AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
|
|
|
- Kevin Hall
- 5 years ago
- Views:
Transcription
1 AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
2 AJCC 7 th edition Lip and Oral cavity Pharynx Larynx
3 KEY CHANGES
4 Skin of head and neck (Vermilion of the lip) Lip and oral cavity Oral cavity (Mucosal of the lip)
5 Oral cavity Depth of Invasion (DOI) add into T category Delete invasion of extrinsic muscle of tongue in T category Instead, bilateral tongue involvement is added
6 Nasopharynx Pharynx HPV-Mediated (p16 +) Oropharyngeal Cancer Oropharynx (p16 -) Hypopharynx
7 Nasopharynx HPV-Mediated (p16 +) Oropharyngeal Cancer T0 category Separate staging algorithm for HPVassociated cancer Oropharynx (p16 -) Hypopharynx No T0 category New chapter for cervical lymph node and unknown primary tumors
8 N stage Separate clinical and pathological N stage Extranodal extension (ENE) add into N category Separated N stage in HPV-associated oropharyngeal carcinoma
9 LIP AND ORAL CAVITY ALL EPITHELIAL & MINOR SALIVARY GLAND CANCER

10 Vermilion of lip belongs to skin cancer (Ch.15)
11 Tumor size: actual measurement of the unfixed tumor
12
13

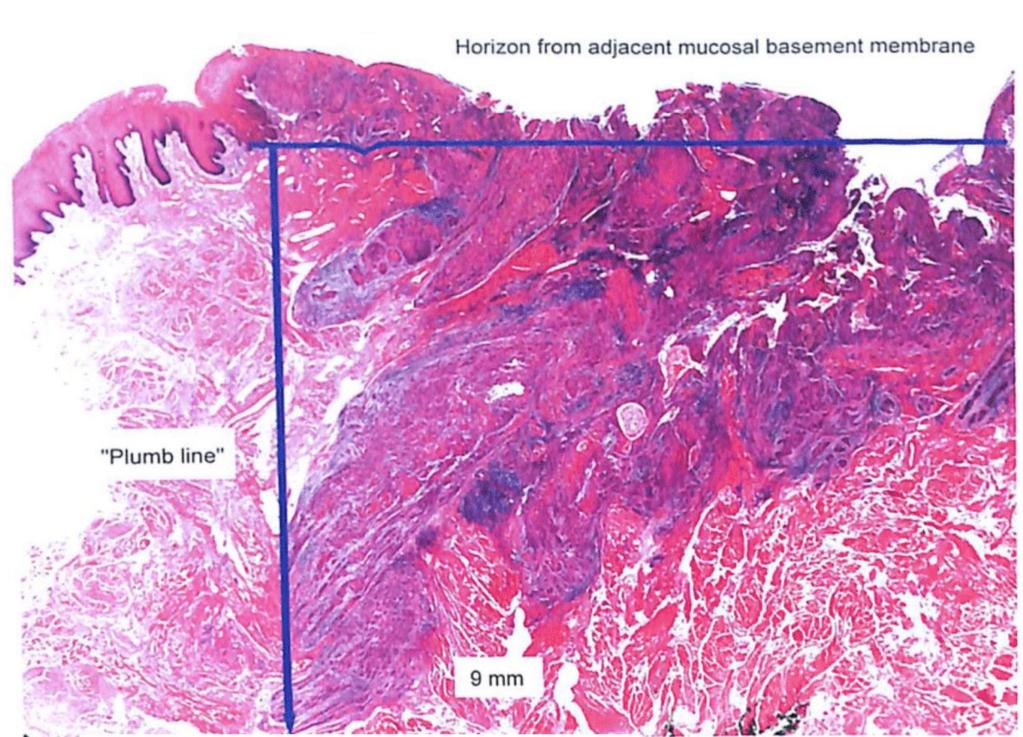
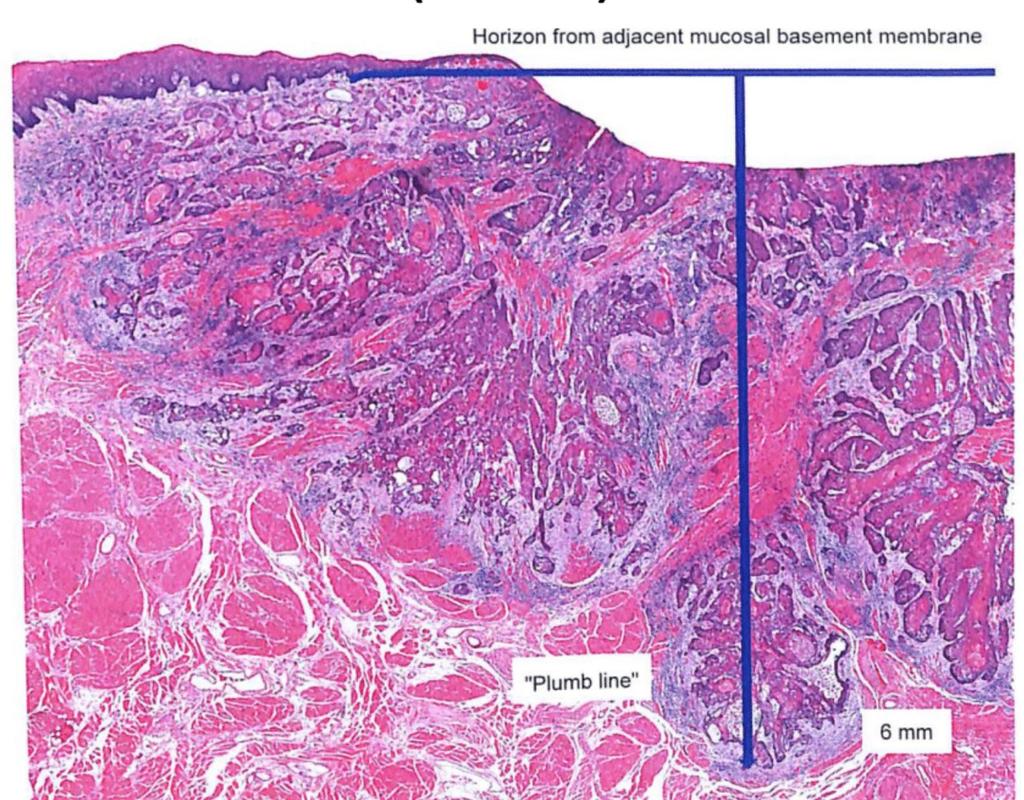
14 Tumor thickness Depth of invasion Tumor thickness DOI
15 How about exophytic tumor? No conclusion!
16 How to determine the horizontal line? No conclusion!
17 Key concept of DOI How much depth comparing to normal mucosa!
18 DOI Tumor size 2 cm >2-4 cm >4 cm 5 mm T1 T2 T3 >5-10mm T2 T2 T3 >10 mm T3 T3 T3 >20mm T4a T4a T4a


19 Note: Superficial erosion of bone / tooth socket is insufficient to classify as T4
20 Lip: Through cortical bone, inferior alveolar n. floor of mouth, skin of the face T4a Oral cavity: Adjacent structure(s) only (Through cortical bone, maxillary sinus, skin of the face, extrinsic muscle of tongue Bilateral tongue involvement) T4b Masticator space, pterygoid plates, skull base / encases the internal carotid artery

21 Additional regional LN group: Suboccipital Retropharyngeal Parapharyngeal Buccinator (fascial) Preauricular Select neck dissection >10 LN Radical neck dissection >15 LN Periparotid and intraparotid
22

23 ENE (-) ENEn None ENE (+) ENEmi ENEma Microscopic ENE 2mm ENE > 2mm or gross ENE

24 Size of invasive carcinoma in lymph node
25 Without ENE LN number LN size 3 cm >3-6 cm >6 cm 1 N1 N2a N3a >1 N2b N2b Contralateral / Bilateral N2c N2c N3a
26 With ENE LN number LN size 3 cm >3-6 cm >6 cm 1 N2a N3b N3b >1 N3b N3b N3b Contralateral / Bilateral N3b N3b N3b
27 N T Is a 4b M1 0 0 I II III IVA IVB IVC 1 III III III IVA IVB IVC 2 IVA IVA IVA IVA IVB IVC 3 IVB IVB IVB IVB IVB IVC M1 IVC IVC IVC IVC IVC IVC
28
29
30
31
32 Additional Prognostic Factors Recommended for Clinical Care Extranodal extension Depth of invasion Resection margins Worst pattern of invasion Perineural invasion Lymphovascular invasion Overall health Comorbidity Lifestyle factor Tobacco Use
33 Additional Prognostic Factors Recommended for Clinical Care Extranodal extension Depth of invasion Resection margins Worst pattern of invasion Perineural invasion Lymphovascular invasion Overall health Comorbidity Lifestyle factor Tobacco Use

34 Worst Pattern of Invasion (WPOI)-5 Tumor dispersion of 1 mm between tumor satellites. 1 mm
35 Definition of WPOI-5 Tumor dispersion of 1mm between tumor satellite. Tumor dispersion through soft tissue. Disperse extratumoral perineural invasion. Extratumoral lymphovascular invasion.


36 WPOI-5 Strandy pattern with intervening skeletal muscle WPOI-5 Often associated with PNI
37 Significance of WPOI-5 Stage I/II OSCC, primary tumor > 4mm DOI. Significantly predictive of locoregional recurrence and disease specific survival. The probability in developing locoregional recurrence is 42%

38 Wrapping around nerves Perineural invasion Bumping into a nerve Insufficient for perineural invasion
39 Lymphovascular invasion Should be reported as Either intratumoral or extratumoral Focal or multifocal
40 OROPHARYNX (P16 -) & HYPOPHARYNX ALL EPITHELIAL (P16 -) & MINOR SALIVARY GLAND CANCER
41 No change in anatomical site
42 Oropharyngeal Squamous cell carcinoma P16 IHC stain (75%) + - / Not performed Squamous cell carcioma, HPV-positive Grading is not advocated Squamous cell carcioma, HPV-negative Similar grading to other sites

43 Oropharynx (p16 -) Tumor size: actual measurement of the unfixed tumor T1 T2 T3 2 cm > 2-4 cm > 4 cm

44 T4a Larynx, extrinsic muscle of tongue, medial pterygoid, hard palate, mandible T4b Lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, skull base / encases carotid artery
45 Hypopharynx Pyriform sinuses Post-cricoid region Lateral and posterior hypopharyngeal wall

46 Hypopharynx T1 Tumor 2 cm, limited to 1 subsite
47 Hypopharynx Subsite: Pyriform sinuses Lateral and posterior hypopharyngeal wall Postcricoid region T2 Tumor > 2-4 cm, invade >1 subsites


48 Hypopharynx T3 Tumor > 4cm / fixation of hemilarynx / extension to esophagus mucosa
49 Subsite Tumor size 2 cm >2-4 cm >4 cm 1 T1 T2 T3 >1 T2 T2 T3 Fixation of hemilarynx / Invasion of esophagus mucosa T3 T3 T3

50 Hypopharynx T4a Thyroid/cricoid cartilage, hyoid bone, thyroid gland, central compartment soft tissue, esophageal muscular wall T4b Prevertebral fascia Encases carotid artery Involves mediastinal structures
51 Without ENE LN number LN size 3 cm >3-6 cm >6 cm 1 N1 N2a N3a >1 N2b N2b Contralateral / Bilateral N2c N2c N3a
52 With ENE LN number LN size 3 cm >3-6 cm >6 cm 1 N2a N3b N3b >1 N3b N3b N3b Contralateral / Bilateral N3b N3b N3b
53 N T Is a 4b M1 0 0 I II III IVA IVB IVC 1 III III III IVA IVB IVC 2 IVA IVA IVA IVA IVB IVC 3 IVB IVB IVB IVB IVB IVC M1 IVC IVC IVC IVC IVC IVC
54 Additional Prognostic Factors Recommended for Clinical Care Extranodal Extension Overall health Comorbidity Lifestyle factor Tobacco Use
55 LARYNX CARCINOMA OF THE SUPPRAGLOTTIC, GLOTTIC & SUBGLOTTIC LARYNX
56 Supraglottic Glottic Subglottic Suprahyoid epiglottis Infrahyoid epiglottis AE fold / arytenoids Ventricular band True vocal cord Subglottic
57 Supraglottis T1 Tumor limited to 1 subsite T2 Tumor invades > 1 subsites / glottis / region outside the supraglottis
58 Supraglottis T1 Tumor limited to 1 subsite T2 Tumor invades > 1 subsites / glottis / region outside the supraglottis
59 Supraglottis Tumor limited to larynx with vocal cord fixation / invades postcricoid area, preepiglottic space, paraglottic space, inner cortex of thyroid cortex T3
60 Glottis T1a Limited to 1 vocal cord T1b Invalves both vocal cords
61 Glottis T2 Extends to supraglottis / subglottis Impaired vocal cord mobility
62 Glottis T3 Vocal cord fixation Invasion of paraglottic space/ inner cortex of thyroid cartilage
63 Subglottis T1 Tumor limited to the subglottis
64 Subglottis T2 Tumor extends to vocal cord(s)
65 Subglottis T3 Vocal cord fixation Invasion of paraglottic space/ inner cortex of thyroid cartilage

