Section of Endcrinology, Department of Medicine, Rush University Medical Center, Chicago, IL 60612, USA 2
|
|
|
- James Mitchell
- 5 years ago
- Views:
Transcription
1 Case Reports in Endocrinology Volume 2011, Article ID , 5 pages doi: /2011/ Case Report Life-Threatening Hypocalcemia following Subtotal Parathyroidectomy in a Patient with Renal Failure and Previous Roux-en-Y Gastric Bypass Surgery Betsy Palal, 1 Marvin Sinsakul, 2 and Sirimon Reutrakul 1 1 Section of Endcrinology, Department of Medicine, Rush University Medical Center, Chicago, IL 60612, USA 2 Section of Nephrology, Department of Medicine, Rush University Medical Center, Chicago, IL 60612, USA Correspondence should be addressed to Sirimon Reutrakul, sirimon reutrakul@rush.edu Received 10 September 2011; Accepted 2 October 2011 Academic Editors: L. Meyer and N. Sakane Copyright 2011 Betsy Palal et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Roux-en-Y gastric bypass (RYGB) can result in calcium and vitamin D deficiency. Parathyroid surgery carries the risk of immediate and long-term hypocalcemia. Methods and Results. We describe a 54-year-old woman with history of end-stage renal disease and gastric bypass surgery who developed calciphylaxis requiring a 3.5 -gland parathyroidectomy. Seven weeks later, she presented with weakness, perioral numbness, leg cramps, a positive Chvostek s sign, hypotension, prolonged QT-interval, and serum calcium of 5.4 mg/dl. Oral and intravenous calcium, calcitriol, and high calcium bath hemodialysis were given. She required 18 days of intravenous calcium and an outpatient maintenance regimen of calcitriol 6 mcg/day, calcium carbonate 8 grams/day, calcium citrate 1.2 grams/day, and ergocalciferol 50,000 IU/week. Conclusion. The patient s life-threatening prolonged hypocalcemia and large requirements of calcium and calcitriol were due to a combination of malabsorption, hypoparathyroidism, and renal failure. Special considerations should be given to bariatric surgery patients undergoing neck exploration. 1. Introduction The prevalence of obesity in the United States has drastically increased over the last several decades. The percentage of adults who are obese (BMI 30) increased from 15.3% in 1995 to 23.9% in 2005, with 4.8% considered to be morbidly obese (BMI 40) [1]. The use of bariatric surgery, first introduced in 1950, has increased dramatically as a way to treat this problem, from 16,000 procedures in 1997 to more than 100,000 in 2003 [2]. The surgery resulted in long-term weight loss and reduction in total mortality especially from diabetes, cancer, and heart disease [3, 4]. Roux-en-Y gastric bypass (RYBG) and biliopancreatic diversion (BPD) are the two commonly performed operations. Because of the malabsorptive nature of the procedures, they can result in protein malnutrition as well as vitamin and mineral deficiency (calcium and vitamin D, iron, folate, thiamine, vitamin B 12, and vitamin A) [5]. Specifically, these procedures bypass the duodenum and jejunum, which are the preferential sites for calcium absorption. Overall, 10 25% of patients develop calcium deficiency by 2 yr and 25 48% by 4 yr; 17 52% of patients develop a vitamin D deficiency by 2 yr and 50 63% by 4 yr [5 11]. As a result, the body upregulates parathyroid hormone (PTH; secondary hyperparathyroidism), causing increased production of vitamin D and calcium resorption from the bone and helping to maintain calcium level. These patients, therefore, need regular monitoring and supplementations of calcium and vitamin D. Secondary hyperparathyroidism commonly develops in chronic renal failure. Elevated PTH is a result of hyperphosphatemia, due to reduction in phosphate excretion, and hypocalcemia, due to impaired conversion of 25-hydroxy vitamin D to the active form 1,25-dihydroxy vitamin D and decreased intestinal absorption of calcium. This is usually medically managed by phosphate binders, vitamin D analogues, and calcimimetics such as cinacalcet to reduce serum phosphate and PTH levels. However, about 1-2% of patients require parathyroidectomy each year due to failure of medical management or the development of calciphylaxis
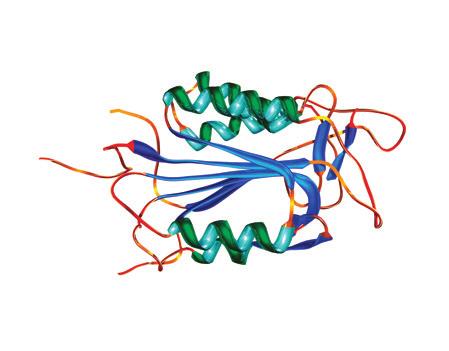
2 2 Case Reports in Endocrinology Serum calcium (mg/dl) Day 3 CaCO g/day Calcitriol 1.5 mcg/day Calcium infusion 0.8 g/h Drisdol 50,000 IU/day 3days Day 1 CaCO 3 6 g/day Calcitriol 0.75 mcg/day Calcium infusion 0.8 g/h Day 5 CaCO 3 8 g/day Calcitriol 2 mcg/day Calcium infusion 0.4 g/h Day 12 Calcium citrate 1.2 g/day Calcitriol 4 mcg/day Calcium infusion g/h Teriparatide 20 mcg/day 6.8 Day 11 Calcitriol 4 mcg/day Calcium infusion 0.2 g/h 7.1 Day 18 Calcium citrate 1.2 g/day Calcitriol 6 mcg/day Teriparatide 20 mcg/day Day 14 Calcium citrate 1.2 g/day Calcitriol 4 mcg/day Calcium infusion g/h Teriparatide 20 mcg/day 5 Hospital days Figure 1: Calcium levels and treatment during the hospital course. [12]. This occurs when the levels of calcium and phosphate in the blood exceed their solubility level, leading to calciumphosphate deposits in small- and medium-sized arteries causing ischemia and necrosis of skin and soft tissue. Calciphylaxis is associated with high mortality of 60 80% [13, 14] due to infection and ulcerations. Parathyroid surgery carries the risk of immediate and long-term hypocalcemia. This can become more complicated when parathyroidectomy is performed in patients with multiple comorbidities that affect calcium and vitamin D metabolism. Here, we describe a patient who had undergone an RYGB, and later developed end-stage renal disease (ESRD). She underwent a 3.5-gland parathyroidectomy for a calciphylaxis of the breast and developed life-threatening prolonged hypocalcemia. 2. Materials and Methods We reviewed the patient s clinical and laboratory findings, and clinical course from her medical record. Literature reviewed and possible mechanisms are provided. 3. Results A 54-year-old female with significant past medical history of ESRD on hemodialysis underwent a 3.5-gland parathyroidectomy due to severe calciphylaxis of her breast which required multiple debridements. She had a history of RYGB five years prior due to morbid obesity (BMI 71 kg/m 2 ). Prior to the parathyroidectomy, her calcium levels were mg/dl (reference range ), phosphorus 4.7 mg/dl (reference range ), magnesium mg/dl (reference range ), PTH 1971 pg/ml (reference range 22 60), and serum creatinine 5.6 mg/dl (reference range ). Vitamin D status was not known. She had been treated with sevelamer and cinacalcet in the attempt to control secondary hyperparathyroidism. During surgery, after all four parathyroid glands were identified, intraoperative PTH (iopth) was 2466 pg/ml. A 3.5-gland parathyroidectomy was performed. Ten minutes later, an iopth was 119 pg/ml. This was deemed to be satisfactory. Cryopreservation of parathyroid tissue was not performed. On postoperative day 1, calcium was 7.0 mg/dl and ionized calcium was 0.7 mmol/l (reference range ) and PTH was 49 pg/ml. She was discharged on calcitriol 0.5 mcg/day and calcium carbonate 9 grams/day. Pathology revealed hyperplastic parathyroid glands. Seven weeks later she presented to the emergency department with complaints of generalized weakness, perioral numbness, and leg cramps for several days. Her physical examination was remarkable for BP 140/70 mmhg, a positive Chvostek s sign and a healing right breast ulcer. An EKG revealed a prolonged QT-interval. Her calcium level was 5.4 mg/dl with a PTH level of 87 pg/ml, phosphorus 3.1 mg/dl (reference range ), and magnesium 2.1 mg/dl (reference range ). She was treated with oral calcium carbonate 6 grams/day, in divided doses, calcitriol 0.75 mcg/day, and a continuous calcium gluconate infusion. Overnight, the patient developed hypotension (BP 60/40 mmhg) requiring a transfer to the intensive care unit and an initiation of vasopressor. The detail of her hospital course is shown in Figure 1.
3 Case Reports in Endocrinology 3 After 48 hours, calcium increased to 8.3 mg/dl, with an improvement of blood pressure and the vasopressor was stopped. Hemodialysis with a high calcium bath was performed. When attempting to hold the calcium infusion, her calcium dramatically dropped to 5.0 mg/dl, along with intermittent episodes of hypotension, requiring the infusion to be restarted. Calcitriol was increase to 1.5 mcg/day on hospital day 3. On hospital day 4, her oral calcium carbonate was increased to 7.5 grams/day and ergocalciferol 50,000 IU weekly was added for a 25-hydroxy vitamin D level of 16 ng/ml (reference range ). On hospital day 11, calcium and calcitriol supplementations were changed to suspension and solution forms due to concern of the patients inability to absorb the tablet form. Multiple attempts to wean off the calcium infusion were unsuccessful. On hospital day 12, teriparatide 20 mcg/day was started. Eventually, her calcium level and blood pressure became more stabilized and she was transferred from the ICU to the medical floor after two weeks. She required a total of 18 days of continuous calcium infusion. The patient was discharged on calcium carbonate suspension 8 grams/day, calcium citrate suspension 1.2 grams/day, calcitriol solution 6 mcg/day, ergocalciferol 50,000 IU weekly, and teriparatide 20 mcg/day. She continued on a high calcium bath dialysis. At her follow-up visit 4 weeks later her calcium was 9.7 mg/dl, and teriparatide was stopped. Her calcium levels remained stable between 8.4 and 9.0 mg/dl on the same regimen nine months later. Phosphorus levels were mg/dl, magnesium mg/dl, PTH pg/ml, and 25- hydroxy vitamin D ng/ml during the same period. 4. Discussion This case demonstrates the risk of severe hypocalcemia in bariatric patients who develop hypoparathyroidism. To our knowledge, this is the first reported case of life-threatening prolonged hypocalcemia after parathyroidectomy in the setting of previous RYGB and ESRD. This was due to a combination of malabsorption, hypoparathyroidism, ESRD, and hungry bone syndrome. While any of these four etiologies can cause hypocalcemia, our case is the first to describe these combinations and highlights the importance of different body systems in regulating calcium levels. Hypocalcemia and vitamin D deficiency after a malabsorptive bariatric surgery are due to multiple reasons. The duodenum and jejunum, the preferential sites for calcium absorption, are bypassed. In the setting of low calcium intake, the duodenum can absorb % of calcium by a vitamin D-dependent transcellular active transport. When this is bypassed, the calcium absorption takes place through the less efficient paracellular mechanism [15]. Partial gastrectomy reduces gastric acidity, resulting in an impaired absorption of calcium salts. Malabsorption of fat-soluble vitamins due to poor mixing of bile salts decreases the amount of vitamin D available and contributes further to the decreased calcium absorption [11]. In addition, gastric bypass patients consume only about 50% of the recommended daily requirements of vitamin D unless taking regular supplement, and many cannot tolerate calcium-rich diets [16, 17]. Therefore, these patients should have calcium and vitamin D, as well as phosphorus, PTH, and alkaline phosphatase levels done preoperatively and every 6 months thereafter [5]. Yearly bone mineral density measurement is recommended until stable. Daily calcium grams/day, preferably calcium citrate with vitamin D should be given [5]. Vitamin D supplementation can be provided with ergocalciferol, 50,000 IU one to three times weekly. Therapy should be adjusted based on serum markers and measures of bone density. Renal failure-related secondary hyperparathyroidism occurs in as many as 90% of patients by the time hemodialysis is initiated [18], and is usually medically managed. When medical management fails (persistently elevated PTH > 800 pg/ml, hyperphosphatemia with calcium phosphorus>70, hypercalciuria, hypercalcemia, pathologic fractures, ectopic soft tissue or vascular calcifications, or calciphylaxis), parathyroidectomy should be considered [19]. The recent surgery rate in 2007, however, has decreased from previously reported in 2002, likely due to improved medical treatment and guideline publication [20]. Preoperative localization studies are not always routinely performed, with the exception of reoperation, due to the low sensitivity of ultrasound and 99m Tc-sestamibi scintigraphy in patients with multiplegland disease as seen in renal failure. In addition, the ability of imaging techniques to identify ectopic parathyroid is limited in this circumstance. Therefore, bilateral neck exploration is the standard of care for these patients [19]. Three different surgical approaches have been described, including subtotal parathyroidectomy (removal of 3.5 glands leaving a remnant in situ), total parathyroidectomy with autotransplantation, and total parathyroidectomy without autotransplantation. The cure rate was higher in patients after total parathyroidectomy with autotransplantation than subtotal parathyroidectomy, 100% versus 90% [21, 22]. More recently, total parathyroidectomy without autotransplantation has been proposed and shown to be associated with a lower rate of recurrence than those with autotransplantation [23]. When performed, autotransplantation in the forearm is preferred for the convenience of reoperation in case