Stabilization of the Newborn for Transport. Relevant Disclosure. Learning Objectives
|
|
|
- Clyde Parks
- 6 years ago
- Views:
Transcription
1 Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section, Department of Pediatrics OU Health Sciences Center Relevant Disclosure Under Accreditation Council for Continuing Medical Education guidelines, disclosure must be made regarding relevant financial relationships with commercial interests within the last 12 months. I have no relevant financial relationships or affiliations with commercial interests to disclose Learning Objectives Upon completion of this session, participants will improve their competence and performance by being able to: Review the history of neonatal transport Explain why neonatal transports are necessary Identify common conditions and Discuss treatments prior to transport Review how to contact NeoFlight and arrange for a neonatal transport Describe what to expect when the NeoFlight team arrives 1
2 History 1834 first description of neonatal intubation 1853 to 1855 establishment of Children hospitals 1857 Jean Louis Paul Denuce ( ) had concept of a incubator 1878 French obstetrician Stephane Tarnier developed the Tarnier Martin Couveuse incubator History 1899 First portable transportation incubator by Joseph Bolivar DeLee ( ) 1948 First organized transportation program 1950 s & 60 s Silverman and associates proved the need for heat and humidity for premature survival in randomized controlled trials 1960 s & 70 s Hospital based neonatal transport programs were created Why transport??? Main reason to deliver a sick or at risk (preterm) neonate needing special care to a tertiary care center that offers subspecialties and optimal resources to provide intensive care that can not be provided at the referring hospital Studies have shown this improves overall outcome 2
3 Who should be transported??? Extreme premature newborns Newborns with malformations Newborns with surgical conditions Newborns with conditions that can not be managed locally due to constraints of resources and staff at that local facility Goal of preparation for transport STABILIZATION!!!! Stability of a baby s condition is far more important than speed of transport Care given in the first few hours after birth is just as important if not more important to a newborn s outcome as the care given days or weeks at a regional intensive care nursery Basic Preparation for Transport Check Vital signs Temp, Resp rate, Heart rate, and BP Lab tests Blood glucose, Hematocrit, Blood gas, other tests Establish an IV line Obtain x rays if warranted Prepare copies of charts and x rays 3
4 THINGS TO CONSIDER S. Sugar and Safe Care T. Temperature A. Airway B. Blood pressure L. Lab work E. Emotional support IV Fluids/Access Peripheral IV (PIV) or Umbilical lines (UAC arterial or UVC venous) will need to be placed Use D10W as your main fluid to maintain appropriate serum glucose levels and to avoid excessive electrolytes early on (usually since urine output may not have been established well yet) Normal Saline (NS) can be used for fluid resuscitation in cases of hypovolemia or initial blood loss If using an Umbilical line or Central line then make sure there is 0.5 to 1 unit of heparin per 1 ml of IV Fluid (IVF) to prevent the line from clotting Hypoglycemia Newborns at risk include: Preterm infants (<37 wks) Small for gestational age (SGA) infants Infants of diabetic mothers (IDM) Large for gestational age (LGA) infants Stressed, sick infants Infants exposed to certain maternal medications in utero 4
5 Hypoglycemia Signs/Symptoms of Hypoglycemia Weak, High pitched cry Poor feeding Hypothermia Tremors/Jitteriness Hypotonia/Lethargy Seizures Tachypnea Hypoglycemia Blood glucose level below 40 mg/dl If below this and baby is asymptomatic and not sick then allow to feed and check a postprandial glucose level 30 min after the feed If hypoglycemia persists then obtain IV access and give a 2 ml/kg IV bolus of D10W Glucose levels should be checked every 30 min until stable and then every 4 hrs Hypoglycemia In a sick baby then do NOT feed and instead just obtain IV access and give a 2 ml/kg bolus of D10W and start IVF of D10W (without electrolytes) at 80 ml/kg/day Maintain blood glucose levels between mg/dl Continue to monitor blood glucose levels every 30 min until stable and then every 4 hrs 5
6 Temperature Normal core temperature between 36.5 and 37.5 C ( F) Hypothermia Mild: C ( F) Moderate: C ( F) Severe: <32 C (<89.6 F) Deviations from normal core temperature range increases metabolic rate and oxygen consumption Temperature Newborns most vulnerable for hypothermia: Preterm (especially < 32 wks) Small for Gestational Age (SGA) Require prolong resuscitation Acutely ill newborns Newborns with open skin defects Temperature Mechanisms of Heat Loss Conduction protect the baby from contact with cold objects Convection protect from air currents and keep air warm (26 to 28 C or 78.8 to 82.4 F) Evaporation quickly dry the baby and remove wet linens (plastic bags help) Radiation Keep baby away from cold window or walls and place in an incubator 6
7 Airway Establishing a patent airway in a newborn is essential in newborn stabilization It is important that a newborn s lungs establishes the functional residual capacity (FRC) in a timely manner for gas exchange to occur Airway Insufficient breathing fails to force fluid from the lungs Lack of ventilation of the lungs results in sustained constriction of pulmonary arterioles, preventing blood oxygenation Hypoxia and ischemia can cause bradycardia resulting in systemic hypotension Airway Issues that hinder breathing Respiratory distress due to surfactant deficiency Secretions or meconium in the way Respiratory depression due to hypoxia ischemia Respiratory depression due to maternal drugs Excessive or deep suctioning by care providers 7

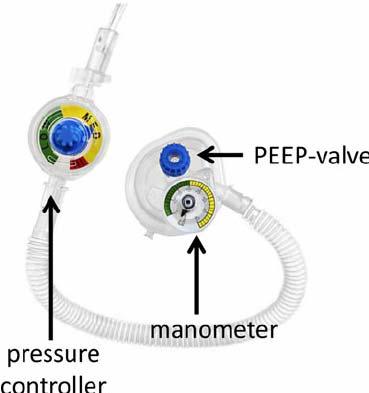
8 Airway Indications for positive pressure ventilation (PPV) Apnea/ gasping Heart rate less than 100 bpm, even if breathing Persistent central cyanosis despite 100% free flow oxygen Abnormal blood gas showing poor ventilation or oxygenation Airway Ways to provide PPV: Self inflating bag or Flow inflating bag T piece respirator Ventilator 8


9 9



10 10
 to monitor ventilation Vitals assessed routinely Respiratory Issues Congenital Diaphragmatic Hernia (CDH): Decreased breath sounds on affected side Bowel sounds on the affected side")
11 Airway Once an airway is secure then constant monitoring of the patient is needed Pulse oximeter Chest X ray (CXR) should be obtained Blood gas (preferably arterial at first in order to properly assess PaO2) to monitor ventilation Vitals assessed routinely Respiratory Issues Congenital Diaphragmatic Hernia (CDH): Decreased breath sounds on affected side Bowel sounds on the affected side Scaphoid abdomen If known or suspected do not give mask PPV or continuous positive airway pressure (CPAP), instead intubate immediately and administer PPV or CPAP Place orogastric (OG) or nasogastric (NG) tube and remove air from stomach to facilitate lung expansion Obtain CXR and blood gas 11
12 Respiratory Issues Pneumothorax: Presents with respiratory and cardiovascular deterioration Definitive diagnosis is with CXR but transillumination can help Treatment: Needle aspiration or chest tube placement Studies have not shown that Nitrogen washout promotes faster resolution compared to RA Respiratory Issues Meconium aspiration: New recommendations by Newborn Resuscitation Program (NRP) that even depressed infants do not have to be intubated and suctioned immediately Instead treat as a normally depressed infant and if intubation is warranted and there is obvious meconium in the airway or endotracheal tube (ETT) that is hindering effective ventilation then suction Respiratory Issues Tracheoesophageal Fistula/ Atresia: History of polyhydramnios Present with respiratory distress with excessive salivation and choking, coughing, and cyanosis with feeding Make NPO (nothing by mouth) and provide IVF hydration and nutrition Place replogle suction on low intermittent wall suction to esophageal pouch Obtain CXR after placement 12
13 Respiratory Issues Airway obstruction Nose provide oral airway Mouth place prone and/or nasopharyngeal (NP) tube Larynx or Trachea intubate if possible or try an laryngeal mask airway (LMA) Blood Pressure/Cardiac SHOCK Presents with tachypnea, pale skin, cyanosis, bradycardia, tachycardia, hypotension, weak pulses, poor perfusion (prolonged cap refill), poor urine output Once you have hypotension then you have begun uncompensated shock Blood Pressure/Cardiac Types of Shock: Hypovolemic volume loss Cardiogenic poor contractility Septic hypotension from vasodilation and loss of fluid (capillary leak) 13
14 Blood Pressure/Cardiac Lab tests helpful in Shock Blood gas to look for metabolic acidosis Blood lactate Complete blood count (CBC) and c reactive protein (CRP) Blood culture Coagulation studies Liver function tests Blood glucose level Electrolytes, blood urea nitrogen (BUN), Creatinine, Calcium Possibly cardiac enzymes Blood Pressure/Cardiac Treatment of shock: Identify the cause(s) Treat or correct the cause(s) Hypovolemia give NS 10 ml/kg IV over 15 to 30 minutes, may need blood transfusion too if suspected blood loss Cardiac correct hypoxia, hypoglycemia, hypotension, acidosis, arrhythmia, calcium, etc. Septic inotropes (dopamine) and fluid is usually needed Blood Pressure/Cardiac Congenital Heart Defects (CHD) If you suspect a CHD from physical exam or due to the newborn failing the CCHD screen then call the NeoFlight Access Center at OU Children s Hospital While on the phone a Pediatric Cardiologist may also be involved on the conversation and management options will be discussed ECHOs for CHD should always be read and interpreted by a PEDIATRIC Cardiologist per AAP guidelines 14
15 Hypoxic Ischemic Encephalopathy (HIE) Potential Acute Perinatal Events may include: Variable/late fetal HR decelerations Prolapsed/ruptured or tight nuchal cord Uterine rupture Maternal hemorrhage/placental abruption Maternal trauma or CPR Any event that contributes to asphyxia prior to, at, or following birth Hypoxic Ischemic Encephalopathy (HIE) Criteria: 35 weeks gestation and are 1800 grams Contraindications Known cardiac disease Imperforate anus Evidence of head trauma or skull fracture causing major intracranial hemorrhage Birth weight of less than 1,800 gm Major congenital malformations Must meet 1 criteria in Category 1 and 3 in Category 2 Hypoxic Ischemic Encephalopathy (HIE) Criteria: Have at least one criteria below Category 1 Cord gas or ABG 1 hour of life with a: ph 7.0 or Base Deficit 16 APGAR 5 at 10 minutes Continued need for PPV or intubated at 10 minutes of life, required chest compressions, or epinephrine 15
16 Hypoxic Ischemic Encephalopathy (HIE) Criteria: Have at least 3 criteria below or have Seizures Category 2 Decreased Level of consciousness Decreased Activity Abnormal Posture Decreased Tone Weak/Absent Reflexes Abnormal Autonomic System findings (Pupils, heart rate, apnea) Hypoxic Ischemic Encephalopathy (HIE) Time is of the essence since cooling needs to begin within 6 hours of birth Passive cooling can and should begin at referring facility (prior to NeoFlight team s arrival) NEVER cool with ice packs PASSIVE Cooling Turn off radiant warmer (DO NOT Cool with cooling or ice packs) Monitor RECTAL temp every 15 minutes Goal Rectal Temperature: 34.4 C 35 C (93.92 F 95 F) If less <34 C (93.2 F), then turn on radiant warmer on Servo mode and set at 0.5 C higher than baby s current temp NEVER Rapidly COOL or REWARM a baby 16
17 PASSIVE Cooling Patient should be NPO and on D10W IVF at 60 ml/kg/day of total fluids Blood glucose needs to be monitored closely If SEIZURES are present then give loading dose of phenobarbital (20 mg/kg IV x1) Monitor vitals every 15 minutes with rectal temps Check blood gases per need of respiratory support, avoiding hyperventilation and hyperoxia Emotional Support Encourage emotional attachment between the parents and the newborn prior to transport Make sure the parent s have a clear understanding of their baby s condition and need for transport Offer up any other resources for support that the parents will need Consent for transport will need to be obtained Arranging Neonate Transport NeoFlight is a neonatal dedicated transport team based at OU Children s hospital at OU Medical Center Call or Prompted to press 1 for a neonate transfer Access center will connect you with NeoFlight team member and a Neonatologist 17
18 NeoFlight Transport After the referral call is made you will have an estimated time of arrival (ETA) NeoFlight team upon arriving at the facility will obtain more information on the patient s condition, review the chart, assess the patient, obtain any needed tests, and provide any treatment needed NeoFlight Transport NeoFlight is under medical control from a neonatologist at OU Medical Center, however the referring physician is in charge prior to the team leaving the facility The team will make sure prior to departure that the patient is stabilized to the fullest capacity for transport The team will need copies of the chart, results, and radiological studies to bring to the receiving facility Resources Karlsen, K. (2013). The S.T.A.B.L.E. Program pre transport post resuscitation stabilization care of sick infants: Guidelines for neonatal healthcare providers: Learner provider manual (6th ed.). Park City, UT: S.T.A.B.L.E. Program. 18
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
 NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
NRP Raising the Bar for Providers and Instructors
 NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context
 Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني
 Lecture 6 PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني Neonatal Resuscitation Program (NRP) 2010 MCQ? In neonatal resuscitation program, the preterm neonates need special preparations
Lecture 6 PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني Neonatal Resuscitation Program (NRP) 2010 MCQ? In neonatal resuscitation program, the preterm neonates need special preparations
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Neonatal/Pediatric Cardiopulmonary Care
 Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised by P.
 TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised 05-13-13 by P. Joe SCREENING FOR POTENTIAL COOLING PATIENTS Patients who are >
TREATMENT OF HYPOXIC ISCHEMIC ENCEPHALOPATHY WITH COOLING Children s Hospital & Research Center Oakland Guideline Revised 05-13-13 by P. Joe SCREENING FOR POTENTIAL COOLING PATIENTS Patients who are >
Resuscitation efforts for Mom & Baby
 Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
5 Million neonatal deaths each year worldwide. 20% caused by neonatal asphyxia. Improvement of the outcome of 1 million newborns every year
 1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
1st Annual Clinical Simulation Conference
 1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Table 1: The major changes in AHA / AAP neonatal resuscitation guidelines2010 compared to previous recommendations in 2005
 Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Preface. The ACoRN Neonatal Society. ACoRN xiii
 Preface For most health professionals, few events are more challenging or stressful than caring for a sick or preterm baby. It is therefore not surprising that the management and stabilization of these
Preface For most health professionals, few events are more challenging or stressful than caring for a sick or preterm baby. It is therefore not surprising that the management and stabilization of these
OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General
![OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General](/thumbs/85/91909911.jpg "OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General") OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Surfactant Administration
 Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Neonatal Resuscitation
 Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
2. General Cardiac Arrest Protocol Medical Newborn/Neonatal. Protocol 8-3 Resuscitation 4. Medical Supraventricular
 PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
Admission/Discharge Form for Infants Born in Please DO NOT mail or fax this form to the CPQCC Data Center. This form is for internal use ONLY.
 Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Practical Application of CPAP
 CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
Birth Asphyxia. Perinatal Depression. Birth Asphyxia. Risk Factors maternal. Risk Factors fetal. Risk Factors Intrapartum 2/12/2011
 Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
NEONATOLOGY Healthy newborn. Neonatal sequelaes
 NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
Presented By : Kamlah Olaimat
 Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
These signs should lead to the administration of high concentrations of
 Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Pediatric Code Blue. Goals of Resuscitation. Focus Conference November Ensure organ perfusion
 Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
8/20/12. Discuss the importance of thermoregulation in the neonate.
 Sharon Rush MSN NNP-BC Discuss the importance of thermoregulation in the neonate. To maintain correct body temperature range in order to: Reduce oxygen consumption Reduce calorie expenditure Maximize metabolic
Sharon Rush MSN NNP-BC Discuss the importance of thermoregulation in the neonate. To maintain correct body temperature range in order to: Reduce oxygen consumption Reduce calorie expenditure Maximize metabolic
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013
 NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Neonatal Intensive Care Unit Skills Checklist
 _ XXX-XX- Print Name Last 4 of SS # Date Completed Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
_ XXX-XX- Print Name Last 4 of SS # Date Completed Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Neonatal Resuscitation in What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011
 Neonatal Resuscitation in 2011- What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011 Conflicts I have no actual or potential conflict of interest in relation to this
Neonatal Resuscitation in 2011- What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011 Conflicts I have no actual or potential conflict of interest in relation to this
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA
 GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
ACoRN Workbook 2012 Update
 ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
SHOCK IN THE NEONATE. Developed by - Lisa Fikac, MSN, RNC-NIC. Expiration Date - 8/19/17
 SHOCK IN THE NEONATE Developed by - Lisa Fikac, MSN, RNC-NIC Expiration Date - 8/19/17 This continuing education activity is provided by Cape Fear Valley Health System, Training and Development Department,
SHOCK IN THE NEONATE Developed by - Lisa Fikac, MSN, RNC-NIC Expiration Date - 8/19/17 This continuing education activity is provided by Cape Fear Valley Health System, Training and Development Department,
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Pediatric Advanced Life Support Overview Judy Haluka BS, RCIS, EMT-P
 Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
Neonatal Hypoglycemia. Presented By : Kamlah Olaimat 25\7\2010
 Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
Oh SCH It s a neonatal emergency
 trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Simulation 08: Cyanotic Preterm Infant in Respiratory Distress
 Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION
 DEFINITION") CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
PCEP. Perinatal Continuing Education Program. Pretest Answer Key Book IV: Specialized Newborn Care. Unit 1: Direct Blood Pressure Measurement
 1. C. Severe anemia 2. True 3. True 4. False Perinatal Continuing Education Program Pretest Answer Key Book IV: Specialized Newborn Care Unit 1: Direct Blood Pressure Measurement 5. True 6. A. Baby s heart
1. C. Severe anemia 2. True 3. True 4. False Perinatal Continuing Education Program Pretest Answer Key Book IV: Specialized Newborn Care Unit 1: Direct Blood Pressure Measurement 5. True 6. A. Baby s heart
Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical
 Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical City Children s Hospital, Dallas Hypoxia Shortage of
Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical City Children s Hospital, Dallas Hypoxia Shortage of
PRACTICE GUIDELINES WOMEN S HEALTH PROGRAM
 C Title: NEWBORN: HYPOGLYCEMIA IN NEONATES BORN AT 35+0 WEEKS GESTATION AND GREATER: DIAGNOSIS AND MANAGEMENT IN THE FIRST 72 HOURS Authorization Section Head, Neonatology, Program Director, Women s Health
C Title: NEWBORN: HYPOGLYCEMIA IN NEONATES BORN AT 35+0 WEEKS GESTATION AND GREATER: DIAGNOSIS AND MANAGEMENT IN THE FIRST 72 HOURS Authorization Section Head, Neonatology, Program Director, Women s Health
Dr. (Kate) Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS IN THE NEWBORN
 Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS IN THE NEWBORN") Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. (Kate) Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. (Kate) Katherine Miller GUELPH ON 121 RESPIRATORY DISTRESS
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Introduce the basics of the newborn resuscitation period Practice calculations for TPN orders Learn how to manage basic ventilator settings
 Introduce the basics of the newborn resuscitation period Practice calculations for TPN orders Learn how to manage basic ventilator settings Complex concepts you may be expected to know Not taught this
Introduce the basics of the newborn resuscitation period Practice calculations for TPN orders Learn how to manage basic ventilator settings Complex concepts you may be expected to know Not taught this
Transfer guidelines for surgical infants
 Transfer guidelines for surgical infants Document Title and Reference : Transfer guidelines for surgical infants Main Author (s) Transport Team Clinical Guidelines group Ratified by: GMNICP Date Ratified:
Transfer guidelines for surgical infants Document Title and Reference : Transfer guidelines for surgical infants Main Author (s) Transport Team Clinical Guidelines group Ratified by: GMNICP Date Ratified:
Neonatal/Pediatric Cardiopulmonary Care. Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN. Other. Other Diseases
 PPHN. Other. Other Diseases") Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Wales Neonatal Network Guideline Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
The Crashing Pediatric Patient: Stopping the Fall
 The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Pediatric Learning Solutions A clinical education program exclusively for pediatric professionals
 Pediatric Learning Solutions A clinical education program exclusively for pediatric professionals The following Pediatric Learning Solutions courses align to focus areas of the Neonatal CCRN Exam Content
Pediatric Learning Solutions A clinical education program exclusively for pediatric professionals The following Pediatric Learning Solutions courses align to focus areas of the Neonatal CCRN Exam Content
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
PEPP Course: PEPP BLS Pretest
 PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
Blue Babies, Twitchy Toddlers, and Kool Kids. By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN
 Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
Inclusion criteria for cooling: Babies should be assessed for 3 criteria: A, B and C. See Appendix 1 for a decision making flowchart.
 Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Guideline for the management of Infants with Moderate or Severe Perinatal Asphyxia requiring cooling. (Including flowchart for infants fulfilling A criteria or A and B criteria only) Perinatal asphyxia
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Pedi-Cap CO 2 detector
 Pedi-Cap CO 2 detector Presentation redeveloped for this program by Rosemarie Boland from an original presentation by Johnston, Adams & Stewart, (2006) Background Clinical methods of endotracheal tube
Pedi-Cap CO 2 detector Presentation redeveloped for this program by Rosemarie Boland from an original presentation by Johnston, Adams & Stewart, (2006) Background Clinical methods of endotracheal tube
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Hypoxic Ischemic Encephalopathy. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
Pediatric Learning Solutions course alignment with the Neonatal/Pediatric Specialty Examination Detailed Content Outline.
 Pediatric Learning Solutions course alignment with the Neonatal/Pediatric Specialty Examination Detailed Content Outline. The following Pediatric Learning Solutions courses align to focus areas of the
Pediatric Learning Solutions course alignment with the Neonatal/Pediatric Specialty Examination Detailed Content Outline. The following Pediatric Learning Solutions courses align to focus areas of the
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen
 Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
ISPUB.COM. The Use of LMA in Newborn Resuscitation. R Vadhera INTRODUCTION VENTILATION
 ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel