Workshop Cyst & Lucency. How to Approach
|
|
|
- Blaze Lambert
- 5 years ago
- Views:
Transcription
1 Workshop Cyst & Lucency How to Approach


2 To Approach Cystic Lung Disease True cysts? Cavitary disease Cystic bronchiectasis Mosaic attenuation Subpleural cysts Bullae Paraseptal emphysema Honeycombing Birt Hogg Dubè syndrome (BHD) Parenchymal cysts Solitary/Multiple If multiple: No associated HRCT findings Associated nodules Associated ground glass nodules/opacity
3 How to Approach Cystic Lung Disease Parenchymal cysts w/o other abnormalities 1. Solitary: incidental, pneumatocele, bronchogenic cyst 2. Focal, multifocal, diffuse: o o o Focal: > 1 cyst in one lobe of the lung. Multifocal : > 1 lobe but not all lobes. Diffuse: involving all 5 lobes.
4 Multiple Parenchymal Cysts No associated findings LAM/TS BHD PLCH Metastasis Infection Papillomatosis Associated nodules PLCH LIP Light-chain deposition disease (LCDD) Amyloid Metastasis Associated GGO Pneumocytis Jivorecii pneumonia DIP Chronic HP
5 Chapter 1
6 Question 1 (Code )
7 Question 1 (Code )
8 Question 1 (Code )
9 Question 1 (Code )
")
10 Air trapping Pulmonary Oligemia GGO with crazy paving Answers of question 1 (Code )
11 Pattern of abnormality Size of PA Bronchus Associated findings Expiration Air trapping Oligemia GGO Geographic area, equal to lobule Normal/ slightly small Dilated and/or thick wall Centrilobular nodule/tib attenuation <100 HU Geographic area, larger than lobule Small with collateral artery Normal to slightly dilated Infarction/Scar attenuation >100 HU Poorly-defined area Normal Normal

12 Air trapping Air trapping Question 1 (Code ) Geographic area of low density, equal to lobule Normal or slightly small PA in low density area Dilated bronchus and/or thick wall May seen ill-defined centrilobular nodule/tib Expiration: No or slightly increase in attenuation (<100 HU) Not improve in follow-up
")
13 Pulmonary oligemia Oligemia Geographic area of low density, larger than lobule Small PA in low density area, collateral vessel Normal to slightly dilated bronchus Subpleural scar or infarct Expiration: attenuation >100 HU Not improve in follow-up Question 1 (Code )
14 Code 5.15
")
15 Ground glass opacity Ground glass opacity Poorly-defined area between high and low density area Normal PA Normal bronchus Expiration: attenuation >100 HU May improve on follow-up Question 1 (Code )

16
17 Question 2 (Code 5.15) Inspiration Expiration
18 Question 2 (Code 5.15) Inspiration Expiration
")
19 Question 2 (Code 5.15) Inspiration
20 Question 2 (Code 5.15) Expiration
21 Question 2 (Code 5.15) Inspiration
22 Question 2 (Code 5.15) Expiration


23 Pulmonary oligemia Geographic area of low density, larger than lobule Small PA in low density area, collateral vessel Expiration: attenuation >100 HU Question 2 (Code 5.15)

24 Question 2 (Code 5.15)
25 Question 3 (Code 5.16) Inspiration Expiration
26 Question 3 (Code 5.16) Inspiration
27 Question 3 (Code 5.16) Expiration


28 Air trapping Geographic area of low density, equal to lobule Normal or slightly small PA Dilated bronchus and/or thick wall Expiration: no/ slightly attenuation <100 HU Question 3 (Code 5.16)
29 Inspiration Expiration

30 Inspiration Expiration Question 4: Code 5.25
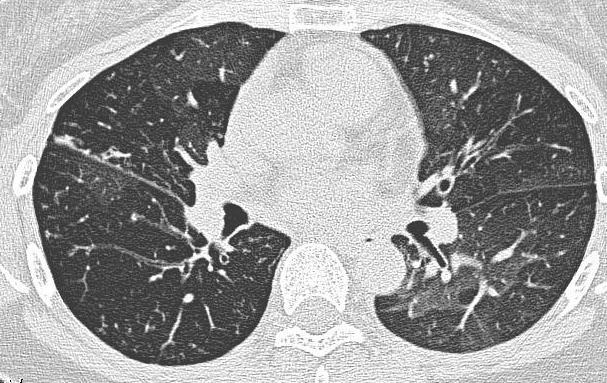
31 Air trapping in constrictive bronchiolitis Geographic area of low density, equal to lobule Normal or slightly small PA Dilated bronchus and/or thick wall Expiration: no/ slightly attenuation <100 HU Question 4: Code 5.25

32 Question 5 (Code 5.13)

33 Question 5 (Code 5.13)
34 Question 5 (Code 5.13)
35 Question 5 (Code 5.13)
36 Question 5 (Code 5.13)


37 Bronchiectasis Lack of bronchial tapering Signet-ring sign Cluster of grapes sign Usually found ill-defined centrilobular nodule and/or air trapping Question 5 (Code 5.13)
38 Chapter 2
39 Subpleural Cysts Parenchymal cysts

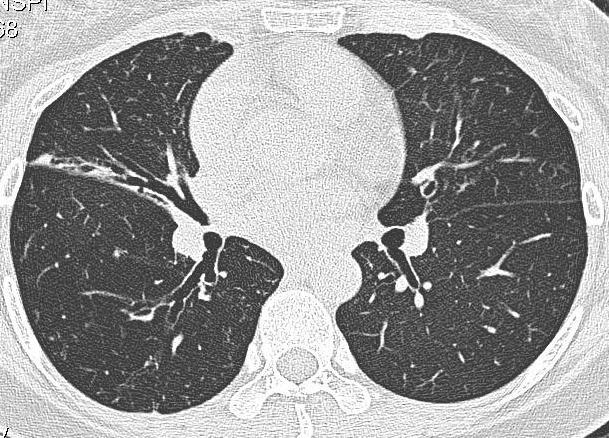
40 Subpleural Cysts Bullae Round focal lucency > 1 cm in Ø Thin, almost imperceptible wall. May be formed by coalescence of paraseptal emphysema. Can enlarged over time.

41 Subpleural Cysts Paraseptal emphysema Well-defined lucent area < 1 cm. Subpleural & peribronchovascular area. Cyst walls: not abut each other. bound by pleural surface and interlobular septa. Coalescence of cysts bullae. Preserve lung architecture.

42 Honeycombing Air-filled cystic spaces 3-10 mm in Several layers & Share walls Subpleural lung Associated traction bronchiectasis, architectural distortion, volume loss
43 Question 6 (Code 5.2)
44 Question 6 (Code 5.2)
45 Question 6 (Code 5.2)
46 Question 6 (Code 5.2)
47 Question 6 (Code 5.2)

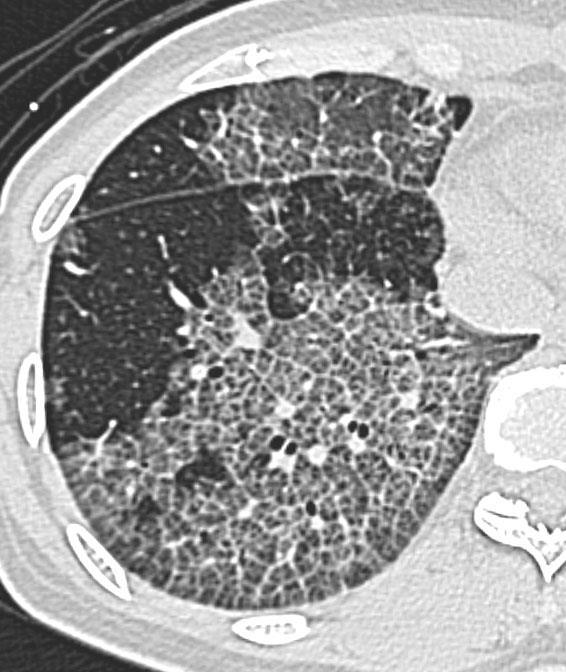
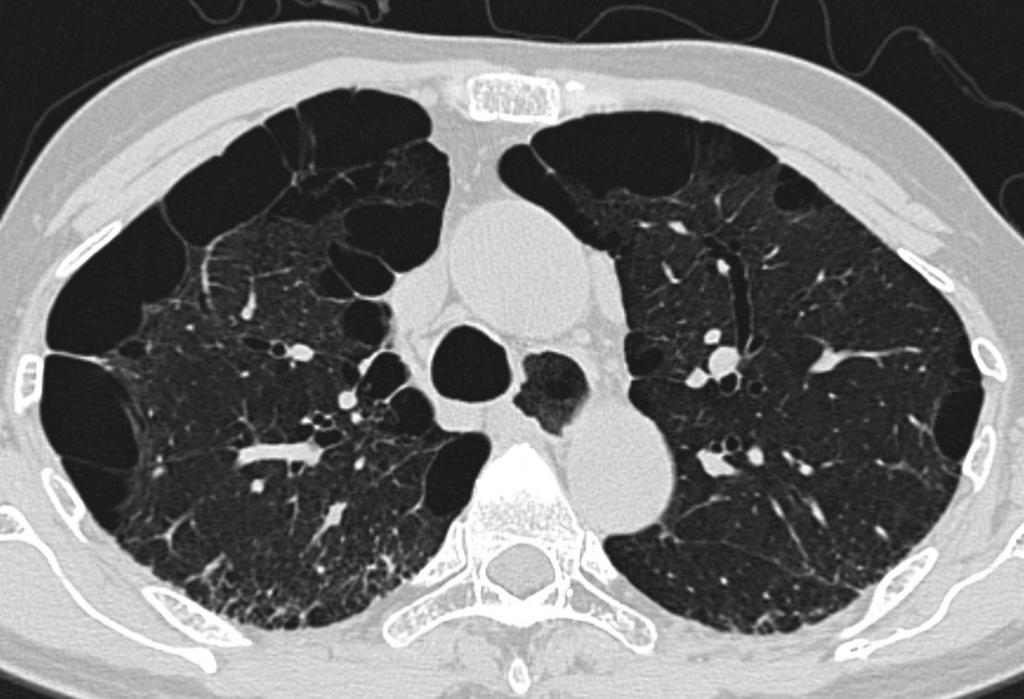
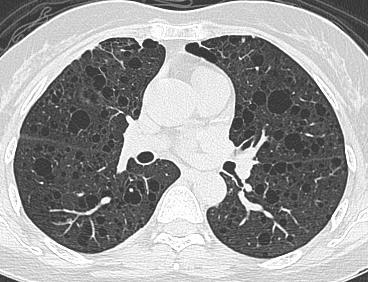
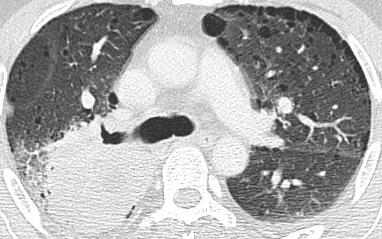
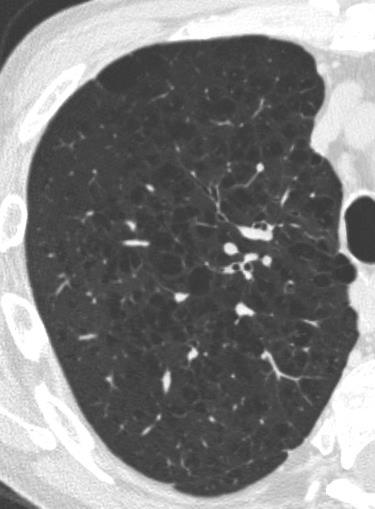
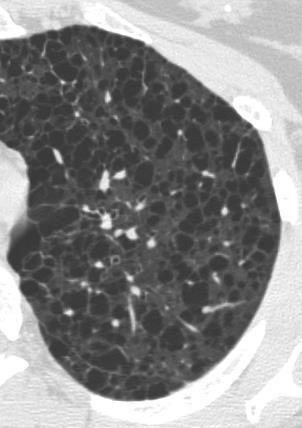
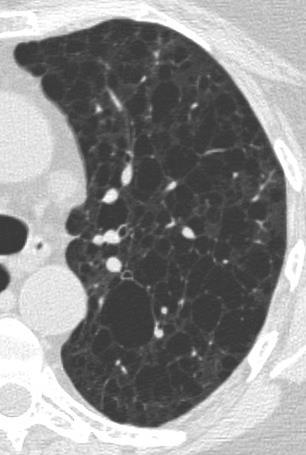
48 Question 6 (Code 5.2) Airspace enlargement with fibrosis (AEF) Multiple thin-walled (mostly < 1 mm thick) cyst, various size Affected lobes: o upper lobe. o upper & middle part of lower lobes. Distribution: Slightly apart from pleura Clinical important: No risk of acute exacerbation (in contrast to UIP) Watanabe et al, Eur J Radiology2015
49 Paraseptal emphysema Honeycombing Characters Usually one layer Several layers Variable AEF Wall thickness Imperceptible 1-3 mm Mostly < 1 mm Affected lobe Usually upper lobe Usually lower lobe Upper lobe Upper & middle part of lower lobes. Location Subpleural Subpleural Slightly apart from pleura Volume of affected area No volume loss Volume loss No volume loss Watanabe et al, Eur J Radiology2015
50 31

