Where Have we Come From, and Where are we Going
|
|
|
- Georgina Casey
- 5 years ago
- Views:
Transcription
1 Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency Medicine
2 No Disclosures
3 Define the changing nature of trauma patients, based on national data sources Use trending data to suggest methods to improve systems for trauma preparedness, and how the military system of best trauma care will be integrated into the civilian practice Define changes in the care of trauma patient management that will impact outcomes Suggest needed changes in programs for trauma prevention, and designing performance measures
4 What should be No unexpected trauma deaths Effective systems of prevention Source: Zero Preventable Deaths Military trauma system program documents
5 What is: Preventable deaths occur, with uncoordinated trauma prevention programs Overutilization of immobilization, and subsequent complications Source: NHAMCS data reports since National Trauma Data Bank Current trauma literature
6 What interventions are indicated Organized systems of care Joint Trauma System models in the military, applied in civilian system Improved education on trauma care for prehospital and ED providers Coordinated prevention programs Public education Stop the Bleed campaign

7 Traffic fatality estimates released by the National Safety Council, a nonprofit organization that works closely with federal auto-safety regulators 40,200 people died in accidents involving motor vehicles in 2016, a 6 percent rise from the year before First time since 2007 that more than 40,000 people have died in motor vehicle accidents in a single year 2016 total comes after a 7 percent rise in 2015 Means the two-year increase 14 percent is the largest in more than a half a century

8


9 Emergency Patients Keep Coming Estimates

10 General Population EMS Emergency Department Walk-ins to ED 371 / 1000 Population 80/1000 Population Total use 451 / 1000 Population 82% Walk-Ins 17% Arrival by EMS Transfer 2% Admit 17% Treat & Release 81% LBTC 2%

11
12 Leading cause of death age For all age groups together, it is third behind cancer and atherosclerosis. Leading cause of Years of Productive Life Lost (YPLL), meaning that young active people are most frequent victims. Motor vehicle crash fatalities in 2011 were 32,367. (lowest death toll since 1949). All forms accidental death decreasing, esp work-related Cost of death and disability is over $671B in 2013 Prevention Works! And why our health system gets more expensive
13
14
15 Year % of Patients age % of Patients over 75 Injury Visits per 1000 population age Injury Visits per 1000 population over age % 7%
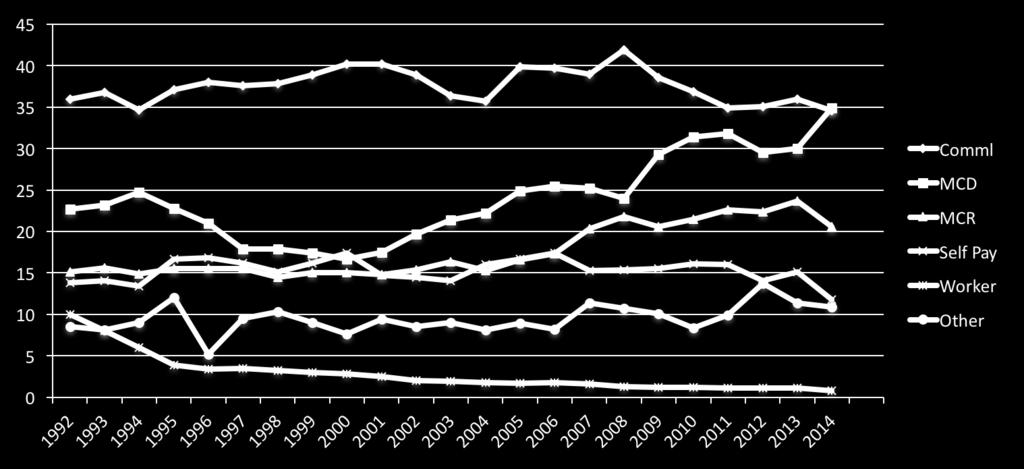
16 Payor % of ED Visits, 2014 % of Trauma Patients in NTDB Commercial 34.6% 35.1% Medicaid, CHIP 34.9% 16.3% Medicare 16% 27% Self Pay 12% 11.3% Worker Comp 0.8% 1%
17

18 A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths after Injury in the Joint Trauma System models in the military, applied in civilian system C William Schwab, MD Scudder Oration delivered at the ACS Clinical Congress 2014 Improve education on trauma care for prehospital and ED providers Coordinated prevention programs Improve public education Stop the Bleed campaign

19 The Changing Face of MCIs The New Priorities of Trauma MCIs
20 Still Anything, Anytime, Anywhere, Any Number Care Options are changing Equipment is Changing Rapidly
21

22 Military and Civilian Applications of Techniques and Tools Senior Trauma Sports Injuries and High Profile Care Packaging Ways to Stop Bleeding Preventing Late Complications

23 Rapid response and extrication, integrating new technologies for locating incidents, and predicting severity, integrating visuals Prevent additional injury and initiate therapy in a timely manner Rapid transport to an appropriate receiving facility, giving advance notification to the medical personnel in that facility No field categorization system has yet been developed to precisely predict which patient needs which level of trauma center Especially with older patients
24 Response Capabilities for MCIs Active Shooter Protocols Appropriate use of Helicopters Widespread use of Tourniquets Selective use of Spinal Motion Restriction
25 Prevent Cold, Acidotic, Coagulopathic Permissive Hypotension along with prevention of Hypothermia Medications Tranexamic Acid, a clot stabilizer Progesterone as a neuro protective agent for Traumatic Brain Injuries

26 On thinners Pre-existing conditions Did primary medical event cause trauma? Package poorly using current tools Develop complications easily Usual markers of shock are missing
27 The Changing Face of MCIs The Old Image of Trauma MCIs Newer Versions
28 Cervical Immobilization versus Spine Immobilization Pelvic Binders Fluid Warmers, Fluid Coolers Dressings Opsite, Tegaderm
29 Military versus Civilian Applications Disaster vs. Day to Day Adult, Pediatric, Geriatric, Special Needs
30 ABCs Selective Spinal Motion Restriction Airway, Breathing Circulation (Warm) IV s where needed (Above and below diaphragm)

31
32 What Effect w or w/o Helicopter Telemedicine What Hospital will Treat Him? Hospital Response In-House Hospital Response to the scene Trauma Centers are Reappearing
33 Airways Different then Cardiac Arrest Tourniquets Length of Needles for Chest Decompress IO Apparatus DARPA Foam
34 Sum of responses at organ and cellular level which reflect Inadequate perfusion (The P Word) Serum Lactate helps evaluate Pulse Oximeter best existing tool End Tidal CO2 may help evaluate
35 Maintain or restore basic Perfusion Monitor patient continually to determine response to therapy and ongoing fluid needs Don t infuse cold fluids Damage Control Resuscitation Endovascular control

36 Gross hemorrhage controlled with direct pressure or pressure cuff, then tourniquet Trauma Dressings Skin Dressings Opsite, Tegaderm Elderly Skin Tear Dressings
37 Tranexemic Acid Progesterone for TBI Pulse Oximeter as a Perfusion Meter ETCO2 for Head Trauma
38 Preserve Life Preserve Limb Tourniquet
39 Synthetic derivative of the amino acid lysine Potent pro-hemostatic drug that stops fibrin degradation Prevents clot breakdown Drug reduces the need for blood transfusion in surgery pts CRASH-2 trial showed TXA given early after trauma saves lives
40 U.S. military already gives TXA to soldiers with severe bleeding and includes TXA acid in its protocol for combat casualties Greatest benefit was seen when TXA was administered within 1 hour of injury TXA has been approved by the FDA for use in hemophiliacs undergoing dental work and for menorrhagia NOT specifically FDA approved for hemorrhage in trauma patients Approximately $200 for treatment
41 Immobilization for movement Packaging, different for C Spine versus total spine Safe Airway and Breathing Circulation assessment and care Don t Create New Wounds
42 Haddon s Matrix Response Initial Rescue Definitive Care Rehabilitation
43 Military versus Civilian Applications Tourniquets, Pelvic Binders Packaging of Trauma Patients and Trauma Dressings IO Apparatus Disaster Products, Victim Tracking DARPA Foam Hospital Response In-House Fluid Warmers, Fluid Coolers Tranexemic Acid, Progesterone Virtual Presence and Telemedicine ETCO2 for Head Trauma Pulse Oximeter as a Perfusion Meter Airways Different then Cardiac Arrest Cervical Immobilization versus Spine Immobilization Balloon Catheters and other Endovascular Applications
44 The Challenges of Change Congratulations on Successes in Prevention That is our Future
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Prehospital Hemorrhage Control
 Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Burnt and Blasted: How to Manage Common Injuries from a Galaxy Far, Far Away. Concepts From the Conflicts: New Advances in Trauma Care
