Pourquoi je fais moins d EMG laryngées. Philippe H. Dejonckere
|
|
|
- Alisha Potter
- 6 years ago
- Views:
Transcription



1 Pourquoi je fais moins d EMG laryngées Philippe H. Dejonckere

2

3
4 EMG Technique électrophysiologique qui renseigne sur l activité électrique musculaire (tonus & mouvement) Phonation = mouvement Indication basique : «toute pathologie du mouvement relative au mécanisme phonatoire»
5 Surface / hooked wire / needle Surface : noninvasive > kinesiology Hooked wire Research (limited to superficial muscles; poor specificity) Functional diagnosis (dyskinetic dysphonia) Therapy : Feedback Research (specificity of muscles; multiple channel; correlation with physiological parameters ) Needle electrode Motor neuron disease + neuromuscular junction + myopathies
6 Surface EMG
7 Surface / hooked wire / needle Surface : noninvasive > kinesiology Hooked wire Research (limited to superficial muscles; poor specificity) Functional diagnosis (dyskinetic dysphonia) Therapy : Feedback Research (specificity of muscles; multiple channel; correlation with physiological parameters ) Needle electrode Motor neuron disease + neuromuscular junction + myopathies

8

9


10

11

12

13
14
15 Surface / hooked wire / needle Surface : noninvasive > kinesiology Hooked wire Research (limited to superficial muscles; poor specificity) Functional diagnosis (dyskinetic dysphonia) Therapy : Feedback Research (specificity of muscles; multiple channel; correlation with physiological parameters ) Needle electrode Motor neuron disease + neuromuscular junction + myopathies
16
17 EMG laryngée Indication basique : «toute pathologie du mouvement relative au mécanisme phonatoire» Y compris les expertises médico- légales, vu le caractère objectif



18

19
20

21
22 Indication basique : EMG laryngée «toute pathologie du mouvement relative au mécanisme phonatoire» Y compris les expertises médicolégales, vu le caractère objectif?


23 EMG LEMG
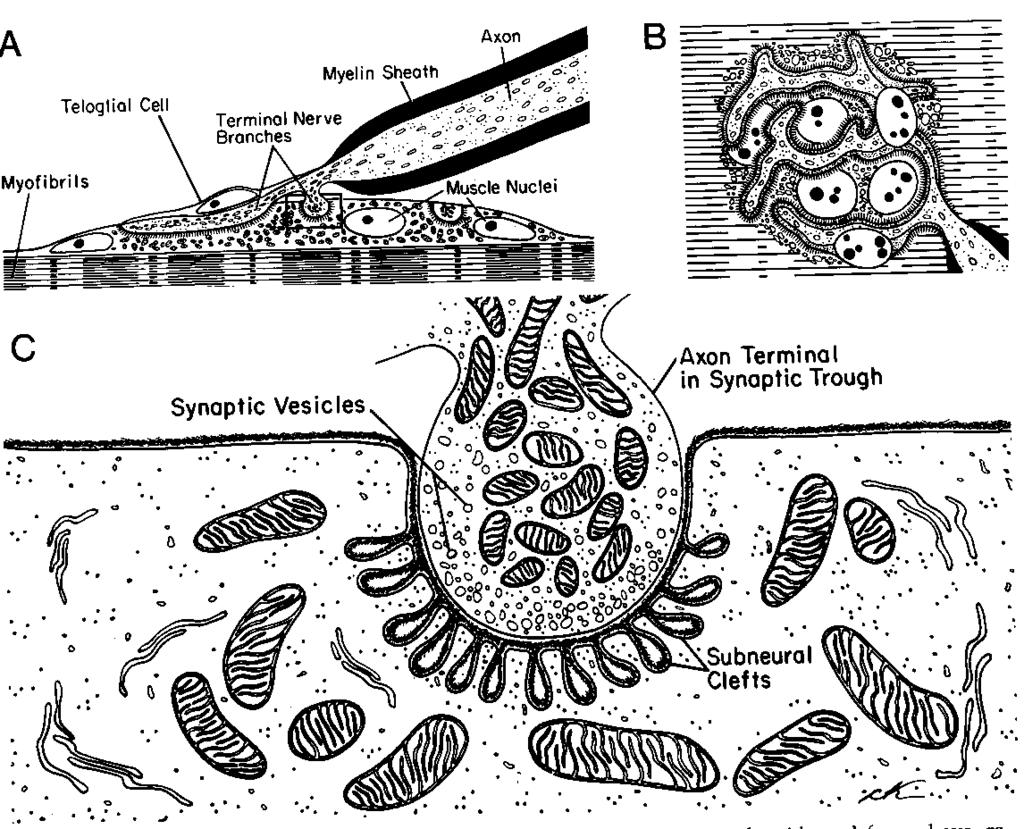
24 Specificities of intrinsic laryngeal muscles Small muscles (Voc : 300 mg; CT : 900 mg) Small MUs (quite low innervation ratio : muscle fibres / nerve fibre), particularly the M. Voc. Possible dual or multiple innervation of the same muscle fibre Shorter MUPs than skeletal muscles Microphonic effect

25 Triple motor endplate in a human thyroarytenoid muscle
26
27
28 EMG laryngée Indication basique : «toute pathologie du mouvement relative au mécanisme phonatoire» Y compris les expertises médico- légales, vu le caractère objectif
29 Laryngeal Mobility Disorders 1. Reduced mobility 2. Abnormal movements ( movement disorders )
30 Central Peripheral
31 Reduced mobility (1) 1. Neuromuscular etiology Paresis Paralysis peripheral motorneuron supranuclear neuromuscular junction myopathy peripheral motorneuron neuromuscular junction
32 Reduced mobility (2) 1. Mechanical etiology infiltration ankylosis (?) luxation (?) arthritis / arthrosis

33
34
35 Abnormal movements (1) * Bradykinesis usually generalized (M. Parkinson) * Dystonia (spasmodicity) - focal - segmental - multifocal - generalized

36

37 Spasmodic dysphonia pre treatment
38 Abnormal movements (2) * Tremor - essential - in neurological context Parkinson (rest) cerebellar ataxia (phonation) polyneuropathy * Myoclonus - essential - brainstem (mostly supranuclear)
39
40 Unilateral Vocal Fold Paralysis / Paresis
 dyspnoea : : NOLI TANGERE!")
41 Bilateral paralysis with (even slight) dyspnoea : : NOLI TANGERE!!!

42
43
44 Unilateral Vocal Fold paralysis / paresis
45

46
47
48

49
50
51

52 !
53 Causes of unilateral VF paralysis/paresis * Congenital (birth trauma?) * Trauma - wounds, blunt traumata - fracture skull base - surgery : skull basis, neck (thyroid!) - internal (cuff intubation tube) (?) * Compression - tumor, lymph node, aneurysma, * Tumor - neurinoma, chemodectoma * Infection : viral mononeuritis (?) * Idiopathic

54 Surgical Causes of Vocal Cord Paralysis
55 Pre-phonatory tuning Rest activity, slightly rhythmic (respiration)
56
57
58 > 25 / s
59
60
61
62
63
64 Evaluation EMG (general)
65 Discrepancies laryngoscopy - EMG 71 cases of unilateral paresis (laryngoscopy) 58 : EMG partial neurogenic peripheral damage NLI 13 : EMG normal 179 cases of partial neurogenic damage EMG (M. Voc) 119 : laryngoscopic paralysis 58 : laryngoscopic paresis 2 : normal mobility
66 Reasons for discrepancy EMG - Laryngoscopy Anatomical particularities / variants Bilateral innervation of IA Anastomosis NLS NLI Controlateral innervation Mechanical factors Laryngeal torsion / asymmetry Joint fibrosis Paradoxical reinnervation Muscle atrophy / fibrosis

67

68

69
70 Reasons for discrepancy EMG - Laryngoscopy Anatomical particularities / variants Bilateral innervation of IA Anastomosis NLS NLI Controlateral innervation Mechanical factors Laryngeal torsion / asymmetry Joint fibrosis Paradoxical reinnervation Muscle atrophy / fibrosis
71
72 Reasons for discrepancy EMG - Laryngoscopy Anatomical particularities / variants Bilateral innervation of IA Anastomosis NLS NLI Controlateral innervation Mechanical factors Laryngeal torsion / asymmetry Joint fibrosis Paradoxical reinnervation Muscle atrophy / fibrosis

73
74 Reasons for discrepancy EMG - Laryngoscopy Anatomical particularities / variants Bilateral innervation of IA Anastomosis NLS NLI Controlateral innervation Mechanical factors Laryngeal torsion / asymmetry Joint fibrosis Paradoxical reinnervation Muscle atrophy / fibrosis

75
76 SUMMARY Differential diagnosis : peripheral neurogenic damage vs. other etiology (central / mechanical) Partial / total? Presence of collateral regeneration? Reinnervation? Topography?

77
78 Additional entities Myasthenia Myopathies Spasmodic dysphonia

79 Autoimmune disorder characterized by Ab against Acetylcholine receptors at the postsynaptic junction Myasthenia Gravis Manifests as: Fluctuating muscle weakness Fatiguability Eye muscle weakness NOTES: Eye muscle weakness defines the characteristics of this disease. There are five classes for MG ranging from minimal eye weakness to severe with associated limb abnormalities or bulbar abnormalities affecting the cranial nerves. Of clinical note, a thymoma, if present, should be excised as there is a strong correlation between MG and a thymoma being present.
80

81

82
83 Position of Paralyzed Fold Initially thought to be related to site of injury. RLN versus vagal (RLN + SLN) Paramedian = RLN injury Lateral = RLN + SLN injury Cricothyroid muscle (SLN) was believed to influence the vocal fold position in laryngeal paralysis.
84 Position of Paralyzed Cord 27 Pts with unilateral VF Paralysis underwent FOL and LEMG. VF positions were paramedian in 8 patients, intermediate in 7, and lateral in 11. LEMG, 13 patients had isolated recurrent laryngeal nerve lesions and 13 patients had combined (superior and recurrent laryngeal nerve) lesions. No correlation between the vocal fold position and the status of the cricothyroid muscle.
85 The patient s point of view : Surgical treatment options depend on prognosis? Also age, life expextancy, occupation, compliance to ST, comorbidity, swallowing problems etc
86
87



88 Medialization Laryngoplasty


89 Medialization Laryngoplasty


90 Arytenoid Adduction

91

92 Vocal Fold Injection Short Term Long Term (?)


93

94
95 TREATMENT OF BILATERAL VFP
96 Treatment

97 Cordotomy


98 Re-Innervation Concept that nerve fibers from surrounding areas will re-stimulate the muscles of the Recurrent Laryngeal Nerve Can be achieved surgically as well: Ansa Cervicalis Phrenic Preganglionic Sympathetic Neurons NOTES: Re-Innervation is beneficial because muscles tend to atrophy unless they maintain innervation. Whether this is done naturally or surgically, it helps to create stability to the TVF which allows for better contact and voice. Reinnervation of the TA muscle restores tension resulting in a more normal mucosal wave. Reinnervation of the PCA and LA muscles stabilizesthe arytenoids and prevents inferior displacement of the vocal process, which may occur in some patients.


99 Re-Innervation, cont. Typical Connections: Ansa RLN Hypoglossal RLN Ansa Thyroarytenoid Pedicle 15 months Pre-Surgical observation time Signs of Reinnervation by 4 months post-op Thyroid cancer was the most common cause of patients undergoing re-innervation Best Measure of Surgical Improvement is MPT NOTES: The amount of time following initial visit/event to surgical time was 15 months. In a meta-analysis, most patients were followed around 4 months after surgery. Their improvements were measured by Maximum Phonation Time which was nearly doubled in all studies. Glottic gap was also improved in all studies that reported this finding. While these findings make reinnervation a viable possibility, it is not performed alone with any frequency and not compared to injection thyroplasty or medialization. Most studies reporting on Re-innervation combine this procedure with injection or medialization procedures. Only six studies have demonstrated viable results in humans. There has also been no direct comparison with trials comparing reinnervation with thyroplasty.
100 When all else fails?

101 Biofeedback in swallowing disorders
102 Therapy with semg
103 Conclusion Les atouts de l EMG laryngée : La kinésiologie La recherche en physiologie laryngée Les myopathies et les affections de la jonction neuromusculaire Quelques diagnostics différentiels spécifiques (p. ex. : neurogène vs. mécanique dans un larynx posttraumatique) Le choix du côté à opérer pour une cordotomie (Kashima) : patient trachéotomisé! Contexte de techniques de pointe : pacing, réinnervation, transplantation Bio feedback en déglutologie
104 Indication basique : EMG laryngée «toute pathologie du mouvement relative au mécanisme phonatoire» Y compris les expertises médicolégales, vu le caractère objectif?

105 Merci de votre attention!

106
Superior Laryngeal Nerve Injury: Diagnosis and Management. Presented by: Nyall London October 10, 2014
 Superior Laryngeal Nerve Injury: Diagnosis and Management Presented by: Nyall London October 10, 2014 1 Case Presentation 49 year old male s/p right side approach anterior cervical discectomy and fusion
Superior Laryngeal Nerve Injury: Diagnosis and Management Presented by: Nyall London October 10, 2014 1 Case Presentation 49 year old male s/p right side approach anterior cervical discectomy and fusion
Vocal Cord Paresis:Background and Case Reports The Greater Baltimore Medical Center, The Johns Hopkins Voice Center at GBMC Stroboscopy Grand Rounds
 Presented by: David F Smith, MD, PhD March 2, 2012 Vocal Cord Paresis:Background and Case Reports The Greater Baltimore Medical Center, The Johns Hopkins Voice Center at GBMC Stroboscopy Grand Rounds 1
Presented by: David F Smith, MD, PhD March 2, 2012 Vocal Cord Paresis:Background and Case Reports The Greater Baltimore Medical Center, The Johns Hopkins Voice Center at GBMC Stroboscopy Grand Rounds 1
BILATERAL ABDUCTOR VOCAL CORD PALSY. Dr NITYA G Final year PG KIMS
 BILATERAL ABDUCTOR VOCAL CORD PALSY Dr NITYA G Final year PG KIMS INTRODUCTION Vocal cord paralysis is a sign of a disease It results from dysfunction of Recurrent laryngeal nerves on both sides Paralysis
BILATERAL ABDUCTOR VOCAL CORD PALSY Dr NITYA G Final year PG KIMS INTRODUCTION Vocal cord paralysis is a sign of a disease It results from dysfunction of Recurrent laryngeal nerves on both sides Paralysis
Contents. Part A Clinical Evaluation of Laryngeal Disorders. 3 Videostroboscopy and Dynamic Voice Evaluation with Flexible Laryngoscopy...
 Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Case Presentation JC: 65 y/o retired plumber CC: Hoarseness HPI: Admitted to a local hospital on May 30 for severe pneumonia. Intubated in ICU for 10
 GBMC Stroboscopy Rounds October 12, 2007 Case Presentation JC: 65 y/o retired plumber CC: Hoarseness HPI: Admitted to a local hospital on May 30 for severe pneumonia. Intubated in ICU for 10 days, total
GBMC Stroboscopy Rounds October 12, 2007 Case Presentation JC: 65 y/o retired plumber CC: Hoarseness HPI: Admitted to a local hospital on May 30 for severe pneumonia. Intubated in ICU for 10 days, total
Hoarseness. Common referral Hoarseness reflects any abnormality of normal phonation
 Hoarseness Kevin Katzenmeyer, MD Faculty Advisor: Byron J Bailey, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 24, 2001 Hoarseness Common referral
Hoarseness Kevin Katzenmeyer, MD Faculty Advisor: Byron J Bailey, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 24, 2001 Hoarseness Common referral
Sunshine Act Disclosure
 A Laryngologist s Approach to Voice Presentation at the Nebraska Speech- Language-Hearing Association Fall Convention Thursday, September 27, 2018 15:45-16:45 Christopher M. Bingcang, MD Assistant Professor
A Laryngologist s Approach to Voice Presentation at the Nebraska Speech- Language-Hearing Association Fall Convention Thursday, September 27, 2018 15:45-16:45 Christopher M. Bingcang, MD Assistant Professor
Supplementary Online Content
 Supplementary Online Content Wang C-C, Chang M-H, Jiang R-S, et al. Laryngeal electromyography-guided hyaluronic acid vocal fold injection for unilateral vocal fold paralysis: a prospective long-term follow-up
Supplementary Online Content Wang C-C, Chang M-H, Jiang R-S, et al. Laryngeal electromyography-guided hyaluronic acid vocal fold injection for unilateral vocal fold paralysis: a prospective long-term follow-up
Effect of Intralaryngeal Muscle Synkinesis on Perception of Voice Handicap in Patients With Unilateral Vocal Fold Paralysis
 The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Effect of Intralaryngeal Muscle Synkinesis on Perception of Voice Handicap in Patients With Unilateral Vocal
The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Effect of Intralaryngeal Muscle Synkinesis on Perception of Voice Handicap in Patients With Unilateral Vocal
Vocal Cord Medialization Medialization Laryngoplasty
 Vocal Cord Medialization Medialization Laryngoplasty Carolyn Waddington RN MSN FNP CORLN The Methodist Hospital Houston, TX SOHN, Boston, 2010 Objectives Describe the history of the first treatments for
Vocal Cord Medialization Medialization Laryngoplasty Carolyn Waddington RN MSN FNP CORLN The Methodist Hospital Houston, TX SOHN, Boston, 2010 Objectives Describe the history of the first treatments for
MSA. Sleep disorders MULTIPLE SYSTEM ATROPHY AND NOCTURNAL STRIDOR 1/26/2015. Alex Iranzo Neurology Service Hospital Clinic de Barcelona Spain
 MULTIPLE SYSTEM ATROPHY AND NOCTURNAL STRIDOR Alex Iranzo Neurology Service Hospital Clinic de Barcelona Spain MSA Neurodegenerative disease Parkinsonism, cerebellar, dysautonomia Mean survival is less
MULTIPLE SYSTEM ATROPHY AND NOCTURNAL STRIDOR Alex Iranzo Neurology Service Hospital Clinic de Barcelona Spain MSA Neurodegenerative disease Parkinsonism, cerebellar, dysautonomia Mean survival is less
Disclosures. Primary Methods for Treating UVP. Key Factors Influencing Treatment Planning. Guiding principle with Treatment Planning 2/4/2018
 Zen and art of vocal mechanics: Key Factors That Influence Unilateral Vocal Fold Paralysis (UVP) Treatment Decisions Julie Barkmeier Kraemer, Ph.D. Professor, Division of Otolaryngology Clinic Director,
Zen and art of vocal mechanics: Key Factors That Influence Unilateral Vocal Fold Paralysis (UVP) Treatment Decisions Julie Barkmeier Kraemer, Ph.D. Professor, Division of Otolaryngology Clinic Director,
Laryngeal electromyography findings of vocal fold immobility in patients after radiotherapy for nasopharyngeal carcinoma
 ORIGINAL ARTICLE Laryngeal electromyography findings of vocal fold immobility in patients after radiotherapy for nasopharyngeal carcinoma Yi-Ling Hsieh, MD, 1 Ming-Hong Chang, MD, 2 Chen-Chi Wang, MD 1,3,4*
ORIGINAL ARTICLE Laryngeal electromyography findings of vocal fold immobility in patients after radiotherapy for nasopharyngeal carcinoma Yi-Ling Hsieh, MD, 1 Ming-Hong Chang, MD, 2 Chen-Chi Wang, MD 1,3,4*
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation
 Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Vocal Fold Motion Impairment. Surgical options 10/17/2008. Voice Changes after Treatment for Bilateral Vocal Fold Motion Impairment
 Voice Changes after Treatment for Bilateral Vocal Fold Motion Impairment Betty S. Tsai, MD Mark S. Courey, MD Sarah L. Schneider, MS, CCC-SLP Soha Al-Jurf, MS, CCC-SLP UCSF Department of Otolaryngology
Voice Changes after Treatment for Bilateral Vocal Fold Motion Impairment Betty S. Tsai, MD Mark S. Courey, MD Sarah L. Schneider, MS, CCC-SLP Soha Al-Jurf, MS, CCC-SLP UCSF Department of Otolaryngology
Lisa T. Fry, PhD Marshall University. Joseph C. Stemple, PhD University of Kentucky
 Lisa T. Fry, PhD Marshall University Joseph C. Stemple, PhD University of Kentucky Muscular Components of Voice Disorders Resonance Requires balance among the 3 Phonation Disruption in 1 may perturb the
Lisa T. Fry, PhD Marshall University Joseph C. Stemple, PhD University of Kentucky Muscular Components of Voice Disorders Resonance Requires balance among the 3 Phonation Disruption in 1 may perturb the
Electrophysiological studies. Dr Carmen Górriz Gil Otorhinolaryngologist Voice Unit
 Electrophysiological studies Dr Carmen Górriz Gil Otorhinolaryngologist Voice Unit Who does LEMG? ENT + Neurophysiologist, neurologist Dr Martínez Dr Álvarez Dr Gª Berrocal Dr Vicente EMG Technique Sitting
Electrophysiological studies Dr Carmen Górriz Gil Otorhinolaryngologist Voice Unit Who does LEMG? ENT + Neurophysiologist, neurologist Dr Martínez Dr Álvarez Dr Gª Berrocal Dr Vicente EMG Technique Sitting
Analysis of Laryngoscopic Features in Patients With Unilateral Vocal Fold Paresis
 The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Analysis of Laryngoscopic Features in Patients With Unilateral Vocal Fold Paresis Peak Woo, MD; Arjun K.
The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Analysis of Laryngoscopic Features in Patients With Unilateral Vocal Fold Paresis Peak Woo, MD; Arjun K.
The Immobile Vocal Fold: Paralysis vs. Fixation
 The Immobile Vocal Fold: Paralysis vs. Fixation DISCLOSURE Ted Mau, MD PhD Director UT Southwestern Voice Center I have nothing to disclose www.utsouthwestern.org/voice DALLAS, TEXAS OUTLINE Terminology
The Immobile Vocal Fold: Paralysis vs. Fixation DISCLOSURE Ted Mau, MD PhD Director UT Southwestern Voice Center I have nothing to disclose www.utsouthwestern.org/voice DALLAS, TEXAS OUTLINE Terminology
Laryngeal Electromyography: Basic Concepts and Clinical Uses
 Robert T. Sataloff, M.D., D.M.A. Robert T. Sataloff, M.D., D.M.A. Laryngeal Electromyography: Basic Concepts and Clinical Uses Yolanda D. Heman-Ackah, M.D. and Robert T. Sataloff, M.D., D.M.A. UNDERSTANDING
Robert T. Sataloff, M.D., D.M.A. Robert T. Sataloff, M.D., D.M.A. Laryngeal Electromyography: Basic Concepts and Clinical Uses Yolanda D. Heman-Ackah, M.D. and Robert T. Sataloff, M.D., D.M.A. UNDERSTANDING
Causes of recurrent laryngeal nerve paralysis
 Auris Nasus Larynx 29 (2002) 41 45 www.elsevier.com/locate/anl Causes of recurrent laryngeal nerve paralysis Eiji Yumoto a, *, Ryosei Minoda a, Masamitsu Hyodo b, Takahiko Yamagata b a Department of Otolaryngology-Head
Auris Nasus Larynx 29 (2002) 41 45 www.elsevier.com/locate/anl Causes of recurrent laryngeal nerve paralysis Eiji Yumoto a, *, Ryosei Minoda a, Masamitsu Hyodo b, Takahiko Yamagata b a Department of Otolaryngology-Head
Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis
 Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis Denervation and Reinnervation Eiji Yumoto 123 Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis Eiji Yumoto
Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis Denervation and Reinnervation Eiji Yumoto 123 Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis Eiji Yumoto
Innervation of the cricothyroid muscle by the recurrent laryngeal nerve
 ORIGINAL ARTICLE Innervation of the cricothyroid muscle by the recurrent laryngeal nerve Hiroo Masuoka, MD, PhD,* Akira Miyauchi, MD, PhD, Tomonori Yabuta, MD, PhD, Mitsuhiro Fukushima, MD, PhD, Akihiro
ORIGINAL ARTICLE Innervation of the cricothyroid muscle by the recurrent laryngeal nerve Hiroo Masuoka, MD, PhD,* Akira Miyauchi, MD, PhD, Tomonori Yabuta, MD, PhD, Mitsuhiro Fukushima, MD, PhD, Akihiro
POST-OPERATIVE LARYNGEAL COMPLICATIONS AFTER ENDOCRINE SURGERY
 POST-OPERATIVE LARYNGEAL COMPLICATIONS AFTER ENDOCRINE SURGERY Amy L. Rutt, D.O. Mayo Clinic Jacksonville, FL AOCOO-HNS Foundation 2015 MFMER slide-1 Etiology 1985-1995 (n=280) 1995-2005 (n=363) Overall
POST-OPERATIVE LARYNGEAL COMPLICATIONS AFTER ENDOCRINE SURGERY Amy L. Rutt, D.O. Mayo Clinic Jacksonville, FL AOCOO-HNS Foundation 2015 MFMER slide-1 Etiology 1985-1995 (n=280) 1995-2005 (n=363) Overall
VOCAL CORD PALSY. Department of ENT, Head and Neck Surgery DR OSEGHALE DR AKPALABA
 VOCAL CORD PALSY Department of ENT, Head and Neck Surgery DR OSEGHALE DR AKPALABA Case Presentation M /70 years Pensioner Christain Bini Resides in Benin Had total thyroidectomy. Follicular Ca of thyroid
VOCAL CORD PALSY Department of ENT, Head and Neck Surgery DR OSEGHALE DR AKPALABA Case Presentation M /70 years Pensioner Christain Bini Resides in Benin Had total thyroidectomy. Follicular Ca of thyroid
Cricothyroid Muscle Dysfunction Impairs Vocal Fold Vibration in Unilateral Vocal Fold Paralysis
 The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Cricothyroid Muscle Dysfunction Impairs Vocal Fold Vibration in Unilateral Vocal Fold Paralysis Yu-Cheng
The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Cricothyroid Muscle Dysfunction Impairs Vocal Fold Vibration in Unilateral Vocal Fold Paralysis Yu-Cheng
A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility
 Original Article Submitted: 3 Aug 2015 Accepted: 6 Mar 2016 A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility Azman MAWADDAH 1, Mat Baki MARINA 1, Sawali
Original Article Submitted: 3 Aug 2015 Accepted: 6 Mar 2016 A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility Azman MAWADDAH 1, Mat Baki MARINA 1, Sawali
Objectives. Purpose. Conference Calls 2 hrs. Process 9/7/2013. Clinical Practice Guideline: Improving Voice Outcomes after Thyroid Surgery
 Objectives Clinical Practice Guideline: Improving Voice Outcomes after Thyroid Surgery 37 th Annual Congress & Nursing Symposium Vancouver, BC September 29, 2013 Carolyn Waddington RN MS FNP-C CORLN Explain
Objectives Clinical Practice Guideline: Improving Voice Outcomes after Thyroid Surgery 37 th Annual Congress & Nursing Symposium Vancouver, BC September 29, 2013 Carolyn Waddington RN MS FNP-C CORLN Explain
Making sense of Nerve conduction & EMG
 Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
Laryngeal Biomechanics: An Overview of Mucosal Wave Mechanics
 Journal of Voice Vol. 7, No. 2, pp. 123-128 1993 Raven Press, Lt~l., New York Laryngeal Biomechanics: An Overview of Mucosal Wave Mechanics Gerald S. Berke and Bruce R. Gerratt Head and Neck Surgery, University
Journal of Voice Vol. 7, No. 2, pp. 123-128 1993 Raven Press, Lt~l., New York Laryngeal Biomechanics: An Overview of Mucosal Wave Mechanics Gerald S. Berke and Bruce R. Gerratt Head and Neck Surgery, University
Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB
 Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB 2.11.16 Disclosures I have no relevant conflicts or potential conflicts to disclose regarding
Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB 2.11.16 Disclosures I have no relevant conflicts or potential conflicts to disclose regarding
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
CLINICAL APPLICATION AND RESULTS OF THE ELECTROPHYSIOLOGICAL LARYNGEAL NERVES IDENTIFICATION IN SURGERIES IN CASE OF GOITER
 Archives of the Balkan Medical Union Copyright 208 Balkan Medical Union vol., no., pp. 2-28 March 208 ORIGINAL PAPER CLINICAL APPLICATION AND RESULTS OF THE ELECTROPHYSIOLOGICAL LARYNGEAL NERVES IDENTIFICATION
Archives of the Balkan Medical Union Copyright 208 Balkan Medical Union vol., no., pp. 2-28 March 208 ORIGINAL PAPER CLINICAL APPLICATION AND RESULTS OF THE ELECTROPHYSIOLOGICAL LARYNGEAL NERVES IDENTIFICATION
Identification number: TÁMOP /1/A
 Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
A Comparison of Outcomes in Interventions for Unilateral Vocal Fold Paralysis: A Systematic Review
 The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Systematic Review A Comparison of Outcomes in Interventions for Unilateral Vocal Fold Paralysis: A Systematic
The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Systematic Review A Comparison of Outcomes in Interventions for Unilateral Vocal Fold Paralysis: A Systematic
Voice Restoration in Presbyphonia. Strobe Rounds March 10 th, 2017 Andrew H. Lee, MD PGY2
 Voice Restoration in Presbyphonia Strobe Rounds March 10 th, 2017 Andrew H. Lee, MD PGY2 1 Disclaimers & Disclosures None 2 3 Agenda Background Etiology Management Options 4 Background Structural changes
Voice Restoration in Presbyphonia Strobe Rounds March 10 th, 2017 Andrew H. Lee, MD PGY2 1 Disclaimers & Disclosures None 2 3 Agenda Background Etiology Management Options 4 Background Structural changes
Recurrent Laryngeal Nerve Recovery Patterns Assessed by Serial Electromyography
 The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Recurrent Laryngeal Nerve Recovery Patterns Assessed by Serial Electromyography Randal C. Paniello, MD, PhD;
The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Recurrent Laryngeal Nerve Recovery Patterns Assessed by Serial Electromyography Randal C. Paniello, MD, PhD;
Normal Voice. Evaluation of a Patient with Hoarseness. No disclosures. Hoarseness. Assessment. Assessment
 Evaluation of a Patient with Hoarseness No disclosures Mari Hagiwara, MD NYU Langone Medical Center ASHNR 2017 Hoarseness Symptom: any deviation from normal voice quality as perceived by self or others;
Evaluation of a Patient with Hoarseness No disclosures Mari Hagiwara, MD NYU Langone Medical Center ASHNR 2017 Hoarseness Symptom: any deviation from normal voice quality as perceived by self or others;
Chapter 112: Phonosurgical Procedures. Paul W. Flint, Charles W. Cummings
 Chapter 112: Phonosurgical Procedures Paul W. Flint, Charles W. Cummings While still in its infancy, laryngeal phonosurgery has grown to encompass a variety of procedures designed to effect alterations
Chapter 112: Phonosurgical Procedures Paul W. Flint, Charles W. Cummings While still in its infancy, laryngeal phonosurgery has grown to encompass a variety of procedures designed to effect alterations
A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility
 Original Original Article Submitted: 3 Aug 2015 Accepted: 6 Mar 2016 Online: 30 June 2016 A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility Azman Mawaddah
Original Original Article Submitted: 3 Aug 2015 Accepted: 6 Mar 2016 Online: 30 June 2016 A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility Azman Mawaddah
Larynx - cartilaginous structure holding the vocal folds which protrude into airstream
 1! Larynx - cartilaginous structure holding the vocal folds which protrude into airstream 2! Flow increase - like thumb over garden hose Pressure drop - narrower space forces pressure drop due to speed
1! Larynx - cartilaginous structure holding the vocal folds which protrude into airstream 2! Flow increase - like thumb over garden hose Pressure drop - narrower space forces pressure drop due to speed
Evaluating the timing of injection laryngoplasty for vocal fold paralysis in an attempt to avoid future type 1 thyroplasty
 Alghonaim et al. Journal of Otolaryngology - Head and Neck Surgery 2013, 42:24 ORIGINAL RESEARCH ARTICLE Open Access Evaluating the timing of injection laryngoplasty for vocal fold paralysis in an attempt
Alghonaim et al. Journal of Otolaryngology - Head and Neck Surgery 2013, 42:24 ORIGINAL RESEARCH ARTICLE Open Access Evaluating the timing of injection laryngoplasty for vocal fold paralysis in an attempt
Prior Authorization Review Panel MCO Policy Submission
 Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions. 4 May 2012
 SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions 4 May 2012 1. With regard to the muscles of the neck: a. the platysma muscle is supplied by the accessory nerve. b. the stylohyoid muscle is supplied by
SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions 4 May 2012 1. With regard to the muscles of the neck: a. the platysma muscle is supplied by the accessory nerve. b. the stylohyoid muscle is supplied by
Benign Lesions of the Vocal Folds
 Benign Lesions of the Vocal Folds Noah Meltzer, M.D. Zandy Hillel, M.D. December 14, 2007 Learning Objectives 1) Review the presentation, pathophysiology, and stroboscopic exams of benign vocal fold lesions.
Benign Lesions of the Vocal Folds Noah Meltzer, M.D. Zandy Hillel, M.D. December 14, 2007 Learning Objectives 1) Review the presentation, pathophysiology, and stroboscopic exams of benign vocal fold lesions.
 This article was published in an Elsevier journal. The attached copy is furnished to the author for non-commercial research and education use, including for instruction at the author s institution, sharing
This article was published in an Elsevier journal. The attached copy is furnished to the author for non-commercial research and education use, including for instruction at the author s institution, sharing
Structure and Nerve Supply of The Larynx
 Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical sciences Structure and Nerve Supply of The Larynx This presentation was originally prepared by: Dr. Kumar Notes were added by:
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical sciences Structure and Nerve Supply of The Larynx This presentation was originally prepared by: Dr. Kumar Notes were added by:
Evaluation of the Hoarse Patient
 Evaluation of the Hoarse Patient Herve J. LeBoeuf, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation May 17, 2000 Anatomy- Vagus N. ambiguus: Motor - skeletal
Evaluation of the Hoarse Patient Herve J. LeBoeuf, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation May 17, 2000 Anatomy- Vagus N. ambiguus: Motor - skeletal
Hoarseness. Evidence-based Key points for Approach
 Hoarseness Evidence-based Key points for Approach Sasan Dabiri, Assistant Professor Department of otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medial Sciences Definition:
Hoarseness Evidence-based Key points for Approach Sasan Dabiri, Assistant Professor Department of otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medial Sciences Definition:
Index. Note: Page numbers of article titles are in boldface type.
 Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Treatment of Adductor Spasmodic Dysphonia with Selective Laryngeal Adductor Denervation and Reinnervation Surgery
 Otolaryngol Clin N Am 39 (2006) 101 109 Treatment of Adductor Spasmodic Dysphonia with Selective Laryngeal Adductor Denervation and Reinnervation Surgery Dinesh K. Chhetri, MD*, Gerald S. Berke, MD Division
Otolaryngol Clin N Am 39 (2006) 101 109 Treatment of Adductor Spasmodic Dysphonia with Selective Laryngeal Adductor Denervation and Reinnervation Surgery Dinesh K. Chhetri, MD*, Gerald S. Berke, MD Division
Cadaveric position of unilateral vocal cord: a case of cricoid fracture with ipsilateral arytenoid dislocation
 Cadaveric position of unilateral vocal cord: a case of cricoid fracture with ipsilateral Nirmalkumar Gopalakrishnan 1*, Kalaichezhian Mariappan 1, Venkatraman Indiran 1, Prabakaran Maduraimuthu 1, Chandrasekhar
Cadaveric position of unilateral vocal cord: a case of cricoid fracture with ipsilateral Nirmalkumar Gopalakrishnan 1*, Kalaichezhian Mariappan 1, Venkatraman Indiran 1, Prabakaran Maduraimuthu 1, Chandrasekhar
For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER
 GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
Using CT to Localize Side and Level of Vocal Cord Paralysis
 Shy-Chyi Chin 1 Simon Edelstein 2 Cheng-Yu Chen 1 Peter M. Som 2 Received May 16, 2002; accepted after revision ugust 29, 2002. 1 Department of Radiology, Tri-Service General Hospital, National Defense
Shy-Chyi Chin 1 Simon Edelstein 2 Cheng-Yu Chen 1 Peter M. Som 2 Received May 16, 2002; accepted after revision ugust 29, 2002. 1 Department of Radiology, Tri-Service General Hospital, National Defense
Graded activation of the intrinsic laryngeal muscles for vocal fold posturing
 Graded activation of the intrinsic laryngeal muscles for vocal fold posturing Dinesh K. Chhetri, a) Juergen Neubauer, and David A. Berry The Laryngeal Dynamics and Physiology Laboratories, Division of
Graded activation of the intrinsic laryngeal muscles for vocal fold posturing Dinesh K. Chhetri, a) Juergen Neubauer, and David A. Berry The Laryngeal Dynamics and Physiology Laboratories, Division of
Table of Contents. Preface... xi. Part I: Introduction to Movement Disorders
 Table of Contents Visit www.healthreferenceseries.com to view A Contents Guide to the Health Reference Series, a listing of more than 14,000 topics and the volumes in which they are covered. Preface...
Table of Contents Visit www.healthreferenceseries.com to view A Contents Guide to the Health Reference Series, a listing of more than 14,000 topics and the volumes in which they are covered. Preface...
Cranial Nerve Monitoring Part II: What do I have to do if cranial nerves are being monitored?
 Cranial Nerve Monitoring Part II: What do I have to do if cranial nerves are being monitored? Laura Hemmer, M.D., FASA SNACC Neuromonitoring Subcommittee Linda S. Aglio, M.D., M.S. Arne Budde, M.D. Laura
Cranial Nerve Monitoring Part II: What do I have to do if cranial nerves are being monitored? Laura Hemmer, M.D., FASA SNACC Neuromonitoring Subcommittee Linda S. Aglio, M.D., M.S. Arne Budde, M.D. Laura
Carcinoma of the larynx L 4. Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%.
 L 4 Carcinoma of the larynx Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%. Incidence: It is more common in males than females in ratio 5:1.
L 4 Carcinoma of the larynx Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%. Incidence: It is more common in males than females in ratio 5:1.
DISORDERS OF THE MOTOR SYSTEM. Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
DISORDERS OF THE MOTOR SYSTEM Jeanette J. Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine THE MOTOR SYSTEM To understand disorders of the motor system, we need to review how a
Continuing Education Independent Study Series
 Continuing Education Independent Study Series Association of Surgical Technologists Publication made possible by an educational grant provided by Kim berly-clark Corporation OF SURGICAL Association of
Continuing Education Independent Study Series Association of Surgical Technologists Publication made possible by an educational grant provided by Kim berly-clark Corporation OF SURGICAL Association of
Vocal Fold Paralysis: Improved Adductor Recovery by Vincristine Blockade of Posterior Cricoarytenoid
 The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Vocal Fold Paralysis: Improved Adductor Recovery by Vincristine Blockade of Posterior Cricoarytenoid Randal
The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Vocal Fold Paralysis: Improved Adductor Recovery by Vincristine Blockade of Posterior Cricoarytenoid Randal
CROSS-INNERVATION OF THE THYROARYTENOID MUSCLE BY A BRANCH FROM THE EXTERNAL DIVISION OF THE SUPERIOR LARYNGEAL NERVE
 Ann Owl Rltinol Laryngol 106:1997 CROSS-INNERVATION OF THE THYROARYTENOID MUSCLE BY A BRANCH FROM THE EXTERNAL DIVISION OF THE SUPERIOR LARYNGEAL NERVE SlNA NASRI, MD LAS VEGAS, NEVADA JOEL A. SERCARZ,
Ann Owl Rltinol Laryngol 106:1997 CROSS-INNERVATION OF THE THYROARYTENOID MUSCLE BY A BRANCH FROM THE EXTERNAL DIVISION OF THE SUPERIOR LARYNGEAL NERVE SlNA NASRI, MD LAS VEGAS, NEVADA JOEL A. SERCARZ,
Injection Laryngoplasty Outcomes in Irradiated and Nonirradiated Unilateral Vocal Fold Paralysis
 The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Injection Laryngoplasty Outcomes in Irradiated and Nonirradiated Unilateral Vocal Fold Paralysis Joseph Chang,
The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Injection Laryngoplasty Outcomes in Irradiated and Nonirradiated Unilateral Vocal Fold Paralysis Joseph Chang,
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
International Journal of Medical Science and Education pissn eissn
 Original research article International Journal of Medical Science and Education pissn- 2348 4438 eissn-2349-3208 INCIDENCE AND ETIO-PATHOGENESIS OF VOCAL CORD PARALYSIS IN A TERTIARY CARE HOSPITAL Natwar
Original research article International Journal of Medical Science and Education pissn- 2348 4438 eissn-2349-3208 INCIDENCE AND ETIO-PATHOGENESIS OF VOCAL CORD PARALYSIS IN A TERTIARY CARE HOSPITAL Natwar
Early management of laryngeal injuries'
 656 Journal of the Royal Society of Medicine Volume 74 September 1981 Early management of laryngeal injuries' A G D Maran MD FRCS Department of Otolaryngology, P M Stell chm FRCS Department of Otolaryngology,
656 Journal of the Royal Society of Medicine Volume 74 September 1981 Early management of laryngeal injuries' A G D Maran MD FRCS Department of Otolaryngology, P M Stell chm FRCS Department of Otolaryngology,
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
ISPUB.COM. Medialization Thyroplasty Using Silatic Implant. S Singh Yadav, J Singh Gulia, K Singh, S Singh INTRODUCTION MATERIAL AND METHODS
 ISPUB.COM The Internet Journal of Head and Neck Surgery Volume 1 Number 1 Medialization Thyroplasty Using Silatic Implant S Singh Yadav, J Singh Gulia, K Singh, S Singh Citation S Singh Yadav, J Singh
ISPUB.COM The Internet Journal of Head and Neck Surgery Volume 1 Number 1 Medialization Thyroplasty Using Silatic Implant S Singh Yadav, J Singh Gulia, K Singh, S Singh Citation S Singh Yadav, J Singh
New technologies in Endocrine Surgery
 New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
Clinical Policy Title: Supraglottoplasty and laryngoplasty
 Clinical Policy Title: Supraglottoplasty and laryngoplasty Clinical Policy Number: 07.03.02 Effective Date: April 1, 2015 Initial Review Date: January 21, 2015 Most Recent Review Date: February 15, 2017
Clinical Policy Title: Supraglottoplasty and laryngoplasty Clinical Policy Number: 07.03.02 Effective Date: April 1, 2015 Initial Review Date: January 21, 2015 Most Recent Review Date: February 15, 2017
Disorders of language and speech. Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology
 Disorders of language and speech Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology http://neurology.pote.hu major categories disorders of language and speech cortical types aphasias
Disorders of language and speech Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology http://neurology.pote.hu major categories disorders of language and speech cortical types aphasias
Voice Disorders in Medically Complex Children
 Voice Disorders in Medically Complex Children Roger C. Nuss, MD, FACS Geralyn Harvey Woodnorth, M.A., CCC-SLP Department of Otolaryngology and Communication Enhancement Children s Hospital Boston Harvard
Voice Disorders in Medically Complex Children Roger C. Nuss, MD, FACS Geralyn Harvey Woodnorth, M.A., CCC-SLP Department of Otolaryngology and Communication Enhancement Children s Hospital Boston Harvard
Clinical Policy Title: Supraglottoplasty and laryngoplasty
 Clinical Policy Title: Supraglottoplasty and laryngoplasty Clinical Policy Number: 07.03.02 Effective Date: April 1, 2015 Initial Review Date: January 21, 2015 Most Recent Review Date: February 15, 2017
Clinical Policy Title: Supraglottoplasty and laryngoplasty Clinical Policy Number: 07.03.02 Effective Date: April 1, 2015 Initial Review Date: January 21, 2015 Most Recent Review Date: February 15, 2017
MYASTHENIA GRAVIS. Mr. D.Raju, M.pharm, Lecturer
 MYASTHENIA GRAVIS Mr. D.Raju, M.pharm, Lecturer OUTLINE Background Anatomy Pathophysiology Clinical Presentation Treatment BACKGROUND Acquired autoimmune disorder Clinically characterized by: Weakness
MYASTHENIA GRAVIS Mr. D.Raju, M.pharm, Lecturer OUTLINE Background Anatomy Pathophysiology Clinical Presentation Treatment BACKGROUND Acquired autoimmune disorder Clinically characterized by: Weakness
Difficulties with: vision, hemosthasia, suture and flaps transposition
 Universidade Federal de São Paulo UNIFESP-EPM EPM New surgical technique for the larynx Transventricular Chondroplastic Laryngotomy - TCL Marcos Sarvat, Nédio Steffen, Henrique Olival-Costa, and Paulo
Universidade Federal de São Paulo UNIFESP-EPM EPM New surgical technique for the larynx Transventricular Chondroplastic Laryngotomy - TCL Marcos Sarvat, Nédio Steffen, Henrique Olival-Costa, and Paulo
Introduction. Kana Yoshioka 1 Akira Miyauchi. Minoru Kihara 2 Akihiro Miya
 World J Surg (2016) 40:2948 2955 DOI 10.1007/s00268-016-3634-7 ORIGINAL SCIENTIFIC REPORT Surgical Methods and Experiences of Surgeons did not Significantly Affect the Recovery in Phonation Following Reconstruction
World J Surg (2016) 40:2948 2955 DOI 10.1007/s00268-016-3634-7 ORIGINAL SCIENTIFIC REPORT Surgical Methods and Experiences of Surgeons did not Significantly Affect the Recovery in Phonation Following Reconstruction
SmartXide 2 - SmartXide HS
 SmartXide 2 - SmartXide HS Laryngeal Microsurgery with Scanner-Assisted CO 2 Laser White Paper - October 2011 White Paper SmartXide 2 - SmartXide HS October 2011 Laryngeal Microsurgery with Scanner-Assisted
SmartXide 2 - SmartXide HS Laryngeal Microsurgery with Scanner-Assisted CO 2 Laser White Paper - October 2011 White Paper SmartXide 2 - SmartXide HS October 2011 Laryngeal Microsurgery with Scanner-Assisted
Phonosurgery. The poor lymphatic drainage of the lamina propria predisposes it to collect tissue fluid (Reinke's oedema)
") Phonosurgery Phonosurgery is defined as 'any surgery designed primarily for the improvement or restoration of the voice'. Complete assessment of a patient with a voice disorder should now include video
Phonosurgery Phonosurgery is defined as 'any surgery designed primarily for the improvement or restoration of the voice'. Complete assessment of a patient with a voice disorder should now include video
A40-year-old woman presented to the otolaryngology
 CME Practice CMAJ Cases A case of hoarseness and vocal cord immobility Amy M. Trottier MSc MD, Emad Massoud MB, Timothy Brown MD Competing interests: None declared. This article has been peer reviewed.
CME Practice CMAJ Cases A case of hoarseness and vocal cord immobility Amy M. Trottier MSc MD, Emad Massoud MB, Timothy Brown MD Competing interests: None declared. This article has been peer reviewed.
Sleep-Disordered Breathing and Risk of Sudden Death in Multiple System Atrophy
 Sleep-Disordered Breathing and Risk of Sudden Death in Multiple System Atrophy Lisa Cutchen MD Sleep Medicine Fellow University of New Mexico Sleep Disorders Center New Mexico Thoracic Society February
Sleep-Disordered Breathing and Risk of Sudden Death in Multiple System Atrophy Lisa Cutchen MD Sleep Medicine Fellow University of New Mexico Sleep Disorders Center New Mexico Thoracic Society February
Chapter 12 Audio-visual analysis of vocal tremor derived from acoustics, laryngovideostroboscopy
 107 12 Audio-visual analysis of vocal tremor derived from acoustics, laryngovideostroboscopy & HSDI Chapter 12 Audio-visual analysis of vocal tremor derived from acoustics, laryngovideostroboscopy & HSDI
107 12 Audio-visual analysis of vocal tremor derived from acoustics, laryngovideostroboscopy & HSDI Chapter 12 Audio-visual analysis of vocal tremor derived from acoustics, laryngovideostroboscopy & HSDI
Timing of Nimodipine Therapy for the Treatment of Vocal Fold Paralysis
 The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Timing of Nimodipine Therapy for the Treatment of Vocal Fold Paralysis Shaum S. Sridharan, MD; Clark A. Rosen,
The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Timing of Nimodipine Therapy for the Treatment of Vocal Fold Paralysis Shaum S. Sridharan, MD; Clark A. Rosen,
Clinical application of laryngeal electromyography a point of view
 Romanian Journal of Rhinology, Vol. 7, No. 25, January-March 2017 Original study Clinical application of laryngeal electromyography a point of view Georgiana Pasu ENT&HNS Department, Sfanta Maria Hospital,
Romanian Journal of Rhinology, Vol. 7, No. 25, January-March 2017 Original study Clinical application of laryngeal electromyography a point of view Georgiana Pasu ENT&HNS Department, Sfanta Maria Hospital,
atrophy with autonomic failure
 Journal of Nelurology, Neurosurgery, and Psychiatry, 1981, 44, 49-53 Laryngeal electromyography in multiple system atrophy with autonomic G M GUINDI, R BANNISTER, W P R GIBSON, AND J K PAYNE From the National
Journal of Nelurology, Neurosurgery, and Psychiatry, 1981, 44, 49-53 Laryngeal electromyography in multiple system atrophy with autonomic G M GUINDI, R BANNISTER, W P R GIBSON, AND J K PAYNE From the National
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
Diseases of Muscle and Neuromuscular Junction
 Diseases of Muscle and Neuromuscular Junction Diseases of Muscle and Neuromuscular Junction Neuromuscular Junction Muscle Myastenia Gravis Eaton-Lambert Syndrome Toxic Infllammatory Denervation Atrophy
Diseases of Muscle and Neuromuscular Junction Diseases of Muscle and Neuromuscular Junction Neuromuscular Junction Muscle Myastenia Gravis Eaton-Lambert Syndrome Toxic Infllammatory Denervation Atrophy
Case Report Recurrent Vocal Fold Paralysis and Parsonage-Turner Syndrome
 Case Reports in Otolaryngology Volume 2013, Article ID 763201, 4 pages http://dx.doi.org/10.1155/2013/763201 Case Report Recurrent Vocal Fold Paralysis and Parsonage-Turner Syndrome Marcus Vinicius Pinto,
Case Reports in Otolaryngology Volume 2013, Article ID 763201, 4 pages http://dx.doi.org/10.1155/2013/763201 Case Report Recurrent Vocal Fold Paralysis and Parsonage-Turner Syndrome Marcus Vinicius Pinto,
InterQual Level of Care 2018 Index
 InterQual Level of Care 2018 Index Rehabilitation Criteria Index Words by Subset The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where
InterQual Level of Care 2018 Index Rehabilitation Criteria Index Words by Subset The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where
Lumbosacral plexus lesion Lumbosacral plexus disorders G54.1 Neuralgic amyotrophy Neuralgic amyotrophy G
 ICD-9-CM and ICD-10-CM NEUROMUSCULAR DIAGNOSIS CODES Focal Neuropathy ICD-9-CM ICD-10-CM Mononeuropathy G56.00 Carpal tunnel syndrome 354.00 Other median nerve lesion 354.10 Lesion of ulnar nerve 354.20
ICD-9-CM and ICD-10-CM NEUROMUSCULAR DIAGNOSIS CODES Focal Neuropathy ICD-9-CM ICD-10-CM Mononeuropathy G56.00 Carpal tunnel syndrome 354.00 Other median nerve lesion 354.10 Lesion of ulnar nerve 354.20
Laryngeal Electromyography and Prognosis of Unilateral Vocal Fold Paralysis A Long-term Prospective Study
 The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Laryngeal Electromyography and Prognosis of Unilateral Vocal Fold Paralysis A Long-term Prospective Study
The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Laryngeal Electromyography and Prognosis of Unilateral Vocal Fold Paralysis A Long-term Prospective Study
Larynx. Rudimentary. Behind the posterior surface : -stylopharyngeus - salpingopharyngeus -platopharyngeus
 Larynx The larynx is an organ that provides a protective sphincter at the inlet of the air passages and is responsible for voice production. It extends from C3-C6: *Posterior: the pharynx *Lateral: the
Larynx The larynx is an organ that provides a protective sphincter at the inlet of the air passages and is responsible for voice production. It extends from C3-C6: *Posterior: the pharynx *Lateral: the
Specialist Referral Service Willows Information Sheets. Laryngeal paralysis
 Specialist Referral Service Willows Information Sheets Laryngeal paralysis Laryngeal paralysis tends to affect middle aged and older animals, especially large breed dogs such as Labrador Retrievers, Golden
Specialist Referral Service Willows Information Sheets Laryngeal paralysis Laryngeal paralysis tends to affect middle aged and older animals, especially large breed dogs such as Labrador Retrievers, Golden
Tympanic Bulla Temporal Bone. Digastric Muscle. Masseter Muscle
 Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Myasthenia Gravis. Mike Gilchrist 10/30/06
 Myasthenia Gravis Mike Gilchrist 10/30/06 Overview Background Pathogenesis Clinical Manifestations Diagnosis Treatment Associated Conditions Background Severe muscle disease Most common disorder of neuromuscular
Myasthenia Gravis Mike Gilchrist 10/30/06 Overview Background Pathogenesis Clinical Manifestations Diagnosis Treatment Associated Conditions Background Severe muscle disease Most common disorder of neuromuscular
BOTULINUM TOXIN: RESEARCH ISSUES ARISING FROM PRACTICE
 % of baseline CMAP Botulinum toxin: mechanism of action BOTULINUM TOXIN: RESEARCH ISSUES ARISING FROM PRACTICE Clinical benefits of botulinum toxin (BT) injections depend primarily on the toxin's peripheral
% of baseline CMAP Botulinum toxin: mechanism of action BOTULINUM TOXIN: RESEARCH ISSUES ARISING FROM PRACTICE Clinical benefits of botulinum toxin (BT) injections depend primarily on the toxin's peripheral
CASE STUDIES CONTENTS PART REINKE' S EDEMA, 3 VOCAL CORD DYSFUNCTION, 7. fiabit COUGH, 15 MUSCLE TENSION DYSPHONIA, 18 PUBERPHONIA, 33
 CONTENTS PART I CASE STUDIES REINKE' S EDEMA, 3 CASE STUDY 1-1: Postoperative Reinke's Edema, 4 VOCAL CORD DYSFUNCTION, 7 CASE STUDY 2-1: Vocal Cord Dysfunction, 8 CASE STUDY 2-2: Vocal Cord Dysfunction,
CONTENTS PART I CASE STUDIES REINKE' S EDEMA, 3 CASE STUDY 1-1: Postoperative Reinke's Edema, 4 VOCAL CORD DYSFUNCTION, 7 CASE STUDY 2-1: Vocal Cord Dysfunction, 8 CASE STUDY 2-2: Vocal Cord Dysfunction,
External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other
 Internal trauma (Endotracheal intubation, tracheostomy) Other") Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
The Larynx. Prof. Dr.Mohammed Hisham Al-Muhtaseb
 The Larynx Prof. Dr.Mohammed Hisham Al-Muhtaseb The Larynx Extends from the middle of C3 vertebra till the level of the lower border of C6 Continue as Trachea Above it opens into the laryngo-pharynx Suspended
The Larynx Prof. Dr.Mohammed Hisham Al-Muhtaseb The Larynx Extends from the middle of C3 vertebra till the level of the lower border of C6 Continue as Trachea Above it opens into the laryngo-pharynx Suspended