Calcium and Parathyroid Disorders
|
|
|
- Jeffry Charles
- 6 years ago
- Views:
Transcription



1 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November 11, 2017
2 None Disclosures
3 Outline Physiology of calcium, parathyroid hormone and vitamin D Hypercalcemia Primary hyperparathyroidism Hypocalcemia
4 PHYSIOLOGY AKA HOW THINGS WORK
5 Physiologic Roles of Calcium Maintains electrochemical gradient across cell membranes Excitation contraction coupling in cardiac and other muscles Coagulation, synaptic transmission Hormone release and intracellular messenger: Calcium acts as a second messenger Transforms extracellular signals into intracellular responses
6 Physiologic Roles of Calcium Extracellular (ionized) calcium is tightly regulated Hypercalcemia => raises potential across cell making it difficult to excite Hypocalcemia => reduced membrane potential making cell hyperexcitable
7 ==> 150 mg Filtered Ca = 10,000 mg Reabsorbed Ca = 9,850 mg

8 NIH Office of Dietary Supplements Fact Sheet


9 Dietary Calcium Sources NIH Office of Dietary Supplements Fact Sheet
10 Elemental Calcium ==> needs acidic environment
11

12 Parathyroid Glands Size = 3-4 mm Weight = 40 mg Number = 4, but ~10% people have one supernumerary gland & 2% have three parathyroid glands Location = neck, but ectopic locations include 6.3% in mediastinum and 2% in atypical locations in the neck

13 Parathyroid Hormone Secretion is predominantly regulated by serum calcium concentrations serum Ca = PTH secretion serum Ca = PTH secretion Cleared within 2-4 minutes
14
15 Parathyroid Hormone Regulation Calcium sensing receptor (CaSr) cell surface receptor that senses extracellular calcium found in parathyroid glands and kidney Binding of Ca to CaSR inhibits PTH secretion and level of PTH mrna Familial Hypocalciuric Hypercalcemia (FHH): inactivating mutation of the CaSR higher set point for calcium sensing
16 Actions of PTH Kidney: Stimulate 1,25(OH) 2 D production Stimulate Calcium Reabsorption Block Phosphate Reabsorption Bone: Activate Osteoclastic Resorption (acute) Activate Osteoblastic Bone Formation (subacute, chronic) Intestine:Activate Calcium Transport (indirect via 1,25(OH) 2 D) Modified from Stewart AF, Cecil Essentials of Medicine 8 th ed,
17 resorption absorptio n (indirectly) reabsorption Vit D hydroxylation
18 Vitamin D
19 Vitamin D Wide range of other biologic actions: inhibits cellular proliferation and angiogenesis, stimulates insulin production, inhibits renin production, stimulates macrophages 25 (OH) D major circulating form best indicator of vitamin D status 1,000 X > concentration than 1,25 (OH) 2 D Deficiency: children => rickets, adults => Osteomalacia
20 Vitamin D Supplementation Vitamin D 2 (ergocalciferol) => plant source Vitamin D 3 (cholecalciferol) => animal source Recent data that D 3 is more effective at raising serum vitamin D levels compared to D 2
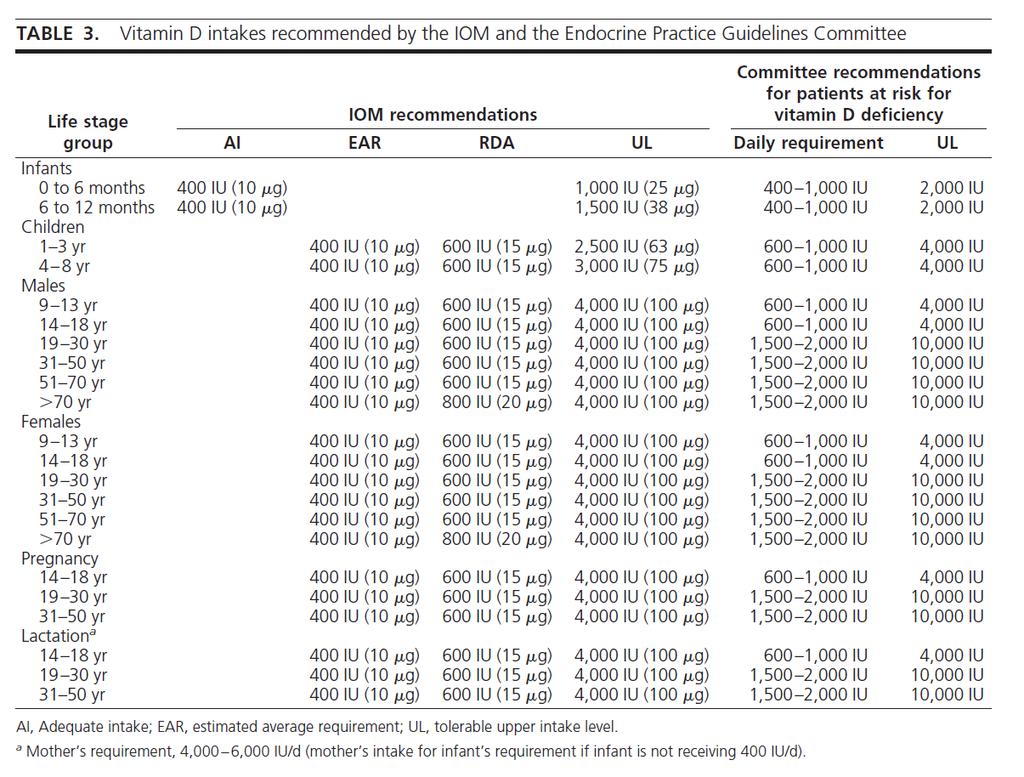
21 How Much Vitamin D Do We Need? Depends on who you ask IOM provides guidance for dietary standards in the general public, used by government to set dietary regulations Endocrine Society Practice guidelines intended for use by clinicians who have patients who are at risk for deficiency Goal: Serum 25 Vitamin D > 30 ng/ml
22
23 Hyperparathyroidism
24 HYPERCALCEMIA AKA DOC I M TIRED ALL THE TIME
25 Hypercalcemia Corrected total or ionized calcium > 2 SD above normal mean ( mg/dl or mm) No formal grading criteria for severity: <12.0 mg/dl => mild mg/dl => moderate > 14.0 mg/dl => severe
26 Hypercalcemia Serum Calcium: % ionized (active) 40-45% bound to albumin 10 % bound to citrate Total calcium varies with alterations in binding proteins, specifically albumin Corrected calcium should be used for decision making Corrected Total Ca + = Measured Ca + mg/dl ( 4.0 measured albumin)
27 Manifestations of Hypercalcemia Signs and symptoms depend on severity and rapidity of onset electrical gradient across a cell depolarization potential response to chemical or neural stimulus
28 Manifestations of Hypercalcemia Neurologic: Fatigue => obtunded => coma Influenced by rate of onset, age, baseline MS Seizures (cerebral vasoconstriction) Renal: Polyuria => thirst and dehydration Calcium directly inhibits H2O reabsorption due to osmotic diuresis Calcium inhibits ADH effect on distal nephron = nephrogenic DI Nephrocalcinosis = deposition of Ca-Phos salts in renal interstitium Hypercalciuria => nephrolithiasis Renal insufficiency or failure over time
29 Manifestations of Hypercalcemia Cardiovascular: Shortened QTc interval: deposition of Ca-Phos in cardiac conduction system Arteriolar vasoconstriction Musculo-skeletal: Skeletal muscle weakness: contractility Gastrointestinal: Constipation, nausea, vomiting, ileus (due to smooth muscle hypoactivity) Pancreatitis: calcium deposits within pancreas

30 Differential Diagnosis of Hypercalcemia Check PTH PTH PTH Primary Hyperparathyroidism Tertiary Hyperparathyroidism Parathyroid Carcinoma FHH Everything Else

31 Differential Diagnosis of Hypercalcemia
32 Primary Hyperparathyroidism Primary Disorder Abnormality SCa SPO 4 TMP FCaE CaE* 25-D 1,25 (OH) 2 D PTH Primary Increased PTH N, N hyperparathyroidism secretion Most common cause of hypercalcemia in the outpatient setting Used to be disease of bones, stones, groans, and psychic moans but now usually discovered incidentally high normal or Ca + with inappropriately normal or PTH
33
34 Primary Hyperparathyroidism Caused by over secretion of PTH by parathyroid gland loss of normal feedback of PTH by serum calcium 85% benign solitary parathyroid adenoma 15% hyperplasia of two or more parathyroid glands Consider hereditary endocrine disorders: MEN I and MEN II Rare parathyroid carcinoma (1.25 cases per 10 million)
35 Primary Hyperparathyroidism Most patients are asymptomatic with mild elevated Ca + = mg/dl Symptoms => same as Ca, bone pain Evaluation: Serum calcium, albumin, phosphorous, creatinine, PTH, 25 OH vitamin D (correct if low) 24 urine calcium and creatinine DXA scan (with forearm BMD) Imaging: Order sestamibi scan (+/- SPECT) only after diagnosis is confirmed biochemically
36 Primary Hyperparathyroidism: Definitive treatment is surgical Refer to an experienced surgeon! Who is a surgical candidate? Any symptomatic patient Asymptomatic patients with any of the following: Age <50 Management Serum total calcium 1.0 mg/dl above ULN T-score -2.5 SD at any site or vertebral fracture Cr clearance < 60cc/min, Ur Ca >400 mg/d and high biochemical stone risk, presence of nephrolithiasis or nephrocalcinosis Bilezikian JP, JCEM 2014.
37 Primary Hyperparathyroidism: Medical Management Antiresorptives (bisphosphonates) for low bone density Calcimimetic (cinacalcet) symptomatic or severe hypercalcemia in non-surgical candidate Yearly monitoring for those with mild disease S Calcium, albumin, phosphorous, PTH, 25 OH Vit D Urine calcium and creatinine if indicated BMD every 1-2 years (include distal radius)

38 Differential Diagnosis of Hypercalcemia Check PTH PTH PTH Primary Hyperparathyroidism Tertiary Hyperparathyroidism Parathyroid Carcinoma Everything Else
39 Non-PTH Mediated Hypercalcemia Familial Hypocalciuric Hypercalcemia Malignancy associated hypercalcemia Granulomatous disorders (lymphoma, sarcoidosis) Endocrine disorders (hyperthyroidism, Addison s, Pheochromocytoma) Milk alkali syndrome Immobilization (among adolescents, Paget s) Acute Renal Failure TPN/hyperproteinemia End Stage Liver Disease Medications
40 Malignancy Associated Hypercalcemia Most common cause of hypercalcemia in inpatient setting Common cause of death among cancer patients: severe hypercalcemia leads to coma and renal failure Breast, lung, renal, ovarian, hematologic Secretion of Parathyroid hormone-related protein (PTHrP) causing humoral hypercalcemia of malignancy Skeletal metastases cytokine mediated osteoclastic bone destruction Lymphomas can make 1,25 (OH) 2 Vitamin D Rare tumors make ectopic PTH
41 Malignancy Associated Hypercalcemia: Treatment Treat underlying malignancy Acute management: Vigorous intravenous hydration Loop diuretics only to prevent CHF Calcitonin Often responds acutely to meds that block bone resorption IV Bisphosphonates: Zoledronate or Pamidronate
42 Sarcoidosis Granulomatous disease: giant granuloma cells multiple organs Prototype of hypercalcemia associated with granulomatous diseases Occurs in 10% of sarcoid patients 1,25 (OH) 2 D production by macrophages and giant cells => intestinal hyperabsorption of calcium Lesser extent renal calcium absorption and osteoclastic bone resorption Treatment: Glucocorticoids
43 Medications Hypervitaminosis A Hypervitaminosis D Thiazide diuretics Lithium Estrogens, androgens Tamoxifen
44 HYPOCALCEMIA AKA DOC I M TINGLING ALL OVER
45 Hypocalcemia Corrected total or ionized calcium < 2 SD below normal mean (<8.5 mg/dl = <1.16 mm) As with hypercalcemia, total calcium needs to be corrected for albumin when assessing hypocalcemia Evaluation includes measurement of: Serum calcium, albumin Serum ionized Ca, Mg, Phos, PTH, and 25 OH Vit D
46 Manifestations of Hypocalcemia Signs and symptoms depend on severity and rapidity of onset electrical gradient across a cell depolarization potential response to chemical or neural stimulus => hyperexcitability
47 Manifestations of Hypocalcemia Neurologic: Fatigue, seizures, perioral numbness, tingling Basal ganglia and intra-cerebral calcifications Cardio-vascular: Prolonged QTc interval, arrhythmias CHF Cardiomyopathy
48 Manifestations of Hypocalcemia Musculo-skeletal: Muscle twitches, cramps, tetany Chvostek s sign => twitching of facial muscle Trousseau s sign => spasms of forearm with BP cuff > systolic Gastrointestinal: Cramping Other: Bronchospasm Cataracts
49 Differential Diagnosis of Hypocalcemia Hypoparathyroidism Psuedohypoparathyroidism Vitamin D Disorders Hypoalbuminemia Magnesium disorders Rapid Bone formation Hyperphosphatemia Medications Pancreatitis
50 Hypoparathyroidism Rare, results from no or little PTH low ionized calcium with low PTH Phos often elevated early in disease Low 1,25 (OH) 2 vitamin D Result is hypocalcemia that is often symptomatic at onset Etiology Surgical Idiopathic/Autoimmune Infiltrative diseases Wilson s, hemochromatosis Congenital
51 Hypoparathyroidism: Treatment One of the few endocrine disorders that has previously not been treated with replacement hormone 2 main components of therapy: Calcium supplementation (~2 gm a day) 1,25 (OH) 2 vitamin D (rocaltrol, calcitriol) Important to monitor serum and urine calcium closely to avoid calcium-phosphate precipitation Recombinant PTH 1-84 recently (2015) approved for treatment of long-standing severe hypoparathyroidism
52 Severe Hypocalcemia Among Inpatients Treat with IV calcium if: Symptomatic (carpopedal spasm, tetany, seizures) QT prolongation Acute hypocalcemia, corrected Ca <7.5 mg/dl Administer IV calcium gluconate (mix 1 amp with 50 ml D5 to avoid hypotension and bradycardia) Start calcium gluconate infusion (11 amps in 890mL NS = 1 mg/ml elemental Ca) 50 ml/hr Start oral calcium carbonate 2 gm TID Start calcitriol 0.25 mcg BID Treat hypomagnesemia and monitor Ca closely
53 QUESTIONS? Have you tried Googling that?
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Hypocalcemia 6/8/12. Normal value. Physiologic functions. Nephron a functional unit of kidney. Influencing factors in Calcium and Phosphate Balance
 Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Calcium metabolism and the Parathyroid Glands. Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands
 Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
CALCIUM BALANCE. James T. McCarthy & Rajiv Kumar
 CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyper and hypocalcaemia. Prof Tricia Tan
 Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
Disclosure. Topic Outline. Calcium, Vitamin D, PTH Disorders. PTH/Calcium-Normal Physiology. I have nothing to disclose
 Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Hypercalcemia. Brian Rose, M.D. Bozeman Health June 6, 2018
 Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
Hypoparathyroidism By John Halpern, DO, FACEP Coauthored by N. Ewen Wang, MD
 Hypoparathyroidism By John Halpern, DO, FACEP Coauthored by N. Ewen Wang, MD Reprinted with permission from: E-Medicine: Instant Access to the Minds of Medicine http://www.emedicine.com/emerg/topic276.htm
Hypoparathyroidism By John Halpern, DO, FACEP Coauthored by N. Ewen Wang, MD Reprinted with permission from: E-Medicine: Instant Access to the Minds of Medicine http://www.emedicine.com/emerg/topic276.htm
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
GLOSSARY OF TERMS. produced in response to an antigen to bond with and neutralize that antigen / the body's way of destroying foreign invaders
 TERM 24-hour urine acidosis acquired aemia (prefix) albumin alkalosis anemia antibodies antigen autocrine autoimmune basal ganglion bone turnover calcilytic calcimimetic calcitonin Calcitriol Calcium carbonate
TERM 24-hour urine acidosis acquired aemia (prefix) albumin alkalosis anemia antibodies antigen autocrine autoimmune basal ganglion bone turnover calcilytic calcimimetic calcitonin Calcitriol Calcium carbonate
Agents that Affect Bone & Mineral Homeostasis
 Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
76 year-old female presents with muscle cramps. Jess Hwang 12/6/12
 76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
HYPERCALCAEMIA 101 FOR THE INTERNIST
 HYPERCALCAEMIA 101 FOR THE INTERNIST Dr Chionh Siok Bee Dept of Medicine, National University Hospital siok_bee_chionh@nuhs.edu.sg Medicine Review Course 18/09/2011 Outline of Talk Definition of hypercalcaemia
HYPERCALCAEMIA 101 FOR THE INTERNIST Dr Chionh Siok Bee Dept of Medicine, National University Hospital siok_bee_chionh@nuhs.edu.sg Medicine Review Course 18/09/2011 Outline of Talk Definition of hypercalcaemia
Endocrine Regulation of Calcium and Phosphate Metabolism
 Endocrine Regulation of Calcium and Phosphate Metabolism Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C516, Block C, Research Building, School of Medicine Tel: 88208252 Email: wanghuiping@zju.edu.cn
Endocrine Regulation of Calcium and Phosphate Metabolism Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C516, Block C, Research Building, School of Medicine Tel: 88208252 Email: wanghuiping@zju.edu.cn
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
Magnesium Homeostasis
 ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary
 Prior Authorization with Quantity Limit Program Summary") Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 2 Available Product Indication Dosing and Administration Natpara (parathyroid hormone)
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 2 Available Product Indication Dosing and Administration Natpara (parathyroid hormone)
Clinical biochemistry of calcium and vitamin D
 Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
Clinical biochemistry of calcium and vitamin D Dr Andrew Day Consultant in Clinical Biochemistry and Metabolic Medicine University Hospitals Bristol NHS Trust e-mail: andrew.day@uhbristol.nhs.uk A 48-year
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia
 BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
The Parathyroid Glands
 The Parathyroid Glands Bởi: OpenStaxCollege The parathyroid glands are tiny, round structures usually found embedded in the posterior surface of the thyroid gland ([link]). A thick connective tissue capsule
The Parathyroid Glands Bởi: OpenStaxCollege The parathyroid glands are tiny, round structures usually found embedded in the posterior surface of the thyroid gland ([link]). A thick connective tissue capsule
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Calcium Nephrolithiasis and Bone Health. Noah S. Schenkman, MD
 Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
SUMMARY OF PRODUCT CHARACTERISTICS
 SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Colecalciferol Meda 800 IU tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 800 IU
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Colecalciferol Meda 800 IU tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 800 IU
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Natpara (parathyroid hormone) Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Natpara (parathyroid hormone) Prime Therapeutics will review Prior Authorization
Natpara (parathyroid hormone) Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Natpara (parathyroid hormone) Prime Therapeutics will review Prior Authorization
20F With Hypocalcemia
 20F With Hypocalcemia Isabel Casimiro, MD PhD * 5/11/17 * has no relevant financial relationships with any commercial interests. How to Approach Hypocalcemia? How to Approach Hypocalcemia? Etiology: Think
20F With Hypocalcemia Isabel Casimiro, MD PhD * 5/11/17 * has no relevant financial relationships with any commercial interests. How to Approach Hypocalcemia? How to Approach Hypocalcemia? Etiology: Think
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
When the level of calcium in the blood falls too low, the parathyroid glands secrete just enough PTH to restore the blood calcium level.
 Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Disclosure. Primary Hyperparathyroidism 4 th IW. Topic Outline. Calcium, Vitamin D, PTH Disorders. I have nothing to disclose related to this topic
 Disclosure Calcium, Vitamin D, PTH Disorders Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF I have nothing to disclose related to this topic Topic Outline Calcium/Vitamin
Disclosure Calcium, Vitamin D, PTH Disorders Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF I have nothing to disclose related to this topic Topic Outline Calcium/Vitamin
Head and Neck Endocrine Surgery
 Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Since the advent of multichannel serum chemistry
 ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
Management of patients with thyroid cancer scheduled for thyroidectomy at RCHSD
 Management of patients with thyroid cancer scheduled for thyroidectomy at RCHSD Pre-Operative labs To be drawn when Thyroidectomy for the management of thyroid cancer is first considered Vitamin D-25 OH
Management of patients with thyroid cancer scheduled for thyroidectomy at RCHSD Pre-Operative labs To be drawn when Thyroidectomy for the management of thyroid cancer is first considered Vitamin D-25 OH
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
OMICS Journals are welcoming Submissions
 OMICS Journals are welcoming Submissions OMICS International welcomes submissions that are original and technically so as to serve both the developing world and developed countries in the best possible
OMICS Journals are welcoming Submissions OMICS International welcomes submissions that are original and technically so as to serve both the developing world and developed countries in the best possible
Lecture 4 Calcium & Phosphate Disorders Loh. Calcium distribution
 Lecture 4 lcium & Phosphate Disorders Loh lcium functions: Bone & teeth maintenance Platelet adhesion Neuromuscular activity Blood coagulation Endocrine & exocrine functions Heart electrophysiology Smooth
Lecture 4 lcium & Phosphate Disorders Loh lcium functions: Bone & teeth maintenance Platelet adhesion Neuromuscular activity Blood coagulation Endocrine & exocrine functions Heart electrophysiology Smooth
Parathyroid Imaging. A Guide to Parathyroid Surgery
 Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
REGULATION OF CALCIUM AND PHOSPHATE HOMEOSTASIS
 REGULATION OF CALCIUM AND PHOSPHATE HOMEOSTASIS Linda S. Costanzo Virginia Commonwealth University, Medical College of Virginia, Richmond, Virginia 23298 Teaching Ca 2 and phosphate homeostasis in a physiology
REGULATION OF CALCIUM AND PHOSPHATE HOMEOSTASIS Linda S. Costanzo Virginia Commonwealth University, Medical College of Virginia, Richmond, Virginia 23298 Teaching Ca 2 and phosphate homeostasis in a physiology
Case. IRIM 2012: Calcium Cases. Case. Case. Distribution of Calcium. Question: What Test Would You Order Next?
 IRIM 2012: Calcium Cases Carolyn Becker MD Brigham and Women s Hospital Harvard Medical School Case A 65 yo man with multiple myeloma is admitted with pneumonia and sepsis. Exam: febrile, BP 80/60, P 120,
IRIM 2012: Calcium Cases Carolyn Becker MD Brigham and Women s Hospital Harvard Medical School Case A 65 yo man with multiple myeloma is admitted with pneumonia and sepsis. Exam: febrile, BP 80/60, P 120,
David Bruyette, DVM, DACVIM
 VCAwestlaspecialty.com David Bruyette, DVM, DACVIM Disorders of calcium metabolism are common endocrine disorders in both dogs and cats. In this article we present a logical diagnostic approach to patients
VCAwestlaspecialty.com David Bruyette, DVM, DACVIM Disorders of calcium metabolism are common endocrine disorders in both dogs and cats. In this article we present a logical diagnostic approach to patients
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary
 Prior Authorization with Quantity Limit Program Summary") Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
H 2 O, Electrolytes and Acid-Base Balance
 H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
Rahaf AL-Jafari. Marah Qaddourah. Rahmeh Abdullah. Saleem. 1 P a g e
 15 Rahaf AL-Jafari Marah Qaddourah Rahmeh Abdullah Saleem 1 P a g e If you are following with the record you may notice a little bit difference in information sequences. Hormones that function on growth
15 Rahaf AL-Jafari Marah Qaddourah Rahmeh Abdullah Saleem 1 P a g e If you are following with the record you may notice a little bit difference in information sequences. Hormones that function on growth
Awaisheh. Mousa Al-Abbadi. Abdullah Alaraj. 1 Page
 f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
Summary of Product Characteristics
 1 NAME OF THE MEDICINAL PRODUCT Desunin 4000 IU Tablets Summary of Product Characteristics 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 4000 IU (equivalent
1 NAME OF THE MEDICINAL PRODUCT Desunin 4000 IU Tablets Summary of Product Characteristics 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 4000 IU (equivalent
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
BARTS ENDOCRINE E-PROTOCOLS CALCIUM DISORDERS AND BONE
 HYPERCALCAEMIA CALCIUM DISORDERS Clinical features to record Symptoms: Thirst, polyuria, nocturia, tiredness, poor concentration, depression, constipation, episodes of renal colic/calculi, hypertension,
HYPERCALCAEMIA CALCIUM DISORDERS Clinical features to record Symptoms: Thirst, polyuria, nocturia, tiredness, poor concentration, depression, constipation, episodes of renal colic/calculi, hypertension,
Symptom management: Hypercalcemia
 Symptom management: Hypercalcemia Dr Claire Higham 10.11.16 NLCFN National Conference 2016 Consultant Endocrinologist The Christie Hospital Manchester, UK Hypercalcemia of malignancy 2-30% of patients
Symptom management: Hypercalcemia Dr Claire Higham 10.11.16 NLCFN National Conference 2016 Consultant Endocrinologist The Christie Hospital Manchester, UK Hypercalcemia of malignancy 2-30% of patients
Management of hypercalcemia of malignancy
 Integrative Cancer Science and Therapeutics Research Article ISSN: 2056-4546 Management of hypercalcemia of malignancy Sonia Amin Thomas (Sonia Patel)* and Soo-Hwan Chung Philadelphia College of Osteopathic
Integrative Cancer Science and Therapeutics Research Article ISSN: 2056-4546 Management of hypercalcemia of malignancy Sonia Amin Thomas (Sonia Patel)* and Soo-Hwan Chung Philadelphia College of Osteopathic
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy
 "Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels
 17.6 The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels Partially embedded in the posterior surface of the lateral lobes of the thyroid gland
17.6 The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels Partially embedded in the posterior surface of the lateral lobes of the thyroid gland
Parathyroid Disease Scenarios for the Practicing Clinician. Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix
 Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Primary Hyperparathyroidism
 Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Calcium-sensing receptors
 Making sense of calcium Calcium-sensing receptors Prof Arthur D Conigrave School of Molecular Bioscience, University of Sydney Department of Endocrinology, Royal Prince Alfred Hospital The calcium-sensing
Making sense of calcium Calcium-sensing receptors Prof Arthur D Conigrave School of Molecular Bioscience, University of Sydney Department of Endocrinology, Royal Prince Alfred Hospital The calcium-sensing
Dosage in renal impairment Kalcipos-D chewable tablets should not be used in patients with severe renal impairment.
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D 500 mg/400 IU chewable tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains: calcium 500 mg as
SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D 500 mg/400 IU chewable tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains: calcium 500 mg as
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
What is the right calcium balance?
 For patients with hypoparathyroidism What is the right calcium balance? Indications and Usage1 NATPARA is a parathyroid hormone indicated as an adjunct to calcium and vitamin D to control hypocalcemia
For patients with hypoparathyroidism What is the right calcium balance? Indications and Usage1 NATPARA is a parathyroid hormone indicated as an adjunct to calcium and vitamin D to control hypocalcemia
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Hypercalcemia may be detected incidentally. Practice CMAJ. Primary hyperparathyroidism. Primer. Key points. The case. What causes hypercalcemia?
 CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
SUMMARY OF THE PRODUCT CHARACTERISTICS
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Calcichew-D3 Mite Citron 500 mg/200 IU chewable tablets 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One tablet contains: Calcium carbonate
SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Calcichew-D3 Mite Citron 500 mg/200 IU chewable tablets 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One tablet contains: Calcium carbonate
4/20/2015. The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy. Learning Objectives
 Testing During Surgical Parathyroidectomy. Learning Objectives") The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
CASE PRESENTATION. Kārlis Rācenis MD - Latvia
 CASE PRESENTATION Kārlis Rācenis MD - Latvia o Patient men, 32-years-old o Admitted to the hospital at 12.09.16 due to kidney biopsy no complains 21.07 29.07.2016 Admitted to the hospital Acute kidney
CASE PRESENTATION Kārlis Rācenis MD - Latvia o Patient men, 32-years-old o Admitted to the hospital at 12.09.16 due to kidney biopsy no complains 21.07 29.07.2016 Admitted to the hospital Acute kidney
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD
 The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
SUMMARY OF THE PRODUCT CHARACTERISTICS
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D mite 500 mg/200 IU film-coated tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains 500 mg
SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D mite 500 mg/200 IU film-coated tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains 500 mg
Current Management of Metastatic Bone Disease
 Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
Calcium Conundrums. California Chapter AACE. September 2015
 Calcium Conundrums California Chapter AACE September 2015 Michael W. Yeh, MD Chief, Section of Endocrine Surgery Associate Professor of Surgery and Medicine David Geffen School of Medicine at UCLA www.endocrinesurgery.ucla.edu
Calcium Conundrums California Chapter AACE September 2015 Michael W. Yeh, MD Chief, Section of Endocrine Surgery Associate Professor of Surgery and Medicine David Geffen School of Medicine at UCLA www.endocrinesurgery.ucla.edu
Calcium is an important element found
 Paediatrica Indonesiana VOLUME 54 May NUMBER 3 Original Article Effect of calcium and vitamin D supplementation on serum calcium level in children with idiopathic nephrotic syndrome Vaya Dasitania, Alex
Paediatrica Indonesiana VOLUME 54 May NUMBER 3 Original Article Effect of calcium and vitamin D supplementation on serum calcium level in children with idiopathic nephrotic syndrome Vaya Dasitania, Alex
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes.
 Academic lectures 3rd year of Medical faculty Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes. ENDOCRINOLOGY
Academic lectures 3rd year of Medical faculty Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes. ENDOCRINOLOGY
Functional Medicine University s Functional Diagnostic Medicine Training Program
 Functional Diagnostic Medicine Training Program Module 7 * FMDT 563E Physiology of the Parathyroid Glands (Vitamin D Metabolism and Assessment) Limits of Liability & Disclaimer of Warranty We have designed
Functional Diagnostic Medicine Training Program Module 7 * FMDT 563E Physiology of the Parathyroid Glands (Vitamin D Metabolism and Assessment) Limits of Liability & Disclaimer of Warranty We have designed
CAL360 Tablets (Calcium citrate malate + Vitamin D3 )
") Published on: 18 Jan 2016 CAL360 Tablets ( citrate malate + Vitamin D3 ) Composition Each film-coated tablet contains: Citrate Malate equivalent to Elementary 250 mg Cholecalciferol Concentrate (powder
Published on: 18 Jan 2016 CAL360 Tablets ( citrate malate + Vitamin D3 ) Composition Each film-coated tablet contains: Citrate Malate equivalent to Elementary 250 mg Cholecalciferol Concentrate (powder
CHAPTER 27 LECTURE OUTLINE
 CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
Chapter 47. Media Directory. Calcium. Thyroid. Control of Calcium by Endocrine System. Drugs for Bone and Joint Disorders
 Chapter 47 Media Directory Slide 66 Calcitriol Animation Drugs for Bone and Joint Disorders Upper Saddle River, New Jersey 07458 All rights reserved. Calcium Adequate levels in body necessary To transmit
Chapter 47 Media Directory Slide 66 Calcitriol Animation Drugs for Bone and Joint Disorders Upper Saddle River, New Jersey 07458 All rights reserved. Calcium Adequate levels in body necessary To transmit
Chapter 2. Fluid, Electrolyte, and Acid-Base Imbalances
 Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Vitamins. Vitamins (continued) Lipid-Soluble Vitamins (A, D, E, K) Vitamins Serve Important Roles in Function of Body
 Lipid-Soluble Vitamins (A, D, E, K) Vitamins Serve Important Roles in Function of Body") Vitamins Drugs for Nutritional Disorders Organic substances are needed in small amounts Promote growth Maintain health Vitamins Human cells cannot produce vitamins Exception: vitamin D Vitamins or provitamins
Vitamins Drugs for Nutritional Disorders Organic substances are needed in small amounts Promote growth Maintain health Vitamins Human cells cannot produce vitamins Exception: vitamin D Vitamins or provitamins
Chapter 78 Parathyroid Glands
 Page 1 of 71 Editors: Mulholland, Michael W.; Lillemoe, Keith D.; Doherty, Gerard M.; Maier, Ronald V.; Upchurch, Gilbert R. Title: Greenfield's Surgery: SCIENTIFIC PRINCIPLES AND PRACTICE, 4th Edition
Page 1 of 71 Editors: Mulholland, Michael W.; Lillemoe, Keith D.; Doherty, Gerard M.; Maier, Ronald V.; Upchurch, Gilbert R. Title: Greenfield's Surgery: SCIENTIFIC PRINCIPLES AND PRACTICE, 4th Edition
Inpatient Pediatric Endocrinology. Tala Dajani MD MPH Pediatric Endocrinology of Phoenix
 Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems
Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems