Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case
|
|
|
- Jonathan Allen
- 6 years ago
- Views:
Transcription
1 Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital, Peking Union Medical College & Chinese Academy of Medical Sciences, Beijing , China Correspondence to: Dongbing Zhao. Department of Abdominal Surgery, Cancer Institute & Hospital, Peking Union Medical College & Chinese Academy of Medical Sciences, No 17, Pan Jia Yuan Nan Li, Chaoyang District, Beijing , China. Abstract: Pancreatic neuroendocrine tumor (pnet) is a rare pancreatic tumor, with its incidence showing a rising trend in recent years. Most of its distant metastases are found in the liver. This article describes a 59-year-old male patient with pnet with liver metastasis and multiple abdominal metastases, focusing on the management of this tumor in its advanced stage. Keywords: Pancreatic neuroendocrine tumor (pnet); liver metastasis; multiple abdominal metastases Received: 24 April 2016; Accepted: 22 June 2016; Published: 23 August doi: /tgh View this article at: Disease history and treatment A 59-year-old male patient was found to be with an abdominal wall neoplasm in April No special treatment was applied. Since then he suffered from passage of loose stools (4 5 times daily), and the stool volume was relatively large. His body weight decreased by 5 kg, although he had no facial flushing, bronchial spasm, faint, blood glucose fluctuations, or erythema migrans. He had no other history of disease. Computed tomography (CT) performed in other hospital revealed the presence of a mass at the head of pancreas. Multiple liver metastases as well as multiple masses in greater omentum, mesentery, and abdominal and pelvic cavities were observed and considered to be metastatic lesions. Liver biopsy in other hospital revealed the presence of adenocarcinoma invasion within the fibrous tissue. A diagnosis of tumor could not be confirmed during a pathological consultation in our hospital. Tumor markers: AFP, CEA, CA125, CA199, and CA153 were normal. Gastroscopy and colonoscopy in other hospital showed no abnormality. Abdominal and pelvic CT (on May 2, 2013, in our hospital): (I) a mass in neck of pancreas, which was considered as malignant; (II) multiple liver metastases; (III) multiple abdominal/pelvic cavity and retroperitoneal lymph node metastases; and (IV) omental metastasis (Figure 1). Ultrasound-guided puncture of the abdominal wall mass (on May 2, 2013): cytology showed the presence of tumor cells, and a diagnosis of a neuroendocrine tumor was considered based in combination with the immunochemical results. Immunohistochemical findings: BerEp4(+++), calrentinin(+), Syn(++), CD56(±), and HME-1( ), CgA(±), MOC31(+++), and Ki-67(15%+). Pathology: infiltration of an extremely small number of small round cell tumor cells was seen in fibrous tissue. In combination with clinical findings, the possibility of a metastasis with acinar differentiation was considered. Immunohistochemical findings: AE1/AE3(3+), hepotocyte( ), CgA(2+), Syn(3+), Ki67(3%+), CD56(2+), NSE(3+), CD117(-), AAT(2+), and ACT(1+) (Figure 2). Diagnosis: pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases. Somatostatin receptor scintigraphy (on May 7, 2013): high expression of somatostatin receptor was seen in pancreas, liver, and abdominal and pelvic cavities, which met the diagnostic
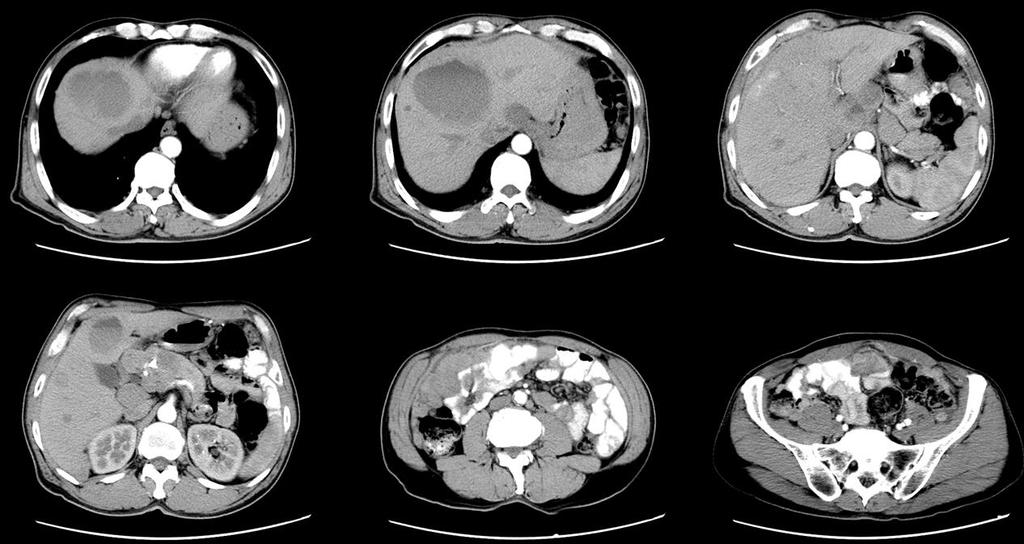
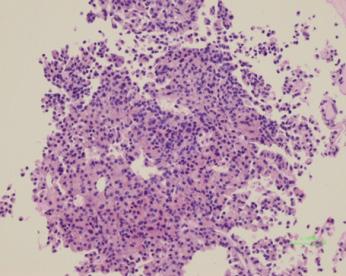
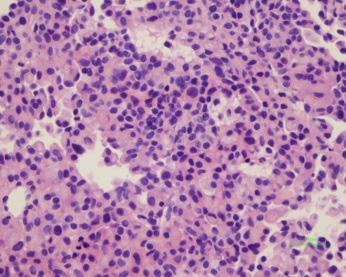
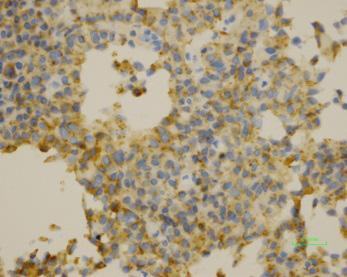
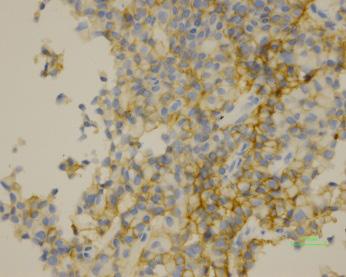
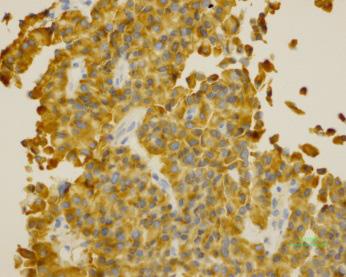
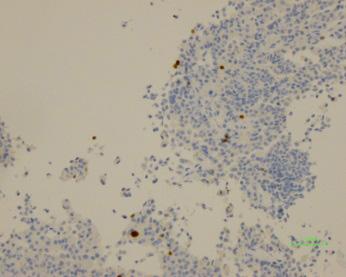
2 Page 2 of 8 Translational Gastroenterology and Hepatology, 2016 Figure 1 Abdominal and pelvic CT (May 2, 2013). Figure 2 Pathoimmunohistochemical findings ( 200) (May 2, 2013).
 consultation on May 14, 2013 suggested that the diagnoses were pancreatic NEN (G2) with accompanying multiple abdominal and pelvic metastases and multiple hepatic")

3 Translational Gastroenterology and Hepatology, 2016 Page 3 of 8 Figure 3 Somatostatin receptor scintigraphy (May 7, 2013). criteria of neuroendocrine neoplasms (NENs) (Figure 3). Multidisciplinary treatment (MDT) consultation on May 14, 2013 suggested that the diagnoses were pancreatic NEN (G2) with accompanying multiple abdominal and pelvic metastases and multiple hepatic metastases. Currently the disease was in a relatively advanced stage, and the patient also had the symptoms of carcinoid syndrome. A combined therapy with sandostatin and sutent was recommended. The patient then received routine follow-up examinations. He felt that his general conditions were better than before and the abdominal mass became smaller; the appetite increased and there was no diarrhea; bowel movement once a day, weight gain 10 pounds. He defecated once daily and his body weight increased by 5 kg. PET-CT after treatment is Figure 4 and comparison of abdominal CT findings before and after treatment is shown in Figures 5 8. Figure 4 PET-CT (gallium-68) on December 26, 2013.












4 Page 4 of 8 Translational Gastroenterology and Hepatology, 2016 Figure 5 On August 5, The mass in the neck of the pancreas shrank. Among the multiple metastases inside liver, some enlarged while others shrank. The multiple swollen intraperitoneal, retroperitoneal, and right iliac lymph nodes and the omentum were similar as before. Figure 6 On April 20, The mass in the neck of the pancreas was similar as before. Among the intrahepatic multiple masses, the large ones were mostly cystic. Among the multiple swollen intraperitoneal, retroperitoneal, and right iliac lymph nodes, some slightly enlarged while others were smaller than before. The solid masses slightly shrank. Translational Gastroenterology and Hepatology. All rights reserved. tgh.amegroups.com










, right")

5 Translational Gastroenterology and Hepatology, 2016 Page 5 of 8 Figure 7 On June 18, The mass in the neck of the pancreas slightly shrank. The intrahepatic multiple masses varied in size and were hypodense, with the large ones being mostly cystic. Among the multiple swollen intraperitoneal, retroperitoneal, and right iliac lymph nodes, some were slightly rounder than before, while new lymph nodes occurred in the mesenteric gap. Figure 8 On May 17, The mass in the neck of the pancreas was similar as before. The intrahepatic multiple masses varied in size and were hypodense; some masses were smaller than before, while others remained the same. Among the multiple swollen intraperitoneal, retroperitoneal, and right iliac lymph nodes, some slightly enlarged, which were considered to be metastases. Multiple small nodules newly occurred in two lungs and under the pleura, which were considered to be metastases. Multiple swollen lymph nodes were seen in mediastinum (stations 1, 2R, 4R/L, and 7), right lung hilum, right diaphragmatic pericardium, and cardia and were considered to be metastases. Translational Gastroenterology and Hepatology. All rights reserved. tgh.amegroups.com
6 Page 6 of 8 Translational Gastroenterology and Hepatology, 2016 Table 1 World Health Organization s classification of neuroendocrine symptoms and improve the prognosis. tumors [2010] Grade Non-surgical treatment Mitotic rate Ki-67 index (/10 HPF) (%) Non-surgical approaches can be applied for advanced NET G1 (low grade) <2 2 pnet with liver metastasis or multiple metastases. These approaches include medical treatment (e.g., biotherapy, NET G2 (intermediate grade) molecularly targeted therapy, and chemotherapy), NEC G3 (high grade) >20 >20 radiotherapy, and local treatments including radiofrequency ablation and arterial chemoembolization. These approaches can control symptoms, improve quality of life, and prolong Sutent was withdrawn in July 2015 due to drug resistance. Currently the patient is not on any treatment. survival. Among the medical treatments, biotherapy is mainly based on somatostatins. While somatostatin-based biotherapy has an objective response rate of <10% for pnet, the disease control rates range 50 60%. They are particularly Discussion Pancreatic neuroendocrine tumor (pnet), formerly useful for advanced pnet. Somatostatins (e.g., slowrelease formulation of lanreotide and long-acting octreotide) known as islet cell tumors, account for about 3% of primary can act on the somatostatin receptor on pnet cells and thus effectively alleviate and control the neuro-endocrine pancreatic cancer. According to the hormone secretion symptoms, inhibit the growth of pnet, and prolong status and the patient s clinical presentations, pnet can be survival (3). As shown in many retrospective studies and classified as functioning and non-functioning grading and randomized prospective studies, somatostatins can be used prognosis (Tables 1,2). in patients with slowly progressing pnets (G1/G2) and The common serological markers of pnet include somatostatin receptor-positive pancreatic neuroendocrine chromogranin A (CgA) and neuron-specific enolase (NSE), cancer (pnec) (G3), with relatively mild adverse reactions. whose abnormal increase often indicates the possibility of Among the medical treatments, the main molecularly targeted a neuroendocrine tumor. Medical imaging modalities such drugs include sunitinib and everolimus. The mammalian as contrast-enhanced CT and MRI are highly valuable target of rapamycin (mtor) signaling pathway gene is the for the diagnosis of pnet, which are mostly shown as common mutation in pnet, accounting for about 16%. hypervascular lesions with enhancement appearances at Blocking this signaling pathway can inhibit the growth of early arterial phase. parts of pnet. Everolimus is an orally administered mtor inhibitor, whereas sunitinib is a multitargeted tyrosine kinase Multidisciplinary treatment of pnet (Figure 9) inhibitor and can prolong the disease-free progression of pnet (4). Both drugs have good efficacy and tolerance Surgery for advanced and metastatic pnet. Among the medical Liver metastasis accounts for about 90% of the distant treatments, chemotherapy is not useful for neuroendocrine metastases of pnet and is a major prognostic factor for this tumor. Research has shown that the concurrent resection of both the primary lesion and resectable liver metastases is feasible and can improve the prognosis (1). Palliative surgery refers to the removal of most of the metastasis (>90% of the lesion), during which the concurrent or staged resection of the primary lesion or liver metastases may be considered. If staged resection is performed, the liver metastases should be resected first, followed by the resection of the primary lesions, with an attempt to avoid the transfer of liver abscess and liver cancer cells from the biliary-enteric anastomosis to the intestinal tract (2). While liver transplantation is not a routine treatment for pnet, surgical methods can control tumors. It can only be applied in patients with advanced tumors that are unresectable. The role of streptozotocin combined with 5-fluorouracil (5-FU) and/or epirubicin in treating G1/G2 pnens has been well demonstrated and thus has become standard treatments. Temozolomide alone or in combination with capecitabine also has certain role in treating metastatic pancreatic neuroendocrine neoplasms (pnens). Oxaliplatin or irinotecan can also be used as the second-line treatment options for pnens. Radiotherapy is mainly used for brain or bone metastases. Among the local treatments, radiofrequency ablation and arterial interventional therapy have important roles in treating pnet with liver metastasis; they can effectively control the liver metastases and alleviate the neuroendocrine symptoms.
 Hormone syndrome Benign Highly differentiated 1 cm <2 Benign or low malignant")
7 Translational Gastroenterology and Hepatology, 2016 Page 7 of 8 Table 2 World Health Organization s prognostic factors of pancreatic neuroendocrine neoplasms (pnens) Biological behaviors Metastasis Muscularis infiltration Histology differentiation degree Tumors maximum diameter Vascular invasion Ki-67 index (%) Hormone syndrome Benign Highly differentiated 1 cm <2 Benign or low malignant potential Highly differentiated 2 cm +/ <2 Low malignant potential + + Highly differentiated >2 cm + >2 + High malignant potential + + Poorly differentiated Any + >30 PD or PPPD at pancreatic head and neck >2 cm Either functioning or non-functioning Resection of pancreatic body and tail or segmental pancreatic resection Regular follow-up visits pnet <2 cm Non-functioning Excision or local resection Metastasis Solitary resectable metastases can be surgically removed; otherwise chemotherapy Figure 9 Algorithm of the management of pancreatic neuroendocrine tumors (pnets). Acknowledgements None. from the patient for publication of this manuscript and any accompanying images. Footnote Conflicts of Interest: The authors have no conflicts of interest to declare. Informed Consent: Written informed consent was obtained References 1. Cusati D, Zhang L, Harmsen WS, et al. Metastatic nonfunctioning pancreatic neuroendocrine carcinoma to liver: surgical treatment and outcomes. J Am Coll Surg 2012;215:117-24; discussion
8 Page 8 of 8 Translational Gastroenterology and Hepatology, De Jong MC, Farnell MB, Sclabas G, et al. Liver-directed therapy for hepatic metastases in patients undergoing pancreaticoduodenectomy: a dual-center analysis. Ann Surg 2010;252: Martín-Richard M, Massutí B, Pineda E, et al. Antiproliferative effects of lanreotide autogel in patients with progressive, well-differentiated neuroendocrine tumours: a Spanish, multicentre, open-label, single arm phase II study. BMC Cancer 2013;13: Raymond E, Dahan L, Raoul JL, et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med 2011;364: doi: /tgh Cite this article as: Wang Y, Zhao D. Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case. Transl Gastroenterol Hepatol 2016;1:65.
Interventional therapy for rectal neuroendocrine tumor with liver metastases: report of one case
 Case Report Interventional therapy for rectal neuroendocrine tumor with liver metastases: report of one case Lingxiao Liu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Interventional Radiology, 2 Department
Case Report Interventional therapy for rectal neuroendocrine tumor with liver metastases: report of one case Lingxiao Liu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Interventional Radiology, 2 Department
Type 2 gastric neuroendocrine tumor: report of one case
 Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Resection of postoperative liver metastasis from pancreatic neuroendocrine tumors: report of one case
 Case Report Resection of postoperative liver metastasis from pancreatic neuroendocrine tumors: report of one case Xiao Chen, Hu Ren, Yihebali Chi, Shun He, Zhen Huang, Xuhui Hu, Hong Zhao Department of
Case Report Resection of postoperative liver metastasis from pancreatic neuroendocrine tumors: report of one case Xiao Chen, Hu Ren, Yihebali Chi, Shun He, Zhen Huang, Xuhui Hu, Hong Zhao Department of
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
Gastrinoma: Medical Management. Haley Gallup
 Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS
 TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Metastatic multiple endocrine neoplasia type 1: report of one case
 Case Report Metastatic multiple endocrine neoplasia type 1: report of one case Cheng Huang 1 *, Xiaodong Zhu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Liver Surgery, Fudan University Zhongshan Hospital,
Case Report Metastatic multiple endocrine neoplasia type 1: report of one case Cheng Huang 1 *, Xiaodong Zhu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Liver Surgery, Fudan University Zhongshan Hospital,
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
NICaN Pancreatic Neuroendocrine Tumour SACT protocols. 1.0 Dr M Eatock Final version issued
 Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
EUS FNA NEUROENDOCRINE TUMORS. A. Ginès Endocopy Unit Hospital Cínic. Barcelona (Spain)
") EUS FNA NEUROENDOCRINE TUMORS A. Ginès Endocopy Unit Hospital Cínic. Barcelona (Spain) GI NEUROENDOCRINE TUMORS GENERAL CONCEPTS Rare neoplasms arising from the neuroendocrine cells of the GI tract Include:
EUS FNA NEUROENDOCRINE TUMORS A. Ginès Endocopy Unit Hospital Cínic. Barcelona (Spain) GI NEUROENDOCRINE TUMORS GENERAL CONCEPTS Rare neoplasms arising from the neuroendocrine cells of the GI tract Include:
MEDICAL MANAGEMENT OF METASTATIC GEP-NET
 MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Grade 2 Ileum NET with liver and bone metastasis
 Grade 2 Ileum NET with liver and bone metastasis BERNARDO MARQUES ENDOCRINOLOGY DEPARTMENT PORTUGUESE INSTITUTE OF ONCOLOGY - COIMBRA April 2018, Lugano, Switzerland JPB, male, 67 years old April 2015
Grade 2 Ileum NET with liver and bone metastasis BERNARDO MARQUES ENDOCRINOLOGY DEPARTMENT PORTUGUESE INSTITUTE OF ONCOLOGY - COIMBRA April 2018, Lugano, Switzerland JPB, male, 67 years old April 2015
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid
 Neuroendocrine Tumors and Lung Carcinoid") Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS)
") FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS) Gilda s Club Quad Cities November 5 th, 2018 Joseph Dillon, MD Neuroendocrine Tumor Clinic University of Iowa Hospitals & Clinics
FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS) Gilda s Club Quad Cities November 5 th, 2018 Joseph Dillon, MD Neuroendocrine Tumor Clinic University of Iowa Hospitals & Clinics
Neuro-endocrine and pancreatic non-adenocarcinomas. Marc Engelbrecht, AMC, Amsterdam
 Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
A rare case of retroperitoneal paraganglioma case report and literature review
 Case Report A rare case of retroperitoneal paraganglioma case report and literature review Peng Li, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital, Chinese Academy of Medical
Case Report A rare case of retroperitoneal paraganglioma case report and literature review Peng Li, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital, Chinese Academy of Medical
Diagnosing and monitoring NET
 Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Comprehensive treatment of a functional pancreatic neuroendocrine tumor with multifocal liver metastases
 Case Report Comprehensive treatment of a functional pancreatic neuroendocrine tumor with multifocal liver metastases Wei Wang 1,2,3 *, Sharvesh Raj Seeruttun 1,2,3 *, Cheng Fang 1,2,3, Zhiwei Zhou 1,2,3
Case Report Comprehensive treatment of a functional pancreatic neuroendocrine tumor with multifocal liver metastases Wei Wang 1,2,3 *, Sharvesh Raj Seeruttun 1,2,3 *, Cheng Fang 1,2,3, Zhiwei Zhou 1,2,3
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide)
") GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
Cancer of Unknown Primary (CUP)
") Cancer of Unknown Primary (CUP) Pathways and Guidelines V1.0 London Cancer September 2013 The following pathways and guidelines document has been compiled by the London Cancer CUP technical subgroup and
Cancer of Unknown Primary (CUP) Pathways and Guidelines V1.0 London Cancer September 2013 The following pathways and guidelines document has been compiled by the London Cancer CUP technical subgroup and
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες
 NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Case Presentation. Marianne Ellen Pavel. Charité University Medicine Berlin. ESMO Preceptorship on GI Neuroendocrine Tumors
 Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
Community Case. Saeed Awan R5
 Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Prolonged Survival in a Patient with Neuroendocrine Tumor of the Cecum and Diffuse Peritoneal Carcinomatosis
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Strategies in the Management of Neuroendocrine Tumors. Dr. Jean Maroun Dr. Elena Tsvetkova
 Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Objectives. Terminology 03/11/2013. Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Pathology Update 2013
 Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives
 Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Treatment algorithm Neuroendocrine tumours. Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece
 Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Surgery for NET Challenges and specific aspects
 Surgery for NET Challenges and specific aspects Raymond Aerts, MD Department of Abdominal Surgery and Liver Transplantation University Clinics Leuven ESMO Preceptorship on GI neuroendocrine tumours (NETs)
Surgery for NET Challenges and specific aspects Raymond Aerts, MD Department of Abdominal Surgery and Liver Transplantation University Clinics Leuven ESMO Preceptorship on GI neuroendocrine tumours (NETs)
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology
 Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Index. Surg Oncol Clin N Am 15 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
RADIOFREQUENCY ABLATION
 RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Case report. Kováčová Martina Comenius University in Bratislava Slovakia Faculty of medicine
 Case report Kováčová Martina Comenius University in Bratislava Slovakia Faculty of medicine Past medical history 38 years old male patient No past medical or surgical history prior to presentation No medications
Case report Kováčová Martina Comenius University in Bratislava Slovakia Faculty of medicine Past medical history 38 years old male patient No past medical or surgical history prior to presentation No medications
GASTROINTESTINAL MALIGNANCIES
 Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
David Lewin MD Medical University of South Carolina
 Top 10 Advances in GI Pathology David Lewin MD Medical University of South Carolina No Disclosures Overview Top Articles/ presentations in the following areas Imaging (3) Molecular (2) Therapeutics (3)
Top 10 Advances in GI Pathology David Lewin MD Medical University of South Carolina No Disclosures Overview Top Articles/ presentations in the following areas Imaging (3) Molecular (2) Therapeutics (3)
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Case Report. Ameya D. Puranik, MD, FEBNM; Harshad R. Kulkarni, MD; Aviral Singh, MD; Richard P. Baum, MD, PhD ABSTRACT
 Case Report 8-YEAR SURVIVAL WITH A METASTATIC THYMIC NEUROENDOCRINE TUMOR: EMPHASIS ON REDEFINING TREATMENT OBJECTIVES USING PERSONALIZED PEPTIDE RECEPTOR RADIONUCLIDE THERAPY WITH 177 Lu- AND 90 Y-LABELED
Case Report 8-YEAR SURVIVAL WITH A METASTATIC THYMIC NEUROENDOCRINE TUMOR: EMPHASIS ON REDEFINING TREATMENT OBJECTIVES USING PERSONALIZED PEPTIDE RECEPTOR RADIONUCLIDE THERAPY WITH 177 Lu- AND 90 Y-LABELED
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
CRITICAL ANALYSIS OF NEN GUIDELINES. G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines
 CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
Multimodality therapy for a case of neuroendocrine tumor in the hilum with multiple hepatic metastases
 Case Report Multimodality therapy for a case of neuroendocrine tumor in the hilum with multiple hepatic metastases Yuan Li, Zhen Huang, Yefan Zhang, Hong Zhao Department of bdominal Surgery, Cancer Institute
Case Report Multimodality therapy for a case of neuroendocrine tumor in the hilum with multiple hepatic metastases Yuan Li, Zhen Huang, Yefan Zhang, Hong Zhao Department of bdominal Surgery, Cancer Institute
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Embolotherapy for Cholangiocarcinoma: 2016 Update
 Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Characteristics and treatment of patients with neuroendocrine carcinoma of the gastroesophageal junction: an analysis of 13 cases
 Original Article Characteristics and treatment of patients with neuroendocrine carcinoma of the gastroesophageal junction: an analysis of 13 cases Yingzhi Qin 1 *, Chao Guo 1 *, Xiaoyan Chang 2, Yeye Chen
Original Article Characteristics and treatment of patients with neuroendocrine carcinoma of the gastroesophageal junction: an analysis of 13 cases Yingzhi Qin 1 *, Chao Guo 1 *, Xiaoyan Chang 2, Yeye Chen
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Neuroendocrine Carcinoma. Lebanon Neuroendocrine Neoplasms of H&N Nov /7/2011. Broad Classification:
 H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
Neuroendocrine Tumors
 Neuroendocrine Tumors FCDS Annual Conference Boca Raton Marriott at Boca Center July 28, 2016 Steven Peace, BS, CTR Anatomy and Physiology of the (Neuro)Endocrine System WHO Classification, Tumor Grade
Neuroendocrine Tumors FCDS Annual Conference Boca Raton Marriott at Boca Center July 28, 2016 Steven Peace, BS, CTR Anatomy and Physiology of the (Neuro)Endocrine System WHO Classification, Tumor Grade
SURGERY OF NETS. Iakovos N Nomikos MD FACS. Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece
 SURGERY OF NETS Iakovos N Nomikos MD FACS Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece Epidemiology 5-fold increase in occurrence of NETS over past 30 years
SURGERY OF NETS Iakovos N Nomikos MD FACS Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece Epidemiology 5-fold increase in occurrence of NETS over past 30 years
NAACCR Webinar Series 4/5/2018 COLLECTING CANCER DATA: PANCREAS
 COLLECTING CANCER DATA: PANCREAS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: PANCREAS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Liver and Pancreatic Case discussion
 The Royal Marsden Liver and Pancreatic Case discussion Dr Ian Chau Consultant Medical Oncologist The Royal Marsden 77 year old gentleman with 2 months history of vague abdominal ache and clinically finding
The Royal Marsden Liver and Pancreatic Case discussion Dr Ian Chau Consultant Medical Oncologist The Royal Marsden 77 year old gentleman with 2 months history of vague abdominal ache and clinically finding
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD) Type of Article: Case Report
: Online published version of an accepted article before publication in the final form. Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD) Type of Article: Case Report
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Neuroendocrine Tumors: Just the Basics. George Fisher, MD PhD
 Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
A nonresponding small cell lung cancer combined with adenocarcinoma
 Case Report A nonresponding small cell lung cancer combined with adenocarcinoma Hongyang Lu 1,2, Shifeng Yang 3 1 Zhejiang Key Laboratory of Diagnosis & Treatment Technology on Thoracic Oncology (Lung
Case Report A nonresponding small cell lung cancer combined with adenocarcinoma Hongyang Lu 1,2, Shifeng Yang 3 1 Zhejiang Key Laboratory of Diagnosis & Treatment Technology on Thoracic Oncology (Lung
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
Protocol for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat: UPPER GI CANCER
 Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: UPPER GI CANCER Patient information given at each stage following agreed information pathway
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: UPPER GI CANCER Patient information given at each stage following agreed information pathway
Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
 Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
A retrospective analysis of neuroendocrine tumour of pancreas: a single institute study
 International Journal of Research in Medical Sciences Chheda YP et al. Int J Res Med Sci. 2015 Nov;3(11):3041-3045 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20150928
International Journal of Research in Medical Sciences Chheda YP et al. Int J Res Med Sci. 2015 Nov;3(11):3041-3045 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20150928
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT )
") An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Images In Gastroenterology
 Images In Gastroenterology Thong-Ngam D, et al. THAI J GASTROENTEROL 2005 Vol. 6 No. 2 May - Aug. 2005 105 Imaging of Gastrointestinal Stromal Tumors Pornpim Fuangtharnthip, M.D. Narumol Hargroove, M.D.
Images In Gastroenterology Thong-Ngam D, et al. THAI J GASTROENTEROL 2005 Vol. 6 No. 2 May - Aug. 2005 105 Imaging of Gastrointestinal Stromal Tumors Pornpim Fuangtharnthip, M.D. Narumol Hargroove, M.D.
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works.
 Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works. Arturo Loaiza-Bonilla, MD, FACP Assistant Professor of Clinical Medicine
Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works. Arturo Loaiza-Bonilla, MD, FACP Assistant Professor of Clinical Medicine
Small cell neuroendocrine carcinoma icd 10
 Small cell neuroendocrine carcinoma icd 10 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM C34.90 - includes detailed rules, notes, synonyms, ICD -9- crosswalks, DRG. In most series, LCLC's
Small cell neuroendocrine carcinoma icd 10 1-10-2017 Free, official coding info for 2018 ICD - 10 -CM C34.90 - includes detailed rules, notes, synonyms, ICD -9- crosswalks, DRG. In most series, LCLC's
Interactive Staging Bee
 Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Ongoing and future clinical investigation in GEP NENs
 ESMO PRECEPTORSHIP PROGRAMME Multidisciplinary management, standards of care and future perspectives Lugano, Switzerland 13-14 April 2018 CHAIR: Nicola Fazio, Italy George Pentheroudakis, Greece Ongoing
ESMO PRECEPTORSHIP PROGRAMME Multidisciplinary management, standards of care and future perspectives Lugano, Switzerland 13-14 April 2018 CHAIR: Nicola Fazio, Italy George Pentheroudakis, Greece Ongoing
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure