Ruth L. Katz, M.D. Chief Research Cytopathology, Professor of Pathology, University of Texas. M.D. Anderson Cancer Center.
|
|
|
- Lilian Melton
- 5 years ago
- Views:
Transcription
1 Practical FNA in Lymphoma Diagnosis: What the Clinician wants to Know and How to Get There! Ruth L. Katz, M.D. Chief Research Cytopathology, Professor of Pathology, University of Texas M.D. Anderson Cancer Center Houston, Texas Presentation Bullet Points Diagnosis of lymphoma using WHO Classification Grade of Lymphoma Proliferation Index?Transformation FISH Complementary Papanicolaou and Romanowsky stains Immunophenotyping by Cytospin or FCM or both An Approach to the Diagnosis of Lymphoma by Fine Needle Aspiration: What the Clinician Needs to Know By Ruth L. Katz, M.D. Professor of Pathology
2 Chief Research Cytopathology Director, Image Cytometry Diagnostic Laboratory Pathology/Cytopathology U.T. M.D. Anderson Cancer Center 1515 Holcombe Boulevard 53 Houston, Texas Office: Fax: USCAP 2007, Fine-Needle Aspiration of Lymph Nodes Ruth L. Katz, M. D. INTRODUCTION In the past, the role of fine-needle aspiration (FNA) biopsy of lymph nodes was basically to evaluate for metastatic disease; however, over the last two decades there has been a gradual increase in the number of publications documenting the value of FNA in the diagnosis and subclassification of non-hodgkin lymphomas, particularly in institutions which use cytomorphology in conjunction with ancillary studies. At M.D. Anderson Cancer Center highly accurate lymphoma diagnoses can be made when compared to the corresponding histology, when FNAs are combined with immunophenotyping and Ki-67, and classified by the WHO classification. In many institutions, FNA of lymphomas is used primarily to document residual or recurrent disease or to stage the patient; however, with the advent of the WHO classification for lymphoma combined with sophisticated phenotyping by flow cytometry and molecular studies such as fluorescence-in-situ hybridization (FISH) for non-random chromosomal translocations, it is possible to use FNA as a primary modality for classifying some subtypes of non-hodgkin s lymphoma. To some extent, the role of FNA in rendering a primary diagnosis of lymphoma remains controversial. Many of the limitations in diagnosing lymphoproliferative disorders by FNA have been addressed and center particularly on the lack of architecture provided by tissue smears to further subclassify certain lymphomas. In many instances of follicular lymphoma (FL) careful examination of the smear will reveal recognizable follicular structures that may represent the neoplastic follicles of FL. Moreover, the absence of architecture can be overcome to a significant extent with the use of immunophenotyping to assess B-cell and T-cell differentiation, FISH or pcr to assess cytogenetic abnormalities and Ki-67 for proliferation activity as most subtypes of lymphoma have distinctive cytomorphologic, immunophenotypic, molecular and proliferation profiles. However, a subsequent biopsy should always be performed if there is inadequate material, ambiguous results, or if the clinical and radiographic findings are not in keeping with the cytologic interpretation. This handout emphasizes the most important features that the pathologist performing the FNA should provide in the report, namely: Diagnosis by the WHO classification Grade of lymphoma Immunophenotype Proliferation status (Ki-67)
3 Presence of transformation. HANDLING OF THE LYMPHOCYTE-RICH FNA SPECIMEN It is strongly recommended that a standardized approach be implemented in the handling and triaging of FNA specimens that includes cytomorphology along with immunophenotyping and proliferation markers as together they have excellent potential for a cytology-based diagnosis. These lymphocyte-rich, highly cellular specimens are easily obtained and if they are handled according to the schema presented below, more than 90% of the aspirates can be diagnosed accurately. If a patient presents with a clinical history suggestive of a lymphoproliferative disorder, the pathologist should make adequate preparations before performing FNA. It is important to locate a laboratory that can handle immunophenotyping of FNA specimens using flow cytometry or immunocytochemical stains on cytospin preparations. An adequate portion of the aspirate should always be saved in tissue culture medium (RPMI) or other transport media for immunophenotyping. It is helpful to perform a cell count to determine if there is adequate cellularity for ancillary studies. At MD Anderson Cancer Center we use a Coulter Counter to quantitate the rinsed cells that have been placed in RPMI media until a total of at least 10 million cells have been collected. When evaluating a lymphoproliferative disorder, one should assess the cellular features and cell composition. The cell size may be small (equal or slightly larger than a normal resting lymphocyte), intermediate (one and one-half times the size of a normal lymphocyte, and no greater than the nucleus of a histiocyte), or large (two to three times the size of a normal lymphocyte). The nuclei may be round, cleaved, or lobulated. The cell population may be monomorphous with one cell type predominating, or polymorphous containing a mixture of cells. Depending on the cytologic evaluation and the clinical history, appropriate ancillary studies can be requested. Our approach to the work-up of lymphoproliferative disorders always includes the following whenever possible: 1. Cytomorphology assessed on Papanicolaou stain (alcohol-fixed) and Diff-Quik (airdried) smears and classified according to the WHO classification 2. Immunophenotyping by flow cytometry or immunocytochemistry on cytospin preparations 3. Proliferation index determined by image analysis on Feulgen stained slides, or immunostaining with Ki-67 and used in conjunction with morphology to grade lymphomas, or rule out transformation. 4. Genotyping by polymerase chain reaction (PCR) is rarely performed except for nonmarking lymphomas, low-grade T-cell lymphomas, partially involved nodes, or equivocal marker studies; cytogenetics, or fluorescence-in-situ-hybridization (FISH) can be used to confirm lymphomas with characteristic chromosomal abnormalities 5. Aspirated material for cultures and special stains (Gomori methenamine-silver, acid fast bacilli (GMS), and gram stain) if an infectious process is suspected Cytospin preparations for marker studies are made from the aspirated cells that are collected in a preservation medium such as RPMI and concentrated by a density gradient technique. A panel of immunomarkers for small B cell lymphomas should include kappa, lambda, CD3, CD5, CD10, CD19, CD20, CD23, bcl-6 and Ki-67 with additional cytospins made and stored at -80 degrees C in the event that further studies are needed. Immunocytochemistry is performed on air-dried cytospins that are left to air-dry under the hood overnight, and then fixed in acetone for 10 minutes just prior to commencement of immunostaining. Immunophenotyping and proliferative activity can also be determined by flow cytometry. A minimum of 10 million cells is needed for most of these studies, and this amount can usually be obtained in two to three passes.
4 Flow Cytometric Immunophenotyping (FCI) Three- or four-color flow cytometric analysis is used on the cells from FNAs rinsed in RPMI, and is an excellent method for evaluating low cellularity specimens (less than 5 million cells). Sensitivity is very high and may detect aberrant cells at 1/1000 to 1/10,000. Cells are stained in the RPMI solution with appropriate antibodies (see below) and the specimens are subjected to whole blood lysis following incubation with antibodies using NH4Cl and washing with PBS. Cells are then fixed with 1% paraformaldehyde and analyzed on a FACScan (Becton-Dickinson) using CELLQuest software (Becton-Dickinson). All antibodies are purchased from Becton Dickinson (San Jose, CA), except for CD10 (Coulter) and FMC7 (Immunotech). The following antibody combinations tailored specifically for FNA usage are as follows: CD3-APC/CD45-PerCP/CD23-PE/FMC7-FITC, CD45-PerCP/CD19-APC/CD10-FITC, CD20- APC/CD45-PerCP/Lambda-PE/Kappa-FITC, CD45-PerCP/ CD-11 C-PE/CD-22-FITC Controls are isotype controls using IgG1- or IgG2-PerCP/IgG1-PE/IgG1-FITC, while monocytes are excluded from the gate using a CD45/CD14 combination. For each tube a minimum of 500,000 cells are incubated with 10 microliters of antibody at 2-8 C for 15 minutes in the dark. The minimal requirement is to have 50,000 cells per tube to analyze 10,000 events and this is better performed if there is an almost pure population of lymphoma cells such as one frequently obtains by FNA. For analysis 10,000 cells are acquired from each tube and lymphoid cells are gated based on CD45 antigen density and right angle light scatter pattern. Results are expressed as the percentage of cells expressing antigen within the gated region. Disadvantages of FCI compared to immunocytochemistry on slides include poorer assessment of certain nuclear or cytoplasmic markers than by immunocytochemistry, loss of cytoplasm on large cell lymphoid processes resulting in false negative results (need to check forward light scatter on histograms to see if large cell population is present), and no direct correlation between morphology and phenotype, which of course is possible by slide based immunocytochemistry. Interpretation of the patterns generated by the flow data is critical to accurate interpretation of a malignant versus a reactive population. For an excellent discussion of the applications of FCI the reader is referred to the paper by Jeffrey L. Jorgensen, Cancer Cytopathology, Dec 25, 2005, Vol 105, Number 6. Proliferation Studies Proliferation indices can be determined by flow cytometry, image analysis, or immunocytochemistry using Ki-67 % labeling index. DNA image analysis can also determine the DNA ploidy and the proliferative index, which has shown a strong correlation with the grade and outcome of lymphoma. This technique is particularly useful in aspirates that yield low cellularity and can be performed on a single cytospin preparation prepared in a similar manner as for immunocytochemical analysis, but fixed in image fixative and Feulgen stained. At our institution, a cutoff of 26% Ki-67 labeling index is used to separate low-grade versus high-grade lymphoma. Ki-67 is very helpful in grading follicular lymphoma (see table below).
5 The distribution of Ki67 (%) by groups of follicular lymphoma. Ki67 (%) Group of Follicular Lymphoma N Median (range) Grade (2-26) Grade (8-25) Grade (5-90) Transformed (25-90) P-value < (Kruskal-Wallis test) between Grades1 and 2, and Grade3 and t Reactive Hyperplasia (Chronic Lymphandenitis) A number of conditions are associated with characteristic architectural patterns in reactive hyperplasia. Unfortunately, a compartmentalized architectural pattern (follicular versus inter-follicular versus sinusoidal) cannot be assessed by FNA. Usually, the purpose of the FNA is not to determine the specific cause of the reactive hyperplasia, but to exclude malignancy and infectious organisms. Chronic Lymphandenitis, more commonly referred to as reactive hyperplasia, is the most common diagnosis rendered on lymph node aspirates because most enlarged lymph nodes are benign and reactive. Clinically, chronic lymphandenitis can occur at any age, but is usually seen in children. The cervical, axillary, and inguinal lymph nodes are more often involved, since they drain large areas of the body. Reactive nodes are usually less than 3 cm in diameter; however, they may be larger in children. Cytomorphology: Reactive hyperplasia is characterized by a polymorphous cell population comprising the whole range of follicular center cells (small and large, cleaved and noncleaved), immunoblasts, small lymphocytes, plasmacytoid lymphocytes, neutrophils, tingible body macrophages, and reactive follicular center fragments. These are best recognized at low power on Diff-Quik smears, in which the cells of different sizes cling together, held in place by follicular dendritic cells or antigen-presenting cells. Apoptotic fragments and mitoses may be seen in these cell groups. Ancillary Studies: Immunophenotyping typically shows a polyclonal population with absence of light chain restriction. Reactive T-cells may constitute a large component; however, if they exceed 80%, then a low-grade T-cell lymphoma should be considered. Differential Diagnosis: Follicular lymphoma lacks a well-defined transition of small to large cells; two neoplastic subpopulations,one comprising small to intermediate or large cleaved or centrocytic cells, and a second large centroblastic population, are seen. However this morphology may be complicated by up to 30-50% smaller lymphocytes, representing residual T- cells, that may be present. In general, follicular lymphomas show many more, and larger, atypical centroblasts than even the most florid reactive hyperplasia. Monoclonality for B-cell derivation and CD10 positivity is demonstrated by marker studies. T-cell lymphomas also may contain plasma cells, eosinophils, and epithelioid histiocytes. Demonstration of T-cell derivation may be more difficult because of the bland nature of the cells, and genotyping may be required. Reactive hyperplasia may be also be confused with marginal zone lymphoma which may present with a mixed cell population of small to intermediate-sized cells with bland histiocyte-
6 like or monocytoid nuclei, small lymphocytes, plasma cells, and large noncleaved cells. Marginal zone lymphomas are monoclonal for immunoglobulin (Ig) light chains, and lack expression of CD5 and CD10 (4). They co-express CD22 and CD11c. LYMPHOMAS Classification of Lymphomas In the last decade there has been remarkable progress in the understanding of lymphomas based on laboratory and clinical findings, i.e., morphologic features, immunophenotype, cytogenetic analysis, molecular findings, and clinical manifestations and course. This information has been used to help define entities in the Revised European-American Classification of Lymphoid Neoplasms (REAL) as proposed by the International Lymphoma Study Group in This classification system categorizes entities based on the neoplasm s cell of origin. Since the REAL classification has a greater emphasis on cytomorphologic features in conjunction with immunophenotyping and molecular studies, it can be easily applied to aspiration specimens using a multiparameter approach. The WHO classification for lymphomas is similar to the REAL classification for lymphomas (Table 1) with minor modifications as subsequent data has become available.this handout highlights the small B cell non-hodgkin s lymphomas which are encountered in everyday practice, and not all the lymphomas in the WHO classification are discussed. Certain lymphoma entities can be cytologically graded within entities: hence, follicular lymphoma may be graded as Grade 1, 2, 3 based on the number of large transformed cells within follicular structures noted on the smears; mantle cell lymphoma may be defined as classical or blastoid, based on presence of blastic cells in the latter. Diffuse large cell B-cell lymphoma encompasses entities previously known as centroblastic, immunoblastic, T-cell or histiocyte rich, and anaplastic large B-cell. Burkitt s-like lymphoma (BLL) defines a lymphoma which formerly fell between the morphological categories of Burkitt s lymphoma (BL) and diffuse large cell lymphoma, and frequently shared the same translocation of t(8;14), or variant translocations t(2;8) and t(8;22) as BL, or t(14;18) seen in a small subset of diffuse-large cell lymphoma. In order to call a lymphoma BLL by the WHO classification, it is now a requirement that at least 99% of cells be cycling as demonstrated by Ki-67. NON-HODGKIN LYMPHOMA Small Lymphocytic Lymphoma In the WHO classification, B-cell chronic lymphocytic leukemia and small lymphocytic lymphoma are grouped together as mature B cell neoplasms. The majority of cases occur in older adults. Most patients present with bone marrow and blood involvement; however, occasionally they are aleukemic with nodal involvement. Many of the latter cases will eventually develop disease in the bone marrow and blood. The clinical course is indolent, but not curable. It may transform to prolymphocytic lymphoma, large cell lymphoma (Richter s syndrome), and rarely to Hodgkin lymphoma. Cytomorphology: Small lymphocytic lymphoma is composed of a monotonous population of small round lymphocytes with nuclei containing a coarsely clumped checkerboard chromatin pattern. Scattered in the background are large cells representing prolymphocytes and paraimmunoblasts. Prolymphocytes are slightly larger than paraimmunoblasts, but they both have round nuclei, with prominent nucleoli and gray-blue cytoplasm.
7 An increase in the numbers of paraimmunoblasts may indicate a more aggressive clinical course than the typical small lymphocytic lymphoma, while a predominance of large cells is indicative of a transformation to large cell lymphoma (Richter s syndrome). Ancillary Studies: Immunophenotyping shows light chain restriction and positivity for cell-associated antigens (CD19, CD20, CD79a), CD5, and CD23, while CD10 and FMC7 are negative. Cytokinetic studies of small lymphocytic lymphoma show a diploid population with low proliferative activity (Ki-67 has a mean labeling index of 5%). In contrast, transformed large cell lymphoma (Richter s syndrome) has a high proliferation index. Trisomy for chromosome 12 and abnormalities for 13q14, Lamp1, p53 and ATM gene(11q22-23) may be detected by FISH on cytospin preparations (7). Differential Diagnosis: Although both small lymphocytic lymphoma and mantle cell lymphoma show aberrant co-expression of CD5 and lack CD10, small lymphocytic lymphoma is positive for CD23, while mantle cell lymphoma is not. Both follicular lymphoma and marginal zone lymphoma are CD5 and CD10 negative. Lymphocyte predominant Hodgkin Lymphoma should be considered if there are polyploid cells (so-called L & H cells or popcorn cells) in a background of mature lymphocytes instead of paraimmunoblasts. Mantle Cell Lymphoma Mantle cell lymphoma usually occurs in older adults with a predilection for males. At the time of diagnosis, the disease is often widespread and can involve lymph nodes, spleen, bone marrow, blood, and extranodal sites. It is more aggressive than the other B-cell non-hodgkin s lymphomas composed of small cells, and has a median survival of 3 to 5 years. Cytomorphology: Mantle cell lymphoma shows a variety of morphologies ranging from the classic variant, to a pleomorphic variant and a blastic variant. The classic variant shows a monotonous population of uniform, small-to-intermediate sized cells, with slight to marked nuclear membrane irregularities and indentations. The chromatin pattern is fine, giving a lighter appearance to the nuclei, compared with those seen in small lymphocytic lymphoma. Nucleoli generally are small and inconspicuous, and the cytoplasm is scanty. In most cases, minor populations of cells with small round nuclei, as well as cells with angulated irregular nuclei are noted. The cells of the blastic variant are intermediate in size and resemble blasts of lymphoblastic T-cell lymphoma. The pleomorphic variant has a range of cell types, including the small angulated cells and larger transformed cells. Monocytoid cells and histiocytes with ingested debris may be seen. Mitoses may be seen. Ancillary Studies: The cells show positive immunostaining for B-cell associated antigens (CD19, CD20, CD22), CD5, and FMC7, and negative for CD10, and CD23. Usually lambdalight-chain restriction is more common than kappa-light-chain restriction. Cytokinetic studies of the classic variant usually show a diploid population with low to intermediate proliferative activity. The blastic variant typically is tetraploid, with very high Ki- 67 labeling index. A characteristic chromosomal t(11;14)(q13;32q) translocation has been demonstrated involving the Ig heavy chain locus and the Bcl-l locus on the long arm of chromosome 11. This translocation results in overexpression of the PRAD/bcl-1 gene that encodes for cyclin D1, a cellcycle protein. Immunostaining in our laboratory for cyclin D1 on cytospin preparations has been variable but if a cell block is performed, antigen retrieval and immunocytochemistry for Cyclin- D1 antibody will be successful. The polymerase chain reaction detects breakpoints in the major translocation cluster (MTC) region of bcl-1; however, this is positive in only 30-50% of mantle cell lymphomas (74). The t (11; 14) translocation can be demonstrated by FISH in a high percentage of MCL on cytology specimens.
8 Differential Diagnosis: Differentiating mantle cell lymphoma from small lymphocytic lymphoma and follicular center lymphoma is based on the absence of blast cells (paraimmunoblasts and centroblasts) and a homogeneous population of cells. In addition, immunophenotyping is very important in distinguishing the B-cell lymphomas composed on small cells. While both mantle cell lymphoma and small lymphocytic lymphoma are CD5 positive, and CD10 negative, only the latter is positive for CD23. Follicular lymphoma shows CD10 expression. Mantle cell lymphoma may be confused with the centrocyte-like cells of marginal zone lymphoma; however, the latter shows a far more heterogeneous population of cells including monocytoid B-cells, plasma cells, and centroblasts. Like mantle cell lymphoma, marginal zone lymphoma is negative for CD3 and CD10, but it can be differentiated by its lack of CD5. Marginal Zone Lymphoma Marginal zone lymphoma is rare, low grade, B-cell neoplasm that has two major clinical presentations, extranodal and nodal. Extranodal marginal zone lymphoma is also known as mucosal-associated lymphoid tissue (MALT) and the majority of these cases have localized disease. Cytomorphology: There is a heterogeneous population composed of cleaved forms (centrocytes), mature cells small lymphoid, plasma cells, and monocytoid cells. Ancillary Studies: Immunophenotyping shows cells positive for B-cell-associated antigens (CD19, CD20, CD22, CD79a), but negative for CD10, CD23, CD103, and CD5 (rare cases are positive). Cytogenetics: t (11;18) AP12 (apoptosis inhibitor gene); 18q 21 (MLT). Differential Diagnosis: Reactive processes can be differentiated by demonstration of a polyclonal cell population. By cytology, hairy cell leukemia can be difficult to distinguish from the monocytoid B-cells of marginal zone lymphoma. MZL may occur in the spleen and produce a syndrome of splenic lymphoma, with villous lymphocytes mimicking hairy cell leukemia. Small lymphocytic lymphoma and mantle cell lymphoma can be differentiated by CD5 positivity, while follicular lymphomas are positive for CD10. Follicular Lymphoma (FL): Cytologic Grades 1 (Predominantly Small Cells), 2 (Mixed Small and Large Cells), and 3 (Predominantly Large Cells) Follicular lymphomas are B-cell neoplasms composed of a mixture of cleaved follicular center cells (centrocytes) and large noncleaved follicular center cells (centroblasts). FL has the ability to recapitulate the follicular architecture, at least focally; however, diffuse areas may also be present. We use a cytologic classification loosely based on the histologic criteria of Mann and Berard. We initially look for follicular structures in which to base our estimation of cell types. The numbers of large, noncleaved (centroblasts) as a percentage of small centrocytic cells per high power field within a follicular structure are counted. In the absence of follicles, we count representative fields. The presence of confluent areas of large cells may indicate a partial transformation to a higher grade FL. Follicular Lymphoma Grading as Used in Cytopathology* Groups Follicles cell count % Grade 1 (n = 31) 9.7 ( ) Grade 2 (n = 46) 24.7 ( ) * Grade 3 (n = 10) 48.3 ( ) *#
9 * = p < 0.05 vs. grade 1 group # = p < 0.05 vs. grade 2 group + Based on centroblasts within follicles 200 cells (all cell types) within follicles are counted on papanicolau stained direct smears. The number of centroblasts / 200 cells are expressed as a percentage. Reference: Wei Sun, MD, Nancy Caraway, MD, and Ruth L. Katz, MD, Cytologica,September Acta Cytomorphology: Follicular lymphoma, Grade 1, is composed predominantly of small cells that are slightly larger than mature lymphocytes. Nuclei have moderately to markedly irregular or wrinkled nuclear contours and inconspicuous nucleoli. Less than 15% of the cell population is composed of large noncleaved cells, which are characterized by large round nuclei with fine chromatin and two to three peripherally placed nucleoli. Follicular lymphoma, Grade 2 shows an admixture of small cleaved and large cleaved cells, and between 16% and 36% of large noncleaved cells. Small cleaved and large cleaved cells are present in relatively equal numbers. Follicular lymphoma, Grade 3, shows predominantly large cells (>37%), with irregular nuclear contours, vesicular chromatin, and inconspicuous nucleoli, as well as variable numbers of large noncleaved cells. Ancillary Studies: Immunophenotyping is positive for B-cell-associated antigens (CD19, CD20, CD22, CD79a) and bcl-2 and bcl-6 proteins. There is variable staining for CD10 and CD23. CD5 and CD43 are negative. Cytogenetic analysis usually shows the t(14;18)(q32;21) translocation resulting in the rearrangement of the bcl-2 gene. This is easily performed by FISH on a single cytospin. Differential Diagnosis: The small-cleaved cells of mantle cell lymphoma stain with CD5, and are not CD10 positive. SLL shows CD19/CD5 co-expression and CD23 positive, and CD10 negative. FL Grade 1 cells co-express CD10 and CD19. CONCLUSION As more pathologists become aware of the potential of FNA diagnosis of lymphoma, when combined with immunophenotyping and adjunctive studies, more of these procedures will be performed. The ultimate beneficiaries of the FNA procedure will be the patients, who, in some instances, may still require a formal surgical excision to subclassify their lymphomas, but will know in advance what to expect, and will have the appropriate staging studies performed without delay. Many patients, however, will not require any further surgical procedure and will be treated according to the FNA diagnosis and the clinical presentation. In the presence of unexplained lymphadenopathy, unresponsive to antibiotics, FNA and ancillary studies of a lymphoid-rich aspirate should become the initial diagnostic procedure. If performed properly with ancillary studies, it will yield valuable diagnostic information that will facilitate appropriate patient management at a lower cost. TABLE I Entities from the updated WHO Classification of Lymphoid Neoplasms that may be amenable to Cytological Diagnosis. B-cell Neoplasms Precursor B-cell neoplasm: Precursor B-lymphoblastic leukemia/lymphoma
10 Mature B-cell Neoplasms B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma Lymphoplasmacytic lymphoma Plasma cell myeloma/plasmacytoma Nodal marginal zone B-cell lymphoma Follicular lymphoma Mantle cell lymphoma Diffuse large B-cell lymphoma Mediastinal large B-cell lymphoma Primary effusion lymphoma Burkitt s lymphoma (includes Burkitt s like ) T- and NK cell neoplasms Precursor T-cell neoplasm: Precursor T-lymphoblastic lymphoma/leukemia (precursor T-cell acute lymphoblastic leukemia) Mature T cell neoplasms Extra-nodal NK/T-cell lymphoma, nasal type Mycosis fungoides Anaplastic large cell lymphoma, T/null-cell, primary cutaneous type Peripheral T-cell lymphoma, not otherwise characterized Angioblastic T-cell lymphoma Anaplastic large cell lymphoma, T/null cell, primary systemic type Hodgkin lymphoma Lymphocyte predominance Hodgkin lymphoma Classical Hodgkin lymphoma (encompasses nodular sclerosis Hodgkin s lymphoma (grades 1 and 2), lymphocyte- rich classical HL and lymphocyte -depleted HL) RFEFERENCES 1. Jemal A, Murray T, Ward E, et al. Cancer statistics CA Cancer J Clin. 2005; 55: Hehn ST, Grogan TM, Miller TP. Utility of fine-needle aspiration as a diagnostic technique in lymphoma. J Clin Oncol. 2004; 22: Mourad WA, Tulbah A, Shoukri M, et al. Primary diagnosis and REAL/WJO classification of non-hodgkin's lymphoma by fine-needle aspiration: cytomorphologic and immunophenotypic approach. Diagn Cytopathol. 2003; 28: Young NA, AL-Saleem TI, Ehya H, Smith MR. Utilization of fine-needle aspiration cytology and flow cytometry in the diagnosis and subclassification of primary and recurrent lymphoma. Cancer. 1998; 84: Young NA, Al-Saleem T. Diagnosis of lymphoma by fine-needle aspiration cytology using the revised European-American classification of lymphoid neoplasms. Cancer. 1999; 87: Meda BA, Buss DH, Woodruff RD, et al. Diagnosis and subclassification of primary and recurrent lymphoma. The usefulness and limitations of combined fine-needle aspiration cytomorphology and flow cytometry. Am J Clin Pathol. 2000; 113: Sigstad E, Dong HP, Davidson B, Berner A, Tierens A, Risberg B. The role of flow cytometric immunophenotyping in improving the diagnostic accuracy in referred fineneedle aspiration specimens. Diagn Cytopathol. 2004; 31:
11 8. Zeppa P, Marino G, Troncone G, et al. Fine-needle cytology and flow cytometry immunophenotyping and subclassification of non-hodgkin lymphoma: a critical review of 307 cases with technical suggestions. Cancer. 2004; 102: Jaffe E, Harris N, Stein H, Vardiman J. Tumors of hematopoietic and lymphoid tissues. In: World Health Organization of classification of tumors. Lyon, France: IARC Press, Jorgensen JL. State of the Art Symposium: flow cytometry in the diagnosis of lymphoproliferative disorders by fine-needle aspiration. Cancer (Cancer Cytopathol). 2005; 105: Caraway NP, Gu J, Lin P, Romaguera JE, Glassman A, Katz RL. The utility of interphase fluorescence in situ hybridization for the detection of the translocation t(11;14)(q13;q32) in the diagnosis of mantle cell lymphoma on fine-needle aspiration specimens. Cancer (Cancer Cytopathol). 2005; 105: Gong Y, Caraway N, Gu J, et al. Evaluation of interphase fluorescence in situ hybridization for the (14:18) (q32;q21) translocation in the diagnosis of follicular lymphoma on fine-needle aspirates. Cancer : Caraway NP. State of the Art Symposium: strategies to diagnose lymphoproliferative disorders by fine-needle aspiration using ancillary studies. Cancer (Cancer Cytopathol). 2005; 105: Katz RL, Patel S, Brooks T. Immunocytochemistry of lymphoproliferative disorders using the Ficoll-Hypaque technique on cytologic specimens. In: Schmidt WA, editor. Cytopathology Annual. Baltimore: Williams & Wilkins, 1993: Mann R, Berard C. Criteria for the cytologic subclassification of follicular lymphomas: a proposed alternative method. Hematol Oncol. 1983; 1: Sun W, Caraway NP, Zhang HZ, Khanna A, Payne LG, Katz RL. Grading follicular lymphoma on fine-needle aspiration specimens. Comparison with proliferative index by DNA image analysis and Ki-67 labeling index. Acta Cytol. 2004; 48: Young NA. State of the Art Symposium: grading follicular lymphoma on fine-needle aspiration specimens: a practical approach. Cancer (Cancer Cytopathol). 18. Goy A, Stewart J, Barkoh BA, et al. State of the Art Symposium: feasibility of gene expression profiling generated from fine-needle aspiration from patients with follicular lymphoma and diffuse large B-cell lymphoma. Cancer (Cancer Cytopathol). 19. Katz RL, Modern Approach to lymphoma Diagnosis by Fine-Needle Aspiration, Restoring respect to a valuable procedure, Cancer Cytopathology, December 25, 2005, Vol 105, Number 6. Please also see Dr. Katz PowerPoint presentation for her further handout information. References 1. Katz RL. Modern Approach to Lymphoma Diagnosis by Fine-Needle Aspiration: Restoring Respect to a Valuable Procedure. Cancer Cytopathology, and , February 2006.
12 2. Jorgensen JL. State of the Art Symposium: Flow Cytometry in the Diagnosis of Lymphoproliferative Disorders by Fine-Needle Aspiration. Cancer Cytopathology, 105(6) December, Caraway NP. Strategies to Diagnose Lymphoproliferative Disorders by Fine- Needle Aspiration by Using Ancillary Studies. Cancer (Cancer Cytopathology) 105(6) December, Young NA, Moriarty AT, Haja JC, Wilbur DC. Fine-Needle Aspiration Biopsy of Lymphoproliferative Disorders Interpretations Based on Morphologic Criteria Alone: Results from the College of American Pathologists Interlaboratory Comparison Program in Nongynecologic Cytopathology. Arch Pathol Lab Med. 130(12): December, 2006.
13 Practical FNA in Lymphoma Diagnosis: What the Clinician wants to Know and How to Get There! USCAP, San Diego, 2007 Ruth L. Katz, M.D. Chief Research Cytopathology, Professor of Pathology, University of Texas M.D. Anderson Cancer Center Houston, Texas
14 What does the treating clinician need to know from the FNA in order to treat? Valuable not Redundant procedure!
15 Indications for Fine Needle Aspiration of Lymphoproliferative Disorders at University of Texas M. D. Anderson Cancer Center Diagnosis To firmly establish relapse and cell type For primary diagnosis of selected cases To rule out transformation of low grade lymphoma To diagnose second primaries, i.e., LCL in patients with previous Hodgkin s disease, new non-lymphoid primaries To obtain tissue for immunophenotyping or FISH To clarify stage of disease To rule out divergent histologies To obtain fresh material for research purposes such as DNA microarrays
16 What the treating physician needs to know and what the Diagnosis should contain Diagnosis of lymphoma, WHO Classification Grade of Lymphoma Immunophenotype Proliferation index? Transformation
17 How to get sufficient cells! Aspiration without suction (French technique) using 25 gauge needle Suction introduces blood! Move needle in rapid iterations up and down 250 times (takes about 90 seconds) Look for creamy white tissue arising in hub of needle (Radiologists use same method) Place tiny drop to make smears (gently), air dried (Diff Quik) and Alcohol fixed Pap smears
18 Tricks of the Trade Flush most of specimen by reattaching syringe with air to needle and flush into RPMI 1640 Carry on aspirating and rinsing needle until a minimum of 10 million cells obtained by Coulter Count, hematocytometer or visual inspection..usually 2-3 passes sufficient Examine smears and triage for ancillary studies based on morphology
19 Establishing a standardized approach to the work up of lymphocyte-rich FNA is Key to Success!
20 Complementary Papanicolaou and Romanowsky stains Classify by WHO classification Immunophenotyping by Cytospin or FCM or both FISH on selected cases
21 MYTH In order to make a diagnosis of lymphoma, the whole lymph node should be excised and examined histologically.
22 Lymphoma With Architecture Follicular center cell Mantle cell (follic/diffuse/mz) Marginal zone

23



24 Follicular Lymphoma

25 Diffuse large Cell Lymphoma
26 CLL/SLL IgH c-myc BL IgH PAX-5 t(9;14) LPL t(8;14) IgH BCL-1 AP12 MLT t(11;14) MZ GC MargZ t(11;18) MCL MALT BCL-2 IgH X BCL-6 t(14;18) FL DLBCL (3;X) P53 INACTIVATION
27 Methods: Cell Count (10 million) Flow Cytometry Immunocytochemistry Labeling Index (Ki-67) Kappa & Lambda B-cell markers T-cell markers CD-19/CD10 CD-19/CD5 CD5/CD20 Cytospins Ficoll-Hypaque density gradient FISH Cytospin DAKO (Ki-67) % of staining 200 cells Specific markers are performed by either FC/IHC or both depending on each case

28

29



30 Pre-Ficoll Hypaque Pleural Fluid, SLL, Plasmacytoid Post-Ficoll Hypaque Pleural Fluid, SLL, Plasmacytoid

31 Ki-67
32 Immunophenotyping General Statements FCM vs. Cytospins High degree of concordance irrespective of method Tailored panel vs. larger battery Spurious or inconclusive results by both methods if necrotic, or large lymphoma cells with fragile cytoplasm Need to interpret results in conjunction with the morphology on smears and the pattern on the flow histogram
33 Problems with Immunophenotyping Flow Cytometry Gating on wrong populations by FCM (miss a small malignant subpopulation, example; Reporting markers on a predominant reactive small lymphocytic subpopulation without noting tight clonal distribution or trailing seen in a benign process Sampling problems, excessive peripheral blood contamination


34 Reactive vs. Lymphoma? Note large cells Kappa lambda
35 Problems in Flow Cytometry Related to Improper Gating R1 Small cells All lymphoid cells regardless of size gated Large cells Net result - looks polyclonal


36 FCM With Correct Gating R4 Gated on larger lymphoid cells Monotypic Lambda tight
37 MONOMORPHOUS POPULATION OF DISASSOCIATED CELLS + LYMPHOGLANDULAR BODIES NON HODGKIN LYMPHOMA SMALL CELLS SMALL LYMPHOCYTIC/PLASMACYTOID IDENTIFY PREDOMINANT CELL TYPE MANTLE CELL, FOLLICULAR LYMPHOMA GRADE1, MARGINAL ZONE, LP HODGKIN S LYMPHOMA MEDIUM SIZED CELLS LYMPHOBLASTIC MANTLE CELL LYMPHOMA, BLASTOID VARIANT BUITT S LYMPHOMA LARGE CELLS LARGE CELL LYMPHOMA IMMUNOBLASTIC LYMPHOMA ANAPLASTIC LARGE CELL LYMPHOMA (Ki-1)
38 WHO CLASSIFICATION B-Cell Neoplasms Precursor B-cell neoplasm: precursor B-lymphoblastic leukemia, lymphoma Peripheral B-cell neoplasma B-cell chronic lymphocytic leukemia, prolymphocytic leukemia, small lymphocytic lymphoma Lymphoplasmacytoid lymphoma, immunocytoma Mantle cell lymphoma Follicle center lymphoma, Grades1,2,3 Marginal zone B-cell lymphoma Extranodal (MALT-type with or without monocytoid B cells) Hairy cell leukemia Plasmacytoma, plasma cell myeloma Diffuse large B-cell lymphoma Burkitt s lymphoma



39 Lymphomas Composed of Small Cells
40 Differential diagnosis of Small Cell Lymphomas SLL/CLL, B or T cell Lymphoplasmacytic lymphoma Mantle Cell lymphoma Marginal zone lymphoma/malt/splenic lymphoma with villous lymphocytes Follicular lymphoma Lymphocyte rich Hodgkin Lymphoma Progressive transformation of Germinal Centers
41 Low Grade B-Cell Lymphoma Small Cells Large Cells Phenotype FISH B-CLL/SLL Round Prolymphocyte CD5+,CD23+, cep 12, p53, LSI13, LAMP1, ATM Paraimmunoblast slg+(k,lambda), CD10-, Co-express CD5/CD19 Mantle Cell Cleaved, None slg+(k,lambda) Lymphoma notched (+- round/oval) CD5+ CD10-/+ t(11;14) CD23- (q13;q32) Co-express CD5/CD19


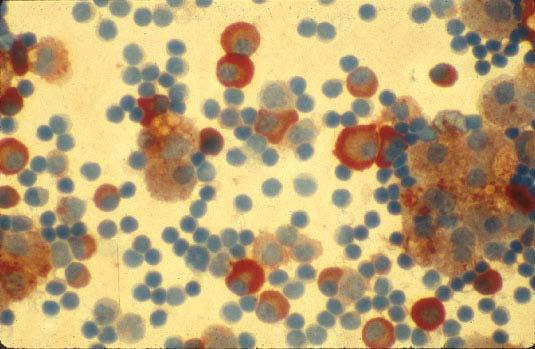
42 Small Lymphocytic Lymphoma SLL, transforming, prolymphocytes and centroblasts

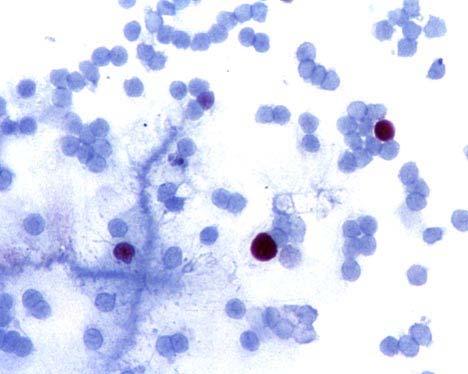
43 SLL, paraimmunoblasts


44 Small Lymphocytic Lymphoma transformed to large cell Lymphoma (Richter s Syndrome) 56 YO woman with history of SLL, and recent posterior chest wall mass





45 Kappa Lambda




46 CD23 CD5 Ki-67 p53

 TRISOMY 12,")

47 Small Lymphocytic Lymphoma transformed to Large Cell Lymphoma (Richter s Syndrome) TRISOMY 12, DEL13q14, DEL13q34 TRISOMY 12, DEL13q14,DEL13q34 DEL P53, POLYSOMYOF ATM
48 Results of FISH Panel for SLL derived from 42 FNAs SLL PANEL GRADE NO:OF CASES 12 13q14 LAMP1 P53 ATM 11q22-23 SLL LOW GRADE 20 3/20 (15%) 8/20 (40%) 1/20 (5%) 3/20 (15%) 8/20 (40%) SLL HIGH GRADE* 22 2/22 (9%) 14/22 (63.6%) 5/22 (22.7%) 11/22 (50%) 8/22 (36.3%) *SLL High grade, Accelerated phase, Richter s syndrome P53 deletion associated with poor survival
49 Mantle Cell Lymphoma: Cytomorphologic Features Monotonous population of small, atypical lymphoid cells Slightly irregular eccentrically placed nuclei, condensed chromatin, absent or small nucleoli, scant pale cytoplasm Prolymphocytes, paraimmunoblasts, and large noncleaved cells are absent
50 Morphologic Variants of MCL Blastic (blastoid, anaplastic, pleomorphic, Centrocytoid-centroblastic) important to diagnose Lymphoblastic-like cells with very dispersed chromatin, usually inconspicuous nucleoli and a high mitotic rare Large cell-like with more prominent nucleoli Predominance of small round lymphocytes


51 Mantle Cell Lymphoma, classic variant

52 Mantle Cell Lymphoma higher proliferation with tingible body macrophages

53 Mantle Cell Lymphoma, pleomorphic

54 Mantle Cell Blastoid Variant

55 Interphase FISH positive for bcl-1 (t 11;14) performed on Cytospin of Mantle Cell Lymphoma showing Multiple Fusion signals ( preferred to Cyclin D1 immunostain) R
56 Marginal Zone vs Mantle Cell Features favoring Mantle cell include: Monomorphic cellular population Prominent nuclear irregularities Scattered pink histiocytes Frequent mitoses Features favoring Marginal Zone include: Polymorphous cell population Frequent plasma cells Centrocyte-like cells with clear cytoplasm Overlapping morphologic features, immunophenotyping is essential
57 FNA Diagnosis: Nodal Marginal Zone Lymphoma Seventy three year old lady with decreased appetite, fatigue, 30 lb weight loss, night sweats, CT scan showed massive splenomegaly and abdominal lymphadenopathy. Previous excisional biopsy of lymph node in inguinal region was non-diagnostic. Outside FNA suggested low grade B cell lymphoma. At MDACC, a periportal lymph node FNA was performed.



58 Well spaced montonous small to intermediate lymphoid cells. FCM showed monoclonal kappa,cd19, CD22, CD11c, CD23 dim, negative CD5 and negative CD10, c/w MZL
 Effacement of")

59 Marginal Zone Lymphoma Spleen, (weight 2390 grams) Effacement of architecture, and replacement by monotonous poplation of both medium and large cells


60 Ki-67, 25% to 50 % Bcl-2 positive cells K Spleen with Marginal Zone Lymphoma, and i focal large cell transformation, increased - Ki-67 labeling index 6

61 Follow up: Patient developed a large right pleural effusion, hypotension, and renal failure. Pleural Fluid, Large B cell lymphoma transformed from MZL


62 Ki67, 50% Monotypic kappa Pleural fluid, Large cell lymphoma, transformed from MZL. Patient expired due to lymphoma.
63 Differential Diagnosis of a Polymorphous Mixed Cell Population Reactive Hyperplasia Lymphoma MZL / MALT Follicular lymphoma, grade 2 Peripheral T-Cell lymphoma Immunocytoma,(transfor med SLL plasmacytoid)


64 Reactive Lymphoid Hyperplasia, spectrum of lymphoid cells Reactive Lymphoid Hyperplasia Mitosis and Apoptosis

65 Follicular Lymphoma, grade 2, admixture of large centroblasts and smaller centrocytic cells

66 Follicular Lymphoma versus reactive hyperplasia? Reactive Hyperplasia:Germinal center cells, and apoptosis with tingible body macrophages X40
67 Reactive Hyperplasia Kappa Lambda CD3 Ki67, 90% Here we rely on cytospin immunophenotyping to resolve the problem advantage of morphology together with phenotyping and Ki-67


68 Florid Reactive Hyperplasia..Pitfall!!
69 Reactive Hyperplasia: Polymorphous infiltrate: small round, small cleaved, small and large non-cleaved Plasmacytoid lymphocytes, immunoblasts, tingible body macrophages Florid immunoblastic reaction may confuse with large cell lymphoma Apoptosis Frequently high Ki-67 Polyclonal, lacks CD10
70 Follicular Lymphoma, Approach to Diagnosis by FNA
71 FOLLICULAR LYMPHOMA Follicular Lymphoma most prevalent subtype of NHL in the Western Hemisphere, is very frequently aspirated in retroperitoneum A B cell neoplasm compared of a mixture of cleaved follicular center cells (centrocytes) and large non-cleaved follicular center cells (centroblasts). FL may have a pure follicular pattern or it may have a partial follicular and diffuse pattern on histology WHO classification grades FL from 1-3 to reflect the reality of a cytologic continuum Grade 3 lymphomas are associated with poorer survival compared to grade 1 and 2, if treated with regimens not containing anthracyclines
72 Grading of Follicular Lymphoma
73 Follicular Lymphoma: Grading on histology according to WHO classification Grading Grade 1 Grade 2 Grade 3 Definition 0-5 centroblasts per hpf* 6-15 centroblasts per hpf* >15 centroblasts per hpf* 3a Centrocytes present 3b Solid sheets of centroblasts
74 Follicular Lymphoma Grading as Used in Cytopathology* Groups Centroblast cell count (%) Grade 1 (n =31) 9.7 ( ) Grade 2 (n = 46) 24.7 ( ) * Grade 3 (n = 10) 48.3 ( ) * # * = p < 0.05 vs. grade 1 group # = p < 0.05 vs grade 2 group +Grading is based on centroblasts within follicles, Easier to perform on Pap smears


75 Pap DQ FL grade 1 Centroblast count within follicles, 10% Ki-67


76 Pap DQ FL grade 2 Centroblast count within follicles 25% Ki-67



77 Pap DQ FL grade 3a Ki-67 Centroblast count within follicles >50%, Note residual centrocytes


78 >90% centroblasts within follicles,and forming sheets FL grade 3b




79 Follicular Lymphoma, Grade 3, Transformed from Grade 1 FL Diff Quik Pap Kappa Ki-67 80%


80 Ki-67 = 80.00% PI = 8.10%, tetraploid,cells %>5c = 46.0% Transformed Follicular Lymphoma Bcl - 6 CD79a
81 The Distribution of Ki67 (%) by Grade of Follicular Lymphoma. A Clinical Outcome Study of 57 Patients (40/57 relapsed FL) Ki67 (%) Follicular Lymphoma N Median (range) Grade (2-26) Grade (8-25) Grade (5-90) Transformed (25-90) SD (P-value < ) between combined grades 1 and 2, and grade3 and grade 3 transformed. Cut off between LG (1 and 2) and HG (3 inc TL) is 25% No SD betweenfl1 and FL2 by Ki67.
82 Survival Probability Ki-67 <=40 (2/33) Ki-67 > 40 (9/18) p-value = Kaplan-Meir Estimate for Overall Survival by Ki-67 (N=51), using >/< 40% cut-off Time (years) Survival Probability p =0.06 PI <= 2.5 (4/36) PI > 2.5 (7/20) p-value = 0.06
83 It is possible to determine the grade of FL on an FNA by determining the percentage of centroblasts within the follicular structures. This should be done after clonality has been established by FCM or immunocytochemistry.
84 FNA Morphology+ Immuno (Flow/ICC) + Labeling Index and grading WHO Cytologic Diagnoses = Histologic Diagnoses
85 When do we request a biopsy? Insufficient numbers of cells to do immunophenotyping New cases of lymphoma where tissue has never been obtained, is easy to obtain and diagnosis by FNA is unclear Composite lymphoma (MZL lymphoma) or when architecture is important for treatment such as mantle zone lymphoma For classifying Hodgkin Lymphoma For unusual benign lymphadenopathies, such as Castleman s disease when excision may be curative When diagnosis is not straight forward or does not fit clinical history or presentation For some suspected low grade T cell lymphomas where gene rearrangement studies are equivocal
86 Using Multiparameter Testing on FNA, Will Enable The Treating Physician To Have: Reasonable approach to first evaluation of lymphadenopathy Can be used confirm recurrent disease in patients with lymphoma May be used as definitive diagnosis particularly when contraindication to biopsy such as palliative therapy in a compromised patient Access to sites such as the retroperitoneum and mediastinum without resorting to open biopsy
87 Conclusions Collection technique and on-site documentation of adequacy (quantity and quality) optimizes FNA Dx outcome Case by case allocation of cytologic material for ancillary studies remains critical for successful cytologic evaluation Above all, understand the limitations of the technique, and be an advocate for the patient rather than for a particular technique of diagnosis!!
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs. Nancy P. Caraway, M.D.
 A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms
 Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms Rana S. Hoda FINE NEEDLE ASPIRATION Introduction Fine needle aspiration (FNA) is a well-established
Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms Rana S. Hoda FINE NEEDLE ASPIRATION Introduction Fine needle aspiration (FNA) is a well-established
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Lymph node cytopathology : A practical approach to lymphoproliferative disorders
 Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
Unknown Case 6. Ann T. Moriarty, MD
 Unknown Case 6 Ann T. Moriarty, MD Unknown Case 6 61 year old male with an enlarged cervical lymph node. He has a history of lung carcinoma, renal cell carcinoma and lymphoma. Case 6 Image 1: Fine needle
Unknown Case 6 Ann T. Moriarty, MD Unknown Case 6 61 year old male with an enlarged cervical lymph node. He has a history of lung carcinoma, renal cell carcinoma and lymphoma. Case 6 Image 1: Fine needle
Abstract. Anatomic Pathology / DIAGNOSIS AND SUBCLASSIFICATION OF PRIMARY AND RECURRENT LYMPHOMA
 Anatomic Pathology / DIAGNOSIS AND SUBCLASSIFICATION OF PRIMARY AND RECURRENT LYMPHOMA Diagnosis and Subclassification of Primary and Recurrent Lymphoma The Usefulness and Limitations of Combined Fine-Needle
Anatomic Pathology / DIAGNOSIS AND SUBCLASSIFICATION OF PRIMARY AND RECURRENT LYMPHOMA Diagnosis and Subclassification of Primary and Recurrent Lymphoma The Usefulness and Limitations of Combined Fine-Needle
Diagnosis of lymphoid neoplasms has been
 Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Fine-Needle Aspiration Cytology in the Diagnosis of Lymphoma The Next Step
 Fine-Needle Aspiration Cytology in the Diagnosis of Lymphoma The Next Step Linda M. Sandhaus, MD Since 985, almost 2 articles have been published in the medical literature on the subject of fine-needle
Fine-Needle Aspiration Cytology in the Diagnosis of Lymphoma The Next Step Linda M. Sandhaus, MD Since 985, almost 2 articles have been published in the medical literature on the subject of fine-needle
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
PhenoPath. Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA
 PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Successful flow cytometric immunophenotyping of body fluid specimens
 Successful flow cytometric immunophenotyping of body fluid specimens Fiona E. Craig, MD Division of Hematopathology Mayo Clinic Arizona 2017 MFMER slide-1 Financial disclosure No conflicts 2017 MFMER slide-2
Successful flow cytometric immunophenotyping of body fluid specimens Fiona E. Craig, MD Division of Hematopathology Mayo Clinic Arizona 2017 MFMER slide-1 Financial disclosure No conflicts 2017 MFMER slide-2
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Tres
 Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Classifications of lymphomas
 Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
, , 2011 HODGKIN LYMPHOMA
 European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Parts 2 and 3
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
GENETIC MARKERS IN LYMPHOMA a practical overview. P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute
 GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
9/28/2017. Follicular Lymphoma and Nodal Marginal Zone Lymphoma. Follicular Lymphoma Definition. Low-Grade B-Cell Lymphomas in WHO Classification
 and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
11/8/2018 DISCLOSURES. I have NO Conflicts of Interest to Disclose. UTILTY OF DETECTING PATTERNS
 Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients
 Hematopathology / LYMPHOMAS WITH IGM PARAPROTEIN Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients Pei Lin, MD, 1 Suyang Hao, MD, 1* Beverly C. Handy, MD, 2 Carlos E. Bueso-Ramos,
Hematopathology / LYMPHOMAS WITH IGM PARAPROTEIN Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients Pei Lin, MD, 1 Suyang Hao, MD, 1* Beverly C. Handy, MD, 2 Carlos E. Bueso-Ramos,
I n the past 10 years, fine needle aspiration (FNA) cytology
 cytology") 821 ORIGINAL ARTICLE Fine needle aspiration cytology in the diagnosis of uncommon types of lymphoma F Mayall, A Darlington, B Harrison... See end of article for authors affiliations... Correspondence to:
821 ORIGINAL ARTICLE Fine needle aspiration cytology in the diagnosis of uncommon types of lymphoma F Mayall, A Darlington, B Harrison... See end of article for authors affiliations... Correspondence to:
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
During past decades, because of the lack of knowledge
 Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Independent Diagnostic Accuracy of Flow Cytometry Obtained From Fine-Needle Aspirates A 10-Year Experience With 451 Cases
 Hematopathology / Diagnostic Accuracy of Flow Cytometry Independent Diagnostic Accuracy of Flow Cytometry Obtained From Fine-Needle Aspirates A 10-Year Experience With 451 Cases Erica C. Savage, MD, 1
Hematopathology / Diagnostic Accuracy of Flow Cytometry Independent Diagnostic Accuracy of Flow Cytometry Obtained From Fine-Needle Aspirates A 10-Year Experience With 451 Cases Erica C. Savage, MD, 1
Methods used to diagnose lymphomas
 Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Non-Hodgkin Lymphoma. Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract.
 Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Mimics of Lymphoma in Routine Biopsies. I have nothing to disclose regarding the information to be reported in this talk.
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
2010 Hematopoietic and Lymphoid ICD-O Codes - Alphabetical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
2012 Hematopoietic and Lymphoid ICD-O Codes - Numerical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Approach to Core Biopsy Specimens
 BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
Mimics of Lymphoma in Routine Biopsies. Mixed follicular and paracortical hyperplasia. Types of Lymphoid Hyperplasia
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Critical Analysis and Diagnostic Usefulness of Limited Immunophenotyping of B-Cell Non-Hodgkin Lymphomas by Flow Cytometry
 Hematopathology / FLOW CYTOMETRIC IMMUNOPHENOTYPING IN B-CELL NON-HODGKIN LYMPHOMA Critical Analysis and Diagnostic Usefulness of Limited Immunophenotyping of B-Cell Non-Hodgkin Lymphomas by Flow Cytometry
Hematopathology / FLOW CYTOMETRIC IMMUNOPHENOTYPING IN B-CELL NON-HODGKIN LYMPHOMA Critical Analysis and Diagnostic Usefulness of Limited Immunophenotyping of B-Cell Non-Hodgkin Lymphomas by Flow Cytometry
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Hematopathology Lab. Third year medical students
 Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Solomon Graf, MD February 22, 2013
 Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
Solomon Graf, MD February 22, 2013 Case Review of FL pathology, prognosis Grading of FL Grade 3 disease High proliferative index in grade 1/2 disease Pediatric FL Future of FL classification 57 yo man
BACKGROUND AND OBJECTIVE:
 Fine needle aspiration cytology in the evaluation of lymphoid lesions: a retrospective study of the utility of flow cytometry in conjunction with morphology Emad M. Said Raddaoui, a Lubna Sayage-Rabie,
Fine needle aspiration cytology in the evaluation of lymphoid lesions: a retrospective study of the utility of flow cytometry in conjunction with morphology Emad M. Said Raddaoui, a Lubna Sayage-Rabie,
Integrated Hematopathology. Morphology and FCI with IHC
 Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
Dispersed Cell Population & Lymphoglandular Bodies: Features of lymphoid aspirates FNA OF LYMPH NODES OF THE HEAD AND NECK
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF LYMPH NODES OF THE HEAD AND
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF LYMPH NODES OF THE HEAD AND
Composite mantle cell and follicular lymphoma. A case report
 Human Pathology (2009) 40, 259 263 www.elsevier.com/locate/humpath Case study Composite mantle cell and follicular lymphoma. A case report Raquel B. Ilgenfritz MD a,, Agnès Le Tourneau MD a, Michel Arborio
Human Pathology (2009) 40, 259 263 www.elsevier.com/locate/humpath Case study Composite mantle cell and follicular lymphoma. A case report Raquel B. Ilgenfritz MD a,, Agnès Le Tourneau MD a, Michel Arborio
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Participants Identification No. % Evaluation
 BMD-02 Cell Identification Participants Identification No. % Evaluation Erythrocyte precursor, normal 228 95.8 Educational Erythrocyte, normal 7 3.0 Educational Erythrocyte precursor with megaloblastic
BMD-02 Cell Identification Participants Identification No. % Evaluation Erythrocyte precursor, normal 228 95.8 Educational Erythrocyte, normal 7 3.0 Educational Erythrocyte precursor with megaloblastic
Lymphocytoma Cutis. Cynthia M. Magro MD. Director of Dermatopathology Weill Medical College of Cornell University New York, New York
 Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
Clinicopathologic features of 112 cases with mantle cell lymphoma
 Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Case Report Parotid gland follicular lymphoma lacking both cytoplasmic and surface light chains: a rare case
 Int J Clin Exp Pathol 2014;7(10):7100-7104 www.ijcep.com /ISSN:1936-2625/IJCEP0001717 Case Report Parotid gland follicular lymphoma lacking both cytoplasmic and surface light chains: a rare case Jenny
Int J Clin Exp Pathol 2014;7(10):7100-7104 www.ijcep.com /ISSN:1936-2625/IJCEP0001717 Case Report Parotid gland follicular lymphoma lacking both cytoplasmic and surface light chains: a rare case Jenny
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD
 HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD") HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
Low-grade B-cell lymphoma
 Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Pathology of the Lymphoid System
 Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
Almost any suspected tumor can be aspirated easily and safely. Some masses are more risky to aspirate including:
 DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
CCND1-IGH Fusion-Amplification and MYC Copy Number Gain in a Case of Pleomorphic Variant Mantle Cell Lymphoma
 AJCP /CASE REPORT CCND1-IGH Fusion-Amplification and MYC Copy Number Gain in a Case of Pleomorphic Variant Mantle Cell Lymphoma Yuan Miao, MD, 1,2 Pei Lin, MD, 1 Wei Wang, MD, 1 L. Jeffrey Medeiros, MD,
AJCP /CASE REPORT CCND1-IGH Fusion-Amplification and MYC Copy Number Gain in a Case of Pleomorphic Variant Mantle Cell Lymphoma Yuan Miao, MD, 1,2 Pei Lin, MD, 1 Wei Wang, MD, 1 L. Jeffrey Medeiros, MD,
Flow cytometric analysis of B-cell lymphoproliferative disorders
 Flow cytometric analysis of B-cell lymphoproliferative disorders David M. Dorfman, M.D., Ph.D. Department of Pathology Brigham and Women s Hospital and Harvard Medical School Boston, MA Objectives Review
Flow cytometric analysis of B-cell lymphoproliferative disorders David M. Dorfman, M.D., Ph.D. Department of Pathology Brigham and Women s Hospital and Harvard Medical School Boston, MA Objectives Review
5/16/2018 HEMATOPATHOLOGY FOR CYTOPATHOLOGISTS HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS I HAVE NOTHING TO C DISCLOSE
 HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium I HAVE NOTHING TO C DISCLOSE Kathryn
HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium I HAVE NOTHING TO C DISCLOSE Kathryn
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
The Value of Transformed Lymphocyte Count in Subclassification of Non-Hodgkin's Lymphoma by Fine-Needle Aspiration
 HEMATOPATHOLOGY Original Article The Value of Transformed Lymphocyte Count in Subclassification of Non-Hodgkin's Lymphoma by Fine-Needle Aspiration NANCY A. YOUNG, MD, 1 TAHSEEN I. AL-SALEEM, MD, 1 ZINA
HEMATOPATHOLOGY Original Article The Value of Transformed Lymphocyte Count in Subclassification of Non-Hodgkin's Lymphoma by Fine-Needle Aspiration NANCY A. YOUNG, MD, 1 TAHSEEN I. AL-SALEEM, MD, 1 ZINA
Lack of Surface Immunoglobulin Light Chain Expression by Flow Cytometric Immunophenotyping Can Help Diagnose Peripheral B-Cell Lymphoma
 Hematopathology / SURFACE IMMUNOGLOBULIN LIGHT CHAIN NEGATIVE PERIPHERAL B-CELL LYMPHOMA Lack of Surface Immunoglobulin Light Chain Expression by Flow Cytometric Immunophenotyping Can Help Diagnose Peripheral
Hematopathology / SURFACE IMMUNOGLOBULIN LIGHT CHAIN NEGATIVE PERIPHERAL B-CELL LYMPHOMA Lack of Surface Immunoglobulin Light Chain Expression by Flow Cytometric Immunophenotyping Can Help Diagnose Peripheral
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
Low-Grade B-Cell Lymphomas in WHO Classification. Follicular Lymphoma Definition. Follicular Lymphoma Clinical Features 11/7/2017 DISCLOSURES
 Low-Grade B-Cell Lymphomas in WHO Classification DISCLOSURES I do not have anything to disclose Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6 % Small lymphocytic lymphoma/cll
Low-Grade B-Cell Lymphomas in WHO Classification DISCLOSURES I do not have anything to disclose Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6 % Small lymphocytic lymphoma/cll
Fine needle aspiration cytology in the investigation of non-hodgkin s lymphoma
 J Clin Pathol 1998;51:189 196 189 Papers Department of Cytopathology, Aberdeen Royal Infirmary, Aberdeen, UK MDJeVers M McKean Department of Immunopathology, Aberdeen Royal Infirmary J Milton R Herriot
J Clin Pathol 1998;51:189 196 189 Papers Department of Cytopathology, Aberdeen Royal Infirmary, Aberdeen, UK MDJeVers M McKean Department of Immunopathology, Aberdeen Royal Infirmary J Milton R Herriot
Follicular Lymphoma: the WHO
 Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
CD5 Positive Follicular Lymphomas- A Diagnostic Dilemma in a Resource Restricted Laboratory Setting
 Original Article DOI: 10.21276/APALM.1364 CD5 Positive Follicular Lymphomas- A Diagnostic Dilemma in a Resource Restricted Laboratory Setting Sakthi Sankari S 1 *, Arjunan A 2, Bhuvaneswari M.G. 2, Sindhuja
Original Article DOI: 10.21276/APALM.1364 CD5 Positive Follicular Lymphomas- A Diagnostic Dilemma in a Resource Restricted Laboratory Setting Sakthi Sankari S 1 *, Arjunan A 2, Bhuvaneswari M.G. 2, Sindhuja
Lymphoma and Pseudolymphoma
 Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
Leukemic Phase of Mantle Cell Lymphoma, Blastoid Variant
 Hematopathology / LEUKEMIC BLASTOID MANTLE CELL LYMPHOMA Leukemic Phase of Mantle Cell Lymphoma, Blastoid Variant Timothy P. Singleton, MD, Margaret M. Anderson, MD, Charles W. Ross, MD, and Bertram Schnitzer,
Hematopathology / LEUKEMIC BLASTOID MANTLE CELL LYMPHOMA Leukemic Phase of Mantle Cell Lymphoma, Blastoid Variant Timothy P. Singleton, MD, Margaret M. Anderson, MD, Charles W. Ross, MD, and Bertram Schnitzer,