 Burnt and Blasted: How to Manage Common Injuries from a Galaxy Far, Far Away WE - 204/ 0.5 Hour(s) Faculty: Jacob Avila, MD This session will cover how to manage injuries on earth or in a galaxy far, far
Burnt and Blasted: How to Manage Common Injuries from a Galaxy Far, Far Away WE - 204/ 0.5 Hour(s) Faculty: Jacob Avila, MD This session will cover how to manage injuries on earth or in a galaxy far, far
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG. TargetSolutions. Technology with a Purpose
 EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG 1 Technology with a Purpose TargetSolutions delivers employee training that helps organizations achieve compliance, mitigate We risk, believe reduce a well-trained
EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG 1 Technology with a Purpose TargetSolutions delivers employee training that helps organizations achieve compliance, mitigate We risk, believe reduce a well-trained
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
MEMORANDUM Date: To: From: Subject:
 COUNTY OF EL DORADO HEALTH & HUMAN SERVICES BOARD OF SUPERVISORS Director Chris Weston Program Manager II 931 Spring Street Placerville, CA 95667 530-621-6100 Phone / 530-295-2501 Fax 1360 Johnson Boulevard,
COUNTY OF EL DORADO HEALTH & HUMAN SERVICES BOARD OF SUPERVISORS Director Chris Weston Program Manager II 931 Spring Street Placerville, CA 95667 530-621-6100 Phone / 530-295-2501 Fax 1360 Johnson Boulevard,
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject Emergency Medical Services Administrative Policies and Procedures Table of Contents
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject Emergency Medical Services Administrative Policies and Procedures Table of Contents
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
TEXT - Emergency Care by Brady, 13th edition&
 BASIC EMT Spring 2019& SUNY Canton, CREST Building& Monday & Wednesday 6:30-9:30 p.m.& Saturday 9 a.m. 12 noon & 1 4 p.m.& Instructor: Donald Thompson, CIC& TEXT - Emergency Care by Brady, 13th edition&
BASIC EMT Spring 2019& SUNY Canton, CREST Building& Monday & Wednesday 6:30-9:30 p.m.& Saturday 9 a.m. 12 noon & 1 4 p.m.& Instructor: Donald Thompson, CIC& TEXT - Emergency Care by Brady, 13th edition&
Hypotension / Shock. Adult Medical Section Protocols. Protocol 30
 Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
The new standard in hemorrhage control
 The new standard in hemorrhage control Contents The need for hemostats What is Celox Rapid? Benefits How it works Performance Independent trials of Celox Gauze The need for hemostats in trauma Combat lives
The new standard in hemorrhage control Contents The need for hemostats What is Celox Rapid? Benefits How it works Performance Independent trials of Celox Gauze The need for hemostats in trauma Combat lives
TRAUMA PATIENT ASSESSMENT
 SECTION: Adult Trauma Emergencies PROTOCOL TITLE: Injury General Trauma Management REVISED: 06/2015 OVERVIEW Each year, one out of three Americans sustains a traumatic injury. Trauma is a major cause of
SECTION: Adult Trauma Emergencies PROTOCOL TITLE: Injury General Trauma Management REVISED: 06/2015 OVERVIEW Each year, one out of three Americans sustains a traumatic injury. Trauma is a major cause of
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Pre-Hospital Critical Care June 2016
 Pre-Hospital Critical Care June 2016 Mark J G Dunn Consultant in Critical Care, Emergency Medicine and Retrieval Medicine The Royal Infirmary of Edinburgh Emergency Medical Retrieval Service, ScotSTAR,
Pre-Hospital Critical Care June 2016 Mark J G Dunn Consultant in Critical Care, Emergency Medicine and Retrieval Medicine The Royal Infirmary of Edinburgh Emergency Medical Retrieval Service, ScotSTAR,
BASIC EMT Fall 2015 SUNY Canton, Wicks Hall 102 Monday & Wednesday 6:30-9:30 p.m. Saturday 9 a.m. 12 noon & 1 4 p.m. Instructor: Chris Miller
 BASIC EMT Fall 2015 SUNY Canton, Wicks Hall 102 Monday & Wednesday 6:30-9:30 p.m. Saturday 9 a.m. 12 noon & 1 4 p.m. Instructor: Chris Miller TEXT - Emergency Care by Brady, 12th edition PLEASE NOTE: Starting
BASIC EMT Fall 2015 SUNY Canton, Wicks Hall 102 Monday & Wednesday 6:30-9:30 p.m. Saturday 9 a.m. 12 noon & 1 4 p.m. Instructor: Chris Miller TEXT - Emergency Care by Brady, 12th edition PLEASE NOTE: Starting
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
HYPOTHERMIA IN TRAUMA. Kevin Palmer EMT-P, DiMM
 HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
Firefighter Pre Hospital Care Program Module 25. Triage
 Firefighter Pre Hospital Care Program Module 25 Triage Firefighter Pre Hospital Care Program Module 25 At the end of the lesson and upon completion of the FETN post test quiz, the participant will demonstrate
Firefighter Pre Hospital Care Program Module 25 Triage Firefighter Pre Hospital Care Program Module 25 At the end of the lesson and upon completion of the FETN post test quiz, the participant will demonstrate
HOW TO START ASSALTING YOUR TRIAGE SCHEMES - SORTING THE DIFFERENT TRIAGE SCHEMES
 HOW TO START ASSALTING YOUR TRIAGE SCHEMES - SORTING THE DIFFERENT TRIAGE SCHEMES W. Scott Gilmore, MD, EMT-P, FACEP Medical Director, St. Louis Fire Department Disclosures I have no significant financial
HOW TO START ASSALTING YOUR TRIAGE SCHEMES - SORTING THE DIFFERENT TRIAGE SCHEMES W. Scott Gilmore, MD, EMT-P, FACEP Medical Director, St. Louis Fire Department Disclosures I have no significant financial
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY
 SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY PURPOSE: To identify those patients who are at greatest risk for severe injury and determine the most appropriate facility to transport persons with different
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY PURPOSE: To identify those patients who are at greatest risk for severe injury and determine the most appropriate facility to transport persons with different
Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions
 Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned
Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
EMS Resuscitations Centers: Bring in your Dead?
 EMS Resuscitations Centers: Bring in your Dead? C. Crawford Mechem, MD EMS Medical Director Philadelphia Fire Department Department of Emergency Medicine University of Pennsylvania School of Medicine I
EMS Resuscitations Centers: Bring in your Dead? C. Crawford Mechem, MD EMS Medical Director Philadelphia Fire Department Department of Emergency Medicine University of Pennsylvania School of Medicine I
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Competencies and Objectives
 Competencies and Objectives Chapter 1 EMS Systems Preparatory Emergency Medical Services (EMS) Systems Research Public Health Chapter 2 Workforce Safety and Wellness Medicine Infectious Diseases Preparatory
Competencies and Objectives Chapter 1 EMS Systems Preparatory Emergency Medical Services (EMS) Systems Research Public Health Chapter 2 Workforce Safety and Wellness Medicine Infectious Diseases Preparatory
REBOA new snake in the grass?
 REBOA new snake in the grass? Does it have a place in South Africa and other LMICs? Tim Hardcastle Trauma Surgeon IALCH/UKZN Controversies in Surgery 2016 History nothing new under the sun (Solomon = Ecclesiates)
REBOA new snake in the grass? Does it have a place in South Africa and other LMICs? Tim Hardcastle Trauma Surgeon IALCH/UKZN Controversies in Surgery 2016 History nothing new under the sun (Solomon = Ecclesiates)
Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES. Accidental Hypothermia/Cold Exposure
 Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES Accidental Hypothermia/Cold Exposure Goal: To aid EMS Providers in: the recognition and treatment of systemic effects of accidental hypothermia
Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES Accidental Hypothermia/Cold Exposure Goal: To aid EMS Providers in: the recognition and treatment of systemic effects of accidental hypothermia
HSE158 First Aid H.H. Sheik Sultan Tower (0) Floor Corniche Street Abu Dhabi U.A.E
 Floor Corniche Street Abu Dhabi U.A.E") HSE158 First Aid H.H. Sheik Sultan Tower (0) Floor Corniche Street Abu Dhabi U.A.E www.ictd.ae ictd@ictd.ae Course Introduction: The First Aid course is specifically designed for those individuals working
HSE158 First Aid H.H. Sheik Sultan Tower (0) Floor Corniche Street Abu Dhabi U.A.E www.ictd.ae ictd@ictd.ae Course Introduction: The First Aid course is specifically designed for those individuals working
ADMINISTRATIVE REQUIREMENT MANUAL EFFECTIVE DATE
 PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
5/30/2013. I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow. Trauma = #1 cause of death persons <40 yo 1
 I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA THE PREHOSPITAL APPROACH TO CHEST INJURY MANAGEMENT
 Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
Improving Rural Trauma Outcomes: Local Damage Control? R Simons, V Vogt Haines, K McCarroll. Enhanced Surgical Skills Program Banff, January 2018
 Improving Rural Trauma Outcomes: Local Damage Control? R Simons, V Vogt Haines, K McCarroll Enhanced Surgical Skills Program Banff, January 2018 Session Objectives Define problem of high injury mortality
Improving Rural Trauma Outcomes: Local Damage Control? R Simons, V Vogt Haines, K McCarroll Enhanced Surgical Skills Program Banff, January 2018 Session Objectives Define problem of high injury mortality
Stop the Bleed The White House Hemorrhage Control Initiative
 Stop the Bleed The White House Hemorrhage Control Initiative David M Sailors MD Asst Prof Surgery UGA/MCG Medical Partnership Team Physician UGA Athletic Association University of Georgia Athens Georgia
Stop the Bleed The White House Hemorrhage Control Initiative David M Sailors MD Asst Prof Surgery UGA/MCG Medical Partnership Team Physician UGA Athletic Association University of Georgia Athens Georgia
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY
 SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
PARAMEDIC RECERT PROPOSAL (NCCP standards)
") PARAMEDIC RECERT PROPOSAL (NCCP standards) Module I TOPIC Airway, Respiration, Ventilation and Neurotological Management Ventilation ETCO2 Automated Transport Ventilators Oxygenation CPAP Capnography Neurological
PARAMEDIC RECERT PROPOSAL (NCCP standards) Module I TOPIC Airway, Respiration, Ventilation and Neurotological Management Ventilation ETCO2 Automated Transport Ventilators Oxygenation CPAP Capnography Neurological
Disaster Triage START/JUMPSTART
 Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center AGENDA Attendance Ground Rules Presentation Scenarios Additional Resources Evaluation/Certificate Objectives: Define a Mass Casualty
Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center AGENDA Attendance Ground Rules Presentation Scenarios Additional Resources Evaluation/Certificate Objectives: Define a Mass Casualty
2007 NATIONAL EMS SCOPE OF PRACTICE MODEL CHANGE NOTICES. Change Notice 1.0
 2007 NATIONAL EMS SCOPE OF PRACTICE MODEL CHANGE NOTICES November 1, 2017 Change Notice 1.0 The following changes to the National EMS Scope of Practice Model (February 2007) DOT HS 810 657 are effective
2007 NATIONAL EMS SCOPE OF PRACTICE MODEL CHANGE NOTICES November 1, 2017 Change Notice 1.0 The following changes to the National EMS Scope of Practice Model (February 2007) DOT HS 810 657 are effective
Course Description Theory and Skills of immediate life saving care. Meets the requirements for certification as an Emergency Care Attendant (ECA).
.") Emergency Care Attendant (EMSP 1305) Credit: 3 semester credit hours (3 hours lecture, 0 hours lab) Prerequisite/Co-requisite: Must be at least 17 and be at least a senior in high school. Course Description
Emergency Care Attendant (EMSP 1305) Credit: 3 semester credit hours (3 hours lecture, 0 hours lab) Prerequisite/Co-requisite: Must be at least 17 and be at least a senior in high school. Course Description
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
CLINICAL MANUAL. Trauma System Activation Trauma Code Criteria
 CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
M.A.R.C.H. M.A.R.C.H. 10/11/2017. Hartford Consensus 2 April Comparison of Statistics for Battle Casualties,
 Presented by: Envision/EM Care 15 th Annual Advanced Emergency and Acute Care Medicine Conference Stop the Bleed EAST COAST TACTICAL MEDICINE Dr. A. Scott Whyte Danny Devlin Emergency Physician Level II
Presented by: Envision/EM Care 15 th Annual Advanced Emergency and Acute Care Medicine Conference Stop the Bleed EAST COAST TACTICAL MEDICINE Dr. A. Scott Whyte Danny Devlin Emergency Physician Level II
itclamp 50 Clinical Training M-115-CE Rev C
 itclamp 50 Clinical Training M-115-CE Rev C Objectives Explain the impact of bleeding in trauma Recognize the importance of rapid haemorrhage control Classify wounds on the spectrum of bleeding Select
itclamp 50 Clinical Training M-115-CE Rev C Objectives Explain the impact of bleeding in trauma Recognize the importance of rapid haemorrhage control Classify wounds on the spectrum of bleeding Select
The Mangled Extremity: Best Practice for Optimal Outcomes. Kristen Ray R.N., MSN
 The Mangled Extremity: Best Practice for Optimal Outcomes Kristen Ray R.N., MSN Learning Objectives At the end of the session, participants will be able to: Verbalize the initial management principles
The Mangled Extremity: Best Practice for Optimal Outcomes Kristen Ray R.N., MSN Learning Objectives At the end of the session, participants will be able to: Verbalize the initial management principles
Subject Ch Hours Date Preparatory Intro to Course 4 9/4. Safety and Wellness 2 2 9/11 Public Health 3 2. Medical, Legal and Ethical Issues 4 4 9/13
 Subject Ch Hours Date Preparatory Intro to Course 4 9/4 Intro to Course (continued) 2 9/6 EMS Systems 1 2 Safety and Wellness 2 2 9/11 Public Health 3 2 Medical, Legal and Ethical Issues 4 4 9/13 Medical,
Subject Ch Hours Date Preparatory Intro to Course 4 9/4 Intro to Course (continued) 2 9/6 EMS Systems 1 2 Safety and Wellness 2 2 9/11 Public Health 3 2 Medical, Legal and Ethical Issues 4 4 9/13 Medical,
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Civilian versus Military Trauma Management
 Western University From the SelectedWorks of Vivian C. McAlister November, 2010 Civilian versus Military Trauma Management Vivian C. McAlister Available at: https://works.bepress.com/vivianmcalister/151/
Western University From the SelectedWorks of Vivian C. McAlister November, 2010 Civilian versus Military Trauma Management Vivian C. McAlister Available at: https://works.bepress.com/vivianmcalister/151/
1/16/2014 NONE WILL BE TALKING ABOUT NON FDA APPROVED DRUGS WILL LET YOU KNOW WHEN NOT ENDORSING ANY PARTICULAR PIECE OF EQUIPMENT
 CUTTING EDGE TACTICAL MEDICINE SECRETS FROM THE BATTLEFIELD Brendan Anzalone, DO, Maj, USAF, MC Emergency Physician Special Tactics Medicine USAF Special Operations Surgical/Critical Care Evacuation Team
CUTTING EDGE TACTICAL MEDICINE SECRETS FROM THE BATTLEFIELD Brendan Anzalone, DO, Maj, USAF, MC Emergency Physician Special Tactics Medicine USAF Special Operations Surgical/Critical Care Evacuation Team
Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine
 Running on Empty Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine Nationwide id Children s Hospital Associate Professor, Department of Pediatrics The Ohio State
Running on Empty Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine Nationwide id Children s Hospital Associate Professor, Department of Pediatrics The Ohio State
DATE TOPIC INSTRUCTOR. MODULE I Preparatory. 08/21/ MILLER Course Overview (books, paperwork, etc.)
") Autumn 2018 EMT (Evening Class) August 21, 2018 December 15, 2018 Emergency Medical Technician Tuesdays & Thursdays 1800 2200 3-Wednesdays 1800 2200 as scheduled 2-Saturdays 0800 1700 as scheduled DATE
Autumn 2018 EMT (Evening Class) August 21, 2018 December 15, 2018 Emergency Medical Technician Tuesdays & Thursdays 1800 2200 3-Wednesdays 1800 2200 as scheduled 2-Saturdays 0800 1700 as scheduled DATE
Trauma Alert Step 2 Additions
 Trauma Alert Step 2 Additions MANGLED, DEGLOVED OR PULSELESS EXTREMITY PELVIC INJURY WITH HIGH-RISK MECHANISM OF INJURY Many thanks to Paramedic FTO Justin Bramlette for assembling this training presentation
Trauma Alert Step 2 Additions MANGLED, DEGLOVED OR PULSELESS EXTREMITY PELVIC INJURY WITH HIGH-RISK MECHANISM OF INJURY Many thanks to Paramedic FTO Justin Bramlette for assembling this training presentation
VA OEMS Approved TargetSolutions Together with CentreLearn Course Listing
 Please view the following list of VA OEMS approved courses. The area numbers per each level of certification are listed below. Any course that you take that is not on this list will not count for VA OEMS
Please view the following list of VA OEMS approved courses. The area numbers per each level of certification are listed below. Any course that you take that is not on this list will not count for VA OEMS
Pediatric Trauma Practice. Guideline for Management of the Child in Shock. Background
 Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Injury caused by an object breaking the skin and entering the body. immediate intervention to repair internal
 1 Chapter 16: Trauma & Trauma Systems 2 Trauma Leading killer of persons under in US. -150,000 Deaths annually -44,000 MVC -28,000 GSW Most medical problem in terms of lost wages, initial care, rehabilitation,
1 Chapter 16: Trauma & Trauma Systems 2 Trauma Leading killer of persons under in US. -150,000 Deaths annually -44,000 MVC -28,000 GSW Most medical problem in terms of lost wages, initial care, rehabilitation,
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD
 ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Implementation and execution of civilian RDCR programs Minnesota RDCR
 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 406 Manage Shock Casualties TERMINAL LEARNING OBJECTIVES 1. Given a casualty in an operational environment,
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 406 Manage Shock Casualties TERMINAL LEARNING OBJECTIVES 1. Given a casualty in an operational environment,
Training Surgeons for Disasters
 SURGICAL RESPONSE TO DISASTERS Training Surgeons for Disasters M. Margaret Knudson MD, FACS Chief of Surgery, San Francisco General Hospital and Trauma Center A MASS CASUALTY EVENT IS NOT JUST ANOTHER
SURGICAL RESPONSE TO DISASTERS Training Surgeons for Disasters M. Margaret Knudson MD, FACS Chief of Surgery, San Francisco General Hospital and Trauma Center A MASS CASUALTY EVENT IS NOT JUST ANOTHER
Emergency Medical Technician Common Course Outline
 Emergency Medical Technician Common Course Outline Course Information Organization South Central College Revision History 2008-2009 Course Number HEMS1200 Department EMS Total Credits 6 Description This
Emergency Medical Technician Common Course Outline Course Information Organization South Central College Revision History 2008-2009 Course Number HEMS1200 Department EMS Total Credits 6 Description This
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Mesa County EMS Protocol Test 2016
 Mesa County EMS Protocol Test 2016 1. Which of the following is incorrect? a. Each EMS and Fire agency should have protocols in place for evaluation of personnel involved in fire suppression operations
Mesa County EMS Protocol Test 2016 1. Which of the following is incorrect? a. Each EMS and Fire agency should have protocols in place for evaluation of personnel involved in fire suppression operations
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
9/15/2015. Introduction (1 of 3) Chapter 8. Introduction (2 of 3) What is the difference? Scene Size-up (1 of 2) Patient Assessment
 Chapter 8. Introduction (2 of 3) What is the difference? Scene Size-up (1 of 2) Patient Assessment") Introduction (1 of 3) Chapter 8 Patient Assessment Patient assessment is very important. EMTs must master the patient assessment process. Patient assessment is used, to some degree, in every patient encounter.
Introduction (1 of 3) Chapter 8 Patient Assessment Patient assessment is very important. EMTs must master the patient assessment process. Patient assessment is used, to some degree, in every patient encounter.
Traumatic Cardiac Arrest Protocol
 Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
Old protocol is top bullet and italicized. Revised protocol is subsequent bullets and color coded:
 Old protocol is top bullet and italicized Revised protocol is subsequent bullets and color coded: RED is a State Change Blue is unique to Suffolk County VI. If patient has not taken aspirin and has no
Old protocol is top bullet and italicized Revised protocol is subsequent bullets and color coded: RED is a State Change Blue is unique to Suffolk County VI. If patient has not taken aspirin and has no
Disaster Triage START/JUMPSTART. Objectives: What is the Goal of MCI Management?
 Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center Objectives: Define a Mass Casualty Incident and the unique challenges of an MCI Understand the differences between dayto-day triage
Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center Objectives: Define a Mass Casualty Incident and the unique challenges of an MCI Understand the differences between dayto-day triage
6. Knowledge and Skill Comparison (Paramedic)
") 6. Knowledge and Skill Comparison (Paramedic) The order of content is not meant to imply the order of delivery. a. Paramedic: New Course Considerations When planning and conducting a new Paramedic course,
6. Knowledge and Skill Comparison (Paramedic) The order of content is not meant to imply the order of delivery. a. Paramedic: New Course Considerations When planning and conducting a new Paramedic course,
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
UPDATE IN TRAUMA ANESTHESIA ARANA Spring Meeting May 5th, 2017 Joe Romero CRNA, MS, CPT USAR
 UPDATE IN TRAUMA ANESTHESIA 2018 ARANA Spring Meeting May 5th, 2017 Joe Romero CRNA, MS, CPT USAR UPDATE IN TRAUMA ANESTHESIA 2018 - An overview of trauma demographics, mechanisms, and current literature
UPDATE IN TRAUMA ANESTHESIA 2018 ARANA Spring Meeting May 5th, 2017 Joe Romero CRNA, MS, CPT USAR UPDATE IN TRAUMA ANESTHESIA 2018 - An overview of trauma demographics, mechanisms, and current literature
Combined CFRN and CTRN Detailed Content Outline
 Clinical items (primarily category, Assessment (15-20%), 1. General principles of transport nursing practice 19 31 A. Transport physiology 1. Physiologic stressors of transport 2. Effects of altitude on
Clinical items (primarily category, Assessment (15-20%), 1. General principles of transport nursing practice 19 31 A. Transport physiology 1. Physiologic stressors of transport 2. Effects of altitude on
Sierra Sacramento Valley EMS Agency Policy/Protocol Manual Table of Contents
 SECTION 100 STATE LAW AND REGULATION 100 Index 101 California Health And Safety Code, Division 2.5 Emergency Medical Services 102 California Code Of Regulations, Title 22, Division 9 SECTION 200 LEMSA
SECTION 100 STATE LAW AND REGULATION 100 Index 101 California Health And Safety Code, Division 2.5 Emergency Medical Services 102 California Code Of Regulations, Title 22, Division 9 SECTION 200 LEMSA
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
11/1/2014. Just The. Pearls. Everything I do is Off-Label! This is the ultimate lecture for the ADHD emergency physician.
 Just The Everything I do is Off-Label! Pearls This is the ultimate lecture for the ADHD emergency physician. 1 >20 Tips in 60 Minutes You re repeatin yourself ½ Trauma ½ Medical Arrest Crit Care in The
Just The Everything I do is Off-Label! Pearls This is the ultimate lecture for the ADHD emergency physician. 1 >20 Tips in 60 Minutes You re repeatin yourself ½ Trauma ½ Medical Arrest Crit Care in The
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Expert Group Meeting-Trauma
 Why was Trauma Summit needed? There are no clear guidelines/algorithms to assist acute management of trauma patients in the Indian setting. One of our visions is to assist young doctors in acute care medicine
Why was Trauma Summit needed? There are no clear guidelines/algorithms to assist acute management of trauma patients in the Indian setting. One of our visions is to assist young doctors in acute care medicine
Emergency Preservation and Resuscitation
 Emergency Preservation and Resuscitation Samuel A. Tisherman, MD, FACS, FCCM Director, Center for Critical Care and Trauma Education Director, SICU RA Cowley Shock Trauma Center Disclosures Co-author of
Emergency Preservation and Resuscitation Samuel A. Tisherman, MD, FACS, FCCM Director, Center for Critical Care and Trauma Education Director, SICU RA Cowley Shock Trauma Center Disclosures Co-author of
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
JUNCTIONAL STAB WOUND SAVING THE UN-SAVABLE
 JUNCTIONAL STAB WOUND SAVING THE UN-SAVABLE MARVIN WAYNE, MD, FACEP, FAAEM, FAHA ASSOCIATE CLINICAL PROF. DEPT. OF EM, UNIVERISTY OF WASHINGTON EMS MEDICAL DIRECTOR WHATCOM COUNTY WA EMERGENCY DEPT. PEACEHEALTH
JUNCTIONAL STAB WOUND SAVING THE UN-SAVABLE MARVIN WAYNE, MD, FACEP, FAAEM, FAHA ASSOCIATE CLINICAL PROF. DEPT. OF EM, UNIVERISTY OF WASHINGTON EMS MEDICAL DIRECTOR WHATCOM COUNTY WA EMERGENCY DEPT. PEACEHEALTH
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
PEDIATRIC MASSIVE TRANSFUSION
 PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss