Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass?
|
|
|
- Gary Strickland
- 5 years ago
- Views:
Transcription


1 Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass? Andrew W. Asimos, MD, FACEP Medical Director, Carolinas Stroke Network Carolinas Healthcare System Professor, Department of Emergency Medicine Carolinas Medical Center Charlotte, NC Matthew S. Siket, MD, MS, FACEP Co-Director, The Stroke Centers at Rhode Island Hospital & The Miriam Hospital Assistant Professor of Emergency Medicine The Warren Alpert Medical School of Brown University Providence, RI
2 Presenter Disclosure Information Andrew W. Asimos, MD Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass? FINANCIAL DISCLOSURE: Research Support: Stryker Neurovascular Teaching: Haymarket Medical Education (underwritten by Medtronic Inc.) Expert witness medical review in cases involving neurological emergencies UNLABELED/UNAPPROVED USES DISCLOSURE: IV tpa treatment of ischemic stroke beyond 3 hours of symptom onset

3 Stroke Triage and Destination Scenarios
4 Direct Routing Rationale An estimated 56% of patients live within one hour of a thrombectomy-capable hospital Smith EE, Schwamm LH. Stroke. 2015;46(6): Patients with Large Vessel Occlusion (LVO) Acute Ischemic Strokes (AIS) should be transported directly to an endovascular center Delays in interhospital transfers for ET reduce the likelihood of performing endovascular intervention Prabhakaran S et al. Stroke 2011;42: Interhospital transfer prior to thrombectomy is associated with delayed treatment and worse outcome Froehler MT et al. Circulation 2017; doi.org/ /circulationaha




5 Routing Algorithm Suspected stroke patient symptoms begin call EMS dispatched EMS travels to scene On Scene EMS assessment of stroke severity Positive screen for LVO and time since symptom onset 6 hours Negative screen for LVO or time since symptom onset > 6 hours Within permitted additional transport time to endovascular stroke center? No Yes Patient transport to nearest endovascular stroke center Patient transport to nearest hospital


6
7 Questions you need to ask and answer before implementing a regional routing protocol What rates of suspected severe stroke over-/undertriage are acceptable regionally? What are the sensitivities/specificities of your EMS dispatchers for stroke? What is the prevalence of LVO and/or ICH in the population that your EMS agencies transport for suspected acute stroke? What is the inter-rater reliability and accuracy of the chosen stroke severity screen for identifying LVOs (and ICHs?)? How have any time stipulations within the severity based triage protocol been determined? (e.g. time since LKW for screening eligibility, maximum added allowable transport time for routing)

8 Where do you start? At some point, either dispatch or the medics need to consider stroke as the diagnosis



9 The PLUMBER Study The Prevalence of Large vessel occlusion stroke in MecklenBurg County Emergency Response Study Cross sectional study of all patients transported by the Mecklenburg county EMS agency who were either Dispatched as a possible stroke and/or Primary impression of stroke recorded by prehospital providers Dozois AR, Hampton L, Kingston CW, Lambert G, Porcelli TJ, Sorenson D, Templin M, VonCannon S and Asimos AW. Stroke 2017;48: in press
10 LVO Prevalence in PLUMBER Dozois AR, Hampton L, Kingston CW, Lambert G, Porcelli TJ, Sorenson D, Templin M, VonCannon S and Asimos AW. Stroke 2017;48: in press

11 Poor accuracy of stroke identification by EMS Dispatch Sensitivity of 35-53% Caceres JA et al. J Stroke and Cerebrovasc Dis 2013;22(8):e610-e614. Krebes S et al. Stroke 2012;43: Specificity of 15-18% Viereck S et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2016;24:89 DOI /s Ramanujam P et al. Prehosp Emer Care 2008;12(3) Flowchart Showing the Triage and Initial Diagnoses of the Cleveland Clinic MSU Itrat A et al. JAMA Neurol 2016;73(2):162-8.

12 Serial Use of Stroke Screens Stroke Identification Screen (SIS) followed by a Stroke Severity Screen (SSS) Experience with the serial use of a SIS followed by a SSS has never been reported in the medical literature
13 Serial Use of Stroke Screens PLUMBER experience 2.7% of patients with an LVO had a normal CPSS (n=3/113), including occlusions of the ICA, M1, and the basilar artery Among patients with a positive CPSS, the prevalence of LVO increased to 11.2% (95% CI 9.3%-13.3%) Dozois AR. May18, 2017, SAEM Annual Meeting, Orlando, FL

14 Serial Use of Stroke Screens
15 Stroke Severity Screens

16 Stroke Severity Screens

17 Predictive Values of Stroke Severity Screens Based on a 5% and 10% Prevalence of LVO



18 Recommended Time Stipulations
19 Rebuttal Agree that inefficient transfer systems of care are a huge issue Agree that CSCs and PSCs should work together to improve stroke care for everyone Rhode Island PSC ELVO protocol work is promising McTaggart RA et al. JAMA Neurol 2017;74(7):
20 Los Angeles Motor Scale (LAMS) PURE MOTOR LAMS Definition Facial Droop Absent 0 NIHSS 0-1 Present 1 NIHSS 2-3 Arm Drift Absent 0 NIHSS 0 Drift down 1 NIHSS 1 Falls Rapidly 2 NIHSS 2-4 Grip Strength Normal 0 Admission Exam 5/5 Weak 1 Admission Exam 2-4/5 No Grip 2 Admission Exam 0-1 Positive LAMS: 4 Nazliel B et al. Stroke 2008;39:


21



:A83 LP-A83. http://stroke.")
22 Derivation 81% 89% Noorian A, Sanossian N, Liebeskind DS, et al. Abstract 83: Field Validation of Prehospital LAMS Score to Identify Large Vessel Occlusion Ischemic Stroke Patients for Direct Routing to Emergency Neuroendovascular Centers. Stroke. 2016;47(Suppl 1):A83 LP-A83.
:A18 LP-A18.")
23 RACE Scale Perez de la Ossa N, Abilleira S, Ribó M, et al. Abstract 18: External Validation of the RACE Scale After Its Implementation in the Stroke Code Protocol in Catalonia. Stroke. 2017;48(Suppl 1):A18 LP-A18.
:A18 LP-A18.")
24 Perez de la Ossa N, Abilleira S, Ribó M, et al. Abstract 18: External Validation of the RACE Scale After Its Implementation in the Stroke Code Protocol in Catalonia. Stroke. 2017;48(Suppl 1):A18 LP-A18.

25
26 North Carolina versus Rhode Island EMS in North Carolina 1,290 total agencies 410 EMS agencies 620 fire based 40,767 credentialed EMS professionals May not be affiliated Source: NC OEMS, Division of Health Service Regulation North Carolina Department of Health and Human Services EMS in Rhode Island 95 total agencies Majority are fire based (52) or third service (16) municipal departments 4,200 licensed providers Jayaraman MV et al. J NeuroIntervent Surg 2017;9(3):
27 North Carolina Telestroke Map: 2017

28 North Carolina Telestroke Map: 2017


29 10 minute policy Covers 68% of population 20 minute policy Covers 99% of population 30 minute policy Covers 100% of population Average minutes added to transport 0 < Bogle BM, Asimos AW and Rosamond WD. Stroke 2017;48(10):
30 Number of Patients transported to an Endovascular Center instead of closer hospital Sens/Spec: LAMS /0.89 RACE /0.68 C-STAT / LVOs 1.7x patients False positives x patients Bogle BM, Asimos AW and Rosamond WD. Stroke 2017;48(10): Minutes of permitted additional transport time
31 Minutes per year of additional transport time Sens/Spec: LAMS /0.89 RACE /0.68 C-STAT /0.40 9,060 9, x 5,370 5,462 2,445 2,437 1,773 2, Bogle BM, Asimos AW and Rosamond WD. Stroke 2017;48(10):
32 Number Needed to Route (NNR) Number of patients enduring additional transport time to route one LVO patient to an endovascular center Sensitivity: Specificity: LAMS RACE C-STAT Bogle BM, Asimos AW and Rosamond WD. Stroke 2017;48(10):
33 The specific scale chosen may be less important than the paradigm that some field severity assessment should be done to screen for possible ELVO. -MV Jayaraman et al. J Neurointervent Surg 2017;9(3):
34 Summary Premature to widely implement the Mission Lifeline Severity based triage algorithm Regions should continue to explore innovative approaches to regionalization of acute stroke care Prehospital telemedicine to triage Stroke Tank studies Novel Pull versus Push protocols


35 CATALIZE ALADIN Carolinas Accelerated Transfer Algorithm UtiLIZing Expedited Automated Large Artery Occlusion Detection IN Stroke
36 Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass? Matthew S. Siket, MD, MS, FACEP Co-Director, The Stroke Centers at Rhode Island Hospital & The Miriam Hospital Assistant Professor of Emergency Medicine The Warren Alpert Medical School of Brown University Providence, RI
37 Disclosures None





38




39 I m a Local Yokel




40 ESCAPE SWIFT- PRIME REVASCAT MR CLEAN NNT for a good outcome ranged from 3 to 7 EXTEND-IA Courtesy of Jayaraman MV


41 Time Dependent Effect Saver Jl et al. JAMA 2016

42 A drop of brain, a day of life Kawano et al. Brain 2017 & Saver JL. Brain 2017 Save a minute, save a week Meretoja A et al. Neurology 2017 for every 15 minute faster ED door-to-reperfusion time, an estimated 39 patients would be less disabled at 3 months, including 25 more who would achieve functional independence. [out of every 1000 achieving reperfusion] - Saver JL et al. JAMA 2016

43 In 2015, 10,284 thrombectomies were performed in the US of 31,866 LVOs presenting with LKW<6h and ASPECTS >6 In Q3 2016, 27.3% of eligible patients were treated Rai AT et al. BMJ 2016 Smith EE et al. Circulation 2017 Adeoye O et al. Stroke 2014
 in one study Mokin M, et al.")
44 Reasons for Failure Lack of recognition Delay to diagnosis Inefficient transfer systems-of-care ASPECTS decay during inter-facility transfer Occurred in 1/3 of patients (31%) in one study Mokin M, et al. JNIS 2017




45
46 Field Triage Mobile Stroke Units Centralized & Coordinated Dispatch Mobile Endovascular Teams Prehospital Stroke Severity Scales (accuracy range ) 3ISS LAMS CPSSS VAN PASS FAST-ED RACE LOC * * * Gaze * * * * * * Face * * * Arm * * * * * * * Grip * Leg * Aphasia * * * Neglect * * * Perez de la Ossa N et al. Stroke 2016

47 Zhao H et al. Stroke 2017
 LAMS is the right choice for RI Demonstrated convergent, divergent and")
 25% of EMS-transported stroke patients will have LAMS 4-5, of which >70%")
48 RISTF convened and agreed to LAMS 4-5 field triage to CSC if within a 30 minute drive time (JNIS 2016) LAMS is the right choice for RI Demonstrated convergent, divergent and predictive validity (Kim JT et al. Stroke 2017) 25% of EMS-transported stroke patients will have LAMS 4-5, of which >70% will be CSC appropriate (unpublished, ISC abstract 2017)
49 Drip n Ship or Mothership? Modelling dependent on: D2N and DIDO times at PSC D2N and D2G times at CSC Reperfusion rates at CSC Holodinsky J et al. Stroke 2017


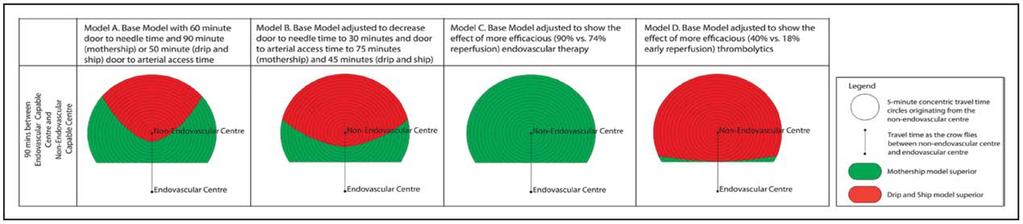


50 Model Favors Mothership when recanalization rates ~90% 20min 30min 90min 120min Holodinsky J et al. Stroke 2017

51 No Brainer Conditions required for drip n ship to be preferred: Longer onset-to-first medical response PSC D2N times < 30 min PSC DIDO times < 50 min CSC D2N times >60 min CSC Door-to-reperfusion time >200 min Transport time > 45 min Milne SW et al. Stroke 2017 Ng FC et al. Stroke 2017


52 Unfortunate Interpretation
53 CSCs and PSCs should work together to improve stroke care for everyone


54 RI Initiative: 1. Notify CSC on arrival 2. Immediate CT/CTA 3. Image sharing to cloud-based platform RESULTS: 40 minute reduction in DIDO time (p<.001) Twice as likely to have a favorable outcome (50% vs. 25%, P<.04) JAMA Neurol 2017
 Collectively, 80.")
55 We ve been down this road before 25% reduction in death for severely injured patients who went to a Level I trauma center Sasser SM et al. MMWR 2012 Current national field triage guidelines for identifying seriously injured persons use 4 criteria (anatomic, physiologic, MOI and special considerations) Collectively, 80.1% sensitive and 87.3% specific for early critical resource use 37.3% overtriage rate Studied in over 1.5 million patients Newgard CD et al. J Am Coll Surg 2016
56 At the end of the day, this is really an ethical debate, not a data duel





57 Visionary Mission: Lifeline Stroke Co-Chairs Lee Schwamm-istotle Peter Panagos-ocrates

58 We know severity-based triage offers the most benefit to patients with LVO It obviates the harm caused by stroke progression while awaiting definitive care Creates a just and fair system wherein all patients have the same access to specialized care

59 THANK
60 Rebuttal
61 The severity scales are poor tools They have demonstrated accuracy and predict CSC need (ELVO & ICH) It is estimated that ~25% of suspected stroke patients will have a LAMS 4-5 Overtriage with LAMS appears to be <30%, which is better than current trauma triage criteria
62 This will hurt low-volume centers Not if implemented correctly. At TMH, we have seen a rise in the number of stroke patients and an improvement in D2N times in 2017, despite administering half as much tpa as 2016 Working with CSCs will help ensure efficient transfer of appropriate patients and retention of non-indicated transfers
63 Patient volume will overwhelm CSCs LVO and ICH account for a minority of acute stroke patients Providing EMS and referring facilities with feedback, education and monitoring will help ensure protocol compliance Transparent system-wide data review is important for continued engagement and process refinement

64 It is taking patients out of their communities for an unlikely diagnosis LVO likely accounts for 10-25% of AIS and the appropriateness criteria for intervention is continually expanding These patients are the most likely to suffer long-term disability and death from their stroke Expediting a process by which they can receive definitive care, if needed, is the best thing we can do for them
65 In Summary The Mission: Lifeline EMS Stroke Triage Algorithm is an appropriate first step in the right direction It should be implemented across the country and individualized to meet each region s needs We in RI are a successful model of how this can be implemented and are proud of the what s being done

66 Thank you for this opportunity. Enjoy beautiful Newport and the NECC
Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass?
 Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass? Andrew W. Asimos, MD, FACEP Medical Director, Carolinas Stroke Network Carolinas Healthcare System Professor, Department
Transport of Suspected Large Vessel Occlusion: What s the Right Protocol for Bypass? Andrew W. Asimos, MD, FACEP Medical Director, Carolinas Stroke Network Carolinas Healthcare System Professor, Department
DISCLOSURES HUY TRAN MD UNM DEPARTMENT OF NEUROLOGY AND NEUROSURGERY NO DISCLOSURES
 DISCLOSURES ANDREW HARRELL MD FAEMS UNM DEPARTMENT OF EMERGENCY MEDICINEUNM EMS MEDICAL DIRECTION CONSORTIUM MEDICAL DIRECTOR, ALBUQUERQUE FIRE DEPARTMENT MEDICAL DIRECTOR, GRAND CANYON NATIONAL PARK TEMS
DISCLOSURES ANDREW HARRELL MD FAEMS UNM DEPARTMENT OF EMERGENCY MEDICINEUNM EMS MEDICAL DIRECTION CONSORTIUM MEDICAL DIRECTOR, ALBUQUERQUE FIRE DEPARTMENT MEDICAL DIRECTOR, GRAND CANYON NATIONAL PARK TEMS
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center. What do we know?
 Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers
 Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Acute Ischaemic Stroke Pathways Drip and Ship
 Acute Ischaemic Stroke Pathways Drip and Ship Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor
Acute Ischaemic Stroke Pathways Drip and Ship Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor
Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field. Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke
 Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke Suggested Protocols Suggested protocols are just that. They are not
Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke Suggested Protocols Suggested protocols are just that. They are not
Evolution of Mission: Lifeline Stroke The Stroke of the Severity-Based Stroke Triage Algorithm
 Evolution of Mission: Lifeline Stroke The Stroke of the Severity-Based Stroke Triage Algorithm Peter D. Panagos, MD, FAHA, FACEP Professor of Emergency Medicine and Neurology Washington University Saint
Evolution of Mission: Lifeline Stroke The Stroke of the Severity-Based Stroke Triage Algorithm Peter D. Panagos, MD, FAHA, FACEP Professor of Emergency Medicine and Neurology Washington University Saint
Statewide Acute Stroke Triage The Washington Story
 Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
WHY TIMELINESS MATTERS. W&M Wren Association Lecture Series
 WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare
 Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
DISCLOSURES. Learning Objectives. David Lee Gordon, MD, FAHA Update in Stroke 2007 FINANCIAL DISCLOSURE UNLABELED/UNAPPROVED USES DISCLOSURE
 Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
North Carolina Stroke Systems of Care Survey. Presented on behalf of the Integrating & Accessing Care Work Group of the Stroke Advisory Council
 North Carolina Stroke Systems of Care Survey Presented on behalf of the Integrating & Accessing Care Work Group of the Stroke Advisory Council Survey Overview The survey was developed with input from the
North Carolina Stroke Systems of Care Survey Presented on behalf of the Integrating & Accessing Care Work Group of the Stroke Advisory Council Survey Overview The survey was developed with input from the
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools
 Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
PREHOSPITAL ACUTE STROKE TRIAGE TIME: A PRAGMATIC TRIAL. StrokeNet SC Call November 8, 2017 Jason McMullan, Opeolu Adeoye, Nerses Sanossian
 PREHOSPITAL ACUTE STROKE TRIAGE TIME: A PRAGMATIC TRIAL StrokeNet SC Call November 8, 2017 Jason McMullan, Opeolu Adeoye, Nerses Sanossian STATUS UPDATE Original presentation to ASWG 6/2017 Reviewed at
PREHOSPITAL ACUTE STROKE TRIAGE TIME: A PRAGMATIC TRIAL StrokeNet SC Call November 8, 2017 Jason McMullan, Opeolu Adeoye, Nerses Sanossian STATUS UPDATE Original presentation to ASWG 6/2017 Reviewed at
Mark J. Alberts, MD. Turning the Wheels of Stroke Care
 Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of
Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of
ELVO update. Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon
 ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
Optimizing Care for Patients with Acute Ischemic Stroke Thrombolytic Therapy for Low NIHSS
 Optimizing Care for Patients with Acute Ischemic Stroke Thrombolytic Therapy for Low NIHSS Nerses Sanossian, MD, FAHA Presentation not eligible for CME credit Disclosures Today s objectives Case study:
Optimizing Care for Patients with Acute Ischemic Stroke Thrombolytic Therapy for Low NIHSS Nerses Sanossian, MD, FAHA Presentation not eligible for CME credit Disclosures Today s objectives Case study:
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
Updates on Endovascular Therapy
 Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
Slide 1. Slide 2. Slide 3 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER DISCLOSURES MY PATH TO EMS
 Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
Can We Apply Lessons Learned in Stroke Centers to Change Aspects of Cardiac Arrest Care?
 Can We Apply Lessons Learned in Stroke Centers to Change Aspects of Cardiac Arrest Care? 1 Mark J. Alberts, MD, FAHA Professor of Neurology Vice-Chair, Clinical Affairs Department of Neurology and Neurotherapeutics
Can We Apply Lessons Learned in Stroke Centers to Change Aspects of Cardiac Arrest Care? 1 Mark J. Alberts, MD, FAHA Professor of Neurology Vice-Chair, Clinical Affairs Department of Neurology and Neurotherapeutics
Role of recombinant tissue plasminogen activator in the updated stroke approach
 Role of recombinant tissue plasminogen activator in the updated stroke approach Joshua Z. Willey, MD, MS Assistant Professor of Neurology Division of Stroke, Columbia University October 2015 jzw2@columbia.edu
Role of recombinant tissue plasminogen activator in the updated stroke approach Joshua Z. Willey, MD, MS Assistant Professor of Neurology Division of Stroke, Columbia University October 2015 jzw2@columbia.edu
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion
 Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
ABNORMAL STROKE EXAM FINDINGS:
 Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group
 Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Disclosures. Current Management of Acute Ischemic Stroke. Overview. Focal brain ischemia. Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015
 Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes
 Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke
 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke. Kenneth V Snyder MD PhD SUNY Buffalo, NY
 Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Update on Neurologic Emergencies
 Update on Neurologic Emergencies KAREN GREENBERG, DO, FACOEP ARIA JEFFERSON HEALTH SYSTEM VIRTUA HEALTH SYSTEM KENNEDY HEALTH SYSTEM Disclosures Genentech Speakers Bureau I have disclosed a relevant relationship
Update on Neurologic Emergencies KAREN GREENBERG, DO, FACOEP ARIA JEFFERSON HEALTH SYSTEM VIRTUA HEALTH SYSTEM KENNEDY HEALTH SYSTEM Disclosures Genentech Speakers Bureau I have disclosed a relevant relationship
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Endovascular Stroke Therapy
 Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS
 CADIAN STROKE BEST PRACTICE RECOMMENDATIONS Emergency Medical Services (EMS) Management of Acute Stroke Patients Jean-Martin Boulanger and Kenneth Butcher (Writing Group Chairs) on Behalf of the ACUTE
CADIAN STROKE BEST PRACTICE RECOMMENDATIONS Emergency Medical Services (EMS) Management of Acute Stroke Patients Jean-Martin Boulanger and Kenneth Butcher (Writing Group Chairs) on Behalf of the ACUTE
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Systems of Care
 Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Maximising Delivery of Thrombectomy
 Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Shands at the University of Florida Stroke Program
 Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
10/26/2016. Disclosures. Mobile Stroke Units
 Mobile Stroke Units Andrei V. Alexandrov, MD Semmes-Murphey Professor and Chairman Department of Neurology Medical Director, Mobile Stroke Unit, UT Clinical Health Memphis, TN Disclosures Funding: Assisi
Mobile Stroke Units Andrei V. Alexandrov, MD Semmes-Murphey Professor and Chairman Department of Neurology Medical Director, Mobile Stroke Unit, UT Clinical Health Memphis, TN Disclosures Funding: Assisi
Illinois Stroke System Policy Overview
 Illinois Stroke System Policy Overview Christopher T. Richards, MD, MS, FAEMS Department of Emergency Medicine, Northwestern Feinberg School of Medicine Associate EMS Medical Director, Region XI EMS System
Illinois Stroke System Policy Overview Christopher T. Richards, MD, MS, FAEMS Department of Emergency Medicine, Northwestern Feinberg School of Medicine Associate EMS Medical Director, Region XI EMS System
Interventions to Improve Acute Ischemic Stroke Treatment Times
 Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 3-19-2018 Interventions to Improve Acute Ischemic Stroke Treatment Times Jayme Strauss Baptist Hospital of
Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 3-19-2018 Interventions to Improve Acute Ischemic Stroke Treatment Times Jayme Strauss Baptist Hospital of
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
12/4/2017. Disclosures. Study organization. Stryker Medtronic Penumbra Viz Route 92. Data safety monitoring board Tudor G.
 12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Large Vessel Occlusion Scales Increase Delivery to Endovascular Centers Without Excessive Harm From Misclassifications
 Large Vessel Occlusion Scales Increase Delivery to Endovascular Centers Without Excessive Harm From Misclassifications Henry Zhao, MBBS; Skye Coote, MN; Lauren Pesavento, BN; Leonid Churilov, PhD; Helen
Large Vessel Occlusion Scales Increase Delivery to Endovascular Centers Without Excessive Harm From Misclassifications Henry Zhao, MBBS; Skye Coote, MN; Lauren Pesavento, BN; Leonid Churilov, PhD; Helen
Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II
 Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II Gregg C. Fonarow MD, Eric E. Smith MD, MPH, Jeffrey L. Saver MD, Lee H. Schwamm, MD UCLA Division of Cardiology; Department
Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II Gregg C. Fonarow MD, Eric E. Smith MD, MPH, Jeffrey L. Saver MD, Lee H. Schwamm, MD UCLA Division of Cardiology; Department
Endovascular Clot Retrieval. Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital
 Christchurch Hospital") Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
NYC REMAC PUBLIC NOTICE PROPOSED REVISIONS PREHOSPITAL TREATMENT PROTOCOLS THE REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL OF NEW YORK CITY, INC.
 THE REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL OF NEW YORK CITY, INC. NYC REMAC PUBLIC NOTICE PROPOSED REVISIONS PREHOSPITAL TREATMENT PROTOCOLS The Regional Emergency Medical Advisory Committee (REMAC)
THE REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL OF NEW YORK CITY, INC. NYC REMAC PUBLIC NOTICE PROPOSED REVISIONS PREHOSPITAL TREATMENT PROTOCOLS The Regional Emergency Medical Advisory Committee (REMAC)
Mission: Lifeline Stroke Nebraska
 Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Field Assessment Stroke Triage for Emergency Destination A Simple and Accurate Prehospital Scale to Detect Large Vessel Occlusion Strokes
 Field Assessment Stroke Triage for Emergency Destination A Simple and Accurate Prehospital Scale to Detect Large Vessel Occlusion Strokes Fabricio O. Lima, Universidade Fortaleza Gisele S. Silva, Federal
Field Assessment Stroke Triage for Emergency Destination A Simple and Accurate Prehospital Scale to Detect Large Vessel Occlusion Strokes Fabricio O. Lima, Universidade Fortaleza Gisele S. Silva, Federal
polleverywhere.com To Join: Text KERRYAHRENS516 to For all future texts, you text your choice A-E
 polleverywhere.com To Join: Text KERRYAHRENS516 to 37607 For all future texts, you text your choice A-E Kerry Ahrens, MD MS I have no financial disclosures at this time. Kerry Ahrens MD, MS Emergency
polleverywhere.com To Join: Text KERRYAHRENS516 to 37607 For all future texts, you text your choice A-E Kerry Ahrens, MD MS I have no financial disclosures at this time. Kerry Ahrens MD, MS Emergency
Stroke Systems of Care Update
 Stroke Systems of Care Update Edward C. Jauch, MD MS FAHA FACEP Professor and Director, Division of Emergency Medicine Professor, Department of Neurosciences Associate Vice Chair, Research, Department
Stroke Systems of Care Update Edward C. Jauch, MD MS FAHA FACEP Professor and Director, Division of Emergency Medicine Professor, Department of Neurosciences Associate Vice Chair, Research, Department
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Interventional Stroke Treatment
 Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Disclosure. Advances in Interventional Neurology. Disclosure. Natural History of Disease 3/15/2018. Vishal B. Jani MD
 Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience
 Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience June 1st, 2018 Thomas Jeerakathil BSc, MD, MSc, FRCP(C) Professor Division of Neurology University of Alberta Northern Stroke Lead
Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience June 1st, 2018 Thomas Jeerakathil BSc, MD, MSc, FRCP(C) Professor Division of Neurology University of Alberta Northern Stroke Lead
EMS Recognition Webinar August 24, 2017
 EMS Recognition Webinar August 24, 2017 Today s objectives: Provide you with some rationale regarding the importance of reducing FMC to device time Provide you with an overview of the 2017 Mission: Lifeline
EMS Recognition Webinar August 24, 2017 Today s objectives: Provide you with some rationale regarding the importance of reducing FMC to device time Provide you with an overview of the 2017 Mission: Lifeline
Prehospital stroke scales and large vessel occlusion: A systematic review
 Accepted: 17 January 2018 DOI: 10.1111/ane.12908 ORIGINAL ARTICLE Prehospital stroke scales and large vessel occlusion: A systematic review S. Vidale 1 E. Agostoni 1,2 1 Department of Neurology & Stroke
Accepted: 17 January 2018 DOI: 10.1111/ane.12908 ORIGINAL ARTICLE Prehospital stroke scales and large vessel occlusion: A systematic review S. Vidale 1 E. Agostoni 1,2 1 Department of Neurology & Stroke
Best medical therapy (includes iv t-pa in eligible patients)
") UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
UDATE ON REVASCAT: (Randomized Trial Of Revascularization With Solitaire FR Device Versus Best Medical Therapy In The Treatment Of Acute Stroke Due To Anterior Circulation Large Vessel Occlusion Presenting
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer
 WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Strokecenter Key lessons of MR CLEAN study
 Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Get With The Guidelines - Stroke and Trends in New Jersey
 The Road to Recovery: Get With The Guidelines - Stroke and Trends in New Jersey Zainab Magdon-Ismail, DrPH Vice President, Quality & Systems Improvement Founders Affiliate (NJ-ME) American Heart Association
The Road to Recovery: Get With The Guidelines - Stroke and Trends in New Jersey Zainab Magdon-Ismail, DrPH Vice President, Quality & Systems Improvement Founders Affiliate (NJ-ME) American Heart Association
911 Dispatch initiated! Stroke Assessment-!! Decreasing time to treatment at Stroke Centers
 911 Dispatch initiated! Stroke Assessment-!! Decreasing time to treatment at Stroke Centers David Miramontes MD FACEP NREMT Emily Kidd MD FACEP Office of the Medical Director Stroke Embolic Strokes are
911 Dispatch initiated! Stroke Assessment-!! Decreasing time to treatment at Stroke Centers David Miramontes MD FACEP NREMT Emily Kidd MD FACEP Office of the Medical Director Stroke Embolic Strokes are
Further Pragmatic Trials of Thrombectomy are Needed
 Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
DISCLOSURES OBJECTIVES 11/18/2014. Stroke Network Update. None. Discuss
 Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Bypassing primary stroke centre reduces delay and improves outcomes for patients with large vessel occlusion
 Original research article Bypassing primary stroke centre reduces delay and improves outcomes for patients with large vessel occlusion European Stroke Journal 2016, Vol. 1(2) 85 92! European Stroke Organisation
Original research article Bypassing primary stroke centre reduces delay and improves outcomes for patients with large vessel occlusion European Stroke Journal 2016, Vol. 1(2) 85 92! European Stroke Organisation
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Mission: Lifeline Addressing the System of STEMI Care
 Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
New Zealand Out-of-Hospital Acute Stroke Destination Policy
 DRAFT FOR CONSULTATION New Zealand Out-of-Hospital Acute Stroke Destination Policy Northland and Auckland Areas This policy is for the use of clinical personnel when determining the destination hospital
DRAFT FOR CONSULTATION New Zealand Out-of-Hospital Acute Stroke Destination Policy Northland and Auckland Areas This policy is for the use of clinical personnel when determining the destination hospital
PHANTOM-S study Prehospital acute neurologic therapy and optimization of medical care in stroke Matthias Wendt on behalf of the PHANTOM-S study group
 PHANTOM-S study Prehospital acute neurologic therapy and optimization of medical care in stroke Matthias Wendt on behalf of the PHANTOM-S study group Recent guidelines 1. Intravenous rtpa (0.9 mg/kg, maximum
PHANTOM-S study Prehospital acute neurologic therapy and optimization of medical care in stroke Matthias Wendt on behalf of the PHANTOM-S study group Recent guidelines 1. Intravenous rtpa (0.9 mg/kg, maximum