Updates in primary hyperaldosteronism and the rule
|
|
|
- Christian Hood
- 6 years ago
- Views:
Transcription

1 Updates in primary hyperaldosteronism and the rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine
2 Changes in health-care and the rule Patient with ACS 20 years ago, ASA absolutely contraindicated Patient with COPD exacerbation 20 years ago, steroids absolutely contraindicated Patient with peptic ulcer disease 20 years ago, antibiotics are useless Patient with hypertension 20 years, BP 160/90 is the target
3 The Rule Rule: Over a continual cycle of 20 years, 50% of what we think we know in medicine Is found to be wrong Promise: Medical care is better now than in the past, and The future will be even better! Implication: We should be humble, even when we think we know what we re doing
4 Hypertension and the Rule 40 years ago Hypertension frequently due to aldosterone 20 years ago Hypertension rarely due to aldosterone Now Hypertension frequently due to aldosterone

5 Severity of hypertension and the prevalence of primary aldosteronism 14% 12% 13.2% 10% 8% 6% 8.0% 4% 2% 0% 2.0% 1.6% >180/ / /90-99 <130/85 Hypertension 42: 161, 2003.
6 Why should we care? Identifying and treating primary aldosteronism makes a difference! Better blood pressure control Holy grail of hypertension management Identify the etiology Treat the etiology Better outcomes

7 Untreated primary aldosteronism increases cardiovascular events 20% 20% 15% 15% 11% 10% 8% 6% Essential hypertension Primary Aldosteronism 5% 3% 3% 2% 0% MI or reversible ischemia CVA or TIA Sustained arrhythmia PAD C Catena, et al, Arch Int Med 168:80-85, 2008.

8 Treating primary aldosteronism reduces CV risk Combined incidence of MI, CVA, revascularization or sustained arrhythmia C Catena, et al, Arch Int Med 168:80-85, 2008.
9 Blood pressure is regulated by the reninangiotensin system BP or Plasma Volume Renin Angiotensinogen Angiotensin I ACE Angiotensin II
 10000 Normal 115")

10 How important is aldosterone: relative importance of Ang II vs aldosterone ng AI/ml/hr or pg/ml MAP (mm Hg) Normal 115 Aldosterone Synthase Deficient Renin Ang II 85 WT KO Makhanova N, et al. Am J Physiol Renal 290:F61-9, 2006.
11 How does aldosterone increase BP? NaCl retention Increased amiloride-sensitive Na + channel expression Increased expression of Cl - -absorbing pendrin protein Increased thiazide-sensitive NaCl cotransporter expression But, if this was all Thiazide diuretic plus amiloride would be enough
12 But, NaCl-dependent volume expansion is NOT the only mechanism

13 Renin-Angiotensin System and BP BP or Plasma Volume Angiotensinogen Renin BP BP Angiotensin I ACE Renal NaCl Retention Decreased Increased Vasodilation Vasoconstriction Endothelin Angiotensin II SNS Tone CNS Aldosterone Adrenal Gland
14 Primary aldosteronism - how to define aldosterone excess? Outside normal limits Plasma aldosterone Random After NaCl loading Problem: Normal limits don t consider the current physiologic state of the person Excessive aldosterone for this person
15 When is aldosterone too much? Aldosterone excessive for primary endogenous regulators (K+ and AII) Absence of hyperkalemia Renin used as surrogate for AII Aldosterone:Renin Ratio (ARR) measurements > 2.5x normal ratio (300:1 in SI units) Aldosterone not suppressed Different investigators use >300, 450 and 600
16 When is aldosterone too much? ARR has difficulties due to variability because of low renin values Plasma renin activity change from ng/ml/hr Not physiologically significant Causes 2x-fold change in ARR (50% reduction) My preference: Plasma renin activity is suppressed Typically ng/ml/hr; Plasma aldosterone is not I use plasma aldosterone > 300 pmol/l
17 Key Point Primary aldosteronism does not require aldosterone levels outside the normal range!
18 Use of ARR leads to more cases of primary aldosteronism being identified Cases diagnosed per year Before ARR With ARR J Clin Endocrinol Metab 89: , 2004
19 % Hypokalemic Hypokalemia is less frequent using ARR screening Before ARR 100% 90% 98% After ARR 96% 100% 75% 66% 50% 37% 37% 25% 25% 22% 9% 0% Torino Rochester Brisbane Singapore Santiago J Clin Endocrinol Metab 89: , 2004
20 APA Cases Per Year More cases of aldosterone-producing adenoma identified Before ARR With ARR Torino Rochester Brisbane Singapore Santiago J Clin Endocrinol Metab 89: , 2004

21 % with BAH Likelihood of bilateral adrenal hyperplasia is higher 100% 75% Before ARR With ARR 70% 91% 72% 70% 50% 50% 25% 30% 32% 25% 14% 17% 0% Torino Rochester Brisbane Singapore Santiago J Clin Endocrinol Metab 89: , 2004
22 Causes of primary hyperaldosteronism Histology Hyperplasia Bilateral adrenal hyperplasia Unilateral adrenal hyperplasia Adenoma Aldosterone-producing adenoma (APA) Bilateral adrenal adenoma Treatment-defined Unilateral Aldosterone-producing adenoma Unilateral adrenal hyperplasia Bilateral Bilateral adrenal hyperplasia Bilateral adrenal adenoma


23 Differentiating unilateral vs bilateral aldosterone release Indirect assessment Imaging CT scan adrenal imaging protocol 20-30% incorrect assignment risk MUST use adrenal protocol Direct assessment Adrenal vein aldosterone measurement

24 Limitation of adrenal vein sampling Modified from C Clemente. Human Anatomy, 1975
25 Limitation of adrenal vein sampling Modified from C Clemente. Human Anatomy, 1975
26 Confirmation of successful adrenal vein sampling Anatomic confirmation is NOT adequate Biochemical confirmation is NECESSARY Adrenal vein aldosterone Inadequate to differentiate APA from unsuccessful cannulation Adrenal vein cortisol If ACTH levels low, adrenal cortisol production low ACTH/Cortrosyn-stimulated adrenal vein cortisol Also increases aldosterone production As much as 40-fold Possible differential effects on hyperplastic and adenomatous glands Can lead to incorrect assignment of aldosterone site
27 Treatment of primary hyperaldosteronism Unilateral Laparoscopic adrenalectomy
28 SBP DBP Response to adrenalectomy Cure, 50% Improved 100% 1.2 ± 1.3 medications per day Predictor Age < Before After 70 A Meyer, et al. World J Surgery 29:155-9, 2005.

29 Response to adrenalectomy 100% 80% 60% 98% Predictors of cure Family history in multiple individuals Number of medications 40% 33% 20% 0% Cure Improved AM Sawka, et al. Ann Intern Med 135:258-61, 2001.
30 Treatment of primary hyperaldosteronism Unilateral Laparoscopic adrenalectomy Bilateral Aldosterone receptor antagonists Spironolactone Eplerenone

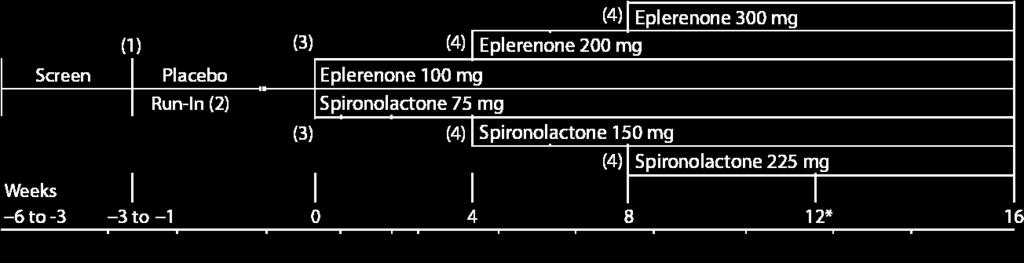
31 Which is better, spironolactone or eplerenone?

32 SBP response to eplerenone vs spironolactone HK Parthasarathy, et al, J Hypertension 29: , 2011.

33 DBP response to eplerenone vs spironolactone HK Parthasarathy, et al, J Hypertension 29: , 2011.

34 Likelihood of response DBP < 90 or Δ 10 80% 70% 71% 75% 68% 60% 50% 45% 46% 47% % Responding 40% 30% 30% 35% Spironolactone Eplerenone 20% 10% 0% Weeks HK Parthasarathy, et al, J Hypertension 29: , 2011.

35 Study withdrawals 40% 35% 30% 25% 20% 15% 20% 11% Spironolactone Eplerenone 10% 5% 4% 4% 0% Total withdrawals Treatment failure Adverse event Other HK Parthasarathy, et al, J Hypertension 29: , 2011.

36 Study withdrawals 40% 37% 35% 30% 25% 20% 15% 10% 5% 20% 4% 20% 11% 10% 4% 7% Spironolactone Eplerenone 0% Total withdrawals Treatment failure Adverse event Other HK Parthasarathy, et al, J Hypertension 29: , 2011.
37 Why does spironolactone appear more effective? Eplerenone Half-life, ~4 hrs Metabolites Biologically inactive Spironolactone Half-life 1-2 hrs Metabolites, Biologically active Half-life, ~15 hrs Effectively is a pro-drug of a variety of compounds with long half-lives
38 Tolerability differences Favoring eplerenone Breast discomfort (M&F) Breast tenderness (M&F) Favoring spironolactone Feeling out of touch with reality Difficulty thinking Feeling lost, disoriented Unawareness of what is going on General weakness Difficulty planning, organizing Tiredness, feeling weary HK Parthasarathy, et al, J Hypertension 29: , 2011.

39 Refractory Hypertension ARR and Plasma Aldosterone Aldosterone suppressed; Plasma renin activity suppressed Primary Aldosteronism unlikely Suppressed ARR Plasma aldosterone after oral NaCl loading Non-suppressed ARR >750 and [Aldo] > 300; Renin suppressed; Aldosterone not! Primary Aldosteronism Surgical Candidate? Begin MR Blocker Yes Positive Adrenal Protocol CT Scan No Adrenal Vein Aldosterone Sampling Negative Optimize MR Blocker Unilateral Aldosterone Release Laparoscopic Adrenalectomy Bilateral Aldosterone Release Optimize MR Blocker No Optimize MR Blocker Adequate BP Response? Yes Continue Therapy
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Clarification of hypertension Diagnosis of primary hyperaldosteronism
 Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Primary Aldosteronism & Implications for Primary Hypertension
 & Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
& Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
About 20% of the Canadian population
 Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Aldosterone synthase inhibitors. John McMurray BHF Cardiovascular Research Centre University of Glasgow
 Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN
 Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism
 Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
pharmacology sheet #9 Adrenal Steroids Mineral corticoids & Glucocorticoids
 Adrenal Steroids Mineral corticoids & Glucocorticoids Extra notes : Slide 2: - All Steroids are synthesized in the adrenal gland and secreted from it, It consists of an outer cortex and an inner medulla.
Adrenal Steroids Mineral corticoids & Glucocorticoids Extra notes : Slide 2: - All Steroids are synthesized in the adrenal gland and secreted from it, It consists of an outer cortex and an inner medulla.
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT?
 ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ENDOCRINE FORMS OF HYPERTENSION. Michael Stowasser
 ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Hypertension and Diabetes. Edward Shahady MD Medical Director Diabetes Master Clinician Program Florida Academy of Family Physicians
 Hypertension and Diabetes Edward Shahady MD Medical Director Diabetes Master Clinician Program Florida Academy of Family Physicians Objectives Describe the prevalence of hypertension and hypertension control
Hypertension and Diabetes Edward Shahady MD Medical Director Diabetes Master Clinician Program Florida Academy of Family Physicians Objectives Describe the prevalence of hypertension and hypertension control
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes
 ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
--Manuscript Draft-- Primary Aldosteronism; adrenal vein sampling; aldosterone producing adenoma. Brisbane, Queensland, AUSTRALIA
 Journal of Hypertension Repeating adrenal vein sampling when neither aldosterone/cortisol ratio exceeds peripheral yields a high incidence of aldosterone-producing adenoma --Manuscript Draft-- Manuscript
Journal of Hypertension Repeating adrenal vein sampling when neither aldosterone/cortisol ratio exceeds peripheral yields a high incidence of aldosterone-producing adenoma --Manuscript Draft-- Manuscript
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Heart Failure Treatments
 Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Spectrum of Hypertension & Hypokalemia
 Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Amplified Screening and Workup Protocol for Primary Aldosteronism: A Strategy to Improve
 Amplified Screening and Workup Protocol for Primary Aldosteronism: A Strategy to Improve New Zealand s Woefully Low Diagnostic Rates? / Original Article Authors Walter van der Merwe Veronica van der Merwe
Amplified Screening and Workup Protocol for Primary Aldosteronism: A Strategy to Improve New Zealand s Woefully Low Diagnostic Rates? / Original Article Authors Walter van der Merwe Veronica van der Merwe
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Disclosure of Relationships
 Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
FOUR CASES OF HYPOVOLEMIC RENIN-ALDOSTERONE AXIS DEFICIENCY WITHOUT HYPERKALEMIA FOLLOWING UNILATERAL ADRENALECTOMY FOR PRIMARY ALDOSTERONISM
 Case Report FOUR CASES OF HYPOVOLEMIC RENIN-ALDOSTERONE AXIS DEFICIENCY WITHOUT HYPERKALEMIA FOLLOWING UNILATERAL ADRENALECTOMY FOR PRIMARY ALDOSTERONISM Marion Vallet, MD 1 *; Alexandre Martin, MD 1 *;
Case Report FOUR CASES OF HYPOVOLEMIC RENIN-ALDOSTERONE AXIS DEFICIENCY WITHOUT HYPERKALEMIA FOLLOWING UNILATERAL ADRENALECTOMY FOR PRIMARY ALDOSTERONISM Marion Vallet, MD 1 *; Alexandre Martin, MD 1 *;
Analysis of AVP functions via V1a and V1b receptors with knockout mice. Akito Tanoue
 Analysis of AVP functions via V1a and V1b receptors with knockout mice Akito Tanoue Department of Pharmacology, National Research Institute for Child Health and Development Arginine-Vasopressin (AVP) is
Analysis of AVP functions via V1a and V1b receptors with knockout mice Akito Tanoue Department of Pharmacology, National Research Institute for Child Health and Development Arginine-Vasopressin (AVP) is
A 64 year old man referred for evaluation of suspected hyperaldosteronism
 A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
Therefore MAP=CO x TPR = HR x SV x TPR
 Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use aldosterone blockers? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart
DECLARATION OF CONFLICT OF INTEREST TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use aldosterone blockers? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart
Patients with primary aldosteronism (PA) are at a higher
 are at a higher") ORIGINAL ARTICLE Endocrine Care Predictors of Decreasing Glomerular Filtration Rate and Prevalence of Chronic Kidney Disease After Treatment of Primary Aldosteronism: Renal Outcome of 213 Cases Yoshitsugu
ORIGINAL ARTICLE Endocrine Care Predictors of Decreasing Glomerular Filtration Rate and Prevalence of Chronic Kidney Disease After Treatment of Primary Aldosteronism: Renal Outcome of 213 Cases Yoshitsugu
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
The real picture. Prorenin (Renin) PRR AT3 AT4. AT4 receptor. PAI 1 Abassi, Biochem Pharm, 2009
 PRR AT3 AT4. AT4 receptor. PAI 1 Abassi, Biochem Pharm, 2009") The real picture. Prorenin (Renin) PRR AT3-8 AT4 AT10-12 AT3 AT4 receptor PAI 1 Abassi, Biochem Pharm, 2009 Resistant Hypertension; Case based discussion Moving Targets? RAAS blockade in hypertensive CKD
The real picture. Prorenin (Renin) PRR AT3-8 AT4 AT10-12 AT3 AT4 receptor PAI 1 Abassi, Biochem Pharm, 2009 Resistant Hypertension; Case based discussion Moving Targets? RAAS blockade in hypertensive CKD
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hyperaldosteronism: Conn's Syndrome
 RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich,
 The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
Resistant hypertension is defined as blood. Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension.
 Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Hypertension Cases. Katharine Dahl, MD January 10, 2017
 Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Diuretics (Saluretics)
") Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
DIRECT RENIN INHIBITOR (DRI) EFFECT ON GFR AND USE IN RENAL ARTERY STENOSIS SCREENING
 EFFECT ON GFR AND USE IN RENAL ARTERY STENOSIS SCREENING") DIRECT RENIN INHIBITOR (DRI) EFFECT ON GFR AND USE IN RENAL ARTERY STENOSIS SCREENING Harold Thomas Pretorius, MD, PhD, Nichole Richards, and Michael Harrell Abstract Objective: A new method using a nuclear
DIRECT RENIN INHIBITOR (DRI) EFFECT ON GFR AND USE IN RENAL ARTERY STENOSIS SCREENING Harold Thomas Pretorius, MD, PhD, Nichole Richards, and Michael Harrell Abstract Objective: A new method using a nuclear
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Adrenal Steroids Mineralocorticoids & Glucocorticoids. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine The Jordan University April 2014
 Adrenal Steroids Mineralocorticoids & Glucocorticoids Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine The Jordan University April 2014 Medulla (E, NE) Adrenal Gland Cortex Mineralocorticoids (Aldosterone)
Adrenal Steroids Mineralocorticoids & Glucocorticoids Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine The Jordan University April 2014 Medulla (E, NE) Adrenal Gland Cortex Mineralocorticoids (Aldosterone)
Changes in the clinical manifestations of primary aldosteronism
 ORIGINAL ARTICLE Korean J Intern Med 2014;29:217-225 Changes in the clinical manifestations of primary aldosteronism Sun Hwa Kim, Jae Hee Ahn, Ho Cheol Hong, Hae Yoon Choi, Yoon Jung Kim, Nam Hoon Kim,
ORIGINAL ARTICLE Korean J Intern Med 2014;29:217-225 Changes in the clinical manifestations of primary aldosteronism Sun Hwa Kim, Jae Hee Ahn, Ho Cheol Hong, Hae Yoon Choi, Yoon Jung Kim, Nam Hoon Kim,
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Disorders of the Adrenal Cortex
 Disorders of the Adrenal Cortex Cushing s Syndrome and Primary Aldosteronism 凌雁 Yan Ling Department of Endocrinology and Metabolism Zhongshan Hospital Fudan University Cushing s Syndrome Definition of
Disorders of the Adrenal Cortex Cushing s Syndrome and Primary Aldosteronism 凌雁 Yan Ling Department of Endocrinology and Metabolism Zhongshan Hospital Fudan University Cushing s Syndrome Definition of
Special Lecture 11/08/2013. Hypertension Dr. HN Mayrovitz
 Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Potassium A NNA VINNIKOVA, M. D.
 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Prevalence and characterization of somatic mutations in Chinese aldosterone-producing adenoma. patients. Supplemental data. First author: Baojun Wang
 Prevalence and characterization of somatic mutations in Chinese aldosterone-producing adenoma patients Supplemental data First author: Baojun Wang Patients and tumor samples A total of 87 patients with
Prevalence and characterization of somatic mutations in Chinese aldosterone-producing adenoma patients Supplemental data First author: Baojun Wang Patients and tumor samples A total of 87 patients with
Blood Pressure Regulation 2. Faisal I. Mohammed, MD,PhD
 Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2. Faisal I. Mohammed, MD,PhD
 Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Blood Pressure Regulation 2 Faisal I. Mohammed, MD,PhD 1 Objectives Outline the intermediate term and long term regulators of ABP. Describe the role of Epinephrine, Antidiuretic hormone (ADH), Renin-Angiotensin-Aldosterone
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment
 Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson