Objective Aging and neurodegenerative diseases Common neurodegenerative diseases Pathogenesis Treatment strategies based on basic-science
|
|
|
- Claud Bates
- 5 years ago
- Views:
Transcription




1 Effect of Aging on Nervous System From Basic Neuroscience to Clinical Practice: Neurodegenerative Diseases Associate Professor Somsak Tiamkao Division of Neurology, Department of Medicine Faculty of Medicine, Khon Kaen University Old mens are boys again Tremulous hand and voices Stoop posture Slow Shuffling step Objective Aging and neurodegenerative diseases Common neurodegenerative diseases Pathogenesis Treatment strategies based on basic-science Collaborate Research Good Quality of Life Neurological Signs of Aging Eye signs: smaller pupil, hyperopia, dark adaptation Progressive hearing loss Diminution in the sense of smell, taste Reduced motor sign Reflex change Stance, posture, gait Cognitive function, learning, memory Physiologic and Anatomical Deterioration Age-Related Diseases Brain weight Blood flow to brain Cardiac output at rest Number of fiber in nerves Number of taste buds Power of hand grip Percentage decrease Cerebral atherosclerosis: stroke Brain tumor Infection Adverse drug reaction Falls Degenerative disease: AD 1


2 Degenerative:definition Decline from a previous level of normalcy to a lower level of function Gowers in 1902 suggested term "abiotrophy" Abiotrophy meant a lack of "vital endurance" resulting in their premature death. Degeneration refers to a more rapid process of neuronal, myelin, or tissue breakdown General Clinical Characteristics Begin insidiously, after a long period of normal nervous system function, and pursue a gradually progressive course that may continue for many years, often a decade longer. 2

3 B. Circumscribed cerebral atrophy 1. Pick disease (lobar sclerosis) 2. Mesolimbocortical dementia of non- Alzheimer type 3. Thalamic degeneration Neurodegenerative Disease Generalized degenerative disease Restricted degenerative disorder Gait and motor impairment: NPH Falls: postural reflex impairment Tremor Blepharospasm II Syndrome of progressive dementia in combination with other neurologic abnormalities A. Huntington chorea B. Other(nonhuntingtonian) types of chorea C. Cortical striatal-spinal degeneration (Jakob) and the dementia-parkinson-amyotrophic lateral sclerosis complex (Guamanian and others) D. Cortical-basal ganglionic degeneration Classification I. Syndrome of progressive dementia, other neurologic signs being absent / inconspicuous A. Diffuse cerebral atrophy 1. Alzheimer disease 2. Diffuse cerebral cortical atrophy of non-alzheimer type 3. Some cases of Lewy-body dementia E. Dentatorubropallidoluysian degeneration F. Cerebrocerebellar degeneration G. Familial dementia with spastic paraparesis or myoclonus H. Lewy-body disease I. Polyglucosan body disease 3
 and olivopontocerebellar atrophy (multiple system atrophy) C. Progressive supranuclear palsy D.")
4 III. Syndrome of disordered posture and movement A. Parkinson disease B. Striatonigral degeneration with or autonomic failure (Shy-Drager syndrome) and olivopontocerebellar atrophy (multiple system atrophy) C. Progressive supranuclear palsy D. Dystonia musculorum deformans (torsion spasm) C. Complicated cerebellar ataxias 1. Olivopontocerebellar degeneration with or without basal ganglia degeneration (multiple system atrophy) 2. Gerstmann-StraÜssler-Scheinker disease 3. Machado-Joseph disease 4. Other late-onset, autosomal dominant and sporadic ataxias D. Paraneoplastic and alcoholic-nutritional cerebellar degenerations E. Hallervorden-Spatz disease F. Restricted dystonias including spasmodic torticollis and Meige syndrome G. Familial tremors H. Multiple tic disease I. Acanthocytic chorea V. Syndrome of slowly developing muscular weakness and atrophy (nuclear amyotrophy) A. Without sensory changes: motor system disease 1. Amyotrophic lateral sclerosis 2. Progressive spinal muscular atrophy 3. Progressive bulbar palsy 4. Primary lateral sclerosis 5. Hereditary forms of progressive muscular atrophy and spastic paraplegia IV. Syndrome of progressive ataxia A. Predominantly spinal forms of hereditary ataxia 1. Friedreich ataxia 2. Non-Friedreich ataxia(with retained reflexes,hypogonadism, or myoclonus) B. Pure cerebellar forms of hereditary ataxia 1.Holmes familial cortical cerebellar atrophy 2.Late cerebellar cortical atrophy of Marie-Foix- Alajouanine B. With sensory changes 1. Hereditary sensory neuropathies 2. Hereditary sensorimotor neuropathiesperoneal muscular atrophy (Charcot-Marie- Tooth); hypertrophic interstitial polyneuropathy (Déjerine Sottas): heredopathia atactica polyneuritiformis (Refsum); etc 4

 B. Pigmentary degeneration of retina (retinitis pigmentosa) C. Stargardt disease D.")
, drugs E : Endocrine M : Metabolic E : Epilepsy N : Neoplasm, nutrition D E M E N T I A T : Toxic,")

5 VI. Syndrome of spastic paraplegia without amyotrophy A. Hereditary spastic paraplegia B. Primary lateral sclerosis The prevalence of dementia in elderly was 9.8 VII. Syndrome of progressive blindness or ophthalmoplegia with or without other neurologic disorders A. Hereditary optic neuropathy (Leber) B. Pigmentary degeneration of retina (retinitis pigmentosa) C. Stargardt disease D. Progressive external ophthalmoplegia with or without deafness or other system atrophies (Kearns-Sayre syndrome) D E M E N T I A D : Degenerative (AD), drugs E : Endocrine M : Metabolic E : Epilepsy N : Neoplasm, nutrition D E M E N T I A T : Toxic, trauma I : Infection, inflammation, infarction A : Atherosclerosis, alcohol VIII. Syndrome characterized by neurosensory deafness A. Pure neurosensory deafness B. Hereditary hearing loss with retinal disease C. Hereditary hearing loss with system atrophies of the nervous system Differential diagnosis; 2D 4A D epression D elirium A phasia A gnosia A nxiety A mnesia 5
6 1. ก (6 ) (1) ( )... (1)... (1)... (1) ( ) ( )... (1)... (1) ( ) ก (3 ) ( 1 ก ก 1 ก ) ก ก 86-7 (1) (1) (1) ก ก (3 ) (3) ก 3 ก 1 ( ) ก ก ก ก 1 ก... * ก ก ก 3 ก ก ก ก 5. ก (10 ) (1) ก ก ก... (1) ก ก... (1) ก ก ก (5 ) ก ( 1 ) (1) ก... (1)... (1)... (1)... (1)... ( 3 ) ก ก 3 1 (1) ก... (1) ก... (1) ก ก ก... (1) ก... ( ) (2) ก ( ก ) (1) ก ก ก... ก ก... 6
.")





7 ก ก (3 ) 3 ก ก (1)... (1)... (1) Vascular Dementia White matter disease Lacuna infarction B Neuroimaging helps differentiate AD AD + CVD VaD VaD and AD PET scan in Vascular Dementia VaD AD+CVD AD Many patients have overlap of AD and significant CVD The clinical overlap is referred to AD+CVD Healthy Brain Predominance of Large Infarcts Images courtesy of Michael Mega, UCLA. 7

 and transport it to")


 NGF then binds to TrkA receptors and is transported retrogradely to the cell")
8 Projecting cholinergic systems in the brain An important characteristic of the cholinergic neurons of the basal forebrain is their dependence on nerve growth factor (NGF). They synthesize the nerve growth factor receptor (TrkA receptor) and transport it to their terminals in the cerebral cortex Effect of NGF and pro-ngf on cell survival Cholinergic regions in basal forebrain AChE staining Normal Cellular and Molecular Neurobiology 2006; Aug 31 Epub ahead of print Cholinergic depletion and amyloidogenesis may be 2 interactive processes in AD ACh increases NGF production by cortical neurons Cerebral cholinergic projections from human basal forebrain Selden et al. Brain (1998) NGF then binds to TrkA receptors and is transported retrogradely to the cell bodies of NBM where it exerts a neurotrophic effects. NGF increases nonamyloidogenic processing Aβ42 interfere with NGF signaling. 8
 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.")
, galantamine (n=127), p=0.003. Placebo (n=59), galantamine (n=70), p<0.001.")


9 Target for ChEIs treatment Volumetric MRI Effect of Nicotinic Stimulation on Working Memory MCI MRI results Galantamine Placebo Rate of Brain Atrophy (%/y) * Total Population* Males Females *p = p < p = *Placebo (n=142), galantamine (n=127), p= Placebo (n=59), galantamine (n=70), p< Placebo (n=83), galantamine (n=57), p= Neuroprotective effects of galantamine Trophic factor dependency of cholinergic neurons Pro-NGF increase, NGF decrease in AD Pro-NGF is cleaved to NGF by tpa, plasminogen and Timp1 which are decreased in AD NGF binds with TrKA receptors which is expressed in basal forebrain cholinergic neurons (trophic effect) Atrophy of nucleus basalis of Meynert (NBM) in AD Bruno & Cuello PNAS 2006 Brain Res Bull 2005;64:


 60 40 20 0 Donepezil 10 mg/d GAL PRC 24 mg/d GAL IR 2 x 12 mg/d ACh release Low levels needed 8 AM 11 AM 2 PM 5 PM 8 PM 11 PM 2 AM 5 AM")
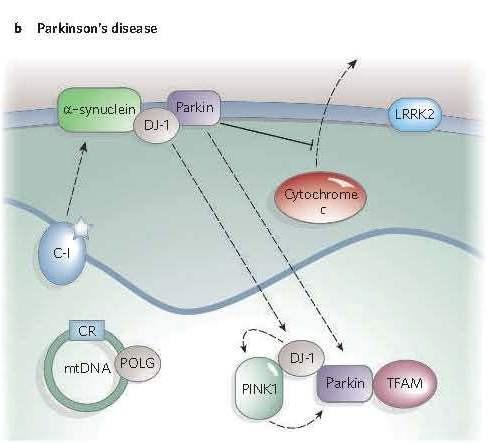
10 Cholinergic Circadian Rhythm High nocturnal ACh sleep-related AEs wakefulness 1 nightmares 2 sleep medication 3 memory consolidation AChE inhibition therapies should support cholinergic circadian rhythm AChE = acetylcholinesterase; AE = adverse event 1. Saint-Mleux B, et al. J Neurosci. 2004;24: Pagel JF. Hum Psychopharmacol. 2003;18: Stahl SM, et al. J Clin Psychiatry. 2003;64: Fig. Structure of mitochondrion The Galantamine ER - Pellet Based ER Capusle 25% as Immediate release Rate controlling membrane 75% as Extended release Sugar sphere Fig. The ubiquitin proteasome system Galantamine PRC: Low nocturnal ACh Proteins that have a function in major neurodegenerative diseases with mitochondrial involvement 80 0,6 Drug concentration (ng/ml) Donepezil 10 mg/d GAL PRC 24 mg/d GAL IR 2 x 12 mg/d ACh release Low levels needed 8 AM 11 AM 2 PM 5 PM 8 PM 11 PM 2 AM 5 AM Clock time 0,4 0,2 0 ACh release (pmol/min) Davis B, Sadik K. Dement Geriatr Cogn Disord. 2006;21:








11 Mitochondrial involvement in less common neurodegenerative disease Parkinson s Disease Substantia Nigra Parkinson s Disease Aetiology of Parkinson's disease Environmental or endogenous toxins Aetiology Single or multiple genes Pathogenesis free mitochondrial iron oxidative protein radicals dysfunction stress aggregation Parkinson's disease(s) 11


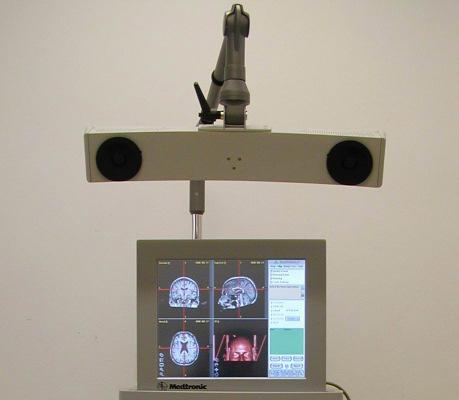



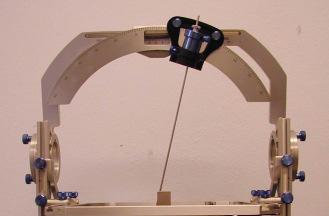




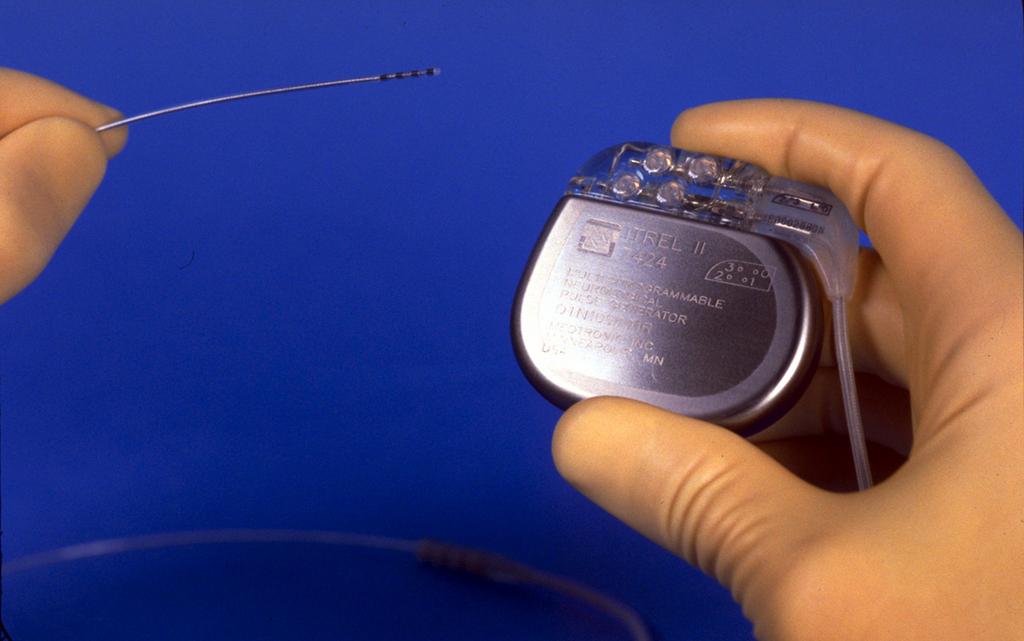
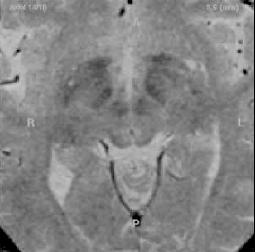



12 A. Normal Motor Circuit B. Motor Circuit in PD C. Motor Circuit In PD with Levodopainduced Dyskinesia CORTEX CORTEX CORTEX PUTAMEN PUTAMEN PUTAMEN SNc SNc Implanted Components DA DA SNc GPe GPe GPe VL VL STN STN VL STN GPi GPi GPi SNr SNr SNr PPN PPN PPN Excitatory Inhibitory C W Olanow, J A Obeso et al. TINS Supplement Surgery in Parkinson s disease Substantia nigra axial Instruments T2W FSE coronal Deep Brain Stimulation Off On 12






13 Amyotrophic Lateral Sclerosis 13

! 3.")
 % %)! ) * $ +% %& % +(.")
 % - ( 2 % 4")
5# - ( 8.")
 $!\" ( %! 9.")
14 Health Promotion Prevention is the Best 10 1.!" # $ %& ' % #( ( $ 2. % % $ )! 3. *""' %& ' %& +, +,! ) % %)! ) * $ +% %& % +(. %& ') ) )! )!/ ) 5. 0 %&! ' ( * 1 %& 0 ) % - ( 2 % 4 0 ) 6. %& -. ( 7., ' +% %&,." -. )5# - ( 8. )6 " ( $ ( )6! % ( % 4 0 ) $!" ( %! 9. ),,, %& ' 7 ),, 10. %&,, ( *! 8 * %&! 95 % 4 0 ) * ( # ( $. 14

15 Thank you The Kynurenine pathway 15
Table of Contents. Preface... xi. Part I: Introduction to Movement Disorders
 Table of Contents Visit www.healthreferenceseries.com to view A Contents Guide to the Health Reference Series, a listing of more than 14,000 topics and the volumes in which they are covered. Preface...
Table of Contents Visit www.healthreferenceseries.com to view A Contents Guide to the Health Reference Series, a listing of more than 14,000 topics and the volumes in which they are covered. Preface...
Cheyenne 11/28 Neurological Disorders II. Transmissible Spongiform Encephalopathy
 Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
DISORDERS OF THE MOTOR SYSTEM. Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
Basal ganglia Sujata Sofat, class of 2009
 Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
Index SLEEP MEDICINE CLINICS. Note: Page numbers of article titles are in boldface type.
 299 SLEEP MEDICINE CLINICS Sleep Med Clin 1 (2006) 299 303 Note: Page numbers of article titles are in boldface type. A Acid reflux, sleep disturbances in older adults related to, 238 Aging, alterations
299 SLEEP MEDICINE CLINICS Sleep Med Clin 1 (2006) 299 303 Note: Page numbers of article titles are in boldface type. A Acid reflux, sleep disturbances in older adults related to, 238 Aging, alterations
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
The motor regulator. 1) Basal ganglia/nucleus
 Basal ganglia/nucleus") The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
A. General features of the basal ganglia, one of our 3 major motor control centers:
 Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. March 1, 2012 THE BASAL GANGLIA Objectives: 1. What are the main
Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. March 1, 2012 THE BASAL GANGLIA Objectives: 1. What are the main
Identification number: TÁMOP /1/A
 Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
A. General features of the basal ganglia, one of our 3 major motor control centers:
 Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. April 22, 2010 THE BASAL GANGLIA Objectives: 1. What are the
Reading: Waxman pp. 141-146 are not very helpful! Computer Resources: HyperBrain, Chapter 12 Dental Neuroanatomy Suzanne S. Stensaas, Ph.D. April 22, 2010 THE BASAL GANGLIA Objectives: 1. What are the
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy"
 Parkinson's Disease First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy" Parkinson s disease (PD) is a neurological disorder characterized by a progressive
Parkinson's Disease First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy" Parkinson s disease (PD) is a neurological disorder characterized by a progressive
212 Index C-SB-13,
 Index A Acetylcholinesterase inhibitor, treatment, 15 Age-associated memory impairment (AAMI), 5 Alzheimer s disease (AD), 40, 95 96 apolipoprotein E genotype and risk for, 58 cellular neurodegeneration
Index A Acetylcholinesterase inhibitor, treatment, 15 Age-associated memory impairment (AAMI), 5 Alzheimer s disease (AD), 40, 95 96 apolipoprotein E genotype and risk for, 58 cellular neurodegeneration
Making Things Happen 2: Motor Disorders
 Making Things Happen 2: Motor Disorders How Your Brain Works Prof. Jan Schnupp wschnupp@cityu.edu.hk HowYourBrainWorks.net On the Menu in This Lecture In the previous lecture we saw how motor cortex and
Making Things Happen 2: Motor Disorders How Your Brain Works Prof. Jan Schnupp wschnupp@cityu.edu.hk HowYourBrainWorks.net On the Menu in This Lecture In the previous lecture we saw how motor cortex and
Biology 3201 Nervous System # 7: Nervous System Disorders
 Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Non-Genetic Ataxia Susan L. Perlman, M.D. Clinical Professor of Neurology David Geffen School of Medicine at UCLA Director, Ataxia Clinic
 Non-Genetic Ataxia Susan L. Perlman, M.D. Clinical Professor of Neurology David Geffen School of Medicine at UCLA Director, Ataxia Clinic Is Anything Non-Genetic? 1,212,000 references in PubMed under genetics
Non-Genetic Ataxia Susan L. Perlman, M.D. Clinical Professor of Neurology David Geffen School of Medicine at UCLA Director, Ataxia Clinic Is Anything Non-Genetic? 1,212,000 references in PubMed under genetics
Strick Lecture 4 March 29, 2006 Page 1
 Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Basal Ganglia George R. Leichnetz, Ph.D.
 Basal Ganglia George R. Leichnetz, Ph.D. OBJECTIVES 1. To understand the brain structures which constitute the basal ganglia, and their interconnections 2. To understand the consequences (clinical manifestations)
Basal Ganglia George R. Leichnetz, Ph.D. OBJECTIVES 1. To understand the brain structures which constitute the basal ganglia, and their interconnections 2. To understand the consequences (clinical manifestations)
COGNITIVE SCIENCE 107A. Motor Systems: Basal Ganglia. Jaime A. Pineda, Ph.D.
 COGNITIVE SCIENCE 107A Motor Systems: Basal Ganglia Jaime A. Pineda, Ph.D. Two major descending s Pyramidal vs. extrapyramidal Motor cortex Pyramidal system Pathway for voluntary movement Most fibers originate
COGNITIVE SCIENCE 107A Motor Systems: Basal Ganglia Jaime A. Pineda, Ph.D. Two major descending s Pyramidal vs. extrapyramidal Motor cortex Pyramidal system Pathway for voluntary movement Most fibers originate
GBME graduate course. Chapter 43. The Basal Ganglia
 GBME graduate course Chapter 43. The Basal Ganglia Basal ganglia in history Parkinson s disease Huntington s disease Parkinson s disease 1817 Parkinson's disease (PD) is a degenerative disorder of the
GBME graduate course Chapter 43. The Basal Ganglia Basal ganglia in history Parkinson s disease Huntington s disease Parkinson s disease 1817 Parkinson's disease (PD) is a degenerative disorder of the
CN V! touch! pain! Touch! P/T!
 CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Extrapyramidal Motor System. Basal Ganglia or Striatum. Basal Ganglia or Striatum 3/3/2010
 Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Dr. Farah Nabil Abbas. MBChB, MSc, PhD
 Dr. Farah Nabil Abbas MBChB, MSc, PhD The Basal Ganglia *Functions in association with motor cortex and corticospinal pathways. *Regarded as accessory motor system besides cerebellum. *Receive most of
Dr. Farah Nabil Abbas MBChB, MSc, PhD The Basal Ganglia *Functions in association with motor cortex and corticospinal pathways. *Regarded as accessory motor system besides cerebellum. *Receive most of
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS
 MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
MUSCULOSKELETAL AND NEUROLOGICAL DISORDERS There are a wide variety of Neurologic and Musculoskeletal disorders which can impact driving safety. Impairment may be the result of altered muscular, skeletal,
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology
 Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Movement disorders in childhood: assessment and diagnosis. Lucinda Carr
 Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Anatomy of the basal ganglia. Dana Cohen Gonda Brain Research Center, room 410
 Anatomy of the basal ganglia Dana Cohen Gonda Brain Research Center, room 410 danacoh@gmail.com The basal ganglia The nuclei form a small minority of the brain s neuronal population. Little is known about
Anatomy of the basal ganglia Dana Cohen Gonda Brain Research Center, room 410 danacoh@gmail.com The basal ganglia The nuclei form a small minority of the brain s neuronal population. Little is known about
Multiple System Atrophy
 Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Lecture XIII. Brain Diseases I - Parkinsonism! Brain Diseases I!
 Lecture XIII. Brain Diseases I - Parkinsonism! Bio 3411! Wednesday!! Lecture XIII. Brain Diseases - I.! 1! Brain Diseases I! NEUROSCIENCE 5 th ed! Page!!Figure!!Feature! 408 18.9 A!!Substantia Nigra in
Lecture XIII. Brain Diseases I - Parkinsonism! Bio 3411! Wednesday!! Lecture XIII. Brain Diseases - I.! 1! Brain Diseases I! NEUROSCIENCE 5 th ed! Page!!Figure!!Feature! 408 18.9 A!!Substantia Nigra in
Dementia syndrome. Manifestation DISORDERS & DEMENTIA. Reasons of demencia
 Manifestation DEGENERATIVE DISORDERS & DEMENTIA Roman Beňačka, MD,PhD Department of Pathophysiology Medical Faculty, Šafarik University Košice Increase in time required to retrieve information Less able
Manifestation DEGENERATIVE DISORDERS & DEMENTIA Roman Beňačka, MD,PhD Department of Pathophysiology Medical Faculty, Šafarik University Košice Increase in time required to retrieve information Less able
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Teach-SHEET Basal Ganglia
 Teach-SHEET Basal Ganglia Purves D, et al. Neuroscience, 5 th Ed., Sinauer Associates, 2012 Common organizational principles Basic Circuits or Loops: Motor loop concerned with learned movements (scaling
Teach-SHEET Basal Ganglia Purves D, et al. Neuroscience, 5 th Ed., Sinauer Associates, 2012 Common organizational principles Basic Circuits or Loops: Motor loop concerned with learned movements (scaling
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Connections of basal ganglia
 Connections of basal ganglia Introduction The basal ganglia, or basal nuclei, are areas of subcortical grey matter that play a prominent role in modulating movement, as well as cognitive and emotional
Connections of basal ganglia Introduction The basal ganglia, or basal nuclei, are areas of subcortical grey matter that play a prominent role in modulating movement, as well as cognitive and emotional
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Basal Ganglia. Steven McLoon Department of Neuroscience University of Minnesota
 Basal Ganglia Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Graduate School Discussion Wednesday, Nov 1, 11:00am MoosT 2-690 with Paul Mermelstein (invite your friends)
Basal Ganglia Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Graduate School Discussion Wednesday, Nov 1, 11:00am MoosT 2-690 with Paul Mermelstein (invite your friends)
Visualization and simulated animations of pathology and symptoms of Parkinson s disease
 Visualization and simulated animations of pathology and symptoms of Parkinson s disease Prof. Yifan HAN Email: bctycan@ust.hk 1. Introduction 2. Biochemistry of Parkinson s disease 3. Course Design 4.
Visualization and simulated animations of pathology and symptoms of Parkinson s disease Prof. Yifan HAN Email: bctycan@ust.hk 1. Introduction 2. Biochemistry of Parkinson s disease 3. Course Design 4.
Lecture 42: Final Review. Martin Wessendorf, Ph.D.
 Lecture 42: Final Review Martin Wessendorf, Ph.D. Lecture 33 cortex Heilbronner 5 lobes of the cortex Lateral view (left side) Mid-saggital view (right side) Cellular organization of cortex White matter
Lecture 42: Final Review Martin Wessendorf, Ph.D. Lecture 33 cortex Heilbronner 5 lobes of the cortex Lateral view (left side) Mid-saggital view (right side) Cellular organization of cortex White matter
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Chapter 20. Media Directory. Amyotrophic Lateral Sclerosis. Alzheimer s Disease. Huntington s Chorea. Multiple Sclerosis
 Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
MOVEMENT OUTLINE. The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement
 MOVEMENT 2 Dr. Steinmetz 3 OUTLINE The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement Parkinson s Disease Huntington s Disease 1 4 TYPES
MOVEMENT 2 Dr. Steinmetz 3 OUTLINE The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement Parkinson s Disease Huntington s Disease 1 4 TYPES
Imaging biomarkers for Parkinson s disease
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 6 MDS-ES/EAN: Neuroimaging in movement disorders - Level 2 Imaging biomarkers for Parkinson
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 6 MDS-ES/EAN: Neuroimaging in movement disorders - Level 2 Imaging biomarkers for Parkinson
Initial symptom or syndrome: (1) FOCAL WEAKNESS OR NUMBNESS
 FOCAL WEAKNESS OR NUMBNESS") View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
Basal Ganglia. Today s lecture is about Basal Ganglia and it covers:
 Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Basal Ganglia Motor system is complex interaction between Lower motor neurons (spinal cord and brainstem circuits) and Upper motor neurons (pyramidal and extrapyramidal tracts) plus two main regulators
Basal nuclei, cerebellum and movement
 Basal nuclei, cerebellum and movement MSTN121 - Neurophysiology Session 9 Department of Myotherapy Basal Nuclei (Ganglia) Basal Nuclei (Ganglia) Role: Predict the effects of various actions, then make
Basal nuclei, cerebellum and movement MSTN121 - Neurophysiology Session 9 Department of Myotherapy Basal Nuclei (Ganglia) Basal Nuclei (Ganglia) Role: Predict the effects of various actions, then make
The Marmoset Monkey as Model for Neurological Disorders
 The Marmoset Monkey as Model for Neurological Disorders Jan Langermans and Ingrid Philippens From Laboratory to Clinic Disease models neuroscience: Parkinson, Sleep, Stress, Alzheimer, MS MS Models: rhmog
The Marmoset Monkey as Model for Neurological Disorders Jan Langermans and Ingrid Philippens From Laboratory to Clinic Disease models neuroscience: Parkinson, Sleep, Stress, Alzheimer, MS MS Models: rhmog
GENETICS AND TREATMENT OF DYSTONIA
 GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
Department of Neurology, Rigshospitalet, 9 Blegdamsvej, PAULSON, O.B. Involuntary Movements. Tohoku J. Exp. Med., 1990, 161,
 Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y
 Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Shift 1, 8 July 2018, 09:30-13:00
 Shift 1, 8 July 2018, 09:30-13:00 CNS patterning A001-A014 Stem cells: basic biology and postnatal neurogenesis - part I Development of neural systems: Molecular and genetic characterisationa Epigenetic
Shift 1, 8 July 2018, 09:30-13:00 CNS patterning A001-A014 Stem cells: basic biology and postnatal neurogenesis - part I Development of neural systems: Molecular and genetic characterisationa Epigenetic
Dementia. Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
How to Effectively Manage the Motor Symptoms of HD
 How to Effectively Manage the Motor Symptoms of HD Yvette Bordelon, MD, PhD Associate Clinical Professor of Neurology David Geffen School of Medicine at UCLA The information provided by speakers in workshops,
How to Effectively Manage the Motor Symptoms of HD Yvette Bordelon, MD, PhD Associate Clinical Professor of Neurology David Geffen School of Medicine at UCLA The information provided by speakers in workshops,
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
panel tests assessing multiple genes at the same time for the diagnosis of one or more related disorders
 NGS tests panel tests assessing multiple genes at the same time for the diagnosis of one or more related disorders UKGTN website lists 13 laboratories offering a total of 56 panel test UKGTN listed panel
NGS tests panel tests assessing multiple genes at the same time for the diagnosis of one or more related disorders UKGTN website lists 13 laboratories offering a total of 56 panel test UKGTN listed panel
PSY 315 Lecture 11 (2/23/2011) (Motor Control) Dr. Achtman PSY 215. Lecture 11 Topic: Motor System Chapter 8, pages
 (Motor Control) Dr. Achtman PSY 215. Lecture 11 Topic: Motor System Chapter 8, pages") Corrections: No Corrections Announcements: Exam #2 next Wednesday, March 2, 2011 Monday February 28, 2011 we will be going over the somatosensory system, and there will be time left in class to review
Corrections: No Corrections Announcements: Exam #2 next Wednesday, March 2, 2011 Monday February 28, 2011 we will be going over the somatosensory system, and there will be time left in class to review
Objectives. RAIN Difficult Diagnosis 2014: A 75 year old woman with falls. Case History: First visit. Case History: First Visit
 Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
