2/27/19 TALES FROM THE COMMUNITY PEM DEPT: SCARY CASES! Solomon Behar, MD, FAAP, FACEP March 2, 2019
|
|
|
- Dortha Simpson
- 5 years ago
- Views:
Transcription

1 TALES FROM THE COMMUNITY PEM DEPT: SCARY CASES! Solomon Behar, MD, FAAP, FACEP March 2,

2 OBJECTIVES v Understand the ddx and management of abdominal masses in kids v Understand strategies for dealing with the patient in refractory status epilepticus and alternate routes of giving AEDs v Discuss the ddx of torticollis in children v Discuss the ddx and management of UGI bleeding in kids A HAIRY SITUATION 2
3 4 YR F LEFT SIDED ABDOMINAL MASS v No V/D, some hard BMs, no blood, normal UOP/quality, v No weight loss or B symptoms, picky eater v PMHx: Fe deficiency v AF, Normal VS v Normal exam except for firm LUQ mass v Labs: WBC 6.1, Hgb 7.8 (MCV 67), Plt 623 v Normal renal function, UA DDX ABDOMINAL MASS IN KIDS v Age Infants: think RENAL, MALIGNANCY Young kids: RENAL, POOP, HSM, MALIGNANCY Older kids: POOP, HSM, MALIGNANCY v Location v Associated symptoms: fever, weight loss, hematuria, HTN, vomiting, blood in stool? 3


4 MALIGNANT MASSES v Wilm s Tumor MC primary renal tumor Asymptomatic abdominal mass Hematuria, pain, vomiting, HTN WAGR syndrome Aniridia GU anomalies MR Hemihypertrophy Peak age 2-3 yrs MALIGNANT MASSES v Neuroblastoma Ill appearing Horner s syndrome, Opsoclonusmyoclonus Hoarseness, Periorbital ecchymosis Elevated HVA, VMA in urine 90% dx before age 5 yrs 4
5 YOUNGER/SLOWER GROWINGà more likely benign OLDER/FASTER GROWINGà more likely malignant WORK-UP v UA, check BP v CBC, CMP, tumor lysis labs infectious work-up?, tumor markers? v Imaging: KUB/US to start 5





6 TRICHOBEZOAR= RAPUNZEL SYNDROME 6

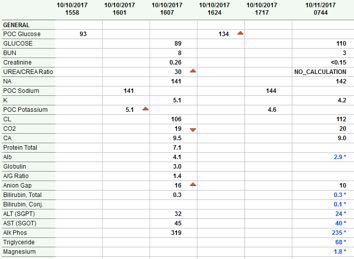
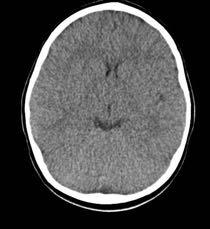
7 SICK IN THE HEAD 8 MOS F EMS D IN FOR SEIZURE v 60 GTC refractory to therapy v T 101.2, HR 200 s, vomiting orange x4 during resusc v Pupils big and equal, intermittent vocalizing v Small rhinorrhea today v Mom lives in motel with baby v No home meds, no TB contacts 7



8 WHAT WOULD YOU GIVE? v Benzos v Fos-phenytoin v Leviteracetam v (phenobarbital) v Dextrose v Pyridoxine v Abx? Alternate routes? IN midazolam (0.2mg/kg) PR diazepam (0.5 mg/kg, max 20mg) 8


9 9

10 10

11 PAIN IN THE NECK 2 ½ YR OLD F WON T MOVE NECK, FEVER, AND PHOTOPHOBIA v Started with cough, URI, sore throat starting 4-5 d ago v Mom thought she slept funny v Febrile to 102.5, fussy, torticollis to right v Refused to move neck, mental status ok,?photophobia v 2-3+ tonsils, red OP, uvula midline. Mouth closed, refusing PO v Cervical LAD R>L v No stridor 11


12 DDX? v Meningitis v Lymphadenitis v Bad pharyngitis v RPA v Epidural abscess v Dystonia WORK-UP? v WBC 18.9, left shift v CRP: elevated v LP: 12



13 13
14 RETROPHARYNGEAL ABSCESS v Age < 6 yrs v Polymicrobial v ENT consult STAT v IV antibiotics +/- OR BE CAREFUL WHAT YOU WISH FOR 14

15 13 YO M MRCP, AUTISM, BREAKTHROUGH SEIZURE v BIB EMS, not seizing v Afebrile, HR 160 s, BP ok v Pale but awake v No bruising or petechiae v No recent illness, but not acting himself x2 weeks WHY YOU NEED TO DO COMPLETE PHYSICALS 15


16 Normal coags, normal LFT s 16
17 UGI BLEEDING IN KIDS: DDX VIT K! v Epistaxis** v PUD/H Pylori v Esophagitis/GER v FB, esp button battery v Caustic ingestion v Coagulopathy v Mallory-Weiss v Pulm HTN/varices v Vascular lesions/polyps v IBD (Crohn s) v Medications (NSAIDs) MANAGEMENT v Resuscitate with IVF s v prbc s/ffp if HD unstable, Hgb <8 v Start PPI (1 mg/kg) v If variceal source, octreotide (1mcg/kg bolus, 1-2 mcg/kg/hr gtt) v Emergent endoscopy or OR v??? NG lavage??? 17


18 18




19 DR. DANNY CHOI Thank you! SEE YOU IN THE LBC! HAPPY HALLOWEEN 19
5/23/14. Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments
 Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Pediatric Case Studies. Case 1
 Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
Real Cases: Bad Outcomes
 Real Cases: Bad Outcomes Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Real Cases: Bad Outcomes Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
GOOD MORNING! July 3, 2014
 GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
The Crashing Pediatric Patient: Stopping the Fall
 The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Treating A Sore Throat With Intubation. A case of Epiglottitis in an elderly patient. Sherif Yani, PGY3 St Joseph s FM Residency
 Treating A Sore Throat With Intubation A case of Epiglottitis in an elderly patient. Sherif Yani, PGY3 St Joseph s FM Residency Outline H&P Diagnosis Management Discussion Take-Home Points History 88 y/o
Treating A Sore Throat With Intubation A case of Epiglottitis in an elderly patient. Sherif Yani, PGY3 St Joseph s FM Residency Outline H&P Diagnosis Management Discussion Take-Home Points History 88 y/o
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
First Take Home point
 Common Presentations of Childhood Cancer First Take Home point Childhood Cancer is a rare disease New Cases of Cancer in the U.S. in 2003 Number 140000 120000 100000 80000 60000 40000 20000 0 130,000 105,000000
Common Presentations of Childhood Cancer First Take Home point Childhood Cancer is a rare disease New Cases of Cancer in the U.S. in 2003 Number 140000 120000 100000 80000 60000 40000 20000 0 130,000 105,000000
PDF created with pdffactory Pro trial version
 Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Steroid Storms: Controversies and Considerations in PEM
 Steroid Storms: Controversies and Considerations in PEM Kimball Prentiss, MD, FAAP Division of Pediatric Emergency Medicine September 19, 2018 CCEM Conference, Northampton Objectives Develop an understanding
Steroid Storms: Controversies and Considerations in PEM Kimball Prentiss, MD, FAAP Division of Pediatric Emergency Medicine September 19, 2018 CCEM Conference, Northampton Objectives Develop an understanding
WHOLE LOTTA SHAKIN GOIN ON
 WHOLE LOTTA SHAKIN GOIN ON ADAM M. YATES, MD FACEP ASSOCIATE CHIEF OF EMERGENCY SERVICES UPMC MERCY SEIZURE DEFINITIONS Partial(focal) only involves part of the brain General Involves entire brain Simple
WHOLE LOTTA SHAKIN GOIN ON ADAM M. YATES, MD FACEP ASSOCIATE CHIEF OF EMERGENCY SERVICES UPMC MERCY SEIZURE DEFINITIONS Partial(focal) only involves part of the brain General Involves entire brain Simple
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
KIDS PUT THINGS IN THE CRAZIEST PLACES...
 KIDS PUT THINGS IN THE CRAZIEST PLACES... YOU CAN T MAKE ME EAT MY DINNER! 2 year old observed to stuff corn up right nostril Judith Klein, MD FACEP Assistant Professor of Emergency Medicine UCSF-SFGH
KIDS PUT THINGS IN THE CRAZIEST PLACES... YOU CAN T MAKE ME EAT MY DINNER! 2 year old observed to stuff corn up right nostril Judith Klein, MD FACEP Assistant Professor of Emergency Medicine UCSF-SFGH
Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases
 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases") Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases Disclosures Advisory board member for GSK (for belimumab pregnancy registry). Co-founder of Grid
Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases Disclosures Advisory board member for GSK (for belimumab pregnancy registry). Co-founder of Grid
Pediatric Gastroenterology Referral Guidelines
 Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
It s Monday! July 28, 2014
 It s Monday! July 28, 2014 Prep Question The mother of a 6-year-old girl reports during a health supervision visit that her daughter has nighttime wetting and occasional daytime accidents with urgency.
It s Monday! July 28, 2014 Prep Question The mother of a 6-year-old girl reports during a health supervision visit that her daughter has nighttime wetting and occasional daytime accidents with urgency.
Management of Complex Febrile Seizures
 Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Scenario #4A: Geriatric Trauma Resuscitation Version-5
 Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Fever in Babies. Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
 Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
New Concepts in Acute Coronary Syndromes Beyond 2000 (XX) Interactive Case Presentations
 Interactive Case Presentations") New Concepts in Acute Coronary Syndromes Beyond 2000 (XX) Interactive Case Presentations Dr. Richard Bon Surrey Memorial Hospital, Surrey, BC Canadian Cardiovascular Congress 2014 October 26, 2014 Conflicts
New Concepts in Acute Coronary Syndromes Beyond 2000 (XX) Interactive Case Presentations Dr. Richard Bon Surrey Memorial Hospital, Surrey, BC Canadian Cardiovascular Congress 2014 October 26, 2014 Conflicts
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
Dr.Dafalla Ahmed Babiker Jazan University
 Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
Mediastinitis. Jonathan Parks, MD Kings County Medical Center December 3, 2015
 Mediastinitis Jonathan Parks, MD Kings County Medical Center December 3, 2015 Case Presentation 69 year-old male from nursing home PMHx: COPD, asthma, HTN, Afib on pradaxa, PTSD, BPH c/o pulled pork stuck
Mediastinitis Jonathan Parks, MD Kings County Medical Center December 3, 2015 Case Presentation 69 year-old male from nursing home PMHx: COPD, asthma, HTN, Afib on pradaxa, PTSD, BPH c/o pulled pork stuck
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
ENT Combined Meeting Presentation. Eric Post Tygerberg Hospital 31 Jan 06
 ENT Combined Meeting Presentation Eric Post Tygerberg Hospital 31 Jan 06 Case presentation 1 72 yo F Kuils Rivier Acute onset and progressive FOM swelling Develop progressive swelling of tongue Ooze blood
ENT Combined Meeting Presentation Eric Post Tygerberg Hospital 31 Jan 06 Case presentation 1 72 yo F Kuils Rivier Acute onset and progressive FOM swelling Develop progressive swelling of tongue Ooze blood
Standardized Nurse Activated Protocols (SNAPs)
") SNAPs by presenting complaint/problem help nurses initiate care before the patient is seen by a physician. SNAPs should be approved by ED team consensus If patient unstable in any way, immediately notify
SNAPs by presenting complaint/problem help nurses initiate care before the patient is seen by a physician. SNAPs should be approved by ED team consensus If patient unstable in any way, immediately notify
Down the Tube: Caustic Ingestions. Significance & Management in the ED. Laura Chng PGY-3
 Down the Tube: Caustic Ingestions Significance & Management in the ED Laura Chng PGY-3 Caustic Ingestions Not common but you ll see them Controversial You drank WHAT? ED management can change outcome Who
Down the Tube: Caustic Ingestions Significance & Management in the ED Laura Chng PGY-3 Caustic Ingestions Not common but you ll see them Controversial You drank WHAT? ED management can change outcome Who
Status Epilepticus in Children
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
NonConvulsive Seizure
 Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Student Guide Module 5: Management of Prevalent Infections in Children Following a Disaster
 Student Guide Module 5: Management of Prevalent Infections in Children Following a Disaster Objectives for this session Section I - Integrated Management of Childhood Illness (IMCI) Understand the IMCI
Student Guide Module 5: Management of Prevalent Infections in Children Following a Disaster Objectives for this session Section I - Integrated Management of Childhood Illness (IMCI) Understand the IMCI
Doctor, I Have Strep Throat. Nancy W Weber D.O. FACOEP FACEP MBA Sparrow/MSU Emergency Medicine Residency October 22, 2018
 Doctor, I Have Strep Throat Nancy W Weber D.O. FACOEP FACEP MBA Sparrow/MSU Emergency Medicine Residency October 22, 2018 Disclosures None The Patient: 41YOF CC: Sore throat x 3 days HPI: Sore throat increasing
Doctor, I Have Strep Throat Nancy W Weber D.O. FACOEP FACEP MBA Sparrow/MSU Emergency Medicine Residency October 22, 2018 Disclosures None The Patient: 41YOF CC: Sore throat x 3 days HPI: Sore throat increasing
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
CASES FOR DISCUSSION. Yohannes B
 CASES FOR DISCUSSION Yohannes B HCV CASE-1 A 34 years old apparently healthy lady who came to us after being told to have HCV infection on medical checkup done as part of a visa approval process to travel
CASES FOR DISCUSSION Yohannes B HCV CASE-1 A 34 years old apparently healthy lady who came to us after being told to have HCV infection on medical checkup done as part of a visa approval process to travel
Welcome to Big Sky Country. Pediatrics Infectious disease update. Todd TwogoodMD
 Welcome to Big Sky Country Pediatrics Infectious disease update Todd TwogoodMD My kid is always sick!! We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
Welcome to Big Sky Country Pediatrics Infectious disease update Todd TwogoodMD My kid is always sick!! We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
My kid is always sick!!
 Welcome to Big Sky Country My kid is always sick!! Pediatrics Infectious disease update Todd Twogood MD We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
Welcome to Big Sky Country My kid is always sick!! Pediatrics Infectious disease update Todd Twogood MD We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
JUST FOR KIDS SELECTED IMPORTANT SAFETY INFORMATION
 JUST FOR KIDS For children ages 6-17 with moderately to severely active Crohn s disease or ulcerative colitis (UC) who haven t responded well to other therapies SELECTED IMPORTANT SAFETY INFORMATION REMICADE
JUST FOR KIDS For children ages 6-17 with moderately to severely active Crohn s disease or ulcerative colitis (UC) who haven t responded well to other therapies SELECTED IMPORTANT SAFETY INFORMATION REMICADE
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Case Study 6C. [TQ, 7-months-old infant girl] Dengue Clinical Management. Acknowledgements
![Case Study 6C. [TQ, 7-months-old infant girl] Dengue Clinical Management. Acknowledgements](/thumbs/77/74744886.jpg "Case Study 6C. [TQ, 7-months-old infant girl] Dengue Clinical Management. Acknowledgements") Case Study 6C [TQ, 7-months-old infant girl] Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials
Case Study 6C [TQ, 7-months-old infant girl] Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEBRILE SEIZURES. IAP UG Teaching slides
 FEBRILE SEIZURES 1 DEFINITION Febrile seizures are seizures that occur between the age of 6 and 60 months with a temperature of 38 C or higher, that are not the result of central nervous system infection
FEBRILE SEIZURES 1 DEFINITION Febrile seizures are seizures that occur between the age of 6 and 60 months with a temperature of 38 C or higher, that are not the result of central nervous system infection
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Liver Transplant: What s Different? Brian Lin, MD, FACEP Emergency Medicine, Kaiser Permanente, San Francisco UCSF Clinical Assistant Professor
 Liver Transplant: What s Different? Brian Lin, MD, FACEP Emergency Medicine, Kaiser Permanente, San Francisco UCSF Clinical Assistant Professor No Disclosures. Background 45 years 1998-2008: 90,830 transplants
Liver Transplant: What s Different? Brian Lin, MD, FACEP Emergency Medicine, Kaiser Permanente, San Francisco UCSF Clinical Assistant Professor No Disclosures. Background 45 years 1998-2008: 90,830 transplants
TOPICS. Wheezing/Asthma THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE
 THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE Ghazala Q. Sharieff MD, MBA Wheezing/asthma Croup Immunizations and fever Appendicitis Complex febrile seizures Procedures Head Injury Zofran
THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE Ghazala Q. Sharieff MD, MBA Wheezing/asthma Croup Immunizations and fever Appendicitis Complex febrile seizures Procedures Head Injury Zofran
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GASTROINTESTINAL BLEEDING. Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
 GASTROINTESTINAL BLEEDING Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Gastrointestinal Bleeding Hematemesis- Vomiting of bright red blood
GASTROINTESTINAL BLEEDING Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Gastrointestinal Bleeding Hematemesis- Vomiting of bright red blood
Grand Rounds: Pediatric Dysphagia Due to Anatomic & Neurologic Etiologies
 Joan C. Arvedson, PhD, BC-NCD, BRS-S Children's Hospital of Wisconsin Milwaukee Department of Pediatrics, Medical College of Wisconsin Maureen A. Lefton-Greif, PhD, CCC/SLP, BRS-S Johns Hopkins Medical
Joan C. Arvedson, PhD, BC-NCD, BRS-S Children's Hospital of Wisconsin Milwaukee Department of Pediatrics, Medical College of Wisconsin Maureen A. Lefton-Greif, PhD, CCC/SLP, BRS-S Johns Hopkins Medical
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
ENCEPHALITIS. Diana Montoya Melo
 ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
WHAT ARE PAEDIATRIC CANCERS
 WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
The Basics. Presentations. The Olympics, of course. Common pitfalls Tips on improving
 August 2012 The Basics Presentations Common pitfalls Tips on improving The Olympics, of course What is clinical reasoning?? The process by which doctors funnel their thinking towards probable diagnosis
August 2012 The Basics Presentations Common pitfalls Tips on improving The Olympics, of course What is clinical reasoning?? The process by which doctors funnel their thinking towards probable diagnosis
Outline. What is a seizure? What is epilepsy? Updates in Seizure Management Terminology, Triage & Treatment
 Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
echam Training Scenarios
 echam Training Scenarios #1: You are 250 miles from the nearest hospital or subregional clinic. You are on a call and receive notification at 1230am of a 4-wheeler accident involving severe injuries. It
echam Training Scenarios #1: You are 250 miles from the nearest hospital or subregional clinic. You are on a call and receive notification at 1230am of a 4-wheeler accident involving severe injuries. It
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Red Stick ID Visual Diagnosis Questions August 22, 2014
 Red Stick ID Visual Diagnosis Questions August 22, 2014 James H. Brien, DO Case #1 The setting is a Pediatric Clinic in San Antonio, Texas on a Saturday in 1989. However, it could have been yesterday in
Red Stick ID Visual Diagnosis Questions August 22, 2014 James H. Brien, DO Case #1 The setting is a Pediatric Clinic in San Antonio, Texas on a Saturday in 1989. However, it could have been yesterday in
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
INTRODUCTION TO UPPER ENDOSCOPY
 INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
Pediatric Procedural Sedation
 Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Leukocytosis. dr. Erdélyi, Dániel 2 nd Department of Paediatrics Semmelweis University
 Leukocytosis dr. Erdélyi, Dániel 2 nd Department of Paediatrics Semmelweis University My first day at work in 1997 3y with fever, cough Is this bronchitis, pneumonia, pharyngitis, sinusitis, else? Is this
Leukocytosis dr. Erdélyi, Dániel 2 nd Department of Paediatrics Semmelweis University My first day at work in 1997 3y with fever, cough Is this bronchitis, pneumonia, pharyngitis, sinusitis, else? Is this
PEDIATRIC INFECTIOUS DISEASES UPDATE. Neonatal HSV. Recognition, Diagnosis, and Management Coleen Cunningham MD
 Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
9 year-old Female with Papillary Thyroid Cancer. Katie O Sullivan, M.D. Fellow Medicine/Pediatric Endocrinology Thursday, January 16 th, 2014
 9 year-old Female with Papillary Thyroid Cancer Katie O Sullivan, M.D. Fellow Medicine/Pediatric Endocrinology Thursday, January 16 th, 2014 Chief Complaint Mass on the right side of the neck x 2-3 weeks
9 year-old Female with Papillary Thyroid Cancer Katie O Sullivan, M.D. Fellow Medicine/Pediatric Endocrinology Thursday, January 16 th, 2014 Chief Complaint Mass on the right side of the neck x 2-3 weeks
New Guidelines for Tonsillectomy Daniel C. Chelius, Jr., MD Pediatric Otolaryngolo Pediatric Otolary gy--head Head and Neck S and Neck u S rgery
 New Guidelines for Tonsillectomy Daniel C. Chelius, Jr., MD Pediatric Otolaryngology-Head and Neck Surgery November 16, 2011 EXIT Procedures Sinus surgery/skull base surgery Head and Neck Cancers Thyroid/Parathyroid
New Guidelines for Tonsillectomy Daniel C. Chelius, Jr., MD Pediatric Otolaryngology-Head and Neck Surgery November 16, 2011 EXIT Procedures Sinus surgery/skull base surgery Head and Neck Cancers Thyroid/Parathyroid
The Limits of Harm Reduction? Neil McKeganey Centre for Substance Use Research West of Scotland Science Park Glasgow Scotland
 The Limits of Harm Reduction? Neil McKeganey Centre for Substance Use Research West of Scotland Science Park Glasgow Scotland Principle of Harm Reduction First Do No Harm Hippocratic Oath I will use treatment
The Limits of Harm Reduction? Neil McKeganey Centre for Substance Use Research West of Scotland Science Park Glasgow Scotland Principle of Harm Reduction First Do No Harm Hippocratic Oath I will use treatment
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants
 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
CrackCast Episode 18 Seizures
 CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
Citywide Infectious Disease Conference. March 27 th, 2018
 Citywide Infectious Disease Conference March 27 th, 2018 Citywide Show and Tell Case 1 Summary 60 s year old Puerto Rican born man SCC of Esophagus, treated with radiation and chemotherapy and then esophageal
Citywide Infectious Disease Conference March 27 th, 2018 Citywide Show and Tell Case 1 Summary 60 s year old Puerto Rican born man SCC of Esophagus, treated with radiation and chemotherapy and then esophageal
Infectious diseases Dr n. med. Agnieszka Topczewska-Cabanek
 Infectious diseases Dr n. med. Agnieszka Topczewska-Cabanek Viral: Exanthema subitum (Roseaola infantum) Herpetic stomatitis Measles Rubella Chickenpox Erythema infectious (5th Disease, Slapped cheec disease)
Infectious diseases Dr n. med. Agnieszka Topczewska-Cabanek Viral: Exanthema subitum (Roseaola infantum) Herpetic stomatitis Measles Rubella Chickenpox Erythema infectious (5th Disease, Slapped cheec disease)
Medical Hockey Scenarios What Would You Do? Case Presentation. Dr. Noah Forman AOSSM August 2015
 Medical Hockey Scenarios What Would You Do? Case Presentation Dr. Noah Forman AOSSM August 2015 What Would You Do? Discussion Points Mechanism of injury Assessment of injury and player presentation Are
Medical Hockey Scenarios What Would You Do? Case Presentation Dr. Noah Forman AOSSM August 2015 What Would You Do? Discussion Points Mechanism of injury Assessment of injury and player presentation Are
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Can t Stop the Seizing!
 Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Guideline for the Management of Upper Gastrointestinal Bleeding in Children
 Guideline for the Management of Upper Gastrointestinal Bleeding in Children 1. Introduction Upper gastrointestinal (UGI) bleeding in children poses a challenge to paediatricians and paediatric surgeons.
Guideline for the Management of Upper Gastrointestinal Bleeding in Children 1. Introduction Upper gastrointestinal (UGI) bleeding in children poses a challenge to paediatricians and paediatric surgeons.
NEW PATIENT HEALTH HISTORY
 NEW PATIENT HEALTH HISTORY Patient Name Today s Date Age Birth Date Date of last physical examination What is your reason for initial visit? Pharmacy Name & Telephone # NOTE: If you have prior records
NEW PATIENT HEALTH HISTORY Patient Name Today s Date Age Birth Date Date of last physical examination What is your reason for initial visit? Pharmacy Name & Telephone # NOTE: If you have prior records
Management of the Hospitalized IBD Patient. Drew DuPont MD
 Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
Refractory Seizures. Dr James Edwards EMCORE May 30th 2014
 Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD
 ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
11/21/2017 JUST THE FACTS!
 JUST THE FACTS! Katharine C Long, MD Establish differential diagnosis for the critically ill infant Create management approach for the critically ill infant Identify laboratory tests and interventions
JUST THE FACTS! Katharine C Long, MD Establish differential diagnosis for the critically ill infant Create management approach for the critically ill infant Identify laboratory tests and interventions
Matthew Ulrickson, MD Banner MD Anderson Cancer Center September 12, 2017
 Matthew Ulrickson, MD Banner MD Anderson Cancer Center September 12, 2017 Discuss the clinical presentation and diagnosis of acute leukemia * Discuss the impact of molecular features on prognosis and management
Matthew Ulrickson, MD Banner MD Anderson Cancer Center September 12, 2017 Discuss the clinical presentation and diagnosis of acute leukemia * Discuss the impact of molecular features on prognosis and management
Fever in Children. Sue Moore APRN, ENP-C (almost retired)
") Fever in Children Sue Moore APRN, ENP-C (almost retired) Topics Definiton Taking the temp Function of fever Reasons for treating fever How antipyretics work Fever: Temperature over 38 C Taking the Temp
Fever in Children Sue Moore APRN, ENP-C (almost retired) Topics Definiton Taking the temp Function of fever Reasons for treating fever How antipyretics work Fever: Temperature over 38 C Taking the Temp
STORMY DENGUE with bloody problems. Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai
 STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Case Presentation. Rafid Asfar, MD
 Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Hand-Carried Ultrasound Performed by a Hospitalist to Assist with Clinical Decisions in Medicine Inpatients: a Case Series
 Hand-Carried Ultrasound Performed by a Hospitalist to Assist with Clinical Decisions in Medicine Inpatients: a Case Series Stefan Tchernodrinski, MD Cook County Hospital Chicago, Illinois Introduction
Hand-Carried Ultrasound Performed by a Hospitalist to Assist with Clinical Decisions in Medicine Inpatients: a Case Series Stefan Tchernodrinski, MD Cook County Hospital Chicago, Illinois Introduction
Hi doctor, can you come and see my patient, she s just had a coffee ground vomit. Dr Rhona Hurley, FY2
 Hi doctor, can you come and see my patient, she s just had a coffee ground vomit. Dr Rhona Hurley, FY2 Ask for more information What now? o What might you ask? o Do you have enough information about this
Hi doctor, can you come and see my patient, she s just had a coffee ground vomit. Dr Rhona Hurley, FY2 Ask for more information What now? o What might you ask? o Do you have enough information about this
Fever in Children. Topics. Fever: Temperature over. Definiton Taking the temp Function of fever Reasons for treating fever How antipyretics work
 Fever in Children Sue Moore RN, MSN, CCRN, CFRN, NP-C Topics Definiton Taking the temp Function of fever Reasons for treating fever How antipyretics work Fever: Temperature over 1 Taking the Temp Which
Fever in Children Sue Moore RN, MSN, CCRN, CFRN, NP-C Topics Definiton Taking the temp Function of fever Reasons for treating fever How antipyretics work Fever: Temperature over 1 Taking the Temp Which
echam Training Scenarios
 echam Training Scenarios #1: You are 250 miles from the nearest hospital or subregional clinic. You are on a call and receive notification at 1230am of a 4-wheeler accident involving severe injuries. It
echam Training Scenarios #1: You are 250 miles from the nearest hospital or subregional clinic. You are on a call and receive notification at 1230am of a 4-wheeler accident involving severe injuries. It
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
Children ARE just small adults
 History of Pediatrics Children ARE just small adults VICKI L. SAKATA, MD, FAAEM, FAAP SENIOR MEDICAL ADVISOR, NWHRN WA 1 DMAT MAC T MEDICAL OFFICER MARY BRIDGE CHILDREN S HOSPITAL Ex toto non sic pueri
History of Pediatrics Children ARE just small adults VICKI L. SAKATA, MD, FAAEM, FAAP SENIOR MEDICAL ADVISOR, NWHRN WA 1 DMAT MAC T MEDICAL OFFICER MARY BRIDGE CHILDREN S HOSPITAL Ex toto non sic pueri