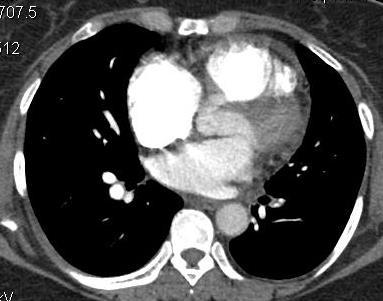
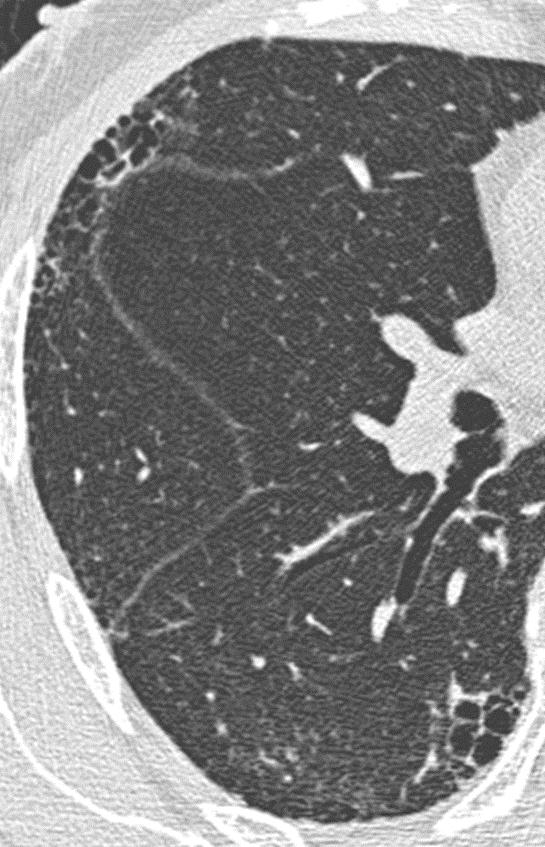
51 Thick-walled cystic lesions (TWCLs) Described in CTD associated CPFE by Cottin et al. Arbitrarily defined as cysts > 2 cm in Ø & delimitated by a wall >1 mm thick in an area of the lung where reticulation was present. Cottin et al, Arthritis & Rheumatism 2011 (Code 5.3.2)
52 Question 7 (Code 5.1)
53 Question 7 (Code 5.1)
54 Question 7 (Code 5.1)
55 Question 7 (Code 5.1)
56 Question 7 (Code 5.1)


57 Question 7 (Code 5.1) Paraseptal emphysema & Bulla
 Question 7 (Code 5.")
58 Thick-walled cystic lesions (TWCLs) Question 7 (Code 5.1)
59 Question 8 (Code 5.11)
60 Question 8 (Code 5.11)
61 Question 8 (Code 5.11)
62 Question 9 (Code 5.11)
63 Question 8 (Code 5.11)
64 Question 8 (Code 5.11) Cyst location: subpleural e.g. bullae, traction bronchiectasis/bronchiolectasis, honeycomb. Vertical distribution: lower Ancillary findings: esophageal dilatation Dx: Systemic sclerosis related f-nsip.


65 Question 9 (Code 5.24)

66 Question 9 (Code 5.24)

67 Question 9 (Code 5.24)

68 Question 9 (Code 5.24)

69 Question 9 (Code 5.24)
70 Neurofibromatosis I Autosomal dominant Café au lait spot, peripheral nerve tumor Thin walled bullae, and cysts in upper-mid lung zone. Fibrosis in lower lung zone. Chest wall and mediastinal involvement Question 9 (Code 5.24)
71 Chapter 3
72

73 Centrilobular emphysema Location: Upper zone predominance. Centrilobular lucency. No distinct wall. Exhibit a central dot: branch of pulmonary artery in the 2 o pulmonary lobule.
74
75 Panlobular Emphysema Basal predominance Diffuse decrease in lung attenuation Pulmonary vascular pruning

76 Panbular emphysema (Code 5.1)
77 Multiple Parenchymal Cysts No associated findings LAM/TS BHD PLCH Metastasis Infection Papillomatosis Associated nodules PLCH LIP Light-chain deposition disease (LCDD) Amyloid Metastasis Associated GGO Pneumocytis Jivorecii pneumonia DIP Chronic HP
78 To Approach Cystic Lung Disease The important features to approach multiple cystic lesions Distribution of cysts Most important Cyst shape and size. Presence of any ancillary findings.
79 Question 10 (Code 5.20)
80 Question 10 (Code 5.20)
")
81 Question 10 (Code 5.20)
82 Question 10 (Code 5.20)
83 Question 10 (Code 5.20)
84 Question 10 (Code 5.20) LAM Female Uniform thin wall cyst No preferential distribution Occasional pneumocyte hyperplasia nodule Associated with renal angiomyolipoma
85 Question 11 (Code 5.22)
86 Question 11 (Code 5.22)
87 Question 11 (Code 5.22)
88 Question 11 (Code 5.22)
89 Question 11 (Code 5.22)


90 Question 11 (Code 5.22) LCH Almost exclusively in smokers. Young adult, slightly older in women. No gender predilection. Typically combination of nodules, cavitated nodules and cysts. Bizarre-shaped, thick & irregular walled cysts. Poorly or well defined nodules, regress overtime. Associated emphysema, bullae Upper lobe predominance. Relatively sparing lung base & CPA Extrapulmonary manifestations: Bone, pituitary (DI) and skin involvement
91 Question 12 (Code 5.17)
92 Question 12 (Code 5.17)
93 Question 12 (Code 5.17)
94 Question 12 (Code 5.17)
95 Question 12 (Code 5.17)
")
96 Question 12 (Code 5.17)
 Tuberous sclerosis Uniform, small cyst Adenomatoid pneumocyte hyperplasia nodule Basal")
97 Question 12 (Code 5.17) Tuberous sclerosis Uniform, small cyst Adenomatoid pneumocyte hyperplasia nodule Basal predominate Increased lung volume a/w renal AML, LAM, SEGA, cardiac rhabdomyoma
98 Cystic lung diseases LCH LAM Tuberous sclerosis Clinical Young adult smokers No gender predilection Female, pneumothorax, chylothorax No sex predilection Familial predisposition Cysts Bizarre-shaped, thick & irregular wall Round shaped, thin wall Nodule Poorly or well defined, regress overtime Occasional pneumocyte hyperplasia Adenomatoid pneumocyte hyperplasia Distribution Upper lobe, Spare lung base & CPA No preferential distribution Basal predominate Associated abnormality Bone, pituitary (DI) and skin involvement Renal AML Renal & hepatic AML, cardiac rhabdomyoma, CNS (SEGA)
99 Question 13: Code 5.26
100 Question 13: Code 5.26
101 Question 13: Code 5.26
102 Question 13: Code 5.26
103 Question 13: Code 5.26

104 LAM Female Uniform thin wall cyst No preferential distribution Occasional pneumocyte hyperplasia nodule Associated with renal angiomyolipoma Question 13: Code 5.26
105 Question 14 (Code 5.4)
106 Question 14 (Code 5.4)
107 Question 14 (Code 5.4)
108 Question 14 (Code 5.4)
109 Question 14 (Code 5.4)


110 Emphysema & interstitial fibrosis Centrilobular emphysema: well defined lucent area with imperceptible wall. Honeycombing: thick walled small cysts located subpleural and basal in distribution Question 14 (Code 5.4)
111 Question 15 (Code 5.18)
112 Question 15 (Code 5.18)
113 Question 15 (Code 5.18)
114 Question 15 (Code 5.18)
115 Question 15 (Code 5.18)
 LCH Bizzare shaped Upper lobe, spare costophrenic angles Preserve or increase lung volume Poorly or")
116 Question 15 (Code 5.18) LCH Bizzare shaped Upper lobe, spare costophrenic angles Preserve or increase lung volume Poorly or well defined, regress overtime nodule Associate with Bone, pituitary and skin involvement


117 Question 15 (Code 5.18) Bizarre-shaped cysts - Cloverleaf
118 Question 16: Code 5.27
119 Question 16: Code 5.27
120 Question 16: Code 5.27
121 Question 16: Code 5.27
122 Question 16: Code 5.27
123 Cystic Metastasis Random distribution Peripheral, basal and subpleural distribution. Metastatic disease: H&N, sarcoma, squamous cell CA Question 16: Code 5.27
124 Question 17: Code 5.28
125 Question 17: Code 5.28
126 Question 17: Code 5.28
127 Question 17: Code 5.28
128 Question 17: Code 5.28

129 Tracheobronchial Papillomatosis Solid nodules. Cystic lesions with thin/thick walls Randomly in central, peripheral and occasionally subpleural Lesions in larynx and trachea. Question 17: Code 5.28
130 A 59-year-old female with left breast cancer Question 18 (Code 5.23)
131 Question 18 (Code 5.23)
132 Question 18 (Code 5.23)
133 Question 18 (Code 5.23)
134 Question 18 (Code 5.23)


135 Question 18 (Code 5.23) Dx:???
136 Amyloidosis 6th decade of life. Commonly in a/w Sjögren s syndrome (with/without LIP), lymphoproliferative disease or mucosa-associated lymphoid tissue (MALT) lymphoma. Clinical manifestation: tracheobronchial form: diffuse or focal tracheal narrowing. nodular form: lung nodules. diffuse form with miliary nodules, reticulonodular opacities, and honeycombing Raoof et al, Chest 2016

137 Amyloidosis Nodules: Lower & subpleural predominance. Slow growth. Sharp, smooth, lobulated contours. Varying in size from 0.5 to 15 cm. Often central cavitation or calcification. Cyst: Large thin walled cysts with internal septae abutting bronchiocentric nodules Peripheral predilection Seaman et al, AJR 2011 Raoof et al, Chest 2016
138 Light-Chain Deposition Disease (LCDD) A rare disorder of middle-aged patients (mean age, 67 years). Characterized by deposition of monoclonal immunoglobulin light chains in various organs, including kidneys, lungs, skin, joints, or blood vessels. 75% occur in association with multiple myeloma or macroglobulinemia. Raoof et al, Chest 2016

139 Light-Chain Deposition Disease Lung involvement: rare. CT: Cysts: o believed to correspond to dilation of the small airways. o thin-walled, round, and up to 2 cm in size. Nodules: irregular, multiple, and can be bilateral or unilateral. Patchy areas of consolidation. Lymphadenopathy. (LCDD) Raoof et al, Chest 2016

140 Birt-Hogg-Dubé Syndrome Rare autosomal-dominant inherited disorder; mutations in the folliculin (FLCN) gene which encodes the protein FLCN. Characterized by hair follicle tumors, M.C fibrofolliculomas. High predisposition to malignant renal tumors: often bilateral and multifocal. Other associated systemic conditions: colonic polyposis and ophthalmologic disorders, such as progressive flecked chorioretinopathy & chorioretinal scars Souza et al, AJR 2005
141 Birt-Hogg-Dubé Syndrome Lung cysts in association with BHD 1st described by Toro et al. in > 80% patients, women = men and likely develop in early to mid adulthood (30 40 years). Multiple, thin-walled cysts. Predominant in peripheral lung zones at lung bases and along the mediastinum. Unique feature: abut or encase the proximal portion of the lower pulmonary veins. Souza et al, AJR 2005 Gupta et al, Fam Cancer 2013

142 Birt-Hogg-Dubé Syndrome Souza et al, AJR 2005
143 Birt-Hogg-Dubé Syndrome Should be suspected in a young patient presenting with spontaneous pneumothorax, with personal/family history of pneumothorax, skin lesions or renal tumors. DDx: Lymphangioleiomyomatosis; o Less in number of cysts in BHD. o AML more typical for LAM Langerhans cell histiocytosis. Lymphocytic interstitial pneumonitis. Pneumocystis carinii pneumonia. Souza et al, AJR 2005 Gupta et al, Fam Cancer 2013
144 Question 19: Code 5.29
145 Question 19: Code 5.29
146 Question 19: Code 5.29
147 Question 19: Code 5.29
148 Question 19: Code 5.29

149 Pulmonary Langerhans Cell Histiocytosis 7 years later Question 19: Code 5.29
150 Question 20: Code 5.30
151 Question 20: Code 5.30
152 Question 20: Code 5.30
153 Question 20: Code 5.30
154 Question 20: Code 5.30
155 Lymphocytic interstitial pneumonia (LIP) associated with SjÖgren Syndrome Question 20: Code 5.30 M.C. a/w CNT disease (SjÖgren syndrome, RA, SLE), HIV, drug exposure, allogenic hematopoietic stem cell transplants. Idiopathic rare. Cysts: thin-walled, random or basilar/perivascular distribution. GGO, centrilobular nodules. Thickened interlobular septa. Enlarged mediastinal nodes.
156 Thank you
Cystic Lung Disease. Cristopher A. Meyer, MD
 Cystic Lung Disease Cristopher A. Meyer, MD Air filled structure with definable wall typically less than 1 mm thick Cris A. Meyer, M.D. Professor of Radiology University of Wisconsin School of Medicine
Cystic Lung Disease Cristopher A. Meyer, MD Air filled structure with definable wall typically less than 1 mm thick Cris A. Meyer, M.D. Professor of Radiology University of Wisconsin School of Medicine
Spectrum of Cystic Lung Disease and its Mimics. Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology
 Spectrum of Cystic Lung Disease and its Mimics Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology No Financial Disclosures Learning Objectives 1. Review the
Spectrum of Cystic Lung Disease and its Mimics Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology No Financial Disclosures Learning Objectives 1. Review the
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Daria Manos RSNA 2016 RC 401. https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html
 Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Cystic lung diseases 7/21/2017. Cystic Lung Diseases. CT definition of a lung cyst. Important clinical clues
 Cystic Lung Diseases Cystic lung diseases Aurelie Fabre Increased Awareness Spontaneous Pneumothorax High resolution imaging (HRCT) Multidisciplinary approach like interstitial lung disease CT definition
Cystic Lung Diseases Cystic lung diseases Aurelie Fabre Increased Awareness Spontaneous Pneumothorax High resolution imaging (HRCT) Multidisciplinary approach like interstitial lung disease CT definition
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Manish Powari Regional Training Day 10/12/2014
 Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
Radiologic Approach to Smoking Related Interstitial Lung Disease
 Radiologic Approach to Smoking Related Interstitial Lung Disease Poster No.: C-1854 Congress: ECR 2013 Type: Educational Exhibit Authors: K.-N. Lee, J.-Y. Han, E.-J. Kang, J. Kang; Busan/KR Keywords: Toxicity,
Radiologic Approach to Smoking Related Interstitial Lung Disease Poster No.: C-1854 Congress: ECR 2013 Type: Educational Exhibit Authors: K.-N. Lee, J.-Y. Han, E.-J. Kang, J. Kang; Busan/KR Keywords: Toxicity,
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Diffuse Cystic Lung Disease at High-Resolution CT
 Cardiopulmonary Imaging Pictorial Essay Seaman et al. HRCT of Diffuse Cystic Lung Disease Cardiopulmonary Imaging Pictorial Essay Downloaded from www.ajronline.org by 37.44.193.85 on 01/05/18 from IP address
Cardiopulmonary Imaging Pictorial Essay Seaman et al. HRCT of Diffuse Cystic Lung Disease Cardiopulmonary Imaging Pictorial Essay Downloaded from www.ajronline.org by 37.44.193.85 on 01/05/18 from IP address
Mimics in chest disease: interstitial opacities
 Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Epidemiology and classification of smoking related interstitial lung diseases
 Epidemiology and classification of smoking related interstitial lung diseases Šterclová M. Department of Respiratory Diseases, Thomayer Hospital, Prague, Czech Republic Supported by an IGA Grant No G 1207
Epidemiology and classification of smoking related interstitial lung diseases Šterclová M. Department of Respiratory Diseases, Thomayer Hospital, Prague, Czech Republic Supported by an IGA Grant No G 1207
Multiple Cystlike Lung Lesions
 Residents Section Pattern of the Month Cantin et al. Multiple Cystlike Lung Lesions in the dult Residents Section Pattern of the Month Residents inradiology Luce Cantin 1 lexander. ankier Ronald L. Eisenberg
Residents Section Pattern of the Month Cantin et al. Multiple Cystlike Lung Lesions in the dult Residents Section Pattern of the Month Residents inradiology Luce Cantin 1 lexander. ankier Ronald L. Eisenberg
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Liebow and Carrington's original classification of IIP
 Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Bubbles in the lung. Page 1 of 29
 Bubbles in the lung. Poster No.: C-1048 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Arango, A. Martínez de Alegría, R. García Figueiras, S. Baleato González, M. C. Ageitos Casais, M. V. Trujillo
Bubbles in the lung. Poster No.: C-1048 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Arango, A. Martínez de Alegría, R. García Figueiras, S. Baleato González, M. C. Ageitos Casais, M. V. Trujillo
Radiologic-pathologic correlation of pulmonary diseases
 The 1578 th Chest Conference/ 3 rd Biennial Clinical- Radiologic-Pathologic Correlation Radiologic-pathologic correlation of pulmonary diseases Harumi Itoh, M.D. University of Fukui, Japan Centriacinar
The 1578 th Chest Conference/ 3 rd Biennial Clinical- Radiologic-Pathologic Correlation Radiologic-pathologic correlation of pulmonary diseases Harumi Itoh, M.D. University of Fukui, Japan Centriacinar
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
Pulmonary manifestations of Rheumatoid Arthritis: what is there waiting to be found?
 Pulmonary manifestations of Rheumatoid Arthritis: what is there waiting to be found? Poster No.: C-1795 Congress: ECR 2015 Type: Educational Exhibit Authors: M. S. C. Rodrigues, R. Correia, A. Carvalho,
Pulmonary manifestations of Rheumatoid Arthritis: what is there waiting to be found? Poster No.: C-1795 Congress: ECR 2015 Type: Educational Exhibit Authors: M. S. C. Rodrigues, R. Correia, A. Carvalho,
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker. Michael B. Gotway, MD
 August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ USA Clinical History: A 55 year old woman presented
August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ USA Clinical History: A 55 year old woman presented
NONE OVERVIEW FINANCIAL DISCLOSURES UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF (UIP) FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP
 FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP") UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Cystic Lung Diseases: Spectrum of Radiologic Findings
 Cystic Lung Diseases: Spectrum of Radiologic Findings Poster No.: P-0012 Congress: ESTI 2014 Type: Educational Poster Authors: B. Alami, O. Addou, M. Jaffal, Y. Lamrani, M. Boubbou, I. Kamaoui, M. Maaroufi,
Cystic Lung Diseases: Spectrum of Radiologic Findings Poster No.: P-0012 Congress: ESTI 2014 Type: Educational Poster Authors: B. Alami, O. Addou, M. Jaffal, Y. Lamrani, M. Boubbou, I. Kamaoui, M. Maaroufi,
Smoking-related Interstitial Lung Diseases: High-Resolution CT Findings
 Smoking-related Interstitial Lung Diseases: High-Resolution CT Findings Poster No.: C-2358 Congress: ECR 2013 Type: Educational Exhibit Authors: V. Cuartero Revilla, M. Nogueras Carrasco, P. Olmedilla
Smoking-related Interstitial Lung Diseases: High-Resolution CT Findings Poster No.: C-2358 Congress: ECR 2013 Type: Educational Exhibit Authors: V. Cuartero Revilla, M. Nogueras Carrasco, P. Olmedilla
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
October 2012 Imaging Case of the Month. Michael B. Gotway, MD Associate Editor Imaging. Department of Radiology Mayo Clinic Arizona Scottsdale, AZ
 October 2012 Imaging Case of the Month Michael B. Gotway, MD Associate Editor Imaging Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 65-year-old non-smoking woman presented
October 2012 Imaging Case of the Month Michael B. Gotway, MD Associate Editor Imaging Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 65-year-old non-smoking woman presented
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases
 Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
Web Chapter 3. Image Gallery: Lesion detection on low dose chest CT
 Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
The gamut of cystic lung disease: a practical approach to differential diagnosis
 The gamut of cystic lung disease: a practical approach to differential diagnosis Award: Cum Laude Poster No.: P-0100 Congress: ESTI 2014 Type: Educational Poster Authors: C. Leal, R. Santos, J. P. A. Lopes,
The gamut of cystic lung disease: a practical approach to differential diagnosis Award: Cum Laude Poster No.: P-0100 Congress: ESTI 2014 Type: Educational Poster Authors: C. Leal, R. Santos, J. P. A. Lopes,
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
I have no relevant conflicts of interest to disclose
 I have no relevant conflicts of interest to disclose Diffuse parenchymal lung disease (DPLD) and its associations Secondary lobular anatomy DPLD History, clinical findings, temporal evolution, and exposures
I have no relevant conflicts of interest to disclose Diffuse parenchymal lung disease (DPLD) and its associations Secondary lobular anatomy DPLD History, clinical findings, temporal evolution, and exposures
Lung Allograft Dysfunction
 Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
September 2014 Imaging Case of the Month. Michael B. Gotway, MD. Department of Radiology Mayo Clinic Arizona Scottsdale, AZ
 September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
Progress in Idiopathic Pulmonary Fibrosis
 Progress in Idiopathic Pulmonary Fibrosis David A. Lynch, MB Disclosures Progress in Idiopathic Pulmonary Fibrosis David A Lynch, MB Consultant: t Research support: Perceptive Imaging Boehringer Ingelheim
Progress in Idiopathic Pulmonary Fibrosis David A. Lynch, MB Disclosures Progress in Idiopathic Pulmonary Fibrosis David A Lynch, MB Consultant: t Research support: Perceptive Imaging Boehringer Ingelheim
Idiopathic interstitial pneumonias (IIPs) are a group of
 are a group of") SYMPOSIA C. Isabela S. Silva, MD, PhD and Nestor L. Müller, MD, PhD Abstract: The idiopathic interstitial pneumonias (IIPs) are a group of diffuse parenchymal lung diseases of unknown etiology characterized
SYMPOSIA C. Isabela S. Silva, MD, PhD and Nestor L. Müller, MD, PhD Abstract: The idiopathic interstitial pneumonias (IIPs) are a group of diffuse parenchymal lung diseases of unknown etiology characterized
Diagnostic Imaging of Diffuse Infiltrative Disease of the Lung
 Thematic Review Series Respiration 2004;71:4 19 DOI: 10.1159/000075642 Diagnostic Imaging of Diffuse Infiltrative Disease of the Lung Maurizio Zompatori a Claudio Bnà a Venerino Poletti c Enrica Spaggiari
Thematic Review Series Respiration 2004;71:4 19 DOI: 10.1159/000075642 Diagnostic Imaging of Diffuse Infiltrative Disease of the Lung Maurizio Zompatori a Claudio Bnà a Venerino Poletti c Enrica Spaggiari
Boy 8 months TPRC. 21 Sep 06 CXR. Flat and. CLE findings. BPD findings a. Left opacity
 CLE in BPD lung Boy 8 months 17 Sep 06 21 Sep 06 CXR Flat and low position of the diaphragm ICD insertion, right; ET tube slightly shift to the left RUL atelectasis RML hyperinflation, herniating across
CLE in BPD lung Boy 8 months 17 Sep 06 21 Sep 06 CXR Flat and low position of the diaphragm ICD insertion, right; ET tube slightly shift to the left RUL atelectasis RML hyperinflation, herniating across
Typical and atypical findings of pulmonary sarcoidosis at high resolution CT
 Typical and atypical findings of pulmonary sarcoidosis at high resolution CT Poster No.: C-0169 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Raposo Rodríguez, C. Mejía, B. Escobar Mallada,
Typical and atypical findings of pulmonary sarcoidosis at high resolution CT Poster No.: C-0169 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Raposo Rodríguez, C. Mejía, B. Escobar Mallada,
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT
 Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
IPF: Epidemiologia e stato dell arte
 IPF: Epidemiologia e stato dell arte Clinical Classification Diffuse parenchimal lung diseases Exposure-related: - occupational - environmental - medication Desquamative interstitial pneumonia Idiopathic
IPF: Epidemiologia e stato dell arte Clinical Classification Diffuse parenchimal lung diseases Exposure-related: - occupational - environmental - medication Desquamative interstitial pneumonia Idiopathic
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Clinico-Pathologic Conferences Pulmonary Langerhans Cell Histiocytosis and Diabetes Insipidus in a Young Smoker
 Canadian Respiratory Journal Volume 2016, Article ID 3740902, 5 pages http://dx.doi.org/10.1155/2016/3740902 Clinico-Pathologic Conferences Pulmonary Langerhans Cell Histiocytosis and Diabetes Insipidus
Canadian Respiratory Journal Volume 2016, Article ID 3740902, 5 pages http://dx.doi.org/10.1155/2016/3740902 Clinico-Pathologic Conferences Pulmonary Langerhans Cell Histiocytosis and Diabetes Insipidus
Pulmonary Manifestations Of Skeletal Disorders
 Pulmonary Manifestations Of Skeletal Disorders U. A. Saeed, MBBS FCPS, J. Nair, MBBS MD, R. Khosla, MD FRCR, K. Sayegh, MD FRCPC, J. Kosiuk, MD FRCPC, J. Taylor, MD FRCPC; Department of Radiology, McGill
Pulmonary Manifestations Of Skeletal Disorders U. A. Saeed, MBBS FCPS, J. Nair, MBBS MD, R. Khosla, MD FRCR, K. Sayegh, MD FRCPC, J. Kosiuk, MD FRCPC, J. Taylor, MD FRCPC; Department of Radiology, McGill
CTS NEWS. President s Message. Dear members and friends of the California Thoracic Society,
 January 30, 2019 CTS NEWS President s Message Dear members and friends of the California Thoracic Society, I am incredibly honored to be serving as the President of CTS for the next year during such an
January 30, 2019 CTS NEWS President s Message Dear members and friends of the California Thoracic Society, I am incredibly honored to be serving as the President of CTS for the next year during such an
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings
 Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
Pulmonary Manifestations of Systemic Lupus Erythematosus 1
 Pulmonary Manifestations of Systemic Lupus Erythematosus 1 Kee Hyuk Yang, M.D., Yo Won Choi, M.D., Seok Chol Jeon, M.D., Choong Ki Park, M.D., Kyung in Joo, M.D., Chang Kok Hahm, M.D., Seung Ro Lee, M.D.
Pulmonary Manifestations of Systemic Lupus Erythematosus 1 Kee Hyuk Yang, M.D., Yo Won Choi, M.D., Seok Chol Jeon, M.D., Choong Ki Park, M.D., Kyung in Joo, M.D., Chang Kok Hahm, M.D., Seung Ro Lee, M.D.
Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus
 Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus Poster No.: C-1622 Congress: ECR 2012 Type: Scientific Exhibit Authors: C. Cordero Lares, E. Zorita
Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus Poster No.: C-1622 Congress: ECR 2012 Type: Scientific Exhibit Authors: C. Cordero Lares, E. Zorita
Congenital Lung Malformations: Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
The radiological differential diagnosis of the UIP pattern
 5th International Conference on Idiopathic Pulmonary Fibrosis, Modena, 2015, June 12th The radiological differential diagnosis of the UIP pattern Simon Walsh King s College Hospital Foundation Trust London,
5th International Conference on Idiopathic Pulmonary Fibrosis, Modena, 2015, June 12th The radiological differential diagnosis of the UIP pattern Simon Walsh King s College Hospital Foundation Trust London,
The Imaging Analysis of Pulmonary Sarcodiosis
 www.cancercellresearch.org ISSN: 2161-2609 Article The Imaging Analysis of Pulmonary Sarcodiosis Xin He, Chuanyu Zhang* Department of Radiology, Affiliated Hospital of Qingdao University, Qingdao, China
www.cancercellresearch.org ISSN: 2161-2609 Article The Imaging Analysis of Pulmonary Sarcodiosis Xin He, Chuanyu Zhang* Department of Radiology, Affiliated Hospital of Qingdao University, Qingdao, China
Resident Case Review CHEST. Daria Manos CAR 2016
 Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Thoracic Manifestations of Sarcoidosis Using Multi-Slice CT
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 9 Ver. II (Sep. 2015), PP 63-68 www.iosrjournals.org Thoracic Manifestations of Sarcoidosis
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 9 Ver. II (Sep. 2015), PP 63-68 www.iosrjournals.org Thoracic Manifestations of Sarcoidosis
Difficulties Diagnosing Idiopathic Pulmonary Fibrosis
 1. er Encuentro Entre Neumólogos y Radiólogos, Madrid, Spain, 2016, October 14th Difficulties Diagnosing Idiopathic Pulmonary Fibrosis Simon Walsh King s College Hospital Foundation Trust London, United
1. er Encuentro Entre Neumólogos y Radiólogos, Madrid, Spain, 2016, October 14th Difficulties Diagnosing Idiopathic Pulmonary Fibrosis Simon Walsh King s College Hospital Foundation Trust London, United
Histopathologic Approach to Interstitial Lung Disease
 Histopathologic Approach to Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept of Pathology kirk.jones@ucsf.edu Disclosures I have nothing to disclose 1 Why? Much of interstitial lung disease biopsies
Histopathologic Approach to Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept of Pathology kirk.jones@ucsf.edu Disclosures I have nothing to disclose 1 Why? Much of interstitial lung disease biopsies
A Review of Interstitial Lung Diseases. Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco
 A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
How to identify interstitial pneumonias.
 How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
Patient with IPF and no honeycombing on HRCT. Case 1 Demosthenes Bouros, Vasilios Tzilas University of Athens
 Patient with IPF and no honeycombing on HRCT Case 1 Demosthenes Bouros, Vasilios Tzilas University of Athens CASE OVERVIEW A 76-year-old male patient presented with progressive exertional dyspnoea refractory
Patient with IPF and no honeycombing on HRCT Case 1 Demosthenes Bouros, Vasilios Tzilas University of Athens CASE OVERVIEW A 76-year-old male patient presented with progressive exertional dyspnoea refractory
Hypersensitivity Pneumonitis: Spectrum of High-Resolution CT and Pathologic Findings
 CT of Hypersensitivity Pneumonitis Chest Imaging Pictorial Essay C. Isabela S. Silva 1 ndrew Churg 2 Nestor L. Müller 1 Silva CIS, Churg, Müller NL Keywords: high-resolution CT, hypersensitivity pneumonitis,
CT of Hypersensitivity Pneumonitis Chest Imaging Pictorial Essay C. Isabela S. Silva 1 ndrew Churg 2 Nestor L. Müller 1 Silva CIS, Churg, Müller NL Keywords: high-resolution CT, hypersensitivity pneumonitis,
Idiopathic Pulmonary of Care
 Chapter 6.1 Living Medical etextbook A Digital Tool at the Point of Care From Projects In Knowledge Pulmonology Idiopathic Pulmonary Fibrosis @Point of Care IPF Case Study: Typical Presentation, Role of
Chapter 6.1 Living Medical etextbook A Digital Tool at the Point of Care From Projects In Knowledge Pulmonology Idiopathic Pulmonary Fibrosis @Point of Care IPF Case Study: Typical Presentation, Role of
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
A Review of Interstitial Lung Diseases
 Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Pediatric High-Resolution Chest CT
 Pediatric High-Resolution Chest CT Alan S. Brody, MD Professor of Radiology and Pediatrics Chief, Thoracic Imaging Cincinnati Children s s Hospital Cincinnati, Ohio, USA Pediatric High-Resolution CT Short
Pediatric High-Resolution Chest CT Alan S. Brody, MD Professor of Radiology and Pediatrics Chief, Thoracic Imaging Cincinnati Children s s Hospital Cincinnati, Ohio, USA Pediatric High-Resolution CT Short
Disclosures. Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting. Relevant financial relationships: None. Off-label usage: None
 Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
ARTICLE IN PRESS. Ahuva Grubstein a, Daniele Bendayan b, Ithak Schactman c, Maya Cohen a, David Shitrit b, Mordechai R. Kramer b,
 Respiratory Medicine (2005) 99, 948 954 Concomitant upper-lobe bullous emphysema, lower-lobe interstitial fibrosis and pulmonary hypertension in heavy smokers: report of eight cases and review of the literature
Respiratory Medicine (2005) 99, 948 954 Concomitant upper-lobe bullous emphysema, lower-lobe interstitial fibrosis and pulmonary hypertension in heavy smokers: report of eight cases and review of the literature
T he diagnostic evaluation of a patient with
 546 REVIEW SERIES Challenges in pulmonary fibrosis? 1: Use of high resolution CT scanning of the lung for the evaluation of patients with idiopathic interstitial pneumonias Michael B Gotway, Michelle M
546 REVIEW SERIES Challenges in pulmonary fibrosis? 1: Use of high resolution CT scanning of the lung for the evaluation of patients with idiopathic interstitial pneumonias Michael B Gotway, Michelle M
Diffuse Interstitial Lung Diseases: Is There Really Anything New?
 : Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There
: Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There
Review Article Pathologic and Radiologic Correlation of Adult Cystic Lung Disease: A Comprehensive Review
 Hindawi Pathology Research International Volume 2017, Article ID 3502438, 17 pages https://doi.org/10.1155/2017/3502438 Review Article Pathologic and Radiologic Correlation of Adult Cystic Lung Disease:
Hindawi Pathology Research International Volume 2017, Article ID 3502438, 17 pages https://doi.org/10.1155/2017/3502438 Review Article Pathologic and Radiologic Correlation of Adult Cystic Lung Disease:
X-Rays. Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady
 X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
Non-neoplastic Lung Disease II
 Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Thoracic Sarcoidosis Imaging Updated: Jul 19, 2013
 Thoracic Sarcoidosis Imaging Updated: Jul 19, 2013 Overview Radiography Computed Tomography Magnetic Resonance Imaging Nuclear Imaging Show All Multimedia Library References Overview For patients with
Thoracic Sarcoidosis Imaging Updated: Jul 19, 2013 Overview Radiography Computed Tomography Magnetic Resonance Imaging Nuclear Imaging Show All Multimedia Library References Overview For patients with
Thoracic sarcoidosis: Pictoral review of typical and atypical findings
 Thoracic sarcoidosis: Pictoral review of typical and atypical findings Poster No.: C-0804 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: A. Ferreira, J. Calha; Lisbon/PT Keywords: Sarcoidosis,
Thoracic sarcoidosis: Pictoral review of typical and atypical findings Poster No.: C-0804 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: A. Ferreira, J. Calha; Lisbon/PT Keywords: Sarcoidosis,
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than
 TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
IPF - Inquadramento clinico
 IPF - Inquadramento clinico Sergio Harari Unità Operativa di Pneumologia UTIR Servizio di Fisiopat. Resp. e Emodinamica Polmonare Ospedale S. Giuseppe, Milano Clinical Classification Diffuse parenchimal
IPF - Inquadramento clinico Sergio Harari Unità Operativa di Pneumologia UTIR Servizio di Fisiopat. Resp. e Emodinamica Polmonare Ospedale S. Giuseppe, Milano Clinical Classification Diffuse parenchimal
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Monday 10 September Interstitial lung disease 15:10 15:35. The uncommon interstitial lung diseases (ILD)
") Interstitial lung disease 15:10 15:35 The uncommon interstitial lung diseases (ILD) Dr Grant Griffiths, Cwm Taf University Health Board, Cardiff Be familiar with the Diagnostic criteria for idiopathic
Interstitial lung disease 15:10 15:35 The uncommon interstitial lung diseases (ILD) Dr Grant Griffiths, Cwm Taf University Health Board, Cardiff Be familiar with the Diagnostic criteria for idiopathic
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
Journal of Radiology Case Reports
 Reversed Halo Sign on CT as a Presentation of Marcus D Freeman 1*, Joseph R Grajo 1, Neel D Karamsadkar 1, Thora S Steffensen 2, Todd R Hazelton 1 1. Radiology department, Tampa General Hospital, Tampa,
Reversed Halo Sign on CT as a Presentation of Marcus D Freeman 1*, Joseph R Grajo 1, Neel D Karamsadkar 1, Thora S Steffensen 2, Todd R Hazelton 1 1. Radiology department, Tampa General Hospital, Tampa,
Anomalous pulmonary air spaces. Management radiological
 Anomalous pulmonary air spaces. Management radiological Poster No.: C-2608 Congress: ECR 2015 Type: Educational Exhibit Authors: J. C. Quintero Rivera, J. E. Millán Suárez, R. A. Corral Rivadulla, M. F.
Anomalous pulmonary air spaces. Management radiological Poster No.: C-2608 Congress: ECR 2015 Type: Educational Exhibit Authors: J. C. Quintero Rivera, J. E. Millán Suárez, R. A. Corral Rivadulla, M. F.
Cystic Lung Disease: a Comparison of Cystic Size, as Seen on Expiratory and Inspiratory HRCT Scans
 Cystic Lung Disease: a Comparison of Cystic Size, as Seen on Expiratory and Inspiratory HRCT Scans Ki-Nam Lee, MD 1 Seong-Kuk Yoon, MD 1 Seok Jin Choi, MD 2 Jin Mo Goo, MD 3 Kyung-Jin Nam, MD 1 Index words:
Cystic Lung Disease: a Comparison of Cystic Size, as Seen on Expiratory and Inspiratory HRCT Scans Ki-Nam Lee, MD 1 Seong-Kuk Yoon, MD 1 Seok Jin Choi, MD 2 Jin Mo Goo, MD 3 Kyung-Jin Nam, MD 1 Index words:
Clinical History. 29 yo woman with polyhydramnios Cardiac mass at fetal ultrasound At 35 weeks, newborn died 30 minutes after delivery
 CASE 1 a Clinical History 29 yo woman with polyhydramnios Cardiac mass at fetal ultrasound At 35 weeks, newborn died 30 minutes after delivery Interface between tumor and normal myocardium Smaller well-demarcated
CASE 1 a Clinical History 29 yo woman with polyhydramnios Cardiac mass at fetal ultrasound At 35 weeks, newborn died 30 minutes after delivery Interface between tumor and normal myocardium Smaller well-demarcated
Criteria for confident HRCT diagnosis of usual interstitial pneumonia (UIP)
") Criteria for confident HRCT diagnosis of usual interstitial pneumonia (UIP) Assem El Essawy (1) & Amr A. Nassef (٢) Abstract Identification of interstitial pneumonia (IP) was mainly based on histological
Criteria for confident HRCT diagnosis of usual interstitial pneumonia (UIP) Assem El Essawy (1) & Amr A. Nassef (٢) Abstract Identification of interstitial pneumonia (IP) was mainly based on histological
Radiolucent Pulmonary Lesions: An Update And Diagnostic Problems
 Radiolucent Pulmonary Lesions: An Update And Diagnostic Problems Poster No.: C-2566 Congress: ECR 2013 Type: Educational Exhibit Authors: A. B. Veas-Lopez, A. Sánchez González, M. L. Rodriguez Rodriguez,
Radiolucent Pulmonary Lesions: An Update And Diagnostic Problems Poster No.: C-2566 Congress: ECR 2013 Type: Educational Exhibit Authors: A. B. Veas-Lopez, A. Sánchez González, M. L. Rodriguez Rodriguez,
Role of Computed Tomography in Diagnosis of Diffuse Lung Diseases Chauhan Jayant 1*, Panchal Pankaj 2, Faruqui Tehzeeb 3
 ORIGINAL ARTICLE Role of Computed Tomography in Diagnosis of Diffuse Lung Diseases Chauhan Jayant 1*, Panchal Pankaj 2, Faruqui Tehzeeb 3 1 MD,DTCD,Additional Professor& HOD, 2,3 MBBS, 3 rd year resident
ORIGINAL ARTICLE Role of Computed Tomography in Diagnosis of Diffuse Lung Diseases Chauhan Jayant 1*, Panchal Pankaj 2, Faruqui Tehzeeb 3 1 MD,DTCD,Additional Professor& HOD, 2,3 MBBS, 3 rd year resident
Coexistence of Lymphangioleiomyomatosis and Angiomyolipomas in a Patient of Tuberous Sclerosis Complex: a case report
 Chin J Radiol 2003; 28: 329-333 329 Coexistence of Lymphangioleiomyomatosis and Angiomyolipomas in a Patient of Tuberous Sclerosis Complex: a case report FENG-CHI HSIEH 1 KAO-LANG LIU 1 YIH-LEONG CHANG
Chin J Radiol 2003; 28: 329-333 329 Coexistence of Lymphangioleiomyomatosis and Angiomyolipomas in a Patient of Tuberous Sclerosis Complex: a case report FENG-CHI HSIEH 1 KAO-LANG LIU 1 YIH-LEONG CHANG