M.A.R.C.H. M.A.R.C.H. 10/11/2017. Hartford Consensus 2 April Comparison of Statistics for Battle Casualties,
|
|
|
- Dwain Norman
- 5 years ago
- Views:
Transcription


1 Presented by: Envision/EM Care 15 th Annual Advanced Emergency and Acute Care Medicine Conference Stop the Bleed EAST COAST TACTICAL MEDICINE Dr. A. Scott Whyte Danny Devlin Emergency Physician Level II Trauma Center Tactical Physician SWAT TCCC/TECC Instructor ACLS/PALS Instructor ATLS Provider (former instructor) EMT Instructor High School Girls Ice Hockey Coach US Army Special Forces Assistant Detachment Commander US Army Ranger Qualified Special Forces Advanced Urban Combat Instructor TCCC/TECC Provider BCON Instructor Evanna Burgwardt BSN, RN, CCRN Emergency Nurse, Level II Trauma Center Cardiac Intensive Care Unit Nurse ACLS/PALS Provider ABLS Provider TCCC Provider BCON Instructor Lawrence Smira US Navy Hospital Corpsman Fleet Marine Force Corpsman Combat Life Saver Instructor EMT TCCC Provider TECC/ BLS Instructor 1
 Why is it important and why should Ilearn this?")


2 OBJECTIVES Case Studies Data Review Bleeding Control Hands On Tourniquet Application Pressure Dressings Hemostatic Dressings Non-Compressible Bleeding Certify Participants B-Con Providers Bleeding Control (B-Con) Why is it important and why should Ilearn this? Boston Marathon bombings April 15, 2013 According to the Boston Public Health Commision: 264 people treated at 27 local hospitals 16people lost limbs at the scene or at the hospital 3lost more than 1limb Many had lower limb injuries and shrapnel from explosive devices low to the ground Charlie Hebdo shooting January 7, Fatalities 11 Wounded All injuries by penetrating by 7.62x39 AK-47 rounds. Penetrating wounds to arms, legs and chest reported. Columbine High School April 20, Deaths 24 Wounding's 21 by gunshots 9mm Pistol rounds, 9mm carbine rounds and 12 gauge shotgun. IED s brought by perpetrators never used. Why should Ilearn this? The life you save may be your own! At the end of the day you owe it to yourself, your family, your partner and those that care for and about you to make it home safely! TCCC is the current training based on this learning. Bleeding Control has proven to save lives. 2

3 Hartford Consensus 2 April 2013 Working group organized by American College of Surgeons Board of Regents and FBI In response to Sandy Hook shootings Excerpt from findings: M.A.R.C.H. Massive hemorrhage control life-threatening bleeding. Airway establish and maintain a patent airway. Respiration decompress suspected tension pneumothorax, seal open chest wounds, and support ventilation/oxygenation as required. M.A.R.C.H. Circulation establish IV/IO access and administer fluids as required to treat shock. Head injury/hypothermia prevent/treat hypotension and hypoxia to prevent worsening of traumatic brain injury and prevent/treat hypothermia. Comparison of Statistics for Battle Casualties, Holcomb et al J Trauma 2006 The U.S. casualty survival rate in Iraq and Afghanistan has been the best in U.S. history. World War II Vietnam OIF/OEF CFR 19.1% 15.8% 9.4% Note: CFR is the Case Fatality Rate the percent of those wounded who die Potentially Preventable Deaths (232) in OIF and OEF (Data based on the Wound Data Munitions Effectiveness Team (WDMET) during the Vietnam War between 1967 and 1969) CNS 9% MSOF 4% Airway 14% NEXT Hemorrhage 85% 31% Compressible (prehospital target) 69% Non-Compressible (FST/CSH target) From evaluation of 982 casualties, and casualties could have more than 1 cause of death. (Kelly J., J Trauma 64:S21, 2008) 3
![U.S. Combat Fatalities: Death from Hemorrhage Extremity [119/888] = 13.5% Junctional [171/888] = 19.2% Truncal [598/888] = 67.](/docs-images/82/85447584/images/4-0.jpg "3% Tourniquets in WWII Wolff AMEDD J April 1945 We believe that the strap-and-buckle tourniquet in common use is ineffective in most instances under field conditions")
: implications for the future of combat casualty care. Journal of Trauma 2012, 73(6) Suppl 5: 431-7.")


4 U.S. Combat Fatalities: Death from Hemorrhage Extremity [119/888] = 13.5% Junctional [171/888] = 19.2% Truncal [598/888] = 67.3% Tourniquets in WWII Wolff AMEDD J April 1945 We believe that the strap-and-buckle tourniquet in common use is ineffective in most instances under field conditions it rarely controls bleeding no matter how tightly applied. Eastridge BJ, Mabry RL, Seguin PG, et al. Death on the battlefield ( ): implications for the future of combat casualty care. Journal of Trauma 2012, 73(6) Suppl 5: Vietnam Over 2500 deaths occurred in Vietnam secondary to hemorrhage from extremity wounds. These casualties had no other injuries. Tourniquets in U.S Military Mid-1990s Old strap-and-buckle tourniquets were still being issued. Medics and corpsmen were being trained in courses where they were taught notto use them. Tourniquets Beekley et al Journal of Trauma st CSH in casualties with severe extremity trauma 67 with prehospital tourniquets; 98 without Seven deaths Four of the seven deaths were potentially preventable had an adequate prehospital tourniquet been placed Eliminating Preventable Death on the Battlefield TCCC in the 75 th Ranger Regiment AllRangers and docs trained in TCCC Ranger preventable death incidence: 3% Overall U.S. military preventable deaths: 24% 4




5 Danny Devlin US Army Special Forces Assistant Detachment Commander US Army Ranger Qualified Special Forces Advanced Urban Combat Instructor TCCC/TECC Provider BCON Instructor 5


6 6

7 7
8 8




9 Lawrence Smira US Navy Hospital Corpsman Fleet Marine Force Corpsman Combat Life Saver Instructor EMT TCCC Provider TECC/ BLS Instructor 9

10 10
11 11




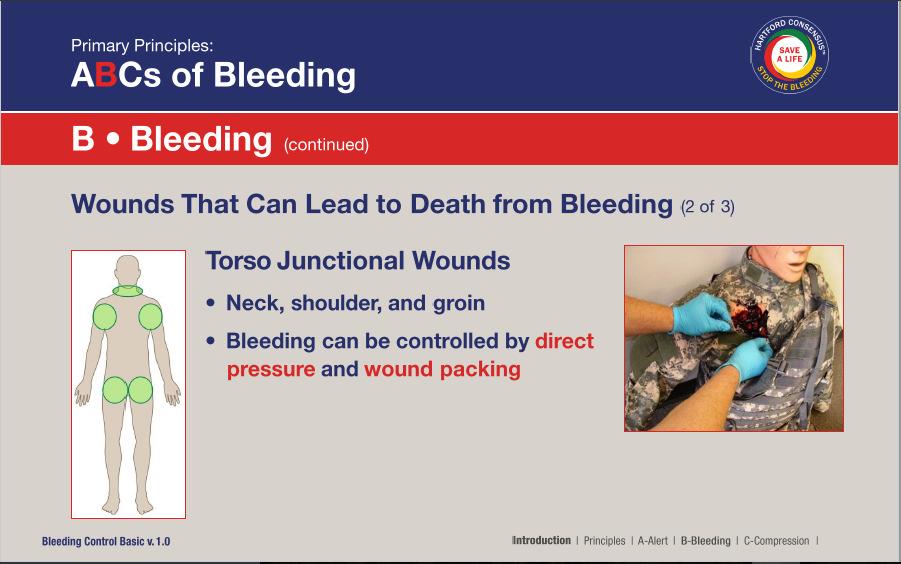
12 JunctionalHemorrhage Junctional hemorrhage includes hemorrhage in the following areas: Groin Buttocks Perineum Axilla Base of neck Junctional Hemorrhage Wounds That May Result in Junctional Hemorrhage Groin hemorrhage is the most common type of junctional bleeding where regular tourniquets cannot work. Kelly JF, et al. J Trauma. 2008;64(suppl 2) Typically caused by dismounted IED attacks 12

13 Junctional Hemorrhage Control Evanna Burgwardt BSN, RN, CCRN Emergency Nurse, Level II Trauma Center Cardiac Intensive Care Unit Nurse ACLS/PALS Provider ABLS Provider TCCC Provider BCON Instructor Blood Loss and Shock Question: How does your body react to blood loss? Answer: It depends on how much blood is lost. 5 Liters Blood Volume Normal Adult Blood Volume: 5 Liters 1 liter by volume 1 liter by volume 1 liter by volume 1 liter by volume 1 liter by volume 4.5 Liters Blood Volume 500 cc Blood Loss 500 cc Blood Loss Mental state: Alert Radial pulse: Full Heart rate: Normal or slightly increased Systolic blood pressure: Normal Respiratory rate: Normal Is the casualty going to die from this? NO 13
14 1000 cc Blood Loss 1000 cc Blood Loss 4.0 Liters Blood Volume Mental state: Alert Radial pulse: Full Heart rate: 100+ Systolic blood pressure: Normal when supine Respiratory rate: May be normal Is the casualty going to die from this? NO 1500 cc Blood Loss 3.5 Liters Blood 3.5 Volume Liters Blood Volume 1500 cc Blood Loss Mental state: Alert but anxious Radial pulse: May be weak Heart rate: 100+ Systolic blood pressure: May be decreased Respiratory rate: 30 Is the casualty going to die from this? PROBABLY NOT 3.0 Liters Blood Volume 2000 cc Blood Loss 2000 cc Blood Loss Mental state: Confused/lethargic Radial pulse: Weak Heart rate: 120+ Systolic blood pressure: Decreased Respiratory rate: > 35 Is the casualty going to die from this? MAYBE 14
15 2.5 Liters Blood Volume 2500 cc Blood Loss 2500 cc Blood Loss Mental state: Unconscious Radial pulse: Absent Heart rate: 140+ Systolic blood pressure: Markedly decreased Respiratory rate: Over 35 Is the casualty going to die from this? MOST LIKELY Danny Devlin US Army Special Forces Assistant Detachment Commander US Army Ranger Qualified Special Forces Advanced Urban Combat Instructor TCCC/TECC Provider BCON Instructor 15

16 16


17 Hemostatic Agent There are many hemostatic agents available. These agents have varying levels of evidence supporting a single agent. The Medical Director must decide the agent of choice. Courtesy Dr. Bijan Kheirabadi Quick Clot Combat Gauze Dr. A. Scott Whyte Emergency Physician Level II Trauma Center Tactical Physician SWAT TCCC/TECC Instructor ACLS/PALS Instructor ATLS Provider (former instructor) EMT Instructor High School Girls Ice Hockey Coach 17

18 18

19 TranexamicAcid (TXA) Hemorrhage is the leading cause of preventable death in the tactical environment. Tourniquets and Tactical Gauze do not work for internal bleeding. TXA is shown to slow or stop some internal bleeding. Tranexamic Acid (TXA) Does not promote new clot formation Prevents clots which are forming from being broken down by the body Helps prevent death from hemorrhage Two major studies have shown a survival benefit from TXA, especially in casualties that require a massive transfusion of blood products. Hemostasis Blood normally flows unimpeded thru intact endothelial blood vessel walls If a wall is damaged, a fast, localized, controlled response tries to stop the bleeding. Three phases of hemostasis: 1. Vascular spasm and retraction 2. Platelet plug formation 3. Coagulation This is followed by fibrinolysis. 1. Vascular Spasm and Retraction Stimuli cause vasospasm: 1. Direct injury to smooth muscle 2. Chemicals released by endothelial cells and platelets 3. Reflexes initiated by local pain receptors Spasm becomes more efficient with increased tissue damage. 2. Platelet Plug Formation Platelets normally inactive When exposed to damaged endothelium and underlying exposed collagen, platelets swell and form spikes, become sticky and adhere to collagen Plates release serotonin (enhances vascular spasm), ADP (attracts more platelets), etc. Platelet plug limited to immediate area of injury by prostacyclin (released by endothelial cells) 19
20 Clotting Cascade 3. Coagulation Phase Intrinsic Pathway All clotting factors are within the blood vessels. Slower clotting Extrinsic Pathway Initiating factor is outside the blood vessels - tissue factor Faster clotting in seconds Clotting Cascade Clotting Cascade Clotting Cascade Transforms blood from a liquid to a gel Begins in 30 seconds Hemostasis 20
21 TranexamicAcid Synthetic amino acid, first introduced in Sweden in Prevents fibrinolysis and breakdown of clot. It is also a very weak inhibitor of thrombin. Tranexamic Acid Mechanism of action: TXA inhibits conversion of plasminogen to plasmin, hence prevents breakdown of clot. Increases collagen synthesis which preserves the fibrin matrix and increases the tensile strength of the clot. These actions help to stabilize the clot. Hemostasis with TXA Tranexamic Acid CRASH-2 Study MATTERS Study To see if tranexamicacid saves lives in bleeding trauma patients CRASH-2: Methods Study Included all adult trauma patients who were within 8 hours of their injury, if their doctor thought that they had or could have significant hemorrhage Patients were randomly allocated to get tranexamic acid or placebo End point: Death in hospital within 4 weeks of injury and all important side effects 20,211 patients 274 hospitals 40 countries (but not the U.S.) 21
22 Results Cause of death TXA Placebo Risk of death P value 10,060 10,067 Bleeding ( ) Thrombosis ( ) Organ failure ( ) 0.25 Head injury ( ) 0.60 CRASH-2 Conclusions Tranexamicacid: Reduces mortality in bleeding trauma patients Does not seem to increase unwanted clotting Must be given early within 3 hours of injury, preferably within 1 hour Is inexpensive Could save hundreds of thousands of lives each year around the world Other ( ) 0.63 Any death ( ) Tranexamic Acid After the CRASH-2 trial, tranexamicacid was added to the WHO List of Essential Medicines (March 2011). Some countries military are using tranexamicacid to treat combat casualties. The U.K. military has been using TXA since Tranexamicacid is being used in many hospitals around the world. Tranexamic acid could (should?) be given in ambulances. CRASH-2 Study Limitations Entry criteria: Adult trauma patients within 8 hours of injury who had or could have significant hemorrhage. BUT Only 50% of patients in each group actually needed transfusion. Participating sites: Many countries with less developed EMS and trauma care systems. No information about prehospital time or care given. CRASH-2 Study Limitations Military Application of TranexamicAcid in Trauma Emergency Resuscitation TXA No TXA P value # Patients (896) Inj. Severity Score TXA MATTERS Study (1 of 2) (NS) Overall Mortality 17.4% 23.9% 0.03 Retrospective Review by U.S. Military TXA vsno TXA in trauma patients receiving 1 or more units of packed RBCs # Pts Massive Transfusion Mortality Massive Transfusion % 28.1% Complications Pulmonary Emb. 2.7% 0.3% DVT 2.4% 0.2%
23 TXA Survival benefit GREATEST when given within 1 hour of injury. Survival benefit still present when given within 3 hours of injury. DO NOT GIVE TXA if more than 3 hours have passed since the casualty was injured survival is DECREASED by TXA given after this point. DON T DELAY WITH TXA! TXAAdministration: 1st Dose Supplied in 1 gram (1000 mg) ampoules. Inject 1 gram of TXA into a 100-cc bag of normal saline or lactated ringer s Infuse slowly over 10 minutes. Rapid IV push may cause hypotension If there is a new-onset drop in BP during the infusion, SLOW DOWN the TXA infusion. Then administer crystalloid or blood products, per local protocol. TXAAdministration: 2nd Dose Typically given after the casualty arrives at Trauma Center. May be given in field if evacuation is delayed and fluid resuscitation has been completed before arrival at the medical facility. If still in field or in evacuation mode when fluid resuscitation is complete, give second dose of TXA as directed for the first dose. SUMMARY Case Studies Data Review Bleeding Control Hands On Tourniquet Application Pressure Dressings Hemostatic Dressings Non-Compressible Bleeding Certify Participants B-Con Providers Congratulations -You are all now certified B-Con Providers! 23
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Where Have we Come From, and Where are we Going
 Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency
Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
The new standard in hemorrhage control
 The new standard in hemorrhage control Contents The need for hemostats What is Celox Rapid? Benefits How it works Performance Independent trials of Celox Gauze The need for hemostats in trauma Combat lives
The new standard in hemorrhage control Contents The need for hemostats What is Celox Rapid? Benefits How it works Performance Independent trials of Celox Gauze The need for hemostats in trauma Combat lives
itclamp 50 Clinical Training M-115-CE Rev C
 itclamp 50 Clinical Training M-115-CE Rev C Objectives Explain the impact of bleeding in trauma Recognize the importance of rapid haemorrhage control Classify wounds on the spectrum of bleeding Select
itclamp 50 Clinical Training M-115-CE Rev C Objectives Explain the impact of bleeding in trauma Recognize the importance of rapid haemorrhage control Classify wounds on the spectrum of bleeding Select
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
2/12/2018 TOURNIQUETS, FROM THE BATTLEFIELD TO YOUR BACKYARD Trauma Symposium RICHARD KING, MD, FACEP 01/26/2018 WARNING
 TOURNIQUETS, FROM THE BATTLEFIELD TO YOUR BACKYARD 2018 Trauma Symposium RICHARD KING, MD, FACEP 01/26/2018 WARNING T H I S P R E S E N TAT I O N C O N TA I N S S O M E V E R Y G R A P H I C I M A G E
TOURNIQUETS, FROM THE BATTLEFIELD TO YOUR BACKYARD 2018 Trauma Symposium RICHARD KING, MD, FACEP 01/26/2018 WARNING T H I S P R E S E N TAT I O N C O N TA I N S S O M E V E R Y G R A P H I C I M A G E
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Tactical Combat Casualty Care Guideline Change Fluid Resuscitation for Hemorrhagic Shock in TCCC
 Tactical Combat Casualty Care Guideline Change 14-01 Fluid Resuscitation for Hemorrhagic Shock in TCCC 2 June 2014 Why a change was needed: The last update to the fluid resuscitation recommendations in
Tactical Combat Casualty Care Guideline Change 14-01 Fluid Resuscitation for Hemorrhagic Shock in TCCC 2 June 2014 Why a change was needed: The last update to the fluid resuscitation recommendations in
DAMAGE CONTROL RESUSCITATION
 DAMAGE CONTROL RESUSCITATION Chapter 4 Contributing Authors Jeremy G. Perkins, MD, FACP, LTC, MC, US Army Alec C. Beekley, MD, FACS, LTC, MC, US Army All figures and tables included in this chapter have
DAMAGE CONTROL RESUSCITATION Chapter 4 Contributing Authors Jeremy G. Perkins, MD, FACP, LTC, MC, US Army Alec C. Beekley, MD, FACS, LTC, MC, US Army All figures and tables included in this chapter have
Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for External Hemorrhage Control
 Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Emergency Blood and Massive Transfusion: The Surgeon s Perspective. Transfusion Medicine Update September 16 17, 2009
 Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
TRAIN MORE, BLEED LESS
 Techline Technologies, Inc. techlinetrauma.com TRAIN MORE, BLEED LESS compact KITS, Vol.1 2017 2016-2017 Techline Technologies, Inc. All rights reserved. Equal Opportunity Employer PG [p] 855.426.0312
Techline Technologies, Inc. techlinetrauma.com TRAIN MORE, BLEED LESS compact KITS, Vol.1 2017 2016-2017 Techline Technologies, Inc. All rights reserved. Equal Opportunity Employer PG [p] 855.426.0312
CRASH ing Trauma Patients: The CRASH trials. Tim Coats Professor of Emergency Medicine University of Leicester, UK
 CRASH ing Trauma Patients: The CRASH trials Tim Coats Professor of Emergency Medicine University of Leicester, UK www.le.ac.uk/emag I DO NOT have an affiliation (financial or otherwise) with a pharmaceutical,
CRASH ing Trauma Patients: The CRASH trials Tim Coats Professor of Emergency Medicine University of Leicester, UK www.le.ac.uk/emag I DO NOT have an affiliation (financial or otherwise) with a pharmaceutical,
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES
 INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 406 Manage Shock Casualties TERMINAL LEARNING OBJECTIVES 1. Given a casualty in an operational environment,
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 406 Manage Shock Casualties TERMINAL LEARNING OBJECTIVES 1. Given a casualty in an operational environment,
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
HYPOTHERMIA IN TRAUMA. Kevin Palmer EMT-P, DiMM
 HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
Director, Burn Center MetroHealth Medical Center Professor of Surgery Case Western Reserve University
 Director, Burn Center MetroHealth Medical Center Professor of Surgery Case Western Reserve University BLAST INJURY Which of following statements concerning blast lung injury are FALSE? 1)Blast lung injury
Director, Burn Center MetroHealth Medical Center Professor of Surgery Case Western Reserve University BLAST INJURY Which of following statements concerning blast lung injury are FALSE? 1)Blast lung injury
Tactical Field Care #2
 Tactical Combat Casualty Care for Medical Personnel August 2017 (Based on TCCC-MP Guidelines 170131) Tactical Field Care #2 OBJECTIVES LIST physical findings suggestive of pelvic fracture. DEMONSTRATE
Tactical Combat Casualty Care for Medical Personnel August 2017 (Based on TCCC-MP Guidelines 170131) Tactical Field Care #2 OBJECTIVES LIST physical findings suggestive of pelvic fracture. DEMONSTRATE
FM 3.0.MH.1 Medical Handbook
 FM 3.0.MH.1 Medical Handbook DISTRIBUTION RESTRICITON: Distribution authorized to 3 rd Battalion, 75th Ranger Regiment Senior Leadership and Instructors to protect operational information that is of use.
FM 3.0.MH.1 Medical Handbook DISTRIBUTION RESTRICITON: Distribution authorized to 3 rd Battalion, 75th Ranger Regiment Senior Leadership and Instructors to protect operational information that is of use.
Prehospital Hemorrhage Control
 Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Chapter 19. Hemostasis
 Chapter 19 Hemostasis Hemostasis Hemostasis is the cessation of bleeding stopping potentially fatal leaks important in small blood vessels not effective in hemorrhage excessive bleeding from large blood
Chapter 19 Hemostasis Hemostasis Hemostasis is the cessation of bleeding stopping potentially fatal leaks important in small blood vessels not effective in hemorrhage excessive bleeding from large blood
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion
 This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms
Bleeding and Haemostasis. Saman W.Boskani HDD, FIBMS Maxillofacial Surgeon
 Bleeding and Haemostasis Saman W.Boskani HDD, FIBMS Maxillofacial Surgeon 1 Beeding Its escaping or extravasation of blood contents from blood vessels Types: - Arterial - Venous - Capillary Differences
Bleeding and Haemostasis Saman W.Boskani HDD, FIBMS Maxillofacial Surgeon 1 Beeding Its escaping or extravasation of blood contents from blood vessels Types: - Arterial - Venous - Capillary Differences
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Physiology of. The Blood hemostasis. By prof. Israa f. jaafar
 Physiology of The Blood hemostasis By prof. Israa f. jaafar Learning objectives Understand the Platelet structure and function Explane the Platelet production Understand the phases of hemostasis: vascular
Physiology of The Blood hemostasis By prof. Israa f. jaafar Learning objectives Understand the Platelet structure and function Explane the Platelet production Understand the phases of hemostasis: vascular
Bundeswehrkrankenhaus Ulm Abteilung HNO Kopf-Halschirurgie
 Kai Johannes Lorenz and Klaus Effinger Department of Otorhinolaryngology, Head and Neck Surgery Department of Radiology and interventional Radiology German Armed Forces Hospital Incidence of hemorrhage
Kai Johannes Lorenz and Klaus Effinger Department of Otorhinolaryngology, Head and Neck Surgery Department of Radiology and interventional Radiology German Armed Forces Hospital Incidence of hemorrhage
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Kay Barrera MD. Surgery Grand Rounds June 19, 2014 SUNY Downstate
 Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Death on the Battlefield Implications for Prevention, Training, and Medical Care
 PR O E C P R O J E C S U S A I N INSIUE OF SURGICAL RESEARCH INSIUE OF SURGICAL RESEARCH Combat Casualty Care P R O E C P R O J E C S U S A I N Death on the Battlefield Implications for Prevention, raining,
PR O E C P R O J E C S U S A I N INSIUE OF SURGICAL RESEARCH INSIUE OF SURGICAL RESEARCH Combat Casualty Care P R O E C P R O J E C S U S A I N Death on the Battlefield Implications for Prevention, raining,
You Are the Emergency Medical Responder
 Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Shock. William Schecter, MD
 Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Blood on the Ground. emsworld.com /node/215693
 Blood on the Ground emsworld.com /node/215693 It s 2:30 in the morning, and Cypress Creek EMS is responding to an emergency call in Harris County, north of Houston. The patient has severe injuries and
Blood on the Ground emsworld.com /node/215693 It s 2:30 in the morning, and Cypress Creek EMS is responding to an emergency call in Harris County, north of Houston. The patient has severe injuries and
UNIT VI. Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav. Copyright 2011 by Saunders, an imprint of Elsevier Inc.
 UNIT VI Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav Hemostasis: Prevention of Blood Loss Vascular constriction Formation of a platelet plug Formation of a blood
UNIT VI Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav Hemostasis: Prevention of Blood Loss Vascular constriction Formation of a platelet plug Formation of a blood
Moath Darweesh. Omar Sami. Saleem Khreisha. 1 P a g e
 7 Moath Darweesh Omar Sami Saleem Khreisha 1 P a g e -First of all, I want to give a quick revision to simplify the whole hemostasis mechanism, it will be much easier here with me. Enjoy (you can skip
7 Moath Darweesh Omar Sami Saleem Khreisha 1 P a g e -First of all, I want to give a quick revision to simplify the whole hemostasis mechanism, it will be much easier here with me. Enjoy (you can skip
Anatomy and Physiology
 Anatomy and Physiology For The First Class 2 nd Semester Thrombocytes = Platelets Thrombocytes = Platelets Blood platelets are non-nucleated disc like cell fragments 2-4 µm in diameter. Platelets are not
Anatomy and Physiology For The First Class 2 nd Semester Thrombocytes = Platelets Thrombocytes = Platelets Blood platelets are non-nucleated disc like cell fragments 2-4 µm in diameter. Platelets are not
Overview of DoD Resuscitation Fluid Research
 Overview of DoD Resuscitation Fluid Research COL Jim Atkins, MD, PhD Director, Division of Military Casualty Research Walter Reed Army Institute of Research Program Area Manager for Resuscitation Studies
Overview of DoD Resuscitation Fluid Research COL Jim Atkins, MD, PhD Director, Division of Military Casualty Research Walter Reed Army Institute of Research Program Area Manager for Resuscitation Studies
Epidemiology. Case. Pre-Hospital SI and Massive Transfusion
 Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Objectives. Pediatric Trauma Update: Objectives: Topics
 Objectives Pediatric Trauma Update: 2013 Christopher Newton MD, FACS, FAAP Medical Director Trauma Services and Surgical Critical Care Children s Hospital Oakland Review recent trends and advancements
Objectives Pediatric Trauma Update: 2013 Christopher Newton MD, FACS, FAAP Medical Director Trauma Services and Surgical Critical Care Children s Hospital Oakland Review recent trends and advancements
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Stop the Bleed The White House Hemorrhage Control Initiative
 Stop the Bleed The White House Hemorrhage Control Initiative David M Sailors MD Asst Prof Surgery UGA/MCG Medical Partnership Team Physician UGA Athletic Association University of Georgia Athens Georgia
Stop the Bleed The White House Hemorrhage Control Initiative David M Sailors MD Asst Prof Surgery UGA/MCG Medical Partnership Team Physician UGA Athletic Association University of Georgia Athens Georgia
The Mangled Extremity: Best Practice for Optimal Outcomes. Kristen Ray R.N., MSN
 The Mangled Extremity: Best Practice for Optimal Outcomes Kristen Ray R.N., MSN Learning Objectives At the end of the session, participants will be able to: Verbalize the initial management principles
The Mangled Extremity: Best Practice for Optimal Outcomes Kristen Ray R.N., MSN Learning Objectives At the end of the session, participants will be able to: Verbalize the initial management principles
Implementation and execution of civilian RDCR programs Minnesota RDCR
 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
Hypotension / Shock. Adult Medical Section Protocols. Protocol 30
 Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hemodynamic Disorders, Thrombosis, and Shock. Richard A. McPherson, M.D.
 Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
: Your Haemorrhage Control Solution
 : Your Haemorrhage Control Solution Shoulder Injury Leg Injury TM HAEMORRHAGE New solutions to control difficult bleeding are needed in emergent care, including pre-hospital, hospital and tactical environments.
: Your Haemorrhage Control Solution Shoulder Injury Leg Injury TM HAEMORRHAGE New solutions to control difficult bleeding are needed in emergent care, including pre-hospital, hospital and tactical environments.
TXA in Combat Casualty Care Does It Adversely Affect Extremity Reconstruction and Flap Thrombosis Rates?
 MILITARY MEDICINE, 180, 3:24, 2015 TXA in Combat Casualty Care Does It Adversely Affect Extremity Reconstruction and Flap Thrombosis Rates? CDR Ian L. Valerio, MC USN; LT Paul Campbell, MC USN; CPT Jennifer
MILITARY MEDICINE, 180, 3:24, 2015 TXA in Combat Casualty Care Does It Adversely Affect Extremity Reconstruction and Flap Thrombosis Rates? CDR Ian L. Valerio, MC USN; LT Paul Campbell, MC USN; CPT Jennifer
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
PEDIATRIC MASSIVE TRANSFUSION
 PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
Disaster Triage START/JUMPSTART
 Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center AGENDA Attendance Ground Rules Presentation Scenarios Additional Resources Evaluation/Certificate Objectives: Define a Mass Casualty
Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center AGENDA Attendance Ground Rules Presentation Scenarios Additional Resources Evaluation/Certificate Objectives: Define a Mass Casualty
Primary Exam Physiology lecture 5. Haemostasis
 Primary Exam Physiology lecture 5 Haemostasis Haemostasis Body s response for the prevention and cessation of bleeding. Broadly consists of: Primary Haemostasis - vascular spasm and platlet plug formation
Primary Exam Physiology lecture 5 Haemostasis Haemostasis Body s response for the prevention and cessation of bleeding. Broadly consists of: Primary Haemostasis - vascular spasm and platlet plug formation
FOR: JONATHAN WOODSON, M.D., ASSISTANT SECRETARY OF DEFENSE (HEAL TH AFFAIRS)
") DEFENSE HEAL TH BOARD FIVE SKYLINE PLACE, SUITE 810 5111 LEESBURG PIKE FALLS CHURCH, VA 22041-3206 SEP 2 3 2011 FOR: JONATHAN WOODSON, M.D., ASSISTANT SECRETARY OF DEFENSE (HEAL TH AFFAIRS) SUBJECT: Recommendations
DEFENSE HEAL TH BOARD FIVE SKYLINE PLACE, SUITE 810 5111 LEESBURG PIKE FALLS CHURCH, VA 22041-3206 SEP 2 3 2011 FOR: JONATHAN WOODSON, M.D., ASSISTANT SECRETARY OF DEFENSE (HEAL TH AFFAIRS) SUBJECT: Recommendations
Civilian versus Military Trauma Management
 Western University From the SelectedWorks of Vivian C. McAlister November, 2010 Civilian versus Military Trauma Management Vivian C. McAlister Available at: https://works.bepress.com/vivianmcalister/151/
Western University From the SelectedWorks of Vivian C. McAlister November, 2010 Civilian versus Military Trauma Management Vivian C. McAlister Available at: https://works.bepress.com/vivianmcalister/151/
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions
 Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned
Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Chapter 19 Cardiovascular System Blood: Functions. Plasma
 Chapter 19 Cardiovascular System Blood: Functions 19-1 Plasma Liquid part of blood. Colloid: liquid containing suspended substances that don t settle out of solution 91% water. Remainder proteins, ions,
Chapter 19 Cardiovascular System Blood: Functions 19-1 Plasma Liquid part of blood. Colloid: liquid containing suspended substances that don t settle out of solution 91% water. Remainder proteins, ions,
Can't Intubate, Can't oxygenate (CICO) The new terminology What is the Military Experience What is the Civilian Experience What is your role.
 The new terminology What is the Military Experience What is the Civilian Experience What is your role.") Disclaimer The views in the presentation are the author's, and do not reflect the views of the Department of Defence I am a full time Australian Defence Force Procedural Specialist (Anaesthetist) Can't
Disclaimer The views in the presentation are the author's, and do not reflect the views of the Department of Defence I am a full time Australian Defence Force Procedural Specialist (Anaesthetist) Can't
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
EL DORADO COUNTY EMS AGENCY PREHOSPITAL PROTOCOLS
 EL DORADO COUNTY EMS AGENCY PREHOSPITAL PROTOCOLS Effective: July 1, 2017 Reviewed: November 9, 2016 Revised: November 9, 2016 EMS Agency Medical Director ALLERGIC REACTION/ANAPHYLAXIS ADULT BLS TREATMENT
EL DORADO COUNTY EMS AGENCY PREHOSPITAL PROTOCOLS Effective: July 1, 2017 Reviewed: November 9, 2016 Revised: November 9, 2016 EMS Agency Medical Director ALLERGIC REACTION/ANAPHYLAXIS ADULT BLS TREATMENT
Hemostasis. Learning objectives Dr. Mária Dux. Components: blood vessel wall thrombocytes (platelets) plasma proteins
 plasma proteins") Hemostasis Learning objectives 14-16 Dr. Mária Dux Components: blood vessel wall thrombocytes (platelets) plasma proteins Hemostatic balance! procoagulating activity anticoagulating activity 1 Thrombocytes
Hemostasis Learning objectives 14-16 Dr. Mária Dux Components: blood vessel wall thrombocytes (platelets) plasma proteins Hemostatic balance! procoagulating activity anticoagulating activity 1 Thrombocytes
HEART HEALTH WEEK 2 SUPPLEMENT. A Beginner s Guide to Cardiovascular Disease ATHEROSCLEROSIS. Fatty deposits can narrow and harden the artery
 WEEK 2 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease ATHEROSCLEROSIS FIGURE 1 Atherosclerosis is an inflammatory process where cholesterol is deposited in the wall of arteries and
WEEK 2 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease ATHEROSCLEROSIS FIGURE 1 Atherosclerosis is an inflammatory process where cholesterol is deposited in the wall of arteries and
The Future of EMS as Revealed through Research. A Window into the Near Future
 The Future of EMS as Revealed through Research A Window into the Near Future Raymond L. Fowler, M.D., FACEP Co-Principal Investigator National Institutes of Health Resuscitation Outcomes Consortium --------------------
The Future of EMS as Revealed through Research A Window into the Near Future Raymond L. Fowler, M.D., FACEP Co-Principal Investigator National Institutes of Health Resuscitation Outcomes Consortium --------------------
Introduction (1 of 3)
") Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Traumatic Cardiac Arrest Protocol
 Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
-Hashim ahmed is the one who wrote this sheet. I just edited it according to our record.
 * Subjects of this lecture : - Hemostasis - Platelets, general information, their ultrastructure and role in hemostasis. - Definitions: Thrombus, Embolus, Arteriosclerosis and Atherosclerosis. *NOTE: Prof
* Subjects of this lecture : - Hemostasis - Platelets, general information, their ultrastructure and role in hemostasis. - Definitions: Thrombus, Embolus, Arteriosclerosis and Atherosclerosis. *NOTE: Prof
2007 NATIONAL EMS SCOPE OF PRACTICE MODEL CHANGE NOTICES. Change Notice 1.0
 2007 NATIONAL EMS SCOPE OF PRACTICE MODEL CHANGE NOTICES November 1, 2017 Change Notice 1.0 The following changes to the National EMS Scope of Practice Model (February 2007) DOT HS 810 657 are effective
2007 NATIONAL EMS SCOPE OF PRACTICE MODEL CHANGE NOTICES November 1, 2017 Change Notice 1.0 The following changes to the National EMS Scope of Practice Model (February 2007) DOT HS 810 657 are effective
Page 1 of 6 THROMBOCYTES
 Page 1 of 6 THROMBOCYTES Platelets are not cells in the strict sense. About one-fourth the diameter of a lymphocyte, they are cytoplasmic fragments of extraordinarily large cells (up to 60 µm in diameter)
Page 1 of 6 THROMBOCYTES Platelets are not cells in the strict sense. About one-fourth the diameter of a lymphocyte, they are cytoplasmic fragments of extraordinarily large cells (up to 60 µm in diameter)
Disaster Triage START/JUMPSTART. Objectives: What is the Goal of MCI Management?
 Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center Objectives: Define a Mass Casualty Incident and the unique challenges of an MCI Understand the differences between dayto-day triage
Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center Objectives: Define a Mass Casualty Incident and the unique challenges of an MCI Understand the differences between dayto-day triage
Modern Military Trauma. from 16 Years of Conflict. Care: Lessons Learned. Joe DuBose MD, FACS FCCM
 Modern Military Trauma Care: Lessons Learned from 16 Years of Conflict Joe DuBose MD, FACS FCCM Associate Professor of Surgery Uniformed Services University of the Health Sciences Lt Col USAF MC Director
Modern Military Trauma Care: Lessons Learned from 16 Years of Conflict Joe DuBose MD, FACS FCCM Associate Professor of Surgery Uniformed Services University of the Health Sciences Lt Col USAF MC Director
Chapter 11. Lecture and Animation Outline
 Chapter 11 Lecture and Animation Outline To run the animations you must be in Slideshow View. Use the buttons on the animation to play, pause, and turn audio/text on or off. Please Note: Once you have
Chapter 11 Lecture and Animation Outline To run the animations you must be in Slideshow View. Use the buttons on the animation to play, pause, and turn audio/text on or off. Please Note: Once you have
Advanced Resuscitative Care in Tactical Combat Casualty Care: TCCC Guidelines Change 18-01
 Advanced Resuscitative Care in Tactical Combat Casualty Care: TCCC Guidelines Change 18-01 14 October 2018 Frank Butler, MD 1* ; John B. Holcomb, MD 2 ; Stacy Shackelford, MD 3 ; Sean Barbabella, MD 4
Advanced Resuscitative Care in Tactical Combat Casualty Care: TCCC Guidelines Change 18-01 14 October 2018 Frank Butler, MD 1* ; John B. Holcomb, MD 2 ; Stacy Shackelford, MD 3 ; Sean Barbabella, MD 4
Chapter 28. Objectives. Objectives 01/09/2013. Bleeding and Soft-Tissue Trauma
 Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
WHITE PAPERS PRESENTATION VIDEO DOCUMENTATION EXPERIMENT WO NDCLOT. The WoundClot Principals for Effective Bleeding Control PRESENTATION
 WHITE PAPERS PRESENTATION VIDEO DOCUMENTATION EXPERIMENT ARTICLES OUR STUDY BLEEDING CONTROL 5 POINT MODEL WO NDCLOT The WoundClot Principals for Effective Bleeding Control PRESENTATION Harnessing SCIENCE
WHITE PAPERS PRESENTATION VIDEO DOCUMENTATION EXPERIMENT ARTICLES OUR STUDY BLEEDING CONTROL 5 POINT MODEL WO NDCLOT The WoundClot Principals for Effective Bleeding Control PRESENTATION Harnessing SCIENCE
DEFENSE HEAL TH BOARD DEFENSE HEAL TH HEADQUARTERS 7700 ARLINGTON BOULEVARD, SUITE 5101 FALLS CHURCH, VA
 DEFENSE HEAL TH BOARD DEFENSE HEAL TH HEADQUARTERS 7700 ARLINGTON BOULEVARD, SUITE 5101 FALLS CHURCH, VA 22042-5101 DEC 2 0 2012 FOR: JONATHAN WOODSON, M.D., ASSISTANT SECRETARY OF DEFENSE (HEALTH AFFAffiS)
DEFENSE HEAL TH BOARD DEFENSE HEAL TH HEADQUARTERS 7700 ARLINGTON BOULEVARD, SUITE 5101 FALLS CHURCH, VA 22042-5101 DEC 2 0 2012 FOR: JONATHAN WOODSON, M.D., ASSISTANT SECRETARY OF DEFENSE (HEALTH AFFAffiS)
Kevin Schulz, MD, FAEMS, FACEP
 Blood Therapy for EMS Kevin Schulz, MD, FAEMS, FACEP - Clinical Assistant Professor of Emergency Medicine, EMS Fellowship Program Director - McGovern School of Medicine at UTHealth - Assistant Medical
Blood Therapy for EMS Kevin Schulz, MD, FAEMS, FACEP - Clinical Assistant Professor of Emergency Medicine, EMS Fellowship Program Director - McGovern School of Medicine at UTHealth - Assistant Medical
 International Trauma Life Support for Prehospital Care Providers Sixth Edition Patricia M. Hicks, MS, NREMTP Roy Alson, PhD, MD, FACEP Donna Hastings, EMT-P John Emory Campbell, MD, FACEP and Alabama Chapter,
International Trauma Life Support for Prehospital Care Providers Sixth Edition Patricia M. Hicks, MS, NREMTP Roy Alson, PhD, MD, FACEP Donna Hastings, EMT-P John Emory Campbell, MD, FACEP and Alabama Chapter,
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Shock Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Shock Revised: 11/2013 (12 questions on trauma exam from this outline) DEFINITIONS Aerobic metabolism
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Shock Revised: 11/2013 (12 questions on trauma exam from this outline) DEFINITIONS Aerobic metabolism
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Report Documentation Page
 Report Documentation Page Form Approved OMB No. 0704-0188 Public reporting burden for the collection of information is estimated to average 1 hour per response, including the time for reviewing instructions,
Report Documentation Page Form Approved OMB No. 0704-0188 Public reporting burden for the collection of information is estimated to average 1 hour per response, including the time for reviewing instructions,
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA THE PREHOSPITAL APPROACH TO CHEST INJURY MANAGEMENT
 Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Improving Rural Trauma Outcomes: Local Damage Control? R Simons, V Vogt Haines, K McCarroll. Enhanced Surgical Skills Program Banff, January 2018
 Improving Rural Trauma Outcomes: Local Damage Control? R Simons, V Vogt Haines, K McCarroll Enhanced Surgical Skills Program Banff, January 2018 Session Objectives Define problem of high injury mortality
Improving Rural Trauma Outcomes: Local Damage Control? R Simons, V Vogt Haines, K McCarroll Enhanced Surgical Skills Program Banff, January 2018 Session Objectives Define problem of high injury mortality