66 Supraglottis / Glottis / Subglottis T4a Tumor invades through the outer cortex of the thyroid cartilage / invades tissue beyond the larynx
67 Beyond the larynx Supraglottis Glottis Subglottis Trachea Soft tissue of neck Deep extrinsic muscle of the tongue Strap muscle Thyroid Esophagus Trachea Cricoid cartilage Soft tissue of neck Deep extrinsic muscle of the tongue Strap muscles Thyroid Esophagus Trachea Soft tissue of neck Deep extrinsic muscle of the tongue Strap muscles Thyroid Esophagus
68 Supraglottis / Glottis / Subglottis T4b Invades prevertebral space Encases carotid artery Invades mediastinal structure
69 Without ENE LN number LN size 3 cm >3-6 cm >6 cm 1 N1 N2a N3a >1 N2b N2b Contralateral / Bilateral N2c N2c N3a
70 With ENE LN number LN size 3 cm >3-6 cm >6 cm 1 N2a N3b N3b >1 N3b N3b N3b Contralateral / Bilateral N3b N3b N3b
71 N T Is a 4b M1 0 0 I II III IVA IVB IVC 1 III III III IVA IVB IVC 2 IVA IVA IVA IVA IVB IVC 3 IVB IVB IVB IVB IVB IVC M1 IVC IVC IVC IVC IVC IVC
72 Additional Prognostic Factors Recommended for Clinical Care Extranodal Extension Comorbidity Lifestyle factor Tobacco Use

73 Thank you for your attention!
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic space
 Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
AJCC update Disclosures. AJCC TNM staging system. Objectives:
 Disclosures AJCC update 2018 Remy Lobo, MD remylobo@med.umich.edu remy.lobo@hsc.utah.edu No relevant disclosures Information is based on the 8 th AJCC manual Amin MB, Edge SB, Greene FL et al, eds. AJCC
Disclosures AJCC update 2018 Remy Lobo, MD remylobo@med.umich.edu remy.lobo@hsc.utah.edu No relevant disclosures Information is based on the 8 th AJCC manual Amin MB, Edge SB, Greene FL et al, eds. AJCC
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient
 Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
Evaluation and Treatment of Dysphagia in the Head and Neck Cancer Patient Linda Stachowiak MS/CCCSLP BCS-S Speech Pathology Oncology Specialist UFHealth Cancer Center at Orlando Health Orlando Florida
L ARYNX S TAGING F ORM
 CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
Q&A. Fabulous Prizes. Collecting Cancer Data: Pharynx 12/6/12. NAACCR Webinar Series Collecting Cancer Data Pharynx
 Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Head and Neck Tumours
 Head and Neck Tumours Introductory Notes The following sites are included: Lip, oral cavity Pharynx: oropharynx, nasopharynx, hypopharynx Larynx: supraglottis, glottis, subglottis Nasal cavity and paranasal
Head and Neck Tumours Introductory Notes The following sites are included: Lip, oral cavity Pharynx: oropharynx, nasopharynx, hypopharynx Larynx: supraglottis, glottis, subglottis Nasal cavity and paranasal
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Physician to Physician AJCC 8 th Edition. Head and Neck. Summary of Changes. AJCC Cancer Staging Manual, 7 th Ed. Head and Neck Chapters
 Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
6 th Reprint Handbook Pages AJCC 7 th Edition
 6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
Esophagus Stomach 4/2/15
 Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
(loco-regional disease)
") (loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
(loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
Upper Aerodigestive Tract (Including Salivary Glands)
") Upper Aerodigestive Tract (Including Salivary Glands) Protocol applies to all invasive carcinomas of the upper aerodigestive tract including the oral cavity (including lip and tongue), pharynx (oropharynx,
Upper Aerodigestive Tract (Including Salivary Glands) Protocol applies to all invasive carcinomas of the upper aerodigestive tract including the oral cavity (including lip and tongue), pharynx (oropharynx,
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
A220: Larynx cancer tissues. (formalin fixed)
") A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
2. Guidelines for Reporting Head and Neck Tumours
 39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
10. HPV-Mediated (p16+) Oropharyngeal Cancer
 Oropharyngeal Cancer") 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Head & Neck Contouring
 Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Larynx (Nonepithelial tumors such as those of lymphoid tissue, soft tissue, bone, and cartilage are not included)
") 5 Larynx (Nonepithelial tumors such as those of lymphoid tissue, soft tissue, bone, and cartilage are not included) At-A-Glance S U M M A R Y O F C H A N G E S T4 lesions have been divided into (moderately
5 Larynx (Nonepithelial tumors such as those of lymphoid tissue, soft tissue, bone, and cartilage are not included) At-A-Glance S U M M A R Y O F C H A N G E S T4 lesions have been divided into (moderately
AJCC Cancer Staging Form Supplement
 AJCC Cancer Staging Form Supplement AJCC Cancer Staging Manual, Eighth Edition Last updated 05 June 2018 AMERICAN JOINT COMMITTEE ON CANCER Executive Office 633 North Saint Clair Street Chicago, IL 60611
AJCC Cancer Staging Form Supplement AJCC Cancer Staging Manual, Eighth Edition Last updated 05 June 2018 AMERICAN JOINT COMMITTEE ON CANCER Executive Office 633 North Saint Clair Street Chicago, IL 60611
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
Head & Neck Cancer Clinical Guidelines
 Head & Neck Cancer Clinical Guidelines Head & Neck NSSG on behalf of NECN Document Information Title: NECN Head and Neck Cancer Clinical Guidelines Author: Head and Neck NSSG Members Circulation List:
Head & Neck Cancer Clinical Guidelines Head & Neck NSSG on behalf of NECN Document Information Title: NECN Head and Neck Cancer Clinical Guidelines Author: Head and Neck NSSG Members Circulation List:
1/14/2019 CRITICAL PATHWAYS IN HEAD AND NECK CANCER DISCLOSURES OBJECTIVES
 CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
CRITICAL PATHWAYS IN HEAD AND NECK CANCER Caroline Nickel, MS CCC-SLP Baylor University Medical Center Dallas, Texas DISCLOSURES Caroline Nickel is employed by Baylor Institute for Rehabilitation. Caroline
Nasal Cavity CS Tumor Size (Revised: 02/03/2010)
") Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
SITES (ALPHABETICAL) HPV CS SITE SPECIFIC FACTOR
 HPV CS SITE SPECIFIC FACTOR") SITES (ALPHABETICAL) HPV CS SITE SPECIFIC FACTOR Anus: Anal Canal; Anus, NOS; Other Parts of Rectum C21.0-C21.2, C21.8 C21.0 Anus, NOS (excludes skin of anus and perianal skin C44.5) C21.1 Anal canal C21.2
SITES (ALPHABETICAL) HPV CS SITE SPECIFIC FACTOR Anus: Anal Canal; Anus, NOS; Other Parts of Rectum C21.0-C21.2, C21.8 C21.0 Anus, NOS (excludes skin of anus and perianal skin C44.5) C21.1 Anal canal C21.2
Protocol for the Examination of Specimens from Patients with Carcinomas of the Larynx
 Protocol for the Examination of Specimens from Patients with Carcinomas of the Larynx Protocol applies to all invasive carcinomas of the larynx, including supraglottis, glottis, and subglottis. Mucosal
Protocol for the Examination of Specimens from Patients with Carcinomas of the Larynx Protocol applies to all invasive carcinomas of the larynx, including supraglottis, glottis, and subglottis. Mucosal
Head & Neck Staging. Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging
 AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging. Head & Neck Staging. Learning Objectives. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
Structure and Nerve Supply of The Larynx
 Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical sciences Structure and Nerve Supply of The Larynx This presentation was originally prepared by: Dr. Kumar Notes were added by:
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical sciences Structure and Nerve Supply of The Larynx This presentation was originally prepared by: Dr. Kumar Notes were added by:
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
NAACCR Webinar Series 1
 Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
CANCERS of OROPHARYNX and HYPOPHARYNX. STAGING and TREATMENT
 1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide
 The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Organ preservation in laryngeal cancer
 Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
14. Mucosal Melanoma of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Protocol for the Examination of Specimens From Patients With Carcinomas of the Pharynx
 Protocol for the Examination of Specimens From Patients With Carcinomas of the Pharynx Protocol applies to all invasive carcinomas of the pharynx (oropharynx, nasopharynx, hypopharynx) including the base
Protocol for the Examination of Specimens From Patients With Carcinomas of the Pharynx Protocol applies to all invasive carcinomas of the pharynx (oropharynx, nasopharynx, hypopharynx) including the base
The Pharynx. Dr. Nabil Khouri MD. MSc, Ph.D
 The Pharynx Dr. Nabil Khouri MD. MSc, Ph.D Introduction The pharynx is the Musculo-fascial halfcylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck Common
The Pharynx Dr. Nabil Khouri MD. MSc, Ph.D Introduction The pharynx is the Musculo-fascial halfcylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck Common
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
Head & Neck Cancer. Two Routes to Cover. Head and Neck Risk Factors cont. Head and Neck Risk Factors. Changes in 2018
 Two Routes to Cover Head & Neck Cancer Changes in 2018 1 2 Head and Neck Risk Factors Tobacco (smoking, chewing, dipping snuff) Alcohol Chewing betel nut products (Asia & So Pacific) Men > women Blacks
Two Routes to Cover Head & Neck Cancer Changes in 2018 1 2 Head and Neck Risk Factors Tobacco (smoking, chewing, dipping snuff) Alcohol Chewing betel nut products (Asia & So Pacific) Men > women Blacks
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Data Definitions for the National Minimum Core Dataset to Support the Introduction of
 Head and Neck Cancer Data Definitions for the National Minimum Core Dataset to Support the Introduction of Head and Neck Cancer Quality Performance Indicators Definitions developed by ISD Scotland in Collaboration
Head and Neck Cancer Data Definitions for the National Minimum Core Dataset to Support the Introduction of Head and Neck Cancer Quality Performance Indicators Definitions developed by ISD Scotland in Collaboration
CERVICAL LYMPH NODES
 CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
Guidelines for the Management of Head and Neck Cancer
 Guidelines for the Management of Head and Neck Cancer Version: 2 Ref: AngCN-SSG-NH5 Contents 1. Introduction... 3 2. General Principles... 3 3. Site Specific Guidelines... 4 3.1 Oral Cavity... 4 3.2 Oropharynx...
Guidelines for the Management of Head and Neck Cancer Version: 2 Ref: AngCN-SSG-NH5 Contents 1. Introduction... 3 2. General Principles... 3 3. Site Specific Guidelines... 4 3.1 Oral Cavity... 4 3.2 Oropharynx...
Management of Salivary Gland Malignancies. No Disclosures or Conflicts of Interest. Anatomy 10/4/2013
 Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Volumi di trattamento del cavo orale
 SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
Prevertebral Region, Pharynx and Soft Palate
 Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
NAACCR Webinar Series 1. Instructors Q&A 10/6/2011. Collecting Cancer Data: Larynx Including Mucosal Melanoma of Larynx.
 NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Larynx Instructors Shannon Vann, CTR Jim Hofferkamp, CTR 2 Q&A Please submit all questions concerning webinar content through the Q&A panel. 3 NAACCR
NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Larynx Instructors Shannon Vann, CTR Jim Hofferkamp, CTR 2 Q&A Please submit all questions concerning webinar content through the Q&A panel. 3 NAACCR
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey
 Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections Salivary glands* will not be covered specifically
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections Salivary glands* will not be covered specifically
Protocol for the Examination of Specimens From Patients With Cancers of the Larynx
 Protocol for the Examination of Specimens From Patients With Cancers of the Larynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Cancers of the Larynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Hiroyuki Hanakawa, Nobuya Monden, Kaori Hashimoto, Aiko Oka, Isao Nozaki, Norihiro Teramoto, Susumu Kawamura
 Accepted Manuscript Radiation-induced laryngeal angiosarcoma: Case report Hiroyuki Hanakawa, Nobuya Monden, Kaori Hashimoto, Aiko Oka, Isao Nozaki, Norihiro Teramoto, Susumu Kawamura PII: S2468-5488(18)30005-5
Accepted Manuscript Radiation-induced laryngeal angiosarcoma: Case report Hiroyuki Hanakawa, Nobuya Monden, Kaori Hashimoto, Aiko Oka, Isao Nozaki, Norihiro Teramoto, Susumu Kawamura PII: S2468-5488(18)30005-5
The Respiratory System
 The Respiratory System Cells continually use O2 & release CO2 Respiratory system designed for gas exchange Cardiovascular system transports gases in blood Failure of either system rapid cell death from
The Respiratory System Cells continually use O2 & release CO2 Respiratory system designed for gas exchange Cardiovascular system transports gases in blood Failure of either system rapid cell death from
Hypopharynx and larynx anatomy
 Hypopharynx and larynx anatomy Poster No.: C-0786 Congress: ECR 2016 Type: Educational Exhibit Authors: A. I. Fernández Martín, N. Delgado Ronda, E. Dominguez 1 3 2 4 5 Franjo, M. Martínez Martínez-Losa,
Hypopharynx and larynx anatomy Poster No.: C-0786 Congress: ECR 2016 Type: Educational Exhibit Authors: A. I. Fernández Martín, N. Delgado Ronda, E. Dominguez 1 3 2 4 5 Franjo, M. Martínez Martínez-Losa,
Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx
 Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Cancers of the Pharynx Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Hypopharyngeal Carcinoma: A Review
 http://www.banglajol.info/index.php/jcamr Journal of Current and Advance Medical Research pissn 2313-447X Review Article Hypopharyngeal Carcinoma: A Review Md. Nazmul ISLAM 1, Mohammad Mamun SIDDIQUI 2,
http://www.banglajol.info/index.php/jcamr Journal of Current and Advance Medical Research pissn 2313-447X Review Article Hypopharyngeal Carcinoma: A Review Md. Nazmul ISLAM 1, Mohammad Mamun SIDDIQUI 2,
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
"The Space Between Us:" A Radiographic Review of Common and Uncommon Pathologic Findings within the Deep Spaces of the Neck
 "The Space Between Us:" A Radiographic Review of Common and Uncommon Pathologic Findings within the Deep Spaces of the Neck Poster No.: C-2457 Congress: ECR 2015 Type: Educational Exhibit Authors: A. K.
"The Space Between Us:" A Radiographic Review of Common and Uncommon Pathologic Findings within the Deep Spaces of the Neck Poster No.: C-2457 Congress: ECR 2015 Type: Educational Exhibit Authors: A. K.
Since the first description of the radical neck dissection by George Crile almost a century
 ORIGINAL ARTICLE Neck Dissection Classification Update Revisions Proposed by the American Head and Neck Society and the American Academy of Otolaryngology Head and Neck Surgery K. Thomas Robbins, MD; Garry
ORIGINAL ARTICLE Neck Dissection Classification Update Revisions Proposed by the American Head and Neck Society and the American Academy of Otolaryngology Head and Neck Surgery K. Thomas Robbins, MD; Garry
Alexander C Vlantis. Total Laryngectomy 57
 07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
Head and Neck Image 頭頸部放射影像學
 Head and Neck Image 頭頸部放射影像學 陳家媛 台北醫學大學 - 市立萬芳醫院 cychen@wanfang.gov.tw Normal Suprahyoid neck: the old way Nasopharynx Oropharynx Oral cavity Staging of SCC Spaces of Suprahyoid Neck: a New Way Deep
Head and Neck Image 頭頸部放射影像學 陳家媛 台北醫學大學 - 市立萬芳醫院 cychen@wanfang.gov.tw Normal Suprahyoid neck: the old way Nasopharynx Oropharynx Oral cavity Staging of SCC Spaces of Suprahyoid Neck: a New Way Deep
The PHARYNX. Dr. Nabil Khouri MD Ph.D
 The PHARYNX Dr. Nabil Khouri MD Ph.D PHARYNX Fibromuscular tube lined with mucous membrane extends from base of skull to lower border of cricoid cartilage (C-6). 12-14 cm long At the lower border of cricoid
The PHARYNX Dr. Nabil Khouri MD Ph.D PHARYNX Fibromuscular tube lined with mucous membrane extends from base of skull to lower border of cricoid cartilage (C-6). 12-14 cm long At the lower border of cricoid
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Anne Marie Brown Macmillan Head & Neck CNS
 Advances in the Treatment of Head & Neck cancer Anne Marie Brown Macmillan Head & Neck CNS Aims To provide a brief revision of Head & Neck anatomy and background statistics To demonstrate the processes
Advances in the Treatment of Head & Neck cancer Anne Marie Brown Macmillan Head & Neck CNS Aims To provide a brief revision of Head & Neck anatomy and background statistics To demonstrate the processes
Head and neck cancer technically refers to any malignancy
 Head and Neck Cancer Michael J. Walden, DO, MD, and Nafi Aygun, MD Cross sectional imaging fills a crucial role in the work up of squamous cell cancer of the head and neck. The radiologist can suggest
Head and Neck Cancer Michael J. Walden, DO, MD, and Nafi Aygun, MD Cross sectional imaging fills a crucial role in the work up of squamous cell cancer of the head and neck. The radiologist can suggest
Read Me. We are the Learning Lab. to look
 Respiratory Tract Anatomy Lab In-Lab Exercises Read Me We are going to look at models and slides. Much of this can be done in the Learning Lab on your own time. The steps do not have to be done in order,
Respiratory Tract Anatomy Lab In-Lab Exercises Read Me We are going to look at models and slides. Much of this can be done in the Learning Lab on your own time. The steps do not have to be done in order,
NAACCR Webinar Series
 NAACCR 2009-2010 Webinar Series Collecting Cancer Data: Lip & Oral Cavity 8/5/2010 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes! NAACCR 2009/2010
NAACCR 2009-2010 Webinar Series Collecting Cancer Data: Lip & Oral Cavity 8/5/2010 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes! NAACCR 2009/2010
Head & Neck Case # 1
 DISCHARGE SUMMARY Head & Neck Case # 1 Date of Admission: 10/30/2010 Date of Discharge: 11/02/2010 Present Medical History: The patient is a 33-year-old lady with a history of right superior alveolar ridge
DISCHARGE SUMMARY Head & Neck Case # 1 Date of Admission: 10/30/2010 Date of Discharge: 11/02/2010 Present Medical History: The patient is a 33-year-old lady with a history of right superior alveolar ridge
(formalin fixed) 6 non-neoplastic spots (6 spots) Corresponding normal tissues with cancers: Yes Diameter: 1. 0 mm
 6 non-neoplastic spots (6 spots) Corresponding normal tissues with cancers: Yes Diameter: 1. 0 mm") CBA729-Test slide, Head and neck cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 6 Tissue type: Test slide, Head and neck cancer tissues No. of spots: 6 spots from each
CBA729-Test slide, Head and neck cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 6 Tissue type: Test slide, Head and neck cancer tissues No. of spots: 6 spots from each
Veins of the Face and the Neck
 Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Transoral Laser Microsurgery in Carcinomas of the Oral Cavity, Pharynx, and Larynx
 The indications and approach using CO 2 laser surgery in carcinomas of the upper aerodigestive tract are reviewed. Lu Jian Jun. The Dulcimer, 2000. Oil on canvas, 36 48. Courtesy of Weinstein Gallery,
The indications and approach using CO 2 laser surgery in carcinomas of the upper aerodigestive tract are reviewed. Lu Jian Jun. The Dulcimer, 2000. Oil on canvas, 36 48. Courtesy of Weinstein Gallery,
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
Imaging: When to get MRI, CT or PET-CT?
 Imaging: When to get MRI, CT or PET-CT? Alina Uzelac, D.O. Assistant Clinical Professor Neuroradiology UCSF Department of Radiology and Biomedical Imaging San Francisco General Hospital Overview CT MRI
Imaging: When to get MRI, CT or PET-CT? Alina Uzelac, D.O. Assistant Clinical Professor Neuroradiology UCSF Department of Radiology and Biomedical Imaging San Francisco General Hospital Overview CT MRI
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
APRIL
 APRIL - 2003 OCTOBER - 2003 February 2009 [KU 652] Sub. Code : 4131 FIRST B.D.S DEGREE EXAMINATION (Modified Regulations III) Paper I HUMAN ANATOMY, HISTOLOGY AND EMBRYOLOGY Time : Three hours
APRIL - 2003 OCTOBER - 2003 February 2009 [KU 652] Sub. Code : 4131 FIRST B.D.S DEGREE EXAMINATION (Modified Regulations III) Paper I HUMAN ANATOMY, HISTOLOGY AND EMBRYOLOGY Time : Three hours
Head and Neck Pathology. Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital)
") Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience. Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore
 Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Neuroradiology/Head and Neck Imaging Review
 Neuroradiology/Head and Neck Imaging Review Plaxton et al. Use of PET/CT for Imaging Cancer of the Head and Neck Neuroradiology/Head and Neck Imaging Review Nicholas. Plaxton 1 David C. randon 2 manda
Neuroradiology/Head and Neck Imaging Review Plaxton et al. Use of PET/CT for Imaging Cancer of the Head and Neck Neuroradiology/Head and Neck Imaging Review Nicholas. Plaxton 1 David C. randon 2 manda
Tympanic Bulla Temporal Bone. Digastric Muscle. Masseter Muscle
 Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Oropharyngeal cancer
 Cancer Imaging (2005) 5, S52 S57 DOI: 10.1102/1470-7330.2005.0030 CI MULTIDISCIPLINARY SYMPOSIUM: HEAD & NECK CANCER Monday 3 October 2005, 14:00 16:00 Oropharyngeal cancer Robert Hermans Department of
Cancer Imaging (2005) 5, S52 S57 DOI: 10.1102/1470-7330.2005.0030 CI MULTIDISCIPLINARY SYMPOSIUM: HEAD & NECK CANCER Monday 3 October 2005, 14:00 16:00 Oropharyngeal cancer Robert Hermans Department of
Rashad Rafiq Mattoo et al. Journal of Biological & Scientific Opinion Volume 4 (5). 2016
. 2016") Research Article Available online through www.jbsoweb.com ISSN 2321-6328 CLINICO-ENDOSCOPIC AND RADIOLOGICAL ASSESSMENT IN THE PRETHERAPEUTIC STAGING OF LARYNGEAL AND HYPOPHARYNGEAL MALIGNANCIES Rashad
Research Article Available online through www.jbsoweb.com ISSN 2321-6328 CLINICO-ENDOSCOPIC AND RADIOLOGICAL ASSESSMENT IN THE PRETHERAPEUTIC STAGING OF LARYNGEAL AND HYPOPHARYNGEAL MALIGNANCIES Rashad
SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions. 4 May 2012
 SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions 4 May 2012 1. With regard to the muscles of the neck: a. the platysma muscle is supplied by the accessory nerve. b. the stylohyoid muscle is supplied by
SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions 4 May 2012 1. With regard to the muscles of the neck: a. the platysma muscle is supplied by the accessory nerve. b. the stylohyoid muscle is supplied by