Calcium Conundrums. California Chapter AACE. September 2015
|
|
|
- Eileen Green
- 5 years ago
- Views:
Transcription

1 Calcium Conundrums California Chapter AACE September 2015 Michael W. Yeh, MD Chief, Section of Endocrine Surgery Associate Professor of Surgery and Medicine David Geffen School of Medicine at UCLA
2 Case #1: Familial Hypercalcemia 50 y/o female Known history of Familial Hypocalciuric Hypercalcemia (FHH) 1-year history of increasing serum calcium and PTH levels
3 Legend Legend Male Male Female Female Deceased Deceased Proband Proband Affected Affected Fig. 1. Family pedigree demonstrating the pattern of inheritance (black markers) and relationship to the proband (arrow).
4 Legend Male Female Deceased Proband Affected
5 Lab History 2/10 3/10 8/10 9/10 12/10 Calcium: (Ionized) 11.1 (6.2) 10.5 (6.9) 11.2 (6.2) PTH: (pg/ml) Urine Ca: (mg/24 hr) Vitamin D: (pg/ml)
6 Is further workup indicated?
7 Lab History 2/10 3/10 8/10 9/10 12/10 Calcium: (Ionized) 11.1 (6.2) 10.5 (6.9) 11.2 (6.2) PTH: (pg/ml) Urine Ca: (mg/24 hr) Vitamin D: (pg/ml)
8 Further Imaging?
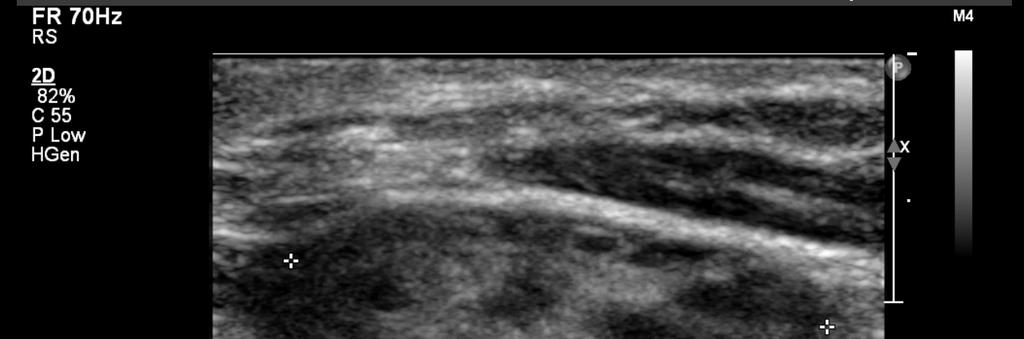
 and sagittal (B)")

9 Neck Ultrasound 0.75 cm Fig. Axial (A) and sagittal (B) views of left lower lobe parathyroid adenoma on focused ultrasound.

10 Sestamibi Scan
11 Would YOU operate?
12 Furthermore What operation would you do? Focused? Unilateral? Bilateral? Measure of success? Interpretation of postoperative surveillance?
 80 70 60 50 40 30 20")
13 607 mg inferior parathyroid adenoma Superior gland normal Surgical Findings Appropriate decrease in IOPTH PTH (pg/ml)
14 Postoperative Surveillance Serum Calcium: 10.7 mg/dl Serum PTH: 32 pg/ml 24-hour urine calcium: 105 mg/24 hours Vitamin D: 38 pg/ml
15 Diagnosis?
16 Primary Hyperparathyroidism AND Familial Hypocalciuric Hypercalcemia
17 Case #2: A Pregnant Dilemma 21 year old G1P0 woman at 14 weeks gestation initially referred to UCLA in April 2012 for hypercalcemia Significant hyperemesis Seen in ER for dehydration Calcium markedly elevated at 12.3
18 Past Medical History Primary hyperparathyroidism Diagnosed at age gland parathyroidectomy at Children s Hospital of Los Angeles in 2003 Hypercalcemia resolved postoperatively
19 Maternal Consequences of Hypercalcemia 67% will experience complications Nephrolithiasis 24-36% Pancreatitis 7-13% Hyperemesis gravidarum Preeclampsia Hypercalcemic crisis (esp. after delivery) Miscarriage: 6-fold higher rate of 2 nd trimester loss
20 Fetal/Neonatal Consequences of Hypercalcemia Perinatal death/stillbirth 5% Previously approximately 25% Neonatal tetany 46% Neonatal hypocalcemia 50% Suppressed parathyroid development Low birth weight Premature birth
21 Next step?
22 Localization Ultrasound: Negative Mibi: No Limited CT parathyroids:

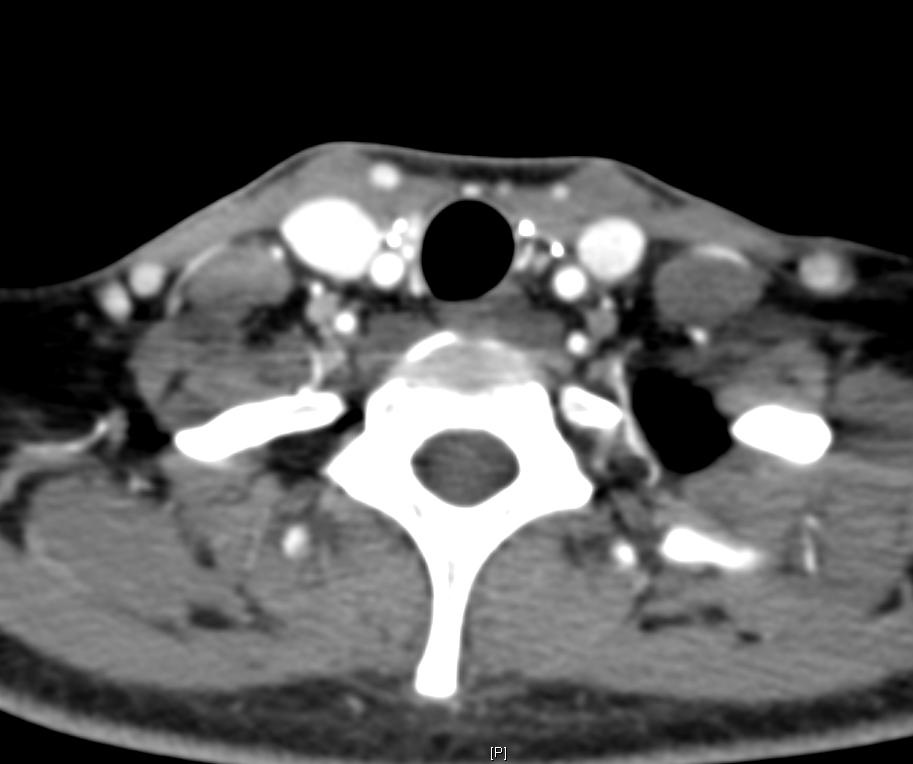
23 Dynamic Parathyroid CT
24 Next step?
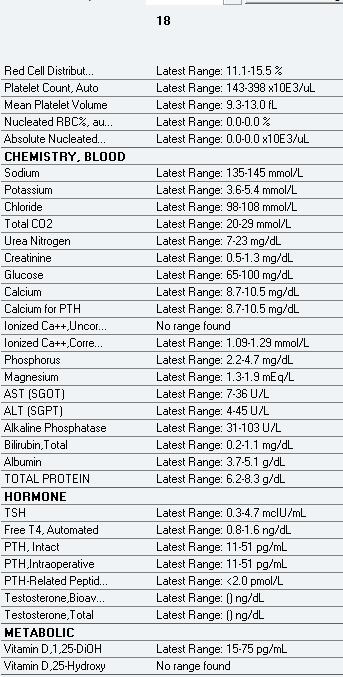
25
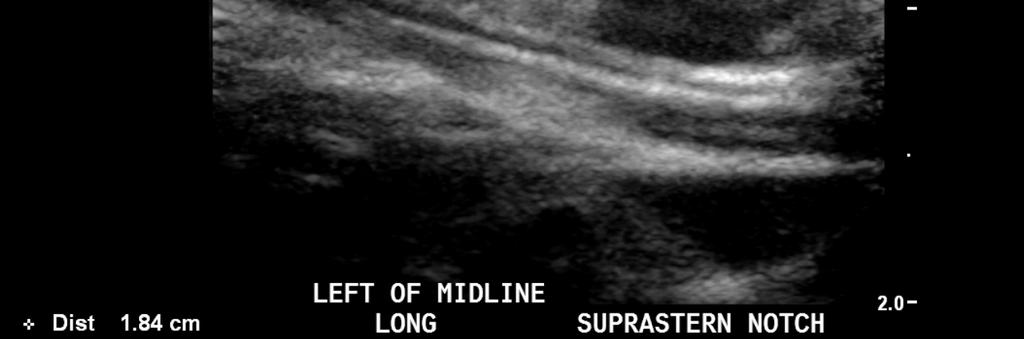
26 Repeat Ultrasound

27 May 22, 2012: FNA Biopsy


28 FNA Biopsy: PTH Stain Aspirate PTH level >3000
29 Next step?

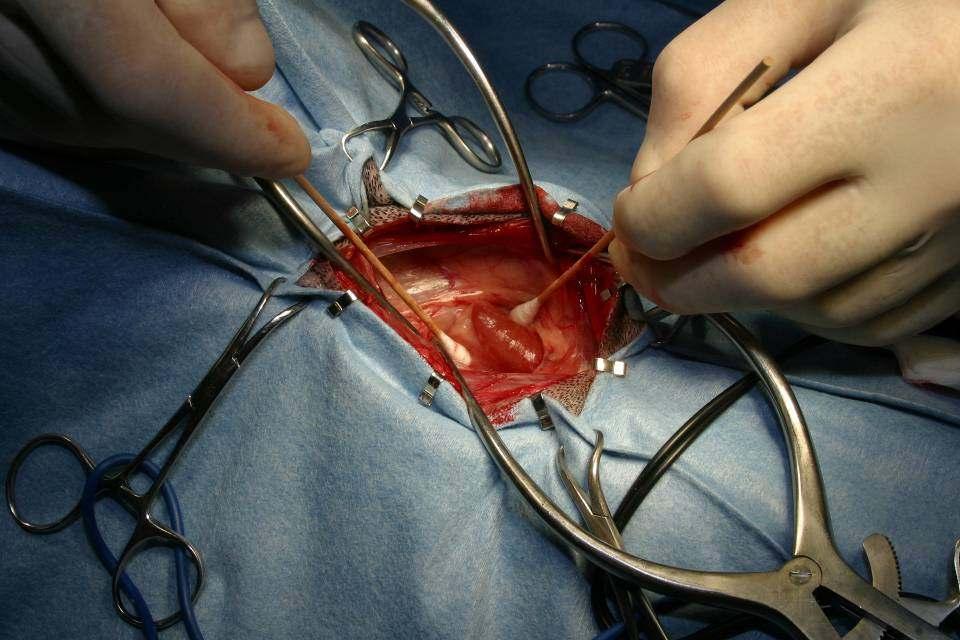
30 Re-do Parathyroidectomy Index mass removed
31 Intra-op PTH PTH (pg/ml) PreOp PreDissect T=5 min T=10 min
32 Next step?

33
")
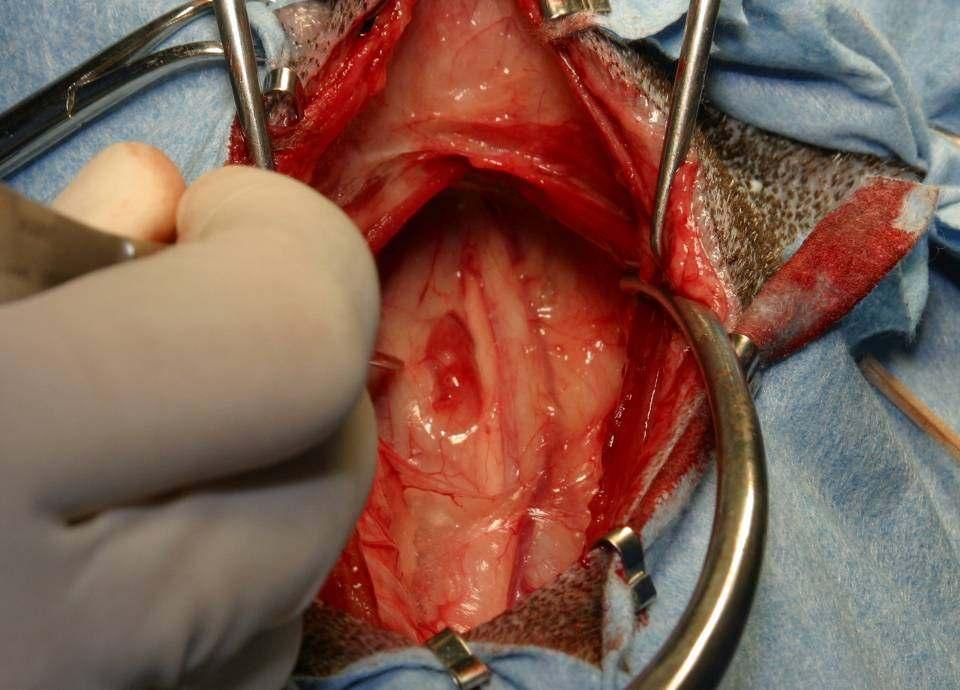
34 Additional masses removed from strap muscle area T=30 min T=15 min T=10 min T=5 min T=10 min T=5 min PreDissect PreOp PTH (pg/ml)

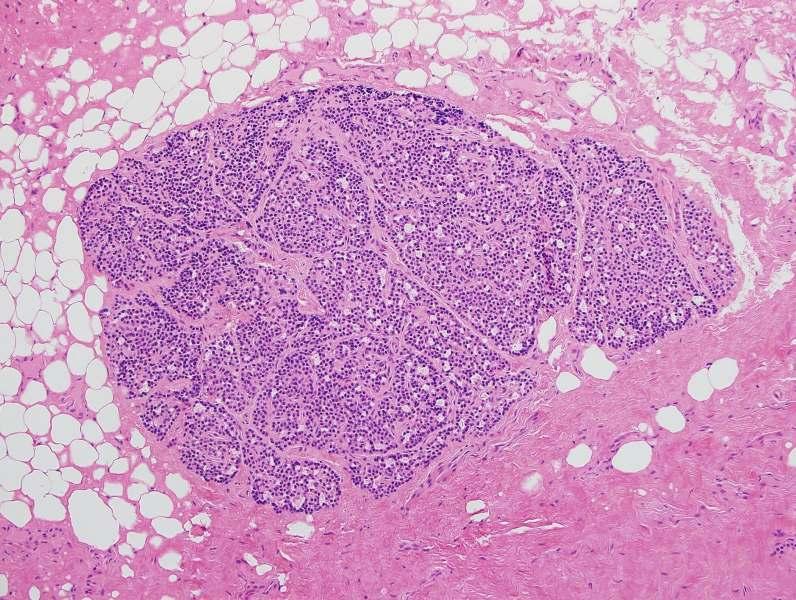
35 Surgical Pathology
36 Parathyromatosis Multiple nodules of benign hyperfunctioning parathyroid tissue scattered throughout the neck and mediastinum Caused by spillage and seeding of parathyroid tissue within the operative field No reports of parathyromatosis and pregnancy in the literature
37 Clinical Course July 16, 2012 (28 weeks) Abdominal pain, nausea and vomiting significantly improved Calcium 10.9, ionized calcium 1.44 PTH 47 August 20, 2012 (33 weeks) Calcium 11.9 Ionized calcium 1.68
38 Calcimimetics: Cinacalcet (Sensipar ) FDA approved March 8, 2004 for treatment of renal hyperparathyroidism and parathyroid carcinoma Type II calcimimetic increases the sensitivity of CaSR to extracellular Ca Half-life hrs Steddon SJ, Lancet 2005 Nemeth, PNAS 1998
39 Case Reports: Cinacalcet & Calcitonin Cinacalcet for hyperparathyroidism in pregnancy and puerperium Horjus et al, J Pediatr Endocrinol Metab Aug;22(8): weeks gestation, calcium 12.9 Cinacalcet used immediately post-delivery 32 weeks gestation, calcium 15.8 Combination of cinacalcet and calcitonin improved calcium to 12
40 Clinical Course September 4, 2012 (35 weeks) Calcium 9.2 Ionized calcium 1.35 September 10, 2012 (36 weeks) Calcium 9.9 Ionized calcium 1.35 PTH 57
41 Clinical Course September 17, 2012 (37 weeks) Calcium 10.9 Ionized calcium 1.66 September 24, 2012 (38 weeks) Calcium 10.7, Ionized calcium 1.55 Admitted for induction of labor at term
42 Clinical Course During induction, developed severe flank pain unrelieved by epidural UA +RBCs presumed diagnosis of kidney stone Did not want to expose baby to additional narcotics, so converted to elective C- section
43 Clinical Course Baby transferred to NICU prophylactically Initial ionized calcium 1.59, phosphorus 4.2 PTH 4 Repeat ionized calcium 1.16 Patient s post-operative labs Ionized calcium levels ranged from Discharged on POD 3 on Sensipar 30mg po QHS
44 Clinical Course Outpatient follow-up in Endocrine Surgery clinic 6 weeks after delivery Patient is asymptomatic after being off Sensipar for 1 week PTH 42, Calcium 10.2, Ionized calcium 1.35 Baby is doing well No problems with feeding or growth
45
46
47 Case #3: Persistent Hypercalcemia 67 yo man in good general health Develops polyuria, confusion, and unsteady gait Serum calcium 16.3 mg/dl (nl )
48 Treatment? IV fluids Calcitonin Pamidronate PTH = 58 pg/ml (nl 11-51) 25-OH Vit D = 22 pg/ml

49 Referred to UCLA (9/18/2012)



50 Imaging? Ultrasound: no definitive lesion Sestamibi: negative
51 Surgery? Left superior: normal Left inferior: normal Right superior: normal Right inferior: 1.5 cm adenoma within thymus PTH (pg/ml) PreOp PreDissect T=5 min T=10 min T=30 min T=24 hr
52

53 Check the pathology!
54 Persistent hypercalcemia Calcium 12.5 on 10/18/2012 Additional treatment? Additional workup?
55
56 More data PTH-related peptide 32 pg/ml (nl 14-27)
57 Stumped! Evaluated by UCLA endocrinology 5x3 cm mass over coccyx Suggested imaging of lower skull, back lesion, and chest to examine for small/miliary lung lesions or small lytic bone lesions
58


59 Treatment? Splenectomy Atypical large lymphoid cells c/w B cell lymphoma H&E CD20
60 Lab Total Calcium (mg/dl) On first presentation After parathyroidectomy Post-op day #1 After parathyroidectomy Post-op day #10 After splenectomy ~ One year after splenectomy PTH (pg/ml) Creatinine (mg/dl) D (pg/ml) D (pg/ml) > PTHrP (pmol/l) < 2


61 IHC for 1-alpha hydroxylase Positive control Lymphoma
62 Final Diagnosis Multifactorial hypercalcemia Primary hyperparathyroidism AND Calcitriol-secreting B cell lymphoma

63 Stewart AF, N Engl J Med 352:373, 2005
64 Case #4: PTH excess 36 year-old woman with functioning renal allograft after transplantation for polycystic kidney disease PTH 3,374 pg/ml and calcium 9.5 mg/dl Symptoms: difficulty concentrating, bone pain, fatigue, memory loss, forgetfulness, depression, difficulty sleeping
65 Additional Medical History 1. Renal osteodystrophy 2. Living related renal transplant Cadaveric renal transplant Cadaveric renal transplant 12/98 5. Parathyroidectomy 1/92 6. Parathyroidectomy 8/98
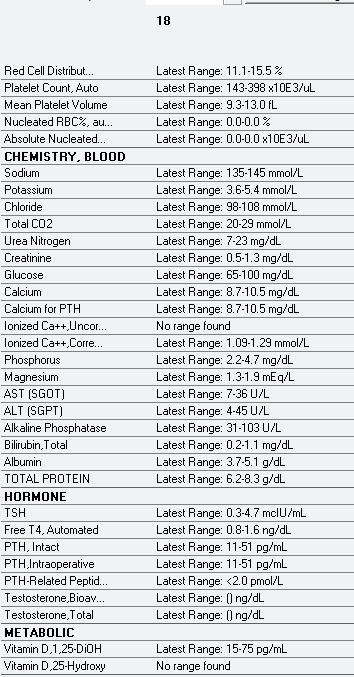
66 History Medications: Prograf 2 mg q. AM and 3 mg q. PM Prednisone 5 mg q. day Sensipar 60 mg q. day Labs: PTH 3,374 pg/ml Calcium 9.5 mg/dl ical 1.20 mmol/l Creatinine 0.6 mg/dl Phosphate 2.5 mg/dl

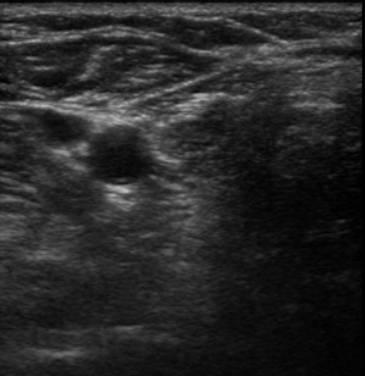
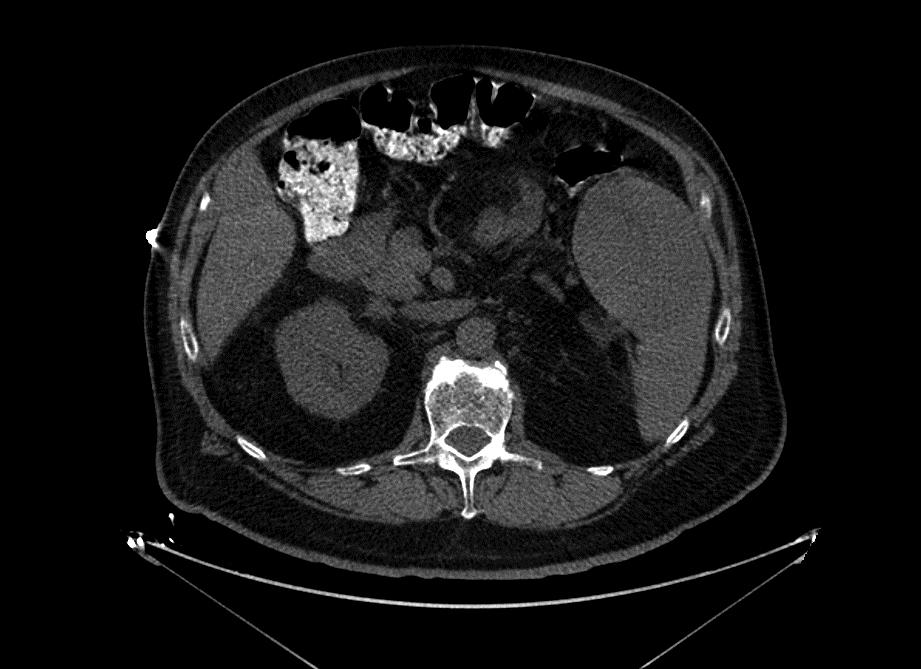
67 Imaging
68 How to manage?
69 Operation Redo parathyroidectomy Findings: Bilateral superior neck tissue consistent with hypercellular parathyroid; bilateral thymus glands without parathyroid tissue
70 Pathology
71 Operation Redo parathyroidectomy Findings: Bilateral superior neck tissue consistent with hypercellular parathyroid; bilateral thymus glands without parathyroid tissue IOPTH: >1,700 pg/ml
72 Post-operative Course Within 3.5 hours: Perioral numbness Inability to talk secondary to clenched jaw Difficulty moving legs due to spasm Crushing chest pain
73 What happened?
74 Laboratory Data Calcium 7.5 mg/dl ical 0.90 mmol/l Alk phos 67 U/L
75 Laboratory Data Calcium 7.5 mg/dl ical 0.90 mmol/l Alk phos 67 U/L Symptoms resolved after IV calcium repletion to ical 1.15 mmol/l
76 Laboratory Data Calcium 7.5 mg/dl ical 0.90 mmol/l Alk phos 67 U/L N telopeptide 24 hr urine: normal Bone specific alkaline phosphatase: normal Symptoms resolved after IV calcium repletion to ical 1.15 mmol/l
77 What happened?
78 PTH Assay Elecsys PTH system (Roche) = murine Ab PTH 3,061 pg/ml Scantibodies HBR (heterophilic blocking reagent) PTH 5 pg/ml Future Diagnostics intraoppth = goat Ab PTH 5 pg/ml
79 True Positive PTH ANALYTE CAPTURE ANTIBODY LABEL ANTIBODY

80 False Positive PTH ANALYTE CAPTURE ANTIBODY LABEL ANTIBODY HETEROPHILIC ANTIBODY
81 Final Diagnosis False elevation in PTH caused by heterophilic antibodies from prior administration of OKT3 leading to incorrect diagnosis of tertiary hyperparathyroidism. Levin and Yeh, Falsely elevated plasma parathyroid hormone level mimicking tertiary hyperparathyroidism. Endocr Pract 2011
82 Bonus Case: Severe Hypercalcemia Michael W. Yeh, MD Program Director, Endocrine Surgery Assistant Professor of Surgery and Medicine David Geffen School of Medicine at UCLA
83 Clinical presentation 8 yo M with incidentally discovered hypercalcemia Total Ca 17.2 mg/dl (2.15 mmol/l) Generally healthy Minor behavioral issues Possibly some decreased energy Family history unknown (adopted)
84 Biochemical workup
85
86 Next step?
87 Imaging Pt unable to comply with sestamibi Family agrees to ultrasound


88
89 The story so far Young patient Severe biochemical abnormalities Unknown family history No known risk factors, exposures Possible ectopic parathyroid adenoma
90 Next step?

91 Toby

92
93
94
95

96
97 Follow up
98 Pathology Parathyroid adenoma Normal thyroid tissue

99 Canine hyperparathyroidism Uncommon: ~300 cases reported Mean age of onset 11.2 years No gender predilection Keeshond > mixed breeding > Labrador Retriever > German shepherd = Golden Retriever > Poodle = Shih Tzu = Springer Spaniel Feldman, Pretreatment clinical and laboratory findings in dogs with primary hyperparathyroidism: 210 cases ( ). J Am Vet Med Assoc, 2005
.")
100 Canine hyperparathyroidism Incidental laboratory finding (geriatric screening) 50% urinary symptoms (stones or infection) 40% nephrolithiasis 90% adenoma Feldman, Pretreatment clinical and laboratory findings in dogs with primary hyperparathyroidism: 210 cases ( ). J Am Vet Med Assoc, 2005
.")
101 Canine hyperparathyroidism Feldman, Pretreatment clinical and laboratory findings in dogs with primary hyperparathyroidism: 210 cases ( ). J Am Vet Med Assoc, 2005

102 Canine hyperparathyroidism Rasor, Retrospective evaluation of three treatment methods for primary hyperparathyroidism in dogs. J Am Anim Hosp Assoc, 2007

103 Canine hyperparathyroidism Rasor, Retrospective evaluation of three treatment methods for primary hyperparathyroidism in dogs. J Am Anim Hosp Assoc, 2007
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Parathyroid Imaging. A Guide to Parathyroid Surgery
 Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Minimally invasive parathyroidectomy
 Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
4/20/2015. The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy. Learning Objectives
 Testing During Surgical Parathyroidectomy. Learning Objectives") The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
Hypercalcemia and Primary Hyperparathyroidism in Dogs
 WEB CHAPTER 11 Hypercalcemia and Primary Hyperparathyroidism in Dogs EDWARD C. FELDMAN, Davis, California Differential Diagnosis and Diagnostic Approach to Hypercalcemia Differential Diagnosis Hypercalcemia
WEB CHAPTER 11 Hypercalcemia and Primary Hyperparathyroidism in Dogs EDWARD C. FELDMAN, Davis, California Differential Diagnosis and Diagnostic Approach to Hypercalcemia Differential Diagnosis Hypercalcemia
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones
 Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Sensipar. Sensipar (cinacalcet) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HPI joint pain/arthritis serum calcium 11.5 PTH 147pg/ml
 HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
PRIMARY HYPERPARATHYROIDISM WITH RICKETS. KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College
 PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
Calcium and Parathyroid Disorders
 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Secondary and Familial Hyperparathyroidism
 Secondary and Familial Jeffrey F. Moley, M.D. Chief, Endocrine and Oncologic Surgery Section, Professor of Surgery Associate Director, The Alvin J. Siteman Cancer Center Occurs in setting of CRF Chronic
Secondary and Familial Jeffrey F. Moley, M.D. Chief, Endocrine and Oncologic Surgery Section, Professor of Surgery Associate Director, The Alvin J. Siteman Cancer Center Occurs in setting of CRF Chronic
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease
 Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
Hyper and hypocalcaemia. Prof Tricia Tan
 Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
David Bruyette, DVM, DACVIM
 VCAwestlaspecialty.com David Bruyette, DVM, DACVIM Disorders of calcium metabolism are common endocrine disorders in both dogs and cats. In this article we present a logical diagnostic approach to patients
VCAwestlaspecialty.com David Bruyette, DVM, DACVIM Disorders of calcium metabolism are common endocrine disorders in both dogs and cats. In this article we present a logical diagnostic approach to patients
Marcin Barczynski, 1 Aleksander Konturek, 2 Alicja Hubalewska-Dydejczyk, 2. Filip Gołkowski, 1 Stanislaw Cichon, 1 Piotr Richter, 1 Wojciech Nowak
 3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
When the level of calcium in the blood falls too low, the parathyroid glands secrete just enough PTH to restore the blood calcium level.
 Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Hypercalcemic Crisis in a Patient with a Huge Mediastinal Atypical Parathyroid Adenoma
 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Skeletal. Parathyroid hormone-related protein Analyte Information
 Skeletal Parathyroid hormone-related protein Analyte Information 1 2012-04-04 Parathyroid hormone related protein (PTHrP) Introduction Parathyroid hormone-related protein (PTHrP) is actually a family of
Skeletal Parathyroid hormone-related protein Analyte Information 1 2012-04-04 Parathyroid hormone related protein (PTHrP) Introduction Parathyroid hormone-related protein (PTHrP) is actually a family of
Sensipar (cinacalcet)
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
76 year-old female presents with muscle cramps. Jess Hwang 12/6/12
 76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Parathyroid Disease Scenarios for the Practicing Clinician. Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix
 Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy
 "Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
PARATHYROID NUCLEAR MEDICINE IMAGING REVIEW DISCLOSURES
 PARATHYROID NUCLEAR MEDICINE IMAGING REVIEW Miguel Hernandez Pampaloni, M.D., Ph.D. Chief, Nuclear Medicine Assistant Professor of Radiology UCSF Department of Radiology and Biomedical Imaging DISCLOSURES
PARATHYROID NUCLEAR MEDICINE IMAGING REVIEW Miguel Hernandez Pampaloni, M.D., Ph.D. Chief, Nuclear Medicine Assistant Professor of Radiology UCSF Department of Radiology and Biomedical Imaging DISCLOSURES
Hypercalcemia. Brian Rose, M.D. Bozeman Health June 6, 2018
 Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Case study Group 2 presentation
 Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
28 yo F w/esrd with a facial deformity
 28 yo F w/esrd with a facial deformity Jess Hwang Endocrinology fellow 1/30/14 History of renal failure-- 2005 Woke up blind one day At the hospital she was told she was 4 months pregnant Diagnosed with
28 yo F w/esrd with a facial deformity Jess Hwang Endocrinology fellow 1/30/14 History of renal failure-- 2005 Woke up blind one day At the hospital she was told she was 4 months pregnant Diagnosed with
Outline. Parathyroid Localization Studies. Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center
 Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
Complementary sestamibi scintigraphy and ultrasound for primary hyperparathyroidism
 Nuclear Medicine and Biomedical Imaging Research Article Complementary sestamibi scintigraphy and ultrasound for primary hyperparathyroidism Yang Z 1,3 *, Li AY 2, Alexander G 3 and Chadha M 3 1 Department
Nuclear Medicine and Biomedical Imaging Research Article Complementary sestamibi scintigraphy and ultrasound for primary hyperparathyroidism Yang Z 1,3 *, Li AY 2, Alexander G 3 and Chadha M 3 1 Department
Key Questions: What are the
 The Case of Kensington s Calcium Gregory K. Ogilvie, DVM Diplomate ACVIM (Specialties of Internal Medicine, Oncology) Diplomate ECVIM-CA (Oncology) CVS Angel Care Cancer Center University of California
The Case of Kensington s Calcium Gregory K. Ogilvie, DVM Diplomate ACVIM (Specialties of Internal Medicine, Oncology) Diplomate ECVIM-CA (Oncology) CVS Angel Care Cancer Center University of California
Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand
 International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma
 ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
Hyperparathyroidism (primary): diagnosis, assessment and initial management
: diagnosis, assessment and initial management") National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
2.0 Synopsis. Paricalcitol Capsules M Clinical Study Report R&D/15/0380. (For National Authority Use Only)
") 2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
Use of PTH at Point of Surgery for Non-Localized Cases of Hyperparathyoidism
 Use of PTH at Point of Surgery for Non-Localized Cases of Hyperparathyoidism Keck Hospital of USC Private, non-profit 400 bed hospital Teaching and research, USC Keck School of Medicine Approx. 40 parathyroid
Use of PTH at Point of Surgery for Non-Localized Cases of Hyperparathyoidism Keck Hospital of USC Private, non-profit 400 bed hospital Teaching and research, USC Keck School of Medicine Approx. 40 parathyroid
The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels
 17.6 The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels Partially embedded in the posterior surface of the lateral lobes of the thyroid gland
17.6 The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels Partially embedded in the posterior surface of the lateral lobes of the thyroid gland
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Medical Expert
 Medical Expert") Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Head and Neck Endocrine Surgery
 Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Pseudohypoparathyroidism: Case Presentation and Literature Review
 Pseudohypoparathyroidism: Case Presentation and Literature Review Aristides Maniatis, MD Rocky Mountain Pediatric Endocrinology PENS: 5/15/06 Disclosures Nothing to disclose Parental permission granted
Pseudohypoparathyroidism: Case Presentation and Literature Review Aristides Maniatis, MD Rocky Mountain Pediatric Endocrinology PENS: 5/15/06 Disclosures Nothing to disclose Parental permission granted
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
80 year old female with parathyroid mass and refractory hypercalcemia. Endorama September 24 th, 2015 Rajesh Jain
 80 year old female with parathyroid mass and refractory hypercalcemia Endorama September 24 th, 2015 Rajesh Jain HPI 80 F with pulmonary hypertension, rheumatic mitral stenosis, atrial fibrillation on
80 year old female with parathyroid mass and refractory hypercalcemia Endorama September 24 th, 2015 Rajesh Jain HPI 80 F with pulmonary hypertension, rheumatic mitral stenosis, atrial fibrillation on
Calcium-sensing receptors
 Making sense of calcium Calcium-sensing receptors Prof Arthur D Conigrave School of Molecular Bioscience, University of Sydney Department of Endocrinology, Royal Prince Alfred Hospital The calcium-sensing
Making sense of calcium Calcium-sensing receptors Prof Arthur D Conigrave School of Molecular Bioscience, University of Sydney Department of Endocrinology, Royal Prince Alfred Hospital The calcium-sensing
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes
 Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
Symptom management: Hypercalcemia
 Symptom management: Hypercalcemia Dr Claire Higham 10.11.16 NLCFN National Conference 2016 Consultant Endocrinologist The Christie Hospital Manchester, UK Hypercalcemia of malignancy 2-30% of patients
Symptom management: Hypercalcemia Dr Claire Higham 10.11.16 NLCFN National Conference 2016 Consultant Endocrinologist The Christie Hospital Manchester, UK Hypercalcemia of malignancy 2-30% of patients
ABSITE Review. RTC Conference Christina Bailey January 15, 2009
 ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Inpatient Pediatric Endocrinology. Tala Dajani MD MPH Pediatric Endocrinology of Phoenix
 Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems
Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems
44 yo man with hypercalcemia. Katie Stanley, MD August 9, 2012
 44 yo man with hypercalcemia Katie Stanley, MD August 9, 2012 HPI 44 yo M with DM1 and ESRD DM1 since age 5 Poorly controlled (A1c 9.1), multiple complications, hypoglycemia unawareness ESRD on HD since
44 yo man with hypercalcemia Katie Stanley, MD August 9, 2012 HPI 44 yo M with DM1 and ESRD DM1 since age 5 Poorly controlled (A1c 9.1), multiple complications, hypoglycemia unawareness ESRD on HD since
Parsabiv (etelcalcetide) NEW PRODUCT SLIDESHOW
 NEW PRODUCT SLIDESHOW") Parsabiv (etelcalcetide) NEW PRODUCT SLIDESHOW Introduction Brand name: Parsabiv Generic name: Etelcalcetide Pharmacological class: Calcimimetic Strength and Formulation: 2.5mg/0.5mL, 5mg/mL, 10mg/2mL;
Parsabiv (etelcalcetide) NEW PRODUCT SLIDESHOW Introduction Brand name: Parsabiv Generic name: Etelcalcetide Pharmacological class: Calcimimetic Strength and Formulation: 2.5mg/0.5mL, 5mg/mL, 10mg/2mL;
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP
 Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
Primary Hyperparathyroidism Diagnosed during the Work-up of Hydrops Fetalis: A Case Report
 Primary Hyperparathyroidism Diagnosed during the Work-up of Hydrops Fetalis: A Case Report 1 Stephanie Alimena, 2 Kulsoom Razvi, 1 Christopher M. Morosky 1 University of Connecticut School of Medicine,
Primary Hyperparathyroidism Diagnosed during the Work-up of Hydrops Fetalis: A Case Report 1 Stephanie Alimena, 2 Kulsoom Razvi, 1 Christopher M. Morosky 1 University of Connecticut School of Medicine,
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Magnesium Homeostasis
 ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
Diagnosis and Treatment of Primary Hyperparathyroidism. Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic
 Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
Kobe University Repository : Kernel
 Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
Hypercalcemia may be detected incidentally. Practice CMAJ. Primary hyperparathyroidism. Primer. Key points. The case. What causes hypercalcemia?
 CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
Disclosure. Topic Outline. Calcium, Vitamin D, PTH Disorders. PTH/Calcium-Normal Physiology. I have nothing to disclose
 Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Primary Hyperparathyroidism
 November 2002 Primary Hyperparathyroidism Lori Coburn, Harvard Medical School Year III Hyperparathyroidism An increase in parathyroid hormone (PTH) production Divided into Primary, Secondary and Tertiary
November 2002 Primary Hyperparathyroidism Lori Coburn, Harvard Medical School Year III Hyperparathyroidism An increase in parathyroid hormone (PTH) production Divided into Primary, Secondary and Tertiary
Calcium metabolism and the Parathyroid Glands. Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands
 Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Primary Hyperparathyroidism
 Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Case Report A Targeted Parathyroidectomy Using Guide Wire Technique in a Pregnant Patient with Primary Hyperparathyroidism
 International Otolaryngology Volume 2009, Article ID 361427, 4 pages doi:10.1155/2009/361427 Case Report A Targeted Parathyroidectomy Using Guide Wire Technique in a Pregnant Patient with Primary Hyperparathyroidism
International Otolaryngology Volume 2009, Article ID 361427, 4 pages doi:10.1155/2009/361427 Case Report A Targeted Parathyroidectomy Using Guide Wire Technique in a Pregnant Patient with Primary Hyperparathyroidism
Clinical biochemistry of calcium and vitamin D
 Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
Endocrine University 2016 AACE-ACE-MAYO CLINIC
 Endocrine University 2016 AACE-ACE-MAYO CLINIC Dev Abraham MD, MRCP (UK), ECNU Professor of Medicine (clinical), Division of Endocrinology Adjunct Professor of Surgery and Pathology Medical Director, Utah
Endocrine University 2016 AACE-ACE-MAYO CLINIC Dev Abraham MD, MRCP (UK), ECNU Professor of Medicine (clinical), Division of Endocrinology Adjunct Professor of Surgery and Pathology Medical Director, Utah
2 Year old Girl with Severe Hypercalcemia. March 7, 2013 Matt Wise, MD All ages
 2 Year old Girl with Severe Hypercalcemia March 7, 2013 Matt Wise, MD All ages HPI 2y3m caucasian girl presents to OSH ER with 1 day of fever to 102, vomiting, increased tiredness Several weeks of excess
2 Year old Girl with Severe Hypercalcemia March 7, 2013 Matt Wise, MD All ages HPI 2y3m caucasian girl presents to OSH ER with 1 day of fever to 102, vomiting, increased tiredness Several weeks of excess
Patient Information Leaflet P1
 Patient Information Leaflet P1 Parathyroid Operations in Adults What are the Parathyroid glands and what do they do? Usually, you have four parathyroid glands. These are located between the thyroid gland
Patient Information Leaflet P1 Parathyroid Operations in Adults What are the Parathyroid glands and what do they do? Usually, you have four parathyroid glands. These are located between the thyroid gland
Parathyroid Imaging What is best
 Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
Coexistence of parathyroid adenoma and papillary thyroid carcinoma. Yong Sang Lee, Kee-Hyun Nam, Woong Youn Chung, Hang-Seok Chang, Cheong Soo Park
 J Korean Surg Soc 2011;81:316-320 http://dx.doi.org/10.4174/jkss.2011.81.5.316 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Coexistence of parathyroid
J Korean Surg Soc 2011;81:316-320 http://dx.doi.org/10.4174/jkss.2011.81.5.316 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Coexistence of parathyroid
THE PARATHYROID GLAND THEORY AND NUCLEAR MEDICINE PRACTICE
 THE PARATHYROID GLAND THEORY AND NUCLEAR MEDICINE PRACTICE George N. Sfakianakis MD Professor of Radiology and Pediatrics Director, Division of Nuclear Medicine UM/JMMC Miami FL October 2009 ENDONCRINE
THE PARATHYROID GLAND THEORY AND NUCLEAR MEDICINE PRACTICE George N. Sfakianakis MD Professor of Radiology and Pediatrics Director, Division of Nuclear Medicine UM/JMMC Miami FL October 2009 ENDONCRINE
Challenges in the Management of Primary HPTH. Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH
 Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
Bone Disorders in CKD
 Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
38 year old Male with Ankylosing Spondylitis. Olesya Krivospitskaya, MD April,
 38 year old Male with Ankylosing Spondylitis Olesya Krivospitskaya, MD April, 11 2013 HPI (Letter from the patient): Diagnosed with Ankylosing Spondylitis and prescribed a Sulfa drug to help with my back
38 year old Male with Ankylosing Spondylitis Olesya Krivospitskaya, MD April, 11 2013 HPI (Letter from the patient): Diagnosed with Ankylosing Spondylitis and prescribed a Sulfa drug to help with my back
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416)
") Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS
 Original Article RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS Charles D. Livingston, MD, FACS ABSTRACT Objective: To examine an individualized approach to patients with primary
Original Article RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS Charles D. Livingston, MD, FACS ABSTRACT Objective: To examine an individualized approach to patients with primary
PARSABIV (etelcalcetide)
") PARSABIV (etelcalcetide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
PARSABIV (etelcalcetide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
THE ASSOCIATION OF PRIMARY HYPERPARATHYROIDISM WITH DISORDERS OF THE THYROID GLAND AND CARPENTRY OUR EXPERIENCE
 24 MEDICINSKI GLASNIK / str. 24-30 Snežana Marinković, Nenad Laketić 1 THE ASSOCIATION OF PRIMARY HYPERPARATHYROIDISM WITH DISORDERS OF THE THYROID GLAND AND CARPENTRY OUR EXPERIENCE Introduction Primary
24 MEDICINSKI GLASNIK / str. 24-30 Snežana Marinković, Nenad Laketić 1 THE ASSOCIATION OF PRIMARY HYPERPARATHYROIDISM WITH DISORDERS OF THE THYROID GLAND AND CARPENTRY OUR EXPERIENCE Introduction Primary
The Parsabiv Beginner s Book
 The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism