Aspiration pneumonia in older people
|
|
|
- Joshua Ryan
- 5 years ago
- Views:
Transcription
1 Aspiration pneumonia in older people Ayman Morish, M.D. Internal medicine, Critical care Medicine and Geriatrics Fellow.
2 Contents Epidemiology Causes of aspiration pneumonia Issues of older age Management Prevention
3 Case 1: admission Jan 26 CHIEF COMPLAINT(S): weakness and feeling unwell HPI: 90-year-old gentleman. Came from an assisted living facility feeling weak for the past 4 days. PMH: ESRD on HD, AFib, COPD, CHF, HTN, CAD. SHx: Assisted living facility. Independent in most of his ADLs and need moderate support with transfer and mobilities.
4 P/E VITALS: tachycardia 121, others unremarkable. Abd: + BS, soft, non-tender, no masses. CVS: S1+S2, Irregularly irregular, holo-systolic murmur. No JVD. Neuro: AAOX3, grossly intact, able to move UE and LE Chest: reduced air entry, no wheezing or crackles. Extremity: No pitting edema, normal pulses.
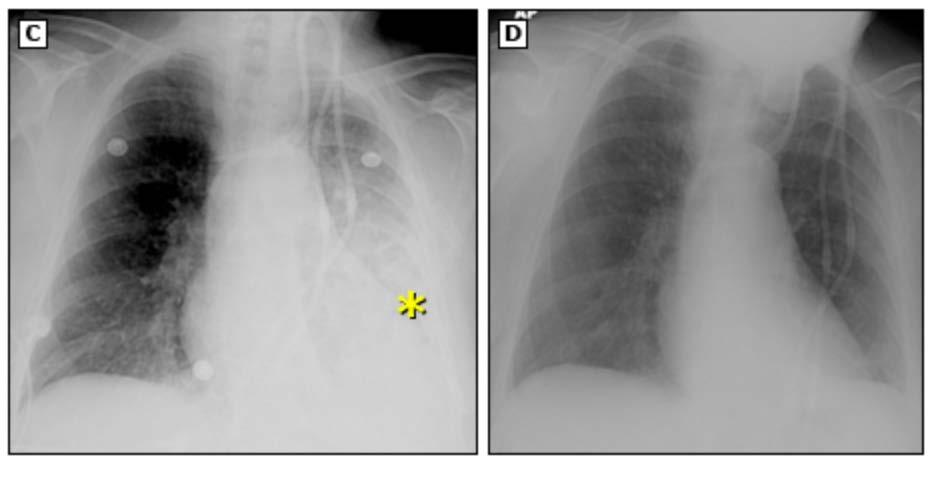
5 Lab and Imagining WBC 6.93 Na 138 K 3.9 BUN 19 Creat 2.9 BNP 2687 CXR: Left LL infiltrate / atelectasis. Hyperinflated lung suggesting COPD.
6 What do you think is going on? Hold your thoughts for now..
7 Case 2: Admission Feb 14 CHIEF COMPLAINT(S): Weakness, cough, nausea and vomiting. HPI: 90-year-old gentleman. Came from an assisted living facility complaining of vomiting 3-4 times, chocking and coughing with eating. Had a recent history of pneumonia 3 weeks ago and was treated with antibiotics. PMH: ESRD on HD, AFib, COPD, CHF, HTN, CAD. SHx: Assisted living facility. Independent in most of his ADLs and need moderate support with transfer and mobilities.
8 P/E VITALS: stable Chest: b/l crackles, left>right Gen: cachectic and ill appearing Abd: + BS, soft, non-tender, no rigidity Mouth: dry oral mucosa CVS: S1+S2, Irregularly irregular, 3/6 murmur in the mitral area. Neuro: AAOX3, No gross motor or sensory deficit Extremities: pitting edema, normal pulses.
9 Lab and Imagining WBC 7.76 K 6.2 BUN 71 Cr 5.7 BNP 4357 CXR: interstitial prominence, left lower lobe airspace opacity consistent with atelectasis or consolidation. Left pleural effusion.
10 What do you think is going on? Hold your thoughts for now..
11 Definitions and mechanisms Aspiration is the misdirection of oropharyngeal or gastric contents into the larynx and lower respiratory tract Aspiration Pneumonitis is a chemical injury by inhalation of gastric contents. Aspiration pneumonia is an infection caused by inhalation of bacteria colonized oropharyngeal contents
12 Epidemiology Adults age 65 years and older account for >50 percent of all pneumonia Incidence of pneumonia increases with aging and frailty Hospitalisations per year for pneumonia 1.1 /1000 young adults 12 /1000 old adults 32 /1000 nursing home residents
13 Epidemiology: cont.. Rate of bacteremia: 1/1000 between age /1000 at age > 75 Rate of nosocomial pneumonia: <2/1000 between /1000 at age > 70 *Kaplan et al. Arch Intern Med 163:317, 2003, ** Johnstone et al. Medicine 87: 329, 2008
14 Bacteriology: anaerobic bacteria is less common than previously thought. Hard to distinct. Aspiration pneumonia represents a distinct entity from typical pneumonia? Pneumonia occurs from micro aspiration of oropharyngeal contents. Similar microbiology and clinical course as aspiration pneumonia
15 Bacteriology: cont... CAP Young adult S. pneumoniae; Mycoplasma; Chlamydia Older adult S. pneumoniae; H. influenza; Chlamydia; S. aureus; Gram-negative rods
16 Bacteriology: cont... NH S. pneumoniae Gram-negative rods S. Aureus Aspiration Pneumonia Same as NH with anaerobes it was isolated from patients with longstanding processes such as lung abscess; and it is unclear what role they play in early infection
17 Work up:

18 Indications for extensive workup
19 Diagnosis: new hypoxemia pulmonary infiltrates on imaging, particularly in gravitydependent lung regions on chest imaging posterior-segments of the upper lobes, basilar segments of the lower lobes fever leukocytosis tachypnea
20 Limitations: Diagnosis is made in <50% of cases Insufficient sample. Gram-negative pathogens and Staph aureus are common. Strep pneumoniae remains the most common pathogen.
21 Risk factors aspiration pneumonia in older people altered mental status Dysphagia in residents of long-term care facilities Difficulty swallowing food (OR 2.0) and medication (OR 8.3) Swallowing dysfunction, e.g. in patients with COPD or after stroke. prolonged supine position Gastroparesis and high residual gastric volumes Aspirations: 71% of patients with CAP compared to 10% in controls
22 Healthy aging and the swallow Older people swallow more slowly Laryngeal closure is delayed Upper oesophageal sphincter opening delayed Oral bolus transport time prolonged Safety of oropharyngeal swallowing is not compromised There is no increase in aspiration comparing to younger adults in radiographic studies
23 Dysphagia 50% of acute stroke patients have clinical dysphagia Most (80%) resolve in the first 7-10 days Associated with big strokes and aphasia Dementia Parkinson disease Multiple sclerosis Mann et al, Stroke 1999; 30:744
24 Poor oral health + oropharyngeal bacterial colonization Can t do oral hygiene! Reduced consciousness level Impaired hand / arm function Can t ask for oral hygiene! Communication barriers Dysphasia Delirium Dementia Increased oral vulnerability Dysphagia Nil by mouth (NPO) Drugs (PPI and antih2) Nutritional status
25 Back to our patients Did they meet the criteria for diagnosis of aspiration pneumonia? What are their risk factors
26 First case was treated with Unasyn (Ampicillin / Sulbactam) Second case treated with ceftriaxone
27 When to treat? Prophylactic antibiotics are not recommended Antibiotics are discouraged shortly after aspiration even with fever, leukocytosis or pulmonary infiltrate. Recommend antibiotics in: 1. Aspiration in high risk patients with colonized gastric contents 2. Aspiration pneumonitis that fails to resolve within 48 hrs 3. Unstable patient with witnessed aspiration
28 Treatment: For nursing home residents, patients with antibiotics use in the last 3 months or patients with comorbidities: Fluoroquinolone (respiratory) alone : moxifloxacin, levofloxacin, or Gemifloxacin or Macrolides (Azithromycin, clarithromycin, or erythromycin) plus β-lactams (amoxicillin (high dose) or amoxicillinclavulanate acid) Alternative β-lactams: ceftriaxone, cefpodoxime or cefuroxime. Alternative to a Macrolide: doxycycline. Amoxicillin-clavulanate acid if need anaerobic bacterial coverage.
29 Treatment: cont.. Nursing-home or Hospital-acquired Pneumonia Requiring Parenteral Treatment: Antipseudomonal cephalosporin (cefepime or ceftazidime) or Antipseudomonal carbapenem (imipenem or meropenem) or ß-lactam/ßlactamase inhibitor (piperacillin-tazobactam) plus Antipseudomonal fluoroquinolone (ciprofloxacin or levofloxacin) or Aminoglycoside (amikacin, gentamicin, or tobramycin) plus MRSA Linezolid or vancomycin Ampicillin-sulbactam if need anaerobic bacterial coverage.
30 Duration of Treatment: A minimum of 5 days plus no fever for 48 h and should have no CAP associated sign of clinical instability: HR >100 bpm Respiratory rate 225/min SBP 00 mmhg 02 saturation <90% or Pa02 mmhg Ability to maintain oral intake abnormal mental status
31 Maintain therapy: Switch from parenteral to oral antibiotics when patient is hemodynamically stable, shows clinical improvement, is afebrile for 16 h, and can tolerate oral medications; Average duration of 7 14 d depending on clinical response. Long-term care facility usually d
32 Recommendations: Start early (<4hrs) in critically ill. Target the causative organism. If no infiltrates develop 48 to 72 hours after an aspiration, it is appropriate to stop antibiotics.
33 Management strategies to reduce the risk of aspiration pneumonia Assistance with regular oral hygiene Screening / investigation for dysphagia High risk subgroups e.g. stroke, dementia, pneumonia, witnessed aspiration Nil-by-mouth during high risk periods Postural interventions. Hand-feeding Small amounts frequently Modified diet / thickened fluids / food supplements

34 Swallowing assessment after a stroke: Routine assessment Look in the mouth! No impaired consciousness Water swallow test Bedside swallow assessment Selected patients Nasoscope Modified Barium swallow (video-fluoroscopy)
35 Conclusions Aspiration is the main cause of pneumonia in later life The risk increased with; dysphagia with oropharyngeal bacterial colonisation Frailty, cognitive impairment and multi-morbidity AP has non-specific presentation Potential for prevention of AP multi-modal / multi-disciplinary strategies
36 Thank you
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
WORKSHOP. The Multiple Facets of CAP. Community acquired pneumonia (CAP) continues. Jennifer s Situation
 continues. Jennifer s Situation") Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center
 Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Fraser Health pandemic preparedness
 Fraser Health pandemic preparedness DRAFT Last revised: April 2006 General Management of Patients in Acute Care Facilities During an Influenza Pandemic 1. OVERVIEW GENERAL MANAGEMENT OF PATIENTS IN ACUTE
Fraser Health pandemic preparedness DRAFT Last revised: April 2006 General Management of Patients in Acute Care Facilities During an Influenza Pandemic 1. OVERVIEW GENERAL MANAGEMENT OF PATIENTS IN ACUTE
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
PNEUMONIA. Patient Case: Chief Complaint: I have been short of breath and have been coughing up rust-colored phlegm for the past 3 days.
 PNEUMONIA Relevant Guidelines: 2008 IDSA CAP guidelines: http://www.idsociety.org/guidelines/patient_care/idsa_practice_guidelines/infections_by_org an_system/lower/upper_respiratory/community-acquired_pneumonia_(cap)/
PNEUMONIA Relevant Guidelines: 2008 IDSA CAP guidelines: http://www.idsociety.org/guidelines/patient_care/idsa_practice_guidelines/infections_by_org an_system/lower/upper_respiratory/community-acquired_pneumonia_(cap)/
Community acquired pneumonia
 Community acquired pneumonia definition Symptoms of an acute LRTI New focal signs on chest examination At least one systemic feature New radiographic shadow Defination{Crofton} IT IS A SYNDROME CAUSED
Community acquired pneumonia definition Symptoms of an acute LRTI New focal signs on chest examination At least one systemic feature New radiographic shadow Defination{Crofton} IT IS A SYNDROME CAUSED
How do we define pneumonia?
 Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
POLICY FOR TREATMENT OF LOWER RESPIRATORY TRACT INFECTIONS
 POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Objectives. Pneumonia. Pneumonia. Epidemiology. Prevalence 1/7/2012. Community-Acquired Pneumonia in infants and children
 Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Turkish Thoracic Society
 Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
Community-Acquired Pneumonia. Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital. Nothing to disclose.
 Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Pneumonia: The Forgotten Killer
 Pneumonia: The Forgotten Killer David Glenn Weismiller, MD, ScM, FAAFP Department of Family and Community Medicine University of Nevada, Las Vegas School of Medicine Disclosure Statement It is the policy
Pneumonia: The Forgotten Killer David Glenn Weismiller, MD, ScM, FAAFP Department of Family and Community Medicine University of Nevada, Las Vegas School of Medicine Disclosure Statement It is the policy
CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: The target audience for this Care Guideline is all MultiCare providers and staff, including those associated with our clinically integrated
Care Guideline CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: The target audience for this Care Guideline is all MultiCare providers and staff, including those associated with our clinically integrated
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Community-acquired pneumonia in adults
 Prim Care Clin Office Pract 30 (2003) 155 171 Community-acquired pneumonia in adults Julio A. Ramirez, MD a,b, * a Department of Medicine, University of Louisville School of Medicine, 512 S. Hancock Street,
Prim Care Clin Office Pract 30 (2003) 155 171 Community-acquired pneumonia in adults Julio A. Ramirez, MD a,b, * a Department of Medicine, University of Louisville School of Medicine, 512 S. Hancock Street,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA
 KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA. I. Background 6 th most common cause of death in U.S. Most common cause of infection related mortality
 Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Community-Acquired Pneumonia OBSOLETE 2
 Community-Acquired Pneumonia OBSOLETE 2 Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with respect to appropriate
Community-Acquired Pneumonia OBSOLETE 2 Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with respect to appropriate
The IDSA/ATS consensus guidelines on the management of CAP in adults
 The IDSA/ATS consensus guidelines on the management of CAP in adults F. Piffer F. Tardini R. Cosentini U.O. Medicina d'urgenza, Gruppo NIV, Fondazione Ospedale Maggiore Policlinico, Mangiagalli e Regina
The IDSA/ATS consensus guidelines on the management of CAP in adults F. Piffer F. Tardini R. Cosentini U.O. Medicina d'urgenza, Gruppo NIV, Fondazione Ospedale Maggiore Policlinico, Mangiagalli e Regina
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Disclosures. Learning Objectives 4/21/2015. Incorporating Nutrition-Focused Physician Assessment into Malnutrition Diagnosis. None
 Incorporating Nutrition-Focused Physician Assessment into Malnutrition Diagnosis Robert DeChicco MS, RD, LD, CNSC Manager, Nutrition Support Team Center for Human Nutrition Cleveland Clinic Health System,
Incorporating Nutrition-Focused Physician Assessment into Malnutrition Diagnosis Robert DeChicco MS, RD, LD, CNSC Manager, Nutrition Support Team Center for Human Nutrition Cleveland Clinic Health System,
Acute Cholangitis. Kelsey Knotts PharmD Candidate Class of 2016
 Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
2019 PHP PRIMARY CARE INCENTIVE
 Primary Care Physicians (PCP) of Physicians Health Network (PHN) may be eligible for an incentive payment in accordance with this PHP PCP Incentive (hereinafter referred to as the PCP Incentive ). As described
Primary Care Physicians (PCP) of Physicians Health Network (PHN) may be eligible for an incentive payment in accordance with this PHP PCP Incentive (hereinafter referred to as the PCP Incentive ). As described
Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC NPSS Asheville, NC
 Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC 2017 NPSS Asheville, NC Objectives Understand the importance of documenting to the highest specificity Understand
Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC 2017 NPSS Asheville, NC Objectives Understand the importance of documenting to the highest specificity Understand
Catherine Casey S. Jones,
 Community Acquired Pneumonia Catherine Casey S. Jones, PhD, RN, ANP-C, AE-C Catherine Casey S. Jones, PhD, RN, ANP-C, AE-C Texas Pulmonary & Critical Care Consultants, PA & Adjunct Professor at Texas Woman
Community Acquired Pneumonia Catherine Casey S. Jones, PhD, RN, ANP-C, AE-C Catherine Casey S. Jones, PhD, RN, ANP-C, AE-C Texas Pulmonary & Critical Care Consultants, PA & Adjunct Professor at Texas Woman
Antibiotics, Expectorants, and Cough Suppressants. Center For Cardiac Fitness Pulmonary Rehab The Miriam Hospital
 Antibiotics, Expectorants, and Cough Suppressants Center For Cardiac Fitness Pulmonary Rehab The Miriam Hospital Objectives Review the mechanism of action (MOA), dosing, benefits, and various options for:
Antibiotics, Expectorants, and Cough Suppressants Center For Cardiac Fitness Pulmonary Rehab The Miriam Hospital Objectives Review the mechanism of action (MOA), dosing, benefits, and various options for:
Online Supplement for:
 Online Supplement for: INFLUENCE OF COMBINED INTRAVENOUS AND TOPICAL ANTIBIOTIC PROPHYLAXIS ON THE INCIDENCE OF INFECTIONS, ORGAN DYSFUNCTIONS, AND MORTALITY IN CRITICALLY ILL SURGICAL PATIENTS A PROSPECTIVE,
Online Supplement for: INFLUENCE OF COMBINED INTRAVENOUS AND TOPICAL ANTIBIOTIC PROPHYLAXIS ON THE INCIDENCE OF INFECTIONS, ORGAN DYSFUNCTIONS, AND MORTALITY IN CRITICALLY ILL SURGICAL PATIENTS A PROSPECTIVE,
Things your mother never told you about antibiotics, UTI s, and Pneumonia. Rob Kaplan, MD July 12 and 14, 2017
 Things your mother never told you about antibiotics, UTI s, and Pneumonia Rob Kaplan, MD July 12 and 14, 2017 Objectives After this talk participants will: Be able to articulate some of the principles
Things your mother never told you about antibiotics, UTI s, and Pneumonia Rob Kaplan, MD July 12 and 14, 2017 Objectives After this talk participants will: Be able to articulate some of the principles
Treating A Sore Throat With Intubation. A case of Epiglottitis in an elderly patient. Sherif Yani, PGY3 St Joseph s FM Residency
 Treating A Sore Throat With Intubation A case of Epiglottitis in an elderly patient. Sherif Yani, PGY3 St Joseph s FM Residency Outline H&P Diagnosis Management Discussion Take-Home Points History 88 y/o
Treating A Sore Throat With Intubation A case of Epiglottitis in an elderly patient. Sherif Yani, PGY3 St Joseph s FM Residency Outline H&P Diagnosis Management Discussion Take-Home Points History 88 y/o
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program
 Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
& Guidelines. For The Management Of. Pneumonia
 Guidelines For The Management Of Pneumonia By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council For Medical
Guidelines For The Management Of Pneumonia By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council For Medical
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Community Acquired Pneumonia-Adults Clinical Practice Guideline MedStar Health
 Community Acquired Pneumonia-Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care of their patients.
Community Acquired Pneumonia-Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care of their patients.
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine
 Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Bacterial Pneumonia Acquired in Nursing Homes
 REVIEW Bacterial Pneumonia Acquired in Nursing Homes Keith M. Norman, BA, and Thomas T. Yoshikawa, MD Pneumonia is the leading cause of infections in nursing home residents who require transfer to an acute
REVIEW Bacterial Pneumonia Acquired in Nursing Homes Keith M. Norman, BA, and Thomas T. Yoshikawa, MD Pneumonia is the leading cause of infections in nursing home residents who require transfer to an acute
Respiratory Tract Infec1ons Long Term Care. Dr Karsten Hammond Infec1ous Diseases 28 March 2015
 Respiratory Tract Infec1ons Long Term Care Dr Karsten Hammond Infec1ous Diseases 28 March 2015 Disclosures I have no financial rela1onships to disclose 82 yo Female In LTC for two years, total care from
Respiratory Tract Infec1ons Long Term Care Dr Karsten Hammond Infec1ous Diseases 28 March 2015 Disclosures I have no financial rela1onships to disclose 82 yo Female In LTC for two years, total care from
This is a common disease - thankfully most cases can be managed as an outpatient
 Chapter 76 Pneumonia Episode Overview: 1. What are the typical associative pathogens? 2. Describe the typical clinical presentation/rfs/management for each of the following: a. S. pneumonia b. H. influenzae
Chapter 76 Pneumonia Episode Overview: 1. What are the typical associative pathogens? 2. Describe the typical clinical presentation/rfs/management for each of the following: a. S. pneumonia b. H. influenzae
Urinary Tract Infections: From Simple to Complex. Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014
 Urinary Tract Infections: From Simple to Complex Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014 Learning Objectives Develop empiric antimicrobial treatment
Urinary Tract Infections: From Simple to Complex Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014 Learning Objectives Develop empiric antimicrobial treatment
Case Report Pulmonary Nocardiosis in the Immunocompetent Host: Case Series
 Hindawi Publishing Corporation Case Reports in Pulmonology Volume 2015, Article ID 314831, 6 pages http://dx.doi.org/10.1155/2015/314831 Case Report Pulmonary Nocardiosis in the Immunocompetent Host: Case
Hindawi Publishing Corporation Case Reports in Pulmonology Volume 2015, Article ID 314831, 6 pages http://dx.doi.org/10.1155/2015/314831 Case Report Pulmonary Nocardiosis in the Immunocompetent Host: Case
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
CLAIRE NOWLAN & SAM SEARLE. Pneumonia in the nursing home
 CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
Critical Care Nursing Theory. Pneumonia. - Pneumonia is an acute infection of the pulmonary parenchyma
 - is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
- is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
Drug Typical Dose CrCl (ml/min) Dose adjustment for renal insufficiency Acyclovir PO (HSV) 400 mg TID >10 <10 or HD PD
 Dose adjustment for renal insufficiency Acyclovir PO (HSV) 400 mg TID >10 <10 or HD PD") Antimicrobial Dosing in Renal Insufficiency (Adults) ASP Handbook * In patients on hemodialysis (), give antimicrobial immediately after dialysis on dialysis days. = Intermittent hemodialysis = Peritoneal
Antimicrobial Dosing in Renal Insufficiency (Adults) ASP Handbook * In patients on hemodialysis (), give antimicrobial immediately after dialysis on dialysis days. = Intermittent hemodialysis = Peritoneal
Nosocomial Pneumonia. <5 Days: Non-Multidrug-Resistant Bacteria
 Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
PNEUMONIA. Dr. A.Torossian, M.D., Ph. D. Department of Respiratory Diseases
 PNEUMONIA Dr. A.Torossian, M.D., Ph. D. Department of Respiratory Diseases Definition Pneumonia is an infection of the lungs caused by bacteria, viruses, fungi and other microorganisms. Classifications
PNEUMONIA Dr. A.Torossian, M.D., Ph. D. Department of Respiratory Diseases Definition Pneumonia is an infection of the lungs caused by bacteria, viruses, fungi and other microorganisms. Classifications
Pediatric Infections: Treatment of Resistant Pathogens. Focus : MRSA and DRSP Infections, Including Pneumonia. Blaise L. Congeni M.D.
 Pediatric Infections: Treatment of Resistant Pathogens Focus : MRSA and DRSP Infections, Including Pneumonia Blaise L. Congeni M.D. Patient 1-LP 8 yo with 8 days of fever and 6 days of cough. She had consistently
Pediatric Infections: Treatment of Resistant Pathogens Focus : MRSA and DRSP Infections, Including Pneumonia Blaise L. Congeni M.D. Patient 1-LP 8 yo with 8 days of fever and 6 days of cough. She had consistently
Prefe f rred d t e t rm: : rhi h no n s o inu n s u iti t s
 HELP It s my sinuses! An overview of pharmacologic treatment of sinusitis Objectives Identify types of sinusitis and underlying pathology Examine common evidence based pharmacologic treatment for sinusitis
HELP It s my sinuses! An overview of pharmacologic treatment of sinusitis Objectives Identify types of sinusitis and underlying pathology Examine common evidence based pharmacologic treatment for sinusitis
Septic shock. Babak Tamizi Far M.D Isfahan university of medical sciences
 Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
Management of Common Respiratory Disorders in Children. Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children. Disclosures. Roadmap 6/10/2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Development of C sporins. Beta-lactam antibiotics - Cephalosporins. Second generation C sporins. Targets - PBP s
 Beta-lactam antibiotics - Cephalosporins Development of C sporins Targets - PBP s Activity - Cidal - growing organisms (like the penicillins) Principles of action - Affinity for PBP s Permeability properties
Beta-lactam antibiotics - Cephalosporins Development of C sporins Targets - PBP s Activity - Cidal - growing organisms (like the penicillins) Principles of action - Affinity for PBP s Permeability properties
Urinary Tract Infections in Hospitalized Patients
 Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES
 MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
-> Education -> Excellence
 Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Methicillin-Resistant Staphylococcus aureus (MRSA) S urveillance Report 2008 Background Methods
 S urveillance Report 2008 Background Methods") Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
SCRIPT 1 - PHYSICIAN COMMUNICATION Localizing Signs and Symptoms with Warning Signs
 SCRIPT 1 - PHYSICIAN COMMUNICATION Localizing Signs and Symptoms with Warning Signs Wisconsin Healthcare Associated Infections in LTC Coalition PHONE CONTACT NECESSARY Resident: Jimmy Issick Date: 11/7/15
SCRIPT 1 - PHYSICIAN COMMUNICATION Localizing Signs and Symptoms with Warning Signs Wisconsin Healthcare Associated Infections in LTC Coalition PHONE CONTACT NECESSARY Resident: Jimmy Issick Date: 11/7/15
Infection Prevention and Control in Long Term Care Part 2
 Infection Prevention and Control in Long Term Care Part 2 Course ID: 1029 - Credit Hours: 2 Author(s) Bonnie Chustz,RN, BSN WCC Disclosures None Accreditation KLA Education Services LLC is accredited by
Infection Prevention and Control in Long Term Care Part 2 Course ID: 1029 - Credit Hours: 2 Author(s) Bonnie Chustz,RN, BSN WCC Disclosures None Accreditation KLA Education Services LLC is accredited by
Antibiotic Stewardship for Skin and Soft Tissue Infection and Respiratory Tract Infections
 Antibiotic Stewardship for Skin and Soft Tissue Infection and Respiratory Tract Infections Ghinwa Dumyati, MD Professor of Medicine Center for Community Health and Infectious Diseases Division University
Antibiotic Stewardship for Skin and Soft Tissue Infection and Respiratory Tract Infections Ghinwa Dumyati, MD Professor of Medicine Center for Community Health and Infectious Diseases Division University
DELL CHILDREN S MEDICAL CENTER EVIDENCE-BASED OUTCOMES CENTER. Community Acquired Pneumonia
 DELL CHILDREN S MEDICAL CENTER Community Acquired Pneumonia LEGAL DISCLAIMER: The information provided by Dell Children s Medical Center of Texas (DCMCT), including but not limited to Clinical Pathways
DELL CHILDREN S MEDICAL CENTER Community Acquired Pneumonia LEGAL DISCLAIMER: The information provided by Dell Children s Medical Center of Texas (DCMCT), including but not limited to Clinical Pathways
Kohlman Evaluation of Living Skills (KELS) of the Hospitalized Patient. Family Medicine Residency Program at Wesley. Objectives
 of the Hospitalized Patient. Family Medicine Residency Program at Wesley. Objectives") Kohlman Evaluation of Living Skills (KELS) of the Hospitalized Patient Jonathan Baalman, MD Family Medicine Residency Program at Wesley 1 Objectives Identify the use of KELS Explain the elements evaluated
Kohlman Evaluation of Living Skills (KELS) of the Hospitalized Patient Jonathan Baalman, MD Family Medicine Residency Program at Wesley 1 Objectives Identify the use of KELS Explain the elements evaluated
Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]
![Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]](/thumbs/83/87318178.jpg "Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]") Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
Orchestrated Efforts to Optimize Antibiotic Prescriptions in a Medical Department
 Orchestrated Efforts to Optimize Antibiotic Prescriptions in a Medical Department Dr. Eugene Tso Division of Infectious Diseases Department of Medicine & Geriatrics United Christian Hospital 11 May 2010
Orchestrated Efforts to Optimize Antibiotic Prescriptions in a Medical Department Dr. Eugene Tso Division of Infectious Diseases Department of Medicine & Geriatrics United Christian Hospital 11 May 2010
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Bacterial Pneumonia Basics
 Bacterial Pneumonia Basics OVERVIEW Inflammation in the lung as a response to disease-causing bacteria, characterized by accumulation of inflammatory cells and fluid in the lung, conducting airways (bronchi
Bacterial Pneumonia Basics OVERVIEW Inflammation in the lung as a response to disease-causing bacteria, characterized by accumulation of inflammatory cells and fluid in the lung, conducting airways (bronchi
Atypical Presentation. Atypical Presentation Part II
 Atypical Presentation Part II Atypical Presentation in Acutely Ill Older Adults Head to Toe Assessment General Weakness/FTT The Frailty Syndrome/Phenotype Dr. Peter O Connor Geriatrician Feb 2008 Physical
Atypical Presentation Part II Atypical Presentation in Acutely Ill Older Adults Head to Toe Assessment General Weakness/FTT The Frailty Syndrome/Phenotype Dr. Peter O Connor Geriatrician Feb 2008 Physical
Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center
 CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
Shirin Abadi, B.Sc.(Pharm.), ACPR, Pharm.D. Clinical Pharmacy Specialist & Pharmacy Education Coordinator, BC Cancer Agency Clinical Associate
, ACPR, Pharm.D. Clinical Pharmacy Specialist & Pharmacy Education Coordinator, BC Cancer Agency Clinical Associate") Shirin Abadi, B.Sc.(Pharm.), ACPR, Pharm.D. Clinical Pharmacy Specialist & Pharmacy Education Coordinator, BC Cancer Agency Clinical Associate Professor of Pharmacy & Associate Member of Medicine, UBC
Shirin Abadi, B.Sc.(Pharm.), ACPR, Pharm.D. Clinical Pharmacy Specialist & Pharmacy Education Coordinator, BC Cancer Agency Clinical Associate Professor of Pharmacy & Associate Member of Medicine, UBC
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY
 PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
Outpatient Management of Patients With Community Acquired Pneumonia Clinical Practice Guideline September 2013
 Clinical Practice Guideline September 2013 General Principles: Community Acquired Pneumonia (CAP), together with influenza, remains the seventh leading cause of death in the United States. According to
Clinical Practice Guideline September 2013 General Principles: Community Acquired Pneumonia (CAP), together with influenza, remains the seventh leading cause of death in the United States. According to
Respiratory Infections
 Respiratory Infections NISHANT PRASAD, MD THE DR. JAMES J. RAHAL, JR. DIVISION OF INFECTIOUS DISEASES NEWYORK-PRESBYTERIAN QUEENS Disclosures Stockholder: Contrafect Corp., Bristol-Myers Squibb Co Research
Respiratory Infections NISHANT PRASAD, MD THE DR. JAMES J. RAHAL, JR. DIVISION OF INFECTIOUS DISEASES NEWYORK-PRESBYTERIAN QUEENS Disclosures Stockholder: Contrafect Corp., Bristol-Myers Squibb Co Research
Pediatric Respiratory Infections
 Pediatric Respiratory Infections Brenda Kelly PharmD BCPS Residency Program Director Virginia Mason Memorial, Yakima, Washington brendakelly@yvmh.org Disclosure The presenter has no actual or potential
Pediatric Respiratory Infections Brenda Kelly PharmD BCPS Residency Program Director Virginia Mason Memorial, Yakima, Washington brendakelly@yvmh.org Disclosure The presenter has no actual or potential
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
The clinical implication and prognostic predictors of Tigecycline treatment for pneumonia involving multidrug-resistant Acinetobacter baumannii
 Journal of Infection (2011) 63, 351e361 The clinical implication and prognostic predictors of Tigecycline treatment for pneumonia involving multidrug-resistant Acinetobacter baumannii R 陳南丞 VS 余文良醫師 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Journal of Infection (2011) 63, 351e361 The clinical implication and prognostic predictors of Tigecycline treatment for pneumonia involving multidrug-resistant Acinetobacter baumannii R 陳南丞 VS 余文良醫師 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Respiratory Infections in Nursing Homes
 Respiratory Infections in Nursing Homes Philip D. Sloane, MD, MPH Elizabeth and Oscar Goodwin Distinguished Professor of Family Medicine Co Director, Program on Aging, Disability, and Long Term Care, Cecil
Respiratory Infections in Nursing Homes Philip D. Sloane, MD, MPH Elizabeth and Oscar Goodwin Distinguished Professor of Family Medicine Co Director, Program on Aging, Disability, and Long Term Care, Cecil
Outline. The Rule of Thirds. Basic Principles about Nursing Home Residents and Respiratory Disease. Bad Teeth and Lung Disease
 Respiratory Infections in Nursing Homes Philip D. Sloane, MD, MPH Elizabeth and Oscar Goodwin Distinguished Professor of Family Medicine Co Director, Program on Aging, Disability, and Long Term Care, Cecil
Respiratory Infections in Nursing Homes Philip D. Sloane, MD, MPH Elizabeth and Oscar Goodwin Distinguished Professor of Family Medicine Co Director, Program on Aging, Disability, and Long Term Care, Cecil
Writing with purpose. Make IT real and simple. On the Medicine Wards for Medical Students, Interns, and Residents
 Writing with purpose Make IT real and simple On the Medicine Wards 2017-2018 for Medical Students, Interns, and Residents Omar S. Darwish, MS, DO Health Science Assistant Professor Coordinator of the M&M
Writing with purpose Make IT real and simple On the Medicine Wards 2017-2018 for Medical Students, Interns, and Residents Omar S. Darwish, MS, DO Health Science Assistant Professor Coordinator of the M&M
Community Acquired Pneumonia in Adults Clinical Practice Guideline Antibiotic Stewardship
 Community Acquired Pneumonia in Adults Clinical Practice Guideline Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care
Community Acquired Pneumonia in Adults Clinical Practice Guideline Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding the care
МІНІСТЕРСТВО ОХОРОНИ ЗДОРОВ Я УКРАЇНИ ХАРКІВСЬКИЙ НАЦІОНАЛЬНИЙ МЕДИЧНИЙ УНІВЕРСИТЕТ. МЕТОДИЧНІ ВКАЗІВКИ ДЛЯ СТУДЕНТІВ англійською мовою.
 МІНІСТЕРСТВО ОХОРОНИ ЗДОРОВ Я УКРАЇНИ ХАРКІВСЬКИЙ НАЦІОНАЛЬНИЙ МЕДИЧНИЙ УНІВЕРСИТЕТ МЕТОДИЧНІ ВКАЗІВКИ ДЛЯ СТУДЕНТІВ англійською мовою Навчальна дисципліна Основи внутрішньої медицини Модуль 1 Змістовний
МІНІСТЕРСТВО ОХОРОНИ ЗДОРОВ Я УКРАЇНИ ХАРКІВСЬКИЙ НАЦІОНАЛЬНИЙ МЕДИЧНИЙ УНІВЕРСИТЕТ МЕТОДИЧНІ ВКАЗІВКИ ДЛЯ СТУДЕНТІВ англійською мовою Навчальна дисципліна Основи внутрішньої медицини Модуль 1 Змістовний
Management of URTI s in Children
 Management of URTI s in Children Robin J Green PhD Antibiotics - Dilemmas for General Practitioners Antibiotic overuse = Resistance Delay in antibiotic use = Mortality Patient expectation Employer expectation
Management of URTI s in Children Robin J Green PhD Antibiotics - Dilemmas for General Practitioners Antibiotic overuse = Resistance Delay in antibiotic use = Mortality Patient expectation Employer expectation