EUS-FNAB of GI Tract: Specimen Handling and Triage
|
|
|
- Emmeline Golden
- 5 years ago
- Views:
Transcription

1 EUS-FNAB of GI Tract: Specimen Handling and Triage Amy Ly, M.D. Director, Fine Needle Aspiration Service Massachusetts General Hospital Assistant Professor of Pathology Harvard Medical School Boston, MA

2 Goal of EUS-FNA is Diagnosis Gastrointestinal Stromal Tumor (GIST) in gastric fundus If definitive diagnosis not rendered, aim to provide some pathology information to triage patient for management.
3 High Quality FNAB High Quality Specimen High cellularity Cells representative of the lesion Quality preparations High Quality Interpretation Training of interpreter Experience of interpreter Team approach to diagnosis
 Move the needle back and forth within the nodule to obtain the sample Release vacuum in syringe")
4 FNAB procedure gauge needle & 10 cc syringe to apply vacuum Insert needle into target under US guidance Apply suction with the plunger (to generate vacuum) Move the needle back and forth within the nodule to obtain the sample Release vacuum in syringe



5 FNAB procedure cont d Expel material onto glass slides Smear and immediately fix with alcohol Fix blood clots and tissue fragments in formalin for cell block preparation Rinse needle in Cytolyt or CytoRich Red for LBC; Rinse in saline or RPMI for flow cytometry

6 EUS-guided FNAB U/S Transducer Color Doppler Aspiration needle Transmural aspiration Cytology specimen Transesophageal: esophageal wall, lymph nodes Transgastric: gastric wall, pancreatic body and tail, lymph nodes Transduodenal: duodenal wall, pancreatic head, lymph nodes



7 Cytology Specimen Preparation 1. Direct Smears (ROSE) Alcohol fixed Air dried 2. Cytospin Fresh fluid 3. Liquid Based Prep Alcohol-Fixed cells ThinPrep SurePath

8 Cytology Specimen Preparation 4. Cell block Formalin-fixed paraffin-embedded Rinsings and dedicated pass into RPMI or formalin Enrich with larger bore needle If cellularity is scant, process fluid as cytospin, ThinPrep, or SurePath 5. Flow cytometry - Rinse in media if lymphoma is suspected
9 Standardized Reporting Terminology (Papanicolaou Society of Cytopathology) I. Nondiagnostic II. Negative: Normal tissue, benign conditions III. Atypical: Suggestive but not diagnostic of low grade neoplasm (e.g. neuroendocrine tumor); indeterminate bile duct lesions IV. Neoplastic: -Benign neoplasm (e.g. serous cystadenoma) -Other (e.g. mucinous cystic neoplasm) V. Suspicious: Suggestive but not diagnostic of malignancy VI. Positive/Malignant


10 Direct Smears: fast, easy, and inexpensive
11 Preparing Direct Smears Goal: Create a monolayer of cells for ease of interpretation At least 2 smears made per FNAB pass - Alcohol fixation for nuclear detail - Rapid H&E stain often used for ROSE FNA material contains delicate tissue fragments do not crush! Spreader Slides should have little to no material on it, and can be discarded.





12 Slides for Direct Smears Frosted slides Non- Frosted slides
13 Best Method for Direct smears Apply gentle pressure and pull spreader slide towards yourself. XYZ XYZ XYZ XYZ spreader slide

14 Best Method for Direct smears Deposit the sample on slide Needle and syringe with aspirated specimen material Use syringe to express the material onto glass slide
15 Best Method for Direct smears Use perpendicular slides to open the aspirate drop. Do not crush the sample. Ideal method as described by Britt-Marie Ljung Copyright 2008 by ASCP
16 Best Method for Direct smears Advantages: Allows separation of material into multiple smears Preserves cellular and architectural detail Perfect ovals- easier to screen at the time of biopsy Practice smearing hand cream and a box of slides Copyright 2008 by ASCP

17 Rapid H&E staining kit for Direct Smears

18 Rapid H&E Direct Smears
19 Less optimal direct smear preparation: Pull apart method Apply gentle pressure and slide apart in parallel. This method is best for peripheral blood smears.


20 Less optimal direct smear preparation: Pop method Pull apart and Pop methods are suboptimal - Entire aspirate is used up on two slides - Increased distortion, too thick for interpretation, loss of architecture and cellular detail

 Rapid Pap similar")

21 Staining Direct Smears Rapid H&E Alcohol fixed smear Easier to interpret Nuclear detail Slower (2-3 min) Rapid Pap similar Diff-Quik Air dried smear Harder to interpret Cytoplasmic detail Faster (30 seconds)



22 Liquid Based- Cytospin Preferred method of processing fresh cyst fluid Provides cell button for cytology and supernatant for CFA Preserves background elements



23 Liquid Based-ThinPrep Cells are fixed in methanol Cannot use aliquot for flow cytometry, but IHC is OK DNA quality for molecular studies is good



24 Liquid Based SurePath Prep Cells are fixed in ethanol Cannot use aliquot for flow cytometry, but IHC is OK DNA quality for molecular studies is good

25 Specimen Quality Quality of cells: Are they viable? Necrosis



26 Specimen Quality Quality of preparation: Interpretable? Crush Artifact: Cells delicate; excess pressure on smears Air-dry Artifact: Drying began before put into alcohol fixative Obscuring blood


27 Specimen Quality Is sample representative of the lesion? Epithelial cells from surface of esophagus, stomach, or duodenum Mucus from GI tract GI contamination is a significant problem

28 Sclerosis Benign Cancer


29 Specimen Quality Quantity of cells Scant cellularity Precludes definitive interpretation Largely blood Too few cells; Atypical, not maligant


30 Cytology vs. Histology Cytology: The study of cells Histology: The study of tissue
31 Limitations of Cytology compared to Histology Lack of architecture Cannot see distribution of ductal structures Cannot see abnormal localization Cannot see if ducts are adjacent to medium sized vessels, wrapping around nerves or isolated in fat Cannot see contours or angulation of ducts Cannot see luminal contents Cannot see stromal reaction

32 Tissue worm

33 Tissue worm left on a Direct Smear


34 Cell Blocks for Cytohistology IPMN-HGA IPMN-LGA Tissue worms are perfect for Cell Block preparations


35 Cell Blocks for Cytohistology Any material left in the syringe can be used for cell block preparation. Wait for it to clot before disturbing it. Gently wash the clot into formalin and submit to pathology for cell block preparation. Use separate container for core biopsy.


36 Cell Blocks for Cytohistology Autoimmune pancreatitis Poorly-differentiated PDAC


37 Cell Blocks for Cytohistology Pancreas- Solid Pseudopapillary Neoplasm Immunohistochemical staining with Beta-Catenin




38 Cell Blocks prepped like Core Biopsies




39 SharkCore (Medtronic)


40 Next Generation Needles in EUS-FNA Acquire (Boston Scientific)


41 Procore Biopsy (Cook-Medical) IPMN-LGD

42 Moray Micro-forceps biopsy (US Endoscopy)





43 Cell Blocks/Core Biopsy Allow for ancillary testing: IHC, molecular etc Poorly differentiated metastatic lung adenocarcinoma
44 Ancillary Testing Refines Diagnosis Special Stains Cellblocks; Smears Immunohistochemistry Cellblocks; Smears Biochemical testing Pancreas cyst fluid: CEA, amylase Molecular Analysis [FISH, Specific Mutations (e.g. KRAS, BRAF) and NGS] Cellblocks Fresh cyst fluid- Pancreas Liquid-Based Cytology (ThinPrep/SurePath)
45 Quality Cytology Quality of the Specimen Quantity of cells Quality of the cells Tissue available for ancillary studies Quality of the interpretation Training of the interpreter Experience of the interpreter Rapid or immediate interpretation Cooperation of the diagnostic team
46 Quality Interpretation Pathologist trained in cytology Preferably with boards in cytopathology Pathologist experienced in the interpretation of FNAB material, particularly from GI tract via EUS Team approach to diagnosis Cooperative interaction between biopsy physician and interpretation group (cytotechnologist and pathologist)
47 Cytology Interpretation Multimodal Approach Patient clinical Information Age and gender Symptoms Past medical history Radiological Information Location of mass (and organ traversed for EUS) Mass characteristics Solid or cystic» Size, contours, invasion» Cystic lesions: single or multilocular; wall thickness, Ca++, intramural nodule» Gross cyst contents: thick/viscous, thin/watery, clear, brown Ancillary tests: CEA, amylase, molecular analysis

48 Quality Interpretation: Familiarity with GI Contamination Transgastric: pancreatic body and tail Transduodenal: pancreatic head

49 Normal Pancreas (bivalved pancreatic head) Courtesy of 4 th Series AFIP Fascicle on Tumors of the Pancreas

50 Normal Pancreas


51 Normal Pancreas Acinar Cells


52 Normal Pancreas Ductal Cells

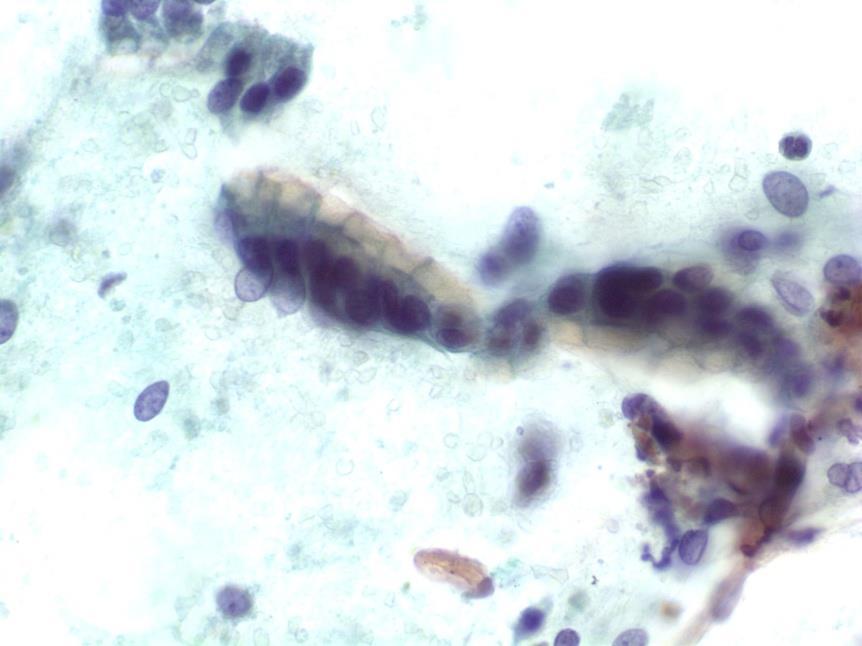
53 Gastric Contamination


54 Duodenal Contamination


55 Solid Differential Diagnosis of Solid Pancreatic Masses Chronic pancreatitis Ductal adenocarcinoma Metastasis Pancreatic neuroendocrine tumor CP Acinar cell carcinoma Pancreatoblastoma Solid-pseudopapillary neoplasm Images: AFIP Pancreas fascicle 2007


56 Differential Diagnosis of Solid Pancreatic Masses Solid Chronic pancreatitis Ductal adenocarcinoma Metastasis Pancreatic neuroendocrine tumor Acinar cell carcinoma Solid-pseudopapillary neoplasm Images: AFIP Pancreas fascicle 2007


57 High Grade Adenocarcinoma Marked nuclear atypia hyperchromasia pleomorphism overlapping Prominent nucleoli Single atypical cells Mitoses Coagulative Necrosis

58 Drunken Honeycomb Anisonucleosis (4:1) Parachromatin clearing Nuclear membrane irregularity

59 Parachromati c eari g Nuc ear cro di g Irregu ar uc ear membra es Visib e cytop asmic muci

60 Dru ke ho eycomb Exaggerated vacuo ated cytop asm

61 Well-differentiated Adenocarcinoma Cell block preparation of needle rinsings

 -Background")

62 Key Cytologic Features: -Fragments of acinar tissue with acini splayed apart by fibrosis -Stromal fragments -Inflammatory cells (lymphocytes, plasma cells, macrophages and siderophages) -Background debris and calcification -Ductal epithelium with only mild cytologic atypia -No definite features of neoplasia Chronic Pancreatitis


63 Autoimmune Pancreatitis: Mass Forming Lesion

64 Autoimmune Pancreatitis Deshpande V, Mino-Kenudson M, Brugge WR, Pitman MB, Castill CF, Warshaw AL Lauwers GY. Am J Surg Pathol. 2005; 29;


65 AIP: Core Biopsy Type 1 Type 2


66 Benign vs Malignant Acinar Cell Population Benign Malignant


 +/-")
67 Acinar Cell Carcinoma Cohesive groups and single cells Many stripped naked nuclei Granular cytoplasm (and background) +/- nucleoli Direct Smears



68 Acinar Cell Carcinoma Cell Block Trypsin+ Endocrine markers-



69 Direct Smears Solid Pseudopapillary Neoplasm Papillary branching Myxoid stroma Clinging cells and single cells Euchromatin Oval, indented, grooved nuclei Perinuclear vacuoles/globules



70 Spenule/accessory spleen Lymphoid tissue Histiocytes Blood vessels CD8+ cells indicating splenic endothelial cells Direct Smear Cell Block



71 Classic Pancreatic Neuroendocrine Tumor Single cells mostly Plasmacytoid Coarse, stippled chromatin -/+ nucleoli Chromogranin+
 Gross examination 2) CEA (best test) 3) Cytology B.")
72 Special Case: Cyst Fluid Evaluation A. Is the cyst mucinous or not? 1) Gross examination 2) CEA (best test) 3) Cytology B. Is the cyst low- or high-grade? Cytology!!
 Cystic degeneration of typically solid tumors PanNET SPN other Other more rare cysts radiologyassistant.")
73 Pancreatic Cysts Differential Diagnosis Pseudocyst Lymphoepithelial cyst Serous cyst Mucinous cyst (MCN and IPMN) Cystic degeneration of typically solid tumors PanNET SPN other Other more rare cysts radiologyassistant.nl
74 Management Options Surgical Distal pancreatectomy Middle pancreatectomy Pancreatoduodenectomy (Whipple) Medical Drain Ablate Observation
75 Current Recommendations for Pancreatic Cyst Management Surgery-recommended MCN, all grades IPMN-HGD IPMN-invasive Cystic PanNET SPN Cystic Acinar Cell Ca. Cystic PDAC Surgery-optional PCT LEC SCA IPMN-LGD IPMN-IGD?? Cytology is critical for cyst classification and management. Decision to operate is based on surgical risk vs malignancy risk.
76 Surgical procedures Whipple Middle pancreatectomy Distal pancreatectomy Other Frequency, (%) 368, (43.2%) 63, (7.4%) 373, (43.8%) 47, (5.5%) Complications (%) 40% 49.2% 36.4% 32.4% Pancreatic fistula 12.5% 35.5% 18.2% 8.8% Delayed gastric emptying 6.5% 0% 0.3% 0% Other major complication 12.9% 12.7% 12.6% 11.8% Median length of stay, days 8 days 6 days 6 days 8 days Operative mortality, n
77 Outcomes MCN MD IPMN BD IPMN SCA CNET SPN n Malignant (%) 10.3% 33.7% 13.7% 0.0% 10.7% 0.0% Outcome 3-year survival (%) 94.0% 83.0% 88.0% 97.0% 98.0% 100.0% 5-year survival (%) 90.0% 78.0% 80.0% 90.0% 98.0% 100.0%








78 Pancreatic Cysts: CT unilocular Simple cysts PCT BD-IPMN w/ LGD MCN w/ LGD Benign imaging multilocular complex SCA BD-IPMN w/ LGD Benign to Worrisome imaging Small or non-enhancing MN: IPMN with HGD MCN w/ inv. Ca. IPMN w/ inv. Ca. SPN Worrisome to High-risk imaging cpannet

79 Worrisome Imaging Cyst > 3cm EUS Recommended (2012 guidelines) Thickened/enhanced cyst walls MPD 5-9 mm Nonenhancing mural nodule Abrupt change in caliber of MPD with distal atrophy

80 Nonspecific EUS Imaging Broad differential diagnosis: Mucinous BD-IPMN MCN Nonmucinous Macrocystic SCA Lymphangioma Benign Malignant ( HGD)



81 Challenges in Cyst Characterization: Morphologic Overlap MCN Pseudocyst IPMN Cohen-Scali F et al. Radiolgy 2003 Khurana B et al. AJR 2003 Kim S et al. AJR 2006
82 Cystic Pancreatic Neuroendocrine Tumors: The Value of Cytology in Pre-Operative Diagnosis Vicente Morales-Oyarvide MD, Won Jae Yoon, MD2, Thun Ingkakul MD, David G Forcione MD, Brenna Casey, MD, William R Brugge MD, Carlos Fernández-del Castillo MD, and Martha B Pitman MD Cancer Cytopathology. 2014; 122: TABLE 2. Accuracy of Cytology and EUS for the Diagnosis of Cystic Pancreatic Neuroendocrine T N Diagnostic Suspicious HR Benign or indeterminate Cytology 35 71% 77% 86% 5% EUS 34 38% 47% 56% 15% Key: EUS, endoscopic ultrasound; HR, high-risk


83 Pancreatic Cyst Fluid Mucinous cyst fluid: Thick and viscous Pseudocyst fluid: Thin, watery, brown
84 CEA by cyst fluid analysis ng/ml Serous Inflammatory Mucinous Borderline Malignant thology
85 CEA and Amylase: Key Points Elevated CEA ( 192 ng/ml) supports a mucinous cyst Does not distinguish IPMN from MCN Level does not correlate with malignancy Rare FP: PCT, GI duplication cyst, LEC Amylase levels Elevated in the 1000 s for most PCT Low amylase level tends to exclude a PCT Level does not distinguish IPMN from MCN

86 Direct Smear Preparation: Acellular thick mucin
87 Mucin appears stringy on LBC processing




88 Atypical Glandular Cells



89 Low Grade High Grade High-Grade Atypical Epithelial Cells in Pancreatic Mucinous Cysts are a More Accurate Predictor of Malignancy than Positive Cytology Martha Bishop Pitman M.D, et.al. (Cancer Cytopath 2010)

90 Cytological Preparations from Cysts No ROSE Direct smears if fluid thick enough Send Fresh undiluted cyst fluid for: CEA; Amylase Molecular Cytology Cytospin Cellblock
91 Pancreatic Cyst Fluid Triage
92 Impact of Next-Generation Sequencing on the Clinical Impression of Pancreatic Cysts Martin Jones, MBBS 1*, Zongli Zheng, MD, PhD 1*, Jessica Wang, MD 1, Emily Albanese 1, Abdurrahman Kadayifci, MD 2, Dora Dias- Santagata, PhD 1, Long Le, MD 1, William R. Brugge, MD 2, Carlos Fernandez-del Castillo, MD 3, Mari Mino-Kenudson 1, MD, A. John Iafrate, MD, PhD 1^, and Martha Pitman, MD 1^ States *Co-first authors ^Co-senior authors Gastrointestinal Endoscopy (in press) 1 Massachusetts General Hospital, Department of Pathology, Boston, MA, United States 2 Massachusetts General Hospital, Department of Medicine, Boston, MA, United States 3 Massachusetts General Hospital, Department of Surgery, Boston, MA, United NGS supported the imaging impression in 78% but changed it in 12% NGS defined a cyst as mucinous in 48% of cysts with a nonelevated CEA KRAS and/or GNAS mutations supported a diagnosis of IPMN in 71% of cases without an elevated CEA KRAS mutation reclassified 19% of cysts non-neoplastic by imaging and with low CEA


93 Imaging Nonspecific Thick cyst wall Solid and cystic Cytology is THE diagnostic test CEA low Amylase low KRAS/GNAS negative Cells usually diagnostic when present Cystic PanNETS Cystic Pancreatic Neuroendocrine Tumors: The Value of Cytology in Pre-Operative Diagnosis Vicente Morales-Oyarvide MD 1, Won Jae Yoon, MD 2, Thun Ingkakul MD 1, David G Forcione MD 3, Brenna Casey, MD 3, William R Brugge MD 3, Carlos Fernández-del Castillo MD 1, Martha B Pitman MD 4 Cancer Cytopathology, 2014; 122:


94 PanNET Cytohistology: Cell Block cpannet Synaptophysin




95 Serous Cystadenoma Smear Cell Block Smear Smear


96 Serous Cystadenoma Cuboidal non-mucinous epithelial cells Hemosiderin-laden macrophages in a clean or bloody, nonpseudocyst like background CEA and amylase low NO KRAS/GNAS 3p deletions support diagnosis



97 Cytohistology: Cell Block Serous Cystadenoma PAS/D


98 Pancreatic Pseudocyst cytology cytospin smear cyst debris, blood, proteinaceous material and yellow hematoidin-like pigment variable inflammation NO cyst lining epithelium CEA low; amylase usually in the 1000 s; no KRAS or GNAS


99 Lymphoepithelial cyst Anucleate squames and abundant keratinous debris Mature superficial squamous cells Lymphocytes are usually present but amount is variable and may be quite scant +/-Cholesterol clefts

100 Cytology Smears for NGS
Advances in Pancreatic. Cytology. Martha B. Pitman, MD. Disclosure of Relevant Financial Relationships
 Advances in Pancreatic Cytology Martha B. Pitman, MD Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Advances in Pancreatic Cytology Martha B. Pitman, MD Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1. Case 1: EUS Report 5/1/2017. Interesting Cases of Pancreatic Masses
 Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Pancreatico-biliary cytology: a practical approach to diagnosis. Corina Cotoi
 Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
EUS-guided FNAB. Differential Diagnosis 3/14/2018. EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses
 EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
Video Microscopy Tutorial 19
 Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
EUS-guided FNAB. Differential Diagnosis 5/1/2017. EUS-FNA of Solid and Cystic Lesions:
 EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
Pancreatic Cysts. Pancreatic Cysts. Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts
 Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts Martha Bishop Pitman, M.D. Director of Cytopathology Massachusetts General Hospital Professor of Pathology Harvard
Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts Martha Bishop Pitman, M.D. Director of Cytopathology Massachusetts General Hospital Professor of Pathology Harvard
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget
 Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Standardization of Nomenclature
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT
 CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
Conflicts of Interest
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital
 Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas
 Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview
An Approach to Pancreatic Cysts. Introduction
 An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS
 ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Objectives. Pancreatic Cysts. Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses
 Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
Matthew McCollough, M.D. April 9, 2009 University of Louisville
 Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts
 Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Pancreatic Cysts. Darius C. Desai, MD FACS St. Luke s University Health Network
 Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
ROSE in EUS guided FNA of Pancreatic Lesions
 ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
DOWNLOAD ENTIRE DOCUMENT FROM
 PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Specimen Collection. Special Collections Fine Needle Aspiration (FNA) Cytology. Laboratory Services April 2017
 Cytology. Laboratory Services April 2017") 1 Specimen Collection Special Collections Fine Needle Aspiration (FNA) Cytology Laboratory Services April 2017 Agenda Before You Begin Collection Smearing Technique Packaging & Transport Proper vs. Improper
1 Specimen Collection Special Collections Fine Needle Aspiration (FNA) Cytology Laboratory Services April 2017 Agenda Before You Begin Collection Smearing Technique Packaging & Transport Proper vs. Improper
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions
 Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
EBUS-FNAB: HOW TO OPTIMIZE YOUR CYTOLOGY SAMPLES, LHSC EXPERIENCE. Dr. Mariamma Joseph Division Head of Cytopathology LHSC and Western University
 EBUS-FNAB: HOW TO OPTIMIZE YOUR CYTOLOGY SAMPLES, LHSC EXPERIENCE Dr. Mariamma Joseph Division Head of Cytopathology LHSC and Western University Objectives Brief overview of EBUS-FNA Strategies to optimize
EBUS-FNAB: HOW TO OPTIMIZE YOUR CYTOLOGY SAMPLES, LHSC EXPERIENCE Dr. Mariamma Joseph Division Head of Cytopathology LHSC and Western University Objectives Brief overview of EBUS-FNA Strategies to optimize
Pancreatic Cystic Neoplasms: Guidelines and beyond
 Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases
 Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
Cytopathology Study Day 16 April RCPath - BAC. Digital cytology: EUS FNA pancreas and head and neck
 Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA. Leena Krogerus Helsinki, FINLAND
 Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
Thyroid follicular neoplasms in cytology. Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia
 Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
INTRODUCTION TO PATHOLOGICAL TECHNIQUES. 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH)
") INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
Management A Guideline Based Approach to the Incidental Pancreatic Cysts. Common Cystic Pancreatic Neoplasms.
 Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes
 Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Abstract. Introduction. Salah Abobaker Ali
 Sensitivity and specificity of combined fine needle aspiration cytology and cell block biopsy versus needle core biopsy in the diagnosis of sonographically detected abdominal masses Salah Abobaker Ali
Sensitivity and specificity of combined fine needle aspiration cytology and cell block biopsy versus needle core biopsy in the diagnosis of sonographically detected abdominal masses Salah Abobaker Ali
Cytology Specimen Management, Triage and Standardized Reporting of Fine Needle Aspiration Biopsies of the Pancreas
 Cytology Specimen Management, Triage and Standardized Reporting of Fine Needle Aspiration Biopsies of the Pancreas The Harvard community has made this article openly available. Please share how this access
Cytology Specimen Management, Triage and Standardized Reporting of Fine Needle Aspiration Biopsies of the Pancreas The Harvard community has made this article openly available. Please share how this access
Outline. Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines
 Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines") Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
State of the Art Symposium
 State of the Art Symposium Syed Z. Ali, MD There is no disclosure necessary Martha B. Pitman, MD There is no disclosure necessary Lester Layfield, MD There is no disclosure necessary Joseph Herman, MD
State of the Art Symposium Syed Z. Ali, MD There is no disclosure necessary Martha B. Pitman, MD There is no disclosure necessary Lester Layfield, MD There is no disclosure necessary Joseph Herman, MD
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Cystic Pancreatic Lesions: Approach to Diagnosis
 Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
Workshop 9. Cytopathology of Solid and Cystic Neoplasms of the Pancreas: Everything You Need To Know For Daily Practice.
 Workshop 9 Cytopathology of Solid and Cystic Neoplasms of the Pancreas: Everything You Need To Know For Daily Practice Michelle Reid, MD Momin Siddiqui, MD,FIAC There are no disclosures necessary. Cytopathology
Workshop 9 Cytopathology of Solid and Cystic Neoplasms of the Pancreas: Everything You Need To Know For Daily Practice Michelle Reid, MD Momin Siddiqui, MD,FIAC There are no disclosures necessary. Cytopathology
Biliary cytolgy and pancreatic endoscopic ultrasound-guided. Helsinki, FINLAND
 Biliary cytolgy and pancreatic endoscopic ultrasound-guided d FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology Obstructions PSC, a premalignant condition, the cure of which is transplantation
Biliary cytolgy and pancreatic endoscopic ultrasound-guided d FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology Obstructions PSC, a premalignant condition, the cure of which is transplantation
Types of IPMN. Pancreas Cysts: An Incidental Finding or Harbinger of Malignancy. Cysts: Early Neoplasia. Mucinous Cystic Lesions. EUS-guided FNA EUS
 Pancreas Cysts: An Incidental Finding or Harbinger of Malignancy EUS-guided FNA William R. Brugge,, MD, FACG Professor of Medicine Harvard Medical School Director, GI Endoscopy Unit Massachusetts General
Pancreas Cysts: An Incidental Finding or Harbinger of Malignancy EUS-guided FNA William R. Brugge,, MD, FACG Professor of Medicine Harvard Medical School Director, GI Endoscopy Unit Massachusetts General
Ultrasound-guided FNA Biopsy. American Thyroid Association 2017
 Ultrasound-guided FNA Biopsy American Thyroid Association 2017 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel School of Medicine at Dartmouth University Disclosures: No relevant
Ultrasound-guided FNA Biopsy American Thyroid Association 2017 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel School of Medicine at Dartmouth University Disclosures: No relevant
Pancreatic malignant tumors are the fifth leading cause of cancerrelated
 44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD
 CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
Pancreatic neoplasms associated with significant amounts of extracellular. Fine-Needle Aspiration Cytology of Mucinous Tumors of the Pancreas CANCER
 92 CANCER CYTOPATHOLOGY Fine-Needle Aspiration Cytology of Tumors of the Pancreas Monica Recine, M.D. 1 Madhukar Kaw, M.D. 2 Douglas B. Evans, M.D. 3 Savitri Krishnamurthy, M.D. 1 1 Division of Pathology
92 CANCER CYTOPATHOLOGY Fine-Needle Aspiration Cytology of Tumors of the Pancreas Monica Recine, M.D. 1 Madhukar Kaw, M.D. 2 Douglas B. Evans, M.D. 3 Savitri Krishnamurthy, M.D. 1 1 Division of Pathology
Biliary Tract Neoplasia: A Cyto-histologic Review. Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital
 Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
SPECIMEN PREPARATION AND ADEQUACY OF THE MATERIAL
 SPECIMEN PREPARATION AND ADEQUACY OF THE MATERIAL Guido FADDA, MD, MIAC Head, Cytopathology Section Department of Anatomic Pathology and Laboratory Medicine Agostino Gemelli School of Medicine and Hospital
SPECIMEN PREPARATION AND ADEQUACY OF THE MATERIAL Guido FADDA, MD, MIAC Head, Cytopathology Section Department of Anatomic Pathology and Laboratory Medicine Agostino Gemelli School of Medicine and Hospital
LGM International, Inc.
 Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
FNA thyroid. Thyroid FNA accuracy. Thyroid FNA And Cytopathology. Variability in FNA sampling via palpation
 Thyroid FNA And Cytopathology University of California, San Francisco FNA thyroid Wide range of accuracy- causes Overview of tools and sampling Preparation techniques Impact of US guidance Impact of training
Thyroid FNA And Cytopathology University of California, San Francisco FNA thyroid Wide range of accuracy- causes Overview of tools and sampling Preparation techniques Impact of US guidance Impact of training
AACE/ACE Advanced Neck Ultrasound Training Course
 AACE/ACE Advanced Neck Ultrasound Training Course Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel School of Medicine at Dartmouth University No Disclosures Goals of FNA Obtain
AACE/ACE Advanced Neck Ultrasound Training Course Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel School of Medicine at Dartmouth University No Disclosures Goals of FNA Obtain
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Salivary Gland FNA ATYPICAL : Criteria and Controversies
 Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Objectives. Intraoperative Consultation of the Whipple Resection Specimen. Pancreas Anatomy. Pancreatic ductal carcinoma 11/10/2014
 Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Dr. Issraa Ali Hussein
 CLINICAL 09888888;rCYTOLOGY Dr. Issraa Ali Hussein objectives Define diagnostic cytology (clinical cytology). Explain the differences between histopathology and cytopathology. Recognize the methods for
CLINICAL 09888888;rCYTOLOGY Dr. Issraa Ali Hussein objectives Define diagnostic cytology (clinical cytology). Explain the differences between histopathology and cytopathology. Recognize the methods for
Cytological evaluation of effusion fluid with cell block technique and cytology smears among Sudanese patients
 EUROPEAN ACADEMIC RESEARCH Vol. IV, Issue 3/ June 2016 ISSN 2286-4822 www.euacademic.org Impact Factor: 3.4546 (UIF) DRJI Value: 5.9 (B+) Cytological evaluation of effusion fluid with cell block technique
EUROPEAN ACADEMIC RESEARCH Vol. IV, Issue 3/ June 2016 ISSN 2286-4822 www.euacademic.org Impact Factor: 3.4546 (UIF) DRJI Value: 5.9 (B+) Cytological evaluation of effusion fluid with cell block technique
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES)
") SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES) Dr. Mariamma Joseph Professor of Pathology Division Head Cytopathology Department of Pathology and Laboratory Medicine LHSC and Western University
SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES) Dr. Mariamma Joseph Professor of Pathology Division Head Cytopathology Department of Pathology and Laboratory Medicine LHSC and Western University
The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms
 JOP. J Pancreas (Online) 20 Mar 20; (2):-9. RESEARCH ARTICLE The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms Megan Winner, Amrita Sethi 2, John M Poneros
JOP. J Pancreas (Online) 20 Mar 20; (2):-9. RESEARCH ARTICLE The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms Megan Winner, Amrita Sethi 2, John M Poneros
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
EUS-FNA OF PANCREATIC EXOCRINE TUMORS COMPARISON OF EXPERIENCES WITH PATHOLOGICAL DIAGNOSIS
 EUS-FNA OF PANCREATIC EXOCRINE TUMORS COMPARISON OF EXPERIENCES WITH PATHOLOGICAL DIAGNOSIS Vincenzo Canzonieri, M.D. CRO - Aviano National Cancer Institute Dept of Pathology EUS European Cyto-Pathologist
EUS-FNA OF PANCREATIC EXOCRINE TUMORS COMPARISON OF EXPERIENCES WITH PATHOLOGICAL DIAGNOSIS Vincenzo Canzonieri, M.D. CRO - Aviano National Cancer Institute Dept of Pathology EUS European Cyto-Pathologist
Original article. Introduction!
 382 Original article Peritoneal seeding in intraductal papillary mucinous neoplasm of the pancreas patients who underwent endoscopic ultrasound-guided fine-needle aspiration: The PIPE Study Authors Won
382 Original article Peritoneal seeding in intraductal papillary mucinous neoplasm of the pancreas patients who underwent endoscopic ultrasound-guided fine-needle aspiration: The PIPE Study Authors Won
Proceeding of the SEVC Southern European Veterinary Conference
 www.ivis.org Proceeding of the SEVC Southern European Veterinary Conference Oct. 17-19, 2008 Barcelona, Spain http://www.sevc.info Reprinted in the IVIS website with the permission of the SEVC www.ivis.org
www.ivis.org Proceeding of the SEVC Southern European Veterinary Conference Oct. 17-19, 2008 Barcelona, Spain http://www.sevc.info Reprinted in the IVIS website with the permission of the SEVC www.ivis.org
"Atypical": Criteria and
 "Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
"Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy.
 November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
DIAGNOSTIC DILEMMA. Case Reports Clinical history. Materials and Methods
 DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
ASCP Competency Assessment
 ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits
 in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits") ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits Charitini Salla, MD Head of Cytopathology Department, Hygeia Hospital, Athens, Greece There is
ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits Charitini Salla, MD Head of Cytopathology Department, Hygeia Hospital, Athens, Greece There is
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,