Objectives RAIN Difficult Diagnosis 2014: A 75 year old woman with falls Alexandra Nelson MD, PhD UCSF Memory and Aging Center/Gladstone Institute of Neurological Disease Recognize important clinical features
C-type: For each numbered item or question, indicate whether it is associated
 C-type: For each numbered item or question, indicate whether it is associated with: (A) A only (B) B only (C) Both A and B (D) Neither A nor B ( ) 1. About neuroleptic malignant syndrome and serotonin
C-type: For each numbered item or question, indicate whether it is associated with: (A) A only (B) B only (C) Both A and B (D) Neither A nor B ( ) 1. About neuroleptic malignant syndrome and serotonin
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
TOXIC AND NUTRITIONAL DISORDER MODULE
 TOXIC AND NUTRITIONAL DISORDER MODULE Objectives: For each of the following entities the student should be able to: 1. Describe the etiology/pathogenesis and/or pathophysiology, gross and microscopic morphology
TOXIC AND NUTRITIONAL DISORDER MODULE Objectives: For each of the following entities the student should be able to: 1. Describe the etiology/pathogenesis and/or pathophysiology, gross and microscopic morphology
PET ligands and metabolic brain imaging Prof. Karl Herholz
 PET ligands Karl Herholz, University of Manchester PET images in this lecture, unless indicated otherwise, are from Max-Planck-Institute for Neurological Research, Cologne, Germany 1 Positron-Emission-Tomography
PET ligands Karl Herholz, University of Manchester PET images in this lecture, unless indicated otherwise, are from Max-Planck-Institute for Neurological Research, Cologne, Germany 1 Positron-Emission-Tomography
Strategies for Neurorestoration: Growth Factors
 Strategies for Neurorestoration: Growth Factors Elena Posse de Chaves, PhD 928-MSB Phone: 492-5966 Email: elena.chaves@ualberta.ca Treatment of Neurodegenerative Diseases Most neurodegenerative diseases
Strategies for Neurorestoration: Growth Factors Elena Posse de Chaves, PhD 928-MSB Phone: 492-5966 Email: elena.chaves@ualberta.ca Treatment of Neurodegenerative Diseases Most neurodegenerative diseases
Damage on one side.. (Notes) Just remember: Unilateral damage to basal ganglia causes contralateral symptoms.
 Just remember: Unilateral damage to basal ganglia causes contralateral symptoms.") Lecture 20 - Basal Ganglia Basal Ganglia (Nolte 5 th Ed pp 464) Damage to the basal ganglia produces involuntary movements. Although the basal ganglia do not influence LMN directly (to cause this involuntary
Lecture 20 - Basal Ganglia Basal Ganglia (Nolte 5 th Ed pp 464) Damage to the basal ganglia produces involuntary movements. Although the basal ganglia do not influence LMN directly (to cause this involuntary
An approach to movement disorders. Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London
 An approach to movement disorders Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London Neurology Diagnosis Two main questions: What parts of the nervous
An approach to movement disorders Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London Neurology Diagnosis Two main questions: What parts of the nervous
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Parts of the motor circuits
 MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
Chronic Traumatic Encephalopathy Provider and Parent Essentials
 Chronic Traumatic Encephalopathy Provider and Parent Essentials Concussion Global Cast July 30, 2014 John Lockhart, MD Seattle Children s Hospital Chronic Traumatic Encephaly (CTE) Working Definition Chronic
Chronic Traumatic Encephalopathy Provider and Parent Essentials Concussion Global Cast July 30, 2014 John Lockhart, MD Seattle Children s Hospital Chronic Traumatic Encephaly (CTE) Working Definition Chronic
Ch 13: Central Nervous System Part 1: The Brain p 374
 Ch 13: Central Nervous System Part 1: The Brain p 374 Discuss the organization of the brain, including the major structures and how they relate to one another! Review the meninges of the spinal cord and
Ch 13: Central Nervous System Part 1: The Brain p 374 Discuss the organization of the brain, including the major structures and how they relate to one another! Review the meninges of the spinal cord and
Neuropathology of Neurodegenerative Disorders Prof. Jillian Kril
 Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Nervous System. 1. What N.S. division controls skeletal muscles? 3. What kind of neuroglia myelinates axons in the PNS?
 . What N.S. division controls skeletal muscles? Nervous System SRS Review %. Central nervous system %. Peripheral nervous system %. Afferent division %. Somatic division %. Autonomic division %. Sympathetic
. What N.S. division controls skeletal muscles? Nervous System SRS Review %. Central nervous system %. Peripheral nervous system %. Afferent division %. Somatic division %. Autonomic division %. Sympathetic
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Biological Bases of Behavior. 8: Control of Movement
 Biological Bases of Behavior 8: Control of Movement m d Skeletal Muscle Movements of our body are accomplished by contraction of the skeletal muscles Flexion: contraction of a flexor muscle draws in a
Biological Bases of Behavior 8: Control of Movement m d Skeletal Muscle Movements of our body are accomplished by contraction of the skeletal muscles Flexion: contraction of a flexor muscle draws in a
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Basal Ganglia. Introduction. Basal Ganglia at a Glance. Role of the BG
 Basal Ganglia Shepherd (2004) Chapter 9 Charles J. Wilson Instructor: Yoonsuck Choe; CPSC 644 Cortical Networks Introduction A set of nuclei in the forebrain and midbrain area in mammals, birds, and reptiles.
Basal Ganglia Shepherd (2004) Chapter 9 Charles J. Wilson Instructor: Yoonsuck Choe; CPSC 644 Cortical Networks Introduction A set of nuclei in the forebrain and midbrain area in mammals, birds, and reptiles.
! slow, progressive, permanent loss of neurologic function.
 UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
UBC ! slow, progressive, permanent loss of neurologic function.! cause unknown.! sporadic, familial or inherited.! degeneration of specific brain region! clinical syndrome.! pathology: abnormal accumulation
Department of Neurology
 OUTCOMES DIVISION OF MEDICINE Department of Neurology About Cleveland Clinic Florida Cleveland Clinic Florida s medical staff are dedicated physicians who have joined the clinic as salaried doctors to
OUTCOMES DIVISION OF MEDICINE Department of Neurology About Cleveland Clinic Florida Cleveland Clinic Florida s medical staff are dedicated physicians who have joined the clinic as salaried doctors to
Neuroscience 410 Huntington Disease - Clinical. March 18, 2008
 Neuroscience 410 March 20, 2007 W. R. Wayne Martin, MD, FRCPC Division of Neurology University of Alberta inherited neurodegenerative disorder autosomal dominant 100% penetrance age of onset: 35-45 yr
Neuroscience 410 March 20, 2007 W. R. Wayne Martin, MD, FRCPC Division of Neurology University of Alberta inherited neurodegenerative disorder autosomal dominant 100% penetrance age of onset: 35-45 yr
10/3/2016. T1 Anatomical structures are clearly identified, white matter (which has a high fat content) appears bright.
 appears bright.") H2O -2 atoms of Hydrogen, 1 of Oxygen Hydrogen just has one single proton and orbited by one single electron Proton has a magnetic moment similar to the earths magnetic pole Also similar to earth in that
H2O -2 atoms of Hydrogen, 1 of Oxygen Hydrogen just has one single proton and orbited by one single electron Proton has a magnetic moment similar to the earths magnetic pole Also similar to earth in that
SELECTIVE VULNERABILITY (HYPOXIA AND HYPOGLYCEMIA)
") DEFICIENCY OF METABOLITE -HYPOXIA AND HYPOGLYCEMIA -HYPOVITAMINOSIS SELECTIVE VULNERABILITY (HYPOXIA AND HYPOGLYCEMIA) -SPECIFIC CELL TYPE NEURONS>OLIGODENDROCYTES>ASTROCYTES -SPECIFIC BRAIN REGION PYRAMIDAL
DEFICIENCY OF METABOLITE -HYPOXIA AND HYPOGLYCEMIA -HYPOVITAMINOSIS SELECTIVE VULNERABILITY (HYPOXIA AND HYPOGLYCEMIA) -SPECIFIC CELL TYPE NEURONS>OLIGODENDROCYTES>ASTROCYTES -SPECIFIC BRAIN REGION PYRAMIDAL
Martin A. Samuels, M.D. MOVEMENT DISORDERS
 Martin A. Samuels, M.D. MOVEMENT DISORDERS I. Nomenclature of Movement Disorders A. Too Little Movement 1. Paralysis (paresis) 2. Rigidity a. spasticity (pyramidal) b. "lead pipe" (extra pyramidal) c.
Martin A. Samuels, M.D. MOVEMENT DISORDERS I. Nomenclature of Movement Disorders A. Too Little Movement 1. Paralysis (paresis) 2. Rigidity a. spasticity (pyramidal) b. "lead pipe" (extra pyramidal) c.
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014
 Spring, 2014") UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 11 th edition 2006 Eman Al-Khateeb,
UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY NEUROPHYSIOLOGY (MEDICAL) Spring, 2014 Textbook of Medical Physiology by: Guyton & Hall, 11 th edition 2006 Eman Al-Khateeb,
HOW NUTRITION CHANGES THE AGING BRAIN. Nafisa Jadavji, PhD
 HOW NUTRITION CHANGES THE AGING BRAIN Nafisa Jadavji, PhD NafisaJadavji@carleton.ca Lecture Outline Introduction Brain Nutrition Peer Review Questions BREAK Dementia and Alzheimer's disease Parkinson s
HOW NUTRITION CHANGES THE AGING BRAIN Nafisa Jadavji, PhD NafisaJadavji@carleton.ca Lecture Outline Introduction Brain Nutrition Peer Review Questions BREAK Dementia and Alzheimer's disease Parkinson s
Allied and Therapeutic Extender Benefit
 Allied and Therapeutic Extender Benefit 2012 Allied and Therapeutic Extender Benefit The Allied and Therapeutic Extender Benefit is available on the Executive and Comprehensive Plans only. Overview This
Allied and Therapeutic Extender Benefit 2012 Allied and Therapeutic Extender Benefit The Allied and Therapeutic Extender Benefit is available on the Executive and Comprehensive Plans only. Overview This
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Decreased Acetylcholine in the Basal Forebrain: Insight to the Neurocognitive Deficits in the Subarachnoid Hemorrhage Patient
 Decreased Acetylcholine in the Basal Forebrain: Insight to the Neurocognitive Deficits in the Subarachnoid Hemorrhage Patient Erol Veznedaroglu, MD Department of Neurosurgery/Division of Cerebrovascular
Decreased Acetylcholine in the Basal Forebrain: Insight to the Neurocognitive Deficits in the Subarachnoid Hemorrhage Patient Erol Veznedaroglu, MD Department of Neurosurgery/Division of Cerebrovascular
Basal ganglia motor circuit
 Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition
Parkinson s Disease Basal ganglia motor circuit 1 Direct pathway (gas pedal) 2 Indirect pathway (brake) To release or augment the tonic inhibition of GPi on thalamus Direct pathway There is a tonic inhibition