Putting the Pieces of the Puzzle Together: A Journey through ABCDEF
|
|
|
- Denis Shaw
- 5 years ago
- Views:
Transcription
1 Putting the Pieces of the Puzzle Together: A Journey through ABCDEF Kristy Colford RN,BSN, CCRN Clinical Nurse Educator Avera McKennan Intensive Care
2 Kristy Colford- Have No Disclosures
3 ZOOM in & ZOOM out A Assess, Prevent, and Manage Pain B Both Spontaneous Awakening Trails and Spontaneous Breathing Trials C Choice of Analgesia and Sedation D Delirium: Assess, Prevent, Manage E Early Mobility and Exercise F Family Engagement and Empowerment Vasilevskis E E Chest 2010;138(5): Davidson J E Am Nurse Today. 2013;8(5):32-38.
4 Objectives Improve outcomes for patients and families by reliable implementing ABCDEF bundle Reduce length of stay in ICU Reduce time on mechanical ventilator Engaging Families to participate in the care and healing of their love ones Enhancing teamwork through implementation of evidence based team building strategies
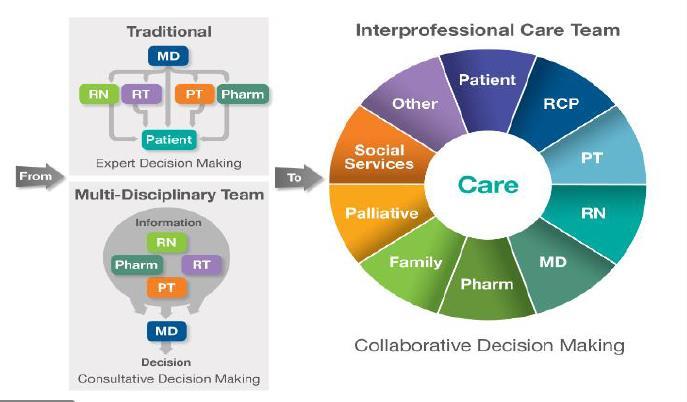
5 Interprofessional Team Definition
6 Interprofessional Teamwork

7
8

9 Improve Patient Comfort, Safety, and Outcomes
10 Pain Care Bundle Assess Assess pain >4x/shift and PRN Significant pain with NRS >3, BPS >5, or CPOT >2 Treat Treat pain within 30 minutes of detecting significant pain & reassess Non-pharmacological treatment Pharmacological treatment Prevent Administer pre-procedural analgesia and/or non-pharmacological interventions Treat pain first, then sedate Barr J Crit Care Med 2013;41(1):
11 Pain: Overview Affects majority of ICU patients Patients with diminished communication or cognitive capabilities at risk Reliable and valid pain assessment is foundation for effective pain treatment Choosing the best intervention to treat pain is challenging
12 Pain Definition Pain is an unpleasant sensory & emotional experience Best reported by person experiencing it Self report is challenging in ICU environment Inability to communicate verbally does not mean individual is not experiencing pain pain.org/education/content.aspx?itemnumber=1698&navitemnumber=576 (IASP in Pain 1979;6: ) (IASP in Pain 1979;6: )

13 Self-Report of Pain- Gold Standard 0-10 Numeric Rating Scales 0-10 visually enlarged horizontal NRS most valid & reliable Chanques G Pain 2010;151:
14
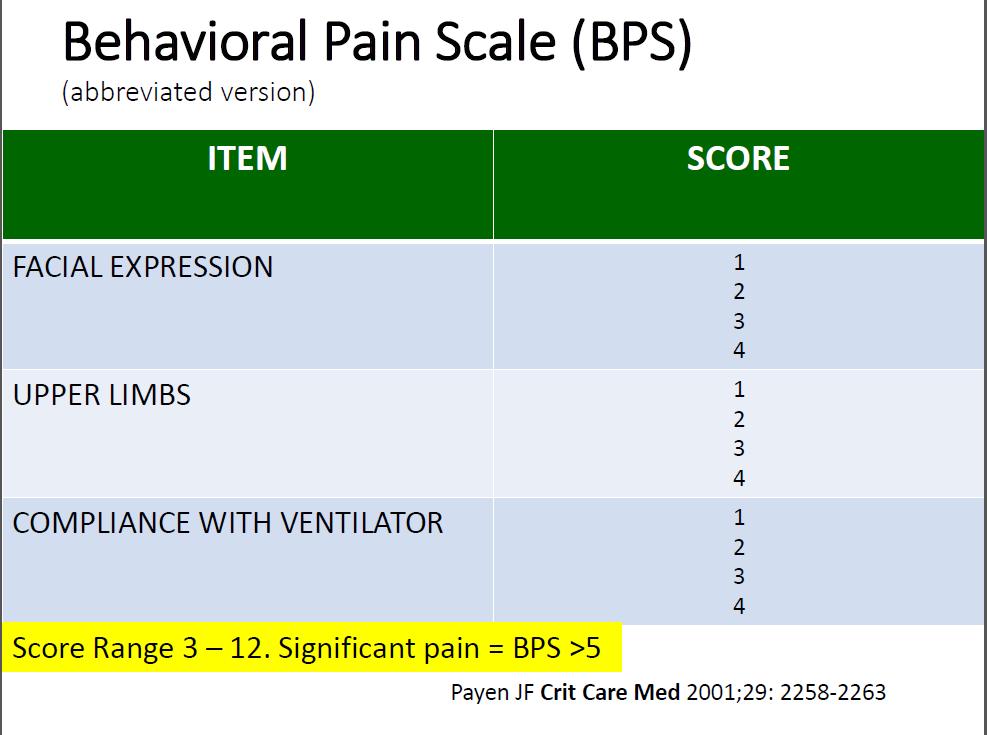
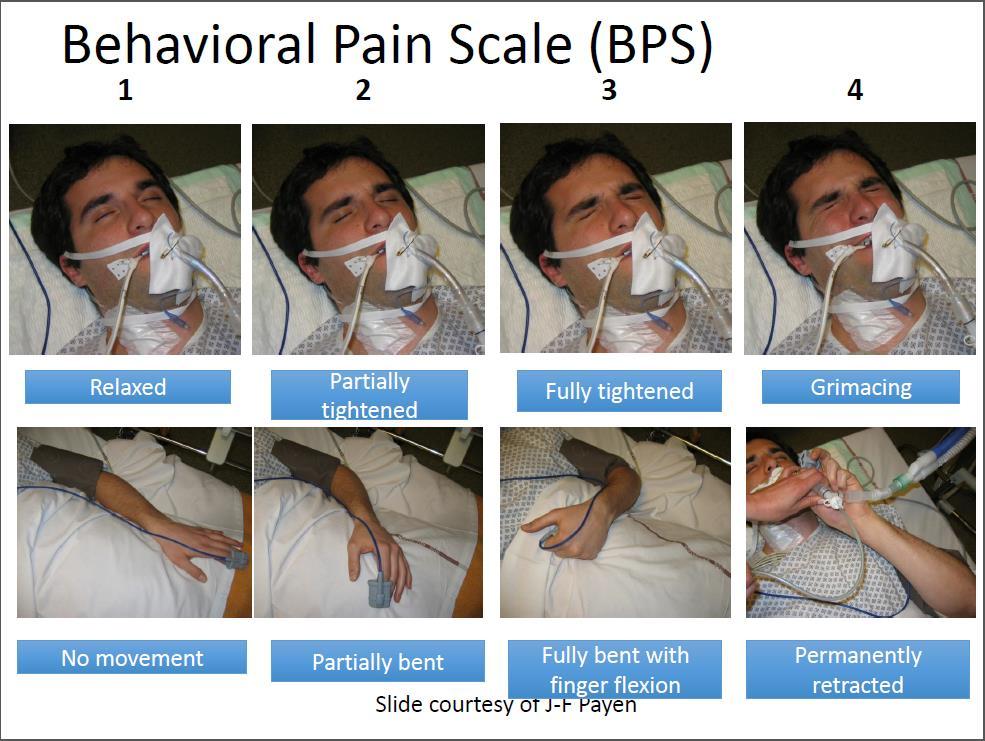
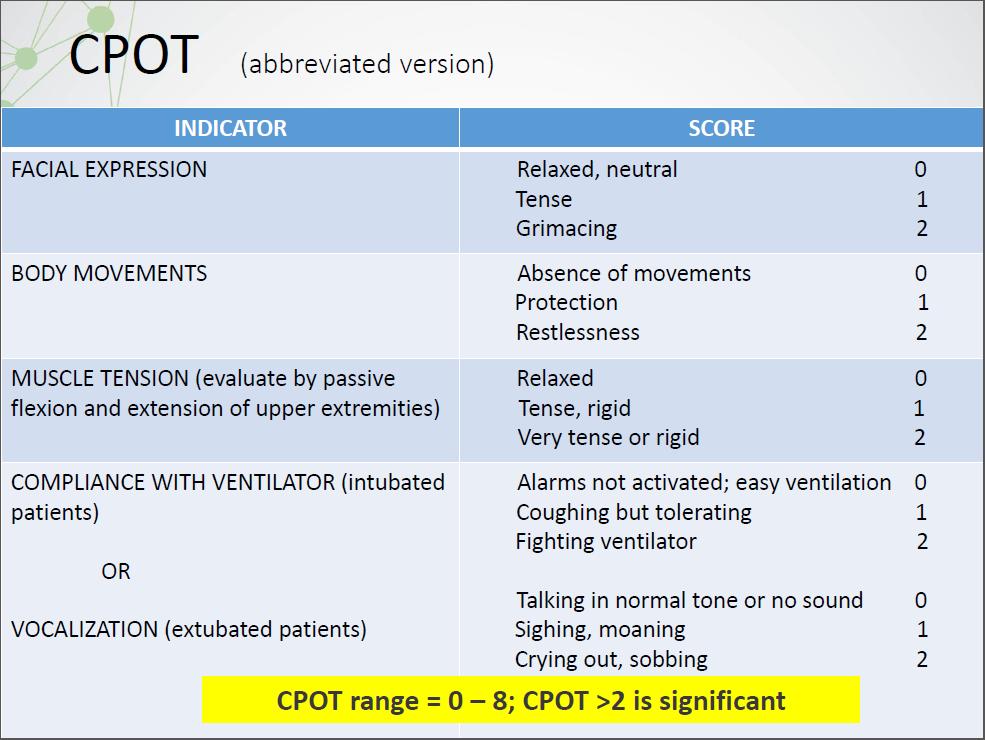
15 Behavioral Pain Scales The Critical Care Pain Observation Tool (CPOT) & the Behavioral Pain Scale (BPS) are the most valid scales for monitoring pain in medical, postoperative, and trauma (except for brain injury) patients unable to self-report in whom motor function is intact & in whom behaviors are observable Barr J Crit Care Med 2013; 41:
 Vital signs may be used as a cue to begin further assessment of pain (+2C).")
16 Can t Rely on Vital Signs for Pain Assessment Vital signs should not be used alone to assess pain (-2C). (are not valid pain indicators) Vital signs may be used as a cue to begin further assessment of pain (+2C). Gelinas C, Clin J Pain 2007; 23: Barr J, Crit Care Med 2013;41(1): Payen JF Crit Care Med 2001;29:
17
18
19
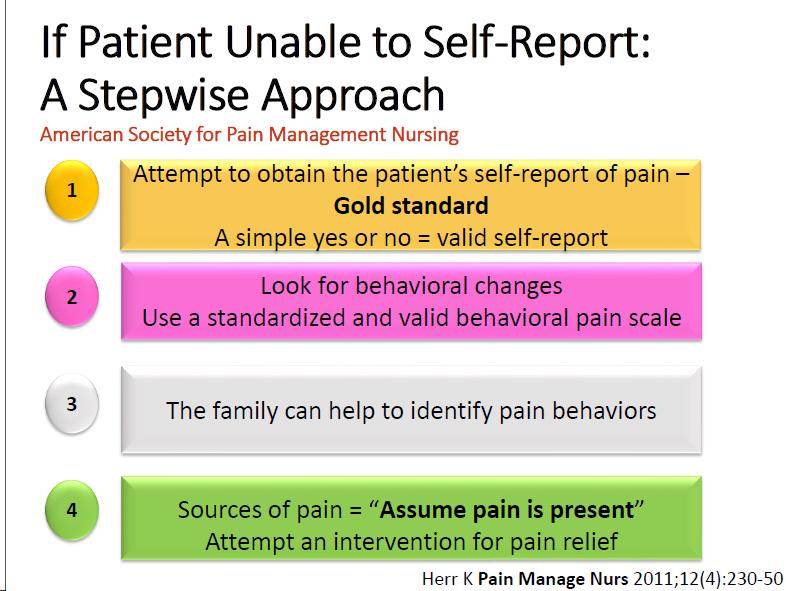
20 The Family can help to identify pain behaviors
21 Proxy Report of Symptoms Symptom Patient-Family Patient-RN Patient-MD Pain Tiredness SOB Restlessness Anxiety Sadness Hunger Fear Thirst Confusion Intraclass correlation coefficients.( Hemphill JF. Am Psychol 2003; 58:78 79) Puntillo K Crit Care Med 2012; 40(10):
22 Assume Pain is Present When patient unable to use self-report or exhibit behaviors can Assume Pain is Present For example, in patients: Receiving NMBAs That are unresponsive but underlying pathology thought to be painful Undergoing activities/procedures know to be painful
23 Goal of ICU Sedation Calm Comfortable Cooperative Reduce anxiety and agitation Facilitate mechanical ventilation Decrease traumatic memory of ICU stay and procedures
24 Negative Consequences of Prolonged, Deep Sedation/Benefits of Light Sedation Deep sedation Reduced six-month survival Hospital mortality Longer duration of mechanical ventilation Longer ICU length of stay Increased physiologic stress in terms of elevated catecholamine concentrations and/or increased oxygen consumption at lighter sedation levels BUT no clear relationship between elevation and clinical outcomes Brook A. Crit Care Med. 1999;27: Girard T. Lancet. 2008;371: Kress J. N Engl J Med. 2000;342: Treggiari M. Crit Care Med. 2009;37:
25 Mental Health After Light or Deep Sedation 137 adults requiring mechanical ventilation-rct Sedation with midazolam Light: Ramsay 1-2, intermittent injection Deep: Ramsay 3-4, continuous infusion Results Primary endpoints (4 weeks after ICU discharge) Trend toward more PTSD symptoms with deep sedation (P=0.07) More trouble remembering the event (P=0.02) More disturbing memories of the ICU (P=0.05) No difference in anxiety or depression scores Other endpoints: light sedation patients averaged 1 day shorter on mechanical ventilation (P = 0.03) 1.5 days shorter length of stay (P = 0.03) Treggiari M. Crit Care Med. 2009;37:

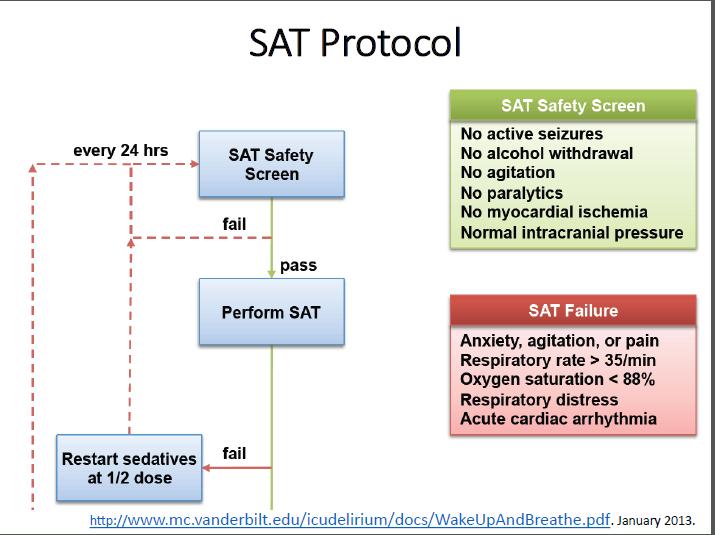
26 Daily Sedation Interruption Decreases Duration of Mechanical Ventilation Hold sedation infusion until patient awake, then restart at 50% of prior dose Awake defined as any 3 of the following: Open eyes in response to voice Use eyes to follow investigator on request Squeeze hand on request Stick out tongue on request Needham D. Crit Care Med. 2012;40:502-9.
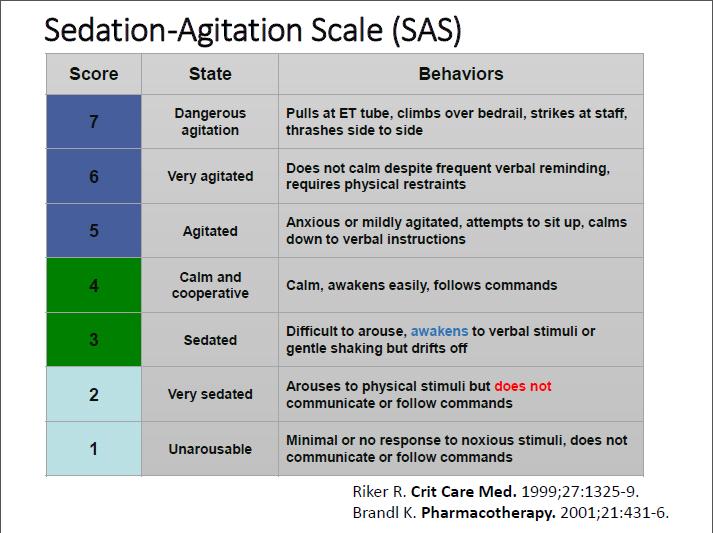
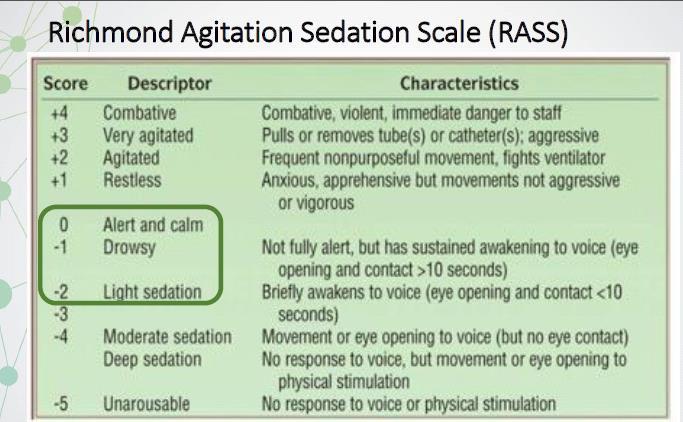
27 PAD Agitation/Sedation Assessment Recommendations Depth and quality of sedation should be routinely assessed in all ICU patients (1B) The RASS & SASS are the most valid and reliable scales for assessing quality and depth of sedation in ICU patients (B) Suggest using objective measures of brain function to adjunctively monitor sedation in patients receiving neuromuscular blocking agents (2B) Use EEG monitoring either to monitor nonconvulsive seizure activity in ICU patients at risk for seizures, or to titrate electrosuppressive medication to achieve burst suppression in ICU patients with elevated intracranial pressure (1A) Barr J. Crit Care Med. 2013;41:
28
29
30 PAD Depth of Sedation Statements Maintaining light levels of sedation in adult ICU patients is associated with improved clinical outcomes, e.g., shorter duration of mechanical ventilation and shorter ICU lengths of stay (LOS) (B). Maintaining light levels of sedation increases the physiologic stress response, but is not associated with an increased incidence of myocardial ischemia (B). The association between depth of sedation and psychological stress in these patients remains unclear (C). Barr. Crit Care Med. 2013;41:
31

32

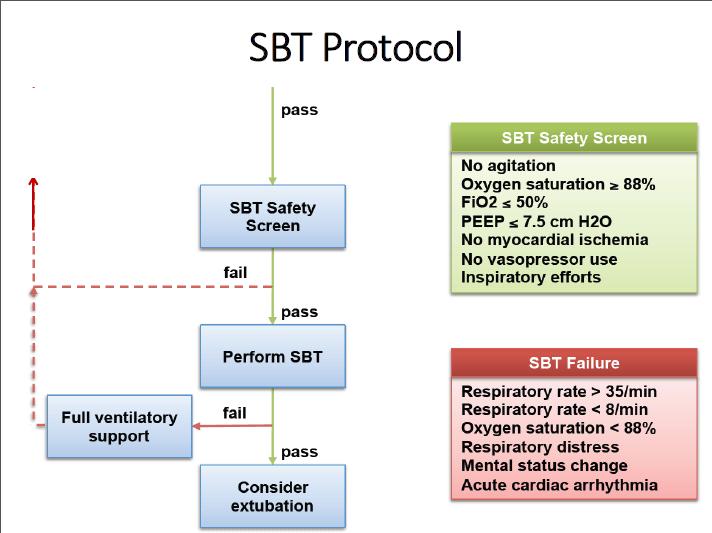
33 Wake Up and Breath Protocol January 2013.
34
35
36 Things to Consider: Barriers Concern by staff Workload and productivity concerns Fear of patient discomfort and asynchrony Fear of inadvertent extubation Fear of self-extubation during decreased sedation Excuses: Let s just give it one more day. It s late in the day, and we don t have coverage tonight. Ostermann M. JAMA. 2000;283: Guttormson J. Intensive Crit Care Nurs. 2010;26: Tanios M. J Crit Care. 2009;24:66-73.
37

38 All ICU patients should be routinely assessed for: Pain (Likert self-report, or BPS/CPOT non-self-report) Agitation/depth of sedation (RASS/SAS) Delirium (CAM-ICU/ICDSC) Important factors influence the choice and dose of analgesia and sedative medications Non-pharmacologic strategies play an important role when managing pain and agitation Barr J. Crit Care Med. 2013;41:
39 Use of opioids: IV opioids should be considered first-line analgesics for the treatment of non-neuropathic pain. (+1C) All IV opioids are equally effective when titrated to similar pain scores. (C) Use of non-opioid analgesics: Non-opioid analgesics should be considered to decrease the amount of opioids administered and to decrease opioid-induced adverse effects. (+2C) Barr J. Crit Care Med. 2013;41:
40 Use of both opioid and non-opioid analgesics: For invasive and potentially painful procedures, analgesics with or without non-pharmacologic therapy may be administered pre-procedurally. (+2C) Recommended prior to chest tube removal. (+1C) For neuropathic pain, enterally administered gabapentin or carbamazepine should be considered, in addition to IV opioids. (+1A) Barr J. Crit Care Med. 2013;41:
 Use daily awakening or a titrated sedation strategy to maintain patient wakefulness.")
41 Avoid deep sedation/coma: Sedative medications should be titrated to maintain lighter levels of sedation, unless clinically contraindicated. (+1B) Use daily awakening or a titrated sedation strategy to maintain patient wakefulness. (1B) Choice of sedative: Non-benzodiazepines may be preferred over benzodiazepines to improve clinical outcomes in mechanically ventilated ICU patients. (+2B) Reduction in sedation requirements: Use of an analgesia-first (i.e., analogsedation) strategy is recommended in mechanically ventilated patients. (+ 2B) Barr J. Crit Care Med. 2013;41:
42
43
44 Analgo-Sedation Strategies Addressing pain and discomfort first before administering sedatives. Utilization of one drug for two purposes: Pain relief and sedation Usually accomplished with an opioid.
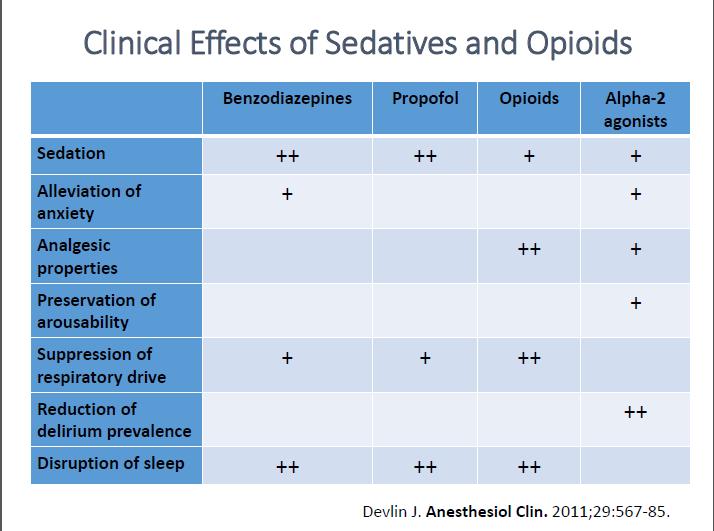
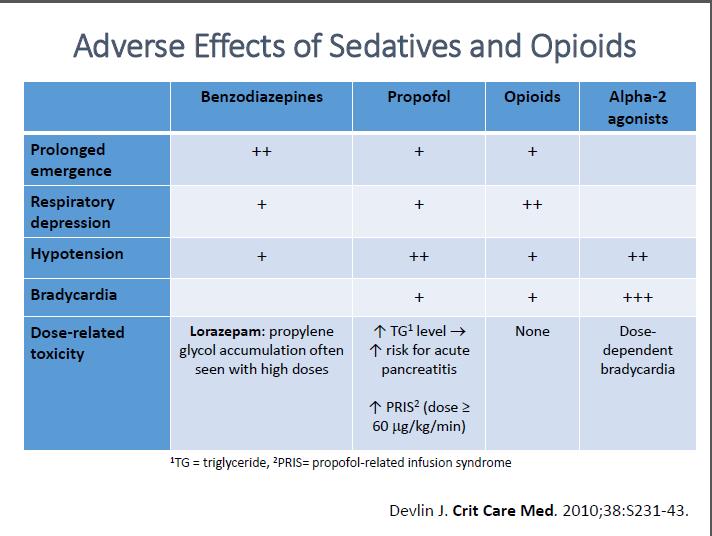
45 Analgo-Sedation Benefits Limitations Reduces pain and discomfort, which are common causes of agitation Avoids potential sedative-related adverse events: Delirium Hemodynamic instability Metabolic acidosis (lorazepam) Immunomodulation Death (PRIS) May interfere with respiratory drive, gastric motility, nutrition Potential for opioid withdrawal ICU LOS, ventilator time, delirium, VAP, mortality, and cost of care are not consistently reduced Rigorously evaluated only in European ICUs Devabhakthuni S. Ann Pharmacother. 2012;46:
46 MENDS Trial: Dexmedetomidine versus Lorazepam Sedation Study Design: Double-blind, randomized, controlled trial of mechanically ventilated medical and surgical ICU patients (N = 106) Results: Dexmedetomidine sedation: more days alive without delirium or coma than with lorazepam (P = 0.01) lower prevalence of coma (P < 0.001) than with lorazepam (P = 0.01) more time spent within sedation goals than with lorazepam (P = 0.04) No differences in 28-day mortality and delirium-free days Incidence of bradycardia and hypotension were similar Pandharipande P. JAMA. 2007;298:
47 SEDCOM Trial: Dexmedetomidine vs Midazolam Sedation Study Design: Double-blind, randomized, multicenter trial comparing longterm (> 24 hr) dexmedetomidine (n = 244) with midazolam (n = 122) Results: No difference between groups in percentage of time patients were in targeted sedation range (P = 0.18) Lower delirium prevalence in the dexmedetomidine group (P 0.001) Shorter sedation duration in the dexmedetomidine group (P = 0.01) Shorter time to extubation in the dexmedetomidine group (P = 0.01) Riker R. JAMA. 2009;301:489-9.
48
49 Associated but Nondiagnostic Symptoms of ICU Delirium Hallucinations, delusions Abnormal psychometric activity (e.g., agitation, lethargy) Emotional disturbances (e.g., fear, anger, depression, apathy) Sleep disturbances
50 Delirium: Epidemiology and Short- Term Outcomes Prevalence 50% to 80% of mechanically ventilated patients 20% to 50% of lower severity patients Associated outcomes Prolonged hospitalization Increased mortality Increased cost Ely E JAMA. 2001;286: Dubois M. Intensive Care Med. 2001;27: Ely E JAMA. 2003;289: Ely E JAMA. 2004;291: Thomason JW. Crit Care. 2005;9:R Milbrandt EB Crit Care Med. 2004; 32:
51 Delirium: Long-Term Outcomes Mortality Each day of delirium in the ICU increases the hazard of 1- year mortality by 10% 1 Cognitive Impairment ICU delirium is an independent risk factor for long-term cognitive impairment 2,3 34% with scores similar to traumatic brain injury 24% with scores similar to Alzheimer disease Pisani MA Am J Respir Crit Care Med. 2009;180: Girard T Crit Care Med.2010;38: Pandharipande PP N Engl J Med. 2013;369(14):
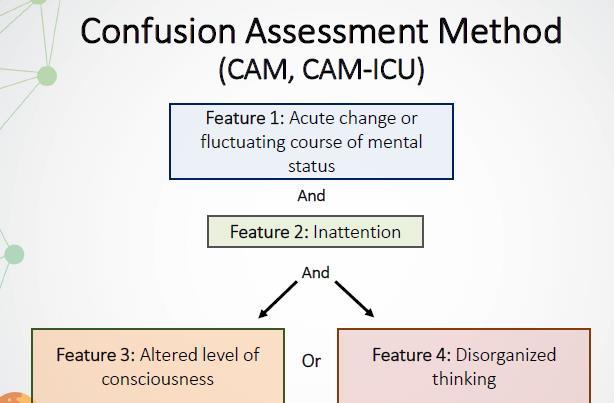
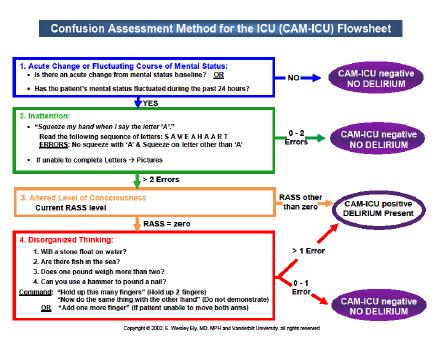
52 PAD Delirium Assessment Recommendations Routinely monitor for delirium in all adult ICU patients (+1B) Use either: Confusion Assessment Method for ICU (CAM-ICU) Intensive Care Delirium Screening Checklist (ICDSC) Barr J Crit Care Med. 2013;41:
53
54
55 Intensive Care Delirium Screening Checklist (ICDSC) 1. Altered level of consciousness 2. Inattention 3. Disorientation 4. Hallucination, delusion, or psychosis 5. Psychomotor agitation or retardation 6. Inappropriate speech or mood 7. Sleep/wake cycle disturbances 8. Symptom fluctuation Figure: Gusmao-Flores D. Crit Care. 2012;16:R115-R125
56 Anticipating Delirium: Risk Factors Baseline Vulnerability Precipitants Underlying brain disease (dementia, stroke, Parkinson) Increased age Institutionalization Chronic disease (HIV, HTN, ETOH dependency, diabetes, etc.) Visual/hearing deficits Medications Infection Dehydration Immobility/restraints Malnutrition Tubes/catheters Electrolyte imbalance Sleep deprivation
57 Interventions for Delirium Early mobility and rehabilitation Sleep enhancement (via nonpharm and hygiene) Reducing unnecessary and deliriogenic medications Structured reorientation Adequate oxygenation American Geriatric Society 2014 Guidelines. J Am Geriat Soc. 2016;63(1): Inouye SK N Engl J Med. 1999;340(9): McNamara L. Am J Crit Care. 2008;17:576.
58 Interventions for Delirium Pain management Constipation relief Nutrition and fluid repletion Sensory assistive devices (vision and hearing) Cognitive stimulation/rehabilitation American Geriatric Society 2014 Guidelines. J Am Geriat Soc. 2016;63(1): Inouye SK N Engl J Med. 1999;340(9): McNamara L. Am J Crit Care. 2008;17:576.
59 Early Exercise Patient s functional performance improved Independent functional status at hospital discharge: intervention 59% vs. control 35% Shorter duration of MV Substantial reduction in duration of delirium 2 vs. 4 days Schweickert WD Lancet. 2009;373:
60 Delirium and Sleep in the ICU Sleep and delirium Sleep disruption is a manifestation of delirium Sleep deprivation yields delirium Sleep deprivation and fragmentation commonly occur Etiologies: Loss of night-day cues, constant environmental stimuli Pain, sedatives, MV, stress ICU sleep hygiene programs Decrease both incidence and duration of delirium in patients Nighttime sedation does not promote sleep Alway AE Am J Crit Care. 2013;22(4): Van Rompaey B Crit Care. 2012;16(3):R73. Kamdar BB Anaesthesia. 2014;69(6): Patel J Anaesthesia. 2014;69(6):
61 ICU Environment, Sleep, and Delirium Daytime Interventions Blinds raised Less than 50% of the day napping Avoid caffeine after 3 PM Nighttime Interventions Before 10 PM Room lights dimmed Room curtain closed Warm bath Unnecessary alarms prevented Room temperature optimized Pain appropriately controlled Television off Result: No difference in perceived sleep quality, but Reductions in delirium/coma incidence (49% vs. 69%) Improved daily noise rating Kamdar BB Crit Care Med. 2014; 41(3):
62 Reorienting ICU Patients Before-after observations in 214 ICU patients Interventions: Night environment, music therapy, visual cues (clock) Reorientation with 5 W s and 1 H Who? Who are you? Who is the nurse/physician? What? What happened? Where? Where are you/we? Why? Why did it happen? How? How did it happen? And what is the illness progression? Result: Delirium incidence reduction Pre 35% vs. post 22% Colombo R Minerva Anestesiol. 2012;78:
63 Helpful Approach to Delirium Management Stop THINK Lastly medicate
64 Reducing Unnecessary STOP: especially consider sedatives Is your patient on the minimal amount necessary? Review medications Medications Doses adjusted for elderly, renal failure, liver failure Do you have a plan to reduce drug exposure? Spontaneous awakening trial Nurse empowerment to titrate drug to a teamdetermined target level of arousal
65 What to THINK if positive for delirium Toxic Situations Congestive heart failure, shock, dehydration Deliriogenic medications (tight titration) New organ failure (liver, kidney, etc.) Hypoxemia Infection/sepsis (nosocomial), Immobilization Nonpharmacological interventions K+ or electrolyte problems

66 Reducing ICU Delirium Treat pain first! Promote consciousness! Prevent delirium Wean MV Increase mobility Increase patient participation Promote patient recovery Reduce complications Improve patient outcomes Collinsworth AW J Intensive Care Med Oct 27
67
68 Did the Patient Achieve his or her Maximal Mobility Activity Today? YES Mobility is everyone s job! RN, PT, OT, etc. Communicate patient s current mobility status to all ICU team members Encourage patients to perform active movements if possible
69 Did Our Patient Achieve his or her Maximal Mobility Activity Today? NO! Why not? Was the patient walking before admission? Is the patient hemodynamically stable? Is the patient awake?
70 Side Effects of Bed Rest Muscle strength in a healthy person can decrease 1.3% to 3% for every day spent on bedrest.1 Effects are more profound in older people and in those with critical illness.2 A new study suggests that 3% to 11% strength loss occurs for every day in bed in an ICU setting.3 Age and days on bedrest are independent predictors of worsening function. Topp R. Am J Crit Care. Clin Issues Yende S. Thorax Fan E. Am JRespir Crit Care Med. 2014;190:
71 Evidence-Based Benefits of Early Progressive Mobility Decrease ICU and hospital LOS Improve overall physical functioning Decrease duration of mechanical ventilation Decrease incidence of delirium Bailey P. Crit Care Med. 2007;35: Morris P. Crit Care Med Aug;36: Schweickert W. Lancet. 2009;373:
72 Early Progressive Mobility in ICU In-bed mobility Passive range-of-motion exercises Turning side to side Sitting on the side of the bed Active strengthening exercises Out-of-bed mobility Standing at bedside Sitting on a regular chair Sitting on a cardiac chair Walking MOBILITY IS EVERYONE S JOB IN THE INTENSIVE CARE UNIT!
73 Considerations Before Mobilizing Patients in ICU Neurologic: Level of alertness Cardiac: Hemodynamic stability Vasoactive medications Pulmonary: Ventilation/oxygenation needs Risk vs. benefit Guidelines vs. Protocols Fewer absolute contraindications Importance of interdisciplinary collaboration
74 Perceived Barriers to Progressive Early Mobility Severity of disease Severity of weakness Premorbid level of function ICU culture that promotes bed rest Nutritional state Sleep deprivation Level of delirium Pain Obesity
75 Absolute Contraindications to Progressive Mobility in ICU Patients on neuromuscular blockade Hemodynamic instability requiring escalating dose or multiple vasopressors Significant oxygenation dysfunction requiring high level of oxygen Unstable fractures Cerebral edema with uncontrolled intracranial pressure Active bleeding Intra-aortic balloon pump on femoral artery Pacer dependent with transvenous temporary pacemaker ECMO with femoral cannulation Femoral arterial sheath Open chest/open abdomen




76

77
78 Characteristics of Patient and Keep ICU patients and families: Informed Family-Centered Care Actively involved in decision-making Actively involved in self management Provide physical comfort /emotional support to patient and families. Maintain clear understanding of patients and families concepts of illness and cultural beliefs. Institute of Medicine. Crossing the Quality Chasm
79 Myths and Misconceptions Family presence interferes with care. Family presence exhausts the patient. Family presence is a burden to families. Family presence spreads infection. Institute for Patient and Family Centered Care

80 Creating the Right Environment Family presence Family and patient engagement Family and patient empowerment

81 Let s Open the Door Today: Resistance is from healthcare workers! Why? Fear of consequences and failure to understand the importance of families. Family presence at the beside is seen as a privilege, not as a necessary component of the patient s care. Burchardi, H. Intensive Care Med. 2002:28; Riccioni L. Trends Anesth and CC. 2014: 4;
82 ICU Flexible Visitation: Patient Decreases: anxiety, confusion, agitation CV complications ICU length of stay Increases: feelings of security patient satisfaction quality and safety Benefits Bell L. AACN practice alert. Nov Davidson J. Crit Care Med. 2007;35:605-22
83 Inviting Families and Patients to Engage in Care Focus on activities that actively involve families in the patient s care. Be sensitive - address questions and concerns. Facilitate communication - cultural/spiritual needs. understanding of Develop strategies for family engagement; provide education and role modeling.
84 How to Engage Family Members Provide brochures-ways that family members can help the patient: Speak softly to patients and use simple words. Re-orient the patient (5 W s + 1H). Talk about family and friends. Bring patient s sensory aides (eyeglasses, hearing aids). Decorate the room with reminders of home. Participate in mobilizing the patient. Document the patient s stay in an ICU diary.
85 ICU Diaries ICU diaries decrease the incidence of PTSD after an ICU stay. Diary contents: Calendar of events and/or milestones. Photographs, both of the patient and the ICU. Entries from staff and/or family. Utilize preprinted templates or websites Great resource:
86 Family Participation on Rounds Who should participate? Decision makers Patients, whenever possible Invite them to join rounds. Provide an opportunity to ask questions, clarify. Ask them, Do you have any additional concerns? Participation fosters: Bi-directional communication Shared decision-making Davidson J. Crit Care Med. 2007;35: Cypress B. Dimens Crit Care Nurs. 2012;31:53-64.

87 Empowering Family Members Family members = patients primary advocates. Provide them the tools and permission to speak up! Create a safe environment to speak openly. Create a culture where it is acceptable for our actions to be questioned. Three key areas: Shared decision-making Safety Future care expectations
88 Melissa and Doug s Story: Recommendations for Others
89 Reference: Puntillo K. Am J Crit Care 2001;10: (Response Procedural Pain) Payen J. Crit Care Med 2001;29: (Behavioral Pain Scale) Gelinas C. Am J Crit Care 2006;15: (CPOT Validation) Payen J. Anesthesiology 2009; 111: (Behavioral Pain Scale)Chanques G. Crit Care Med 2010;151: (Pain Assessment in ICU)Gelinas C. Int J Nursing Stud 2011;48: (Overcoming Barriers to Pain Assessment) Puntillo K. Crit Care Med 2012;40: (Proxy Pain Reports) Puntillo K. Am J Respir Crit Care Med 2014; 89: (New Insights ICU Pain Control) Treggiari M. (Light Sedation) Crit Care Med. 2009;37: Pandharipande P. (Lorazepam Predicts Delirium) Anesthesiology. 2006;104:21-6. Seymour C. (Diurnal Sedation and Liberation) Crit Care Med. 2012;40: Hager D. (Reducing Deep Sedation ALI) Crit Care Med. 2013;41: Shehabi Y. (Goal-Directed Sedation) Crit Care Med. 2013;41: Shehabi Y. (Mortality attributed to Delirium) Intensive Care Med. 2013;39: Tanaka L. (Early Oversedation Outcomes) Crit Care. 2014;18:R156. Burry L. (High Versus Low Sedation Outcomes) Can J Anaesth. 2014;61: Minhas MA. (Protocolized Sedation) Mayo Clin Proc. 2015;90: Balzer F. (Early Deep Sedation decrease 2 year survival) Crit Care. 2015;19:197.
90 Reference Ely E. (SBTs) N Engl J Med. 1996;335: Riker R. (SAS) Crit Care Med. 1999; 27: Kress J. (SATs) N Engl J Med. 2000;342: Sessler C. (RASS) Am J Respir Crit Care Med. 2002, 166: Ely E. (RASS) JAMA. 2003;289: Girard T. (ABC Study) Lancet. 2008;371: Strøm T. (No Sedation) Lancet. 2010;375: Shehabi Y. (Deep Sedation) Am J Respir Crit Care Med. 2012;186: Balas M. (ABCDE) Crit Care Med. 2013;42: Bassett R. (IHI ABCDE Collaborative) Jt Comm J Qual Patient Saf. 2015;41: Klompas M. (CDC ABCDE Collaborative) Am J Respir Crit Care Med. 2015;191: Carson S. (Loraz. vs. Propofol DSI) Crit Care Med. 2006;34: Pandharipande P. (Loraz.-delir. risk factor) Anesthesiology. 2006;104:21-6. Pandharipande P. (MENDS Trial) JAMA. 2007;298: Riker R. (SEDCOM Trial) JAMA. 2009;301: Treggiari M. (Light vs. Deep Sedation-MH) Crit Care Med. 2009;37: Pandharipande P. (MENDS-Outcomes) Crit Care. 2010;14:R38. Strøm T. (No Sedation Protocol) Lancet. 2010;375: Needham D. (EM-ICU outcomes) Arch Phys Med Rehabil. 2010; 91: Jakob S. (MIDEX and PRODEX Trials) JAMA. 2012;307: Fraser G. (MA-Bnz vs. Non-bnz vs. outcomes) Crit Care Med. 2013; 41:S30-8. Dale C. (PAD protocol vs. outcomes) Ann Am Thorac Soc. 2014;11:
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium
 ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
What About All Those Critical Lines? Lines, catheters and drains can be accommodated, secured EVD line stationary bike
 What About All Those Critical Lines? Lines, catheters and drains can be accommodated, secured EVD line stationary bike What About All Those Critical Lines?. Patient lines and drains can be accommodated
What About All Those Critical Lines? Lines, catheters and drains can be accommodated, secured EVD line stationary bike What About All Those Critical Lines?. Patient lines and drains can be accommodated
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation
 Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
KEY REFERENCES laying the foundation for A of ABCDEF bundle
 KEY REFERENCES laying the foundation for A of ABCDEF bundle Puntillo K. Am J Crit Care (Response Procedural Pain) 2001;10:238-251 Payen J. Crit Care Med (Behavioral Pain Scale) 2001;29:2258-2263 Gelinas
KEY REFERENCES laying the foundation for A of ABCDEF bundle Puntillo K. Am J Crit Care (Response Procedural Pain) 2001;10:238-251 Payen J. Crit Care Med (Behavioral Pain Scale) 2001;29:2258-2263 Gelinas
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Delirium Screening and Prevention. Faculty Disclosures. Objectives 5/13/2014. I have nothing to disclose
 Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Faculty Disclosures
 Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
7/6/ ANNUAL MEETING BRINGING THE ABC(DEF) S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES
 S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES") ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Implementing the 2013 PAD Guidelines
 1 of 20 8/11/2013 10:25 PM www.medscape.com Implementing the 2013 PAD Guidelines Top Ten Points to Consider Brenda T. Pun, MSN, RN, ACNP, Michele C. Balas, PhD, RN, APRN-NP, CCRN, Judy Davidson, DNP, RN,
1 of 20 8/11/2013 10:25 PM www.medscape.com Implementing the 2013 PAD Guidelines Top Ten Points to Consider Brenda T. Pun, MSN, RN, ACNP, Michele C. Balas, PhD, RN, APRN-NP, CCRN, Judy Davidson, DNP, RN,
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
SEDATION / ANALGESIA for Brain Failure Patient INASNACC
 SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Juliana Barr, MD, FCCM
 Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER
 Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Delirium Information for patients and relatives. Delirium is common Delirium is treatable Relatives can stay to help us
 Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
Delirium Information for patients and relatives Delirium is common Delirium is treatable Relatives can stay to help us What is delirium? Delirium is caused by a disturbance of brain function. It is used
MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT
 MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT Objectives Understand some of the detrimental effects of critical illness, prolonged bed rest and
MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT Objectives Understand some of the detrimental effects of critical illness, prolonged bed rest and
Management of pain, agitation, and delirium in critically ill patients
 REVIEW ARTICLE Management of pain, agitation, and delirium in critically ill patients Pratik P. Pandharipande 1,2, Mayur B. Patel 2,3, Juliana Barr 4 1 Division of Critical Care, Department of Anesthesiology,
REVIEW ARTICLE Management of pain, agitation, and delirium in critically ill patients Pratik P. Pandharipande 1,2, Mayur B. Patel 2,3, Juliana Barr 4 1 Division of Critical Care, Department of Anesthesiology,
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
CRITICALLY APPRAISED PAPER (CAP) Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Kress, J.P. (2009). Early physical and occupational therapy in mechanically
Monitoring the Brain
 Cognition Monitoring the Brain Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center President Baylor Research Institute Dallas Texas Speaker Disclosure I have received
Cognition Monitoring the Brain Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center President Baylor Research Institute Dallas Texas Speaker Disclosure I have received
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
ABCDEF Bundle Breakout
 ABCDEF Bundle Breakout Andrew Masica, MD, MSCI VP, Chief Clinical Effectiveness Officer Baylor Scott & White Health andrew.masica@bswhealth.org Disclosures/Funding Support Grant R18-HS021459 from the Agency
ABCDEF Bundle Breakout Andrew Masica, MD, MSCI VP, Chief Clinical Effectiveness Officer Baylor Scott & White Health andrew.masica@bswhealth.org Disclosures/Funding Support Grant R18-HS021459 from the Agency
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program. Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN
 Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN Challenge, Journey, Evolution Everest is 29, 035 ft. 5 ½
Start Walking: Improving Outcomes through Use of an Early Progressive Mobility Program Theresa Murray MSN,RN, CCRN,CCNS Samantha Lichti BSN, RN Challenge, Journey, Evolution Everest is 29, 035 ft. 5 ½
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION
 ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
CUSP 4 MVP-VAP Patient Care Bundle
 Spontaneous Awakening and Spontaneous Breathing Trials, Literature Synopsis CUSP 4 MVP-VAP Patient Care Bundle Spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT) reduce the length
Spontaneous Awakening and Spontaneous Breathing Trials, Literature Synopsis CUSP 4 MVP-VAP Patient Care Bundle Spontaneous awakening trials (SAT) and spontaneous breathing trials (SBT) reduce the length
Sleep deprivation. Delirium
 acknowledgements Colleagues at BRI Delirium project group- Sam Heaton SSN (light therapy), Bex Russell Acting sister (this is me), Louise Sherratt- SSN (music therapy), Lucy Alford (RN) diaries) CIS team
acknowledgements Colleagues at BRI Delirium project group- Sam Heaton SSN (light therapy), Bex Russell Acting sister (this is me), Louise Sherratt- SSN (music therapy), Lucy Alford (RN) diaries) CIS team
Geriatric Pain Assessment and Management. Robin Arends, DNP, CNP, FNP-BC
 + Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
+ Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Delirium in Palliative care. Presentation to Volunteers 2016 David Falk
 Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Delirium and Falls. Julia Poole CNC Aged Care RNSH
 Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
Sedation Practice in Intensive Care Evaluation Early Goal Directed Sedation SPICE III
 Sedation Practice in Intensive Care Evaluation Early Goal Directed Sedation SPICE III Yahya SHEHABI Professor Intensive Care Medicine Program Medical Director, Critical Care Monash University, Monash Health
Sedation Practice in Intensive Care Evaluation Early Goal Directed Sedation SPICE III Yahya SHEHABI Professor Intensive Care Medicine Program Medical Director, Critical Care Monash University, Monash Health
Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
 Agitated patient in ICUapproach & management Arjun Srinivasan Agitation Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
Agitated patient in ICUapproach & management Arjun Srinivasan Agitation Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
What are Appropriate End-points for Delirium Prevention/Treatment Studies
 What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Sedation in The ICU: The Biological Cost of the Depression of Consciousness
 Sedation in The ICU: The Biological Cost of the Depression of Consciousness Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center Professor Texas A&M University Clinical
Sedation in The ICU: The Biological Cost of the Depression of Consciousness Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center Professor Texas A&M University Clinical
Preventing Postoperative Cognitive Decline in the Elderly
 Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Ohio/Minnesota Collaborative
 Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Preventing delirium while in hospital Tips for family, whānau, and friends who are supporting an older person
 Preventing delirium while in hospital Tips for family, whānau, and friends who are supporting an older person This brochure shares some simple ways you can help our care staff to prevent delirium, recognize
Preventing delirium while in hospital Tips for family, whānau, and friends who are supporting an older person This brochure shares some simple ways you can help our care staff to prevent delirium, recognize
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México
 Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México The facts Despite the efforts to optimize sedation and comfort of ICU s patients: More than 50% of patients
Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México The facts Despite the efforts to optimize sedation and comfort of ICU s patients: More than 50% of patients