CALCIUM CREATININE CLEARANCE RATIO IS NOT HELPFUL IN DIFFERENTIATING PRIMARY
|
|
|
- Alaina McCarthy
- 5 years ago
- Views:
Transcription
1 ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset and finalized. This version of the manuscript will be replaced with the final, published version after it has been published in the print edition of the journal. The final, published version may differ from this proof. Original Article EP CALCIUM CREATININE CLEARANCE RATIO IS NOT HELPFUL IN DIFFERENTIATING PRIMARY HYPERPARATHYROIDISM FROM FAMILIAL HERPERCALCEMIC HYPOCALCIURIA: A STUDY OF 1000 PATIENTS Edwina C Moore, MD, Eren Berber, MD, Judy Jin, MD, Vikram Krishnamurthy, MD, Joyce Shin, MD, Allan Siperstein, MD Running Title: Validity of CCCR in Primary Hyperparathyroidism From: Department of Endocrine Surgery, Cleveland Clinic, F/ Euclid Avenue, Cleveland, 44195, OHIO, United States Corresponding author: Edwina C Moore, MD Cleveland Clinic - Endocrine Surgery F20/9500 Euclid Avenue Cleveland Ohio edwina.bolshinsky@gmail.com / mooree@ccf.org Conflicts: There are no conflicts of interest
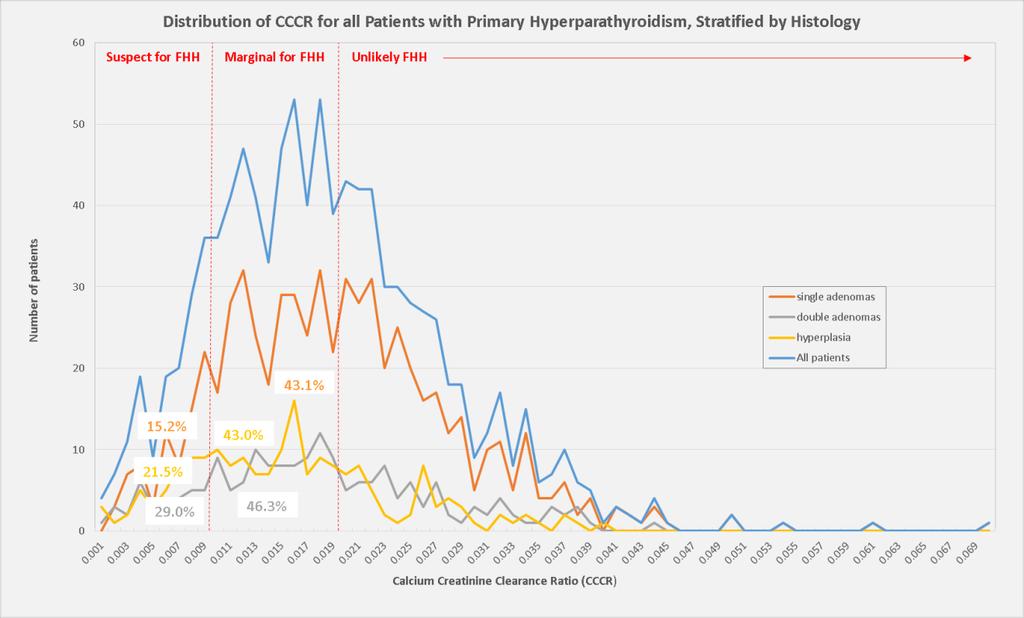
2 Abstract Objective: With increasing recognition of more subtle presentations of primary hyperparathyroidism (phpt), laboratory values are frequently seen in a range that would be expected for patients who have familial hypercalcemic hypocalciuria (FHH). Calcium creatinine clearance ratio (CCCR) has been advocated as a diagnostic tool to differentiate between these two disorders. However, it is limited by an indeterminate range ( ). The aim of this study is to assess the relevance of CCCR in a modern series of patients with surgically managed phpt. Methods: We performed a retrospective cohort study of 1000 patients who underwent parathyroid surgery for phpt over eleven years. CCCR was evaluated by degree of biochemical derangement, single versus multiple gland disease and interfering medications. Results: Patient demographics and resected histopathology were typical for a current series of patients with phpt. In retrospect, none of the patients were suspected to have FHH post operatively. CCCR was less than 0.01 for 19.0%, between for 43.7% and greater than 0.02 in 37.3%. Distribution of CCCR for patients free from interfering medications and different histological subtypes were the same. One third of the cohort had mild calcium elevations, more typical for FHH. Of these, almost two thirds had a CCCR in a range suspect for FHH (<0.02). Conclusion: To our knowledge this is the largest series to evaluate the validity of CCCR for patients with surgically confirmed ppht. The utility of CCCR in screening for FHH is limited, as 63% of modern patients with confirmed phpt have low values.
3 Introduction phpt is one of the most common endocrine disorders, with a disease prevalence of one case per 1000 population (1), but potentially higher as the diagnostic criteria broadens (2). Patients have hyper secretion of parathyroid hormone (PTH), usually from a single adenoma, leading to an elevation of serum calcium. Unfortunately, the clinical and biochemical profile are subject to significant individual variation, which can complicate diagnosis. One of the most critical steps for the endocrine surgeon is to exclude the potential for misdiagnosis with familial hypocalciuric hypercalcemia (FHH). First described in 1966 (3) and named by Foley in 1972 (4), FHH is a rare, autosomal dominant disorder usually caused by a heterozygous inactivating mutation in the calcium sensing receptor gene (CaSR) (5-6). Several additional genetic mutations have subsequently been associated with this disorder (7-9). The physiological defect is calcium hyposensitivity with associated hypercalcemia. It is important to identify these patients among hypercalcemic patients considering surgery, so as to avoid unnecessary surgery. Unlike patients with phpt, patients with FHH are asymptomatic with a normal phenotype and limited potential for sequelae (10). As phpt and FHH differ in their renal processing of calcium several markers of renal calcium excretion have been proposed to distinguish between the two disorders: 24 hour urine calcium
4 excretion, fasting urinary calcium excretion, calcium creatinine ratio and CCCR (5,11-19). Classically, urinary calcium is low in FHH, but despite its name this is not universally the case (20-21). In 2008, Christensen et al proposed a two-step diagnostic algorithm to exclude FHH from patients with suspected phpt. This includes calculating CCCR followed by genetic testing for all patients with CCCR<0.02. This two-step algorithm is reportedly associated with a sensitivity of 98% (17). The CCCR diagnostic cutoffs (<0.01 is FHH and >0.02 is phpt) dates from the first published series in 1981 (13). To our knowledge, no large scale study has confirmed the efficacy of CCCR in a modern series of patients surgically treated (and cured) for phpt, using the cutoffs previously described. Our primary aim was to evaluate the validity of CCCR, as a diagnostic test for FHH, amongst patients with suspected phpt. Secondary aims were to assess its utility for particular subgroups including patients with mild biochemical derangement, patients free from medications known to interfere with urine calcium excretion and histological variants of hyperparathyroidism. Methods Patients Over an eleven year period (Jan Jan ), 1847 patients were managed in a tertiary referral center for parathyroid disease. Preoperative workup and surgery was performed by one
5 of five staff surgeons. Indications for surgery followed the guidelines of the American Association of Endocrine Surgeons (22). Specific inclusion criteria were adult patients with biochemically proven primary hyperparathyroidism. Exclusion criteria were re-operative surgery. The study was approved by the Cleveland Clinic Institutional Review Board. Data collection The institution database, which is prospectively maintained, was accessed for patients surgically treated for phpt. Basic demographics (gender, age, primary complaint, medication history), preoperative biochemical markers (serum calcium, serum creatinine, serum phosphorus, PTH, Vitamin D, 24hour urine calcium and 24hour urine creatinine), indications for surgery, histology and postoperative biochemistry (serum calcium and PTH) were extracted. CCCR was calculated as [24hour urine calcium (mg/24hrs)/total serum calcium (mg/dl)]/[24 hour urine creatinine (mg/24hrs)/total serum creatinine (mg/dl)]. Statistical analysis The data was retrospectively analyzed. Metric variables are described by median and interquartile range (IQR) and categorical variables by absolute and relative frequencies. Regression analyses were completed using Excel and SPSS. Results We identified 1000 patients out of 1847, who had primary hyperparathyroidism and a complete set of biochemistry to calculate CCCR, over 11 years. All of these patients underwent parathyroid surgery and none, in retrospect, were suspected of having FHH.
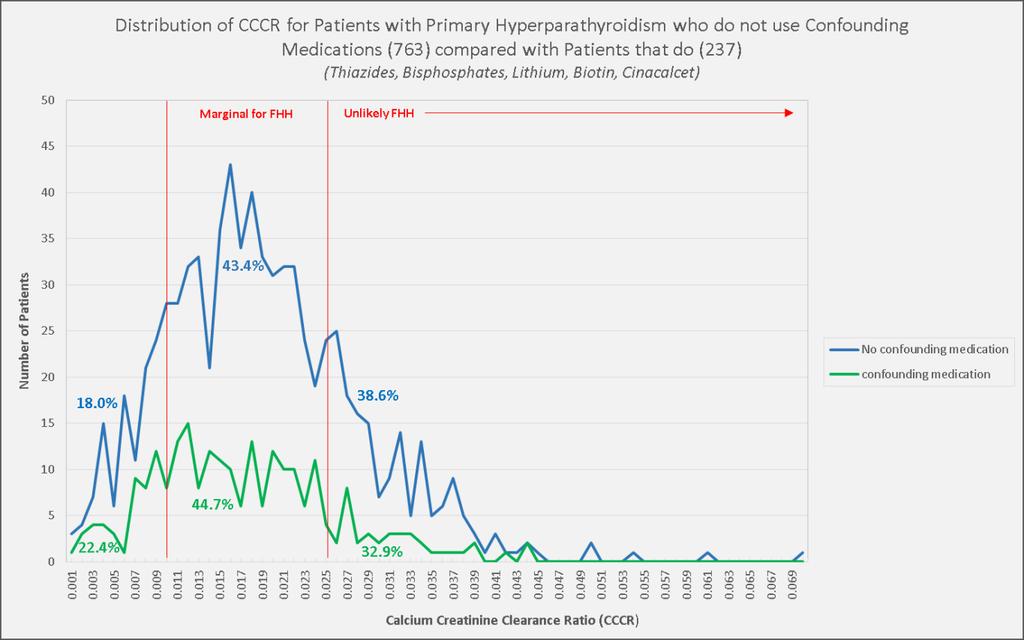
6 The majority of patients were female (79.7%) and the mean age was 60.7 years. Twenty-six patients had a history of prior neck radiation. Almost one in four patients (23.7%) used medications known to affect calcium excretion (thiazide 181, cinacalcet 6, bisphosphonate 62, lithium 10, biotin 6) at the time of surgery. The mean preoperative serum calcium was 10.8 mg/dl and PTH was 111 pg/ml parathyroid glands were excised from 1000 patients. Of these, 624 patients had single adenomas (624 adenomas, 62.4%), 186 patients had double adenomas (372 adenomas, 18.6%) and 190 patients had four gland hyperplasia (760 parathyroid glands, 19.0%). The distribution of CCCR for the total study population was 19.0% for CCCR<0.01, 43.7% for CCCR between and 37.3% for CCCR >0.02. A similar distribution was seen for each histological subtypes. (Inset Table 1 and Figure 1) When patients using medications known to interfere with calcium excretion were excluded (n=237) from the analysis, the distribution of CCCR was unchanged from the total population. More than two thirds of this subset of patients with histologically confirmed and biochemically cured primary hyperparathyroidism were still found to have a preoperative CCCR less than (CCCR< %, CCCR %, CCCR > %). (Inset Figure2) There were 303 patients with mild biochemical derangement (defined as serum Ca <10.8mg/dL and PTH <100pg/mL). Distribution of CCCR for this subgroup showed that 18% (n=137) had a
7 value less than 0.01 and 68.0% (n=206) had a value less than (Inset Figure 3). The distribution of CCCR was unaffected gender. On regression analysis, there was no correlation between PTH and Ca with CCCR. Figure 4 compares the regression analysis of Ca and CCCR for the total population and the subset with four gland hyperplasia. The proportion of patients with hyperplasia who had a low CCCR and a borderline serum calcium, was not statistically different to the proportion of patients in the entire population with a similar biochemical profile (19% v/v 31%). population. (Inset Figure 4). Discussion The treatment for patients with phpt is surgery, with a long term cure a rate of 95-99% depending on criteria used (22-23). By contrast, for patients with FHH who often have a similar clinical and biochemical presentation, surgical cure is 0%. Therefore it is imperative to differentiate between these two disorders preoperatively. The purpose of this study was to evaluate the validity of a widely accepted diagnostic test, CCCR, for a modern population with surgically proven phpt. Our results show that CCCR is not a useful index to preoperatively differentiate phpt from FHH and its routine use should be abandoned. Almost two thirds (62.7%) of our patients had a CCCR<0.02 and therefore by current recommendations would have been recommended to have had preoperative genetic analysis for
8 CaSR mutations. Notwithstanding that this is neither a practical nor a cost effective strategy, it is also completely unnecessary. All of the patients in our population had abnormal parathyroid glands removed at operation and were biochemically cured post operatively. As the prevalence of FHH is extremely rare, reportedly between 1:10000 and 1: (11, 19), it is possible that our population did not include a patient with FHH based on probability. In addition, with increasing recognition of FHH, such patients may have been screened out by primary care providers and never referred to us. However, in our subgroup of patients with mild biochemical derangement, who by definition are more likely to overlap with patients with FHH, two thirds still had a CCCR <0.02. Despite this all of them were found to have parathyroid disease and improved after surgery, thereby eliminating the possibility of misdiagnosis. Historical case series have identified that almost one third of patients with mild phpt have CCCR<0.01 and an additional one third have CCCR<0.02 (25). Our subgroup analysis is complementary. 21.8% of patients with mild phpt in our population had CCCR<0.01 and a further 46.2% had CCCR between 0.01 and Glendenning et al rationalized that as the ratio is influenced by both the degree of urinary calcium excretion and the degree of elevation of serum calcium, CCCR is a sensitive but increasingly less specific for milder presentations (16). In our study, CCCR was non-discriminatory for all biochemical presentations, subtle and more severe. The distribution of pathology in our study was similar to other studies: 61.1 % single adenomas, 20% double adenomas and 18.9% four gland hyperplasia (22-24). We did not find a significant
9 difference in the distribution of CCCR for each histological subtype. For single adenomas, double adenomas and four gland hyperplasia alike, approximately one third of each cohort had a CCCR<0.01 and two thirds had a CCCR <0.02. To our knowledge, this has not previously been described. Genetic testing is presently viewed as the gold standard to diagnose FHH. Notwithstanding, false negatives are possible if there are novel CaSR mutations (26-27) and the vast number of possible mutations makes the diagnostic process even more complex (27-28). Long prior to the availability of genomic tests, Marx et al proposed the diagnosis of FHH depended on observation of characteristic features within a family (13). This remains true and should be upheld. Clinical red flags for FHH include: asymptomatic hypercalcemia beginning in early life, relative hypocalciuria and multiple affected family members in an autosomal dominant inheritance pattern. Fasting urinary calcium excretion (CaE) has also been advocated, in place of CCCR, to diagnose FHH (17, 30). It is advantageous for the ease of spot urinary testing without the need for acidification compared with 24 hour collection (16). CaE<30umol/L GFR indicates avid renal calcium conservation typical of FHH however overlap can occur with phpt in the setting of very high PTH, calcium poor diets and use of thiazide medication (30, 31). For these reasons we did not evaluate CaE. Kalderli et al reviewed factors influencing urinary calcium excretion in phpt (32). They reported that 1,25 (OH)2 D3 and Osteocalcin were the only factors to independently correlate
10 with CCCR. Riss et al also reviewed the impact of thiazides on biochemical parameters in phpt and concluded that withdrawal was necessary for accurate diagnosis prior to surgery (33). By contrast in our study, there was little difference in the distribution of CCCR between patients taking and not taking similar medications and therefore we conclude that it is not relevant. The major limitation of this study was that the timing in the acquisition of preoperative blood and urine tests was variable. This was related to surgical scheduling and high number of external referrals where repeating tests would be unnecessary. However we consistently selected laboratory results that were drawn together and as close as possible to the date of surgery. Secondly, we did not assess 24 hour urine volume (nor fasting status at the time of urine collection) which can theoretically affect urine flow rate and mineral concentration, however in a population with normal renal function this is not likely to be significant. Thirdly, we only included patients with complete sets of laboratory values required to calculate CCCR. Conclusion The role of CCCR to preoperatively differentiate between phpt and FHH is questionable. Its utility is not enhanced by any histological subtype, exclusion of confounding medications or even for mild biochemical presentations. CCCR is cumbersome to perform and interpretation has low yield. It should not be prioritized in the diagnostic algorithm for patients with phpt. References
11 1. Clarke BL. Epidemiology of primary hyperparathyroidism. Endocrine Practice. 2013; 18; Press DM, Siperstein AE, Berber E, et al. The prevalence of undiagnosed and unrecognized primary hyperparathyroidism: A population-based analysis from the electronic medical record. Surgery. 2013: 154; Jackson CE, Boonstra CE. Hereditary Hypercalcemia and parathyroid hyperplasia without definite hyperparathyroidism. Journal of Laboratory and Clinical Medicine. 1966; Foley TP, Harrison HC, Arnaud CD and Harrison HE. Familial Benign Hypercalcemia. Journal of Pediatrics. 1972; 81: Brown EM, Gamba G, Riccardi D et al. Cloning and characterization of an extracellular Ca2+ receptor from bovine parathyroid. Nature. 1993; 366; Thakker RV. Disease associated with the extracellular calcium-sensing receptor. Cell Calcium 2004; 35: Ward BK, Magno AL, Blitvich BJ, et al. Novel mutations in the calcium-sensing receptor gene associated with biochemical and functional differences in familial hypocalciuric hypercalcaemia. Clin Endocrinol (Oxf). 2006; 64: D'Souza-Li L, Yang B, Canaff L, et al. Identification and functional characterization of novel calcium-sensing receptor mutations in familial hypocalciuric hypercalcemia and autosomal dominant hypocalcemia. J Clin Endocrinol Metab. 2002;87: Lietman SA, Tenenbaum-Rakover Y, Jap TS, et al. A novel loss-of-function mutation, Gln459Arg, of the calcium-sensing receptor gene associated with apparent autosomal recessive inheritance of familial hypocalciuric hypercalcemia. J Clin Endocrinol Metab. 2009; 94:
12 10. Pearce SHS, Trump D, Wooding C et al. Calcium-sensing receptor mutations in familial benign hypercalcemia and neonatal hyperparathyroidism. Journal of Clinical Investigation. 1995; 96: Shinall MC, McCrystal Dahir K, Broome JT. Differentiating familial hypocalciuric hypercalcemia from primary hyperparathyroidism. Endocrine Practice 2013;19: Tfelt-Hansen J, Brown EM. The calcium-sensing receptor in hereditary disorders of calcium homeostasis. Clinical Cases of Mineral Bone Metabolism. 2006; 3: Glendenning, P. Diagnosis of primary hyperparathyroidism: controversies, practical issues and the need for Australian guidelines. Internal Medicine Journal. 2003; 33: Christensen SE, Nissen PH, Vestergaard P, Heickendorff L, Brixen K, Mosekilde L. Discriminative power of three indices of renal calcium excretion for the distinction between familial hypocalciuric hypercalcemia and primary hyperparathyroidism: a follow up study on methods. Clinical Endocrinology. 2008; 69: Marx SJ, Attie MF, Levine MA et al. The hypocalciuric or benign variant of familial hypercalcemia: clinical and biochemical features in 15 kindreds. Medicine (Baltimore). 1981;69: Christensen SE, Nissen PH, Vestergaard P, et al. Skeletal consequences of familial hypocalciuric hypercalcaemia vs. primary hyperparathyroidism. Clinical Endocrinology. 2009; 71: Christensen SE. PhD thesis: Calcium and bone metabolism in familial hypocalciuric hypercalcemia and primary hyperparathyroidism, Faculty of Health Sciences, University of Aarhus, Aarhus, Denmark 2009; 1-106
13 18. Carling T, Szabo E, Bai M, et al. Familial hypercalcemia and hypercalciuria caused by a novel mutation in the cytoplasmic tail of the calcium receptor. Journal of Clinical Endocrinology and Metabolism. 2000; 85: Pasieka JL, Andersen MA and Hanley DA. Familial benign hypercalcemia: hypercalciuria and hypocalcemia in affected members of a small kindred. Clinical Endocrinology. 1990; 33: Wilhelm SM, Wang TS, Ruan DT, et al. The American Association of Endocrine Surgeons Guidelines for Definitive Management of Primary Hyperparathyroidism. JAMA. 2016; 151: Udelsman R1, Donovan P, Shaw C. Cure predictability during parathyroidectomy. World Journal of Surgery. 2014; 38: Abboud B, Sleilaty G, Helou E, et al. Existence and anatomic distribution of double parathyroid adenoma. Laryngoscope. 2005; 115: Gunn IR, Wallace JR. Urine Calcium and Serum Ionized Calcium, Total Calcium and Parathyroid Hormone Concentrations in the Diagnosis of Primary Hyperparathyroidism and Familial Benign Hypercalcaemia. Annals of Clinical Biochemistry 1992; 29: Guarnieri V1, Canaff L, Yun FH, et al. Calcium-sensing receptor (CASR) mutations in hypercalcemic states: studies from a single endocrine clinic over three years. Journal of Clinical Endocrinology and Metabolism. 2010; 95: Chou YH, Brown EM, Levi T, et al. The gene responsible for familial hypocalciuric hypercalcemia maps to chromosome 3q in four unrelated families. Nat Genet. 1992; 1:
14 26. Nissen PH, Christensen SE, Heickendirff L, Brixen K, Mosekilde L. Molecular Genetic Analysis of the Calcium Sensing Receptor Gene in Patients Clinically Suspected to Have Familial Hypocalciuric Hypercalcemia: Phenotypic Variation and Mutation Spectrum in a Danish Population. The Journal Clinical Endocrinology & Metabolism. 2007; 92: Hendy GN, Guarnieri V, Canaff L. Calcium-sensing receptor and associated diseases. Prog Mol Biol Transl Sci. 2009; 89: Stuckey BG, Kent GN, Gutteridge DH, Pullan PT, Price RI, Bhagat C. Fasting calcium excretion and parathyroid horomone together distinguish familian hypocalciuric herpercalcemia from primary hyperparathyroidism. Endocrinology. 1987; 27: Friedman PA, Bushinsky DA. Diuretic effects on calcium metabolism. Seminars in nephrology. 1999; 19: Kaderli RM, Riss P, Geroldinger A, Selberherr A, Scheuba C, Niederle B. Factors influencing pre operative urinary calcium excretion in primary hyperparathyroidism. Clinical Endocrinology 2017; : Riss P, KammerM, Selberherr A, et al. The influence of thiazide intake on calcium and parathyroid hormone levels in patients with primary hyperparathyroidism. Clinical Endocrinology. 2016; 85:
15 Table 1: Proportion of patients with phpt and their CCCR, stratified by histology Histology Number CCCR<0.01 % CCCR % CCCR>0.02 % of patients All patients Single Adenomas Double Adenomas Four Gland Hyperplasia
16
17
18 Serum Calcium (mg/dl) 15 Regression Analysis of Serum Calcium and CCCR for the Total Population Suspect for FHH Marginal for FHHUnlikely FHH R² = Calcium Creatinine Clearance Ratio (CCCR)
19 Serum Calcium (mg/dl) 16 Regression Analysis of Serum Calcium and CCCR for Patients with Four Gland Hyperplasia Suspect for FHHMarginal for FHHUnlikely FHH R² = Calcium Creatinine Clearance Ratio (CCCR)
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
HYPERCALCEMIA (FHH) IN A YOUNG HISPANIC MAN. Running title: New mutation Calcium Sensing Receptor causing FHH.
 IN A YOUNG HISPANIC MAN. Running title: New mutation Calcium Sensing Receptor causing FHH.") AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
King s Research Portal
 King s Research Portal DOI: 10.1002/ccr3.1074 Document Version Publisher's PDF, also known as Version of record Link to publication record in King's Research Portal Citation for published version (APA):
King s Research Portal DOI: 10.1002/ccr3.1074 Document Version Publisher's PDF, also known as Version of record Link to publication record in King's Research Portal Citation for published version (APA):
Primary Hyperparathyroidism
 Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
When the level of calcium in the blood falls too low, the parathyroid glands secrete just enough PTH to restore the blood calcium level.
 Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Disclosure. Topic Outline. Calcium, Vitamin D, PTH Disorders. PTH/Calcium-Normal Physiology. I have nothing to disclose
 Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
ORIGINAL ARTICLE. Persistent Parathyroid Hormone Elevation Following Curative Parathyroidectomy for Primary Hyperparathyroidism
 Persistent Parathyroid Hormone Elevation Following Curative Parathyroidectomy for Primary Hyperparathyroidism Elizabeth A. Mittendorf, MD; Christopher R. McHenry, MD ORIGINAL ARTICLE Background: Persistent
Persistent Parathyroid Hormone Elevation Following Curative Parathyroidectomy for Primary Hyperparathyroidism Elizabeth A. Mittendorf, MD; Christopher R. McHenry, MD ORIGINAL ARTICLE Background: Persistent
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease?
 Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
A novel mutation of the calcium-sensing receptor gene in a Greek family from Nisyros
 HORMONES 2015, 14(2):321-325 Letter to the Editor A novel mutation of the calcium-sensing receptor gene in a Greek family from Nisyros Evaggelia Zapanti, 1 Aikaterini Polonifi, 2 Michalis Kokkinos, 2 George
HORMONES 2015, 14(2):321-325 Letter to the Editor A novel mutation of the calcium-sensing receptor gene in a Greek family from Nisyros Evaggelia Zapanti, 1 Aikaterini Polonifi, 2 Michalis Kokkinos, 2 George
Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012.
 Levels Shireen Fatemi, M.D. April, 2012.") Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012 Disclosures I have no financial relationships with commercial interests,
Current Concepts in the Evaluation and Management of Abnormal Parathyroid Hormone (PTH) Levels Shireen Fatemi, M.D. April, 2012 Disclosures I have no financial relationships with commercial interests,
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand
 International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
Disclosure. Primary Hyperparathyroidism 4 th IW. Topic Outline. Calcium, Vitamin D, PTH Disorders. I have nothing to disclose related to this topic
 Disclosure Calcium, Vitamin D, PTH Disorders Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF I have nothing to disclose related to this topic Topic Outline Calcium/Vitamin
Disclosure Calcium, Vitamin D, PTH Disorders Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF I have nothing to disclose related to this topic Topic Outline Calcium/Vitamin
4/20/2015. The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy. Learning Objectives
 Testing During Surgical Parathyroidectomy. Learning Objectives") The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
Calcium-sensing receptors
 Making sense of calcium Calcium-sensing receptors Prof Arthur D Conigrave School of Molecular Bioscience, University of Sydney Department of Endocrinology, Royal Prince Alfred Hospital The calcium-sensing
Making sense of calcium Calcium-sensing receptors Prof Arthur D Conigrave School of Molecular Bioscience, University of Sydney Department of Endocrinology, Royal Prince Alfred Hospital The calcium-sensing
2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT)
") 2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT) Scott M. Wilhelm, MD, FACS Associate Professor and Section Head Endocrine Surgery University Hospitals-Cleveland
2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT) Scott M. Wilhelm, MD, FACS Associate Professor and Section Head Endocrine Surgery University Hospitals-Cleveland
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones
 Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Plasma 25-hydroxyvitamin D, 1,25-dihydroxyvitamin D, and parathyroid hormone in familial hypocalciuric hypercalcemia and primary hyperparathyroidism
 European Journal of Endocrinology (2008) 159 719 727 ISSN 0804-4643 CLINICAL STUDY Plasma 25-hydroxyvitamin D, 1,25-dihydroxyvitamin D, and parathyroid hormone in familial hypocalciuric hypercalcemia and
European Journal of Endocrinology (2008) 159 719 727 ISSN 0804-4643 CLINICAL STUDY Plasma 25-hydroxyvitamin D, 1,25-dihydroxyvitamin D, and parathyroid hormone in familial hypocalciuric hypercalcemia and
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
What this study adds: - Sustained hypercalacemia affects 1 in 500 children in a general hospital setting
 FREQUENCY AND AETIOLOGY OF HYPERCALCAEMIA McNeilly JD 1, Boal R 2, Shaikh MG 2, Ahmed SF 2 1 Dept of Clinical Biochemistry, Queen Elizabeth University Hospital, Greater Glasgow & Clyde NHS Trust, Glasgow,
FREQUENCY AND AETIOLOGY OF HYPERCALCAEMIA McNeilly JD 1, Boal R 2, Shaikh MG 2, Ahmed SF 2 1 Dept of Clinical Biochemistry, Queen Elizabeth University Hospital, Greater Glasgow & Clyde NHS Trust, Glasgow,
Parathyroid Imaging. A Guide to Parathyroid Surgery
 Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
A novel CaSR mutation presenting as a severe case of neonatal familial hypocalciuric hypercalcemia
 Tonyushkina et al. International Journal of Pediatric Endocrinology 2012, 2012:13 CASE REPORT Open Access A novel CaSR mutation presenting as a severe case of neonatal familial hypocalciuric hypercalcemia
Tonyushkina et al. International Journal of Pediatric Endocrinology 2012, 2012:13 CASE REPORT Open Access A novel CaSR mutation presenting as a severe case of neonatal familial hypocalciuric hypercalcemia
Challenges in the Management of Primary HPTH. Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH
 Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
COLLISION DIAGNOSES: PRIMARY HYPERPARATHYROIDISM LAYERED ON FAMILIAL HYPOCALCIURIC HYPERCALCEMIA
 Case Report COLLISION DIGNOSES: PRIMRY HYPERPRTHYROIDISM LYERED ON FMILIL HYPOCLCIURIC HYPERCLCEMI Seth Kay, MD 1 ; Mara Piltin, DO 2 ; Vicoria Loseva, MD 3 ; ridget Sinnott, MD 3 ; J. Robert rennan, MD
Case Report COLLISION DIGNOSES: PRIMRY HYPERPRTHYROIDISM LYERED ON FMILIL HYPOCLCIURIC HYPERCLCEMI Seth Kay, MD 1 ; Mara Piltin, DO 2 ; Vicoria Loseva, MD 3 ; ridget Sinnott, MD 3 ; J. Robert rennan, MD
Since the advent of multichannel serum chemistry
 ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS
 Original Article RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS Charles D. Livingston, MD, FACS ABSTRACT Objective: To examine an individualized approach to patients with primary
Original Article RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS Charles D. Livingston, MD, FACS ABSTRACT Objective: To examine an individualized approach to patients with primary
Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from the West?
 ecommons@aku Section of Urology Department of Surgery August 1999 Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from
ecommons@aku Section of Urology Department of Surgery August 1999 Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from
Minimally invasive parathyroidectomy
 Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Coexistence of parathyroid adenoma and papillary thyroid carcinoma. Yong Sang Lee, Kee-Hyun Nam, Woong Youn Chung, Hang-Seok Chang, Cheong Soo Park
 J Korean Surg Soc 2011;81:316-320 http://dx.doi.org/10.4174/jkss.2011.81.5.316 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Coexistence of parathyroid
J Korean Surg Soc 2011;81:316-320 http://dx.doi.org/10.4174/jkss.2011.81.5.316 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Coexistence of parathyroid
UPDATES ON PRIMARY HYPERPARATHYROIDISM. Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY
 UPDATES ON PRIMARY HYPERPARATHYROIDISM Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY Disclosures Speaker (Honorarium): Shire Off-label use of estrogen, raloxifene
UPDATES ON PRIMARY HYPERPARATHYROIDISM Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY Disclosures Speaker (Honorarium): Shire Off-label use of estrogen, raloxifene
Calcium & Calcium-sensing receptors
 Calcium & Calcium-sensing receptors Prof Arthur D Conigrave School of Life & Environmental Sciences, University of Sydney Department of Endocrinology, Royal Prince Alfred Hospital Collaborators Sydney
Calcium & Calcium-sensing receptors Prof Arthur D Conigrave School of Life & Environmental Sciences, University of Sydney Department of Endocrinology, Royal Prince Alfred Hospital Collaborators Sydney
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy
 "Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma
 ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Calcium Conundrums. California Chapter AACE. September 2015
 Calcium Conundrums California Chapter AACE September 2015 Michael W. Yeh, MD Chief, Section of Endocrine Surgery Associate Professor of Surgery and Medicine David Geffen School of Medicine at UCLA www.endocrinesurgery.ucla.edu
Calcium Conundrums California Chapter AACE September 2015 Michael W. Yeh, MD Chief, Section of Endocrine Surgery Associate Professor of Surgery and Medicine David Geffen School of Medicine at UCLA www.endocrinesurgery.ucla.edu
Hypercalcemia may be detected incidentally. Practice CMAJ. Primary hyperparathyroidism. Primer. Key points. The case. What causes hypercalcemia?
 CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
Comparison of indocyanine green fluorescence and parathyroid autofluorescence imaging in the identification of parathyroid glands during thyroidectomy
 Original Article Comparison of indocyanine green fluorescence and parathyroid autofluorescence imaging in the identification of parathyroid glands during thyroidectomy Bora Kahramangil, Eren Berber Department
Original Article Comparison of indocyanine green fluorescence and parathyroid autofluorescence imaging in the identification of parathyroid glands during thyroidectomy Bora Kahramangil, Eren Berber Department
Supplementary Online Content
 Supplementary Online Content Wilhelm SM, Wang TS, Ruan DT, et al. The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. Published
Supplementary Online Content Wilhelm SM, Wang TS, Ruan DT, et al. The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. Published
Secondary and Familial Hyperparathyroidism
 Secondary and Familial Jeffrey F. Moley, M.D. Chief, Endocrine and Oncologic Surgery Section, Professor of Surgery Associate Director, The Alvin J. Siteman Cancer Center Occurs in setting of CRF Chronic
Secondary and Familial Jeffrey F. Moley, M.D. Chief, Endocrine and Oncologic Surgery Section, Professor of Surgery Associate Director, The Alvin J. Siteman Cancer Center Occurs in setting of CRF Chronic
Six hundred fifty-six consecutive explorations for primary hyperparathyroidism Udelsman R
 Six hundred fifty-six consecutive explorations for primary hyperparathyroidism Udelsman R Record Status This is a critical abstract of an economic evaluation that meets the criteria for inclusion on NHS
Six hundred fifty-six consecutive explorations for primary hyperparathyroidism Udelsman R Record Status This is a critical abstract of an economic evaluation that meets the criteria for inclusion on NHS
Calcium and Parathyroid Disorders
 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Monija Mrgan 1, Sanne Nielsen 1 and Kim Brixen 2. The Role of Calcium in the Human Body
 Acta Clin Croat 2014; 53:220-225 Review Familial hypocalciuric hypercalcemia and calcium sensing receptor Monija Mrgan 1, Sanne Nielsen 1 and Kim Brixen 2 1 Sydvestjysk Sygehus, Esbjerg; 2 Odense Universitetshospital,
Acta Clin Croat 2014; 53:220-225 Review Familial hypocalciuric hypercalcemia and calcium sensing receptor Monija Mrgan 1, Sanne Nielsen 1 and Kim Brixen 2 1 Sydvestjysk Sygehus, Esbjerg; 2 Odense Universitetshospital,
Identification of AP2S1 Mutation and Effects of Low Calcium Formula in an Infant With Hypercalcemia and Hypercalciuria
 JCEM ONLINE Advances in Genetics Endocrine Research Identification of AP2S1 Mutation and Effects of Low Calcium Formula in an Infant With Hypercalcemia and Hypercalciuria Yasuko Fujisawa, Rie Yamaguchi,
JCEM ONLINE Advances in Genetics Endocrine Research Identification of AP2S1 Mutation and Effects of Low Calcium Formula in an Infant With Hypercalcemia and Hypercalciuria Yasuko Fujisawa, Rie Yamaguchi,
What is the right calcium balance?
 For patients with hypoparathyroidism What is the right calcium balance? Indications and Usage1 NATPARA is a parathyroid hormone indicated as an adjunct to calcium and vitamin D to control hypocalcemia
For patients with hypoparathyroidism What is the right calcium balance? Indications and Usage1 NATPARA is a parathyroid hormone indicated as an adjunct to calcium and vitamin D to control hypocalcemia
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment
 Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Marcin Barczynski, 1 Aleksander Konturek, 2 Alicja Hubalewska-Dydejczyk, 2. Filip Gołkowski, 1 Stanislaw Cichon, 1 Piotr Richter, 1 Wojciech Nowak
 3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
Sensipar (cinacalcet)
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
HPI joint pain/arthritis serum calcium 11.5 PTH 147pg/ml
 HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
Cases in Endocrinology
 Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Head and Neck Endocrine Surgery
 Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Hyper and hypocalcaemia. Prof Tricia Tan
 Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
Hyper and hypocalcaemia Prof Tricia Tan Learning Objectives Basic physiology of Ca regulation Case presentations Take home messages Calcium Total body calcium content ~1300g 99% in bone 1% intracellular
ORIGINAL ARTICLE. An Optimal Algorithm for Intraoperative Parathyroid Hormone Monitoring
 ORIGINAL ARTICLE An Optimal Algorithm for Intraoperative Parathyroid Hormone Monitoring Melanie L. Richards, MD; Geoffrey B. Thompson, MD; David R. Farley, MD; Clive S. Grant, MD Background: A minimally
ORIGINAL ARTICLE An Optimal Algorithm for Intraoperative Parathyroid Hormone Monitoring Melanie L. Richards, MD; Geoffrey B. Thompson, MD; David R. Farley, MD; Clive S. Grant, MD Background: A minimally
Primary hyperparathyroidism (HPT) has an incidence of
 has an incidence of") Dual-Phase Tc-Sestamibi Imaging: Its Utility in Parathyroid Hyperplasia and Use of Immediate/ Delayed Image Ratios to Improve Diagnosis of Hyperparathyroidism Leonie Gordon, MD; William Burkhalter, MD;
Dual-Phase Tc-Sestamibi Imaging: Its Utility in Parathyroid Hyperplasia and Use of Immediate/ Delayed Image Ratios to Improve Diagnosis of Hyperparathyroidism Leonie Gordon, MD; William Burkhalter, MD;
International Journal of Biological & Medical Research. An Uncommon Case of Persistent Hypercalcaemia following Parathyroid Surgery
 Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
Elena Castellano, Roberto Attanasio, Laura Gianotti, Flora Cesario, Francesco Tassone, and Giorgio Borretta
 ORIGINAL ARTICLE Forearm DXA Increases the Rate of Patients With Asymptomatic Primary Hyperparathyroidism Meeting Surgical Criteria Elena Castellano, Roberto Attanasio, Laura Gianotti, Flora Cesario, Francesco
ORIGINAL ARTICLE Forearm DXA Increases the Rate of Patients With Asymptomatic Primary Hyperparathyroidism Meeting Surgical Criteria Elena Castellano, Roberto Attanasio, Laura Gianotti, Flora Cesario, Francesco
Research Article The Cost of Prolonged Hospitalization due to Postthyroidectomy Hypocalcemia: A Case-Control Study
 Advances in Endocrinology, Article ID 954194, 4 pages http://dx.doi.org/10.1155/2014/954194 Research Article The Cost of Prolonged Hospitalization due to Postthyroidectomy Hypocalcemia: A Case-Control
Advances in Endocrinology, Article ID 954194, 4 pages http://dx.doi.org/10.1155/2014/954194 Research Article The Cost of Prolonged Hospitalization due to Postthyroidectomy Hypocalcemia: A Case-Control
Summary Statement from a Workshop on Asymptomatic Primary Hyperparathyroidism: A Perspective for the 21st Century
 Summary Statement from a Workshop on Asymptomatic Primary Hyperparathyroidism: A Perspective for the 21st Century John P. Bilezikian, John T. Potts, Jr., Ghada El-Hajj Fuleihan, Michael Kleerekoper, Robert
Summary Statement from a Workshop on Asymptomatic Primary Hyperparathyroidism: A Perspective for the 21st Century John P. Bilezikian, John T. Potts, Jr., Ghada El-Hajj Fuleihan, Michael Kleerekoper, Robert
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary
 Prior Authorization with Quantity Limit Program Summary") Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Sensipar. Sensipar (cinacalcet) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
al.. A homozygous inactivating calcium-sensing receptor mutation, Pro339Thr, is associated with isolated
 A homozygous inactivating calcium-sensing receptor mutation, ProThr, is associated with isolated primary hyperparathyroidism: correlation between location of mutations and severity of hypercalcaemia Fadil
A homozygous inactivating calcium-sensing receptor mutation, ProThr, is associated with isolated primary hyperparathyroidism: correlation between location of mutations and severity of hypercalcaemia Fadil
Preoperative Localization and Intraoperative Parathyroid Hormone Assay in Korean Patients with Primary Hyperparathyroidism
 Original Article Endocrinol Metab 2014;29:464-469 http://dx.doi.org/10.3803/enm.2014.29.4.464 pissn 2093-596X eissn 2093-5978 Preoperative Localization and Intraoperative Parathyroid Hormone Assay in Korean
Original Article Endocrinol Metab 2014;29:464-469 http://dx.doi.org/10.3803/enm.2014.29.4.464 pissn 2093-596X eissn 2093-5978 Preoperative Localization and Intraoperative Parathyroid Hormone Assay in Korean
Post-operative Transient Hypoparathyroidism: Incidence and Risk Factors
 ORIGINAL ARTICLE Post-operative Transient Hypoparathyroidism: Incidence and Risk Factors sensitivity (2)(3), which can cause significant morbidity for patients if it goes unrecognized (4). Symptomatic
ORIGINAL ARTICLE Post-operative Transient Hypoparathyroidism: Incidence and Risk Factors sensitivity (2)(3), which can cause significant morbidity for patients if it goes unrecognized (4). Symptomatic
Normocalcemic Primary Hyperparathyroidism: A Comparison with the Hypercalcemic Form in a Tertiary Referral Population
 Pierreux Jan, Bravenboer Bert. Normocalcemic Primary Hyperparathyroidism: A Horm Metab Res 2018; 00: 00 00 Normocalcemic Primary Hyperparathyroidism: A Comparison with the Hypercalcemic Form in a Tertiary
Pierreux Jan, Bravenboer Bert. Normocalcemic Primary Hyperparathyroidism: A Horm Metab Res 2018; 00: 00 00 Normocalcemic Primary Hyperparathyroidism: A Comparison with the Hypercalcemic Form in a Tertiary
Outline. Parathyroid Localization Studies. Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center
 Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Complementary sestamibi scintigraphy and ultrasound for primary hyperparathyroidism
 Nuclear Medicine and Biomedical Imaging Research Article Complementary sestamibi scintigraphy and ultrasound for primary hyperparathyroidism Yang Z 1,3 *, Li AY 2, Alexander G 3 and Chadha M 3 1 Department
Nuclear Medicine and Biomedical Imaging Research Article Complementary sestamibi scintigraphy and ultrasound for primary hyperparathyroidism Yang Z 1,3 *, Li AY 2, Alexander G 3 and Chadha M 3 1 Department
DIAGNOSING X-LINKED HYPOPHOSPHATEMIA (XLH) BIOCHEMICAL TESTING CONSIDERATIONS
 BIOCHEMICAL TESTING CONSIDERATIONS") DIAGNOSING X-LINKED HYPOPHOSPHATEMIA (XLH) BIOCHEMICAL TESTING CONSIDERATIONS XLH IS CHARACTERIZED BY CHRONIC HYPOPHOSPHATEMIA XLH is a hereditary, progressive, lifelong disorder. In children and adults,
DIAGNOSING X-LINKED HYPOPHOSPHATEMIA (XLH) BIOCHEMICAL TESTING CONSIDERATIONS XLH IS CHARACTERIZED BY CHRONIC HYPOPHOSPHATEMIA XLH is a hereditary, progressive, lifelong disorder. In children and adults,
Current Status and Treatment
 Review article Current Status and Treatment of Primary Hyperparathyroidism By Dina M Elaraj, MD Orlo H Clark, MD Abstract Primary hyperparathyroidism (HPT) is diagnosed in approximately 100,000 patients
Review article Current Status and Treatment of Primary Hyperparathyroidism By Dina M Elaraj, MD Orlo H Clark, MD Abstract Primary hyperparathyroidism (HPT) is diagnosed in approximately 100,000 patients
AP2S1 and GNA11 mutations not a common cause of familial
 Page 1 of 25 Accepted Preprint first posted on 15 November 2016 as Manuscript EJE-16-0842 1 2 AP2S1 and GNA11 mutations not a common cause of familial hypocalciuric hypercalcemia 3 Silje Hovden 1, Lars
Page 1 of 25 Accepted Preprint first posted on 15 November 2016 as Manuscript EJE-16-0842 1 2 AP2S1 and GNA11 mutations not a common cause of familial hypocalciuric hypercalcemia 3 Silje Hovden 1, Lars
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary
 Prior Authorization with Quantity Limit Program Summary") Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 2 Available Product Indication Dosing and Administration Natpara (parathyroid hormone)
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 2 Available Product Indication Dosing and Administration Natpara (parathyroid hormone)
Hypophosphatemic rickets: new treatments
 Hypophosphatemic rickets: new treatments Gema Ariceta Pediatric Nephrology, University Hospital Vall d Hebron, Barcelona 1 11.06.18 Tubulopathies Disclosures Lectures and educational activities sponsored
Hypophosphatemic rickets: new treatments Gema Ariceta Pediatric Nephrology, University Hospital Vall d Hebron, Barcelona 1 11.06.18 Tubulopathies Disclosures Lectures and educational activities sponsored
Iperparatiroidismo normocalcemico: vero o falso?
 Iperparatiroidismo normocalcemico: vero o falso? Bari, 7-10 novembre 2013 TERAPIA E FOLLOW-UP A. Piovesan SCDU Endocrinologia Oncologica AO Città della Salute e della Scienza Molinette Torino THE THIRD
Iperparatiroidismo normocalcemico: vero o falso? Bari, 7-10 novembre 2013 TERAPIA E FOLLOW-UP A. Piovesan SCDU Endocrinologia Oncologica AO Città della Salute e della Scienza Molinette Torino THE THIRD
Diagnostic Challenges in Multiple Endocrine Neoplasia Type 1 (MEN1) : Usefulness of Genetic Analysis
 : Usefulness of Genetic Analysis") Diagnostic Challenges in Multiple Endocrine Neoplasia Type 1 (MEN1) : Usefulness of Genetic Analysis Professor R. V. Thakker, FRS May Professor of Medicine University of Oxford, U.K. Meet The Experts 49
Diagnostic Challenges in Multiple Endocrine Neoplasia Type 1 (MEN1) : Usefulness of Genetic Analysis Professor R. V. Thakker, FRS May Professor of Medicine University of Oxford, U.K. Meet The Experts 49
Acute renal failure and unknown cause hypercalcemia (case report)
") Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Medical Expert
 Medical Expert") Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Protocol GTC : A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients.
 in Chronic Kidney Disease Patients.") Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Inpatient Pediatric Endocrinology. Tala Dajani MD MPH Pediatric Endocrinology of Phoenix
 Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems
Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems
PRIMARY HYPERPARATHYROIDISM WITH RICKETS. KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College
 PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
Update on Hypoparathyroidism: New Therapeutic Options and Management Guidelines
 Update on Hypoparathyroidism: New Therapeutic Options and Management Guidelines Dolores Shoback, MD Professor of Medicine - University of California, San Francisco California AACE Chapter Annual Meeting
Update on Hypoparathyroidism: New Therapeutic Options and Management Guidelines Dolores Shoback, MD Professor of Medicine - University of California, San Francisco California AACE Chapter Annual Meeting
Asymptomatic Primary Hyperparathyroidism
 The new england journal of medicine clinical practice Asymptomatic Primary Hyperparathyroidism John P. Bilezikian, M.D., and Shonni J. Silverberg, M.D. This Journal feature begins with a case vignette
The new england journal of medicine clinical practice Asymptomatic Primary Hyperparathyroidism John P. Bilezikian, M.D., and Shonni J. Silverberg, M.D. This Journal feature begins with a case vignette