The Changing Face of Head and Neck Cancer in the 21st Century: The Impact of HPV on the Epidemiology and Pathology of Oral Cancer. William H.
|
|
|
- Flora Owen
- 5 years ago
- Views:
Transcription
1 The Changing Face of Head and Neck Cancer in the 21st Century: The Impact of HPV on the Epidemiology and Pathology of Oral Cancer William H. Westra From the Department of Pathology and Otolaryngology/Head & Neck Surgery, The Johns Hopkins Medical Institutions, Baltimore, Maryland Correspondence to: William H. Westra, M.D. The Weinberg Bldg, Room N. Broadway Baltimore, Maryland Phone: Fax:
2 Abstract The longstanding notion that head and neck squamous cell carcinoma (HNSCC) is a uniform disease process is changing. Divergence in epidemiologic trends among HNSCCs arising in different anatomic subsites has introduced a view that HNSCC is a heterogeneous group. Analysis of molecular genetic changes discloses not just individual tumor differences, but also consistent large-scale differences that permit the recognition of important tumor subtypes. One recently recognized subtype is the human papillomavirus (HPV)-positive oropharyngeal carcinoma. HPV-positive oropharyngeal cancer now dominates the head and neck oncology landscape, and its escalating incidence is impacting on diagnostic, preventive and therapeutic practices. Introduction Long regarded as a uniform group of tumors that differed only as a function of anatomic site, ongoing studies indicate that HNSCCs may not be as homogenous as previously supposed. Recognition of distinct molecular genetic profiles now permits finer resolution of HNSCC into distinct subtypes that differ with respect to risk factors, pathogenesis, and clinical behavior (1). HPV-associated oropharyngeal carcinoma has recently been recognized as a unique subtype of HNSCC (2). HPV status has a profound effect on patient prognosis, and it may soon guide therapy. Accordingly, HPV status will become a standard component in the diagnostic reporting of all oropharyngeal carcinomas. This review covers recent advances toward defining HPV-related oropharyngeal carcinoma, and draws specific attention to pathology concerns that impact on the diagnosis and reporting of these cancers. Discussion HNSCC is the eighth most common cancer worldwide with approximately 650,000 new cases reported annually. Beginning in the early 1980s, the incidence of HNSCC in the United States and elsewhere has been in retreat. This downward trend has roughly paralleled trends in smoking. Accordingly, HNSCC is often perceived as a preventable disease, and its
3 ultimate demise simply a matter of implementing behavior modification strategies. This great optimism has recently been shaken by a sobering escalation of a specific type of cancer that is asserting its dominance on the head and neck oncology landscape. Specifically, the incidence of oropharyngeal cancer is advancing (3,4). This anomalous rise bucks the prevailing notion that HNSCC incident rates can be controlled through smoking prevention and cessation. Indeed, the escalation of oropharyngeal carcinoma points to the participation of non-traditional behavioral and environmental factors driving this disturbing epidemiologic trend. The prototypic patient with oral cancer is an older man who has smoked cigarettes and drank alcohol for many years. This prototype, however, no longer fits the patient with oral cancer who now enters the doors of our clinics and hospitals. Patients now tend to be younger (between 40 and 60 years) white men who have never smoked cigarettes or drank alcohol (5). Traditional risk factors have been supplanted by other powerful risk factors relating to sexual practices, the most important of these being high number of sexual partners, history of oralgenital sex, and history of oral-anal sex (5,6). Oral anogenital contact is an important route for the transmission of HPV to the oral cavity. Certain conditions and behaviors that alter antitumor immunity may be important in transforming an HPV oral infection towards HPV-related malignancy. As one example, marijuana use has recently been identified as an independent risk factor for HPV-positive HNSCC, and the strength of this association increases with intensity, duration, and cumulative years of marijuana smoking (7). Long scrutinized as a potential source of DNA-damaging carcinogens, marijuana smoke may be more relevant for its immunomodulatory effects. Cannabinoids bind to the CB2 receptor expressed on immunomodulatory cells in human tonsillar tissue. Binding, in turn, can suppress immune responses, diminish host responses to viral pathogens, and attenuate antitumor activity.
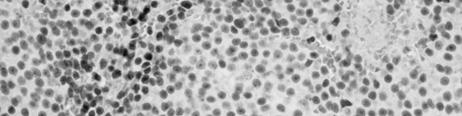
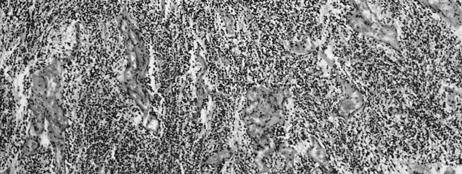
4 HPV, particulary type 16, is detected in about 70% of oropharyngeal carcinomas. These HPV-positive cancers are increasingly recognized as a distinct subgroup of HNSCC with a biological and clinical profile that diverges from that of their HPV-negative counterparts (Table 1). At the molecular genetic level, HPV-positive HNSCCs express the viral oncoproteins E6 and E7, overexpress the p16 gene product, and only infrequently harbor p53 gene mutations. Regarding clinical behavior, HPV16-positive HNSCs are associated with an improved prognosis (8,9). The mechanisms underlying this favorable prognosis may involve the combined effects of immune surveillance to viral-specific tumor antigens, an intact apoptotic response to radiation, and the absence of widespread genetic alterations associated with smoking (i.e., field cancerization). The pathologic features of HPV-positive HNSCs also deviate from the moderately differentiated keratinizing morphology that typifies most HNSCCs. HPV-positive HNSCCs consistently: 1) arise from the tonsillar crypts; 2) are unassociated with dysplasia of the surface epithelium; 3) exhibit lobular growth; 4) are permeated by infiltrating lymphocytes; 5) lack significant keratinization; and 6) demonstrate a prominent basaloid morphology (Figure 1). Two microscopic features of HPV-related oropharyngeal cancers are likely to cause diagnostic ambiguity. First, HPV-related HNSCC is customarily misperceived as a poorly differentiated carcinoma based on the immature appearance of the tumor cells. In point of fact, the appearance of the tumor cells closely emulates the appearance of the reticulated epithelium the specialized epithelium lining the tonsillar crypts from which HPV-related cancers arise (10). In other words, HPV-related oropharyngeal cancers are in fact highly differentiated, not poorly differentiated as so widely assumed. Second, use of the term basaloid as a diagnostic descriptor is confusing for the way it invites an erroneous connection with basaloid squamous cell carcinoma a
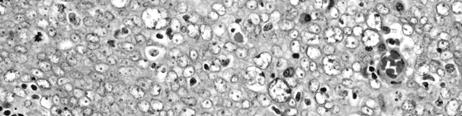
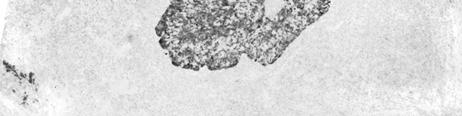
5 subtype of HNSCC notorious for its aggressive clinical behavior. Within the basaloid subtype, detection of HPV is a highly favorable prognostic factor that helps identify a subset of cancers that departs from the highly aggressive behavior associated with this variant (11). Until consensus panels put forward a classification scheme for oropharyngeal carcinomas that underscores their relationship with HPV while avoiding confusion with the aggressive basaloid variant, it is our practice to: 1) classify these tumors as non-keratinizing squamous cell carcinomas, 2) suspend the use of the descriptors such as poorly differentiated and basaloid, and 3) routinely report on the HPV status of all HNSCCs arising in the oropharynx. Determination of HPV status will certainly become standard practice in the pathologic evaluation of oropharyngeal cancers. As a biomarker, HPV detection is emerging as a valid method of discerning the presence and progress of disease encompassing all aspects of patient care from early cancer detection, to tumor localization(12) (Figure 2), to selection of patients most likely to benefit from specific therapies, to post-treatment tumor surveillance. A variety of detection methods are in current use including PCR-based strategies, type-specific in-situ hybridization (ISH) techniques, and immunohistochemical detection of surrogate biomarkers (e.g. p16 protein). Standardization of HPV detection in the clinical arena must begin with selection of the best detection platform for universal application. The preferential use of ISH methods over PCR-based methods is supported both by biological and practical considerations. The reported large variation of HPV prevalence in HNSCC is a largely a reflection of the inability of non-quantitative PCR methods to discern virus that is biologically meaningful from virus that is biologically irrelevant. In contrast, punctuate hybridization signals within the nuclei of tumor cells is a pattern of staining only seen following HPV DNA integration into the host genome, and thus is more closely linked with relevant viral
6 infections. Importantly, the improved specificity of HPV detection by ISH does not come at the expense of sensitivity. The introduction of various signal amplification steps has significantly improved the sensitivity of this technique, even to the point of viral detection down to one viral copy per cell. The development of nonfluorescent chromogens now allows visualization of DNA hybridization using conventional light microscope. Adaptation of ISH to formalin-fixed and paraffin-embedded tissues has made this technique compatible with standard tissue-processing procedures and amendable to retrospective analysis of archival tissue blocks while most PCRbased methods are optimized to fresh frozen samples. ISH is a feasible and cost-effective test for most diagnostic laboratories that routinely process formalin-fixed and paraffin-embedded tissue blocks. In HPV-positive oropharyngeal carcinomas, functional inactivation of Rb by the viral oncoprotein E7 is known to induce an up regulation of p16 expression, reaching levels that can be readily detected by routine immunohistochemistry. Accordingly, p16 immunohistochemistry is often advocated as a reliable surrogate marker of HPV-induced neoplasia of oropharynx. Direct comparison of p16 immunohistochemical staining and HPV-16 ISH for large numbers of HNSCCs reveals a discrepancy rate of about 25%. In a subset of discrepant cases, high p16 expression is due to the presence of some other (non-16) HPV type as confirmed by wide spectrum ISH. The remaining discrepancies likely reflect the imperfection of p16 as a surrogate marker. Using E6/E7 mrna levels as conclusive evidence of HPV involvement, positive p16 immunostaining of HNSCCs is 100% sensitive but only 79% specific (13). The limitations of any single detection assay may be offset using algorithms that combine the strengths of complementary assays. We use a detection strategy that combines HPV ISH with p16 immunohistochemistry. Given a sensitivity that approaches 100%, p16
7 immunostaining is a good first line assay for eliminating HPV-negative cases from additional analysis. HPV-16 ISH can be run concurrently with p16 immunostaining or as a second-line assay following a positive p16 result. Given a specificity approaching 100%, a positive HPV-16 ISH reduces the numbers of false positive cases by p16 staining alone. A p16-positive/hpv-16- negative result singles out a subset of tumors that qualify for rigorous analysis for other (i.e. non- 16) oncogenic HPV types. For this third-line assay, we use a consensus ISH probe that that detects an extended panel of HPV types. P16 immunohistochemistry and HPV ISH are standardized techniques that are easily applied to formalin-fixed and paraffin-embedded tissues. As automated ISH technologies are brought on-line, turnaround time will be further shortened and standardization across various diagnostic laboratories will be enhanced. Conclusion Incident trends for HNSCC have generally paralleled smoking trends. The escalating incidence of oropharyngeal carcinoma in the absence of a parallel rise in smoking and alcohol consumption suggests that nontraditional behavioral and environmental factors are driving this aberration. HPV, particularly type 16, has been established as a causative agent in up to 70% of oropharyngeal cancers. These HPV-positive HNSCCs differ in important respects from HPV-negative HNSCC including risk factors, molecular genetic alterations, microscopic appearance, and clinical behavior. Diagnostic pathologists are now faced with the challenge of accurately discerning HPV status of oropharyngeal cancers.
8 References 1. Pai SI, Westra WH, Molecular Pathology of Head and Neck Cancer: Implications for diagnosis, prognosis and treatment of patients with head and neck squamous cell carcinoma. Annual Rev Pathol (Epub ahead of print) 2. Gillison ML, Koch WM, Capone RB, Spafford M, Westra WH, Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J. Natl. Cancer Inst. 92: Sturgis EM, Cinciripini PM Trends in head and neck cancer incidence in relation to smoking prevalence: an emerging epidemic of human papillomavirus--associated cancers? Cancer 110: Chaturvedi AK, Engels EA, Anderson WF, Gillison ML. Incidence trends for human papillomavirus-related and -unrelated oral squamous cell carcinomas in the United States. J Clin Oncol 26: D Souza G, Kreimer AR, Viscidi R, Pawlita M, Fakhry C, et al Case-control study of human papillomavirus and oropharyngeal cancer. N. Engl. J. Med. 356: Smith EM, Ritchie JM, Summersgill KF, Klussmann JP, Lee JH, et al Age, sexual behavior and human papillomavirus infection in oral cavity and oropharyngeal cancers. Int. J. Cancer 108:766-72
9 7. Gillison ML, D Souza G, Westra WH, Sugar E, Xiao W, et al Distinct risk factor profiles for human papillomavirus-16 positive and negative head and neck cancer. J. Natl. Cancer Inst. 100: Fakhry C, Westra WH, Li S, Cmelak A, Ridge JA, et al Improved survival of patients with human papillomavirus--positive head and neck squamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Inst. 100: Weinberger PM, Yu Z, Haffty BG, Kowalski D, Harigopal M, et al Molecular classification identifies a subset of human papillomavirus--associated oropharyngeal cancers with favorable prognosis. J. Clin. Oncol. 24: Begum S, Cao D, Gillison M, Zahurak M, Westra WH Tissue distribution of human papillomavirus 16 DNA integration in patients with tonsillar carcinoma. Clin. Cancer Res. 11: Begum S, Westra WH Basaloid squamous cell carcinoma of the head and neck is a mixed variant that can be further resolved by HPV status. Am J Surg Pathol 32: Begum S, Gillison ML, Ansari-Lari MA, Shah K, Westra WH Detection of human papillomavirus in cervical lymph nodes: a highly effective strategy for localizing site of tumor origin. Clin. Cancer Res. 9: Smeets SJ, Hesselink AT, Speel EJ, Haesevoets A, Snijders PJ, Pawlita M, Meijer CJ, Braakhuis BJ, Leemans CR, Brakenhoff RH A novel algorithm for reliable detection of human papillomavirus in paraffin embedded head and neck cancer specimen. Int J Cancer 121:
10 Table. Comparison of HPV-positive and HPV-negative head and neck cancers HPV-positive HPV-negative Incidence Increasing Decreasing Age Younger Older Gender 3:1 men 3:1 men Risk factors Sexual behavior Tobacco, alcohol Cofactors Marijuana, immunosuppresion Diet, oral hygiene Molecular genetics findings P16 Rb P53 wild-type P16 Rb P53 mutated Anatomic site Lingual and palatine tonsils All sites Pathologic findings Primary Lymph node metastasis Basaloid Cystic Keratinized Solid Survival Better Worse
11 Figure legend. Figure 1. Typical histopathologic appearance of an HPV-related cancer of the head and neck. (A) The carcinomas tend to arise from the tonsillar crypts and infiltrate the lymphoid stroma as expanding tumor lobules. (B) The lobules of tumor cells are permeated by lymphocytes, lack keratinization, and have a basaloid appearance. Figure 2. Metastatic squamous cell carcinoma of unknown primary origin. The metastasis is cystic (A, hematoxylin and eosin). The presence of HPV as evident by p16 immunohistochemical staining (B) and HPV-16 in-situ hybridization (hybridization dots within tumor cell nuclei, inset) point to the oropharynx as the site of tumor origin.
12 AN UPDATE ON GRADING OF SALIVARY GLAND CARCINOMAS Raja R. Seethala, M.D. Department of Pathology and Laboratory Medicine University of Pittsburgh Medical Center A616.3 PUH 200 Lothrop St Pittsburgh, PA Phone: Fax:
13 Abstract: Histologic grade is a significant predictor of outcome in salivary gland carcinomas. However, the sheer variety of tumor type and the rarity of these tumors pose challenges to devising highly predictive grading schemes. As our knowledge base has evolved, it is clear that carcinoma ex pleomorphic adenoma is not automatically a high grade tumor as is traditionally suggested. These tumors should be further qualified as to type/grade of carcinoma and extent, since intracapsular and minimally invasive carcinomas ex pleomorphic adenoma behave favorably. The two carcinoma types for which grading schemes are common include adenoid cystic carcinoma and mucoepidermoid carcinoma. Adenoid cystic carcinomas are graded based solely on pattern with solid components portending a worse prognosis. Occasionally, adenoid cystic carcinomas may undergo transformation to pleomorphic high grade carcinomas. This feature confers a high propensity for lymph node metastasis and should thus be reported to alert the clinical team. Mucoepidermoid carcinomas are graded in a three tier fashion based on a constellation of features including cystic component, border, mitoses, anaplasia, and perineural invasion among others. All grading schemes are somewhat cumbersome, intimidating and occasionally ambiguous, but evidence suggests that using a scheme consistently shows greater reproducibility than using an intuitive approach. The intermediate grade category demonstrates the most variability between grading systems and thus the most controversy in management. In the AFIP system intermediate grade tumors cluster with high grade tumors, while in the Brandwein system, they cluster with low grade tumors.
14 INTRODUCTION: Salivary gland carcinomas comprise only 3-5% of all head and neck malignancies, yet they are the most diverse with at least twenty four different types recognized by the World Health Organization (WHO) [1]. This diversity combined with the rarity of many of the tumor types and the unpredictability in long-term outcome impose a significant challenge on the management of salivary gland malignancies overall.[2] For prognosis and treatment, despite these aforementioned factors, it is critical to resolve these tumors, using both clinical and pathologic parameters, into therapeutically meaningful categories (Table 1).[3] A review of numerous retrospective studies[4] indicates that histologic tumor grade ranks highly among the most important predictors of outcome for salivary gland carcinomas. High grade salivary carcinomas have a 5 year survival of roughly 40% while low and intermediate grade tumors have a 5 year survival of 85-90%.[2, 4] In sizeable series, histologic grade is an independent predictor of outcome in multivariate analysis, but it also tends to correlate with other adverse prognosticators such as size and nodal status. However, the current approach to grading of salivary gland tumors is subject to many deficiencies and challenges that on a case by case basis may not always accurately predict outcome. Here I review current histologic grading as applied to salivary gland carcinomas in general and with respect to select common tumor types. DISCUSSION General Grading of Salivary Gland Carcinomas The ideal requirements for any grading system are as follows: Accurately predicts outcome Can be used to stratify patients into distinct management categories Applicable to all sites in which a tumor can be seen
15 Simple criteria Quick and time efficient Reproducible with minimal inter and intraobserver variability Practically speaking, this ideal is difficult or even impossible to achieve in salivary gland carcinomas mainly because of the lack of sufficient sample size to devise statistically valid systems that fulfill the aforementioned criteria. Meta analyses hold very little meaning since grading of salivary gland carcinomas is not standardized. Most grading is done intuitively using general cytomorphologic features (pleomorphism, mitoses, necrosis) and is thus highly individualized. Even when grading systems exist, there may be several to address the same tumor type, none of which correlate exactly with one another. Despite these obstacles, using the data available, as well as good clinical acumen, the various tumor types can at least be stratified into a meaningful working stratification scheme that can be used to parse tumors into those that do not require treatment beyond excision (i.e. low risk) of primary tumor and those that do (i.e. high risk). Table 2 divides all entities listed in WHO classification scheme into low risk and high risk categories. Histologic grading will additionally split certain tumor types (i.e. mucoepidermoid carcinoma) between both risk categories. Is grading of salivary gland tumors always necessary? The answer is no. Many tumor types are for the most part definitionally high risk both histologically and biologically (i.e. conventional salivary duct carcinoma, squamous cell carcinoma, small cell neuroendocrine carcinoma) or low risk (i.e. epithelialmyoepithelial carcinoma, polymorphous low grade adenocarcinoma). The caveat is that high grade versions of intrinsically low grade tumors do exist as do low grade versions of typically high grade tumors. Both pathologists and clinicians need to be aware of these variants. Thus: The usual example of such a tumor type may not need to be qualified with a grading descriptor. An unusually high or low grade variant of a tumor should be conveyed in the pathologic report.
16 Perhaps the most relevant example of this phenomenon is with carcinoma ex pleomorphic adenoma. Historically and even currently in the clinical literature,[2-4] carcinoma ex pleomorphic adenoma is automatically considered a high grade malignancy. In most cases, this is true with high grade adenocarcinoma, not otherwise specified (NOS), and salivary duct carcinoma being the most common histologic subtype of the carcinomatous component. However, as many as 15% of tumors are low grade and may behave in a more indolent fashion.[5] More recently, there is evidence to suggest that intracapsular carcinoma ex pleomorphic adenoma and minimally invasive carcinoma (<1.5 mm of invasion) ex pleomorphic adenoma are also indolent variants that should not be considered equivalent to the typical carcinoma ex pleomorphic adenoma. Thus carcinoma ex pleomorphic adenoma in current practice is not sufficient as a stand alone diagnosis. Recommendations for reporting on these tumors are: Histologic type/grade Percentage of carcinoma Extend of invasion of the carcinomatous component (intracapsular, minimally invasive, and invasive). For more common malignancies however, grading systems have evolved and applied with some degree of efficacy. The two major named tumor types that are consistently graded in current practice are adenoid cystic carcinoma, and mucoepidermoid carcinoma. Additionally, adenocarcinoma NOS and cystadenocarcinoma, are also typically assigned a grade, though these tumors are not common enough to generate a formal system. Finally, grading of acinic cell carcinomas is somewhat controversial. Typically considered a low risk tumor, many studies suggest an unusually high rate of lymph node metastasis as compared to other low risk tumors. Additionally histologic studies actually point to the ability to stratify these tumors based on cytomorphologic grading parameters[6, 7] suggesting that a grading system is necessary for these tumors. Adenoid Cystic Carcinoma
17 Adenoid cystic carcinoma is a biphasic (composed of ducts and basal/myoepithelial cells) salivary gland malignancy characterized by tubular cribriform and or solid growth patterns. The biologic course of this tumor overall is slow but relentless 5 year survival is favorable at roughly 75 80%, but 15 year survival is poor at about 35%.[8, 9] Adenoid cystic carcinoma is unusual in that it is cytologically fairly monomorphic, yet locally quite aggressive placing it in a high risk category with regard to the use of adjuvant radiation. In contrast, the likelihood of lymph node involvement may be as low as 5%, and many institutions consider this tumor low risk for lymph node metastases and thus do not perform neck dissection if clinicoradiographically node negative.[3] Grading of adenoid cystic carcinoma has been shown to be prognostically useful in several series.[9-11] Unlike many grading schemes, adenoid cystic carcinoma grading quick and simple in that it is based solely on growth pattern. As early as 1958, Patey and Thackray[12] noted that a solid growth pattern imparts a poor prognosis. Subsequently, grading of this tumor has evolved into stratification into three grades of increasing aggressiveness based on predominant growth pattern: [10, 11] grade 1: tubular, grade 2: cribriform, grade 3: solid. Generally, a tumor with a greater than 30% solid component belongs in the grade 3 category. However, it is suggested that any solid component imparts a poor prognosis, and that the relationship between solid growth pattern percentage and prognosis is somewhat linear and that assigning a cut-off may be arbitrary. The current WHO classification refers to tumors by predominant pattern rather than actually assigning a numeric grade. One of the controversies surrounding grading of adenoid cystic carcinoma is its prognostic utility independent of tumor stage. Spiro et al [8] suggest that this is not the case, however, more recently, da Cruz Perez et al [13] show that grade is an independent prognosticator on multivariate analysis. One potential difference that the grading scheme used by Spiro et al[8] differs from the typical scheme particularly with regards to a solid component cutoff of over >50%. The difficulties in conversion between the two grading schemes are illustrated in Table 3. Reproducibility of grading in adenoid cystic carcinoma
18 has not been well addressed in the literature. In one study,[14] ironically, the grading system used by Spiro et al[8] has less interobserver variability. While prognostically useful, it is unclear whether grading of adenoid cystic carcinoma is useful in patient management. Regardless of grade, all adenoid cystic carcinomas are treated with surgery plus irradiation because locally they are aggressive and high risk. With regard to the neck, most decisions on the neck dissection will not depend on grade, though there is some evidence to suggest that solid/grade 3 adenoid cystic carcinomas have a higher likelihood of lymph node metastasis.[3] With regards to this point, the rare phenomenon of dedifferentiation or high grade transformation may have relevance. Adenoid cystic carcinoma with high grade transformation refers to the presence of a pleomorphic mitotically active high grade carcinoma component arising in an otherwise conventional adenoid cystic carcinoma of any pattern/grade.[15] The transformed component is typically of a purely ductal phenotype with a solid or cribriform appearance. Unlike conventional adenoid cystic carcinoma, which is characterized by small, hyperchromatic, monomorphic nuclei, and scant cytoplasm, transformed components show prominent nuclear size and chromatin variability. Common features include fibrocellular desmoplasia, abundant mitoses, necrosis, and microcalcifications. Unique patterns in high grade transformation include micropapillary and squamoid growth. However, there is still morphologic overlap between solid conventional adenoid cystic carcinoma and high grade transformation and the transition from conventional adenoid cystic to high grade transformation is often gradual. Table 4 delineates key distinguishing features between solid conventional adenoid cystic carcinoma and adenoid cystic carcinoma with high grade transformation. Basically, the aggressive nuclear, stromal, architectural and immunohistochemical features common to both variants are more exaggerated in high grade transformation, while solid conventional adenoid cystic carcinoma shows only slight deviation from tubular or cribriform conventional adenoid cystic carcinoma. These tumors have an exceptionally poor prognosis with a median survival ranging from months, and may thus be even more aggressive that solid or grade 3 adenoid cystic carcinoma. Unlike
19 conventional adenoid cystic carcinoma, this tumor has a lymph node metastatic rate of over 50%. Thus if a transformed component is found in an adenoid cystic carcinoma, a neck dissection is likely warranted. Summary Recommendations for Grading of Adenoid Cystic Carcinoma: Report predominant growth pattern (tubular, cribriform, or solid) If any solid component is present give rough estimate of percentage o It may be reasonable to indicate in a comment that a solid component >30% correlates with aggressive behavior. If evidence of high grade transformation is present, this should be reported and quantitated. o A comment regarding the unusually high propensity for lymph node involvement is recommended. Mucoepidermoid Carcinoma Mucoepidermoid carcinoma is the most common salivary gland malignancy and is histologically comprised of a mixture of mucus cells, intermediate cells and squamoid or epidermoid cells. This tumor may also demonstrate clear cell, oncocytic or columnar cells. There is arguably no other salivary gland tumor in which grading is as important to prognosis and therapy. The reported overall 5 year survival for MEC ranges from 92 to 100% for low grade tumors, 62 to 92% for intermediate grade tumors, and 0 to 43% for high grade tumors.[16] A few recent studies have also highlighted the value of grade in the management of patients. [17, 18] Low grade tumors generally require only surgical treatment, while high grade tumors require adjuvant radiation and neck dissection. The controversy arises in the management of intermediate grade mucoepidermoid carcinoma, and perhaps the root of this controversy lies within the grading system employed. Even when described initially by Stewart et al [19] in 1945, two types of mucoepidermoid carcinoma were documented, a benign and malignant version which equate today to low and high grade respectively. Shortly thereafter, the potential need for an intermediate category was recognized.[20] Today, mucoepidermoid are carcinoma graded by most using three tiers: low, intermediate and high grade. The
20 three most popular grading systems are: the AFIP grading system[21], modified Healey system[22], and the Brandwein [23] system (Table 5). All categories assess a similar set of parameters, both cytomorphologic and architectural, and may also include perineural and angiolymphatic invasion. Both the AFIP and Brandwein system are point based, assigning point values to each adverse histologic parameters and with ascending point scores equating to a higher grade. The modified Healey system can be considered a best fit type system: certain histologic parameters characterize a particular grade, and a tumor is graded based on its predominant morphologic features. Grading of mucoepidermoid carcinoma is not without flaws. One clear deficiency in all systems, particularly the point based schemes, the difficulty in application. Grading under these systems is a cumbersome and time consuming activity, and many of the criteria are not at all well-defined. In fact, based on personal experience, if asked, most pathologists tend not to use a formal system because of the time commitment and lack of user friendliness. However, evidence suggests that the reproducibility of an informal or personal grading scheme is lower than when a standard grading scheme is used.[23, 24]. Given an adequate sample size, all systems appear to be prognostically useful even independent of stage. However, the way in which each system correlates with outcome varies. The AFIP system appears to down grade tumors while the Brandwein system appears to upgrade tumors.[24] While these differences appear minor prognostically, therapeutically they have significant implications. The clinical expectation of a low grade mucoepidermoid carcinoma is that it is a low risk tumor that is almost always cured by surgery alone and has a negligible lymph node metastatic rate. Here the danger of the AFIP system is potentially placing biologically more aggressive tumors into this low grade category increasing the failure rate of low grade tumors. Conversely, high grade mucoepidermoid carcinomas are aggressive tumors requiring adjuvant treatment and neck dissection. The concern with the Brandwein system is that it may place some indolent tumors in this high risk category, in which case some patients may receive unnecessary radiation or additional surgery.
21 The differences in grading schemes are amplified particularly with respect to intermediate grade tumors. There does not appear to be a clear cut answer on the management of patients in this category, but the few studies addressing this question on a single institution yield varying results. Aro et al [17] using the AFIP system suggest that intermediate grade mucoepidermoid carcinoma cluster with high grade mucoepidermoid carcinoma, and should be treated in a similar fashion. However, Nance et al [18] showed that intermediate grade mucoepidermoid carcinoma cluster with low grade mucoepidermoid carcinoma using the Brandwein system. Based on limited experience, the Healey system does not seem to have either of these limitations, but since intermediate grade tumors using this system literally behave in a fashion that is intermediate to low and high grade, management may be even more ambiguous than with the other systems. Finally, variants of mucoepidermoid carcinoma such as oncocytic or sclerosing variants may not be amenable to conventional grading schemes. Limited evidence to date suggests that even oncocytic mucoepidermoid carcinomas that are considered high grade by a conventional grading scheme may behave indolently, with only one recurrence noted.[25] However, evidence is still insufficient to make a firm recommendation to discard grading for these variants. Thus current recommendations for grading mucoepidermoid carcinomas are: Utilize a standard scheme, rather than an intuitive approach. (As a more streamlined well defined system evolves that still retains predictive value, this notion may become more palatable). Regarding which system to use, understanding of the clinical expectations is necessary. In most practices in the United States, it is less acceptable for a low grade tumor to behave in an aggressive fashion than for a high grade tumor to behave indolently and possibly get overtreatment. Thus, the utilization of the Brandwein system or Healey system is preferable. Variants should still be graded in a similar fashion although limited evidence suggests that some variants may behave more indolently even if technically high grade. CONCLUSIONS
22 Though histologic grading of salivary gland carcinomas is somewhat flawed, it does have prognostic value. Carcinoma ex pleomorphic adenoma should no longer be considered a specific diagnosis, but rather, a category in which the carcinoma should be typed, graded and quantitated to impart more prognostically and therapeutically relevant data. The two tumor types for which specific grading systems have evolved are adenoid cystic carcinoma and mucoepidermoid carcinoma. Adenoid cystic carcinoma is graded based on growth pattern with solid growth imparting a poorer prognosis. Rarely, these tumors will undergo high grade transformation in which case the tumor will have a much higher predilection for lymph node metastases than a conventional adenoid cystic carcinoma. In mucoepidermoid carcinomas, standardized grading systems are more reproducible than generic grade assignment, but in their current form, they are cumbersome and time consuming. The outcome in the intermediate grade category is heavily dependent on the grading system used and is thus the most controversial with regards to management and prognosis. The AFIP system downgrades tumors leading to aggressive behavior in the intermediate grade category while the Brandwein system upgrades tumors resulting in indolent behavior.
23 REFERENCES: 1. Eveson JW, Auclair PL, Gnepp DR, et al. Tumors of the salivary glands: Introduction. In: Barnes EL, Eveson JW, Reichart P, Sidransky D, eds. World Health Organization Classification of Tumours: Pathology & Genetics. Head and Neck Tumours. Lyon: IARCPress; 2005: Bell RB, Dierks EJ, Homer L, et al. Management and outcome of patients with malignant salivary gland tumors. J Oral Maxillofac Surg. Jul 2005;63(7): Myers EN, Ferris RL, eds. Salivary gland disorders. Berlin: Springer; Lima RA, Tavares MR, Dias FL, et al. Clinical prognostic factors in malignant parotid gland tumors. Otolaryngol Head Neck Surg. Nov 2005;133(5): Lewis JE, Olsen KD, Sebo TJ. Carcinoma ex pleomorphic adenoma: pathologic analysis of 73 cases. Hum Pathol. Jun 2001;32(6): Lewis JE, Olsen KD, Weiland LH. Acinic cell carcinoma. Clinicopathologic review. Cancer. Jan ;67(1): Michal M, Skalova A, Simpson RH, et al. Well-differentiated acinic cell carcinoma of salivary glands associated with lymphoid stroma. Hum Pathol. May 1997;28(5): Spiro RH, Huvos AG. Stage means more than grade in adenoid cystic carcinoma. Am J Surg. Dec 1992;164(6): Fordice J, Kershaw C, El-Naggar A, et al. Adenoid cystic carcinoma of the head and neck: predictors of morbidity and mortality. Arch Otolaryngol Head Neck Surg. Feb 1999;125(2): Perzin KH, Gullane P, Clairmont AC. Adenoid cystic carcinomas arising in salivary glands: a correlation of histologic features and clinical course. Cancer. Jul 1978;42(1): Szanto PA, Luna MA, Tortoledo ME, et al. Histologic grading of adenoid cystic carcinoma of the salivary glands. Cancer. Sep ;54(6): Patey DH, Thackray AC. The treatment of parotid tumours in the light of a pathological study of parotidectomy material. Br J Surg. Mar ;45(193): da Cruz Perez DE, de Abreu Alves F, Nobuko Nishimoto I, et al. Prognostic factors in head and neck adenoid cystic carcinoma. Oral Oncol. Oct Therkildsen MH, Reibel J, Schiodt T. Observer variability in histological malignancy grading of adenoid cystic carcinomas. Apmis. Jul 1997;105(7): Seethala RR, Hunt JL, Baloch ZW, et al. Adenoid cystic carcinoma with highgrade transformation: a report of 11 cases and a review of the literature. Am J Surg Pathol. Nov 2007;31(11): Ellis G, Auclair P, eds. Tumors of the salivary glands. (3rd Series ed). Washington DC: Armed Forces Institute of Pathology; 1996 Atlas of tumor pathology; No. 17.
24 17. Aro K, Leivo I, Makitie AA. Management and outcome of patients with mucoepidermoid carcinoma of major salivary gland origin: a single institution's 30-year experience. Laryngoscope. Feb 2008;118(2): Nance MA, Seethala RR, Wang Y, et al. Treatment and survival outcomes based on histologic grading in patients with head and neck mucoepidermoid carcinoma. Cancer. Oct ;113(8): Stewart FW, Foote FW, Becker WF. Mucoepidermoid tumors of salivary glands. Ann Surg. 1945;122: Foote FW, Jr., Frazell EL. Tumors of the major salivary glands. Cancer. Nov 1953;6(6): Goode RK, Auclair PL, Ellis GL. Mucoepidermoid carcinoma of the major salivary glands: clinical and histopathologic analysis of 234 cases with evaluation of grading criteria. Cancer. Apr ;82(7): Batsakis JG, Luna MA. Histopathologic grading of salivary gland neoplasms: I. Mucoepidermoid carcinomas. Ann Otol Rhinol Laryngol. Oct 1990;99(10 Pt 1): Brandwein MS, Ferlito A, Bradley PJ, et al. Diagnosis and classification of salivary neoplasms: pathologic challenges and relevance to clinical outcomes. Acta Otolaryngol. Oct 2002;122(7): Seethala RR, Hoschar AP, Bennett A, et al. Reproducibility of grading in salivary gland mucoepidermoid carcinoma and correlation with outcome: Does system really matter? Mod Pathol. 2008;21(S1):241A. 25. Weinreb I, Seethala RR, Perez-Ordonez B, et al. Oncocytic Mucoepidermoid Carcinoma: Clinicopathologic Description in a Series of 12 Cases. Am J Surg Pathol. Oct
25 Table 1. General categories of management of primary salivary gland carcinomas[3] Surgery Surgery and radiotherapy Additional neck dissection Systemic chemotherapy alone Negative margins Low grade histology Low risk (non angioinvasive, non infiltrative) histologic subtype Low T stage (T1 or T2) Close (<2mm) or positive margins High grade histology High risk (highly infiltrative) histologic subtype High T stage (T3 or T4) pn+ Perineural invasion* All cn+ cn0 but high grade histology cn0 but high risk (angioinvasive) histologic subtype cn0 but high T stage ( T3 or T4) Metastatic or unresectable disease T = tumor stage in TNM classification cn+ = clinically node positive cn0 = clinically node negative pn+ = pathologically node positive *somewhat controversial depending on tumor type
26 Table 2: Risk stratification of WHO[1] recognized salivary gland malignancies Low risk High Risk Acinic cell carcinoma Sebaceous carcinoma and lymphadenocarcinoma Low grade Mucoepidermoid carcinoma* High grade Mucoepidermoid carcinoma* Epithelial-myoepithelial carcinoma Adenoid cystic carcinoma** Polymorphous low grade adenocarcinoma Mucinous adenocarcinoma Clear cell carcinoma Squamous cell carcinoma Basal cell adenocarcinoma Small cell carcinoma Low grade salivary duct carcinoma (low grade Large cell carcinoma cribriform cystadenocarcinoma) Myoepithelial Carcinoma Lymphoepithelial carcinoma Oncocytic Carcinoma Metastasizing Pleomorphic adenoma Carcinoma ex Pleomorphic adenoma (intracapsular/minimally invasive or with low grade Carcinoma ex Pleomorphic adenoma (widely invasive or high grade histology) histology) Sialoblastoma Carcinosarcoma Adenocarcinoma NOS and Cystadenocarcinoma, low grade* Adenocarcinoma and Cystadenocarcinoma, NOS, high grade* * Intermediate grade variants of these tumors are controversial in the assignment of risk. For mucoepidermoid carcinoma this may depend on grading scheme used. For adenocarcinoma NOS, there is little data, but what is present suggests that intermediate grade should be placed in the high risk group. ** Adenoid cystic carcinomas are all considered high risk in terms of local recurrence, but only solid adenoid cystic carcinoma (i.e. high pattern grade) is considered high risk for nodal metastasis.
27 Table 3: Comparison of Common Pattern Grading Schemes in Adenoid Cystic Carcinoma Grade Perzin et al[10], Szanto et al[11] Grade Spiro et al[8] 1 Predominantly tubular, no solid component 2 Predominantly cribriform, solid component <30% acceptable 3 Solid component >30% 1 Mostly tubular or cribriform (no stipulations on minor solid components) 2 50% solid 3 Mostly solid
28 Table 4: Comparison of Solid Conventional Adenoid Cystic Carcinoma and High Grade Transformation* Features Solid Conventional Adenoid Cystic Carcinoma Adenoid Cystic Carcinoma with High Grade Transformation Chromatin Dark, homogeneous Vesicular or heterogeneously dispersed Nuclear membranes Delicate Thickened or irregular Nucleoli Present but indistinct Prominent central Nuclear Size At most twice the size of grade I-II ACC nuclei. Uniform size distribution At least 2-3 times the size of grade I-II ACC nuclei (typically more). At least 2 fold nuclear variation Cytoplasm Scant to nearly absent Scant to Moderate Growth Solid nests, rarely spanning more than a 40x high power field high power field Solid confluent nests to sheets often filling a 40x Stroma Paucicellular myxoid or Fibrocellular desmoplastic hyaline Comedonecrosis Focally present, usually punctuate Often present, punctuate to large zones Microcalcifications Rarely present Often Present Unique features Micropapillae, Squamoid areas Mitoses Generally <10/hpf Usually>10/hpf Abluminal cell layer presence by immunohistochemistry Present and complete Ki-67 <50% >50% p53 overexpression (strong reactivity in >50% of cells) Rare Common Bold = Major Features * Adapted from Seethala et al[15] Incomplete and at least focally absent
29 Table 5: Comparison of Grading Systems for Mucoepidermoid Carcinoma Modified Healey [22] AFIP[21] Brandwein[23] Qualitative Point Based Point Based Low Grade Macrocysts, microcysts, transition with excretory ducts Differentiated Mucin producing Epidermoid Cells, often in a 1:1 ration; minimal to moderate intermediate cell population Daughter cyst proliferation from large cysts Minimal to absent pleomorphism, rare mitoses Broad-front, often circumscribed invasion Pools of extravasated mucin with stromal reaction Intermediate Grade No macrocysts, few microcysts, solid nests of cells Large duct not conspicuous Slight to moderate pleomorphism, few mitoses, prominent nuclei and nucleoli Invasive quality, usually well difined and uncircumscribed Chronic inflammation at periphery, fibrosis separates nests of cells and groups of nests High Grade No macrocysts, predominantly solid but may be nearly all glandular Cell constituents range from poorly differentiated to recognizable epidermoid and intermediate to ductal type adenocarcinoma Considerable pleomorphism, easily found mitoses Unquestionable soft tissue, perineural and intravascular invasion Chronic inflammation less prominent, desmoplasia of stroma may outline invasive clusters Intracystic component <20% = 2pts Neural invasion present = 2pts Necrosis present = 3pts Mitosis (4 or more per 10 HPF) = 3pts Anaplasia = 4pts Low Grade = 0-4 pts Intermediate Grade = 5-6 pts HighGrade = 7-14 pts Intracystic component <25% = 2pts Tumor invades in small nests and islands = 2pts Pronounced nuclear atypia = 2pts Lymphatic and/or vascular invasion = 3pts Bony invasion = 3pts >4mitoses per 10 HPF = 3pts Perineural spread = 3pts Necrosis = 3pts Low Grade = 0 pts Intermediate Grade = 2-3 pts High Grade = 4 or more pts
30 Neuroendocrine and Related Neoplasia Selected Diagnostic Problems in the Head and Neck Neuroendocrine and Related Neoplasia Case #1 Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University of Virginia Medical Center Charlottesville, VA A 48-year-old man, non smoker, presented with a 2 cm. supraglottic laryngeal mass. The mass was covered by intact mucosa. A biopsy was performed. Neuroendocrine and Related Neoplasia Neuroendocrine Neoplasms of the Head and Neck Typical Carcinoid of the Larynx Typical carcinoid v. paraganglioma Extremely uncommon tumor, 13 probable cases Predominantly supraglottic larynx 3 with mets to liver, bone, lymph nodes, skin All 3 alive 4 8 years later 1 of 13 patients died of disease El-Naggar & Batsakis, ORL 53:188, 1991 Neuroendocrine Neoplasms of the Head and Neck Paraganglioma of the Larynx Neuroendocrine Carcinoma v. Paraganglioma Diagnostic Features Uncommon tumor, 78 cases reviewed resulted in 34 accepted cases 30 patients with follow-up (mean: 5.2 yrs) 5 local recurrences (limited excision) 1 metastasis (3%) Feature Supraglottic Nesting pattern N.E. markers N.E. Carcinoma Yes Yes Yes Paraganglioma Yes Yes Yes Many purported paragangliomas are well/mod. diff. neuroendocrine carcinomas S100 protein GFAP Cytokeratin no no Yes Yes Yes no Barnes, ORL 53:220, 1991 Pain Yes no 1
31 Neuroendocrine and Related Neoplasia Case #2 A 50-year-old woman presented with a 2 cm. mass in her nose. Neuroendocrine and Related Neoplasia Olfactory Neuroblastoma Unusual Variants Typical carcinoid v. paraganglioma Pituitary adenoma v. olfactory neuroblastoma Pigmented Clear cell Postradiation gangliocytic Rhabdomyoblastic Mixed carcinomatous Ectopic Pituitary Adenoma v. Olfactory Neuroblastoma Diagnostic Features Neuroendocrine and Related Neoplasia Case #3 Feature Pit. Adenoma ONB Location Cytokeratin Rosettes N.E. markers nasopharynx +/- + yes nasal cavity -/+ + yes A 42-year-old man presented with a 2 cm. enlarged cervical lymph node. An excisional biopsy was performed. S100 protein no around nests Pit. Hormones yes no 2
32 Neuroendocrine and Related Neoplasia SNUC v. Lymphoepithelioma v. Basaloid SCCa v. Adenoid Cystic Typical carcinoid v. paraganglioma Pituitary adenoma v. olfactory neuroblastoma SNUC v. lymphoepithelioma v. basaloid squamous cell carcinoma v. adenoid cystic Location Surf. Dyspl. Nucleoli Necrosis Sq. diff. p63 p16 HPV EBER CD117 SMA BSCCa oropharynx* ++ small comedo diffuse ++/- ++/- - focal - SNUC nose/sinus +/- prom. infarctive - +/- focal - - -? - Lymphoep nasopharynx - single +/ diffuse ? - Ad. Cyst. anywhere - absent rare - focal Other Neuroendocrine or Related Diagnostic Problems Neuroendocrine and Related Neoplasia Case #4 Mod. diff. neuroendocrine ca. v. medullary ca. Small cell neuroendocrine ca. NUT midline carcinomas PNET s of the head and neck Dendritic cell tumors Melanoma v. everything else History: 42-year-old woman with a right-sided sinonasal mass extending into the orbit and cranial cavity. Cervical lymph nodes were also enlarged. NUT Midline Carcinoma NUT Midline Carcinoma Epithelial malignancies with characteristic chromosomal translocations and gene fusions are uncommon. In 1991, two cases of carcinoma were described involving the thorax that were shown to have t(15;19) 22 total cases have been described Thirteen of these cases have developed in girls or women Occur over a vast age range (3-78 yrs) and a little more than half the cases have been reported in patients over the age of 20 years Ten cases have involved the head and neck and, of these, 9 have involved the upper aerodigestive tract. Ten other cases have been noted then within the thorax, usually felt to be primary to the mediastinum / thymus (6) 3
33 NUT Midline Carcinoma NUT Midline Carcinoma Most common translocation involving the NUT gene is the t(15;19) (q13;p13.1) Fuses the NUT gene on chromosome 15 to the BRD4 gene In one-third of cases, however, the NUT gene is fused to a different partner gene (NUT variant) (e.g., BRD3 gene at 9q34.2) BRD proteins are known to bind transcriptionally active chromatin and stimulate transcriptional activity Believed that the fusion protein can be localized to the nucleus secondary to its fusion the BRD4 and BRD3 proteins Fusion proteins block epithelial differentiation as si-rna-induced withdrawal of the fusion proteins leads to squamous differentiation and cell cycle arrest NUT Midline Carcinoma NUT Midline Carcinoma Cells have little amphiphilic or eosinophilic cytoplasm Nuclei have irregular contours; tend to be somewhat uniform in size Fine to vesicular chromatin and prominent nucleoli Mitotic figures and apoptotic bodies are common Squamous differentiation may be seen and does not necessarily predict the partner gene Keratinization may appear abrupt, with sheets of immature cells juxtaposed to well-differentiated, mature squamous nests Sometimes cystic Nut Midline Carcinoma NUT Midline Carcinoma Antibody to the NUT protein has been developed, both polyclonal and monoclonal Newer monoclonal antibody has improved function with a sensitivity of 87% and specificity of 100% (AJSP, in press) Epithelial differentiation can almost always be demonstrated with pankeratin immunococktail p63 immunoreactivity is also helpful as it points toward squamous differentiation and was seen in 4 of 5 NMCs that we tested NMCs have not been shown to be associated with carcinoma-related viruses such as EBV and HPV In situ hybridization for these viruses can be used and the identification of the viruses likely excludes the diagnosis of NMC 4
34 The Spectrum of Undiff ENT Carcinomas Neuroendocrine Related Problems in ENT Pathology Take Home Points Nasopharyngeal lymphoepithelioma Sinonasal undifferentiated carcinoma (SNUC) Basaloid squamous cell carcinoma HPV+ Smoking related Solid adenoid cystic carcinoma NUT tumors Small cell carcinoma? Laryngeal carcinoid and paraganglioma may be light microscopically indistinguishable Always consider pituitary adenoma for any mass arising high in the nose. Be wary of diagnosing olfactory neuroblastoma if the tumor does not involve or approach the cribriform plate. SNUC, lymphoepithelioma & HPV+ basaloid squamous cell carcinoma have tremendous morphologic overlap but differ considerably prognostically. Consider p16, p63, HPV-ISH, EBER for distinguishing these entities If cells are small and mitotic rate low, consider solid adenoid cystic ca. HPV neg. basaloid carcinoma -> think about NUT carcinoma 5









35 Neuroendocrine and Related Neoplasia Selected Diagnostic Problems in the Head and Neck Neuroendocrine and Related Neoplasia Case #1 Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University of Virginia Medical Center Charlottesville, VA A 48-year-old man, non smoker, presented with a 2 cm. supraglottic laryngeal mass. The mass was covered by intact mucosa. A biopsy was performed. Neuroendocrine and Related Neoplasia Typical carcinoid v. paraganglioma 1














36 Neuroendocrine Neoplasms of the Head and Neck Typical Carcinoid of the Larynx Normal Laryngeal Paraganglion Extremely uncommon tumor, 13 probable cases Predominantly supraglottic larynx 3 with mets to liver, bone, lymph nodes, skin All 3 alive 4 8 years later 1 of 13 patients died of disease El-Naggar & Batsakis, ORL 53:188, 1991 Paraganglioma Paraganglioma Paraganglioma Paraganglioma S100 CK 2



 Feature Supraglottic Nesting")



37 Neuroendocrine Neoplasms of the Head and Neck Paraganglioma of the Larynx Neuroendocrine Carcinoma v. Paraganglioma Diagnostic Features Uncommon tumor, 78 cases reviewed resulted in 34 accepted cases 30 patients with follow-up (mean: 5.2 yrs) 5 local recurrences (limited excision) 1 metastasis (3%) Feature Supraglottic Nesting pattern N.E. markers N.E. Carcinoma Yes Yes Yes Paraganglioma Yes Yes Yes Many purported paragangliomas are well/mod. diff. neuroendocrine carcinomas S100 protein GFAP Cytokeratin no no Yes Yes Yes no Barnes, ORL 53:220, 1991 Pain Yes no Cytokeratin S-100 Neuroendocrine and Related Neoplasia Case #2 A 50-year-old woman presented with a 2 cm. mass in her nose. 3













38 CK Synapto Neuroendocrine and Related Neoplasia Typical carcinoid v. paraganglioma Pituitary adenoma v. olfactory neuroblastoma FSH 4










39 Olfactory Neuroblastoma Intracranial Extension Olfactory Neuroblastoma Olfactory Neuroblastoma Nested Pattern Olfactory Neuroblastoma Diffuse & vascular Olfactory Neuroblastoma Homer Wright Rosettes Olfactory Neuroblastoma Flexner v. Glandular 5










40 Olfactory Neuroblastoma Olfactory Neuroblastoma Olfactory Neuroblastoma Olfactory Neuroblastoma Olfactory Neuroblastoma Unusual Variants Olfactory Neuroblastoma Pigmented Pigmented Clear cell Postradiation gangliocytic Rhabdomyoblastic Mixed carcinomatous Ectopic 6








41 Olfactory Neuroblastoma Ganglion Cells Olfactory Neuroblastoma Pre-radiation Olfactory Neuroblastoma Post-radiation Olfactory Neuroblastoma Clear Cell Pattern Pituitary Adenoma v. Olfactory Neuroblastoma Diagnostic Features Feature Location Cytokeratin Rosettes N.E. markers S100 protein Pit. Hormones Pit. Adenoma nasopharynx +/- + yes no yes ONB nasal cavity -/+ + yes around nests no Neuroendocrine and Related Neoplasia Case #3 A 42-year-old man presented with a 2 cm. enlarged cervical lymph node. An excisional biopsy was performed. 7












42 CK Neuroendocrine and Related Neoplasia Typical carcinoid v. paraganglioma Pituitary adenoma v. olfactory neuroblastoma SNUC v. lymphoepithelioma v. basaloid squamous cell carcinoma v. adenoid cystic 8


















43 EBER 9














44 p16 HPV 10







45 SNUC v. Lymphoepithelioma v. Basaloid SCCa v. Adenoid Cystic CD117 Location Surf. Dyspl. Nucleoli Necrosis Sq. diff. p63 p16 HPV EBER CD117 SMA BSCCa oropharynx* ++ small comedo diffuse ++/- ++/- - focal - SNUC nose/sinus +/- prom. infarctive - +/- focal - - -? - Lymphoep nasopharynx - single +/ diffuse ? - Ad. Cyst. anywhere - absent rare - focal Other Neuroendocrine or Related Diagnostic Problems Neuroendocrine and Related Neoplasia Case #4 Mod. diff. neuroendocrine ca. v. medullary ca. Small cell neuroendocrine ca. NUT midline carcinomas PNET s of the head and neck Dendritic cell tumors Melanoma v. everything else History: 42-year-old woman with a right-sided sinonasal mass extending into the orbit and cranial cavity. Cervical lymph nodes were also enlarged. 11

 p63 NUT Midline Carcinoma NUT Midline Carcinoma 22 total")
 and a little more than half the")


 (q13;p13.")
46 NUT Midline Carcinoma Epithelial malignancies with characteristic chromosomal translocations and gene fusions are uncommon. In 1991, two cases of carcinoma were described involving the thorax that were shown to have t(15;19) p63 NUT Midline Carcinoma NUT Midline Carcinoma 22 total cases have been described Thirteen of these cases have developed in girls or women Occur over a vast age range (3-78 yrs) and a little more than half the cases have been reported in patients over the age of 20 years Ten cases have involved the head and neck and, of these, 9 have involved the upper aerodigestive tract. Ten other cases have been noted then within the thorax, usually felt to be primary to the mediastinum / thymus (6) Most common translocation involving the NUT gene is the t(15;19) (q13;p13.1) Fuses the NUT gene on chromosome 15 to the BRD4 gene In one-third of cases, however, the NUT gene is fused to a different partner gene (NUT variant) (e.g., BRD3 gene at 9q34.2) 12

47 NUT Midline Carcinoma BRD proteins are known to bind transcriptionally active chromatin and stimulate transcriptional activity Believed that the fusion protein can be localized to the nucleus secondary to its fusion the BRD4 and BRD3 proteins Fusion proteins block epithelial differentiation as si-rna-induced withdrawal of the fusion proteins leads to squamous differentiation and cell cycle arrest NUT Midline Carcinoma NUT Midline Carcinoma Cells have little amphiphilic or eosinophilic cytoplasm Nuclei have irregular contours; tend to be somewhat uniform in size Fine to vesicular chromatin and prominent nucleoli Mitotic figures and apoptotic bodies are common Squamous differentiation may be seen and does not necessarily predict the partner gene Keratinization may appear abrupt, with sheets of immature cells juxtaposed to welldifferentiated, mature squamous nests Sometimes cystic NUT Midline Carcinoma Nut Midline Carcinoma React with antibodies to keratins and p63 Most tumors are immunoreactive with antibody to CK7 and focal immunoreactivity with antibody to CK20 is sometimes seen CD34 immunoreactivity was seen in a little more than half the cases Immunoreactivity with other antigens expressed in small blue cells tumors of childhood has not been noted Evidence of Epstein-Barr virus has not been identified by FISH (EBER) Antibody to the NUT protein has been developed, both polyclonal and monoclonal Newer monoclonal antibody has improved function with a sensitivity of 87% and specificity of 100% (AJSP, in press) 13


48 NUT Midline Carcinoma NUT immunohistochemistry: Top-intact NUT; Bottom- rearranged NUT FISH may currently be the diagnostic test needed for the establishment of a diagnosis Probes have been developed for the regions flanking the typical break point of the NUT gene on chromosome 15 and for the typical breakpoints with BRD4 and BRD3, however, they are not commercially available Primers are also developed for both known fusion proteins, however they are also not currently commercially available NUT Midline Carcinoma The Spectrum of Undiff ENT Carcinomas Epithelial differentiation can almost always be demonstrated with pankeratin immunococktail p63 immunoreactivity is also helpful as it points toward squamous differentiation and was seen in 4 of 5 NMCs that we tested NMCs have not been shown to be associated with carcinoma-related viruses such as EBV and HPV In situ hybridization for these viruses can be used and the identification of the viruses likely excludes the diagnosis of NMC Nasopharyngeal lymphoepithelioma Sinonasal undifferentiated carcinoma (SNUC) Basaloid squamous cell carcinoma HPV+ Smoking related Solid adenoid cystic carcinoma NUT tumors Small cell carcinoma? Other Neuroendocrine or Related Diagnostic Problems Neuroendocrine Related Problems in ENT Pathology Take Home Points Mod. diff. neuroendocrine ca. v. medullary ca. Small cell neuroendocrine ca. NUT midline carcinomas an entity? PNET s of the head and neck Dendritic cell tumors Melanoma v. everything else Laryngeal carcinoid and paraganglioma may be light microscopically indistinguishable Always consider pituitary adenoma for any mass arising high in the nose. Be wary of diagnosing olfactory neuroblastoma if the tumor does not involve or approach the cribriform plate. SNUC, lymphoepithelioma & HPV+ basaloid squamous cell carcinoma have tremendous morphologic overlap but differ considerably prognostically. Consider p16, p63, HPV-ISH, EBER for distinguishing these entities If cells are small and mitotic rate low, consider solid adenoid cystic ca. HPV neg. basaloid carcinoma -> think about NUT carcinoma 14
The Changing Face of Head and Neck Cancer in the 21st Century: The Impact of HPV on the Epidemiology and Pathology of Oral Cancer. William H.
 The Changing Face of Head and Neck Cancer in the 21st Century: The Impact of HPV on the Epidemiology and Pathology of Oral Cancer William H. Westra From the Department of Pathology and Otolaryngology/Head
The Changing Face of Head and Neck Cancer in the 21st Century: The Impact of HPV on the Epidemiology and Pathology of Oral Cancer William H. Westra From the Department of Pathology and Otolaryngology/Head
An Update on Grading of Salivary Gland Carcinomas
 Head and Neck Pathol (2009) 3:69 77 DOI 10.1007/s12105-009-0102-9 PROCEEDINGS OF THE 2009 NORTH AMERICAN SOCIETY OF HEAD AND NECK PATHOLOGY COMPANION MEETING ( BOSTON, MA) An Update on Grading of Salivary
Head and Neck Pathol (2009) 3:69 77 DOI 10.1007/s12105-009-0102-9 PROCEEDINGS OF THE 2009 NORTH AMERICAN SOCIETY OF HEAD AND NECK PATHOLOGY COMPANION MEETING ( BOSTON, MA) An Update on Grading of Salivary
HPV Analysis of Head and Neck Squamous Cell Carcinomas based on Fine-Needle. Aspiration Specimens. William H. Westra M.D.
 HPV Analysis of Head and Neck Squamous Cell Carcinomas based on Fine-Needle Aspiration Specimens William H. Westra M.D. The Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore Maryland
HPV Analysis of Head and Neck Squamous Cell Carcinomas based on Fine-Needle Aspiration Specimens William H. Westra M.D. The Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore Maryland
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
USCAP 2012: Companion Meeting of the AAOOP. Update on lacrimal gland neoplasms: Molecular pathology of interest
 USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Reporting HPV related carcinomas of the head and neck. dr. Nina Zidar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia
 Reporting HPV related carcinomas of the head and neck dr. Nina Zidar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia Conflict of interest/funding X None Company: Product royalties
Reporting HPV related carcinomas of the head and neck dr. Nina Zidar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia Conflict of interest/funding X None Company: Product royalties
Basaloid neoplasms of the head and neck. Basaloid SCC. Clinico-pathologic features 5/5/11. Basaloid Tumors Head and Neck
 Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Small Cell Carcinoma ex-pleomorphic Adenoma of the Parotid Gland
 Head and Neck Pathol (2012) 6:502 506 DOI 10.1007/s12105-012-0376-1 CASE REPORT Small Cell Carcinoma ex-pleomorphic Adenoma of the Parotid Gland Ashley Cimino-Mathews Brian M. Lin Steven S. Chang Kofi
Head and Neck Pathol (2012) 6:502 506 DOI 10.1007/s12105-012-0376-1 CASE REPORT Small Cell Carcinoma ex-pleomorphic Adenoma of the Parotid Gland Ashley Cimino-Mathews Brian M. Lin Steven S. Chang Kofi
HPV and Head and Neck Cancer: What it means for you and your patients
 HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
Head and Neck SCC. HPV in Tumors of the Head and Neck. Overview. Role of HPV in Pathogenesis of Head & Neck Tumors
 HPV in Tumors of the Head and Neck Christina Kong, M.D. Associate Professor, Stanford Dept of Pathology Director, Cytopathology Laboratory & Cytopathology Fellowship ckong@stanford.edu Head and Neck SCC
HPV in Tumors of the Head and Neck Christina Kong, M.D. Associate Professor, Stanford Dept of Pathology Director, Cytopathology Laboratory & Cytopathology Fellowship ckong@stanford.edu Head and Neck SCC
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
Human Papillomavirus and Head and Neck Cancer. Ed Stelow, MD
 Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu
 Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Human Papillomavirus Testing in Head and Neck Carcinomas
 Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
See the latest estimates for new cases of salivary gland cancers in the US and what research is currently being done.
 About Salivary Gland Cancer Overview and Types If you have been diagnosed with salivary gland cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to
About Salivary Gland Cancer Overview and Types If you have been diagnosed with salivary gland cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to
Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017
 Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017 Dr Mary Toner Consultant Pathologist St James Hospital Trinity College
Salivary gland neoplasms: an update 29th Annual Meeting of Arab Division of the International Academy of Pathology MUSCAT, OMAN 2017 Dr Mary Toner Consultant Pathologist St James Hospital Trinity College
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland
 Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
Molecular Diagnostics of Head and Neck Tumors Justin A. Bishop, M.D. Associate Professor of Pathology The Johns Hopkins University Baltimore, Maryland Two Main Topics Molecular insights in salivary gland
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Sarcomatoid (spindle cell) carcinoma of the cricopharynx presenting as dysphagia
 carcinoma of the cricopharynx presenting as dysphagia") Case Report Sarcomatoid (spindle cell) carcinoma of the cricopharynx presenting as dysphagia Jagtap Sunil V. 1, Shukla Dhirajkumar B. 2, Jagtap Swati S. 3, Havle Abhay D. 4 1 Associate Professor, Department
Case Report Sarcomatoid (spindle cell) carcinoma of the cricopharynx presenting as dysphagia Jagtap Sunil V. 1, Shukla Dhirajkumar B. 2, Jagtap Swati S. 3, Havle Abhay D. 4 1 Associate Professor, Department
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
A 60-year old Man with Left Jaw Mass. Simon Chiosea, MD University of Pittsburgh medical Center 3/15/2016
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
ORIGINAL ARTICLE. Polymorphous Low-Grade Adenocarcinoma. Raja R. Seethala, MD; Jonas T. Johnson, MD; E. Leon Barnes, MD; Eugene N.
 ORIGINAL ARTICLE Polymorphous Low-Grade Adenocarcinoma The University of Pittsburgh Experience Raja R. Seethala, MD; Jonas T. Johnson, MD; E. Leon Barnes, MD; Eugene N. Myers, MD Objective: To reappraise
ORIGINAL ARTICLE Polymorphous Low-Grade Adenocarcinoma The University of Pittsburgh Experience Raja R. Seethala, MD; Jonas T. Johnson, MD; E. Leon Barnes, MD; Eugene N. Myers, MD Objective: To reappraise
Dysplasia, Mimics and Other Controversies
 Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Head and Neck Squamous Subtypes
 1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
Spinal Cord Compression caused by Metastatic Epithelial Myoepithelial Carcinoma of the Parotid Gland
 Spinal Cord Compression caused by Metastatic Epithelial Myoepithelial Carcinoma of the Parotid Gland Pages with reference to book, From 249 To 250 Irshad N. Soomro,Akber S. Hussainy,Rashida Ahmed,Sheema
Spinal Cord Compression caused by Metastatic Epithelial Myoepithelial Carcinoma of the Parotid Gland Pages with reference to book, From 249 To 250 Irshad N. Soomro,Akber S. Hussainy,Rashida Ahmed,Sheema
3/28/2017. Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center
 Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
Head and Neck/Endocrine Pathology Specialty Conference Case 4 Raja R. Seethala, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Mammary analogue secretory carcinoma of salivary gland A case report of new entity
 Case Report Mammary analogue secretory carcinoma of salivary gland A case report of new entity Vaibhav Bhika Bari 1*, Sandhya Unmesh Bholay 2 1 Assistant Professor, 2 Associate Professor Rajiv Gandhi Medical
Case Report Mammary analogue secretory carcinoma of salivary gland A case report of new entity Vaibhav Bhika Bari 1*, Sandhya Unmesh Bholay 2 1 Assistant Professor, 2 Associate Professor Rajiv Gandhi Medical
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Salivary Gland FNA ATYPICAL : Criteria and Controversies
 Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
chapter 4. The effect of oncogenic HPV on transformation zone epithelium
 chapter 4. The effect of oncogenic HPV on transformation zone epithelium CHAPTER 1 All squamous cervical cancer (and probably all cervical adenocarcinoma) is associated with oncogenic HPV, and the absence
chapter 4. The effect of oncogenic HPV on transformation zone epithelium CHAPTER 1 All squamous cervical cancer (and probably all cervical adenocarcinoma) is associated with oncogenic HPV, and the absence
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY. F ZAHRA ALY, MD, PhD
 ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Proliferative Breast Disease: implications of core biopsy diagnosis. Proliferative Breast Disease
 Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
CASE REPORT Malignant transformation of breast ductal adenoma: a diagnostic pitfall
 Malaysian J Pathol 2015; 37(3) : 281 285 CASE REPORT Malignant transformation of breast ductal adenoma: a diagnostic pitfall Hiroko HAYASHI, Hiroshi OHTANI,* Junzo YAMAGUCHI,** and Isao SHIMOKAWA Department
Malaysian J Pathol 2015; 37(3) : 281 285 CASE REPORT Malignant transformation of breast ductal adenoma: a diagnostic pitfall Hiroko HAYASHI, Hiroshi OHTANI,* Junzo YAMAGUCHI,** and Isao SHIMOKAWA Department
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Small (and large) Blue Cell Tumors of the Skull Base
 Blue Cell Tumors of the Skull Base") Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Resident Short Reviews. Adenoid Cystic Carcinoma. Jesse Jaso, MD; Reenu Malhotra, MD
 Resident Short Reviews N Adenoid cystic carcinoma is a malignant tumor with a deceptively benign histologic appearance characterized by indolent, locally invasive growth with high propensity for local
Resident Short Reviews N Adenoid cystic carcinoma is a malignant tumor with a deceptively benign histologic appearance characterized by indolent, locally invasive growth with high propensity for local
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT
 NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT Shu-Yu Tai, 1 Chen-Yu Chien, 2 Chih-Feng Tai, 2,4 Wen-Rei Kuo, 2,4 Wan-Ting Huang, 3 and Ling-Feng Wang 2,4 Departments of 1 Family Medicine, 2 Otolaryngology
NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT Shu-Yu Tai, 1 Chen-Yu Chien, 2 Chih-Feng Tai, 2,4 Wen-Rei Kuo, 2,4 Wan-Ting Huang, 3 and Ling-Feng Wang 2,4 Departments of 1 Family Medicine, 2 Otolaryngology
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Triple Negative Breast Cancer
 Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Enterprise Interest None
 Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
3/27/2017. Pulmonary Pathology Specialty Conference. Disclosure of Relevant Financial Relationships. Clinical History:
 Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland
 The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
Evening Specialty Conference: Cytopathology
 : Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
: Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
Histological Type. Morphological and Molecular Typing of breast Cancer. Nottingham Tenovus Primary Breast Cancer Study. Survival (%) Ian Ellis
 Ian Ellis") Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Prognostic factors affecting the clinical outcome of carcinoma ex pleomorphic adenoma in the major salivary gland
 Zhao et al. World Journal of Surgical Oncology 2013, 11:180 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access Prognostic factors affecting the clinical outcome of carcinoma ex pleomorphic adenoma
Zhao et al. World Journal of Surgical Oncology 2013, 11:180 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access Prognostic factors affecting the clinical outcome of carcinoma ex pleomorphic adenoma
Notice of Faculty Disclosures
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF SQUAMOUS CYSTS OF THE HEAD AND
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF SQUAMOUS CYSTS OF THE HEAD AND
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22
 Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22 History of ITET/CASTLE First Report Gross Appearance and Prognosis 1) Miyauchi A et al: Intrathyroidal epithelial
Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22 History of ITET/CASTLE First Report Gross Appearance and Prognosis 1) Miyauchi A et al: Intrathyroidal epithelial
Polymorphous Low-Grade. December 5 th, 2008
 Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Rare Presentation Of Adenoidcystic Carcinoma Of External Auditory Canal With Subcutaneous Metastasis In Temporal Region
 ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 13 Number 2 Rare Presentation Of Adenoidcystic Carcinoma Of External Auditory Canal With Subcutaneous Metastasis In Temporal Region S Kaushik,
ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 13 Number 2 Rare Presentation Of Adenoidcystic Carcinoma Of External Auditory Canal With Subcutaneous Metastasis In Temporal Region S Kaushik,
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
3/24/2017. Disclosure of Relevant Financial Relationships. Mixed Epithelial Endometrial Carcinoma. ISGyP Endometrial Cancer Project
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Review of the AP Part II Practical Examination. Dr David Clift Co Chief Examiner
 Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
4/17/2015. Case 1. A 37 year old man with a 2.2 cm solitary left thyroid mass.
 Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Oncocytic carcinoma: A rare malignancy of the parotid gland
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
Carcinoma ex Pleomorphic Adenoma (CXPA)-A rare parotid malignancy
-A rare parotid malignancy") Indian Journal of Mednodent and Allied Sciences, pp- 54-58 Indian journals.com Case Report Carcinoma ex Pleomorphic Adenoma (CXPA)-A rare parotid malignancy Vani Padmaja GJ 1 *, Sireesha A 2, Sunderi Devi
Indian Journal of Mednodent and Allied Sciences, pp- 54-58 Indian journals.com Case Report Carcinoma ex Pleomorphic Adenoma (CXPA)-A rare parotid malignancy Vani Padmaja GJ 1 *, Sireesha A 2, Sunderi Devi
Educational Cases EQA November T.J. Palmer Raigmore Hospital Inverness
 Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Cytokeratin immunoprofile of primary and metastatic adenoid cystic carcinoma of salivary glands: a report of two cases
 Article / Clinical Case Report Cytokeratin immunoprofile of primary and metastatic adenoid cystic carcinoma of salivary glands: a report of two cases Cibele Pidorodeski Nagano a, Cláudia Malheiros Coutinho-Camillo
Article / Clinical Case Report Cytokeratin immunoprofile of primary and metastatic adenoid cystic carcinoma of salivary glands: a report of two cases Cibele Pidorodeski Nagano a, Cláudia Malheiros Coutinho-Camillo
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
University Journal of Pre and Para Clinical Sciences
 ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
Carcinoma ex Pleomorphic Adenoma on Right Parotid Gland: A Case Report. School of Dentistry, Kyungpook National University
 Korean Journal of Oral and Maxillofacial Pathology 2017;41(4):189-194 ISSN:1225-1577(Print); 2384-0900(Online) Available online at http://journal.kaomp.org https://doi.org/10.17779/kaomp.2017.41.4.006
Korean Journal of Oral and Maxillofacial Pathology 2017;41(4):189-194 ISSN:1225-1577(Print); 2384-0900(Online) Available online at http://journal.kaomp.org https://doi.org/10.17779/kaomp.2017.41.4.006