Endocrine Topic Review. Sethanant Sethakarun, MD
|
|
|
- Jonah Henry
- 5 years ago
- Views:
Transcription

1 Endocrine Topic Review Sethanant Sethakarun, MD
2
3 Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
4 Signs and Symptoms More specific: Reddish purple striae (>1 cm.wide) Facial plethora Proximal muscle weakness Easy bruising In children-weight gain with decreasing growth velocity

5 Signs and Symptoms High sensitivity Feature

6 Signs and symptoms
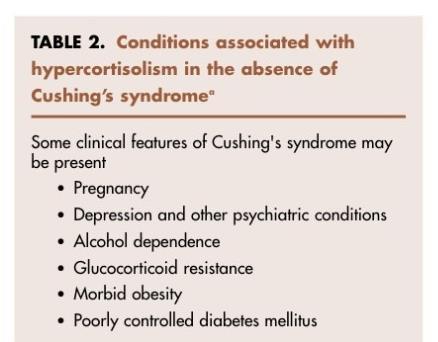
7 Pseudo-Cushing's Syndrome
8 Morbidity and Mortality Severe hypercortisolism: a median survival of 4.6 yr Most deaths caused by vascular (MI, CVA) or infectious complications. Treatment of patients with moderate to severe Cushing's syndrome clearly reduces mortality and morbidity.
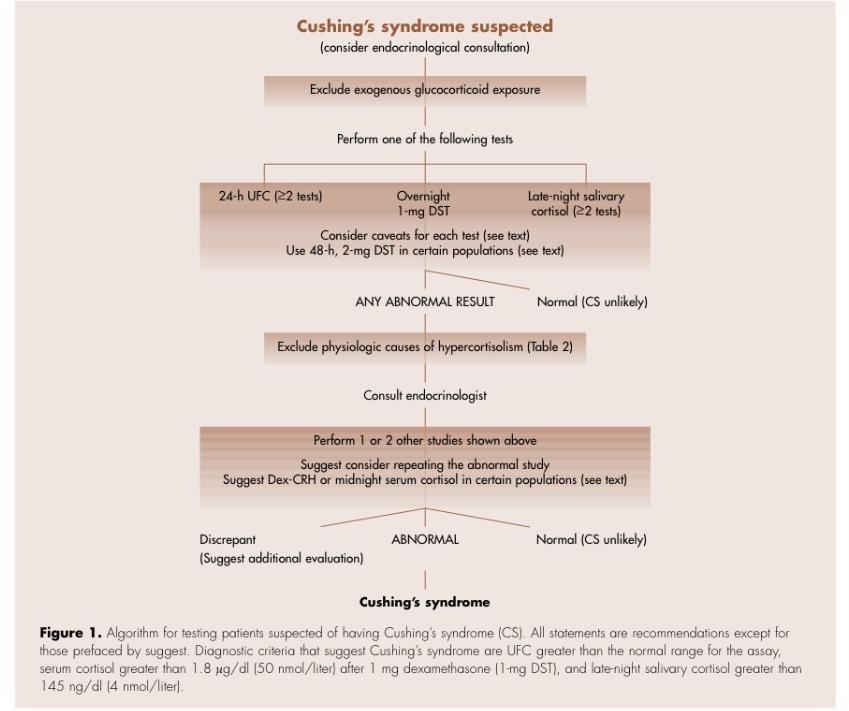
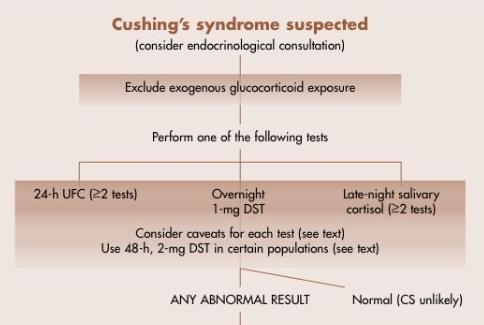
9 Diagnosis
10 Severity of Cushingoid features depends on the potency of the preparation used, its dose, the route and duration of its administration. Current or recent use of these medication. Eg.skin creams, herbal medications, joint or nerve injections, synthetic progesterone derivative, etc. Exclude exogenous glucocorticoid exposure
11
12 Cushing's syndrome tends to progress, accumulation of new features increases the probability that the syndrome is present. In children, the sensitivity of combined reduced linear growth and increased weight is quite high. Patients with incidentally found adrenal nodule usually not present with overt clinical features of Cushing's syndrome, but biochemical hypercortisolism is present in a large fraction. Adrenal incidentaloma, usually not present with overt CS
13 False-positive results are reduced if case detection is limited to individuals with an increased pretest probability of having the disorder.
14 Diagnosis
15 Diagnosis

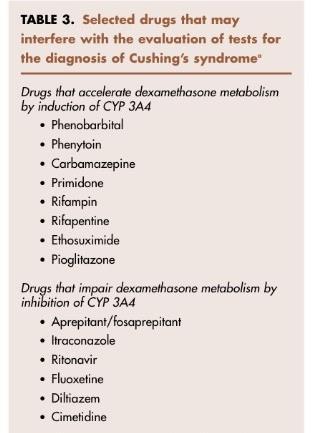
16 Initial testing

17 Initial testing ** **Not available in Thailand
18 Initial testing 4 recommended tests have acceptable diagnostic accuracy when the suggested cutoff points are used. If the initial testing results are normal, then the patient is very unlikely to have Cushing's syndrome. Initial testing!!
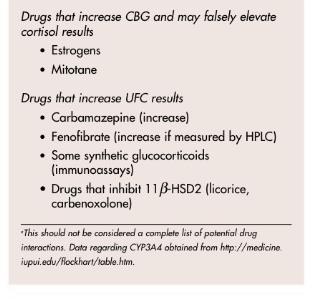
19 Estrogen increase the cortisol-binding globulin (CBG) in the circulation. Because serum assays measure total cortisol, false-positive rates for the overnight DST are seen in 50% of women taking the OCP. Estrogen-containing drugs should be withdrawn for 6 weeks before testing. Because the hypercortisolism of Cushing's syndrome can be variable, at least 2 measurements of urine or salivary cortisol are recommended.
20 Urine Free Cortisol (UFC) UFC reflects both urine metabolites and cortisol. Measures the cortisol that is not bound to CBG, which is filtered by the kidney unchanged. Values are significantly lower in patients with moderate to severe renal impairment. (GFR < 60 ml/min) UFC is not affected by conditions and medications that alter CBG!!
21 Urine Free Cortisol (UFC) Sample collection and instructions: Avoid the use of any glucocorticoid preparations. Because UFC levels in a patient with Cushing's syndrome are variable, at least two collections should be performed. Interpretation: UFC is 3 times higher than upper normal level -> positive
22 1-mg Overnight DST Supraphysiological dose of glucocorticoid results in suppression of ACTH and cortisol secretion. Endogenous Cushing's syndrome of any cause have a failure of this suppression.
23 1-mg Overnight DST Enzyme inducer drugs accelerate dexamethasone metabolism. Enzyme inhibitor drugs impair dexamethasone metabolism. OCP increase CBG and may falsely elevate cortisol.
24
25 1-mg Overnight DST Sample collection and instruction: 1 mg dexamethasone is given between , and cortisol is measured between the following morning. Interpretation: Suppresible when serum cortisol less than 1.8 microgram/dl.
26 Low-dose DST Sample collection and instruction: Dexamethasone is given in doses of 0.5 mg for 48 hrs, beginning at on day 1, at 6 hrs intervals. Serum cortisol is measured at 8.00 after the last dexamethasone dose. Interpretation: Suppresible when serum cortisol is less than 1.8 µg/dl. Improved specificity as compared with the 1-mg test
27 Some patients with Cushing's syndrome, usually those with mild or cyclic disease, may have discordant results.
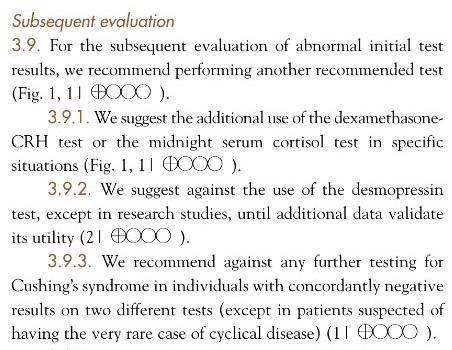
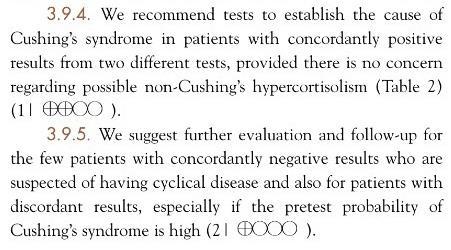
28 Subsequent Evaluation

29 Subsequent Evaluation
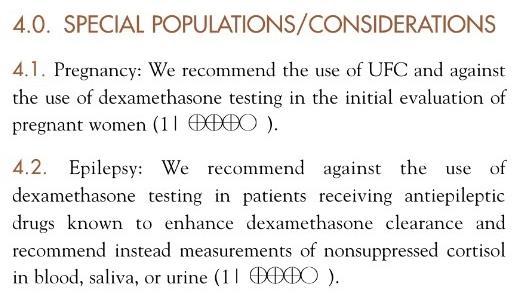
30 Special Populations

31 Pregnancy: UFC excretion is normal in the first trimester, it increases up to 3-fold by term. Dexamethasone testing has an increased potential for false positive results in pregnancy.

32 Epilepsy: Anticonvulsants are enzyme inducer drugs. May cause false positive responses on testing.
33 Renal failure: Excreted urine cortisol values decrease below creatinine clearance of 60 ml/min, and quite low, below 20 ml/min.

34 Cyclic Cusing's syndrome: Measurement of UFC or salivary cortisol may best demonstrate cyclicity. If initial tests are normal but high suspicion, follow-up is recommended with repeat testing.
35 Adrenal incidentaloma: UFC appears to be less sensitive than the 1-mg DST or late night cortisol. A suppressed ACTH or dehydroepiandrosterone sulfate concentration supports the diagnosis of Cushing's syndrome in patients with adrenal mass.


36 Determining the Cause Determining the cause Plasma ACTH High-dose dexamethasone suppression test (HDDST)
37
38 Determining the Cause ACTH level
39 Plasma ACTH Collect plasma ACTH at and the sample should be kept cool all the time. Using EDTA tube
40 Plasma ACTH Interpretation: ACTH < 10 pg/ml ->ACTH-independent Cushing's syndrome. ACTH > 20 pg/ml ->ACTH-dependent Cushing's syndrome. ACTH pg/ml-> repeating ACTH levels.
41 High-dose DST For ACTH dependent Cushing's syndrome. Measure baseline morning cortisol. 2 methods: 1. HDDST-dexamethasone 8 mg at and measure serum cortisol at Standard HDDST-Dexamethasone 2 mg every 6 hrs for 48 hrs and measure serum cortisol 2-6 hrs after last dose of dexamethasone.
42 High-dose DST Interpretation: Suppressible if serum cortisol decrease from baseline 50% or more. If not suppressible: 1. Ectopic ACTH 2. Pituitary macroadenoma
43 Pituitary MRI Should be done in all patients with ACTHdependent Cushing's syndrome.
44 Bilateral Inferior Petrosal Sinus Sampling (BIPSS) For ACTH-dependent Cushing's syndrome with normal finding in pituitary MRI. Require experienced intervention radiologist. Measure petrosal:peripheral ACTH ratio, positive if ratio = 2 or >3 after CRH
45 Ectopic ACTH CT chest and Abdomen Eg. SCLC, carcinoid tumor, islet cell tumors, medullary thyroid cancer, pheochromocytoma "รถ" "แพน" "ค นเล ก" "หมอเม ด" "ให ฟร "
46 ACTH-independent CS CT or MRI adrenal glands -> Adrenal tumor.
47 Treatment Treat complication from hypercortisolism: HT, DM, osteoporosis, gonadal axis. Treat the cause: ACTH-independent: benign adrenal adenoma, adrenocortical carcinoma Pituitary adenoma Ectopic ACTH
48 Treatment Adrenal Adenoma: unilateral adrenalectomy Adrenocortical carcinoma: remove primary tumor followed with adrenolytic agent Pituitary micro/macroadenoma: transphenoidal pituitary surgery Ectopic ACTH: depend on the type of tumor
49 Treatment Adjuvant medical therapy: Inhibit corticosteroid synthesis: ketoconazole, metyrapone Block corticosteroid effect: mifepristone Cytotoxic to adrenal cortical cells: mitotane
50 Reference The Diagnosisn of Cushing's syndrome, The Endocrine Society's clinical guideline.(j Clin Endocrinol Metab93: , 2008) Evidence-based Clinical Practice Guidelines in Endocrinology, สาขาว ชาต อมไร ท อและเมตาบอล สม ภาคว ชาอาย รศาสตร คณะแพทยศาสตร จ ฬาลงกรณ มหาว ทยาล ย MKSAP 15, Endocrinology and Metabolism, American College of Physicians. Pocket Medicine, 4th Edition
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
Cushing s Syndrome. Diagnosis. GuidelineCentral.com. Key Points. Diagnosis
 Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Differential Diagnosis of Cushing s Syndrome
 Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
Cushing s syndrome and adrenal insufficiency
 Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
CUSHING S SYNDROME. Chapter 8. Case: A 43-year-old man with delusions
 Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
Index. F Fatigue, 59 Food-dependent Cushing s syndrome, 286
 A Abdominal red striae, 57, 58 Aberrant hormone receptors, AIMAH familial forms, 215 investigative protocols, 217 218 molecular mechanisms, 216, 217 paracrine mechanisms, 216 steroidogenesis, 212 213 in
A Abdominal red striae, 57, 58 Aberrant hormone receptors, AIMAH familial forms, 215 investigative protocols, 217 218 molecular mechanisms, 216, 217 paracrine mechanisms, 216 steroidogenesis, 212 213 in
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
October 13, Surgical Nuances to Managing Cushing s Disease. Cortisol Regulation. Cushing s Syndrome Excess Cortisol. Sandeep Kunwar, M.D.
 Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
The Investigation of suspected paediatric Cushing s Syndrome (hypercortisolaemia)
") The Investigation of suspected paediatric Cushing s Syndrome (hypercortisolaemia) Formulated by Ingrid. C.E. Wilkinson, Martin O. Savage, William M. Drake and Helen L. Storr in February 2018. Centre for
The Investigation of suspected paediatric Cushing s Syndrome (hypercortisolaemia) Formulated by Ingrid. C.E. Wilkinson, Martin O. Savage, William M. Drake and Helen L. Storr in February 2018. Centre for
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW
 CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
The diagnosis and differential diagnosis of endogenous Cushing s syndrome
 HORMONES 2006, 5(4):231-250 Review The diagnosis and differential diagnosis of endogenous Cushing s syndrome Polyzois Makras, 1 Georgios Toloumis, 1 Dimitrios Papadogias, 2 Gregory A. Kaltsas, 3,4 Michael
HORMONES 2006, 5(4):231-250 Review The diagnosis and differential diagnosis of endogenous Cushing s syndrome Polyzois Makras, 1 Georgios Toloumis, 1 Dimitrios Papadogias, 2 Gregory A. Kaltsas, 3,4 Michael
The Pathological l Basis of Disease
 Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
Cortisol (serum, plasma)
") Cortisol (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Cortisol 1.2 Alternative names Hydrocortisone, 11β; 17, 21 trihydroxypregn 4 ene 3,20 dione 1.3 NMLC code 1.4 Description
Cortisol (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Cortisol 1.2 Alternative names Hydrocortisone, 11β; 17, 21 trihydroxypregn 4 ene 3,20 dione 1.3 NMLC code 1.4 Description
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
ACTH-dependent Cushing s Syndrome Update AACE MI Chapter Annual Meeting September 22, Lynnette K. Nieman DEOB, NIDDK, NIH, DHHS
 ACTH-dependent Cushing s Syndrome Update AACE MI Chapter Annual Meeting September 22, 2018 Lynnette K. Nieman DEOB, NIDDK, NIH, DHHS Objectives At the conclusion of this presentation, participants should
ACTH-dependent Cushing s Syndrome Update AACE MI Chapter Annual Meeting September 22, 2018 Lynnette K. Nieman DEOB, NIDDK, NIH, DHHS Objectives At the conclusion of this presentation, participants should
Clinical Study Clinical Characteristics of Endogenous Cushing s Syndrome at a Medical Center in Southern Taiwan
 International Endocrinology Volume 2013, Article ID 685375, 7 pages http://dx.doi.org/10.1155/2013/685375 Clinical Study Clinical Characteristics of Endogenous Cushing s Syndrome at a Medical Center in
International Endocrinology Volume 2013, Article ID 685375, 7 pages http://dx.doi.org/10.1155/2013/685375 Clinical Study Clinical Characteristics of Endogenous Cushing s Syndrome at a Medical Center in
KNUH. Cushing s syndrome. Endocrinology & Metabolism KNUH
 KNUH Cushing s syndrome Endocrinology & Metabolism KNUH 2006 Harvey William Cushing (1869-1939) Cast of the Hand of Harvey Cushing, 1922 Cushing s syndrome Hypothalamus CRH? Excess of glucocorticoids Disturbance
KNUH Cushing s syndrome Endocrinology & Metabolism KNUH 2006 Harvey William Cushing (1869-1939) Cast of the Hand of Harvey Cushing, 1922 Cushing s syndrome Hypothalamus CRH? Excess of glucocorticoids Disturbance
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Physiology. The Hypothalamic Pituitary Adrenal Axis. Elena A Christofides, MD, FACE
 Elena A Christofides, MD, FACE Endocrinology Associates, Inc Endocrinology Research Associates, Inc Physiology 2 The Hypothalamic Adrenal Axis A Complex Set of Feedback Influences* Hypothalamus releases
Elena A Christofides, MD, FACE Endocrinology Associates, Inc Endocrinology Research Associates, Inc Physiology 2 The Hypothalamic Adrenal Axis A Complex Set of Feedback Influences* Hypothalamus releases
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
2
 1 2 General % Obesity 90 Hypertension 85 Skin Plethora 70 Hirsutism/hair loss 75 Striae 50 Acne 35 Bruising/thinning 35 Musculoskeletal Osteopenia/porosis 80 Weakness 65 Neuropsych % Lability,euphoria,insomnia,
1 2 General % Obesity 90 Hypertension 85 Skin Plethora 70 Hirsutism/hair loss 75 Striae 50 Acne 35 Bruising/thinning 35 Musculoskeletal Osteopenia/porosis 80 Weakness 65 Neuropsych % Lability,euphoria,insomnia,
Pituitary Tumors and Incidentalomas. Bijan Ahrari, MD, FACE, ECNU Palm Medical Group
 Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Corticosteroids รศ. พญ. มาล ยา มโนรถ. Corticosteroids ภาคว ชาเภส ชว ทยา จ ดประสงค การศ กษา
 ภาคว ชาเภส ชว ทยา จ ดประสงค การศ กษา เม อส นส ดการเร ยนการสอน และการศ กษาด วยตนเองเพ มเต ม น กศ กษา สามารถ ทราบถ งชน ดของ glucocorticoid ธรรมชาต ท ส าค ญและกลไกการออกฤทธ ทราบถ งชน ดของ glucocorticoids
ภาคว ชาเภส ชว ทยา จ ดประสงค การศ กษา เม อส นส ดการเร ยนการสอน และการศ กษาด วยตนเองเพ มเต ม น กศ กษา สามารถ ทราบถ งชน ดของ glucocorticoid ธรรมชาต ท ส าค ญและกลไกการออกฤทธ ทราบถ งชน ดของ glucocorticoids
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Neuroendocrine Disorders in Women
 Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Subject Index. hypothalamic-pituitary-adrenal axis 158. Atherosclerosis, ghrelin role AVP, see Arginine vasopressin.
 Subject Index Acromegaly, somatostatin analog therapy dopamine agonist combination therapy 132 efficacy 132, 133 overview 130, 131 receptor subtype response 131, 132 SOM30 studies 131, 132 ACTH, see Adrenocorticotropic
Subject Index Acromegaly, somatostatin analog therapy dopamine agonist combination therapy 132 efficacy 132, 133 overview 130, 131 receptor subtype response 131, 132 SOM30 studies 131, 132 ACTH, see Adrenocorticotropic
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
CUSHING'S SYNDROME. Bharath University, Chrompet, Chennai, Tamil Nadu, India
 TJPRC: International Journal of Nursing and Patient Safety & Care (TJPRC: IJNPSC) Vol. 1, Issue 1, Jun 2016, 57-62 TJPRC Pvt. Ltd. CUSHING'S SYNDROME R. RAMANI 1 & V. HEMAVATHY 2 1 Associate Professor,
TJPRC: International Journal of Nursing and Patient Safety & Care (TJPRC: IJNPSC) Vol. 1, Issue 1, Jun 2016, 57-62 TJPRC Pvt. Ltd. CUSHING'S SYNDROME R. RAMANI 1 & V. HEMAVATHY 2 1 Associate Professor,
Adrenal Tuberculosis in Cushing s Disease with Bilateral Macronodular Adrenocortical Hyperplasia
 Endocrine Journal 2006, 53 (2), 219 223 Adrenal Tuberculosis in Cushing s Disease with Bilateral Macronodular Adrenocortical Hyperplasia HYUK-SANG KWON, SANG-IL KIM, SOON-JIB YOO, KUN-HO YOON, KWANG-WOO
Endocrine Journal 2006, 53 (2), 219 223 Adrenal Tuberculosis in Cushing s Disease with Bilateral Macronodular Adrenocortical Hyperplasia HYUK-SANG KWON, SANG-IL KIM, SOON-JIB YOO, KUN-HO YOON, KWANG-WOO
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess
 The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy
 ISPUB.COM The Internet Journal of Urology Volume 9 Number 1 Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy S Bontha, N Sanalkumar, M Istarabadi, G Lepsien,
ISPUB.COM The Internet Journal of Urology Volume 9 Number 1 Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy S Bontha, N Sanalkumar, M Istarabadi, G Lepsien,
Diagnostic Testing in Cushing's Syndrome: Reassessment of 17-hydroxycorticosteroid and 17-ketosteroid Measurements
 CRTCAL REVEW [ K e i t h D u n c a n, M. D. March, 1985 Diagnostic Testing in Cushing's Syndrome: Reassessment of 17-hydroxycorticosteroid and 17-ketosteroid Measurements ntroduction The measurement of
CRTCAL REVEW [ K e i t h D u n c a n, M. D. March, 1985 Diagnostic Testing in Cushing's Syndrome: Reassessment of 17-hydroxycorticosteroid and 17-ketosteroid Measurements ntroduction The measurement of
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
MedKorat Endocrine Day 2018 Approach to common adrenal disorder
 MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
Challenges in the diagnosis and management of Cushing s syndrome due to ectopic ACTH from bronchial carcinoid
 Challenges in the diagnosis and management of Cushing s syndrome Challenges in the diagnosis and management of Cushing s syndrome due to ectopic ACTH from bronchial carcinoid M S A Cooray 1, N P Somasundaram
Challenges in the diagnosis and management of Cushing s syndrome Challenges in the diagnosis and management of Cushing s syndrome due to ectopic ACTH from bronchial carcinoid M S A Cooray 1, N P Somasundaram
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens
 Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Professor Ian Holdaway. Endocrinologist Auckland District Health Board
 Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
Cushing Syndrome in Pediatrics
 Cushing Syndrome in Pediatrics Constantine A. Stratakis, MD, D (Med) Sci a,b, * KEYWORDS Cushing syndrome Pituitary tumors Cortisol Adrenal cortex Carney complex Adrenocortical hyperplasia Adrenal cancer
Cushing Syndrome in Pediatrics Constantine A. Stratakis, MD, D (Med) Sci a,b, * KEYWORDS Cushing syndrome Pituitary tumors Cortisol Adrenal cortex Carney complex Adrenocortical hyperplasia Adrenal cancer
Sean Hamlett DO FACOI Endocrinology, Diabetes, and Metabolism Freeman Health System Joplin, MO
 Sean Hamlett DO FACOI Endocrinology, Diabetes, and Metabolism Freeman Health System Joplin, MO I will not be discussing any off-label uses of medications. I am a paid speaker for: Amylin, BMS, BI, and
Sean Hamlett DO FACOI Endocrinology, Diabetes, and Metabolism Freeman Health System Joplin, MO I will not be discussing any off-label uses of medications. I am a paid speaker for: Amylin, BMS, BI, and
Therapeutic Objectives. Cushing s Disease Surgical Results. Cushing s Disease Surgical Results: Macroadenomas 10/24/2015
 Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS
 The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS Brett McWhinney, Supervising Scientist, HPLC Section, Pathology Central, Pathology Queensland Overview 1. Overview of Pathology
The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS Brett McWhinney, Supervising Scientist, HPLC Section, Pathology Central, Pathology Queensland Overview 1. Overview of Pathology
Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
False-positive inferior petrosal sinus sampling in the diagnosis of Cushing s disease
 J Neurosurg 83:1087 1091, 1995 False-positive inferior petrosal sinus sampling in the diagnosis of Cushing s disease Report of two cases YOSHIHIRO YAMAMOTO, M.D., D.M.SC., DUDLEY H. DAVIS, M.D., TODD B.
J Neurosurg 83:1087 1091, 1995 False-positive inferior petrosal sinus sampling in the diagnosis of Cushing s disease Report of two cases YOSHIHIRO YAMAMOTO, M.D., D.M.SC., DUDLEY H. DAVIS, M.D., TODD B.
AN UNUSUAL PRESENTATION OF PEDIATRIC CUSHING DISEASE: DIABETIC KETOACIDOSIS
 Case Report AN UNUSUAL PRESENTATION OF PEDIATRIC CUSHING DISEASE: DIABETIC KETOACIDOSIS Gonul Catli, MD 1 ; Ayhan Abaci, MD 2 ; Ozgur Tanrisever, MD 3 ; Cemil Kocyigit, MD 4 ; P. Sule Can, MD 1 ; Bumin
Case Report AN UNUSUAL PRESENTATION OF PEDIATRIC CUSHING DISEASE: DIABETIC KETOACIDOSIS Gonul Catli, MD 1 ; Ayhan Abaci, MD 2 ; Ozgur Tanrisever, MD 3 ; Cemil Kocyigit, MD 4 ; P. Sule Can, MD 1 ; Bumin
stone) Policy covered: in patients d): Korlym is enrolled in diabetes or glucose Cushing s syndrome adult patients with treated with metabolic caused
 Policy covered: in patients d): Korlym is enrolled in diabetes or glucose Cushing s syndrome adult patients with treated with metabolic caused") Korlym (mifepris stone) Policy Number: 5.01.545 Origination: 06/2013 Last Review: 05/2014 Next Review: 05/2015 Policy BCBSKC will provide coverage for Korlym when it is determined to be medically necessary
Korlym (mifepris stone) Policy Number: 5.01.545 Origination: 06/2013 Last Review: 05/2014 Next Review: 05/2015 Policy BCBSKC will provide coverage for Korlym when it is determined to be medically necessary
The endocrine system is complex and sometimes poorly understood.
 1 CE Credit Testing the Endocrine System for Adrenal Disorders and Diabetes Mellitus: It Is All About Signaling Hormones! David Liss, BA, RVT, VTS (ECC) Platt College Alhambra, California For more information,
1 CE Credit Testing the Endocrine System for Adrenal Disorders and Diabetes Mellitus: It Is All About Signaling Hormones! David Liss, BA, RVT, VTS (ECC) Platt College Alhambra, California For more information,
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Cushings Syndrome. Cushings Syndrome
 We have made it easy for you to find a PDF Ebooks without any digging. And by having access to our ebooks online or by storing it on your computer, you have convenient answers with cushings syndrome. To
We have made it easy for you to find a PDF Ebooks without any digging. And by having access to our ebooks online or by storing it on your computer, you have convenient answers with cushings syndrome. To
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing
 Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
The Investigation of Cushing Syndrome: Essentials in Optimizing Appropriate Diagnosis and Management
 The Investigation of Cushing Syndrome: Essentials in Optimizing Appropriate Diagnosis and Management Agata Juszczak, Ashley Grossman From the University of Oxford and Oxford Centre for Diabetes, Endocrinology
The Investigation of Cushing Syndrome: Essentials in Optimizing Appropriate Diagnosis and Management Agata Juszczak, Ashley Grossman From the University of Oxford and Oxford Centre for Diabetes, Endocrinology
TEST NAME: DUTCH Adrenal
 Category Test Result Units Normal Range Creatinine (Urine) Creatinine A (Waking) Within range 0.25 mg/ml 0.2-2 Creatinine B (Morning) Within range 0.28 mg/ml 0.2-2 Creatinine C (Afternoon) Within range
Category Test Result Units Normal Range Creatinine (Urine) Creatinine A (Waking) Within range 0.25 mg/ml 0.2-2 Creatinine B (Morning) Within range 0.28 mg/ml 0.2-2 Creatinine C (Afternoon) Within range
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
CUSHING S SYNDROME AND CUSHING S DISEASE
 PATIENT INFORMATION CUSHING S SYNDROME AND CUSHING S DISEASE YOUR QUESTIONS ANSWERED 2013 Update Contents What are Cushing s syndrome and Cushing s disease? What causes Cushing s syndrome and Cushing s
PATIENT INFORMATION CUSHING S SYNDROME AND CUSHING S DISEASE YOUR QUESTIONS ANSWERED 2013 Update Contents What are Cushing s syndrome and Cushing s disease? What causes Cushing s syndrome and Cushing s
pharmacology sheet #9 Adrenal Steroids Mineral corticoids & Glucocorticoids
 Adrenal Steroids Mineral corticoids & Glucocorticoids Extra notes : Slide 2: - All Steroids are synthesized in the adrenal gland and secreted from it, It consists of an outer cortex and an inner medulla.
Adrenal Steroids Mineral corticoids & Glucocorticoids Extra notes : Slide 2: - All Steroids are synthesized in the adrenal gland and secreted from it, It consists of an outer cortex and an inner medulla.
Treatment of Cushing s Syndrome: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline Treatment of Cushing s Syndrome: An Endocrine Society Clinical Practice Guideline Lynnette K. Nieman (chair), Beverly M. K. Biller, James W. Findling, M. Hassan
SPECIAL FEATURE Clinical Practice Guideline Treatment of Cushing s Syndrome: An Endocrine Society Clinical Practice Guideline Lynnette K. Nieman (chair), Beverly M. K. Biller, James W. Findling, M. Hassan
The Pathological l Basis of Disease
 Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa Qiao.Li@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa Qiao.Li@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endogenous Cushing s syndrome: The Philippine general hospital experience
 ORIGINAL ARTICLE Endogenous Cushing s syndrome: The Philippine general hospital experience Tom Edward N. Lo, Joyce M. Cabradilla, Sue Ann Lim, Cecilia A. Jimeno Section of Endocrinology and Metabolism,
ORIGINAL ARTICLE Endogenous Cushing s syndrome: The Philippine general hospital experience Tom Edward N. Lo, Joyce M. Cabradilla, Sue Ann Lim, Cecilia A. Jimeno Section of Endocrinology and Metabolism,
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules. Celeste Thomas November 1, 2012
 57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
Urinary Hormone Metabolites Adrenal
 Test Name Result Range Urinary Androgens (μg/g Cr) DHEA (Urine) 503.87 H 9.01-93.80 Urinary Glucocorticoids (μg/g Cr) Total Cortisol (Urine) 18.50 8.73-28.52 Total Cortisone (Urine) 35.72 14.12-42.84 Cortisol/Cortisone
Test Name Result Range Urinary Androgens (μg/g Cr) DHEA (Urine) 503.87 H 9.01-93.80 Urinary Glucocorticoids (μg/g Cr) Total Cortisol (Urine) 18.50 8.73-28.52 Total Cortisone (Urine) 35.72 14.12-42.84 Cortisol/Cortisone
ACUTE SEVERE CUSHING SYNDROME: NOT ALWAYS ECTOPIC ACTH SYNDROME
 Case Report ACUTE SEVERE CUSHING SYNDROME: NOT ALWAYS ECTOPIC ACTH SYNDROME Carlos Tavares Bello, MD 1 ; Inês Gil, MD 2 ; Filipa Alves Serra, MD 3 ; João Sequeira Duarte 1 ABSTRACT Objective: Cushing syndrome
Case Report ACUTE SEVERE CUSHING SYNDROME: NOT ALWAYS ECTOPIC ACTH SYNDROME Carlos Tavares Bello, MD 1 ; Inês Gil, MD 2 ; Filipa Alves Serra, MD 3 ; João Sequeira Duarte 1 ABSTRACT Objective: Cushing syndrome
Case Report Metyrapone for Long-Term Medical Management of Cushing s Syndrome
 Case Reports in Endocrinology Volume 2013, Article ID 782068, 4 pages http://dx.doi.org/10.1155/2013/782068 Case Report Metyrapone for Long-Term Medical Management of Cushing s Syndrome Andrea N. Traina,
Case Reports in Endocrinology Volume 2013, Article ID 782068, 4 pages http://dx.doi.org/10.1155/2013/782068 Case Report Metyrapone for Long-Term Medical Management of Cushing s Syndrome Andrea N. Traina,
A short & obese - girl
 A short & obese - girl Presented by :Dr.Amit P Ghawade (DNB Resident-1st Year ) Guide :Dr.S.Ramkumar MD(pediatrics) ICH & HC, Chennai, DM(endocrinology) AIIMS, Delhi Department of Pediatric Endocrinology
A short & obese - girl Presented by :Dr.Amit P Ghawade (DNB Resident-1st Year ) Guide :Dr.S.Ramkumar MD(pediatrics) ICH & HC, Chennai, DM(endocrinology) AIIMS, Delhi Department of Pediatric Endocrinology
Case Report Pediatric Cushing s Disease and Pituitary Incidentaloma: Is This a Real Challenge?
 Case Reports in Endocrinology, Article ID 851942, 5 pages http://dx.doi.org/10.1155/2014/851942 Case Report Pediatric Cushing s Disease and Pituitary Incidentaloma: Is This a Real Challenge? Rosa Maria
Case Reports in Endocrinology, Article ID 851942, 5 pages http://dx.doi.org/10.1155/2014/851942 Case Report Pediatric Cushing s Disease and Pituitary Incidentaloma: Is This a Real Challenge? Rosa Maria
DIAGNOSIS OF CANINE HYPERADRENOCORTICISM: A CASE-BASED APPROACH Ellen N. Behrend, VMD, PhD, DACVIM
 DIAGNOSIS OF CANINE HYPERADRENOCORTICISM: A CASE-BASED APPROACH Ellen N. Behrend, VMD, PhD, DACVIM Case 1: Signalment: 10 yr old, CM, Miniature poodle; History: Presented for teeth cleaning; PE: Severe
DIAGNOSIS OF CANINE HYPERADRENOCORTICISM: A CASE-BASED APPROACH Ellen N. Behrend, VMD, PhD, DACVIM Case 1: Signalment: 10 yr old, CM, Miniature poodle; History: Presented for teeth cleaning; PE: Severe
MANAGEMENT OF PATIENTS WITH CUSHING S DISEASE: A CANADIAN COST OF ILLNESS ANALYSIS
 MANAGEMENT OF PATIENTS WITH CUSHING S DISEASE: A CANADIAN COST OF ILLNESS ANALYSIS S. Van Uum 1, M. Hurry 2, R. Petrella 1, C. Koch 2, G. Dranitsaris 3, A. Lacroix 4 1 Western University, Schulich School
MANAGEMENT OF PATIENTS WITH CUSHING S DISEASE: A CANADIAN COST OF ILLNESS ANALYSIS S. Van Uum 1, M. Hurry 2, R. Petrella 1, C. Koch 2, G. Dranitsaris 3, A. Lacroix 4 1 Western University, Schulich School
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Medical Expert
 Medical Expert") Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Endocrine Diseases. The Pathological Basis of Disease
 Endocrine Diseases The Pathological Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
Adrenal and retropetionium
 Adrenal and retropetionium Disorders of the Adrenal Cortex Hyperaldosteronism: Hyperaldosteronism may be secondary to stimulation of the renin-angiotensin system from renal artery stenosis and to low-flow
Adrenal and retropetionium Disorders of the Adrenal Cortex Hyperaldosteronism: Hyperaldosteronism may be secondary to stimulation of the renin-angiotensin system from renal artery stenosis and to low-flow
UW MEDICINE PATIENT EDUCATION. Cushing s Syndrome DRAFT. What is Cushing s syndrome? What is cortisol? What are the symptoms of Cushing s syndrome?
 UW MEDICINE PATIENT EDUCATION Cushing s Syndrome Causes, symptoms, diagnosis, and treatments This handout explains Cushing s syndrome, its causes, symptoms, and how it is diagnosed. It also includes a
UW MEDICINE PATIENT EDUCATION Cushing s Syndrome Causes, symptoms, diagnosis, and treatments This handout explains Cushing s syndrome, its causes, symptoms, and how it is diagnosed. It also includes a
Il Carcinoma Surrenalico
 Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
Cushing s syndrome with no clinical stigmata a variant of glucocorticoid. resistance syndrome.
 Gossain et al. Clinical Diabetes and Endocrinology (2018) 4:23 https://doi.org/10.1186/s40842-018-0072-5 CASE REPORT Open Access Cushing s syndrome with no clinical stigmata a variant of glucocorticoid
Gossain et al. Clinical Diabetes and Endocrinology (2018) 4:23 https://doi.org/10.1186/s40842-018-0072-5 CASE REPORT Open Access Cushing s syndrome with no clinical stigmata a variant of glucocorticoid
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
A Comparison of Saliva & Wet Urine for Hormone Measurements
 A Comparison of Saliva & Wet Urine for Hormone Measurements Introduction The evaluation of circulating hormone levels through laboratory testing is an essential part of the assessment and diagnosis of
A Comparison of Saliva & Wet Urine for Hormone Measurements Introduction The evaluation of circulating hormone levels through laboratory testing is an essential part of the assessment and diagnosis of
Rhythm Plus- Comprehensive Female Hormone Profile
 Rhythm Plus- Comprehensive Female Hormone Profile Patient: SAMPLE REPORT DOB: Sex: F Order Number: K00000 Completed: Received: Collected: SAMPLE REPORT Sample # Progesterone (pg/ml) Hormone Results Oestradiol
Rhythm Plus- Comprehensive Female Hormone Profile Patient: SAMPLE REPORT DOB: Sex: F Order Number: K00000 Completed: Received: Collected: SAMPLE REPORT Sample # Progesterone (pg/ml) Hormone Results Oestradiol
Audit of Adrenal Function Tests. Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK
 Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore
Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore