Study organization. Study principal investigators Tudor G. Jovin, MD Raul Nogueira, MD
|
|
|
- Giles Floyd
- 6 years ago
- Views:
Transcription


1 DAWN STUDY- MAIN RESULTS DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo Tudor G. Jovin, MD Professor of Neurology and Neurosurgery Director, UPMC Stroke Institute Director UPMC Center for Neuroendovascular Therapy University of Pittsburgh Medical Center
2 Disclosures Drs. Jovin and Nogueira s DAWN-related travel expenses were covered by Stryker Neurovascular for the duration of trial Other steering committee members, DSMB members, CEC members, and core lab report consulting fees for their work in this trial.
3 Study organization Study principal investigators Tudor G. Jovin, MD Raul Nogueira, MD Steering committee Blaise Baxter, MD Demetrius Lopes, MD Prof. Alain Bonafe Vitor Pereira, MD Anthony Furlan, MD Marc Ribo, MD Rishi Gupta, MD Jeffrey Saver, MD Prof. Olav Jansen Core lab Neurovascular Research Imaging Core David Liebeskind, MD Data Safety Monitoring Board Wade Smith, MD - chair Daryl Gress, MD Steven Hetts, MD Roger Lewis, MD, PhD Clinical Events Committee (CEC) Timothy Malisch, MD Ansaar Rai, MD Kevin Sheth, MD Independent Statisticians Berry Consultants Scott Berry PhD Todd Graves PhD
4 Study background Current evidence suggests that benefit of thrombectomy rapidly decays over time and may no longer exist beyond 7.3 hours from stroke onset (or TLSW) 1 Indeed, the current AHA and ESO guidelines define a rigid therapeutic window of 6 hours as level 1a evidence 2,3 This treatment paradigm disregards individual variations in compensatory mechanisms for ischemia led by but not restricted to collateral flow. Growing evidence supports a physiologic rather than a purely time based approach where patients with Clinical-Core Mismatch (e.g. significant clinical deficits but still limited infarct size) may benefit from reperfusion regardless of time to treatment. 4 Wake-up strokes, strokes with unclear onset time, and witnessed late presenting strokes (> 6 hours) represent a large proportion of LVOS (~40%) yet no proven treatment options exist for this population. Outcomes = Collaterals Time 1 Saver et al, JAMA Powers et al, Stroke Wahlgren Int J Stroke 2016 et.al, 4 Jovin et.al, Stroke 2011

5 Rocha M, Stroke 2017
6




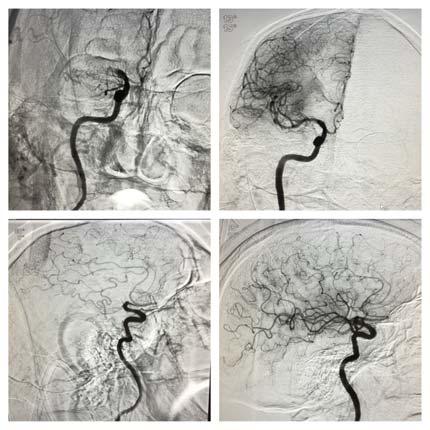
7 Baseline MRI/MRA NIHSS 21 MCA occlusion 4 day MRI/MRA NIHSS 11 MCA partially recanalized


")


8 Baseline MRI/MRA Follow-up MRI/MRA at 24 hours (NIHSS 17) no infarct growth and partial recanalization




9 Baseline MRI/MRA/CTP MRI/MRA at 24 hours, NIHSS 20 MRI at day 5, NIHSS 18
10 Study design Patient population Target vessel Randomization Sites Sample size Study Objective To demonstrate superior functional outcomes at 90 days with Trevo plus medical management compared to medical management alone in appropriately selected patients treated six to 24 hours after last seen well Study Design Global, multi-center, adaptive, population enrichment, prospective, randomized, open, blinded endpoint (PROBE), controlled FDA IDE trial Acute ischemic stroke (AIS) with large vessel occlusion Able to be randomized between six to 24 hours after time last known well Clinical imaging mismatch (CIM) defined by age, core, and NIHSS Intracranial ICA, M1 segment of the MCA 1:1 Trevo + medical management vs. medical management alone Up to 50 sites worldwide (30 US and 20 international) 500 maximum subjects: 250 in the treatment arm and 250 in the control arm. Minimum sample size is 150 subjects. Follow-up 24 hours (-6/+24), day 5-7/discharge, day 30 (± 14), and day 90 (± 14) Jovin et al International Journal of Stroke 2017



 Control")









11 Study Methods: Workflow 6-24h NCCT/DWI: <1/3 MCA Territory CTA/MRA: ICA-T and/or MCA-M1 (Tandem Occlusions Allowed) Control 90-day mrs Informed Consent 1:1 Randomization: -CIM subgroup -ICA-T vs M vs 12-24h - Age 18 - NIHSS 10 - Pre-mRS 0-1 -TLSW to Randomization: 6-24h RAPID CTP/DWI CIM: A. 80 y/o: 1. NIHSS 10 + core <21cc B. <80 y/o: 2. NIHSS 10 + core <31cc 3. NIHSS 20 + core <51cc Thrombectomy -U-W mrs -mrs 0-2 Jovin et al, International Journal of Stroke, 2017
12 Study endpoints Primary endpoint Secondary endpoints Primary safety endpoint Secondary safety endpoint 90-day disability assessed by the modified Rankin scale (mrs) Assessed via Utility-Weighted mrs Nested Dichotomous mrs 0-2 Early response at day 5-7/discharge, defined as a NIHSS drop of 10 points from baseline or NIHSS score 0 or 1 All cause mortality rates Median final infarct size at 24 (-6/+24) hours from randomization Revascularization rates at 24 (-6/+24) hours from randomization Treatment arm: reperfusion rates post device and post procedure by angiography core lab measurement of modified TICI > 2b Stroke related mortality at 90 days Incidence of SICH, by ECASS III definition, within 24 (-6/+24) hours post randomization Incidence of neurological deterioration from baseline NIHSS score through day 5-7/discharge Incidence of procedure-related and device-related serious adverse events through 24 (-6/+24) hours post randomization Jovin et al, International Journal of Stroke, 2017
13 DAWN Trial utility weighted mrs and enrichment Utility weighted mrs Better captures health state transitions across the entire spectrum Patient-centered outcomes analysis mrs Weight Enrichment Designed to fine tune the patient population based on core infarct size Identify subgroups experiencing clinical benefit 0-50 cc 0-45 cc 0-40 cc 0-35 cc 0-30 cc Jovin et al, International Journal of Stroke, 2017
14 Origin of the Utility Weighted mrs Chasnaianunkul et al., Stroke. 2015;46:
15 Key statistical operating characteristics: Bayesian approach First futility/enrichment analysis at 150 subjects First efficacy analysis at 200 subjects Interim analysis after every 50 subjects up to 500 max The threshold for declaring success depends on the degree to which the population has been enriched If there is no enrichment and the probability of a treatment effect is the intervention is deemed efficacious. Similar to a traditional study design one-sided test at the ɑ=0.014 level. Jovin et al, International Journal of Stroke, 2017
16 TRIAL ENROLLMENT RATE AND TERMINATION Site Status Sites Qualified 36 Contracts Executed 31 Sites Initiated 30 Sites Activated to Enroll 30 IRB/EC Approvals 31 Subjects Enrolled 206 Actual / Projected Enrollment * Enrollment stopped at DSMB recommendation Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Subjects Actual Subjects Planned Subjects *Boundary for first enrichment not crossed.



17 Results
18 Randomization and follow-up * 30 day mrs carried forward in 4 pts 100% follow-up to 30 days
19 Demographics Treatment arm N=107 Control arm N=99 P-value Age (years) (median, [IQR]) 72.0 [ ] 73.0 [ ] 0.51 NIHSS, baseline (median, [IQR]) 17 [13-21] 17 [14-21] 0.64 Sex, male (%) 39.3% 51.5% 0.09 Race White/Caucasian 66.0% 63.6% 0.77 Black or African American 21.7% 15.2% 0.28 Other* 12.3% 21.2% 0.09 IV-tPA administered 4.7% 13.1% 0.05 * Inclusive of Asians and International sites that did not disclose race per local authorities
20 Medical history Treatment arm N=107 Control arm N=99 P-value Hypertension 79.0% 75.8% 0.62 Heart failure 18.8% 15.5% 0.58 Coronary artery disease 31.4% 24.0% 0.27 Atrial fibrillation 41.3% 25.0% 0.02 Diabetes mellitus 25.2% 31.6% 0.35 Dyslipidemia 58.8% 59.4% 1.00 Current smoker (within last year) 20.4% 23.5% 0.61 Previous ischemic stroke 12.1% 11.1% 1.00
21 Baseline imaging characteristics Treatment arm N=107 Control arm N=99 P-value Qualifying infarct volume by site RAPID (median, [IQR]) Qualifying RAPID volume obtained by CTP no. (%) Qualifying RAPID volume obtained by DWI MRI no. (%) 7.6 [ ] 8.9 [ ] (62.6) 64 (64.6) 40 (37.4) 35 (35.4) Patients with baseline MRI (%)* 43.0% 37.8% 0.48 Patients with baseline CT/CTA/CTP(%)* 76.6% 76.5% 1.0 * Patients may have both CTP and MRI
22 Baseline occlusion locations core lab adjudicated Intracranial occlusion location no. (%) (Core Lab assessment) Treatment arm N=107 Control arm N=99 Intracranial ICA 22 (20.6) 19 (19.2) M1 middle cerebral artery segment 79 (73.8) 74 (74.7) M2 middle cerebral artery segment 3 (2.8) 3(3.0%) Cervical carotid stenosis no. (%) 0 50% 80 (74.8) 72 (72.7) 51 99% 12 (11.2) 14 (14.1) 100% (occlusion) 15 (14.0) 13 (13.1)
23 Patient presentation Treatment arm N=107 Time since time last seen well to randomization (hrs) Mean ± SD Median (Q1, Q3) Range (min, max) 13.4 ± (10.2, 16.0) (6.1, 23.5) Control arm N= ± (9.4, 15.8) (6.4, 23.9) P- value 0.53 Stroke sub-population Wake up stroke 64.5% 47.5% 0.01 Witnessed stroke 10.3% 14.1% 0.52 Un-witnessed stroke 25.2% 38.4% 0.05
24 Procedural characteristics and outcomes Treatment arm N=107 Procedure duration (minutes) (median IQR) 56.0 [ ] Total number of Trevo device passes (median IQR) 2.0 [ ] Core lab adjudicated TICIs Treatment arm N=107 Post procedure mtici 2B 84.0% Post procedure otici 2B* 72.6% Post procedure TICI % *Protocol advised to stop after otici 2b achieved
25 CEC adjudicated safety outcomes P=0.3 P<0.01 P= % 18.0% 10.5% 13.0% 4.8% 3.2% sich rate Neurological deterioration Stroke related mortality Trevo MM
26 Co-primary endpoints Day 90 weighted mrs Trevo MM Treatment benefit (95% CI) 5.5 ± ± (1.20, 3.12) Bayesian probability of superiority >0.9999* Day 90 mrs (0-2) 48.6% 13.1% 35.5% (23.9%, 47.0%) >0.9999* NNT for 90-day functional independence = 2.8 *Similar to p<0.0001
27 Primary outcome mrs 0/uW mrs 10 mrs 1/uW mrs 9.1 mrs 2/ uw mrs 7.6 mrs 3/ uw mrs 6.5 mrs 4/ uw mrs 3.3 mrs 5-6/ uw mrs 0 TREVO 9% 22% 17% 13% 13% 26% Probability of superiority > CONTROL 4% 5% 4% 16% 34% 36% 73% relative risk reduction of dependency in ADL s NNT for any lower disability 2.0
28 90 Day mrs 0-2 by TLSW to Randomization Trevo MM P-value 6-12h 55.1% 20.0% < h 43.1% 7.4% <0.001 Trevo MM
29 Secondary effectiveness endpoints 100% 80% 24 hour revascularization rates P < % 100% relative improvement 100% 80% All cause mortality 60% 60% P = % 38.4% 40% 20% 20% 18.7% 18.2% 0% Trevo MM 0% Trevo MM
30 Conclusions Thrombectomy with Trevo in DAWN-eligible patients is associated with improvement in clinical outcomes across the entire range of utility weighted mrs and with higher rates of functional independence (mrs 0-2) compared to standard medical therapy (48.6% vs 13.1%, probability of superiority >0.999, NNT = 2.8) For every 100 patients treated with endovascular therapy, 49 will have a less disabled outcome as a result of treatment, including 36 who will be functionally independent The treatment effect size in DAWN is the highest out of any stroke trials to date and suggests that the presence of Clinical-Core Mismatch is a critical predictor of treatment effect independent of time to presentation Treatment effect persisted throughout 24 hours from TLKW; however, earlier treated patients do better Thrombectomy with the Trevo device in patients presenting beyond 6 hours of TLSW had comparable safety profile to thrombectomy performed within 6 hours


31
32 Enrolling Centers North America 1. Abington Memorial, PA 2. Baptist Jacksonville, FL 3. Buffalo, NY 4. Capital Health Trenton, NJ 5. Christiana Delaware, DE 6. CPMC San Francisco, CA 7. Erlanger,Chattanooga, TN 8. Florida Hospital, FL 9. Grady Atlanta, GA 10. JFK, Edison, NJ 11. Kaiser LA 12. Kennestone, Marietta GA 13. KUMC Kansas City, KA 14. Lexington Memorial, KY 15. Riverside, OH 16. Rush, IL 17. St. Joseph Mercy MI 18. Texas Stroke Institute TX 19. Toronto Western, ON 20. UCLA, CA 21. UH Cleveland, OH 22. University of Miami, FL 23. UPMC, PA 24. Valley Baptist, TX Europe 26. Bellvitge Barcelona 27. Germans Trias Barcelona 28. Gui de Chauliac Montpellier 29. Hopital Purpan Toulouse 30. Hospital Clinic Barcelona 31. Vall d'hebron Barcelona Australia 32. Royal Melbourne Hospital UPMC (PI: Jadhav, ATE 10/31/14) SPM Grady (PI: Nogueira/Hassen, ATE 11/25/14) SPM Riverside (PI: Budzik, ATE 08/28/14) SPM Gui de Chauliac Montpellier (PI: Bonafe, ATE Texas Stroke Institute (PI: Bhuva, ATE 04/10/15) - University of Miami (PI: Yavagal, ATE 09/01/16) - Vall d'hebron Barcelona (PI: Ribo, ATE 05/19/16) - Hopital Purpan Toulouse (PI: Cognard, ATE Baptist Jacksonville (PI: Hanel, ATE 01/21/16) UH Cleveland (PI: Sila, ATE 05/04/15) SPM Valley Baptist (PI: Hassan, ATE 03/31/15) SPM Germans Trias I Pujol Badalona (PI: Millán Torné, Buffalo (PI: Levy, ATE 12/01/15) SPM Royal Melbourne (PI: Mitchell, ATE 11/12/15) Rush (PI: Chen, ATE 05/07/15) SPM CPMC (PI: English/Barazangi, ATE 05/05/15) Abington (PI: Shah, ATE 10/29/15) SPM Toronto Western (PI: Silver, ATE 08/26/16) SPM Memorial Regional (PI: Mehta, ATE 02/26/16) Erlanger (PI: Devlin, ATE 06/05/15) SPM Bellvitge (PI: Cardona, ATE 01/31/17) - 1 SPM KUMC (PI: Abraham, ATE 02/01/16) SPM Kaiser LA (PI: Feng, ATE 11/19/15) SPM Florida Hospital (PI: Hellinger, ATE 11/09/15) Capital (PI: Vez, ATE 07/01/14) - 0 SPM JFK (PI: Kirmani, ATE 02/15/17) SPM Hospital Clinic (PI: Urra, ATE 02/22/17) - 0 SPM UCLA (PI: Starkman, ATE 11/21/16) - 0 SPM Kennestone (PI: Gupta, ATE 09/01/16) - 0 SPM Lexington (PI: GIven, ATE 08/29/16) - 0 SPM
33 Real-World Applicability of Endovascular Therapy in ICA and/or MCA-M1 Occlusions Treated in the 6-24-hour Window: Subgroup Analysis of the Prospective Trevo Registry Raul G Nogueira, David Liebeskind, Ron Budzik, Rishi Gupta, Antonin Krajina, Joey English, Ameer Malek, Amrou Sarraj, Ana Paula Narata, Muhammad Taqi, Timothy Miller, Thomas Grobelny, Blaise Baxter, Bruno Mario Bartolini, Laurent Estrade, Tudor Jovin, Erol Veznedaroglu On behalf of the Trevo Retriever Registry Investigators
34 Methods Consecutive Trevo Registry patients fulfilling the basic DAWN trial criteria Baseline NIHSS 10 Intracranial ICA and/or MCA-M1 occlusion Pre-morbid mrs 0-1 Categorized according to their time-from-last-seen-well to arterial puncture as: Early ( 6 hours) vs. Late (6-24 hours) Univariate analyses were performed for group comparisons. Multivariate analysis was performed to identify the predictors of good outcomes (pre-specified)
35 mrs Distribution 57.5% Functional Independence at 90 days mrs 0 mrs 1 mrs 2 mrs 3 6 HOURS TLSW 20.9% 20.3% 16.4% 13.4% 14.2% 3.7% 11.2% mrs 4 mrs 5 mrs 6 P = 0.09 >6 HOURS TLSW 11.1% 22.7% 16.4% 17.4% 15.9% 5.8% 10.6% 50.2 % Functional Independence at 90 days
36 Design 1:1 randomization; standard medical therapy vs. endovascular 45 sites




37


38 HOW MANY SYTROKE PATIENTS QUALIFY??


39 It's a new DAWN! Thank you to all DAWN investigators, patients and families
12/4/2017. Disclosures. Study organization. Stryker Medtronic Penumbra Viz Route 92. Data safety monitoring board Tudor G.
 12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
Intra-arterial Stroke Therapy: 2018 Update
 Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Update. Claire J. Creutzfeldt, MD January 12, 2018
 Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Best medical therapy (includes iv t-pa in eligible patients)
") UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
DAWN Trial: Novel at its Inception and Timely Now
 DAWN Trial: Novel at its Inception and Timely Now SVIN November 7, 2014 9XXXXXXX.AA Page 1 of X DAWN TM Trial Co-PIs Raul Nogueira, MD Associate Professor of Neurology, Neurosurgery and Radiology Emory
DAWN Trial: Novel at its Inception and Timely Now SVIN November 7, 2014 9XXXXXXX.AA Page 1 of X DAWN TM Trial Co-PIs Raul Nogueira, MD Associate Professor of Neurology, Neurosurgery and Radiology Emory
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Ongoing Acute Stroke Studies 10/5/2015
 Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Ongoing Acute Stroke Studies 10/5/2015 Wade S. Smith, MD, PhD Director UCSF Neurovascular Service Daryl R. Gress Professor of Neurocritical Care and Stroke Disclosures NIH U10 NS 086494 (PI) NorCal RCC
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Is there even a time window?
 Is there even a time window? A brief summary of key 2018 trials: DAWN and DEFUSE-3 For Neurosciences Update Conference, February 22, 2018 Maxim D. Hammer, M.D. Executive Summary Based on DAWN and DEFUSE-3,
Is there even a time window? A brief summary of key 2018 trials: DAWN and DEFUSE-3 For Neurosciences Update Conference, February 22, 2018 Maxim D. Hammer, M.D. Executive Summary Based on DAWN and DEFUSE-3,
Primary thrombectomy within 3 hours of onset in acute ischemic stroke from occlusion of middle cerebral artery- a pilot study.
 Primary thrombectomy within 3 hours of onset in acute ischemic stroke from occlusion of middle cerebral artery- a pilot study. Y.Lodi 1,2,3, V.V Reddy 2, A Devasenapathy 2, K.S Shehadeh 3, A Hourani 3
Primary thrombectomy within 3 hours of onset in acute ischemic stroke from occlusion of middle cerebral artery- a pilot study. Y.Lodi 1,2,3, V.V Reddy 2, A Devasenapathy 2, K.S Shehadeh 3, A Hourani 3
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct
 Original Article Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct R.G. Nogueira, A.P. Jadhav, D.C. Haussen, A. Bonafe, R.F. Budzik, P. Bhuva, D.R. Yavagal, M. Ribo, C.
Original Article Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct R.G. Nogueira, A.P. Jadhav, D.C. Haussen, A. Bonafe, R.F. Budzik, P. Bhuva, D.R. Yavagal, M. Ribo, C.
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times
 ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Disclosures. Current Management of Acute Ischemic Stroke. Overview. Focal brain ischemia. Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015
 Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Endovascular Therapy: Beyond the Guidelines
 Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
MR RESCUE: Primary Results
 MR RESCUE: Primary Results (Mechanical Retrieval and REcanalization of Stroke Clots Using Embolectomy) Funded by NIH-NINDS UCLA SPOTRIAS Grant: P50 NS044378 Clinical Trials.gov Number NCT00389467 FDA IDE
MR RESCUE: Primary Results (Mechanical Retrieval and REcanalization of Stroke Clots Using Embolectomy) Funded by NIH-NINDS UCLA SPOTRIAS Grant: P50 NS044378 Clinical Trials.gov Number NCT00389467 FDA IDE
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Endovascular Stroke Therapy
 Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
SWIFT PRIME Update. Washington, DC Oc tober 5, 2015
 Washington, DC Oc tober 5, 2015 SWIFT PRIME Update J. Saver, M. Goyal, A. Bonafé, H. Diener, E. Levy, V. Mendes-Pereira, G. Albers, C. Cognard, D. Cohen, W. Hacke, O. Jansen, T. Jovin, H. Mattle, R. Nogueira,
Washington, DC Oc tober 5, 2015 SWIFT PRIME Update J. Saver, M. Goyal, A. Bonafé, H. Diener, E. Levy, V. Mendes-Pereira, G. Albers, C. Cognard, D. Cohen, W. Hacke, O. Jansen, T. Jovin, H. Mattle, R. Nogueira,
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials
 Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Strokecenter Key lessons of MR CLEAN study
 Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Update on Neurointerventional Therapies: Stroke and Aneurysms
 Update on Neurointerventional Therapies: Stroke and Aneurysms Gary Duckwiler, MD Professor and Director Division of Interventional Neuroradiology David Geffen School of Medicine at UCLA Long Beach Memorial
Update on Neurointerventional Therapies: Stroke and Aneurysms Gary Duckwiler, MD Professor and Director Division of Interventional Neuroradiology David Geffen School of Medicine at UCLA Long Beach Memorial
Updates on Endovascular Therapy
 Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Endovascular stroke research after MRCLEAN. W. van Zwam
 1 Endovascular stroke research after MRCLEAN W. van Zwam 2 Layout 1. What do we know by now 2. Next research questions Anesthesia Aspiration 3. Ongoing and future research Dutch initiatives 3 4 N=70 Intervention
1 Endovascular stroke research after MRCLEAN W. van Zwam 2 Layout 1. What do we know by now 2. Next research questions Anesthesia Aspiration 3. Ongoing and future research Dutch initiatives 3 4 N=70 Intervention
BY MARILYN M. RYMER, MD
 Lytics, Devices, and Advanced Imaging The evolving art and science of acute stroke intervention. BY MARILYN M. RYMER, MD In 1996, when the US Food and Drug Administration (FDA) approved the use of intravenous
Lytics, Devices, and Advanced Imaging The evolving art and science of acute stroke intervention. BY MARILYN M. RYMER, MD In 1996, when the US Food and Drug Administration (FDA) approved the use of intravenous
What is the best imaging protocol for LVO screening when outside of 0-6h window?
 Klinik und Poliklinik für Neuroradiologische Diagnostik und Intervention Zentrum für Radiologie und Endoskopie WLNC, Los Angeles/CA, USA, May 15-17, 2017 What is the best imaging protocol for LVO screening
Klinik und Poliklinik für Neuroradiologische Diagnostik und Intervention Zentrum für Radiologie und Endoskopie WLNC, Los Angeles/CA, USA, May 15-17, 2017 What is the best imaging protocol for LVO screening
Developing the DAISI (Devices for Acute Ischemic Stroke Intervention) Coordinated Registry Network: A NEST Development Project
 Coordinated Registry Network: A NEST Development Project") Travelling through the NETs of the NEST: Toward Collective, Collaborative Intelligence via Continuum of Evidence Generation Developing the DAISI (Devices for Acute Ischemic Stroke Intervention) Coordinated
Travelling through the NETs of the NEST: Toward Collective, Collaborative Intelligence via Continuum of Evidence Generation Developing the DAISI (Devices for Acute Ischemic Stroke Intervention) Coordinated
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention
 Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Trial and Cost Effectiveness Evaluation of Intra arterial Thrombectomy in Acute Ischemic Stroke
 Trial and Cost Effectiveness Evaluation of Intra arterial Thrombectomy in Acute Ischemic Stroke S. Bracard, F. Guillemin, X. Ducrocq for the THRACE investigators Disclosure Personal: No disclosure Study
Trial and Cost Effectiveness Evaluation of Intra arterial Thrombectomy in Acute Ischemic Stroke S. Bracard, F. Guillemin, X. Ducrocq for the THRACE investigators Disclosure Personal: No disclosure Study
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke P A C I F I C N E U R O. O R G
 Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Case Report Successful Mechanical Thrombectomy of a Middle Cerebral Artery Occlusion 14 Hours after Stroke Onset
 Hindawi Case Reports in Neurological Medicine Volume 2017, Article ID 9289218, 4 pages https://doi.org/10.1155/2017/9289218 Case Report Successful Mechanical Thrombectomy of a Middle Cerebral Artery Occlusion
Hindawi Case Reports in Neurological Medicine Volume 2017, Article ID 9289218, 4 pages https://doi.org/10.1155/2017/9289218 Case Report Successful Mechanical Thrombectomy of a Middle Cerebral Artery Occlusion
HERMES Time and Workflow Primary Paper. Statistical Analysis Plan
 HERMES Time and Workflow Primary Paper Statistical Analysis Plan I. Study Aims This is a post-hoc analysis of the pooled HERMES dataset, with the following specific aims: A) To characterize the time period
HERMES Time and Workflow Primary Paper Statistical Analysis Plan I. Study Aims This is a post-hoc analysis of the pooled HERMES dataset, with the following specific aims: A) To characterize the time period
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
WHY TIMELINESS MATTERS. W&M Wren Association Lecture Series
 WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
Endovascular Clot Retrieval. Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital
 Christchurch Hospital") Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Therapy for Acute Ischemic Stroke: Reducing Door-to-puncture Time
 DOI: 10.5797/jnet.oa.2016-0140 Endovascular Therapy for Acute Ischemic Stroke: Reducing Door-to-puncture Time Yoichi Morofuji, 1,2 Nobutaka Horie, 1,2 Yohei Tateishi, 2,3 Minoru Morikawa, 4 Eisaku Sadakata,
DOI: 10.5797/jnet.oa.2016-0140 Endovascular Therapy for Acute Ischemic Stroke: Reducing Door-to-puncture Time Yoichi Morofuji, 1,2 Nobutaka Horie, 1,2 Yohei Tateishi, 2,3 Minoru Morikawa, 4 Eisaku Sadakata,
What Have We Learned: Selection for Endovascular Stroke Therapy
 What Have We Learned: Selection for Endovascular Stroke Therapy Raul G Nogueira, MD Associate Professor in Neurology, Neurosurgery, and Radiology Emory University Director, Neuroendovascular Service Director,
What Have We Learned: Selection for Endovascular Stroke Therapy Raul G Nogueira, MD Associate Professor in Neurology, Neurosurgery, and Radiology Emory University Director, Neuroendovascular Service Director,
Intravenous thrombolysis State of Art. Carlos A. Molina Stroke Unit. Hospital Vall d Hebron Barcelona
 Intravenous thrombolysis State of Art Carlos A. Molina Stroke Unit. Hospital Vall d Hebron Barcelona Independent predictors of good outcome after iv tpa Factor SE OR(95%CI) p Constant 0.467(0.69) Recanalization
Intravenous thrombolysis State of Art Carlos A. Molina Stroke Unit. Hospital Vall d Hebron Barcelona Independent predictors of good outcome after iv tpa Factor SE OR(95%CI) p Constant 0.467(0.69) Recanalization
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Acute Stroke Care: the Nuts and Bolts of it. ECASS I and II ATLANTIS. Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center
 Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Disclosure. Advances in Interventional Neurology. Disclosure. Natural History of Disease 3/15/2018. Vishal B. Jani MD
 Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Computed Tomographic Perfusion to Predict Response to Recanalization in Ischemic Stroke
 Computed Tomographic Perfusion to Predict Response to Recanalization in Ischemic Stroke Maarten G. Lansberg, Stanford University Soren Christensen, Stanford University Stephanie Kemp, Stanford University
Computed Tomographic Perfusion to Predict Response to Recanalization in Ischemic Stroke Maarten G. Lansberg, Stanford University Soren Christensen, Stanford University Stephanie Kemp, Stanford University
BGS Spring Conference 2015
 Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke. Kenneth V Snyder MD PhD SUNY Buffalo, NY
 Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
Interventional Stroke Treatment
 Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Extra- and intracranial tandem occlusions in the anterior circulation - clinical outcome of endovascular treatment in acute major stroke.
 Extra- and intracranial tandem occlusions in the anterior circulation - clinical outcome of endovascular treatment in acute major stroke. Poster No.: C-1669 Congress: ECR 2014 Type: Scientific Exhibit
Extra- and intracranial tandem occlusions in the anterior circulation - clinical outcome of endovascular treatment in acute major stroke. Poster No.: C-1669 Congress: ECR 2014 Type: Scientific Exhibit
ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS
 Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
1/19/2018. Endovascular Therapy for Stroke
 Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Acute Stroke Management What is State of the Art?
 Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Stent Retriever-Mediated Manual Aspiration Thrombectomy for Acute Ischemic Stroke
 Published online: October 7, 2016 Original Paper Stent Retriever-Mediated Manual Aspiration Thrombectomy for Acute Ashutosh P. Jadhav a, b Amin Aghaebrahim a Anat Horev d Dan-Victor Giurgiutiu c Andrew
Published online: October 7, 2016 Original Paper Stent Retriever-Mediated Manual Aspiration Thrombectomy for Acute Ashutosh P. Jadhav a, b Amin Aghaebrahim a Anat Horev d Dan-Victor Giurgiutiu c Andrew
RESEARCH ARTICLE. Computed Tomographic Perfusion to Predict Response to Recanalization in Ischemic Stroke
 RESEARCH ARTICLE Computed Tomographic Perfusion to Predict Response to Recanalization in Ischemic Stroke Maarten G. Lansberg, MD, PhD, 1 Soren Christensen, PhD, 1 Stephanie Kemp, 1 Michael Mlynash, MD,
RESEARCH ARTICLE Computed Tomographic Perfusion to Predict Response to Recanalization in Ischemic Stroke Maarten G. Lansberg, MD, PhD, 1 Soren Christensen, PhD, 1 Stephanie Kemp, 1 Michael Mlynash, MD,
Patient selection for i.v. thrombolysis and thrombectomy
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials
 Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Despite recent cerebrovascular advances, ischemic
 CLINICAL ARTICLE J Neurosurg 126:1123 1130, 2017 Comparison of non stent retriever and stent retriever mechanical thrombectomy devices for the endovascular treatment of acute ischemic stroke Kate A. Hentschel,
CLINICAL ARTICLE J Neurosurg 126:1123 1130, 2017 Comparison of non stent retriever and stent retriever mechanical thrombectomy devices for the endovascular treatment of acute ischemic stroke Kate A. Hentschel,
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes
 Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion
 Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
A DIRECT ASPIRATION FIRST PASS TECHNIQUE (ADAPT) IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 IN PATIENTS WITH ACUTE ISCHEMIC STROKE") A DIRECT ASPIRATION FIRST PASS TECHNIQUE (ADAPT) IN PATIENTS WITH ACUTE ISCHEMIC STROKE Hocine REDJEM Raphaël BLANC Bertrand LAPERGUE Gabriele CICCIO Stanislas SMAJDA Mikael MAZIGHI Georges RODESCH Michel
A DIRECT ASPIRATION FIRST PASS TECHNIQUE (ADAPT) IN PATIENTS WITH ACUTE ISCHEMIC STROKE Hocine REDJEM Raphaël BLANC Bertrand LAPERGUE Gabriele CICCIO Stanislas SMAJDA Mikael MAZIGHI Georges RODESCH Michel
Historical. Medical Policy
 Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
FUTURE DIRECTIONS OF STROKE CARE
 FUTURE DIRECTIONS OF STROKE CARE Jawad F. Kirmani MD Director Stroke & Neurovascular Center New Jersey Neurological Institute Stroke & Neurovascular Center of New Jersey Mohammad Moussavi, MD, Spozhmy
FUTURE DIRECTIONS OF STROKE CARE Jawad F. Kirmani MD Director Stroke & Neurovascular Center New Jersey Neurological Institute Stroke & Neurovascular Center of New Jersey Mohammad Moussavi, MD, Spozhmy
Institutional Priorities and the Impact on Mortality Rates
 Institutional Priorities and the Impact on Mortality Rates John M. McGregor, MD Ciarán Powers, MD, PhD Associate Professor, Clinical Neurosurgery Associate Professor, Neurological Surgery Co-Chair Neurosciences
Institutional Priorities and the Impact on Mortality Rates John M. McGregor, MD Ciarán Powers, MD, PhD Associate Professor, Clinical Neurosurgery Associate Professor, Neurological Surgery Co-Chair Neurosciences
collaterals offset ischemia
 Imaging of Intracranial Stenosis objectives & next steps collaterals offset ischemia systematic evaluation of collaterals hemodynamic impact, not % stenosis develop fractional flow measures collateral
Imaging of Intracranial Stenosis objectives & next steps collaterals offset ischemia systematic evaluation of collaterals hemodynamic impact, not % stenosis develop fractional flow measures collateral
Acute brain vessel thrombectomie: when? Why? How?
 Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Effect of Collateral Blood Flow on Patients Undergoing Endovascular Therapy for Acute Ischemic Stroke
 Effect of Collateral Blood Flow on Patients Undergoing Endovascular Therapy for Acute Ischemic Stroke Michael P. Marks, MD; Maarten G. Lansberg, MD; Michael Mlynash, MD; Jean-Marc Olivot, MD; Matus Straka,
Effect of Collateral Blood Flow on Patients Undergoing Endovascular Therapy for Acute Ischemic Stroke Michael P. Marks, MD; Maarten G. Lansberg, MD; Michael Mlynash, MD; Jean-Marc Olivot, MD; Matus Straka,