Conflicts of Interest
|
|
|
- Blanche Smith
- 5 years ago
- Views:
Transcription
1 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology & Anatomical Sciences Columbia, MO Conflicts of Interest None 1
2 The Pathology Report Legal document of communication between pathologist and clinician Communicates the results of testing Provides information for patient treatment and management Is very much non-standardized in AP Among physicians around the world Among physicians in the same country Among physicians in the same department Pathology Nomenclature Must provide clinically relevant information to the treating physician to allow for proper patient management Should be uniform among pathologists and universally understood by clinicians Must reflect our current understanding of the relevant disease entities 2
3 Standardization of Nomenclature Unifies reporting of disease categories Reduces interobserver variability Improves intraobserver reproducibility Better aligns patient management options with interpretations Improves patient care History of Developing Guidelines for Cytopathology The Papanicolaou Society of Cytopathology Task Force on Standards of Practice. Guidelines of the Papanicolaou Society of Cytopathology for the examination of fine needle aspiration specimens from thyroid nodules. Diagn Cytopathol 1996;15: The Papanicolaou Society of Cytopathology Task Force on Standards of Practice. Guidelines of the Papanicolaou Society of Cytopathology for fine-needle aspiration procedure and reporting. Mod Pathol 1997;10: The Papanicolaou Society of Cytopathology Task Force on Standards of Practice. Guidelines of the Papanicolaou Society of Cytopathology for the examination of cytologic specimens obtained from the respiratory tract. Diagn Cytopathol 1999;21: The Papanicolaou Society of Cytopathology Task Force on Standards of Practice. Papanicolaou Society of Cytopathology guidelines for educational notes, his claimers and similar comments on reports of cervical cytology specimens. Diagn Cytopathol 2003;28: Layfield LJ, Elsheikh TM, Fili A, Nayar R, Shidham V; Papanicolaou Society of Cytopathology. Review of the state of the art and recommendations of the Papanicolaou Society of Cytopathology for urinary cytology procedures and reporting: The Papanicolaou Society of Cytopathology Practice Guidelines Task Force. Diagn Cytopathol 2004;30: Aumodt R, Anderson K, Ashton P, et al. The 1988 Bethesda System for reporting cervical/vaginal cytologic diagnoses: Developed and approved at the National Cancer Institute workshop in Bethesda, MD. Diagn Cytopathol 1989;5: Baloch ZW, Cibas ES, Clark DP, et al. The National Cancer Institute Thyroid fine needle aspiration state of the science conference: A summation. Cytojournal ;5:6. 8. Abati A, Abele J, Bacus SS, et al. Uniform approach to breast FNA biopsy. Diagn Cytopathol 1997;16:
![PSC Pancreaticobiliary Guidelines Committee I - Indications for EUS Guided FNA and Bile Duct Brushings with Pre-procedure Requirements [Douglas Adler, MD - Chair Endoscopist University of Utah]](/docs-images/95/125841680/images/4-0.jpg "Committee II Techniques for Cytologic Sampling of Pancreatic and Bile Duct Lesions [Bill Brugge, MD Chair - Gastroenterologist MGH, Harvard Medical School] Committee III Nomenclature and Diagnostic")
4 PSC Pancreaticobiliary Guidelines Committee I - Indications for EUS Guided FNA and Bile Duct Brushings with Pre-procedure Requirements [Douglas Adler, MD - Chair Endoscopist University of Utah] Committee II Techniques for Cytologic Sampling of Pancreatic and Bile Duct Lesions [Bill Brugge, MD Chair - Gastroenterologist MGH, Harvard Medical School] Committee III Nomenclature and Diagnostic Criteria [Martha Pitman, MD - Chair Cytopathologist MGH, Harvard Medical School] Committee IV Utilization of Ancillary Studies in Pancreas FNA and Bile Duct Brushings [Lester Layfield, MD Chair - Cytopathologist University of Missouri] Committee V Post-Brushing and FNA Testing Follow-Up and Treatment Options [Dan Kurtycz, MD Chair Cytopathologist University of Wisconsin] PSC Guidelines for PB Cytology Published April 2014 Clinical evaluation, imaging studies, indications for cytologic study, and preprocedural requirements for duct brushing studies and pancreatic FNA. Diagn Cytopathol. 2014;42(4): Techniques for cytologic sampling of pancreatic and bile duct lesions. Diagn Cytopathol. 2014;42(4): Standardized terminology and nomenclature for pancreatobiliary cytology. Diagn Cytopathol. 2014;42(4): Utilization of Ancillary Studies in the Cytologic Diagnosis of Biliary and Pancreatic Lesions. Diagn Cytopathol. 2014;42(4): Post-brushing and Fine-Needle Aspiration Biopsy Follow-Up and Treatment Options for Patients With Pancreatobiliary Lesions: Diagn Cytopathol. 2014;42(4): REVIEW Cancer Cytopathol 2014; 122 (6):

5 General Tiered System in Cytology Nondiagnostic Negative Atypical Suspicious Positive 5
6 Pancreatic Pathology: WHO 2010 (abbreviated) Epithelial Tumors Benign Acinar cell cystadenoma Serous cystadenoma Pre-Malignant Lesions PanIN IPMN: LGD, IGD, HGD MCN: LGD,IGD,HGD Malignant Ductal adenocarcinoma and variants Acinar cell carcinoma/cystadenocarcinoma/mixed carcinomas IPMN with invasive carcinoma MCN with invasive carcinoma Pancreatoblastoma Solid-pseudopapillary neoplasm Neuroendocrine Neoplasms Pancreatic neuroendocrine microadenoma Neuroendocrine Tumor Neuroendocrine Carcinoma Negative Atypical Suspicious Positive Management of PB Lesions Malignant Surgery Premalignant Low-intermediate grade Observation with Repeat sampling High-grade/carcinoma Surgery Neoplasm Benign Surgery or observation Medical Management 6
7 Issues to Consider with Terminology of PB Cytology Nondiagnostic is sometimes used when epithelial cells are absent. Required for pseudocyst Common in mucinous cysts with obvious mucin or elevated CEA Serous and acinar cystadenomas are benign but neoplasms. Negative for cancer, true, but atypical due to neoplasm? PanIN are subclinical, non-invasive, pre-malignant lesions that can produce highgrade/malignant appearing cells on FNA. Atypical, Suspicious, Malignant? Does imaging impact the interpretation, e.g. no mass? Issues to Consider with Terminology of PB Cytology IPMN and MCN with LGD (e.g. adenoma) are cysts lined by benign appearing mucinous epithelium but the cysts are pre-malignant neoplasms. Negative or Atypical? IPMN and MCN with intermediate-grade dysplasia (e.g. borderline malignancy) are cysts often lined by high-grade appearing dysplastic cells. Atypical, Suspicious? Other? IPMN and MCN with HGD (e.g. carcinoma in-situ) are cysts classified as premalignant, not malignant (positive) Atypical, Suspicious? Other? 7
8 Issues to Consider with Terminology of PB Cytology Pancreatic Neuroendocrine Tumors are classified by the WHO as neoplasms not carcinomas unless strict criteria are met on histology Positive, Suspicious? Other? Solid-pseudopapillary neoplasm although classified as malignant by WHO is still called a neoplasm and not carcinoma and is similar to PanNETs in that cytological morphology does not correlate with biological behavior. Positive, Suspicious? Other? Issues to Consider with Terminology of PB Cytology Ductal carcinoma (PDAC) represents 9 of 10 malignancies in the pancreas so when cytology reports a positive FNA, clinicians immediately think PDAC. Suspicious for Malignancy connotes a suspicion of PDAC and surgeons feel forced to resect. It is virtually impossible to convince a patient to observe a suspicious mass lesion 8
9 I. Nondiagnostic II. Negative III. Atypical IV. Neoplastic -Benign -Other V. Suspicious VI. Positive/Malignant Proposed Terminology Differential Diagnosis Solid Chronic pancreatitis Ductal adenocarcinoma Acinar cell carcinoma Pancreatic endocrine neoplasm Solid psuedopapillary tumor Pancreatoblastoma Metastasis Cystic Pseudocyst Serous cyst Mucinous cyst (MCN and IPMN) Cystic degeneration of typically solid tumors PEN SPN other Other more rare cysts Simple cysts Lymphoepithelial cyst Peripancreatic cysts 9
10 Cytology Interpretation of Pancreaticobiliary Lesions Multimodal Approach Clinical Information Patient age and gender Symptoms Past medical history Radiological Information Location of mass in the pancreas (and thus organ traversed for EUS) Mass characteristics Solid or cystic Size, contours, invasion Cyst structure: uni- or multilocular; thick/thin wall, Ca++, nodule/mass in the wall Gross cyst contents: thick, viscous, thin, water, clear, brown Ancillary tests: CEA, amylase, KRAS, GNAS Work-up of solid and cystic lesions of pancreas differs. 10
11 Two basic questions for Cyst analysis 1. Is the cyst mucinous or non-mucinous? 2. Is the cyst low-grade or high-grade? 11
12 Cytological Preparations No-ROSE Cysts Direct smears If fluid thick enough Fresh undiluted cyst fluid CEA; Amylase Molecular Cytology Cytospin Cellblock CEA and Amylase: Key Points Elevated CEA ( 192 ng/ml) supports a mucinous cyst Does not distinguish IPMN from MCN Level does not correlate with malignancy Rare FP: PCT, GI duplication cyst, LEC Amylase levels Elevated in the 1000 s for most PCT Low amylase level tends to exclude a PCT Level does not distinguish IPMN from MCN 12
13 Molecular Tests KRAS Mutation(s) support a neoplastic mucinous cyst Does not distinguish IPMN and MCN Does not correlate with grade GNAS Mutation supports IPMN over MCN Does not correlate with grade RNF43 Mutation supports a mucinous cyst Does not distinguish IPMN and MCN 3p deletions 3p25, VHL gene, supports SCA Other 3p deletions also noted in SCA CTNNB1 (beta catenin) deletion Mutation(s) support SPN Fresh Pancreatic Cyst Fluid <0.5cc 0.5 cc ~0.3cc ~0.3cc vortex Centrifuge residual 0.3cc Molecular 2. Molecular 1. CEA supernatant cells ~0.3cc ~0.3cc ~0.3cc 1. CEA 2. Amylase 3. Banking Cytospin(s) Cytology (+/- mucin stains) 13
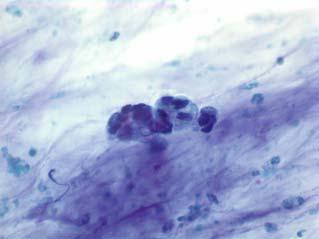
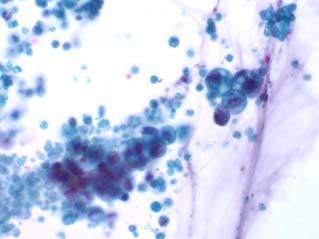

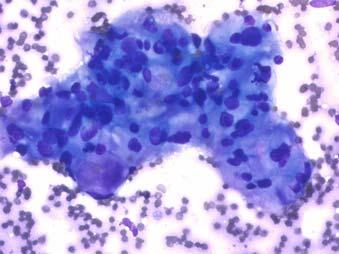
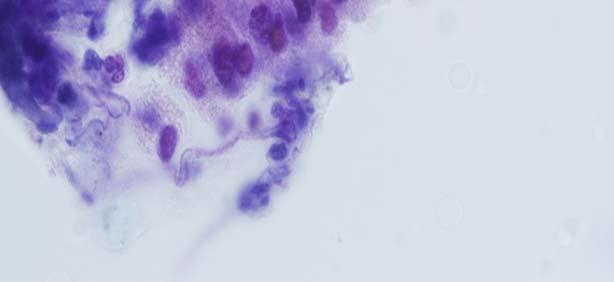
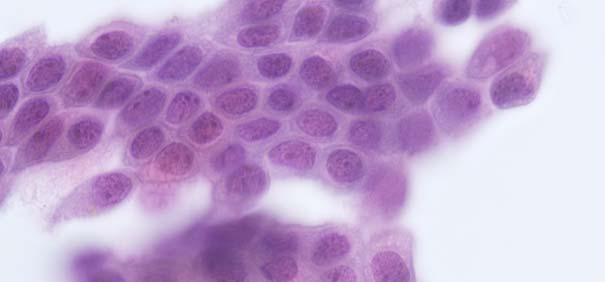
14 Atypical Epithelial Cells Diagnostic Morphology of Carcinoma Already invasive- prognosis decreases ~50% 14




15 Cytological Criteria of High-Grade Epithelial Atypia in the Cyst Fluid of Pancreatic Intraductal Papillary Mucinous Neoplasms Martha B. Pitman, MD, Barbara A. Centeno, MD, Ebubekir S. Daglilar, MD, William R. Brugge, MD, and Mari Mino-Kenudson, MD Cancer Cytopathology epub ahead of print Aug Reference duodenal enterocyte Low-grade High-grade HGA is most accurately identified in mucinous cyst fluids by: 1. an increased N/C ratio, 2. an abnormal chromatin pattern 3. background necrosis Benign/Low Grade Glandular Epithelium High-Grade Atypical Epithelial Cells in Pancreatic Mucinous Cysts are a More Accurate Predictor of Malignancy than Positive Cytology Martha Bishop Pitman M.D, et.al. (Cancer Cytopath 2010) 15

 Components of Cytology Report Adequacy Statement")
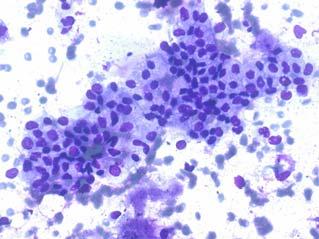
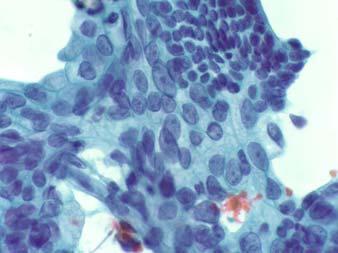
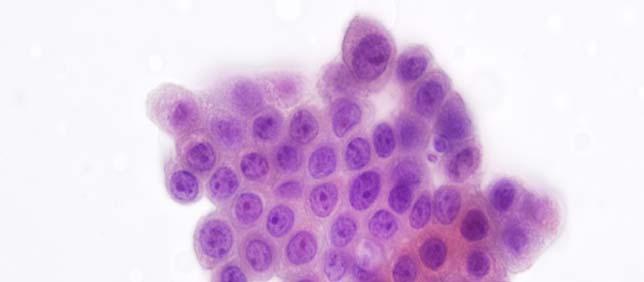
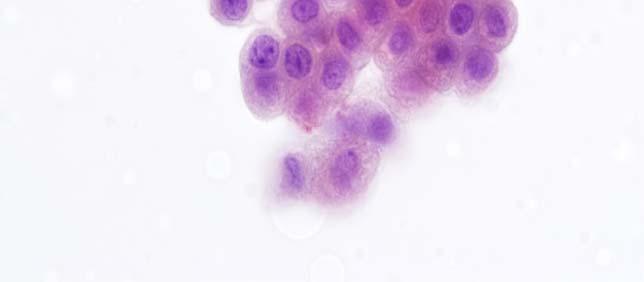
16 High Grade Atypical Glandular Epithelium High-Grade Atypical Epithelial Cells in Pancreatic Mucinous Cysts are a More Accurate Predictor of Malignancy than Positive Cytology Martha Bishop Pitman M.D, et.al. ( Cancer Cytopath 2010) Components of Cytology Report Adequacy Statement Diagnostic Category Subcategory and/or Comments 16
17 Proposed Terminology I. Nondiagnostic II. Negative III. Atypical IV. Neoplastic -Benign -Other V. Suspicious VI. Positive/Malignant Category I Non-diagnostic 17
18 Non-diagnostic Definition: A non-diagnostic cytology specimen is one that provides no diagnostic or useful information about the lesion sampled. Any cellular atypia precludes a non-diagnostic report. Cytological Criteria: Preparation artifact precludes evaluation of the cellular component Obscuring artifact precludes evaluation of the cellular component Gastrointestinal epithelium only Normal pancreatic tissue elements in the setting of a clearly defined solid or cystic mass by imaging Acellular aspirates of a solid mass or pancreatobiliary brushing Acellular aspirate of a cyst without evidence of a mucinous etiology such as thick colloid-like mucin, elevated CEA or KRAS mutation (See Section IV) Knowing which structures are passed through helps recognize contaminants. 18

19 Duodenal Contamination Gastric Contamination 19
20 Gastric Contamination NOT non-diagnostic 20



21 Example Report Evaluation limited by preparation artifact Nondiagnostic Tissue entrapped in blood clot and fibrin precluding cytological evaluation. Example Report Satisfactory for Evaluation Nondiagnostic Gastrointestinal contamination only. 21


22 Example Report Satisfactory for Evaluation Nondiagnostic Normal acinar and ductal epithelium. The biopsy does not explain the well-defined pancreatic mass seen on imaging. Example Report Evaluation limited by scant cellularity Neoplastic: Other Thick, colloid-like extracellular mucin consistent with a neoplastic mucinous cyst. No epithelial component is identified. No necrosis is present. 22
23 Category II Negative (for malignancy) Negative (for malignancy) Indicates the absence of malignancy Can be further qualified by stating the type of benign lesion present When not further qualified, negative is not synonymous with a specific benign lesion 23
24 Negative (for malignancy) False negative rate for a solid mass lesion is approximately 15% and for a cystic lesion may be as high as 60%. False negative rate for bile duct brushings is higher than for EUS-FNA. Malignancy risk for Negative EUS-FNA is 23%. Malignancy risk for Negative brushing sample is 25%. Layfield LJ, Dodd L, Factor R, Schmidt RL. Malignancy risk associated with diagnostic categories defined by the Papanicolaou Society of Cytopathology pancreaticobiliary guidelines. Cancer Cytopathol Jun;122(6): Subcategories for Negative Benign pancreas Chronic Pancreatitis Autoimmune Pancreatitis Pseudocyst Lymphoepithelial Cyst Splenule/Accessory Spleen 24






25 Benign Pancreatic Tissue Correlation with imaging: no visible mass Example Report Satisfactory for Evaluation Negative for Malignancy Benign acinar and ductal epithelium. See note. Note: The biopsy may be representative in the setting of only vague fullness on imaging. Clinical correlation required. 25



26 Pancreatitis Chronic Pancreatitis Active (acute): background inflammation, fat necrosis, calcific debris Autoimmune Pancreatitis cellular stromal fragments embedded with lymphocytes and plasma cells Few ductal cells present Example Report Evaluation limited by scant epithelial component. Negative for Malignancy Cellular stromal fragments with lymphocytes and plasma cells suggestive of autoimmune pancreatitis. 26
.")


27 Example Report Satisfactory for Evaluation Negative (for malignancy) Chronic pancreatitis (See note). Note: Smears show reactive ductal and acinar epithelium with acute and chronic inflammation and necrotic debris. These findings are consistent with the imaging features showing chronic pancreatitis. Lymphoepithelial Cyst Anucleate squames and abundant keratinous debris Mature superficial squamous cells Lymphocytes are usually present but amount is variable and may be quite scant +/-Cholesterol clefts 27




28 Example Report Evaluation limited by poor cellular preservation Negative (for malignancy) Lymphoepithelial cyst. Pseudocyst Inflammation, histiocytes Granular, junky background No cyst lining epithelium Yellow pigment, crystals High amylase (1000 s) Low CEA No mutations 28
.")


29 Example Report Satisfactory for Evaluation Negative (for malignancy) Nonmucinous cyst fluid consistent with pseudocyst (See note). Note: The cyst is inflammatory with only GI epithelium and no recognizable cyst lining epithelium. Yellow pigment is present. The cyst fluid CEA is 2 ng/ml and amylase 56,469 U/L, results that support the diagnosis [or correlation with cyst fluid analysis recommended]. Lymphoid tissue Histiocytes Blood vessels Fibrin aggregates with embedded lymphocytes and plasma cells Spenule/accessory spleen 29


30 Example Report Satisfactory for Evaluation Negative for Malignancy Splenule (ectopic spleen). See note. Note: An immunohistochemical stain for CD8 confirms the presence of splenic venules. Example Report: Negative vs. ND Satisfactory for Evaluation Negative for Malignancy Mucinous cyst debris of uncertain etiology. No high-grade epithelial atypia identified. Correlation with imaging and ancillary studies required. 30
31 Category III Atypical Atypical Definition: cells with cytoplasmic, nuclear, or architectural features not consistent with normal or reactive cellular components of the pancreas or bile ducts, and insufficient features to classify them as a neoplasm or suspicious for a high grade malignancy. The findings do not explain a lesion identified on imaging studies. Follow-up evaluation is warranted. 31
32 Heterogeneous category which includes samples with reactive change, low cellularity, (pre)malignant lesions with nonspecific cytology and cases reflecting cytopathologist s diagnostic caution. Premalignant Lesions of Biliary Tract and Pancreas PanIN (I to III) BilIN (I to III) IPMN (various degrees of dysplasia) Cystic Mucinous Neoplasm (various degrees of dysplasia) 32

33 In general, the concept of dysplasia is most often applied to bile/pancreatic duct brushings and FNAs of cystic lesions. Atypia including Dysplasia PanIN unlikely to be recognized in a cytology specimen as such and more likely to be overdiagnosed Value of correlating cytological findings with imaging PanIN is a subclinical lesion Concept of dysplasia best developed in histologic material. BilIN is poorly defined cytologically From: Hruban RH, Goggins M, Parsons J, Kern SE. Progression Model for Pancreatic Cancer. Clin Cancer Res Aug;6(8):
34 Low grade dysplasia is assigned to the atypical category. Categorization of Dysplasia Bile duct brushings Low-grade dysplasia Atypical category High-grade dysplasia Suspicious category Mucinous Cysts (IPMN or MCN) All grades of dysplasia- Neoplastic: Other category 34


35 Risk of malignancy of Atypical Category EUS-FNA: 79% Duct Brushings: 62% Layfield LJ, Dodd L, Factor R, Schmidt RL. Malignancy risk associated with diagnostic categories defined by the Papanicolaou Society of Cytopathology pancreaticobiliary guidelines. Cancer Cytopathol Jun;122(6): Atypical Mild-moderate cellular atypia, NOS Mucinous/ductal epithelium with mild-moderate nuclear atypia (from a solid lesion or not clearly from a mucinous cyst) BD brushing 35

36 36

37 37

38 Example Report Evaluation limited by scant cellularity Atypical Atypical bile duct epithelium with mucinous metaplasia and mild nuclear atypia. Specimens are interpreted as Atypical when: A specimen is suggestive of a neuroendocrine tumor or solidpseudopapillary neoplasm but tissue is of insufficient quality and quantity to make a specific diagnosis 38

39 Example Report Satisfactory for Evaluation Atypical Atypical epithelial proliferation suggestive but not diagnostic of a neuroendocrine tumor. No tissue for ancillary studies is available. Category IV Neoplastic: Benign Other 39


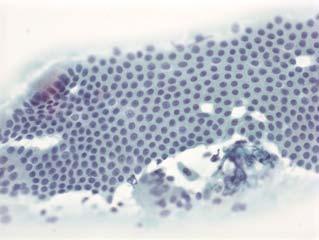
40 Neoplastic: Benign Definition: This interpretation category connotes the presence of a cytological specimen sufficiently cellular and representative, with or without the context of clinical, imaging, and ancillary studies, to be diagnostic of a benign neoplasm. Serous cystadenoma sparse cellularity clean or bloody background flat sheets and loose clusters Bland cuboidal cells clear, finely vacuolated or granular cytoplasm with indistinct borders Associated hemosiderin-laden macrophages Low CEA; low amylase No KRAS mutation 40

41 Example Report Evaluation limited by scant cellularity Neoplastic: Benign Scant nonmucinous cuboidal epithelium in a nonmucinous cyst fluid with low CEA (4ng/ml) and amylase (12 U/L) consistent with the serous cystadenoma. Definition: Neoplastic: Other This interpretation category defines a neoplasm that is either premalignant such as IPMN or MCN with low, intermediate or high grade dysplasia, or a solid-cellular neoplasm such as welldifferentiated PanNET or SPN. 41
42 Neoplastic: Other Pancreatic neuroendocrine tumor Solid-pseudopapillary neoplasm Mucinous cyst (IPMN or MCN), not otherwise specified (NOS), e.g. only thick, colloid-like mucin or elevated CEA or positive KRAS, if known Mucinous cyst (IPMN or MCN) with low-grade atypia/dysplasia Mucinous cyst (IPMN or MCN) with high-grade atypia/dysplasia GIST Controversy and Rational 1. Most PanNETs are malignant, and some believe they all will eventually behave aggressively if unresected 2. All PanNETs have historically been resected for this reason 1. WHO classifies them as neoplasms not carcinomas 1. Cytology classification of PanNETs has historically been as neoplastic process 2. Conservative management of small PanNETs in elderly, asymptomatic patients is an increasingly preferred management option 42
 finely stippled ( salt and pepper ) chromatin moderate to abundant cytoplasm, typically granular but may be vacuolated or oncocytic Controversy and Rational 1.")
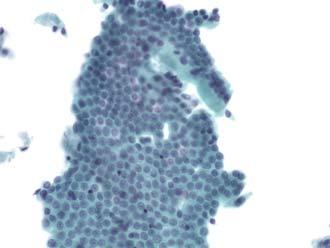
43 Well-differentiated PanNET highly cellular aspirate with solid-cellular smear pattern predominantly isolated cells, bare nuclei pseudorosettes and small clusters uniform, round/oval nuclei eccentric nuclei ( plasmacytoid appearance) finely stippled ( salt and pepper ) chromatin moderate to abundant cytoplasm, typically granular but may be vacuolated or oncocytic Controversy and Rational 1. All SPNs are malignant and have historically been classified as malignant on cytology 1. WHO classifies them as malignant but the tumor name is still neoplasm 2. Most SPN are not aggressive and resection is curative 3. Neoplastic: Other does not classify a lesion as benign or malignant 43




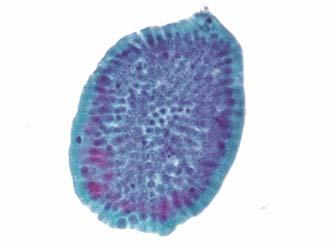
44 Solid-Pseudopapillary Neoplasm highly cellular aspirate with solid-cellular smear pattern myxoid or hyalinized vascular stalks lined by neoplastic cells delicate finely vacuolated cytoplasm with indistinct cell borders perinuclear vacuole PAS/d positive hyalin globule round/oval, bean shaped nuclei nuclear grooves inconspicuous nucleoli foam cells, necrotic debris in the background Mucinous Cysts [IPMN and MCN] Generally hypocellular specimen Variable extracellular mucin thick, colloid-like mucin with or without cyst lining epithelium is diagnostic of a mucinous cyst low-grade dysplasia/atypia: benign appearing mucinous epithelium in sheet and groups, often indistinguishable from gastric epithelium high-grade dysplasia/atypia (intermediate to high-grade): atypical epithelial cells in small, tight bud-like clusters or singly with increased N/C ratio, irregular nuclear membranes and variably vacuolated cytoplasm 44
.")



45 Example Report Satisfactory for Evaluation Neoplastic: Other Mucinous cyst fluid with low-grade dysplasia (See note). Note: Benign-appearing mucinous epithelium is present from this transduodenal FNA in a background of abundant extracellular mucin. [If available, add CEA is elevated at 357 ng/ml supporting the diagnosis]. Example Report Evaluation limited by Absent Epithelial Component Neoplastic: Other Cyst fluid with thick colloid-like extracellular mucin containing cyst debris consistent with a neoplastic mucinous cyst 45
46 Category V Suspicious Definition: Suspicious A specimen is suspicious for malignancy when some but not all of the criteria of a specific malignant neoplasm are present, mainly pancreatic adenocarcinoma. The cytological features raise a strong suspicion for malignancy, but the findings are qualitatively and/or quantitatively insufficient for a conclusive diagnosis. 46
47 The category suspicious for malignancy Represents 5 to 12% of cases Shows high interobserver variability If the category suspicious for malignancy is used for the basis for operative intervention, confirmatory ancillary testing information or substantial clinical and radiological findings must be present and discussed during a treatment planning conference or similar correlation procedure. 47


48 Malignancy Risk of the suspicious for malignancy category is: EUS-FNA: 96% Brushing specimens: 74% Layfield LJ, Dodd L, Factor R, Schmidt RL. Malignancy risk associated with diagnostic categories defined by the Papanicolaou Society of Cytopathology pancreaticobiliary guidelines. Cancer Cytopathol Jun;122(6): Suspicious for Malignancy 48


49 Suspicious for Malignancy Ancillary testing may or may not be helpful in evaluating cases assigned to suspicious for malignancy category KRAS Testing Digital Image Analysis FISH Testing 49
50 KRAS Mutational Analysis Mutations found in 91% of pancreatic adenocarcinomas Mutations also found in ductal hyperplasia, metaplasia, chronic pancreatitis May help in separation of autoimmune pancreatitis from carcinoma Insufficient specificity for clinical usage Digital Image Analysis Aneuploidy and tetraploidy support diagnosis of carcinoma Most useful in brushing specimens Does not significantly improve diagnostic accuracy above cytology alone 50

 Rare atypical epithelial cells")
51 Fluorescence In-Situ Hybridization Commercially available kit Targets pericentromeric regions of chromosomes 3,7 and 17 and chromosomal band 9p21 Can be automated Sensitivity 90%, Specificity 94% Overall best ancillary test for identifying carcinoma PPV 98%, NPV 75% Gores, GJ. Addressing Unmet Clinical Needs: FISHing for Bile Duct Cancer. Cancer Cytopathol Example Report Satisfactory for Evaluation Suspicious (for Malignancy) Rare atypical epithelial cells suspicious for adenocarcinoma. 51
 Solid cellular neoplasm with features suspicious")

52 Example Report Satisfactory for Evaluation Suspicious (for Malignancy) Solid cellular neoplasm with features suspicious for acinar cell carcinoma. Tissue for confirmatory ancillary studies is not available. Category VI Positive (for malignancy) 52
 Pancreatoblastoma Lymphoma Metastases Malignancy risk for malignant category is essentially")
53 Positive/Malignant Definition: unequivocal display of malignant cytologic characteristics Adenocarcinoma of the pancreatobiliary ducts, and variants Acinar cell carcinoma High-grade neuroendocrine carcinoma (small and large cell type) Pancreatoblastoma Lymphoma Metastases Malignancy risk for malignant category is essentially 100%. 53

 Rare mitoses")
54 Pancreatic Ductal Carcinoma and carcinomas of biliary and main pancreatic duct (85-90% of all carcinomas) Cytological Criteria Well-differentiated PDAC Variable cellularity with predominance of one cell type, i.e., ductal cells Cohesive small to medium-sized sheets of cells with smooth borders, and rarely single cells Three-dimensional fragments Moderate nuclear enlargement with high N/C ratios, cellular crowding and overlap Loss of nuclear polarity, often pale nuclei with chromatin clearing and/or clumping, nuclear membrane irregularity with clefts and notches Lack of prominent nucleoli Mild to moderate anisonucleosis (typically more than 4 to 1 in the same gland/duct) Rare mitoses Uncommon necrosis 54
.")



55 Example Report Satisfactory for Evaluation Positive (for Malignancy) Well-differentiated adenocarcinoma (See note). Note: An immunohistochemical stain for SMAD4 shows loss of staining in the suspicious cells supporting a malignant interpretation. Cytological Criteria Moderately Differentiated Pancreatic Ductal Adenocarcinoma Above features with addition of one or more of the following Larger cellular sheets/fragments with increased numbers of single cells More extensive cellular pleomorphism Marked anisonucleosis and occasional prominent nucleoli More crowded three-dimensional or syncytial tissue fragments 55


")
56 Cytologic Criteria Poorly Differentiated Pancreatic Ductal Adenocarcinoma Extreme pleomorphism, with almost total lack of glandular differentiation Larger loosely cohesive syncytial tissue fragments Significant populations of single large malignant cells High N/C ratio, nuclei with coarse dark chromatin and often macro nucleoli Occasional bizarre nuclei with triangular shapes and/or multinucleated cells Mitoses and karyorrhexis Prominent necrosis Example Report Satisfactory for Evaluation Positive (for Malignancy) Adenocarcinoma. 56



 Adenocarcinoma consistent with")
57 Major Diagnostic Criteria for Cholangiocarcinoma Nuclear molding Chromatin clumping Enlarge nuclei Loss of polarity (loss of honey comb pattern Cell-in-cell arrangements Increased N/C ratio Greater than 4-fold variation in nuclear size in a single group of cells Example Report Satisfactory for Evaluation Positive (for Malignancy) Adenocarcinoma consistent with cholangiocarcinoma. 57




.")
58 Cytologic Criteria Acinar Cell Carcinoma Usually hypercellular, mostly small to mid-sized cellular fragments and few single cells Prominent acinar formation without lobular arrangements (in welldifferentiated tumors that can be confused with rosettes of a PanNET), rare syncytia Uniform population of cells larger than ductal carcinoma, minimal pleomorphism Finely granular to denser cytoplasm, granularity is often basophilic Mildly increased N/C ratios, single round to oval nucleus which are eccentrically placed, course chromatin, single prominent nucleoli, focal anisonucleosis Significant anisonucleosis in high-grade tumors Numerous bare stripped off nuclei, rare intranuclear inclusions Rare necrosis Trypsin + Example Report Satisfactory for Evaluation Positive (for Malignancy) Acinar cell carcinoma (See note). Note: An immunohistochemical stain shows the tumor cells to be positive for trypsin supporting the diagnosis. 58


59 Lymphoma of the Pancreas Most lymphomas involving pancreas are secondary Essentially all are non-hodgkin lymphomas 2/3 are large B-cell lymphomas Most involve head of pancreas Cytologic Criteria for Lymphoma Cellular smears of non-cohesive cells Predominance of large immature lymphoid cells Background lymphoglandular bodies Cells have scant cytoplasm Flow cytometry discloses monoclonal cell population 59
60 Metastatic Neoplasms to Pancreas Lung (23%) Breast (8%) Melanoma (5%) Kidney (15%) Thanks to: Martha Bishop Pitman, MD Department of Pathology Massachusetts General Hospital Harvard Medical School Boston, Massachusetts USA 60
Standardization of Nomenclature
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatico-biliary cytology: a practical approach to diagnosis. Corina Cotoi
 Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Case 1. Case 1: EUS Report 5/1/2017. Interesting Cases of Pancreatic Masses
 Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT
 CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Video Microscopy Tutorial 19
 Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Advances in Pancreatic. Cytology. Martha B. Pitman, MD. Disclosure of Relevant Financial Relationships
 Advances in Pancreatic Cytology Martha B. Pitman, MD Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Advances in Pancreatic Cytology Martha B. Pitman, MD Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
EUS-guided FNAB. Differential Diagnosis 5/1/2017. EUS-FNA of Solid and Cystic Lesions:
 EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget
 Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Biliary Tract Neoplasia: A Cyto-histologic Review. Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital
 Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions
 Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Thyroid follicular neoplasms in cytology. Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia
 Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital
 Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases
 Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes
 Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
An Approach to Pancreatic Cysts. Introduction
 An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
ROSE in EUS guided FNA of Pancreatic Lesions
 ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION
 Follicular-patterned thyroid lesions, WC Faquin 1 DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION William C. Faquin, M.D., Ph.D Department of Pathology, Massachusetts
Follicular-patterned thyroid lesions, WC Faquin 1 DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION William C. Faquin, M.D., Ph.D Department of Pathology, Massachusetts
Case #1. Ed Stelow, MD University of Virginia
 Case #1 Ed Stelow, MD University of Virginia Imagine, If You Will It s 4:30 on Friday Last cytology case A thyroid FNA from outside that did not have any onsite interpretation It is from a 45-year old
Case #1 Ed Stelow, MD University of Virginia Imagine, If You Will It s 4:30 on Friday Last cytology case A thyroid FNA from outside that did not have any onsite interpretation It is from a 45-year old
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Objectives. Pancreatic Cysts. Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses
 Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Pancreatic Cysts. Pancreatic Cysts. Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts
 Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts Martha Bishop Pitman, M.D. Director of Cytopathology Massachusetts General Hospital Professor of Pathology Harvard
Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts Martha Bishop Pitman, M.D. Director of Cytopathology Massachusetts General Hospital Professor of Pathology Harvard
Pancreatic malignant tumors are the fifth leading cause of cancerrelated
 44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
EUS-FNAB of GI Tract: Specimen Handling and Triage
 EUS-FNAB of GI Tract: Specimen Handling and Triage Amy Ly, M.D. Director, Fine Needle Aspiration Service Massachusetts General Hospital Assistant Professor of Pathology Harvard Medical School Boston, MA
EUS-FNAB of GI Tract: Specimen Handling and Triage Amy Ly, M.D. Director, Fine Needle Aspiration Service Massachusetts General Hospital Assistant Professor of Pathology Harvard Medical School Boston, MA
Thyroid Cytopathology: Weighing In The Bethesda System
 Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas
 Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo. Case Discussions. 60 year old woman Routine gynecologic control LBC
 BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
Atypia in Diagnostic Cytopathology: Strategies to Reduce Overuse A CQI initiative
 in Diagnostic Cytopathology: Strategies to Reduce Overuse A CQI initiative Dr. Mariamma Joseph and Susan McRae Objectives Review cytology literature on standardization of as a diagnostic term Address the
in Diagnostic Cytopathology: Strategies to Reduce Overuse A CQI initiative Dr. Mariamma Joseph and Susan McRae Objectives Review cytology literature on standardization of as a diagnostic term Address the
Usefulness of Diagnostic Qualifiers for Thyroid Fine-Needle Aspirations With Atypia of Undetermined Significance
 Anatomic Pathology / AUS Qualifiers in Thyroid FNAs Usefulness of Diagnostic Qualifiers for Thyroid Fine-Needle Aspirations With Atypia of Undetermined Significance Paul A. VanderLaan, MD, PhD, 1 Ellen
Anatomic Pathology / AUS Qualifiers in Thyroid FNAs Usefulness of Diagnostic Qualifiers for Thyroid Fine-Needle Aspirations With Atypia of Undetermined Significance Paul A. VanderLaan, MD, PhD, 1 Ellen
EUS-guided FNAB. Differential Diagnosis 3/14/2018. EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses
 EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)
 - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)") SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
LGM International, Inc.
 Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma:
 SUPPLEMENT 1 SPECIAL ISSUE: CYTOPATHOLOGY OF THE THYROID GLAND Guest Editor: Zubair Baloch Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma: A Cytohistologic Review of 22 Cases Xin
SUPPLEMENT 1 SPECIAL ISSUE: CYTOPATHOLOGY OF THE THYROID GLAND Guest Editor: Zubair Baloch Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma: A Cytohistologic Review of 22 Cases Xin
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Biliary cytolgy and pancreatic endoscopic ultrasound-guided. Helsinki, FINLAND
 Biliary cytolgy and pancreatic endoscopic ultrasound-guided d FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology Obstructions PSC, a premalignant condition, the cure of which is transplantation
Biliary cytolgy and pancreatic endoscopic ultrasound-guided d FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology Obstructions PSC, a premalignant condition, the cure of which is transplantation
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA. Leena Krogerus Helsinki, FINLAND
 Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
State of the Art Symposium
 State of the Art Symposium Syed Z. Ali, MD There is no disclosure necessary Martha B. Pitman, MD There is no disclosure necessary Lester Layfield, MD There is no disclosure necessary Joseph Herman, MD
State of the Art Symposium Syed Z. Ali, MD There is no disclosure necessary Martha B. Pitman, MD There is no disclosure necessary Lester Layfield, MD There is no disclosure necessary Joseph Herman, MD
Pancreatobiliary Frozen Section Nightmares
 Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Introduction 10/27/2011. Follicular Lesion/Atypia of Undetermined Significance
 Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
Team approach is essential incorporating: radiology, gastroenterology, surgery and pathology Successful performance is operator dependent
 Committee V Post Brushing and FNA Testing Managment Options Daniel Kurtycz, M.D. Chair Committee V Committee V - Post brushing and FNA management options Team approach is essential incorporating: radiology,
Committee V Post Brushing and FNA Testing Managment Options Daniel Kurtycz, M.D. Chair Committee V Committee V - Post brushing and FNA management options Team approach is essential incorporating: radiology,
DOWNLOAD ENTIRE DOCUMENT FROM
 PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
Case # year old man with a 2 cm right kidney mass
 Case # 4. 52 year old man with a 2 cm right kidney mass Figure 1 Figure 2 Figure 3 Figure 4 Diagnosis: Negative/Non-diagnostic Normal kidney tissue Fine needle aspiration (FNA) of the kidney is performed
Case # 4. 52 year old man with a 2 cm right kidney mass Figure 1 Figure 2 Figure 3 Figure 4 Diagnosis: Negative/Non-diagnostic Normal kidney tissue Fine needle aspiration (FNA) of the kidney is performed
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS
 ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
Enterprise Interest None
 Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits
 in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits") ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits Charitini Salla, MD Head of Cytopathology Department, Hygeia Hospital, Athens, Greece There is
ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits Charitini Salla, MD Head of Cytopathology Department, Hygeia Hospital, Athens, Greece There is
ASCP Competency Assessment
 ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Solid pseudopapillary tumour of the pancreas: Report of five cases
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
The Korean Journal of Cytopathology 15(1) : 60-64, 2004
 : 60-64, 2004") 15 1 The Korean Journal of Cytopathology 15(1) : 60-64, 2004 : INTRODUCTION Papillary carcinoma of the thyroid gland has for long been traditionally diagnosed on the basis of the characteristic papillary
15 1 The Korean Journal of Cytopathology 15(1) : 60-64, 2004 : INTRODUCTION Papillary carcinoma of the thyroid gland has for long been traditionally diagnosed on the basis of the characteristic papillary
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
HANDOUT. Bile Duct Brushing Cytology: A Morphologic and Molecular Approach
 HANDOUT Bile Duct Brushing Cytology: A Morphologic and Molecular Approach Lester J. Layfield, M.D. Professor and Chair Department of Pathology & Anatomical Sciences University of Missouri Introduction
HANDOUT Bile Duct Brushing Cytology: A Morphologic and Molecular Approach Lester J. Layfield, M.D. Professor and Chair Department of Pathology & Anatomical Sciences University of Missouri Introduction
RE-AUDIT OF THYROID FNA USING THE THY GRADING SYSTEM AND HISTOLOGY AT SUNDERLAND ROYAL HOSPITAL, 2011
 Audit: RE-AUDIT OF THYROID FNA USING THE THY GRADING SYSTEM AND HISTOLOGY AT SUNDERLAND ROYAL HOSPITAL, 2011 Auditors: Dr Lena Wilkinson SpR Histopathology Dr. Debra Milne Consultant Histocytopathologist
Audit: RE-AUDIT OF THYROID FNA USING THE THY GRADING SYSTEM AND HISTOLOGY AT SUNDERLAND ROYAL HOSPITAL, 2011 Auditors: Dr Lena Wilkinson SpR Histopathology Dr. Debra Milne Consultant Histocytopathologist
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
DIAGNOSTIC DILEMMA. Case Reports Clinical history. Materials and Methods
 DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
Matthew McCollough, M.D. April 9, 2009 University of Louisville
 Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
XIII CONGRESSO NAZIONALE Roma, 7-9 novembre NODULO TIROIDEO: Agoaspirato o Core Needle Biopsy?
 XIII CONGRESSO NAZIONALE NODULO TIROIDEO: Agoaspirato o Core Needle Biopsy? Anna Crescenzi Policlinico Universitario Campus Bio-Medico Roma Indeterminate lesions are heterogeneous The gray zone CONSERVATIVE
XIII CONGRESSO NAZIONALE NODULO TIROIDEO: Agoaspirato o Core Needle Biopsy? Anna Crescenzi Policlinico Universitario Campus Bio-Medico Roma Indeterminate lesions are heterogeneous The gray zone CONSERVATIVE
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
Cytology Report Format
 Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
Pancreatic neoplasms associated with significant amounts of extracellular. Fine-Needle Aspiration Cytology of Mucinous Tumors of the Pancreas CANCER
 92 CANCER CYTOPATHOLOGY Fine-Needle Aspiration Cytology of Tumors of the Pancreas Monica Recine, M.D. 1 Madhukar Kaw, M.D. 2 Douglas B. Evans, M.D. 3 Savitri Krishnamurthy, M.D. 1 1 Division of Pathology
92 CANCER CYTOPATHOLOGY Fine-Needle Aspiration Cytology of Tumors of the Pancreas Monica Recine, M.D. 1 Madhukar Kaw, M.D. 2 Douglas B. Evans, M.D. 3 Savitri Krishnamurthy, M.D. 1 1 Division of Pathology
Case #1 FNA of nodule in left lobe of thyroid in 67 y.o. woman
 Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Guidelines for Pancreaticobiliary Cytology from the Papanicolaou Society of Cytopathology: A Review
 Guidelines for Pancreaticobiliary Cytology from the Papanicolaou Society of Cytopathology: A Review Martha B. Pitman, MD 1 and Lester J. Layfield, MD 2 The newest installment on state-of-the-art standards
Guidelines for Pancreaticobiliary Cytology from the Papanicolaou Society of Cytopathology: A Review Martha B. Pitman, MD 1 and Lester J. Layfield, MD 2 The newest installment on state-of-the-art standards
system and the Bethesda system applied for reporting thyroid cytopathology
 Original Research Article A comparative study between conventional system and the Bethesda system applied for reporting thyroid cytopathology M. Mamatha 1*, S. Chandra Sekhar 2, H. Sandhya Rani 3, S. Sandhya
Original Research Article A comparative study between conventional system and the Bethesda system applied for reporting thyroid cytopathology M. Mamatha 1*, S. Chandra Sekhar 2, H. Sandhya Rani 3, S. Sandhya
Cytopathology Study Day 16 April RCPath - BAC. Digital cytology: EUS FNA pancreas and head and neck
 Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
NODULAR CYSTIC HIDRADENOMA OVER THE GLUTEAL REGION: A RARE CYTOMORPHOLOGICAL DIAGNOSIS
 NODULAR CYSTIC HIDRADENOMA OVER THE GLUTEAL REGION: A RARE CYTOMORPHOLOGICAL DIAGNOSIS Abstract: The primary as well as metastatic tumours of the skin can be diagnosed by fine needle aspiration cytology
NODULAR CYSTIC HIDRADENOMA OVER THE GLUTEAL REGION: A RARE CYTOMORPHOLOGICAL DIAGNOSIS Abstract: The primary as well as metastatic tumours of the skin can be diagnosed by fine needle aspiration cytology
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Almost any suspected tumor can be aspirated easily and safely. Some masses are more risky to aspirate including:
 DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY. F ZAHRA ALY, MD, PhD
 ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules