3D Geronotlogy: Delirum, Dementia and Deprescribing
|
|
|
- Meredith Murphy
- 5 years ago
- Views:
Transcription

1 3D Geronotlogy: Delirum, Dementia and Deprescribing Dr Michal Boyd, RN, NP, ND, FCNA(NZ), FAANP Nurse Practitioner and Associate Professor NPNZ Conference 28 April 2017 Wellington 1
2 Confusion Assessment Method (CAM) The diagnosis of delirium requires presence of BOTH A and B A B Acute onset / fluctuating Course Inattention o o Is there evidence of an acute change in mental status form patient baseline. Does the behaviour Come and go? Fluctuate during the day? Increase / decrease in severity? Does the patient: o Have difficulty focusing attention? o Become easily distracted? o Have difficulty keeping track of what is said?
3 Confusion Assessment Method (CAM) (cont) and the presence of EITHER C or D C D Disorganised Speech Altered Level of Consciousness Is the patient s thinking: o Disorganised o Incoherent For example, does the patient have: - Rambling speech / irrelevant conversation? - Unpredictable switching of subjects? - Unclear or illogical flow of ideas? Overall is the patients level of consciousness: o Alert (normal) o Vigilant (hyper-alert) o Lethargic (drowsy but easily roused) o Stuperous (difficult to rouse) o Comatose (unrousable)
4 The rest of the CAM screen Disorientation: time, location Memory impairment? Perceptual disturbances? Hallucinations / illusions Altered sleep-wake cycle: sleep in day, insomnia at night
 Thyroid function Troponin I (?")
5 Basic Delirium Screen Tests Midstream urine / urinalysis Full blood count Urea and electrolytes + calcium Renal function Glucose Liver function CRP (ESR?) Thyroid function Troponin I (?) Serum medication levels ECG Chest X-ray CT head, blood cultures, ABG, LP (acute care)
6 Prevent complications Normalize sleep Reorientate reassure Ensure hydration Relaxation techniques Family involvement PERSON WITH DELIRIUM Educate carers, family Identify/Treat reversibility Encourage activity Mobility/ADL Communication Vision Hearing aids Pain relief Antipsychotic med
7 Waitemata DHB Delirium Study Tan and Scott NZMJ, 2015Volume 128 Number 1411

8 Resolved Delirium McAvay et al.. Volume 54, Issue JAGS
9 Pharmacologic treatment Class & Drug Dose Adverse Effects Comments Antipsychotic Haloperidol mg BD po with prn doses q4hrly (peak 4-6hrs) EP symptoms Prolonged QT Usual agent of choice. Effectiveness demonstrated in RCT Avoid IV Atypical antipsychotic Risperidone Olanzapine Quetiapine 0.25mg BD 2.5-5mg daily mg daily EP effects equivalent to or slightly less than Haloperidol Prolonged QT Tested only in small studies Associated with increased mortality in older people with sc Benzodiazepine Lorazepam Temazepam 0.5-1mg, add doses q4hrly as needed Avoid monotherapy Paradoxical excitation, resp depression, oversedation 2 nd line agent Assoc with prolongation, worsening of symptoms Use for withdrawal, Parkinson's

10 Delirium Treatment Yoon et al BMC Psychiatry 13:240

11 Cognitive Impairment Main Causes Degenerative Vascular Infectious Structural Metabolic Alzheimer s Frontotemporal lobe/pick s Lewy Body Dementia Parkinson s Dementia ALS/MND MS Multi-Infarct Dementia Pellagra Vasculitis Lupus HIV CJD Syphilis Herpes Zoster Fungal Bacterial Normal Pressure Hydrocephalus Neoplasm Alcohol / Drugs Trauma Subdural Hematoma Electrolyte Imbalance Medications Wilson s Whipple s Thyroid B12/Folate Huntington s Hepatic

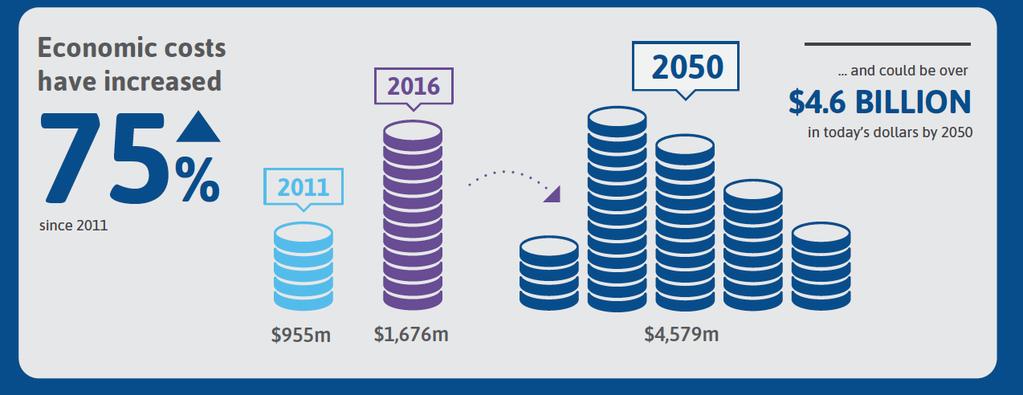
12 Dementia (2016 Access/Deloitte)
 USA Matthews et")

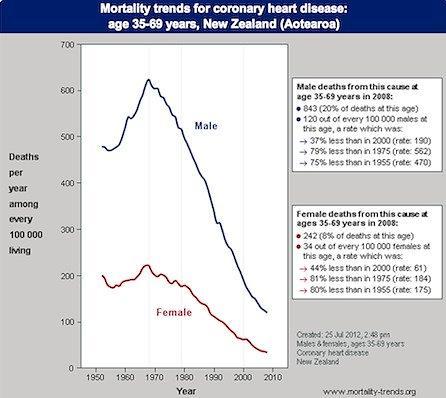
13 Falling rates of dementia in UK and USA UK ( ) USA Matthews et al. Lancet 2013; 382(9902): Satizabal et al., NEJM, February 2016
14
15 Percentage Mild Cognitive Impairment (MCI) Memory impaired but are otherwise functioning well and do not meet clinical criteria for dementia 100% 90% Symptoms include 80% Memory complaint, preferably with corroboration Intact activities of daily living 70% 60% 50% 40% 30% AD MCI Non-Affected 20% Progression MCI dementia ~ 10-15% per year in clinic-based studies (Mariani et al, 2007) 10% 0% Age There are currently no recommended treatments for MCI Medication review Exercise and social engagement Petersen RC. Neurology. 2001;56: Petersen RC et al. Arch Neurol. 1999;56:
16 Cognitive Impairment Pathway Waitemata DHB 2014 Table 1: Description of CIP Participants with atypical cognitive impairment 61 people enrolled in CIP (60 carers) 5% dropped out early 20% other diagnosis 34% dementia diagnosis 41% mild cognitive impairment diagnosis Other Diagnoses Diagnosis Number of Participants No cognitive impairment 4 Depression 2 Alcohol issues/depression 1 Parkinson s disease 1 Seizure disorder/ inconclusive diagnosis 1 Stroke - admitted to *ARC (died) 1 Brain metastasis (died) 1 Moved out of area/subsequent ARC admit 1 *ARC = Aged Residential Care
 obesity high blood pressure diabetes high cholesterol smoking Rowe, et al., J Nucl Med 2011 vol. 52 no. 11")
17 Beta Amyloid Plaques Midlife vascular risk factors were associated with elevated levels of brain amyloid later in life (JAMA 2017) obesity high blood pressure diabetes high cholesterol smoking Rowe, et al., J Nucl Med 2011 vol. 52 no. 11

18 Vascular Dementia Previously thought to be about 20% of all dementias Now thought that there is very little pure vascular dementia Does the ischaemic changes from cardiovascular disease promote plaques and tangles? The Nun Study: lacunar strokes increase dementia risk 20 fold with fewer plaques and neurofibrillary tangles before showing signs of dementia. TREATMENT: Cardiovascular Health Exercise Active Mind Socially Active

19 Link between Fizzy Drinks and Dementia (JAMA April 2017) Those who drink sugary drinks showed: Poorer memory More atrophy Small hippocampus Those that diet soda daily were almost three times likely to develop stroke when compared to those that do not.
20 Deprescribing Definition: The systematic process of identifying and discontinuing drugs when: existing or potential harms outweigh existing or potential benefits within the context of an individual patient s care goals current level of functioning life expectancy values, and preferences. Scott IA et al. JAMA Internal Medicine Scott May IA et al JAMA Internal Medicine May 2015
21 When to consider deprescribing? Patient presents with new symptoms which could be adverse drug effect (i.e. falls, confusion, fatigue) End-stage disease/ terminal illness Receiving high-risk drugs/ combinations Receiving preventive drugs in scenarios where drug can be safely discontinued Scott IA et al. JAMA Internal Medicine May 2015
22 Priority Drugs for Deprescribing Survey of 65 Canadian geriatrics experts (36 pharmacists, 19 physicians, 10 CRNP), Modified Delphi approach Aim to ID and prioritize med classes where evidence-based deprescribing guidelines would be of benefit 5 priorities: benzodiazepines atypical antipsychotics statins tricyclic antidepressants proton pump inhibitors. Farrell B, et al. Plos ONE. Jan 1 2ol 10 Issue 4. re 22
23 5 Steps of Deprescribing 1.) Ascertain all drugs the patient is currently taking and reasons for each one 2.) Consider overall risk of drug-induced harm to determine the appropriate intensity of deprescribing intervention 3.) Assess each drug for its current or future benefit potential compared with current or future harm/ burden potential Scott IA et al. JAMA Internal Medicine May 2015
24 5 Steps (cont).* 4.) Prioritize drugs with lowest benefit-harm ratio lowest likelihood of adverse withdrawal reactions Lowest disease rebound syndromes 5.) Implement a discontinuation regimen and monitor patients closely for improvement in outcomes or onset of adverse effects. Scott IA et al. JAMA Internal Medicine May 2015
25 Drug Withdrawal Trials Systematic review of 31 withdrawal trials (15 RCT, 16 observational) (Iyer at al. Drugs Aging, 2008:25(12) ). Pts 65 and over Multiple drug categories: Antihypertensives, psychotropics, benzodiazepines Dc d without harm in 20 to 100% of patients Reduction in falls and improvement in cognitive and psychomotor function (Psychotropics, Benzos) Also replicated in another review (van der Cammen) 80% of participants with dementia were able to safely stop antipsychotics (Declercq T et al. Cochrane Database Syst Rev. 2013). Australian National Blood Pressure study Found that 37% of participants remained normotensive 1 yr after drug withdrawal (Neson MR, et al. BMJ. 2002)

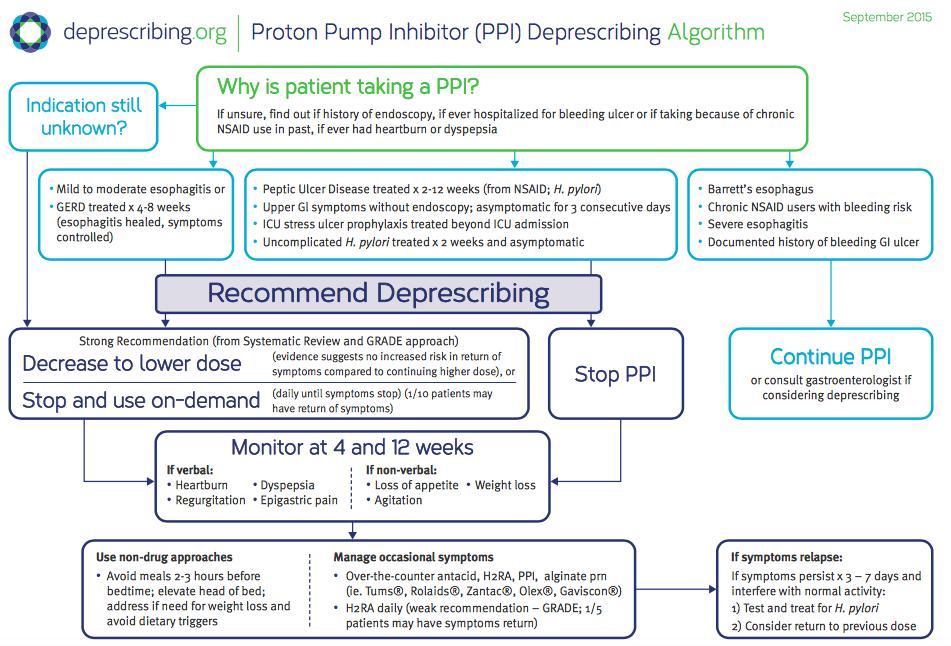
26 Deprescribing.org
27

28
29 Other Tools for Deprescribing PIMs/PIDs/PIP (potentially inappropriate medicines/drugs/prescribing), IPET, STOPP-START Beers example: Drug class or disease PIMs Rationale Recommendation Quality of Evidence Strength of recommendation Antispasmodics Highly anticholinergic, uncertain effectiveness Avoid Moderate Strong PIMs due to concomitant diseases/conditions Syncope & alpha blockers Increases risk of orthostatic hypotension or bradycardia Avoid High Weak PIMs to be used with caution Aspirin for primary prevention of CVD Lack of evidence of benefit vs. risk in 80yrs Use with caution in adults aged 80 yrs Low Weak
30 Bisphosphonates (alendronate/fosamax) Australian Guide to Deprescribing 1-3 years treatment 1 fx prevented for every pts 5 years of on-going of tx with oral agents will have 5 more years of benefit FLEX trial no difference in non-vertebral fx Increase in vertebral fx (5.3% vs 2.4) NNT 34 Need good renal function overall and ability to follow directions for oral med
31 Bisphosphonates For describing Those at low risk of falls who have taken them for 5 years <5 year life expectance No previous vertebral fx in the last 5 years For continuing High fracture risk with T-score <2.5 Monitor with DEXA every 2 years.
 PROSPER: 3.2 year follow-up MI, CVA 17.4% (statin) vs 21.")
32 Estimated time to benefit is 2 years NNT Statins Australian Guides to Describing Most LDL reduction benefit occurs with a low dose No specific studies for those over 80 years old Significantly reduced MI and stroke in older people with high CV risk (without CV disease) PROSPER: 3.2 year follow-up MI, CVA 17.4% (statin) vs 21.7% (no statin) It does not prolong life in the short term
33 Statins In Favour of Desprescribing: Short Life Expectancy can improve QoL Poor overall functional status Low overall cardiovascular risk Side effects: muscle aches, lethargy, decreased cognition Against Deprescribing Pts that are well with a >5 year life expectancy Those with high CVD risk (diabetes, previous MI, CVA)

34 Thank You.
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
QuickTime and a DV - NTSC decompressor are needed to see this picture.
 QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
QuickTime and a DV - NTSC decompressor are needed to see this picture. Case Presentation (Actual Case) 66 y/o Female c/o Hip Pain Fell, but no pre-fall symptoms Did not hit head or have LOC PMHx: DM, ESRD,
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
Optimising Safe & Appropriate Medicines Use and Deprescribing. Katie Smith, Director, East Anglia Medicines Information Service February 2014
 Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Delirium and Falls. Julia Poole CNC Aged Care RNSH
 Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Cognitive Status. Read each question below to the patient. Score one point for each correct response.
 Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
11/11/2016. Disclosures. Natural history of BPSD. Objectives. Assessment of BPSD. Behavioral Management of Persons with Alzheimer s Disease
 Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Diagnosing & managing dementia & delirium
 Aging: Its complex management Dunedin School of Medicine Diagnosing & managing dementia & delirium Falling Confusion Incontinence A. John Campbell University of Otago Medical School New Zealand Impaired
Aging: Its complex management Dunedin School of Medicine Diagnosing & managing dementia & delirium Falling Confusion Incontinence A. John Campbell University of Otago Medical School New Zealand Impaired
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
GUIDELINES FOR DIAGNOSIS, PREVENTION AND TREATMENT OF DELIRIUM IN THE INPATIENT SETTING
 GUIDELINES FOR DIAGNOSIS, PREVENTION AND TREATMENT OF DELIRIUM IN THE INPATIENT SETTING Policy Details NHFT document reference MMG033 Version Final Date Ratified May 2016 Ratified by Medicines Management
GUIDELINES FOR DIAGNOSIS, PREVENTION AND TREATMENT OF DELIRIUM IN THE INPATIENT SETTING Policy Details NHFT document reference MMG033 Version Final Date Ratified May 2016 Ratified by Medicines Management
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018
 From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Geri-PARDY! (2015 Beers Criteria) Pharmacology Edition
 Pharmacology Edition") Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Murthy Gokula MD,CMD
 Murthy Gokula MD,CMD MEDICATIONS & LIFE EXPECTANCY DON T ROUTINELY PRESCRIBE LIPID-LOWERING MEDICATIONS IN INDIVIDUALS WITH A LIMITED LIFE EXPECTANCY: AAHPM About Choosing Wisely First conceived by the
Murthy Gokula MD,CMD MEDICATIONS & LIFE EXPECTANCY DON T ROUTINELY PRESCRIBE LIPID-LOWERING MEDICATIONS IN INDIVIDUALS WITH A LIMITED LIFE EXPECTANCY: AAHPM About Choosing Wisely First conceived by the
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
Disclosures No financial conflicts of interest. Key Questions
 Hospital Delirium: New Evidence in Diagnosis & Treatment Ethan Cumbler MD, FHM, FACP Professor of Medicine Medical Director Acute Care For Elderly Unit University of Colorado School of Medicine Disclosures
Hospital Delirium: New Evidence in Diagnosis & Treatment Ethan Cumbler MD, FHM, FACP Professor of Medicine Medical Director Acute Care For Elderly Unit University of Colorado School of Medicine Disclosures
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Dementia and Delirium
 Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Delirium: A Condition of All Ages. Delirium, also known as acute confusional state, Definition. Epidemiology
 Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Confusion in the acute setting Dr Susan Shenkin
 Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
PSYCHOTROPIC SOLUTIONS
 PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
Delirium in Cancer: Psychopharmacologic Management
 Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Improving Delirium Management: Mapping Out One Unit s Journey. Geriatrics Institute June 27, 2013
 Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Polypharmacy and Deprescribing for Older People
 Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
POST STROKE DELIRIUM. Dr Janet Ballantyne
 POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event
 Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways
Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Cambridge University Press Effective Treatments in Psychiatry Peter Tyrer and Kenneth R. Silk Excerpt More information
 Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4
 DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
DELIRIUM DR S A R A H A B D E L A T I S A S DR H I L A R Y W O L F E N D A L E S T 4 AIMS Define delirium Identify: Different types of delirium Risk factors Preventable causes Screening tools Management
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies. Falls can be classified into four main groups:
 What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Practical Matters in the Care of A Person with Dementia
 Practical Matters in the Care of A Person with Dementia 7 th Annual Neurology Update for Primary Care Deborah S. Hoffnung, PhD, ABPP CN November 16, 2018 1 Typical Aging, MCI/CIND, dementia Common Dementia
Practical Matters in the Care of A Person with Dementia 7 th Annual Neurology Update for Primary Care Deborah S. Hoffnung, PhD, ABPP CN November 16, 2018 1 Typical Aging, MCI/CIND, dementia Common Dementia
The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability
 with Learning Disability") The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability Danielle Adams Principal Clinical Pharmacist Pharmacy and Medicines Optimisation Team HPFT July 2017 1
The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability Danielle Adams Principal Clinical Pharmacist Pharmacy and Medicines Optimisation Team HPFT July 2017 1
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia
 Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
Delirium Assessment and management in relation to falls risk in hospital
 Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
Delirium Assessment and management in relation to falls risk in hospital A house call - Mrs JM 95-year-old lady Normally cognitively intact Multiple medical problems, including falls Housebound, mobile
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Antipsychotics in Dementia
 Antipsychotics in Dementia What s all the fuss? Judy MacDonald RPh BSc Pharm Dr. Ashok Krishnamoorthy MD MRCPsych FRCPC ABAM MS (Neuro Psych) Learning Objectives Recognize common behavioural & psychological
Antipsychotics in Dementia What s all the fuss? Judy MacDonald RPh BSc Pharm Dr. Ashok Krishnamoorthy MD MRCPsych FRCPC ABAM MS (Neuro Psych) Learning Objectives Recognize common behavioural & psychological
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Falls most commonly seen in RACFs are due to tripping, slipping and stumbling (21.6%). Falling down stairs is relatively uncommon in
. Falling down stairs is relatively uncommon in") This Presentation Medications and Falls Dr Peter Tenni M Pharm (Curtin), PhD (UTAS) AACPA Director, CPS A fall is an event which results in a person coming to rest inadvertently on the ground or floor
This Presentation Medications and Falls Dr Peter Tenni M Pharm (Curtin), PhD (UTAS) AACPA Director, CPS A fall is an event which results in a person coming to rest inadvertently on the ground or floor
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist. HMS Training Webinar January 27, 2017
 Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Behavioral Issues in Dementia. March 27, 2014 Dylan Wint, M.D.
 Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
SCE Revision Course Geriatric Medicine & Other
 SCE Revision Course Geriatric Medicine & Other Geriatric Medicine: what the curriculum says you should know Physiology of ageing Atypical presentations: the Geriatric Giants Falls and fragility fractures
SCE Revision Course Geriatric Medicine & Other Geriatric Medicine: what the curriculum says you should know Physiology of ageing Atypical presentations: the Geriatric Giants Falls and fragility fractures
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013
 A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
Update in Geriatrics. Muriel Rainfray Department of Gerontology CHU Bordeaux
 Update in Geriatrics Muriel Rainfray Department of Gerontology CHU Bordeaux What s new about frailty? The frailty phenotype and the frailty index : different instruments for different purposes Matteo Cesari
Update in Geriatrics Muriel Rainfray Department of Gerontology CHU Bordeaux What s new about frailty? The frailty phenotype and the frailty index : different instruments for different purposes Matteo Cesari
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych
 Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016
 Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions
 Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia
 Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
Evidence-Based Clinical Practice Guideline for Deprescribing Cholinesterase Inhibitors and Memantine in People with Dementia ADI 2018, Chicago FACULTY OF MEDICINE Dr Emily Reeve NHMRC Cognitive Decline
Shared decision making for stepdown and stopping decisions. Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes
 Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Medicine Related Falls Risk Assessment Tool (MRFRAT)
") Medicine Related Falls Risk Assessment Tool (MRFRAT) The Medicine Related Falls Risk Assessment tool (MRFRAT) in Appendix 1 is designed to help identify patients at risk of falls due to their current medicine
Medicine Related Falls Risk Assessment Tool (MRFRAT) The Medicine Related Falls Risk Assessment tool (MRFRAT) in Appendix 1 is designed to help identify patients at risk of falls due to their current medicine
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,