of the disease recurrence [24, 25]. Routine cryopreservation is advocated by some although the overall utility rate of cryopreserved parathyroid tissue is estimated at 1.6%, with significantly decreased tissue viability after 24 months [19, 26, 27]. Data on the utility of iopth in these patients is limited and difficult to evaluate [28]. Different criteria have been shown to predict postoperative cure in different studies, such as a 50% decrease from baseline at 10 minutes [29], >90% decrease at 15 minutes [30], and PTH < 45 pg/ml at 30 minutes [31]. While many patients with ESRD do well after total or subtotal parathyroidectomy, with 15 30% experiencing transient hypocalcemia and rarely long-term hypocalcemia [19, 32], this was not the case in our patient. Due to calcium and vitamin D malabsorption associated with RYGB, her PTH played a pivotal role in maintaining her calcium level preoperatively. Subsequent parathyroidectomy resulted in severe hypocalcemia requiring large doses of calcium and vitamin D supplement. The inability to convert 25-hydroxy
4 4 Case Reports in Endocrinology vitamin D to 1,25-dihydroxy vitamin D due to renal failure made it more difficult to normalize her calcium levels. While her initial large calcium and calcitriol requirement could be due to a hungry bone syndrome, this was unchanged during a follow-up period indicating an ongoing malabsorption. Our literature review found few reported cases of severe hypocalcemia, requiring prolonged intravenous calcium infusion and large doses of oral calcium and vitamin D supplement, in RGBY or BPD patients following thyroid surgery complicated by hypoparathyroidism, although none had ESRD [33 36]. Our patient received a short trial of teriparatide injection after difficulty weaning the calcium infusion, given previous reports in patients with primary hypoparathyroidism [37, 38]. It was difficult to determine the effectiveness of this treatment as there were simultaneous adjustments in calcium and vitamin D doses. Delayed autotansplantation might have been considered had the parathyroid tissue been cryopreserved. During outpatient followup, the patient continued to have serum calcium, phosphate, magnesium, and vitamin D levels monitored regularly as recommended in hypoparathyroidism patients [39]. Routine monitoring of urinary calcium and prevention of hypercalciuria is usually recommended, except our patient was anuric. Thyroid and parathyroid surgery, as well as bariatric surgery are common procedures. Physicians should be aware of an increased risk of severe hypocalcemia in gastric bypass patients who subsequently develop hypoparathyroidism and the requirement of larger than usual doses of calcium and calcitriol supplementations. Precautions should be taken when these patients undergo neck exploration. Optimization of calcium and vitamin D repletion prior to surgery, as well as aggressive supplement immediately postoperatively, may be helpful. Disclosure All authors have nothing to disclose. The abstract of this paper was presented as a poster at the Endocrine Society s 93rd Annual Meeting & Expo., Boston, MA, June, Acknowledgments The authors would like to thank Dr. Katherine B. Heiden, assistant professor of surgery, Department of Surgery, and Dr. Guy J. Petruzzelli, professor and vice chairman, Department of Otolaryngology and professor of neurosurgery, Rush University Medical Center, Chicago, IL, for their help in reviewing the paper. References [1] H. M. Blanck, W. H. Dietz, D. A. Galuska et al., State-specific prevalence of obesity among adults - United States, 2005, Morbidity and Mortality Weekly Report, vol. 55, no. 36, pp , [2] C. T. Merrill, A. Elixhauser et al., Procedures in U.S. Hospitals, 2003, Tech. Rep., U.S. Department of Health and Human Services, [3] L. Sjöström,K.Narbro,C.D.Sjöström et al., Effects of bariatric surgery on mortality in Swedish obese subjects, New England Medicine, vol. 357, no. 8, pp , [4]T.D.Adams,R.E.Gress,S.C.Smithetal., Long-term mortality after gastric bypass surgery, New England Journal of Medicine, vol. 357, no. 8, pp , [5] D.Heber,F.L.Greenway,L.M.Kaplan,E.Livingston,J.Salvador, and C. Still, Endocrine and nutritional management of the post-bariatric surgery patient: an endocrine society clinical practice guideline, Clinical Endocrinology and Metabolism, vol. 95, no. 11, pp , [6] K. Dolan, M. Hatzifotis, L. Newbury, and G. Fielding, A comparison of laparoscopic adjustable gastric banding and biliopancreatic diversion in superobesity, Obesity Surgery, vol. 14, no. 2, pp , [7] R.D.Bloomberg,A.Fleishman,J.E.Nalle,D.M.Herron,and S. Kini, Nutritional deficiencies following bariatric surgery: whave we learned? Obesity Surgery, vol. 15, no. 2, pp , [8] R. E. Brolin, L. B. LaMarca, H. A. Kenler et al., Malabsorptive gastric bypass in patients with superobesity, Gastrointestinal Surgery, vol. 6, no. 2, pp , [9] N. Hamoui, K. Kim, G. Anthone, P. F. Crookes, S. R. Klein, and C. W. Deveney, The significance of elevated levels of parathyroid hormone in patients with morbid obesity before and after bariatric surgery, Archives of Surgery, vol. 138, no. 8, pp , [10] L. Newbury, K. Dolan, M. Hatzifotis, N. Low, and G. Fielding, Calcium and vitamin D depletion and elevated parathyroid hormone following biliopancreatic diversion, Obesity Surgery, vol. 13, no. 6, pp , [11] G. H. Slater, C. J. Ren, N. Siegel et al., Serum fat-soluble vitamin deficiency and abnormal calcium metabolism after malabsorptive bariatric surgery, Gastrointestinal Surgery, vol. 8, no. 1, pp , [12] F.Triponez,O.H.Clark,Y.Vanrenthergem,andP.Evenepoel, Surgical treatment of persistent hyperparathyroidism after renal transplantation, Annals of Surgery, vol. 248, no. 1, pp , [13] A. Fine and J. Zacharias, Calciphylaxis is usually nonulcerating: risk factors, outcome and therapy, Kidney International, vol. 61, no. 6, pp , [14] L. R. Essary and M. R. Wick, Cutaneous calciphylaxis: an underrecognized clinicopathologic entity, American Journal of Clinical Pathology, vol. 113, no. 2, pp , [15]J.M.Johnson,J.W.Maher,E.J.DeMaria,R.W.Downs,L. G. Wolfe, and J. M. Kellum, The long-term effects of gastric bypass on vitamin D metabolism, Annals of Surgery, vol. 243, no. 5, pp , [16] C. De Prisco and S. N. Levine, Metabolic bone disease after gastric bypass surgery for obesity, American the Medical Sciences, vol. 329, no. 2, pp , [17] L. V. Crowley, J. Seay, and G. Mullin, Late effects of gastric bypass for obesity, American Gastroenterology, vol. 79, no. 11, pp , [18] M. Milas and C. J. Weber, Near-total parathyroidectomy is beneficial for patients with secondary and tertiary hyperparathyroidism, Surgery, vol. 136, no. 6, pp , [19] S. C. Pitt, R. S. Sippel, and H. Chen, Secondary and tertiary hyperparathyroidism, state of the art surgical management, Surgical Clinics of North America, vol. 89, no. 5, pp , [20] S. Li, Y. W. Chen, Y. Peng, R. N. Foley, and W. L. S. Peter, Trends in parathyroidectomy rates in US hemodialysis
5 Case Reports in Endocrinology 5 patients from 1992 to 2007, American Kidney Diseases, [21] E.-R. Gagné, P. Ureña, S. Leite-Silva et al., Short- and longterm efficacy of total parathyroidectomy with immediate autografting compared with subtotal parathyroidectomy in hemodialysis patients, the American Society of Nephrology, vol. 3, no. 4, pp , [22] M. Rothmund, P. K. Wagner, and C. Schark, Subtotal parathyroidectomy versus total parathyroidectomy and autotransplantation in secondary hyperparathyroidism: a randomized trial, World Surgery, vol. 15, no. 6, pp , [23] S. Ockert, F. Willeke, A. Richter et al., Total parathyroidectomy without autotransplantation as a standard procedure in the treatment of secondary hyperparathyroidism, Langenbeck s Archives of Surgery, vol. 387, no. 5-6, pp , [24] R. Roy and J. A. Lee, Calciphylaxis due to hyperparathyroidism, Endocrine Practice, vol. 17, supplement 1, pp , [25] J. M. Moffett and J. Suliburk, Parathyroid autotransplantation, Endocrine Practice, vol. 17, supplement 1, pp , [26] M.A.Guerrero,D.B.Evans,J.E.Leeetal., Viabilityofcryopreserved parathyroid tissue: when is continued storage versus disposal indicated? World Surgery,vol.32,no.5,pp , [27] S. Borot, V. Lapierre, B. Carnaille, P. Goudet, and A. Penfornis, Results of cryopreserved parathyroid autografts: a retrospective multicenter study, Surgery, vol. 147, no. 4, pp , [28] D. Carneiro-Pla, Contemporary and practical uses of intraoperative parathyroid hormone monitoring, Endocrine Practice, vol. 17 Suppl 1, pp , [29] S. C. Pitt, R. Panneerselvan, H. Chen, and R. S. Sippel, Secondary and tertiary hyperparathyroidism: the utility of iopth monitoring, World Surgery, vol. 34, no. 6, pp , [30] T. Weber, M. Zeier, U. Hinz, T. Schilling, and M. W. Büchler, Impact of intraoperative parathyroid hormone levels on surgical results in patients with renal hyperparathyroidism, World Surgery, vol. 29, no. 9, pp , [31] Y. Ikeda, H. Kurihara, N. Morita, R. Miyabe, and H. Takami, Significance of Monitoring Bio-Intact PTH (1-84) During Parathyroidectomy for Secondary Hyperparathyroidism, Surgical Research, vol. 139, no. 1, pp , [32] R. N. Saunders, R. Karoo, M. S. Metcalfe, and M. L. Nicholson, Four gland parathyroidectomy without reimplantation in patients with chronic renal failure, Postgraduate Medical Journal, vol. 81, no. 954, pp , [33] M. L. Durr, J. R. Saunders, J. A. Califano, R. P. Tufano, W. M. Koch, and P. K. Ha, Severe hypocalcemia complicating thyroid surgery after Roux-en-Y gastric bypass procedure, Archives of Otolaryngology - Head and Neck Surgery, vol. 135, no. 5, pp , [34] M. Manco, G. Nanni, V. Tondolo et al., Hypocalcemia complicating near-total thyroidectomy in patients with coexisting lipid malabsorption due to biliopancreatic diversion, Obesity Surgery, vol. 14, no. 10, pp , [35] P. M. Rojas-Marcos, M. A. Rubio, W. I. Kreskshi, L. Cabrerizo, and A. Sánchez-Pernaute, Severe hypocalcemia following total thyroidectomy after biliopancreatic diversion, Obesity Surgery, vol. 15, no. 3, pp , [36] S. M. Pietras and M. F. Holick, Refractory hypocalcemia following near-total thyroidectomy in a patient with a prior roux-en-y gastric bypass, Obesity Surgery, vol. 19, no. 4, pp , [37] K.K.Winer,C.W.Ko,J.C.Reynoldsetal., Long-termtreatment of hypoparathyroidism: a randomized controlled study comparing parathyroid hormone-(1-34) versus calcitriol and calcium, Clinical Endocrinology and Metabolism, vol. 88, no. 9, pp , [38] K. K. Winer, N. Sinaii, J. Reynolds, D. Peterson, K. Dowdy, and G. B. Cutler, Long-term treatment of 12 children with chronic hypoparathyroidism: a randomized trial comparing synthetic human parathyroid hormone 1-34 versus calcitriol and calcium, Clinical Endocrinology and Metabolism, vol. 95, no. 6, pp , [39] M. I. Khan, S. G. Waguespack, and M. I. Hu, Medical management of postsurgical hypoparathyroidism, Endocrine Practice, vol. 17, supplement 1, pp , 2011.
















6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Research Article The Cost of Prolonged Hospitalization due to Postthyroidectomy Hypocalcemia: A Case-Control Study
 Advances in Endocrinology, Article ID 954194, 4 pages http://dx.doi.org/10.1155/2014/954194 Research Article The Cost of Prolonged Hospitalization due to Postthyroidectomy Hypocalcemia: A Case-Control
Advances in Endocrinology, Article ID 954194, 4 pages http://dx.doi.org/10.1155/2014/954194 Research Article The Cost of Prolonged Hospitalization due to Postthyroidectomy Hypocalcemia: A Case-Control
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Head and Neck Endocrine Surgery
 Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand
 International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
Bariatric Surgery and Bone Health
 Bariatric Surgery and Bone Health No conflicts of interest Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism July 26, 202 BMI and Fracture Risk Low BMI is associated
Bariatric Surgery and Bone Health No conflicts of interest Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism July 26, 202 BMI and Fracture Risk Low BMI is associated
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
Hypocalcemia 6/8/12. Normal value. Physiologic functions. Nephron a functional unit of kidney. Influencing factors in Calcium and Phosphate Balance
 Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
76 year-old female presents with muscle cramps. Jess Hwang 12/6/12
 76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
Research Article Cryopreservation of Parathyroid Glands
 International Endocrinology Volume 2010, Article ID 829540, 5 pages doi:10.1155/2010/829540 Research Article Cryopreservation of Parathyroid Glands Marlon A. Guerrero Department of Surgery, The University
International Endocrinology Volume 2010, Article ID 829540, 5 pages doi:10.1155/2010/829540 Research Article Cryopreservation of Parathyroid Glands Marlon A. Guerrero Department of Surgery, The University
Efficacy of intraoperative parathyroid hormone monitoring to predict success of parathyroidectomy for secondary hyperparathyroidism
 J Korean Surg Soc 2012;83:1-6 http://dx.doi.org/10.4174/jkss.2012.83.1.1 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Efficacy of intraoperative parathyroid
J Korean Surg Soc 2012;83:1-6 http://dx.doi.org/10.4174/jkss.2012.83.1.1 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Efficacy of intraoperative parathyroid
Thyroidectomy in patients who have undergone gastric bypass surgery
 Received: 11 September 2017 Revised: 11 October 2017 Accepted: 11 January 2018 DOI: 10.1002/hed.25098 ORIGINAL ARTICLE Thyroidectomy in patients who have undergone gastric bypass surgery David Goldenberg
Received: 11 September 2017 Revised: 11 October 2017 Accepted: 11 January 2018 DOI: 10.1002/hed.25098 ORIGINAL ARTICLE Thyroidectomy in patients who have undergone gastric bypass surgery David Goldenberg
Calcium metabolism and the Parathyroid Glands. Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands
 Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Sensipar (cinacalcet)
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Is mini bypass as mini as we think it is? Nutritional consequences
 Is mini bypass as mini as we think it is? Nutritional consequences Mini/ single loop bypass What is a mini bypass? Single loop One anastomosis Mini Prevalence Increasing Who is the single loop bypass for?
Is mini bypass as mini as we think it is? Nutritional consequences Mini/ single loop bypass What is a mini bypass? Single loop One anastomosis Mini Prevalence Increasing Who is the single loop bypass for?
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
2.0 Synopsis. Paricalcitol Capsules M Clinical Study Report R&D/15/0380. (For National Authority Use Only)
") 2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
Corporate Presentation January 2013
 Corporate Presentation January 2013 0 Forward-Looking Statements Certain statements and information included in this presentation are forwardlooking statements under the Private Securities Litigation Reform
Corporate Presentation January 2013 0 Forward-Looking Statements Certain statements and information included in this presentation are forwardlooking statements under the Private Securities Litigation Reform
Metabolic Sequelaeof Bariatric Surgery. Roula BOU KHALIL Ass. Prof of Endocrinology SGHUMC Balamand University
 Metabolic Sequelaeof Bariatric Surgery Roula BOU KHALIL Ass. Prof of Endocrinology SGHUMC Balamand University OUTLINE Introduction Indications and metabolic benefits of bariatric surgery Obesity Paradox
Metabolic Sequelaeof Bariatric Surgery Roula BOU KHALIL Ass. Prof of Endocrinology SGHUMC Balamand University OUTLINE Introduction Indications and metabolic benefits of bariatric surgery Obesity Paradox
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
28 yo F w/esrd with a facial deformity
 28 yo F w/esrd with a facial deformity Jess Hwang Endocrinology fellow 1/30/14 History of renal failure-- 2005 Woke up blind one day At the hospital she was told she was 4 months pregnant Diagnosed with
28 yo F w/esrd with a facial deformity Jess Hwang Endocrinology fellow 1/30/14 History of renal failure-- 2005 Woke up blind one day At the hospital she was told she was 4 months pregnant Diagnosed with
Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor
 Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
Sensipar. Sensipar (cinacalcet) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Lecture Goals. Body Mass Index. Obesity Definitions. Bariatric Surgery What the PCP Needs to Know 11/17/2009. Indications for bariatric Surgeries
 Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
Vitamin D. Vitamin functioning as hormone. Todd A Fearer, MD FACP
 Vitamin D Vitamin functioning as hormone Todd A Fearer, MD FACP Vitamin overview Vitamins are organic compounds that are essential in small amounts for normal metabolism They are different from minerals
Vitamin D Vitamin functioning as hormone Todd A Fearer, MD FACP Vitamin overview Vitamins are organic compounds that are essential in small amounts for normal metabolism They are different from minerals
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience
 Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Near total parathyroidectomy for the treatment of renal hyperparathyroidism
 Original Article Near total parathyroidectomy for the treatment of renal hyperparathyroidism Marco Puccini 1,2, Cristina Ceccarelli 2, Ophelia Meniconi 3, Claudia Zullo 3, Valerio Prosperi 2, Mario Miccoli
Original Article Near total parathyroidectomy for the treatment of renal hyperparathyroidism Marco Puccini 1,2, Cristina Ceccarelli 2, Ophelia Meniconi 3, Claudia Zullo 3, Valerio Prosperi 2, Mario Miccoli
Yueming Sun Æ Huihua Cai Æ Jianfeng Bai Æ Hanlin Zhao Æ Yi Miao
 World J Surg (2009) 33:1674 1679 DOI 10.1007/s00268-009-0086-3 Endoscopic Total Parathyroidectomy and Partial Parathyroid Tissue Autotransplantation for Patients with Secondary Hyperparathyroidism: A New
World J Surg (2009) 33:1674 1679 DOI 10.1007/s00268-009-0086-3 Endoscopic Total Parathyroidectomy and Partial Parathyroid Tissue Autotransplantation for Patients with Secondary Hyperparathyroidism: A New
Nutritional Deficiencies following Bariatric Surgery: What Have We Learned?
 Obesity Surgery, 15, 145-154 Review Article Nutritional Deficiencies following Bariatric Surgery: What Have We Learned? Richard D. Bloomberg, MD, FRCSC; Amy Fleishman, MS, RD, CDN; Jennifer E. Nalle, RN,
Obesity Surgery, 15, 145-154 Review Article Nutritional Deficiencies following Bariatric Surgery: What Have We Learned? Richard D. Bloomberg, MD, FRCSC; Amy Fleishman, MS, RD, CDN; Jennifer E. Nalle, RN,
Kobe University Repository : Kernel
 Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
Long-Term Care Updates
 Long-Term Care Updates August 2017 By Alyson Lozicki, PharmD As the prevalence of obesity continues to rise, and with now over one-third (36.5%) of American adults considered obese, the number of weight
Long-Term Care Updates August 2017 By Alyson Lozicki, PharmD As the prevalence of obesity continues to rise, and with now over one-third (36.5%) of American adults considered obese, the number of weight
Managing Endocrine Related Issues after Bariatric Surgery. Jenny Tong, MD, MPH Division of Endocrinology March 3, 2018
 Managing Endocrine Related Issues after Bariatric Surgery Jenny Tong, MD, MPH Division of Endocrinology March 3, 2018 Bariatric Surgery was Associated with Higher Remission Rate than Usual Care 72.3% 38.1%
Managing Endocrine Related Issues after Bariatric Surgery Jenny Tong, MD, MPH Division of Endocrinology March 3, 2018 Bariatric Surgery was Associated with Higher Remission Rate than Usual Care 72.3% 38.1%
Clinical Case Study: Bad Breaks and Metabolic Effects of Bariatric Surgery
 Articles: Naga Yalla. Bad Breaks. Piriyah Sinclair, et al.. Clin Chem 2018;64:47-50 and 72-81. http://clinchem.aaccjnls.org/content/64/1/47,http://clinchem.aaccjnls.org/content/64/1/72 Guests: Dr. Naga
Articles: Naga Yalla. Bad Breaks. Piriyah Sinclair, et al.. Clin Chem 2018;64:47-50 and 72-81. http://clinchem.aaccjnls.org/content/64/1/47,http://clinchem.aaccjnls.org/content/64/1/72 Guests: Dr. Naga
Secondary and Familial Hyperparathyroidism
 Secondary and Familial Jeffrey F. Moley, M.D. Chief, Endocrine and Oncologic Surgery Section, Professor of Surgery Associate Director, The Alvin J. Siteman Cancer Center Occurs in setting of CRF Chronic
Secondary and Familial Jeffrey F. Moley, M.D. Chief, Endocrine and Oncologic Surgery Section, Professor of Surgery Associate Director, The Alvin J. Siteman Cancer Center Occurs in setting of CRF Chronic
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD
 The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
Minimally invasive parathyroidectomy
 Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Rajesh Jain MD Endorama
 50 F with history of duodenal switch presenting for low BMD Rajesh Jain MD Endorama HPI 50 F presenting with low BMD referred by PCP She has a history of malnutrition following duodenal switch procedure
50 F with history of duodenal switch presenting for low BMD Rajesh Jain MD Endorama HPI 50 F presenting with low BMD referred by PCP She has a history of malnutrition following duodenal switch procedure
Case Report Use of Percutaneous Ethanol Injection Therapy for Recurrent Secondary Hyperparathyroidism after Subtotal Parathyroidectomy
 SAGE-Hindawi Access to Research International Nephrology Volume 211, Article ID 246734, 6 pages doi:1.461/211/246734 Case Report Use of Percutaneous Ethanol Injection Therapy for Recurrent Secondary Hyperparathyroidism
SAGE-Hindawi Access to Research International Nephrology Volume 211, Article ID 246734, 6 pages doi:1.461/211/246734 Case Report Use of Percutaneous Ethanol Injection Therapy for Recurrent Secondary Hyperparathyroidism
Case Report Combined Effect of a Locking Plate and Teriparatide for Incomplete Atypical Femoral Fracture: Two Case Reports of Curved Femurs
 Case Reports in Orthopedics Volume 2015, Article ID 213614, 5 pages http://dx.doi.org/10.1155/2015/213614 Case Report Combined Effect of a Locking Plate and Teriparatide for Incomplete Atypical Femoral
Case Reports in Orthopedics Volume 2015, Article ID 213614, 5 pages http://dx.doi.org/10.1155/2015/213614 Case Report Combined Effect of a Locking Plate and Teriparatide for Incomplete Atypical Femoral
Nutritional deficiencies & vitamins after surgery. What needs to be monitored? Ratna Pallapothu, MD, FACS, FASMBS
 Nutritional deficiencies & vitamins after surgery. What needs to be monitored? Ratna Pallapothu, MD, FACS, FASMBS Disclosures No financial disclosures Medical Director Bariatric program at Lourdes Types
Nutritional deficiencies & vitamins after surgery. What needs to be monitored? Ratna Pallapothu, MD, FACS, FASMBS Disclosures No financial disclosures Medical Director Bariatric program at Lourdes Types
Practical recommendations for the post-bariatric surgery medical management
 Practical recommendations for the post-bariatric surgery medical management Dr L. Favre CHUV Sce Endocrinologie, diabétologie et métabolisme 26.04.2018 Bariatric surgery in Switzerland Multidisciplinary
Practical recommendations for the post-bariatric surgery medical management Dr L. Favre CHUV Sce Endocrinologie, diabétologie et métabolisme 26.04.2018 Bariatric surgery in Switzerland Multidisciplinary
Nutrients and Drugs Considerations after Bariatric Surgeries
 Nutrients and Drugs Considerations after Bariatric Surgeries Marwan Akel, Pharm D Clinical AssistantProfessor School of Pharmacy Lebanese International University Overweight and Obesity Prevalence 2013
Nutrients and Drugs Considerations after Bariatric Surgeries Marwan Akel, Pharm D Clinical AssistantProfessor School of Pharmacy Lebanese International University Overweight and Obesity Prevalence 2013
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016
 Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
73 year-old Female with Hypercalcemia
 73 year-old Female with Hypercalcemia Katie O Sullivan, M.D. Fellow, Adult/Pediatric Endocrinology University of Chicago Thursday, December 19 th, 2013 Chief Complaint 73 year-old female who presents for
73 year-old Female with Hypercalcemia Katie O Sullivan, M.D. Fellow, Adult/Pediatric Endocrinology University of Chicago Thursday, December 19 th, 2013 Chief Complaint 73 year-old female who presents for
Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience
 Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
02/27/2018. Objectives. To Replace or Not to Replace: Nutritional Vitamin D in Dialysis.
 To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
Goals 1/9/2018. Obesity over the last decade Surgery has become a safer management strategy Surgical options for management
 The Current State of Surgical Intervention in Management of Morbid Obesity Goals Obesity over the last decade Surgery has become a safer management strategy Surgical options for management 1 Goals Obesity
The Current State of Surgical Intervention in Management of Morbid Obesity Goals Obesity over the last decade Surgery has become a safer management strategy Surgical options for management 1 Goals Obesity
Nutrition in obesity. Topic 23. Module Nutritional support after bariatric surgery. Copyright 2009 by ESPEN LLL Programme.
 Nutrition in obesity Topic 23 Module 23.5 Nutritional support after bariatric surgery Anders Thorell Learning Objectives To understand physiological and nutritional consequences of different bariatric
Nutrition in obesity Topic 23 Module 23.5 Nutritional support after bariatric surgery Anders Thorell Learning Objectives To understand physiological and nutritional consequences of different bariatric
Case Report Rare Skeletal Complications in the Setting of Primary Hyperparathyroidism
 Case Reports in Endocrinology Volume 2015, Article ID 139751, 4 pages http://dx.doi.org/10.1155/2015/139751 Case Report Rare Skeletal Complications in the Setting of Primary Hyperparathyroidism Nikos Sabanis,
Case Reports in Endocrinology Volume 2015, Article ID 139751, 4 pages http://dx.doi.org/10.1155/2015/139751 Case Report Rare Skeletal Complications in the Setting of Primary Hyperparathyroidism Nikos Sabanis,
2017 KDIGO Guidelines Update
 2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
Thallium 201 scanning can diagnose multiple recurrences in forearm implanted parathyroid tissue post total parathyroidectomy:
 CASE REPORT Thallium 201 scanning can diagnose multiple recurrences in forearm implanted parathyroid tissue post total parathyroidectomy: Salman AK., Wagieh S.,Munshy AT. and Al Ghamdy H.* King Abdulla
CASE REPORT Thallium 201 scanning can diagnose multiple recurrences in forearm implanted parathyroid tissue post total parathyroidectomy: Salman AK., Wagieh S.,Munshy AT. and Al Ghamdy H.* King Abdulla
Nutritional Markers following Duodenal Switch for Morbid Obesity
 Obesity Surgery, 14, pp-pp Nutritional Markers following Duodenal Switch for Morbid Obesity Robert A. Rabkin MD, FACS; John M. Rabkin, MD, FACS; Barbara Metcalf, RN; Myra Lazo, MS, PA-C; Michael Rossi,
Obesity Surgery, 14, pp-pp Nutritional Markers following Duodenal Switch for Morbid Obesity Robert A. Rabkin MD, FACS; John M. Rabkin, MD, FACS; Barbara Metcalf, RN; Myra Lazo, MS, PA-C; Michael Rossi,
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
The Parsabiv Beginner s Book
 The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
ORIGINAL ARTICLE. Long-term Results of Subtotal vs Total Parathyroidectomy Without Autotransplantation in Kidney Transplant Recipients
 ORIGINAL ARTICLE Long-term Results of Subtotal vs Total Parathyroidectomy Without Autotransplantation in Kidney Transplant Recipients Nada Rayes, MD; Daniel Seehofer, MD; Ralf Schindler, PhD; Petra Reinke,
ORIGINAL ARTICLE Long-term Results of Subtotal vs Total Parathyroidectomy Without Autotransplantation in Kidney Transplant Recipients Nada Rayes, MD; Daniel Seehofer, MD; Ralf Schindler, PhD; Petra Reinke,
Clinical Study Endoscopic Revision (StomaphyX) versus Formal Surgical Revision (Gastric Bypass) for Failed Vertical Band Gastroplasty
 versus Formal Surgical Revision (Gastric Bypass) for Failed Vertical Band Gastroplasty") Obesity Volume 2013, Article ID 108507, 4 pages http://dx.doi.org/10.1155/2013/108507 Clinical Study Endoscopic Revision (StomaphyX) versus Formal Surgical Revision (Gastric Bypass) for Failed Vertical
Obesity Volume 2013, Article ID 108507, 4 pages http://dx.doi.org/10.1155/2013/108507 Clinical Study Endoscopic Revision (StomaphyX) versus Formal Surgical Revision (Gastric Bypass) for Failed Vertical
10/28/11. Bariatric Surgery: What the Primary Care Provider Should Know. Case Presentation: Rachelle
 Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
DEKAs after Bariatric Surgery*
 DEKAs after Bariatric Surgery* Once Daily All-in-one Multivitamin and Mineral Chewable Tablets with Enhanced Absorption for Dietary Management after Bariatric Surgery Roberto Jongejan, MD, PhD Gus Papas,
DEKAs after Bariatric Surgery* Once Daily All-in-one Multivitamin and Mineral Chewable Tablets with Enhanced Absorption for Dietary Management after Bariatric Surgery Roberto Jongejan, MD, PhD Gus Papas,
Therapeutic golas in the treatment of CKD-MBD
 Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Management of patients with thyroid cancer scheduled for thyroidectomy at RCHSD
 Management of patients with thyroid cancer scheduled for thyroidectomy at RCHSD Pre-Operative labs To be drawn when Thyroidectomy for the management of thyroid cancer is first considered Vitamin D-25 OH
Management of patients with thyroid cancer scheduled for thyroidectomy at RCHSD Pre-Operative labs To be drawn when Thyroidectomy for the management of thyroid cancer is first considered Vitamin D-25 OH
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Conference Paper Antithrombotic Therapy in Patients with Acute Coronary Syndromes: Biological Markers and Personalized Medicine
 Conference Papers in Medicine, Article ID 719, pages http://dx.doi.org/1.1155/13/719 Conference Paper Antithrombotic Therapy in Patients with Acute Coronary Syndromes: Biological Markers and Personalized
Conference Papers in Medicine, Article ID 719, pages http://dx.doi.org/1.1155/13/719 Conference Paper Antithrombotic Therapy in Patients with Acute Coronary Syndromes: Biological Markers and Personalized
Inpatient Pediatric Endocrinology. Tala Dajani MD MPH Pediatric Endocrinology of Phoenix
 Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems
Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems
Marcin Barczynski, 1 Aleksander Konturek, 2 Alicja Hubalewska-Dydejczyk, 2. Filip Gołkowski, 1 Stanislaw Cichon, 1 Piotr Richter, 1 Wojciech Nowak
 3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
Parathyroid Imaging. A Guide to Parathyroid Surgery
 Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
ORIGINAL ARTICLE. Novel Parathyroid Hormone (1-84) Assay as Basis for Parathyroid Hormone Monitoring in Renal Hyperparathyroidism
 Assay as Basis for Parathyroid Hormone Monitoring in Renal Hyperparathyroidism") ORIGINAL ARTICLE Novel Parathyroid Hormone (1-84) Assay as Basis for Parathyroid Hormone Monitoring in Renal Hyperparathyroidism Klaus Kaczirek, MD; Gerhard Prager, MD; Philipp Riss, MD; Gerald Wunderer,
ORIGINAL ARTICLE Novel Parathyroid Hormone (1-84) Assay as Basis for Parathyroid Hormone Monitoring in Renal Hyperparathyroidism Klaus Kaczirek, MD; Gerhard Prager, MD; Philipp Riss, MD; Gerald Wunderer,
BARIATRIC SURGERY. Weight Loss Surgery. A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female
 BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary
 Prior Authorization with Quantity Limit Program Summary") Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Case Report Crossed Renal Ectopia without Fusion An Unusual Cause of Acute Abdominal Pain: A Case Report
 Case Reports in Urology Volume 2012, Article ID 728531, 4 pages doi:10.1155/2012/728531 Case Report Crossed Renal Ectopia without Fusion An Unusual Cause of Acute Abdominal Pain: A Case Report D. P. Ramaema,
Case Reports in Urology Volume 2012, Article ID 728531, 4 pages doi:10.1155/2012/728531 Case Report Crossed Renal Ectopia without Fusion An Unusual Cause of Acute Abdominal Pain: A Case Report D. P. Ramaema,
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Effect of Bariatric Surgery on Cardio-Metabolic Outcomes
 Effect of Bariatric Surgery on Cardio-Metabolic Outcomes Disclosure Research support from Bariatric Advantage (supplements donated for research study) Anne Schafer, MD Associate Professor of Medicine and
Effect of Bariatric Surgery on Cardio-Metabolic Outcomes Disclosure Research support from Bariatric Advantage (supplements donated for research study) Anne Schafer, MD Associate Professor of Medicine and
Vitamins. Vitamins (continued) Lipid-Soluble Vitamins (A, D, E, K) Vitamins Serve Important Roles in Function of Body
 Lipid-Soluble Vitamins (A, D, E, K) Vitamins Serve Important Roles in Function of Body") Vitamins Drugs for Nutritional Disorders Organic substances are needed in small amounts Promote growth Maintain health Vitamins Human cells cannot produce vitamins Exception: vitamin D Vitamins or provitamins
Vitamins Drugs for Nutritional Disorders Organic substances are needed in small amounts Promote growth Maintain health Vitamins Human cells cannot produce vitamins Exception: vitamin D Vitamins or provitamins
Bariatric Surgery: A Cost-effective Treatment of Obesity?
 Bariatric Surgery: A Cost-effective Treatment of Obesity? Shaneeta M. Johnson MD FACS FASMBS 2018 NMA Professional Development Seminar Congressional Black Caucus Foundation Annual Legislative Conference
Bariatric Surgery: A Cost-effective Treatment of Obesity? Shaneeta M. Johnson MD FACS FASMBS 2018 NMA Professional Development Seminar Congressional Black Caucus Foundation Annual Legislative Conference
Research Article Opioid Use Is Not Associated with Incomplete Wireless Capsule Endoscopy for Inpatient or Outpatient Procedures
 Diagnostic and erapeutic Endoscopy, Article ID 651259, 4 pages http://dx.doi.org/10.1155/2014/651259 Research Article Opioid Use Is Not Associated with Incomplete Wireless Capsule Endoscopy for Inpatient
Diagnostic and erapeutic Endoscopy, Article ID 651259, 4 pages http://dx.doi.org/10.1155/2014/651259 Research Article Opioid Use Is Not Associated with Incomplete Wireless Capsule Endoscopy for Inpatient
Chronic Kidney Disease Mineral Bone Disorder (CKD-MBD)
") Oxford Kidney Unit Chronic Kidney Disease Mineral Bone Disorder (CKD-MBD) Information for patients This leaflet will provide you with information about chronic kidney disease mineral bone disorder (CKD-MBD)
Oxford Kidney Unit Chronic Kidney Disease Mineral Bone Disorder (CKD-MBD) Information for patients This leaflet will provide you with information about chronic kidney disease mineral bone disorder (CKD-MBD)
Contents. Authors Name: Christopher Wong: Consultant Nephrologist Anne Waddington: Renal Pharmacist Eimear Fegan : Renal Dietitian
 Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
Parathyroidectomy. Surgery for Parathyroid Problems
 Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease?
 Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
Disclosure. Topic Outline. Calcium, Vitamin D, PTH Disorders. PTH/Calcium-Normal Physiology. I have nothing to disclose
 Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Townhall: Assisting Patients Post Bariatric Surgery Katie McClendon, PharmD, BCPS, FCCP University of Mississippi School of Pharmacy
 Townhall: Assisting Patients Post Bariatric Surgery Katie McClendon, PharmD, BCPS, FCCP University of Mississippi School of Pharmacy Annual Meeting & Exposition Seattle, Washington March 22 25 Disclosures
Townhall: Assisting Patients Post Bariatric Surgery Katie McClendon, PharmD, BCPS, FCCP University of Mississippi School of Pharmacy Annual Meeting & Exposition Seattle, Washington March 22 25 Disclosures
Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report of Neoadjuvant Use Enabling Complete Surgical Resection
 Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Case Reports in Oncological Medicine Volume 2013, Article ID 496351, 4 pages http://dx.doi.org/10.1155/2013/496351 Case Report Denosumab Chemotherapy for Recurrent Giant-Cell Tumor of Bone: A Case Report
Clinical Study Changing Trends in Use of Laparoscopy: A Clinical Audit
 Minimally Invasive Surgery, Article ID 562785, 4 pages http://dx.doi.org/10.1155/2014/562785 Clinical Study Changing Trends in Use of Laparoscopy: A Clinical Audit Ritu Khatuja, 1 Geetika Jain, 1 Sumita
Minimally Invasive Surgery, Article ID 562785, 4 pages http://dx.doi.org/10.1155/2014/562785 Clinical Study Changing Trends in Use of Laparoscopy: A Clinical Audit Ritu Khatuja, 1 Geetika Jain, 1 Sumita
HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE ON MAINTENANCE DIALYSIS THERAPY
 UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones
 Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
INDEX. Note: Page numbers of issue and article titles are in boldface type. cell carcinoma. ENDOCRINE SURGERY
 ENDOCRINE SURGERY INDEX Note: Page numbers of issue and article titles are in boldface type. Adenylate cyclase, in signal transduction 425-426 Adrenal incidentalomas, 499-509 imaging of, 502-504 in patients
ENDOCRINE SURGERY INDEX Note: Page numbers of issue and article titles are in boldface type. Adenylate cyclase, in signal transduction 425-426 Adrenal incidentalomas, 499-509 imaging of, 502-504 in patients
What is the right calcium balance?
 For patients with hypoparathyroidism What is the right calcium balance? Indications and Usage1 NATPARA is a parathyroid hormone indicated as an adjunct to calcium and vitamin D to control hypocalcemia
For patients with hypoparathyroidism What is the right calcium balance? Indications and Usage1 NATPARA is a parathyroid hormone indicated as an adjunct to calcium and vitamin D to control hypocalcemia
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine
 Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from the West?
 ecommons@aku Section of Urology Department of Surgery August 1999 Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from
ecommons@aku Section of Urology Department of Surgery August 1999 Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from
Urinary Calculus Disease. Urinary Stones: Simplified Metabolic Evaluation. Urinary Calculus Disease. Urinary Calculus Disease 2/8/2008
 Urinary Stones: Simplified Metabolic Evaluation Marshall L. Stoller, M.D. Professor and Vice Chairman Department of Urology University of California San Francisco Incidence: 7-21/10,000 3 men: 1 woman
Urinary Stones: Simplified Metabolic Evaluation Marshall L. Stoller, M.D. Professor and Vice Chairman Department of Urology University of California San Francisco Incidence: 7-21/10,000 3 men: 1 woman