthesia M Weiss and T Engelhardt Treat functional airway obstruction Functional airway obstruction is the leading cause of difficult failed facemask ventilation or a deeply anesthetized, hypoxic brain is unlikely to restart spontaneous breathing and establish airway patency. There is no way back
13 Anatomical Airway Obstruction APA/DAS guidelines for the management of the unanticipated difficult airway in paediatric practice Pediatric Anesthesia AE Black et al. the CICV scenario is considered in the context of the paralysed child sugammadex should not be given to reverse rocuronium or vecuronium if the child is rapidly deteriorating with decreasing SpO2 and haemodynamic compromise
14 Functional Airway Obstruction Which port in a Storm? Use of suxamethonium without intravenous access for severe laryngospasm RWM Walker and R Sutton Anesthesia : Suxamethonium 4 mg/kg into the deltoid muscle - should work within 1 min

15 Anterior mediastinal mass
16 Anterior mediastinal mass Anesthetic management of children with an anterior mediastinal mass Journal of Clinical Anesthesia : PA Stricker, HG Gurnaney, and RS Litman Spontaneous ventilation was maintained in 21 of 46 cases 26 patients had signs and symptoms suggestive of cardiopulmonary compromise as well as radiologic evidence of respiratory or cardiovascular compression - muscle relaxant was avoided in 18 of these cases - 17 of these case received iv sedation with spontaneous ventilation and a natural airway, often in the Semi-Fowler s position - one complication in the 8 patients who received muscle relaxant and IPPV - bronchospasm that resolved with administration of a bronchodilator
17 Anterior mediastinal mass The anaesthetic management of children with anterior mediastinal mass Anaesthesia 2008, 63: HA Hack, NB Wright, and RF Wynn 53 anaesthetic charts available for inspection 25/53 - inhalational induction; 2 of these in the sitting position, 1in the lateral position. 28/53 - iv induction in the supine position 18/53 - maintained spontaneous ventilation; FM, LMA, ETT. 35/53 - IPPV no significant difference in the tracheal cross-sectional area
18 Risk of aspiration NAP 4 - aspiration was the main cause of adverse outcome at induction NAP 4 - aspiration was the cause of 50% of anaesthesia deaths and 53% of outcomes of death or brain damage Recommendation: On balance, rapid sequence induction should continue to be taught as a standard technique for protection of the airway. Further focused research might usefully be performed to explore its efficacy, limitations and also explore the consequences of its omission. Chapter 19, page 163
19 Risk of Aspiration Pulmonary Aspiration in pediatric anesthetic practice in the UK: a prospective survey of specialist pediatric centres over a one year period Pediatric Anesthesia : Robert W.M. Walker 1 year, 11 paediatric centres, denominator per cases for elective work 2.2 per cases for non-elective work no deaths 5 cases with serious morbidity - needing PICU
20 Risk of Aspiration Pulmonary Aspiration in pediatric anesthetic practice in the UK: a prospective survey of specialist pediatric centres over a one year period Pediatric Anesthesia : Robert W.M. Walker 12 / 24 cases of pulmonary aspiration of gastric contents occurred at induction 7 /12 cases of pulmonary aspiration of gastric contents at induction = iv induction 5 / 12 cases of pulmonary aspiration of gastric contents at induction = inhalational induction 8 /12 cases of pulmonary aspiration of gastric contents at induction = elective cases (3 had inhalational induction) 4 /12 cases of pulmonary aspiration of gastric contents at induction = non-elective (2 had inhalational induction)
21 Risk of aspiration Perioperative pulmonary aspiration in infants and children Anesthesiology 1999; 90: MA Warner et al. 3.8 per cases 2 per for elective cases 25 per for emergency cases consecutive anaesthetics no deaths
22 Risk of aspiration Pulmonary aspiration in pediatric patients during general anaesthesia: incidence and outcomes Journal of Clinical Anesthesia 1998; 10: LM Borland et al per cases anaesthetics no deaths
23 Risk of aspiration Pulmonary aspiration under GA: a 13-year audit in a tertiary pediatric unit Z Tan and SY Lee Pediatric Anesthesia 2016, 26: cases of pulmonary aspiration / general anaesthetic 2.15 per / 22 - iv induction 10/ 22 - inhalational induction iv vs inhalational induction odds ratio (95%CI ) emergency surgery vs elective surgery odds ratio (95% confidence interval )
24 Risk of aspiration minimise the gastric volume - fasting, prokinetics, and NG tube; use ultrasound to check increase the ph of gastric contents - sodium citrate, ranitidine, PPI RSI - cricoid pressure; apnoeic inducton Effects of different combinations of H2 receptor antagonists with gastrokinetic drugs on gastric fluid ph and volume in children - a comparative study Int j Pharmacol Ther 1997; 35: Kulkarni PN, Batra YK, Wig J
25 Risk of aspiration Avoid: Decreasing intrathoracic pressure: airway obstruction, hiccup Elevating intra-abdominal pressure: laryngoscopy during light anaesthesia, coughing or straining during induction or intubation, inflating the stomach during bag-mask ventilation Oesophageal intubation Haste Hypoxaemia
26 Risk of aspiration - apnoeic induction? Controlled rapid sequence induction and intubation - an analysis of 1001 children D Neuhaus, A Schmitz, A Gerber, et al. Pediatric Anesthesia 2013, 23: gentle face-mask ventilation prior to intubation, avoidance of cricoid pressure, non-depolarising neuromuscular blocking agent moderate hypoxaemia (SpO %) in 0.5%; n = 5 severe hypoxaemia (SpO2 < 80%) in 0.3%; n =3 1 episode of regurgitation without aspiration
27 Is cricoid pressure harmful? airway occlusion distorted anatomy failed intubation difficult or impossible face-mask ventilation relaxation of the lower oesophageal sphincter a trigger for vomiting? may provoke bucking or straining interferes with a smooth induction Cricoid pressure: apply - but be ready to release Anaesthesia 2016, 71, J Turnbull, A Patel, V Athanassoglou, JJ Pandit
28 Cricoid pressure Aspiration and regurgitation prophylaxis in paediatric anaesthesia Pediatric Anesthesia 2001; 11: Engelhardt T, Strachen L, Johnston G Up to 50% of paediatric anaesthetists would not use cricoid pressure in the full stomach situation Do you routinely employ the following prior to anaesthesia in all children regardless of risk factors? 42% (37 / 88 replies) would routinely apply cricoid pressure in children < 1year of age having emergency surgery 49% (43 / 88 replies) would routinely apply cricoid pressure in children aged 1-14 years having emergency surgery
29 Cricoid Pressure Effect of cricoid force on airway calibre in children: a bronchoscopic study British Journal of Anaesthesia 2010; 104: Walker RWM, Ravi R, Haylett K 5N = the force required to cause 50% occlusion of the subglottic airway with the application of cricoid pressure in infants
30 Rapid sequence induction has no use in paediatric anesthesia Pediatric Anesthesia 2015; 25: pp 5-8 Thomas Englehardt Regurgitation and vomiting with aspiration are processes elicited by direct laryngoscopy under light anaesthesia and incomplete muscle paralysis Advocates mask ventilation with pressures not exceeding cmh2o following induction and before intubation in paediatric RSI induction of sufficiently deep anaesthesia avoid cricoid pressure confirm complete muscle paralysis before laryngoscopy
31 Is cricoid pressure effective No RCTs Absence of evidence is not evidence of absence Argument from ignorance - a proposition is true because it has not yet be proved false Aspiration does occur despite the application of CP Anatomy - the oesophagus is postero-lateral to the cricoid ring in 50% of people; lateral displacement increases with CP, but it is the post-cricoid hypo pharynx that is compressed and occluded - MRI, videolaryngosocpy, attempts to pass 4mm NG tube
32
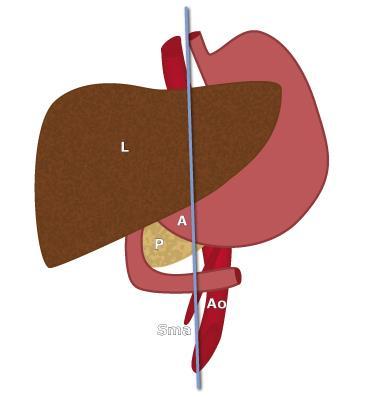
33 Gastric Ultrasound Gastric antrum Right lateral decubitus position only the RLD antrum CSA and age were shown to be independent predictors of endoscopically suctioned gastric volume Sagittal or right para-sagittal Between the left lobe of the liver and the pancreas at the level of the aorta and superior mesenteric artery or inferior vena cava Ultrasound assessment of gastric volume in the fasted pediatric patient undergoing upper gastrointestinal endoscopy: development of a predictive model using endoscopically suctioned volumes Pediatric anesthesia 2015; 25: Adam O. Spencer, Anrew M Walker, Alfred K. Yeung, et al.
34 Gastric Ultrasound Qualitative assessment Grade 0: no fluid visible in the antrum in either the supine or RLD position Grade 1: antral fluid visible in the RLD position but not in the supine position Grade2: antral fluid visible in both the supine and RLD position Quantitative assessment Antral cross-sectional area in the RLD position Volume = (3.5 x RLD CSA) + (0.127 x age in months) Ultrasound assessment of gastric volume in the fasted pediatric patient undergoing upper gastrointestinal endoscopy: development of a predictive model using endoscopically suctioned volumes Pediatric anesthesia 2015; 25: Adam O. Spencer, Anrew M Walker, Alfred K. Yeung, et al.
35 Gastric ultrasound in babies with hypertrophic pyloric stenosis undergoing pyloromyotomy 34 infants Ultrasound of gastric antrum in the right lateral decubitus position before and after aspiration of gastric contents through 10Fr gastric tube Ultrasound examination before aspiration failed in 3/34 - gas in the stomach or infant agitation No failed examinations after gastric aspiration 9/31 empty stomach on first ultrasound 22/31 full stomach on first ultrasound The aspirated gastric volume correlates with the antral cross sectional area measured in the RLD Pearson correlation coefficient 0.83 (95% CI ; p<0.0001) 30/34 non-rapid sequence induction Ultrasound assessment of the gastric contents for the guidance of the anaesthetic strategy in infants with hypertrophic pyloric stenosis: a prospective cohort study British Journal of Anaesthesia 2016; 116(5): A.C. Gagey, M. de Queiroz Siqueira, F.P. Desgranges, et al.

36 The humane argument The pragmatic argument Have you ever induced anaesthesia via an IO? Careful assessment, good judgement, good decision making, smooth execution
37 Conclusion Is inhalational induction justifiable in paediatric emergencies? Anatomical Airway Obstruction yes Anterior mediastinal mass yes Hypertrophic pyloric stenosis yes Neonatal surgery yes Older children at risk of aspiration not my first choice but I would seldom rule it out completely
38 Conclusion To reduce the risk of aspiration Reduce the gastric volume Increase the ph of the gastric contents Smooth induction Ensure an adequate depth of anaesthesia before attempts at intubation Complete muscle paralysis before laryngoscopy
Cricoid pressure: useful or dangerous?
 Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital
 Difficult & Failed Intubation Queen Charlotte s Hospital") (ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
GENERAL ANAESTHESIA AND FAILED INTUBATION
 GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
PAEDIATRIC ANAESTHETIC EMERGENCIES PART I. Dr James Cockcroft, South West School of Anaesthesia. Dr Sarah Rawlinson, Derriford Hospital, Plymouth, UK
 PAEDIATRIC ANAESTHETIC EMERGENCIES PART I Original Article by: Dr Claire Todd, South West School of Anaesthesia Dr James Cockcroft, South West School of Anaesthesia Dr Sarah Rawlinson, Derriford Hospital,
PAEDIATRIC ANAESTHETIC EMERGENCIES PART I Original Article by: Dr Claire Todd, South West School of Anaesthesia Dr James Cockcroft, South West School of Anaesthesia Dr Sarah Rawlinson, Derriford Hospital,
Cuffed or uncuffed ETT in pediatric anesthesia? Dr. Renata Haghedooren Dr. Sophie Chullikal Dr. Julie Lauweryns
 Cuffed or uncuffed ETT in pediatric anesthesia? Dr. Renata Haghedooren Dr. Sophie Chullikal Dr. Julie Lauweryns Overview History Survey Tradition Pro-Con Debate Conclusions History of intubation 1878:
Cuffed or uncuffed ETT in pediatric anesthesia? Dr. Renata Haghedooren Dr. Sophie Chullikal Dr. Julie Lauweryns Overview History Survey Tradition Pro-Con Debate Conclusions History of intubation 1878:
LMA Supreme Second Seal. Maintain the airway. Manage gastric contents. Meet NAP4 recommendations.
 LMA Supreme Second Seal Maintain the airway. Manage gastric contents. Meet NAP4 recommendations. A proven double seal The importance of the Second Seal (oesophageal seal) is significant: it can minimise
LMA Supreme Second Seal Maintain the airway. Manage gastric contents. Meet NAP4 recommendations. A proven double seal The importance of the Second Seal (oesophageal seal) is significant: it can minimise
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
1. Influence of isoflurane exposure in pregnant rats on the learning and memory of offspring
 1. Influence of isoflurane exposure in pregnant rats on the learning and memory of offspring Huang W, Dong Y, Zhao G, et al. BMC Anesthesiology 2018 18:5 Concerns remain about possible effects of general
1. Influence of isoflurane exposure in pregnant rats on the learning and memory of offspring Huang W, Dong Y, Zhao G, et al. BMC Anesthesiology 2018 18:5 Concerns remain about possible effects of general
ASPIRATION DURING ANAESTHESIA
 ASPIRATION DURING ANAESTHESIA MODULE: CRITICAL INCIDENTS TARGET: ALL ANAESTHETISTS BACKGROUND: Passive regurgitation or vomiting can occur during the pre-, peri- or post- operative period risking aspiration
ASPIRATION DURING ANAESTHESIA MODULE: CRITICAL INCIDENTS TARGET: ALL ANAESTHETISTS BACKGROUND: Passive regurgitation or vomiting can occur during the pre-, peri- or post- operative period risking aspiration
Nüchternzeiten in der Kinderanästhesie nüchtern betrachtet
 Nüchternzeiten in der Kinderanästhesie nüchtern betrachtet Pädiatrische Traunseeklausur 2018 04. - 05. Mai 2018 Gmunden (A) Prof. Dr. med. Markus Chefarzt Anästhesieabteilung, Universitäts-Kinderspital
Nüchternzeiten in der Kinderanästhesie nüchtern betrachtet Pädiatrische Traunseeklausur 2018 04. - 05. Mai 2018 Gmunden (A) Prof. Dr. med. Markus Chefarzt Anästhesieabteilung, Universitäts-Kinderspital
Anaesthetic Plan And The Practical Conduct Of Anaesthesia. Dr.S.Vashisht Hillingdon Hospital
 Anaesthetic Plan And The Practical Conduct Of Anaesthesia Dr.S.Vashisht Hillingdon Hospital Anaesthetic Plan Is based on Age / physiological status of the patient (ASA) Co-morbid conditions that may be
Anaesthetic Plan And The Practical Conduct Of Anaesthesia Dr.S.Vashisht Hillingdon Hospital Anaesthetic Plan Is based on Age / physiological status of the patient (ASA) Co-morbid conditions that may be
Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients.
 Title Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients Author(s) Greenland, KB; Ha, ID; Irwin, MG Citation Anaesthesia,
Title Comparison of the Berman Intubating Airway and the Williams Airway Intubator for fibreoptic orotracheal intubation in anaesthetised patients Author(s) Greenland, KB; Ha, ID; Irwin, MG Citation Anaesthesia,
Airway management problem during anaesthesia. Airway management problem in ICU / HDU. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
Subspecialty Rotation: Anesthesia
 Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 CRICOID PRESSURE: MORE RITUAL THAN EFFECTIVE MEASURE?
 EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 CRICOID PRESSURE: MORE RITUAL THAN EFFECTIVE MEASURE? 19RC3 HANS-JOACHIM PRIEBE Department of Anaesthesia University Hospital Freiburg Freiburg,
EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 CRICOID PRESSURE: MORE RITUAL THAN EFFECTIVE MEASURE? 19RC3 HANS-JOACHIM PRIEBE Department of Anaesthesia University Hospital Freiburg Freiburg,
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
DIFFICULT AIRWAY MANAGMENT. Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr)
") DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
Sign up to receive ATOTW weekly
 PULSE OXIMETRY PART 2 ANAESTHESIA TUTORIAL OF THE WEEK 124 9 TH MARCH 2009 Dr. Iain Wilson Royal Devon & Exeter Hospital, UK Correspondence to iain.wilson@rdeft.nhs.uk The WFSA has been working on information
PULSE OXIMETRY PART 2 ANAESTHESIA TUTORIAL OF THE WEEK 124 9 TH MARCH 2009 Dr. Iain Wilson Royal Devon & Exeter Hospital, UK Correspondence to iain.wilson@rdeft.nhs.uk The WFSA has been working on information
Airway Workshop Lecture. University of Ottawa
 Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy
 Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy Department of Anaesthesia University Children s Hospital Zurich Switzerland Epidemiology Herniotomy needed in
Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy Department of Anaesthesia University Children s Hospital Zurich Switzerland Epidemiology Herniotomy needed in
General OR Rotations GOALS & OBJECTIVES
 General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
General OR Rotations GOALS & OBJECTIVES Goals At the end of the CA 1 year General OR rotations, the resident should competently manage uncomplicated ambulatory, orthopedic, maxillo-facial, ENT, gynecologic,
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
Sign up to receive ATOTW weekly -
 INFANTILE HYPERTROPHIC PYLORIC STENOSIS ANAESTHESIA TUTORIAL OF THE WEEK 276 26 TH NOVEMBER 2012 Dr Ian Davies University Hospitals Bristol Correspondence to ian.davies2@nhs.net QUESTIONS Before reading
INFANTILE HYPERTROPHIC PYLORIC STENOSIS ANAESTHESIA TUTORIAL OF THE WEEK 276 26 TH NOVEMBER 2012 Dr Ian Davies University Hospitals Bristol Correspondence to ian.davies2@nhs.net QUESTIONS Before reading
Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal and Anterior Mediastinal Abscess
 Hindawi Case Reports in Pediatrics Volume 2017, Article ID 1848945, 4 pages https://doi.org/10.1155/2017/1848945 Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal
Hindawi Case Reports in Pediatrics Volume 2017, Article ID 1848945, 4 pages https://doi.org/10.1155/2017/1848945 Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal
Updates on Airway Management
 Updates on Airway Management Dr Gemma Malpas Department of Anaesthesia and Perioperative Medicine, Auckland City Hospital, New Zealand Introduction Despite events only occurring infrequently, complications
Updates on Airway Management Dr Gemma Malpas Department of Anaesthesia and Perioperative Medicine, Auckland City Hospital, New Zealand Introduction Despite events only occurring infrequently, complications
The Laryngeal Mask and Other Supraglottic Airways: Application to Clinical Airway Management
 The Laryngeal Mask and Other Supraglottic Airways: Application to Clinical Airway Management D. John Doyle MD PhD FRCPC Department of General Anesthesiology Cleveland Clinic Foundation 9500 Euclid Avenue
The Laryngeal Mask and Other Supraglottic Airways: Application to Clinical Airway Management D. John Doyle MD PhD FRCPC Department of General Anesthesiology Cleveland Clinic Foundation 9500 Euclid Avenue
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
Comparison of Ease of Insertion and Hemodynamic Response to Lma with Propofol and Thiopentone.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 12 Ver. IV (Dec. 2015), PP 22-30 www.iosrjournals.org Comparison of Ease of Insertion and Hemodynamic
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 12 Ver. IV (Dec. 2015), PP 22-30 www.iosrjournals.org Comparison of Ease of Insertion and Hemodynamic
Pediatric Difficult Airway Management. R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee
 Pediatric Difficult Airway Management R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee The pediatric difficult airway is associated with a high risk for complications during
Pediatric Difficult Airway Management R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee The pediatric difficult airway is associated with a high risk for complications during
RAPID SEQUENCE INTUBATION FOR THE RURAL DOC
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
RELEVANT AREAS OF THE ANAESTHETIC CURRICULUM
 LARYNGOSPASM MODULE: CRITICAL INCIDENTS TARGET: ALL ANAESTHETISTS & INTENSIVISTS BACKGROUND: Laryngospasm is a common complication around the time of airway handling in adults and in paediatric patients.
LARYNGOSPASM MODULE: CRITICAL INCIDENTS TARGET: ALL ANAESTHETISTS & INTENSIVISTS BACKGROUND: Laryngospasm is a common complication around the time of airway handling in adults and in paediatric patients.
Airway Management and The Difficult Airway
 Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Unanticipated difficult tracheal intubation - during routine induction of anaesthesia in an adult patient
 Unanticipated difficult tracheal intubation - during routine induction of anaesthesia in an adult patient Direct laryngoscopy Any problems Call for help Plan A: Initial tracheal intubation plan Direct
Unanticipated difficult tracheal intubation - during routine induction of anaesthesia in an adult patient Direct laryngoscopy Any problems Call for help Plan A: Initial tracheal intubation plan Direct
Major complications of airway management in the United Kingdom
 The Royal College of Anaesthetists The Difficult Airway Society 4th National Audit Project of The Royal College of Anaesthetists and The Difficult Airway Society Major complications of airway management
The Royal College of Anaesthetists The Difficult Airway Society 4th National Audit Project of The Royal College of Anaesthetists and The Difficult Airway Society Major complications of airway management
Use of a mechanical simulator for training in applying cricoid pressure
 British Journal of Anaesthesia 1996;77:468 472 Use of a mechanical simulator for training in applying cricoid pressure N. ASHURST, C. C. ROUT, D. A. ROCKE AND E. GOUWS Summary Using an airway management
British Journal of Anaesthesia 1996;77:468 472 Use of a mechanical simulator for training in applying cricoid pressure N. ASHURST, C. C. ROUT, D. A. ROCKE AND E. GOUWS Summary Using an airway management
Australian and New Zealand College of Anaesthetists (ANZCA)
") PS61 2017 Australian and New Zealand College of Anaesthetists (ANZCA) Guidelines for the Management of Evolving Airway Obstruction: Transition to the Can t Intubate Can t Oxygenate Airway Emergency 1.
PS61 2017 Australian and New Zealand College of Anaesthetists (ANZCA) Guidelines for the Management of Evolving Airway Obstruction: Transition to the Can t Intubate Can t Oxygenate Airway Emergency 1.
All I need is an LMA
 All I need is an LMA Narasimhan Sim Jagannathan, M.D. Associate Chairman, Academic Affairs Director, Pediatric Anesthesia Research Ann & Robert H. Lurie Children s Hospital of Chicago Associate Professor
All I need is an LMA Narasimhan Sim Jagannathan, M.D. Associate Chairman, Academic Affairs Director, Pediatric Anesthesia Research Ann & Robert H. Lurie Children s Hospital of Chicago Associate Professor
Airway management problem occurring in the Emergency Department
 NAP4EM Airway management problem occurring in the Emergency Department Inclusion criteria 1. Please indicate the inclusion criteria by selecting one or more from the list below: Death Brain damage Emergency
NAP4EM Airway management problem occurring in the Emergency Department Inclusion criteria 1. Please indicate the inclusion criteria by selecting one or more from the list below: Death Brain damage Emergency
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
ISPUB.COM. The Use of LMA in Newborn Resuscitation. R Vadhera INTRODUCTION VENTILATION
 ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
FAILED INTUBATION DURING RSI: PLAN A, C & D
 FAILED INTUBATION DURING RSI: PLAN A, C & D MODULE: NOVICE & AIRWAY TARGET: NOVICE INITIAL ASSESSMENT OF COMPETENCY ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation
FAILED INTUBATION DURING RSI: PLAN A, C & D MODULE: NOVICE & AIRWAY TARGET: NOVICE INITIAL ASSESSMENT OF COMPETENCY ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation
CASE PRIMERS. Pediatric Anesthesia Fellowship Program. Laryngotracheal Reconstruction (LTR) Tufts Medical Center
 Tufts Medical Center") CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
CASE PRIMERS Pediatric Anesthesia Fellowship Program Tufts Medical Center Department of Anesthesiology and Perioperative Medicine Division of Pediatric Anesthesia 800 Washington Street, Box 298 Boston,
OBJECTIVES OF TRAINING FOR THE ANAESTHESIA TERM
 College of Intensive Care Medicine of Australia and New Zealand ABN: 16 134 292 103 Document type: Training Date established: 2007 Date last reviewed: 2014 OBJECTIVES OF TRAINING FOR THE ANAESTHESIA TERM
College of Intensive Care Medicine of Australia and New Zealand ABN: 16 134 292 103 Document type: Training Date established: 2007 Date last reviewed: 2014 OBJECTIVES OF TRAINING FOR THE ANAESTHESIA TERM
Incidence and predictors of difficult mask ventilation and intubation
 Original Article Incidence and predictors of difficult mask ventilation and intubation Prerana N Shah, Vimal Sundaram Department of Anaesthesiology, Seth G S Medical College and KEM Hospital, Parel, Mumbai
Original Article Incidence and predictors of difficult mask ventilation and intubation Prerana N Shah, Vimal Sundaram Department of Anaesthesiology, Seth G S Medical College and KEM Hospital, Parel, Mumbai
Ventilating the paediatric patient. Lizzie Barrett Nurse Educator November 2016
 Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
Comparison of the Hemodynamic Responses with. with LMA vs Endotracheal Intubation
 Original article Comparison of the Hemodynamic Responses 10.5005/jp-journals-10045-0060 with LMA vs Endotracheal Intubation Comparison of the Hemodynamic Responses with Laryngeal Mask Airway vs Endotracheal
Original article Comparison of the Hemodynamic Responses 10.5005/jp-journals-10045-0060 with LMA vs Endotracheal Intubation Comparison of the Hemodynamic Responses with Laryngeal Mask Airway vs Endotracheal
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS)
") Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Anesthesia recommendations for patients suffering from Mucolipidosis II and III
 orphananesthesia Anesthesia recommendations for patients suffering from Mucolipidosis II and III Disease name: Mucolipidosis Type 2 and 3 ICD 10: E77.0 Synonyms: Mucolipidosis type 2 - I-cell disease N-acetyl-glucosamine
orphananesthesia Anesthesia recommendations for patients suffering from Mucolipidosis II and III Disease name: Mucolipidosis Type 2 and 3 ICD 10: E77.0 Synonyms: Mucolipidosis type 2 - I-cell disease N-acetyl-glucosamine
Rigid bronchoscopy for foreign body removal: anaesthesia and ventilation
 Pediatric Anesthesia 2004 14: 84 89 Rigid bronchoscopy for foreign body removal: anaesthesia and ventilation PATRICK T. FARRELL MBBS, FRCA, FANZCA Department of Anaesthesia, John Hunter Hospital, Newcastle,
Pediatric Anesthesia 2004 14: 84 89 Rigid bronchoscopy for foreign body removal: anaesthesia and ventilation PATRICK T. FARRELL MBBS, FRCA, FANZCA Department of Anaesthesia, John Hunter Hospital, Newcastle,
anatomic relationship between the internal jugular vein and the carotid artery in children after laryngeal mask insertion. An ultrasonographic study.
 The anatomic relationship between the internal jugular vein and the carotid artery in children after laryngeal mask insertion. An ultrasonographic study. Ravi Gopal Nagaraja, Morven Wilson, Graham Wilson,
The anatomic relationship between the internal jugular vein and the carotid artery in children after laryngeal mask insertion. An ultrasonographic study. Ravi Gopal Nagaraja, Morven Wilson, Graham Wilson,
Difficult Airway. Department of Anesthesiology University of Colorado Health Sciences Center (prepared by Brenda A. Bucklin, M.D.)
") Difficult Airway Department of Anesthesiology University of Colorado Health Sciences Center (prepared by Brenda A. Bucklin, M.D.) Objectives Definition & incidence of the difficult airway Evaluation of
Difficult Airway Department of Anesthesiology University of Colorado Health Sciences Center (prepared by Brenda A. Bucklin, M.D.) Objectives Definition & incidence of the difficult airway Evaluation of
ANAESTHESIA FOR BLEEDING TONSIL
 ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
Succinycholine: Succinylcholine has no place in pediatric anesthesia. Wads Ames MBBS FRCA
 Succinycholine: Succinylcholine has no place in pediatric anesthesia Wads Ames MBBS FRCA Food And Drug Administration Created in 1906 Responsible for protecting and promoting public health through the
Succinycholine: Succinylcholine has no place in pediatric anesthesia Wads Ames MBBS FRCA Food And Drug Administration Created in 1906 Responsible for protecting and promoting public health through the
If you suspect airway problems, get a second opinion before you anaesthetise, not after!
 Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Sign up to receive ATOTW weekly -
 UPPER RESPIRATORY TRACT INFECTION AND PAEDIATRIC ANAESTHESIA ANAESTHESIA TUTORIAL OF THE WEEK 246 16 th January 2011 Ma Carmen Bernardo-Ocampo, MD, DPBA Assistant Professor/Attending Anesthesiologist University
UPPER RESPIRATORY TRACT INFECTION AND PAEDIATRIC ANAESTHESIA ANAESTHESIA TUTORIAL OF THE WEEK 246 16 th January 2011 Ma Carmen Bernardo-Ocampo, MD, DPBA Assistant Professor/Attending Anesthesiologist University
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
19RC1 Paediatric airway problems
 19RC1 Paediatric airway problems M. Weiss Department of Anaesthesia, University Children s Hospital, Zurich, Switzerland Saturday, June 6, 2009 13:00-13:45 Room: Yellow 3 In recent years, airway management
19RC1 Paediatric airway problems M. Weiss Department of Anaesthesia, University Children s Hospital, Zurich, Switzerland Saturday, June 6, 2009 13:00-13:45 Room: Yellow 3 In recent years, airway management
Risky Extubation. Andy Higgs. Warrington Hospitals Cheshire UK
 Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
Airway management problem during anaesthesia. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
L.J. Hoeve and R.H.M. van Poppelen * (Received 12 July 1989) (Accepted 10 August 1989)
 (Accepted 10 August 1989)") International Journal of Pediatric Otorhinolaryngolo~. 18 (1990) 241-245 Elsevier 241 PEDOT 00617 Fiberoptic laryngoscopy under in neonates general anesthesia L.J. Hoeve and R.H.M. van Poppelen * Lkpar?ments
International Journal of Pediatric Otorhinolaryngolo~. 18 (1990) 241-245 Elsevier 241 PEDOT 00617 Fiberoptic laryngoscopy under in neonates general anesthesia L.J. Hoeve and R.H.M. van Poppelen * Lkpar?ments
Recent Advances in Airway Management HA Convention 2014
 Recent Advances in Airway Management HA Convention 2014 Dr. HK Cheng Chief of Service (Dept. of Anaesthesia & OT) Service Director (Ambulatory Surgery Centre) Tseung Kwan O Hospital Recent Advances in
Recent Advances in Airway Management HA Convention 2014 Dr. HK Cheng Chief of Service (Dept. of Anaesthesia & OT) Service Director (Ambulatory Surgery Centre) Tseung Kwan O Hospital Recent Advances in
AIRWAY AND RESPIRATORY COMPLICATIONS IN CHILDREN UNDERGOING CLEFT LIP AND PALATE REPAIR
 AIRWAY AND RESPIRATORY COMPLICATIONS IN CHILDREN UNDERGOING CLEFT LIP AND PALATE REPAIR I. DESALU, W.L. ADEYEMO, M.O AKINTIMOYE and A.A. ADEPOJU Department of Anaesthesia, Lagos University Teaching Hospital,
AIRWAY AND RESPIRATORY COMPLICATIONS IN CHILDREN UNDERGOING CLEFT LIP AND PALATE REPAIR I. DESALU, W.L. ADEYEMO, M.O AKINTIMOYE and A.A. ADEPOJU Department of Anaesthesia, Lagos University Teaching Hospital,
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Airway Management. Key points. Rapid Sequence Intubation. Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway
 Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Emergency)tracheostomy)management)/)Patent)upper)airway)
tracheostomy)management)/)Patent)upper)airway)") Emergency)tracheostomy)management)/)Patent)upper)airway) Call,for,airway,expert,help,,Look,,listen,&,feel,at,the,mouth,and,tracheostomy) A)Mapleson)C)system)(e.g.) Waters)circuit ))may)help)assessment)if)available)
Emergency)tracheostomy)management)/)Patent)upper)airway) Call,for,airway,expert,help,,Look,,listen,&,feel,at,the,mouth,and,tracheostomy) A)Mapleson)C)system)(e.g.) Waters)circuit ))may)help)assessment)if)available)
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
TRANSPARENCY COMMITTEE OPINION. 21 January 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 21 January 2009 BRIDION 100 mg/ml, solution for injection Box containing 10 x 2 ml bottles, CIP: 573 553-9 Box containing
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 21 January 2009 BRIDION 100 mg/ml, solution for injection Box containing 10 x 2 ml bottles, CIP: 573 553-9 Box containing
R egurgitation, vomiting and aspiration may occur quite
 1of5 ORIGINAL ARTICLE Crisis management during anaesthesia: regurgitation, vomiting, and aspiration M T Kluger, T Visvanathan, J A Myburgh, R N Westhorpe... See end of article for authors affiliations...
1of5 ORIGINAL ARTICLE Crisis management during anaesthesia: regurgitation, vomiting, and aspiration M T Kluger, T Visvanathan, J A Myburgh, R N Westhorpe... See end of article for authors affiliations...
Section 4.1 Paediatric Tracheostomy Introduction
 Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Tracheostomy and laryngectomy airway emergencies: an overview for medical and nursing staff
 2013 Medical Journal Tracheostomy and laryngectomy airway emergencies: an overview for medical and nursing staff Steven Lobaz 1 and Paul Bush 2 1 ST6 and 2 Consultant Department of Anaesthesia and Intensive
2013 Medical Journal Tracheostomy and laryngectomy airway emergencies: an overview for medical and nursing staff Steven Lobaz 1 and Paul Bush 2 1 ST6 and 2 Consultant Department of Anaesthesia and Intensive
Study Of Effects Of Varying Durations Of Pre-Oxygenation. J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh
 ISPUB.COM The Internet Journal of Anesthesiology Volume 20 Number 1 J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh Citation J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh.. The Internet
ISPUB.COM The Internet Journal of Anesthesiology Volume 20 Number 1 J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh Citation J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh.. The Internet
FAILED ELECTIVE INTUBATION: PLAN A- C
 FAILED ELECTIVE INTUBATION: PLAN A- C MODULE: AIRWAY TARGET: NOVICE, BASIC LEVEL TRAINEES & ALL ANAESTHETISTS BACKGROUND: Management of the unexpectedly difficult airway is a core skill for all anaesthetists.
FAILED ELECTIVE INTUBATION: PLAN A- C MODULE: AIRWAY TARGET: NOVICE, BASIC LEVEL TRAINEES & ALL ANAESTHETISTS BACKGROUND: Management of the unexpectedly difficult airway is a core skill for all anaesthetists.
Cuffed Tracheal Tubes in Children - Myths and Facts. PD Dr. Markus Weiss Department of Anaesthesia University Children s Hospital Zurich Switzerland
 Cuffed Tracheal Tubes in Children - Myths and Department of Anaesthesia University Children s Hospital Zurich Switzerland PRO Reduced gas leak, low fresh gas flow Decreased atmospheric pollution Constant
Cuffed Tracheal Tubes in Children - Myths and Department of Anaesthesia University Children s Hospital Zurich Switzerland PRO Reduced gas leak, low fresh gas flow Decreased atmospheric pollution Constant
Emergency ENT Anaesthesia. Richard Semenov
 Emergency ENT Anaesthesia Richard Semenov Emergency ENT Anaesthesia Dr Richard Semenov MBBS (Adel) FRCA (UK) FANZCA Dept of Anaesthesia Royal Adelaide Hospital My Experience in Emergency ENT Anaesthesia
Emergency ENT Anaesthesia Richard Semenov Emergency ENT Anaesthesia Dr Richard Semenov MBBS (Adel) FRCA (UK) FANZCA Dept of Anaesthesia Royal Adelaide Hospital My Experience in Emergency ENT Anaesthesia
A Successful RSI Program
 RSI A Successful RSI Program Requires understanding of: Indications Contraindications Limitations Requires knowledge of: Physiology Pharmacology Airway techniques Goals of RSI Success rates comparable
RSI A Successful RSI Program Requires understanding of: Indications Contraindications Limitations Requires knowledge of: Physiology Pharmacology Airway techniques Goals of RSI Success rates comparable
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Acute And perioperative care of the burn-injured patient. Anesthesiology, V 122, No 2
 Acute And perioperative care of the burn-injured patient Anesthesiology, V 122, No 2 Reporter:R4 沈士鈞 Supervisor: 蔡欣怡醫師 Pathophysiology Initial evaluation and management Anesthetic managemen nt Pathophysiology
Acute And perioperative care of the burn-injured patient Anesthesiology, V 122, No 2 Reporter:R4 沈士鈞 Supervisor: 蔡欣怡醫師 Pathophysiology Initial evaluation and management Anesthetic managemen nt Pathophysiology
REVERSE LMA INSERTION IN A NEONATE WITH KLIPPEL-FEIL SYNDROME
 REVERSE LMA INSERTION IN A NEONATE WITH KLIPPEL-FEIL SYNDROME - Case report - TARIQ AL ZAHRANI * Klippel-Feil syndrome (KFS) was first described by Maurice Klippel and Andre Feil in 1912 in a patient with
REVERSE LMA INSERTION IN A NEONATE WITH KLIPPEL-FEIL SYNDROME - Case report - TARIQ AL ZAHRANI * Klippel-Feil syndrome (KFS) was first described by Maurice Klippel and Andre Feil in 1912 in a patient with
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
Rapid sequence induction: its place in modern anaesthesia
 : its place in modern anaesthesia Claire Wallace MBChB FRCA Barry McGuire MBChB FRCA Matrix reference 1A01, 1A02,1B02,1C02,2A03 Key points Aspiration is the largest cause of death associated with airway
: its place in modern anaesthesia Claire Wallace MBChB FRCA Barry McGuire MBChB FRCA Matrix reference 1A01, 1A02,1B02,1C02,2A03 Key points Aspiration is the largest cause of death associated with airway
CAN T INTUBATE, CAN T VENTILATE: PLAN A- D
 CAN T INTUBATE, CAN T VENTILATE: PLAN A- D MODULE: AIRWAY TARGET: BASIC LEVEL TRAINEES & ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation is a core skill for all
CAN T INTUBATE, CAN T VENTILATE: PLAN A- D MODULE: AIRWAY TARGET: BASIC LEVEL TRAINEES & ALL ANAESTHETISTS BACKGROUND: Management of the Can t Intubate, Can t Ventilate situation is a core skill for all
Failed tracheal intubation in obstetrics why do we need a guideline?
 Failed tracheal intubation in obstetrics why do we need a guideline? Chris Elton Leicester Royal Infirmary OAA Cases & Clinical Challenges in Obstetric Anaesthesia Churchhouse Westminster 2/3/16 Declarations
Failed tracheal intubation in obstetrics why do we need a guideline? Chris Elton Leicester Royal Infirmary OAA Cases & Clinical Challenges in Obstetric Anaesthesia Churchhouse Westminster 2/3/16 Declarations
Joint Theater Trauma System Clinical Practice Guideline
 Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Anesthesia for removal of inhaled foreign bodies in children
 Pediatric Anesthesia 2004 14: 947 952 doi:10.1111/j.1460-9592.2004.01309.x Anesthesia for removal of inhaled foreign bodies in children AMIT SOODAN MD, DILIP PAWAR MD AND RAJESHWARI SUBRAMANIUM MD Department
Pediatric Anesthesia 2004 14: 947 952 doi:10.1111/j.1460-9592.2004.01309.x Anesthesia for removal of inhaled foreign bodies in children AMIT SOODAN MD, DILIP PAWAR MD AND RAJESHWARI SUBRAMANIUM MD Department
Difficult Airway. Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital
 Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Nobuko Tachibana Yukitoshi Niiyama Michiaki Yamakage
 DOI 10.1007/s00540-014-1847-1 ORIGINAL ARTICLE Incidence of cannot intubate-cannot ventilate (CICV): results of a 3-year retrospective multicenter clinical study in a network of university hospitals Nobuko
DOI 10.1007/s00540-014-1847-1 ORIGINAL ARTICLE Incidence of cannot intubate-cannot ventilate (CICV): results of a 3-year retrospective multicenter clinical study in a network of university hospitals Nobuko
Disclosures. Learning Objectives. Coeditor/author. Associate Science Editor, American Heart Association
 Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
GASTRIC ULTRASOUND. A Point-of-care tool for aspiration risk assessment.
 GASTRIC ULTRASOUND A Point-of-care tool for aspiration risk assessment edu@gastricultrasound.org Indications Any clinical situation where aspiration risk is uncertain. For example: Lack of adherence to
GASTRIC ULTRASOUND A Point-of-care tool for aspiration risk assessment edu@gastricultrasound.org Indications Any clinical situation where aspiration risk is uncertain. For example: Lack of adherence to
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced