HISTORY TB = 25% ADULT DEATHS EGYPTIAN MUMMIES: SPINAL TB. 19th CENTURY INDUSTRIALIZATION. 17 th -18th CENTURIES- URBANIZATION MID 24
|
|
|
- Claribel Weaver
- 5 years ago
- Views:
Transcription

1 HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS

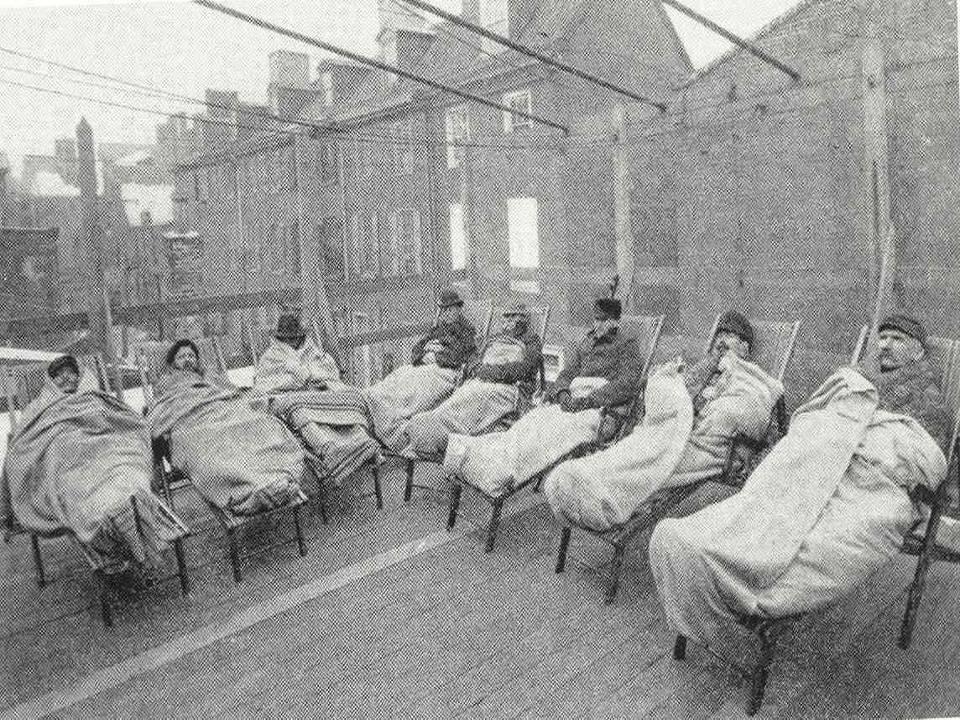
2 GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA


3

4
5 ANTIBIOTICS STREPTOMYCIN RAPID DEVELOPMENT OF FAILURE WITH MONOTHERAPY INH =MAGIC BULLET RIFAMPIN & SHORT COURSE RX EPIDEMIOLOGY M. TUBERCULOSIS INFECTS 1/3 WORLD S POPULATION 9.2 MILLION NEW TB CASES MILLION DEATHS ND TO HIV AS CAUSE OF DEATH FROM INFECTIOUS DISEASE 14.4 MILLION PREVALENT CASES
6 Estimated numbers of new cases, 2006 Estimated number of new TB cases (all forms) No estimate or more Estimated TB incidence rate, 2006 Estimated new TB cases (all forms) per population No estimate or more
 per 100 000 population No report 0 24 25 49 50 99 100 or more")

7 Tuberculosis notification rates, 2006 Notified TB cases (new and relapse) per population No report or more The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health
8 Estimated HIV prevalence in new TB cases, 2006 HIV prevalence in TB cases, (%) No estimate or more The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO All rights reserved Geographical distribution of HIV-positive TB cases, Zimbabw e 4% Zambia UR Tanzania 3% 3% Uganda 2% AFR* 10% Othe rs 15% Côte d'ivoire 2% Ethiopia 3% DR Congo 3% EMR WPR SEAR* India Sw aziland 1% South Africa 29% Ke nya 10% Malawi 5% Mozambique Nigeria 4% 6% 5 0 Russian Fe deratn EUR* AMR* Brazil For each country or region, the number of incident TB cases arising in people with HIV is shown as a percentage of the global total of such cases. AFR* is all countries in the WHO African Region except those shown separately; AMR* excludes Brazil; EUR* excludes the Russian Federation; SEAR* excludes India.
9 Fifteen countries with the highest estimated TB incidence rates per capita and corresponding incidence rates of HIVpositive TB cases, 2006 Swaziland South Africa Djibouti Namibia Lesotho Zimbabw e Timor-Leste Zambia Botswana Sierra Leone Cambodia Mozambique Côte d'ivoire All TB TB with HIV infection Congo Rwanda RISING INCIDENCE WORLDWIDE FAILURE OF PUBLIC HEALTH FAILURE OF POLITICAL WILL RX TO CURE COSTS $12/PT >95% TB IS IN RESOURCE POOR CONTRIES MONEY & INFRASTRUCTURE
10 TB Case Rates,* United States, 2006 D.C. *Cases per 100,000. < 3.5 (year 2000 target) > 4.6 (national average) DEVELOPED WORLD TB DOWNWARD TREND BEFORE ANTIBIOTICS: WHY? 1900-WW2: ANNUAL DECREASE 4-6% IN DEVELOPING COUNTRIES Higher natural resistance Better living conditions-less crowding Effect of sanatoriums

11 No. of Cases Reported TB Cases* United States, ,000 26,000 24,000 22,000 20,000 18,000 16,000 14,000 12,000 10, *Updated as of April 6, Year
12
13
14 Reported TB Cases by Race/Ethnicity* United States, 2006 American Indian or Alaska Native (1%) White (17%) Native Hawaiian or Other Pacific Islander (<1%) Asian (24%) Hispanic or Latino (30%) Black or African-American (27%) *All races are non-hispanic. Persons reporting two or more races accounted for less than 1% of all cases.
15 TB Case Rates by Race/Ethnicity* United States, ** Cases per 100, Asian/Pacific Islander Black or African-American Hispanic American Indian/Alaska Native White *All races are non-hispanic. In 2003, Asian/Pacific Islander category includes persons who reported race as Asian only and/or Native Hawaiian or Other Pacific Islander only. **Updated as of April 6, Number of TB Cases in U.S.-born vs. Foreign-born Persons United States, * No. of Cases U.S.-born Foreign-born *Updated as of April 6, 2007.
16 Percentage of TB Cases Among Foreign-born Persons, United States* DC DC *Updated as of April 6, >50% 25% 49% <25% Trends in TB Cases in Foreign-born Persons, United States, * No. of Cases 10,000 8,000 6,000 4,000 2, Percentage No. of Cases Percentage of Total Cases *Updated as of April 6, 2007.
17 Countries of Birth of Foreign-born Persons Reported with TB United States, 2006 Other Countries (38%) Mexico (25%) Guatemala (3%) Haiti (3%) China (5%) India (7%) Viet Nam (8%) Philippines (11%) M. Tuberculosis complex Mycobacterium tuberculosis Mycobacterium bovis: unpasteurized milk/cheese Mycobacterium africanum & canetti Mycobacterium microti : rodents



18 THE BACILLUS CELL WALL CONTENT=LIPIDS SLOW GROWTH: 20 hours vs. 20 minutes for E.Coli Length of RX TRANSMISSION Lungs=entry portal Inhalation of droplet nuclei Coughing: 3000 droplet nuclei/cough Talking: 5 minutes Sneezing: BEST
19 TRANSMISSION ENHANCERS INOCULUM SIZE: - AUTOPSY SUITE TRANSMISSIONS STRAIN VARIABILITY/VIRULENCE: - KENTUCKY OUTBREAK VENTILATION: BACILLUS LONGEVITY & INFECTIVITY IN AIR Primary Infection: BEFORE IMMUNE RESPONSE TB reaches alveoli Replicates extracellularly and intracellularly Lack of immediate host immune response

20 REPLICATION Intracellularly=within alveolar macrophage MTB prevents acidification of phagosome MTB multiplies for weeks in alveolar macrophages AND DISSEMINATION Metastatic foci established in regional nodes Seed blood Travel to tissues favoring multiplication
21 Development of Immune Response: 6-12 weeks Alveolar macrophage infected with TB secretes Interleukins 12 & 18 These attract CD 4 cells CD 4 cells meet TB antigen macrophage presents to them Transformation of CD 4 cells TRANSFORMED CD 4 CELLS: PROLIFERATE: production of clones of similarly reactive CD 4 cells CUTANEOUS HYPERSENSITIVITY: big enough population of transformed CD4 allows delayed rxn to tuberculin RELEASE INTERFERON GAMMA
22 INTERFERON GAMMA CD4 cells release interferon gamma Interferon gamma stimulates additional macrophage phagocytosis of M. tuberculosis Interferon gamma stimulates macrophage to release tumor necrosis factor alpha (TNF Alpha) Tumor Necrosis Alpha (TNF alpha) TNF alpha increases macrophage ability to kill M. tuberculosis TNF alpha required for granuloma formation Granulomas sequester mycobacteria and prevent uncontrolled dissemination



23 PATHOLOGY OF A GRANULOMA Macrophages secrete lytic enzymes which cause tissue necrosis Epithelioid cell=highly stimulated macrophage Langhans Giant Cell= fused macrophages with multiple nuclei GRANULOMA =SUCCESSFUL TISSUE REACTION & HEALING Small antigen load & high hypersensitivity= Epithelioid cells, giant cells etc. Large antigen load & high hypersensitivity= Necrosis & Caseation Small or large antigen load & no hypersensitivity=few cells No granuloma & huge #s of bacilli: AIDS patients

24 Lack of TNF Alpha Murine experiments: Blockade of TNF alpha resulted in reactivation, high bacillary burden, persistent tuberculosis and death TNF alpha knock-out mice infected with M. tuberculosis followed similar course Primary Infection with Resolution: 85% of Cases Patient asymptomatic/ viral syndrome Enlargement of hilar/ peribronchial nodes Ghon complex: hilar node calcification Positive PPD 6-12 weeks

25 Primary Infection with Progression Progressive Primary Disease Young children <5- cannot resolve initial infection :Progression to active disease, miliary or disseminated, CNS involvement Almost always developing world where TB is endemic
26 TUBERCULOUS PLEURISY HYPERSENSITICITY REACTION EXUDATIVE PLEURAL EFFUSION CULTURE NEGATIVE- FEW BACILLI WW II STUDIES: 65% RELAPSE TO ACTIVE TB IF UNTREATED PRIMARY INFECTION- ADOLESCENCE/YOUNG ADULTS Develop cavitary disease: 23% age % age % 25-29

27 PRIMARY INFECTION: AIDS NOSOCOMIAL OUTBREAKS Multiple nosocomial outbreaks of TB in AIDS wards, homeless shelters and prisons in late 1980s-1990s Undiagnosed patient with active TB in AIDS ward where all patients CD4<50 No CD4s to mobilize so no interferon gamma & no macrophages stimulated to phagocytose or secrete interferon gamma OVERWHELMING TB No immunologic control of bacillus Rapid dissemination MDR strains killed scores in AIDS wards
28 Reactivation: 10-15% of those infected Persistence of viable organisms Containment of infection, lack of active disease Viable organisms remain alive, dormant for years Disease occurs when cellular immune system can no longer contain MTB CAUSES OF REACTIVATION Iatrogenic immunosuppression Transplant; Rheumatologic Rx Immunocompromising diseases Malnutrition Old Age Unknown:?hormonal?stress

29 85% Reactivation=Lungs Caseating necrosis, liquefaction, drainage into the bronchial tree Cavity formation Cavity favors bacillary multiplication to huge #s: organisms / GM tissue 5-6 logs greater than # organisms in non-cavitary disease= MOST CONTAGIOUS Implications for development of drug resistance

30 EXTRAPULMONARY TB Viable organisms remain alive for years Most common organs to which disseminated during primary infection LYMPH NODES: SCROFULA Most frequent form of extrapulmonary TB


31 Usually Cervical Or Supraclavicular

32 Can also be axillary BONES ONE THIRD INVOLVE SPINE From: Hematogenous spread from initial infection Lymphatic spread from pleural disease Contiguous disease Spine



33 POTTS DISEASE Earliest focus: Anterior superior or inferior angle of vertebral body Spreads to interverteberal disk & adjacent vertebra RENAL TUBERCULOSIS HEMATOGENOUS SPREAD AFTER PRIMARY INFECTION SEEDS GLOMERULI & FORMS GRANULOMAS LATER, CASEOUS NECROSIS, FIBROSIS & CALCIFICATION ASYMPTOMATIC UNTIL CALYX/PELVIS ULCERATED STERILE PYURIA: MUST SEND FOR MTB CULTURE USUALLY EVIDENCE OF PULMONARY TB PRESENT 25% MILIARY HAVE POSITIVE URINE CULTURE FOR MTB

34 Diagnosis: Symptoms Systemic symptoms non-specific: fever, fatigue, night sweats, weight loss Pulmonary symptoms: cough, productive or dry Hemoptysis: can be emergency Suggests bronchial wall erosion DIAGNOSTIC PROCEDURES SPUTUM SMEAR: Acid fast=all mycobacterial species Ziehl-Neelsen stain Auramine SMEAR POSITIVE MEANS AT LEAST 10,000 ORGS/ML
 =egg based or Middlebrook 7H11=agar based LIQUID MEDIA=Rapid growth = 1-3 weeks; Middlebrook 7H12")

35 CULTURE=GOLD STANDARD Available in most of world in WHO reference labs SOLID MEDIA=Slow growth =3-8 weeks; Lowenstein Jensen (LJ slant) =egg based or Middlebrook 7H11=agar based LIQUID MEDIA=Rapid growth = 1-3 weeks; Middlebrook 7H12 CULTURE CONT D LIQUID: RAPID GROWTH: 1-3 weeks in Middlebrook 7H12 broth media IDENTIFICATION FROM CULTURE DNA PROBES MTB complex, M.avium complex, M. kansasii, M. gordonae BIOCHEMICAL TESTS Niacin, Nitrate, Catalase, etc. to identify other mycobacteria
36 WHAT IS MTB COMPLEX? M. tuberculosis Complex (MTBC) can include: M. tuberculosis M. bovis, M. bovis BCG M. africanum M. microti M. canetti BIOCHEMICAL TESTS NECESSARY TO DISTINGUISH THESE M. bovis ALMOST ALWAYS RESISTANT TO PYRAZINAMIDE Nucleic Acid Amplification: Can detect MTB in fresh sputum Sensitivity intermediate between acid fast smear and culture AFB smear negative, nucleic acid amplification=40-77% sensitive AFB smear positive, nucleic acid amplification=95% sensitive & 100% specific LUXURY OF DEVELOPED WORLD

37 RFLP=Restriction fragment Length Polymorphism Restriction endonuclease makes DNA fragments Separate fragments by electrophoresis IS 6110 as DNA probe= Insertion sequence occurring repeatedly at highly variable locations on MTB chromosome DNA FINGERPRINTING MOLECULAR EPIDEMIOLOGIC TOOL TO IDENTIFY DIFFERENT TB STRAINS FIRST USED BY DUTCH IN EARLY 1990S TO QUANTIFY SOURCE OF LOCAL TB STRAINS USED TO IDENTIFY NOSOCOMIAL OUTBREAKS IN AIDS WARDS, SHELTERS LUXURY OF DEVELOPED WORLD

38 Chest X-Ray Upper lobe infiltrate with or without cavity Hilar adenopathy with or without infiltrates Pleural effusion, exudative Lower lobe infiltrate Miliary pattern UPPER LOBE INFILTRATE Apical or sub-apical Most common in reactivation disease if immune system intact Radiologic extent of disease reflects tissue damage Tissue damage reflects host s ability to have hypsersensitivity reaction

39 HILAR ADENOPATHY Most common chest X-ray in patients with AIDS (CD4 <200) Reflects minimal cellular immune response PLEURAL EFFUSION Seen in post-primary as above: scant orgs Smear negative but culture positive 25% Seen as complication of reactivation TB: more likely to have orgs Smear positive 50% & culture positive 60-70%


40 MILIARY PATTERN From description of pathologic lesions as millet seeds Chest x-ray shows mm nodules MILIARY PATTERN Following childhood infection and progression Immunocompromisi ng diseases: -alcoholism -cirrhosis -rheumatologic diseases -Rx with immunosuppressive



41 DIAGNOSIS DIFFICULT May have multiple organ involvement Millet seed granulomas in tissue Transbronchial biopsy=highest yield for diagnosis
42 TREATMENT: GENERAL PRINCIPLES ALWAYS USE AT LEAST 2 DRUGS: Begin with 4 pending sensitivities Natural incidence of spontaneous resistance to any 1 drug= 1 in 10,000 organisms Bacilli resistant to 1 will be killed by others Natural resistance to 2 drugs spontaneously= 1 in Prolonged Length of Rx: 6-9 months Directly Observed Therapy Prophylaxis: LTBI Targeted Testing: PPD is NOT a general screen Immunocompromised patients: - HIV infected, chemotherapy, organ transplant, immunosuppressive RX for autoimmune diseases - Close contacts of infectious cases - Previously untreated patients with Chest x-ray evidence of old disease (NOT just granuloma) - Recent Immigrants (in US <5 years) - People who work in high exposure institutions
 T-cell based assay from blood: Need")
=gene product specifically produced by M.")
43 POSITIVE PPD: DEFINITION 5 mm: HIV infected, close contacts of infectious cases, Chest XRay evidence of old disease 10 mm: everyone else ELISPOT (Enzyme-linked immunospot) T-cell based assay from blood: Need 1 tube of blood M. tuberculosis genes NOT present in M. bovis BCG Early secretory antigen target-6 (ESAT- 6)=gene product specifically produced by M.tuberculosis and not by M. bovis BCG or any other mycobacteria
44 Will this replace PPD? T cells specifically target this antigen (ESAT-6) and can be detected by ELISPOT obtaining 1 tube of blood TB outbreak in high school in UK showed ELISPOT higher sensitivity and specificity than PPD skin test Licensed & available as Quantiferon Gold but discordance with PPD in numerous studies; significance not yet clear
45 BCG: Most Widely Used and Most Controversial Vaccine in World M. Bovis strain attenuated through serial passage no standardized strain or procedure to make one largest study: India = no protection from TB infection other studies: England = protection from TB infection prevalence of non-tb mycobacteria may interfere All agree: highly effective for infants & small children against dissemination & meningitis BCG Used in Countries Where TB Endemic BCG may be indicated for infants and small children continuously exposed to MDR patient BCG at birth should not give positive PPD as adult Boosting: 2 step testing for all those with BCG
46 BCG: Most Widely Used and Most Controversial Vaccine in World M. Bovis strain attenuated through serial passage no standardized strain or procedure to make one largest study: India = no protection from TB infection other studies: England = protection from TB infection prevalence of non-tb mycobacteria may interfere All agree: highly effective for infants & small children against dissemination & meningitis BCG Used in Countries Where TB Endemic BCG may be indicated for infants and small children continuously exposed to MDR patient BCG at birth should not give positive PPD as adult Boosting: 2 step testing for all those with BCG
HISTORY TB = 25% ADULT DEATHS EGYPTIAN MUMMIES: SPINAL TB. 17 th -18th CENTURIES- URBANIZATION MID 24
 HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS
HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS
HISTORY TB = 25% ADULT DEATHS MID 24 PRE-ANTIBIOTIC ERA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
HISTORY TB = 25% ADULT DEATHS MID 24 PRE-ANTIBIOTIC ERA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
HISTORY TB = 25% ADULT DEATHS PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
INDUSTRIALIZATION TB = 25% ADULT DEATHS
 HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS 1 GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM
HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS 1 GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM
HISTORY TB = 25% ADULT DEATHS PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Controlling TB in the era of HIV
 Controlling TB in the era of HIV Christy Hanson, PhD, MPH TB Research Advisor Amy Bloom, MD TB/HIV Advisor TB Incidence rates highest in Africa Estimated new TB cases (all forms) per 100 000 population
Controlling TB in the era of HIV Christy Hanson, PhD, MPH TB Research Advisor Amy Bloom, MD TB/HIV Advisor TB Incidence rates highest in Africa Estimated new TB cases (all forms) per 100 000 population
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
MYCOBACTERIUM. Mycobacterium Tuberculosis (Mtb) nontuberculous mycobacteria (NTM) Mycobacterium lepray
 nontuberculous mycobacteria (NTM) Mycobacterium lepray") MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
TB, BCG and other things. Chris Conlon Infectious Diseases Oxford
 TB, BCG and other things Chris Conlon Infectious Diseases Oxford Epidemiology Latent TB IGRA BCG >50/100000
TB, BCG and other things Chris Conlon Infectious Diseases Oxford Epidemiology Latent TB IGRA BCG >50/100000
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
The epidemiology of tuberculosis
 The epidemiology of tuberculosis Tuberculosis Workshop Shanghai, 12-22 May 28 Philippe Glaziou World Health Organization Outline Epidemiology refresher Estimates of tuberculosis disease burden Notifications
The epidemiology of tuberculosis Tuberculosis Workshop Shanghai, 12-22 May 28 Philippe Glaziou World Health Organization Outline Epidemiology refresher Estimates of tuberculosis disease burden Notifications
ANNUAL TUBERCULOSIS REPORT OREGON Oregon Health Authority Public Health Division TB Program November 2012
 ANNUAL TUBERCULOSIS REPORT OREGON 211 Oregon Health Authority Public Health Division TB Program November 212 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-211... page
ANNUAL TUBERCULOSIS REPORT OREGON 211 Oregon Health Authority Public Health Division TB Program November 212 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-211... page
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Respiratory System الفريق الطبي االكاديمي
 Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
TUBERCULOSIS. Famous victims in their intellectual prime: Chopin, Paganini, Thoreau, Keats, Elizabeth Browning, Brontës
 TUBERCULOSIS GENERAL Tuberculosis (TB) kills 1,700,000 annually worldwide. "The Captain of all the men of death that came to take him away was the consumption, for it was that which brought him down to
TUBERCULOSIS GENERAL Tuberculosis (TB) kills 1,700,000 annually worldwide. "The Captain of all the men of death that came to take him away was the consumption, for it was that which brought him down to
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Tuberculosis. Impact of TB. Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH)
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit
 MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit Topics to be covered What is Tuberculosis? TB bacteria and what is unique about it. How is TB different from HIV? How is TB
MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit Topics to be covered What is Tuberculosis? TB bacteria and what is unique about it. How is TB different from HIV? How is TB
4/25/2012. The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB
 Sindy M. Paul, MD, MPH, FACPM May 1, 2012 The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB morbidity, including resistance Identifying people
Sindy M. Paul, MD, MPH, FACPM May 1, 2012 The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB morbidity, including resistance Identifying people
Mycobacterium tuberculosis. Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology
 Dr.Baha, AL-Amiedi Ph. D.Microbiology") Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Annual Tuberculosis Report Oregon 2007
 Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
Tuberculosis Overview
 1/18/2011 Handling TB and HIV Co-Infection Fargo, North Dakota September 15-16, 2010 Tuberculosis Overview Dean Tsukayama, MD September 15, 2010 1 Questions to answer in evaluation of tuberculosis 1. TB
1/18/2011 Handling TB and HIV Co-Infection Fargo, North Dakota September 15-16, 2010 Tuberculosis Overview Dean Tsukayama, MD September 15, 2010 1 Questions to answer in evaluation of tuberculosis 1. TB
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TB trends and TB genotyping
 Management of a TB Contact Investigation for Public Health Workers Albuquerque, NM October 1, 214 TB trends and TB genotyping Marcos Burgos MD October 1, 214 Marcos Burgos, MD has the following disclosures
Management of a TB Contact Investigation for Public Health Workers Albuquerque, NM October 1, 214 TB trends and TB genotyping Marcos Burgos MD October 1, 214 Marcos Burgos, MD has the following disclosures
TB in Foreign Born and High Risk Populations
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB Intensive Chicago, Illinois September 25-27, 2007
 TB Intensive Chicago, Illinois September 25-27, 2007 The Epidemiology of Tuberculosis William Clapp, MD September 25, 2007 1 The Epidemiology of Tuberculosis William Clapp MD Heartland National TB Center
TB Intensive Chicago, Illinois September 25-27, 2007 The Epidemiology of Tuberculosis William Clapp, MD September 25, 2007 1 The Epidemiology of Tuberculosis William Clapp MD Heartland National TB Center
The Epidemiology of Tuberculosis in Minnesota,
 The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
The American Experience with TB Elimination
 Reaching the Goal of TB Elimination by 2035 March 3, 2015 The American Experience with TB Elimination John Jereb, M.D. Medical officer Division of Tuberculosis Elimination National Center for HIV/AIDS,
Reaching the Goal of TB Elimination by 2035 March 3, 2015 The American Experience with TB Elimination John Jereb, M.D. Medical officer Division of Tuberculosis Elimination National Center for HIV/AIDS,
Medical Bacteriology- Lecture 10. Mycobacterium. Actinomycetes. Nocardia
 Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
2016 Annual Tuberculosis Report For Fresno County
 206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
Descriptive Epidemiology Project: Tuberculosis in the. United States. MPH 510: Applied Epidemiology. Summer A 2014
 Descriptive Epidemiology Project: Tuberculosis in the United States MPH 510: Applied Epidemiology Summer A 2014 June 1, 2014 1 The white plague affected thousands upon thousands of people in the 18 th
Descriptive Epidemiology Project: Tuberculosis in the United States MPH 510: Applied Epidemiology Summer A 2014 June 1, 2014 1 The white plague affected thousands upon thousands of people in the 18 th
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Tuberculosis What you need to know. James Zoretic M.D., M.P.H. Regions 2 and 3 Director
 Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Medical Bacteriology- lecture 13. Mycobacterium Actinomycetes
 Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Diagnosis & Management of Latent TB Infection
 Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Diagnosis & Management of Latent TB Infection Prof. Ashok Rattan, MD, MAMS, INSA DFG, WHO Lab Director Academics, Industry: Research, Diagnosis, Public Health, Academics Adviser: Laboratory Operations,
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
number Done by Corrected by Doctor Hamid Al Zoubi
 number 15 Done by أبو عجمي ة مها Corrected by Waseem Abu Obeida Doctor Hamid Al Zoubi In case you don t know - (Bacillus = rod) and (bacilli = rods) - hypersensitivity tests can be either immediate (within
number 15 Done by أبو عجمي ة مها Corrected by Waseem Abu Obeida Doctor Hamid Al Zoubi In case you don t know - (Bacillus = rod) and (bacilli = rods) - hypersensitivity tests can be either immediate (within
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Epidemiology of Substance Abuse and Tuberculosis: Where is the Problem? Mary Long, MPSH; Heartland Phillip Lindsey, MD; OK State
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Epidemiology of Substance Abuse and Tuberculosis: Where is the Problem? Mary Long, MPSH; Heartland Phillip Lindsey, MD; OK State
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
Global, National, Regional
 Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Appendix C. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix C Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix C Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Learning Objectives: Case 1 11/12/2015. Tuberculosis: Focus on Transmission and Pathogenesis. TB: Some Important Terms
 A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
WANTED Manuscript supporting the prevailing paradigm of tuberculosis by any author DEAD or ALIVE $1,000 REWARD. 3 TB India HSCP
 A New Paradigm for the Pathogenesis of Pulmonary Tuberculosis Bronchogenic tuberculosis The missing link between primary and post-primary disease Robert Hunter MD, PhD Dept. of Pathology and Laboratory
A New Paradigm for the Pathogenesis of Pulmonary Tuberculosis Bronchogenic tuberculosis The missing link between primary and post-primary disease Robert Hunter MD, PhD Dept. of Pathology and Laboratory
Global, National, Regional
 Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
511,000 (57% new cases) ~50,000 ~30,000
 ~50,000 ~30,000") Latest global TB estimates - 2007 (Updated Mar 2009) All forms of TB Greatest number of cases in Asia; greatest rates per capita in Africa Multidrug-resistant TB (MDR-TB) Estimated number of cases 9.27
Latest global TB estimates - 2007 (Updated Mar 2009) All forms of TB Greatest number of cases in Asia; greatest rates per capita in Africa Multidrug-resistant TB (MDR-TB) Estimated number of cases 9.27
Role of the Laboratory in TB Diagnosis and Management
 Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service
 Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service North Central London TB Service TBService@nhs.net After Action Review Could we have
Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service North Central London TB Service TBService@nhs.net After Action Review Could we have
SWABCHA Fact Sheet: Tuberculosis (TB)
") SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
Research Methods for TB Diagnostics. Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012
 Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
TB EPIDEMIOLOGY. Outline. Estimated Global TB Burden, TB epidemiology
 TB EPIDEMIOLOGY TB Clinical Intensive Course Curry International Tuberculosis Center September 30, 2015 Varsha Nimbal, MPH Tuberculosis Control Branch California Department of Public Health 1 Outline TB
TB EPIDEMIOLOGY TB Clinical Intensive Course Curry International Tuberculosis Center September 30, 2015 Varsha Nimbal, MPH Tuberculosis Control Branch California Department of Public Health 1 Outline TB
TB IN EMERGENCIES. Disease Control in Humanitarian Emergencies (DCE)
") TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
TB IN EMERGENCIES Department of Epidemic and Pandemic Alert and Response (EPR) Health Security and Environment Cluster (HSE) (Acknowledgements WHO Stop TB Programme WHO/STB) 1 Why TB? >33% of the global
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian