Heme (Bleeding and Coagulopathies) in the ICU
|
|
|
- Jayson Singleton
- 6 years ago
- Views:
Transcription
 in the")
1 Heme (Bleeding and Coagulopathies) in the ICU

2 General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related bleeding is high will discuss where evidence is good and bad! NEJM 2014;370:847-59
3 Overview
4 NEJM 2014;370:847-59

5 Common ICU Disorders NEJM 2014;370:847-59
6 First Principal in Management Simple but hard to do: AVOID correction of LAB abnormalities with blood products unless there is a CLINICAL bleeding problem, a surgery is required, or both NEJM 2014;370:847-59
7 Major Bleeding and Transfusions
8 Major Bleeding and Transfusions Transfusions used liberally in critical care until transfusion-related infections known (e.g. HIV, hepatitis) and blood supply more limited Initial transfusion practice based on military and civilian casualties, not RCTs Improved survival with FFP per unit of RBC but these data flawed Now widespread use of FFP but not w/o risk TRALI, ARDS This issue being investigated with current trials ongoing North American Pragmatic, Randomized Optimal Platelets and Plasma Ratios (multicenter RCT - trauma pts requiring massive transfusion, effect of products or transfusion ratios of plasma, plts, or RBCs on rates of death at 24h and 30d) ended 12/2013 NEJM 2014;370:847-59
9 NEJM 2014;370: Major Bleeding and Transfusions Using FFP in North America but in Europe, many abandoned use and use concentrates instead Others using tranexamic acid (derivative of lysine, acts as antifibrinolytic and competitively inhibits plasminogen) New trial at Pitt called STAAMP (Study of Tranexamic Acid during Air Medical Prehospital Transport, 1 gm to pts at risk of hemorrhage, 30d mortality) Tranexamic acid already recommended for major bleeding after trauma RCT called CRASH-2 (Clinical Randomization of an Antifibrinolytic in Significant Hemorrhage Study) Those getting TA had 1/3 reduction in bleeding (within 3 hrs) and did not have higher rates thrombosis although needs more study
10 NEJM 2014;370: Hemostatic Support for Procedures No evidence for using FFP to correct abnormal results on coag screening prior to procedure No consensus for what results should trigger use of FFP so people have different practices Author suggest PT ratio<1.5 is safe for CVC insertion as thrombin generation is normal at that level In general, vitamin K needed for formation of factors 2,7,9, and 10, may be low in critical care settings Author suggests supplementation with vitamin K
11 NEJM 1999;340: Transfusion Strategy & Critical Care TRICC Trial 1999 RCT, 838 critically ill pts enrolled with euvolemia after initial tx by MDs 418 patients to restrictive strategy (Hgb>7) and maintained betw patients to liberal strategy (Hgb>10) and maintained betw Examined 30d mortality 30d mortality similar between groups but much less among pts who were less acutely ill
12 NEJM 1999;340: Transfusion Strategy & Critical Care No difference in 30d mortality from all causes (p=0.11) Mortality rates during hospitalization were lower in restrictive strategy group (p=0.05) Mortality in ICU and 60d mortality lower in restrictive strategy group (p=0.29, p=0.23) but not significantly so Those with cardiac disease did not have more adverse outcomes in restrictive strategy group
13 NEJM 1999;340: Restrictive strategy was at least as effective and possibly superior to liberal strategy in critically ill One landmark RCT examining transfusion requirements in critical care in critically ill patients, Hgb<9 within 72h of admission 418 pts to restrictive strategy (Hgb<7) 420 pts to liberal strategy (Hgb<10) Primary outcome rate of death at 30d Secondary outcomes rate of death at 60d, survival time in first 30d Overall, 30d mortality similar betw groups
14 Acute UGIB & Transfusions Prior RCTs of transfusion strategies excluded GI bleeders Observational and animal studies suggested transfusion may be harmful, especially in those with portal HTN This trial was an RCT to determine whether restrictive strategy was better than liberal transfusion strategy in pts with UGIB based on current guidelines at time of study in patients (461 to restrictive, 460 to liberal) enrolled Randomized according to presence/absence of liver cirrhosis NEJM 2013;368:11-21
15 Acute UGIB & Transfusions Restrictive strategy Hgb threshold 7 Liberal strategy Hgb threshold 9 Started with 1U transfusion Primary outcome: rate of death within 45 d Secondary outcomes: rate of further bleeding and in-hospital complications Followed other standards of care for UGIB Rate of death from any cause lower in restrictive group (p=0.02) Adverse events lower in restrictive group (p=0.02) NEJM 2013;368:11-21
16 Restrictive strategy resulted in shorter hospital stay, less need for rescue therapy, and further bleeding Transfusion may counteract splanchnic vasoconstriction caused by hypovolemia and induce increase splanchnic blood flow/pressure impair clot formation May induce abns in coag properties In those with cirrhosis and portal HTN, transfusion may cause rebound in portal pressure that precipitates rebleeding NEJM 2013;368:11-21
17 Transfusions & Sepsis TRISS trial, Oct 2014 in NEJM 998 pts admitted to ICU with septic shock and Hgb of 9 or less Randomized to Hgb<7 or Hgb<9, received 1U of leukoreduced RBCs at a time Those with MI s excluded Primary outcome = death at 90d NEJM 2014;371:
18 90-day mortality the same between groups and adverse events similar. Half as much blood needed in restrictive group (~1500 fewer units). NEJM 2014;371:
19 DIC
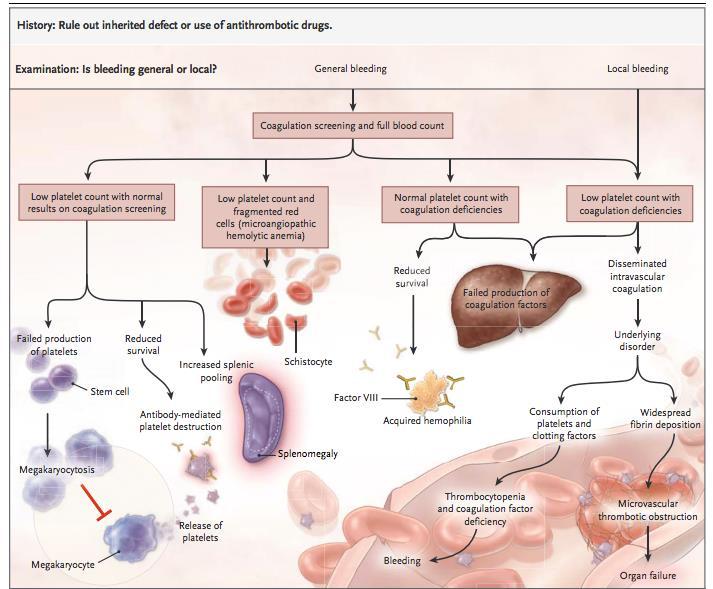
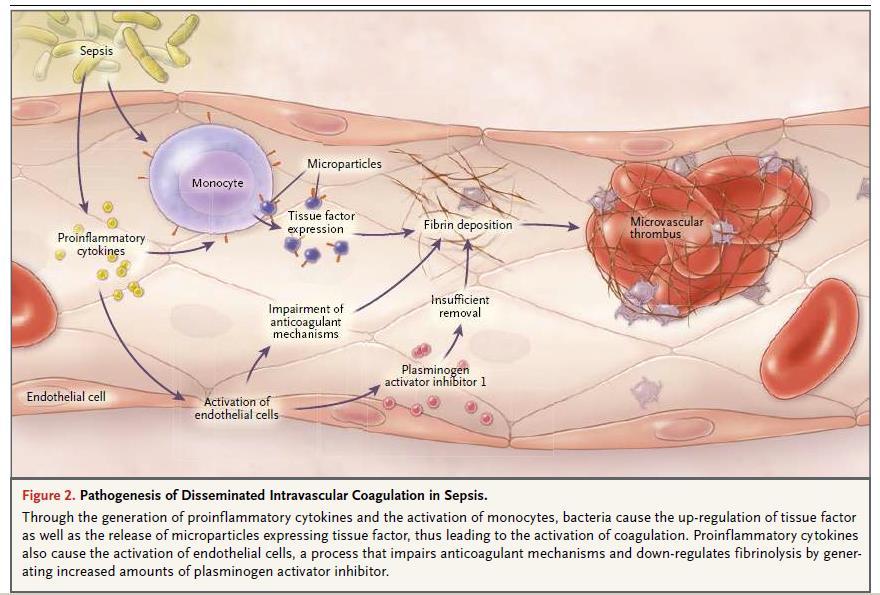
20 NEJM 2014;370: DIC Clinicopathological diagnosis Characterized by intravascular activation of coagulation with loss of localization arising from a variety of causes Can be scored on ISTH scoring system Usu presents as hemorrhage and 5-10% of cases also have microthrombi alone Consumption of plts and coagulation factors as well as consumption of physiologic anticoagulants to inhibit them LOTS of bleeding! Sepsis is most common cause in ICU setting (infections caused by S. aureus and E. coli known offenders)
21 NEJM 2014;370:847-59
22 NEJM 2014;370: DIC Major RCTs in supplementation of physiologic anticoagulants (activated protein C, antithrombin, and tissue factor pathway inhibitor) in sepsis NO reduction in death rates and increased bleeding episodes seen in these RCTs Manage DIC by managing underlying cause Transfusion guidelines based on expert opinion Suggests replacement of coagulation proteins and plts in those who are bleeding Plts>50K and FFP for PT and PTT < 1.5x normal Fibrinogen maintained at level >1.5g/L (150g/dL) Some advocate UFH in thrombotic phenotype but controversial due to difficulty in monitoring and bleeding provocation

23 Thrombocytopenia Pathophysiological Mechanisms Immunologic Causes Thrombotic Microangiopathies NEJM 2014;370:847-59
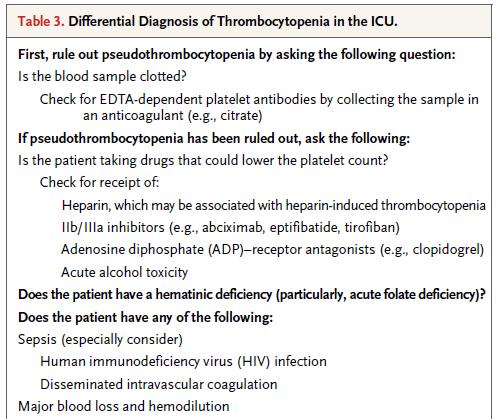
24 NEJM 2014;370: Thrombocytopenia in the ICU Decreased production or increased destruction (immune or nonimmune) of plts or splenic sequestration 20% of medical ICU patients, tend to be sicker Long differential so important to rule out etiology with urgent action needed HIT, TTP 10K is reasonable plt threshold in stable pts Those with sustained failure of plts (myelodysplasia or aplastic anemia) may be stable in 5-10K range If bleeding, plts > 50K If risk of CNS bleeding or undergoing neurosrgy, plts > 100K (although data is lacking)
25 NEJM 2014;370:847-59
26 Immunologic Causes HIT is uncommon, drug-induced, autoimmune, prothrombotic disorder Formation of IgG antibodies causing plt activation (Ab to complexes of plt factor 4 + heparin) Need Thrombocytopenia >50% fall, Timing w/i 5-10d or less than day 1 if recent exposure (30d), new Thromobosis/skin necrosis, no other causes of plt fall
27 Thrombotic Microangiopathies Consists of profound thrombocytopenia + microangiopathic hemolytic anemia Thrombotic thrombocytopenia purpura (TTP) Deficiency of a disintegrin and metalloproteinase with thrombospondin type 1 motif 12 (ADAMTS13) Results in plt aggregation Untreated cases have death rate > 90% Treat with early plasmapheresis and can use rituximab (with autoimmune form) to reduce recurrence Death usu by MI due to plt thrombi in coronaries Hemolytic-uremic syndrome (HUS) HELLP syndrome
28 Liver & Renal Disease
29 NEJM 2014;370: Liver Disease Combined reduction in coagulation factors + reduction in physiologic anticoagulants So coagulation is rebalanced If bleeding does occur, then base transfusion on plt count, PT, PTT, fibrinogen (although based on expert opinion only) Remember the UGIB restrictive approach (only transfuse for Hgb<7) Tranexamic acid trial for GIB ongoing (HALT-IT) 2016 expect data on primary outcome Vitamin K can be routinely administered to aid in coag factor synthesis
30 NEJM 2014;370: Renal Disease Platelet dysfunction dysfunctional von Willebrand factor production of thromboxane (increases plt aggregation) camp, cgmp uremic toxins (plt dysfxn), anemia, and altered plt granules Decreased production of erythropoietin anemia loss of laminar flow in arterioles so red cells don t push plts and plasma along endothelium prolongation of bleeding time Dialysis improves plt function Erythropoietin, cryoprecipitate, conjugated estrogens, desmopressin, and tranexamic acid all shown to reduce bleeding time

31 NEJM 2014;370: Bleeding Associated with Antithrombotic Therapy
32 Summary Not an abundance of evidence to guide transfusion in critical care No need for transfusions based on abnormal labs alone BUT if patient is bleeding, need to react For major UGIB bleeding, threshold for transfusion is Hgb<7 Look for DIC in the ICU, you will find it and most likely, you will already be treating underlying disorder AND if bleeding, then need to react although it may not improve outcomes You will see thrombocytopenia all the time and the differential is big but HIT and TTP require urgent treatment Although remember these are RARE compared to other etiologies Consider renal and liver disease (chronic or acute!) when bleeding occurs in a critically ill patient Tranexamic acid trials will be one to watch!
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Managing Coagulopathy in Intensive Care Setting
 Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute lung injury (ALI) transfusion-related, 363 372. See also Transfusion-related acute lung injury (TRALI) ALI. See Acute lung injury
Index Note: Page numbers of article titles are in boldface type. A Acute lung injury (ALI) transfusion-related, 363 372. See also Transfusion-related acute lung injury (TRALI) ALI. See Acute lung injury
Bleeding and Thrombotic Disorders. Kristine Krafts, M.D.
 Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Most Common Hemostasis Consults: Thrombocytopenia
 Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Blood Product Utilization A Mythbusters! Style Review. Amanda Haynes, DO 4/28/18
 Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
PCCN Review Hematology
 PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
INHERITED COAGULOPATHY
 Disorder Etiology Pathophysiology and Presentation Lab Findings and Diagnosis Treatment INHERITED COAGULOPATHY HEMOPHILIA A and B Hemophilia A: deficiency in XIII (85%) Hemophilia B: deficiency in IX (15%)
Disorder Etiology Pathophysiology and Presentation Lab Findings and Diagnosis Treatment INHERITED COAGULOPATHY HEMOPHILIA A and B Hemophilia A: deficiency in XIII (85%) Hemophilia B: deficiency in IX (15%)
Hemostatic System - general information
 PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
DIC. Bert Vandewiele Fellow Critical Care 23 May 2011
 DIC Bert Vandewiele Fellow Critical Care 23 May 2011 Dissiminated Intravascular Coagulopathie 11/3/2011 Dr. Bert Vandewiele 2 Dissiminated Intravascular Coagulopathie = Consumption coagulopathie = Defibrination
DIC Bert Vandewiele Fellow Critical Care 23 May 2011 Dissiminated Intravascular Coagulopathie 11/3/2011 Dr. Bert Vandewiele 2 Dissiminated Intravascular Coagulopathie = Consumption coagulopathie = Defibrination
LAMA SHATAT TTP, ITP, DIC
 TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Pathology note 8 BLEEDING DISORDER
 Pathology note 8 BLEEDING DISORDER Slide75 ( Types of clotting factors deficiency): Today we will talk about public public factor deficiency it could be acquired or inherited, acquired diseases are more
Pathology note 8 BLEEDING DISORDER Slide75 ( Types of clotting factors deficiency): Today we will talk about public public factor deficiency it could be acquired or inherited, acquired diseases are more
Disseminated Intravascular Coagulation. M.Bahmanpour MD Assistant professor IUMS
 به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016
 Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Risk of ID transmission. Patient Blood Management - Blood Safety and Component Utilization. Transfusion and Cancer 4/9/2014
 Patient Blood Management - Blood Safety and Component Utilization Lowell Tilzer M.D. Pathology and Lab Medicine Kansas University Med Center Risk of ID transmission Pre NAT Post NAT HIV 1:607,000 ~1:2.5
Patient Blood Management - Blood Safety and Component Utilization Lowell Tilzer M.D. Pathology and Lab Medicine Kansas University Med Center Risk of ID transmission Pre NAT Post NAT HIV 1:607,000 ~1:2.5
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006
 TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
Platelet Disorders. By : Saja Al-Oran
 Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Platelet Disorders By : Saja Al-Oran Introduction The platelet arise from the fragmentation of the cytoplasm of megakaryocyte in the bone marrow. circulate in the blood as disc-shaped anucleate particles
Thrombotic thrombocytopenic purpura: a look at the future
 Thrombotic thrombocytopenic purpura: a look at the future Andrea Artoni, MD Ph.D. Angelo Bianchi Bonomi Hemophilia and Thrombosis Center IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy andrea.artoni@policlinico.mi.it
Thrombotic thrombocytopenic purpura: a look at the future Andrea Artoni, MD Ph.D. Angelo Bianchi Bonomi Hemophilia and Thrombosis Center IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy andrea.artoni@policlinico.mi.it
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
 DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Medicine Update KEMC Nov 5, 2014
 Transfusion Medicine Update KEMC Nov 5, 2014 Allison Collins MD FRCPC Ontario Regional Blood Coordinating Network Physician Clinical Project Coordinator Disclosure I have no conflict of interest with this
Transfusion Medicine Update KEMC Nov 5, 2014 Allison Collins MD FRCPC Ontario Regional Blood Coordinating Network Physician Clinical Project Coordinator Disclosure I have no conflict of interest with this
1) unexplained microangiopathic hemolytic anemia (Coombs negative anemia),
 unexplained microangiopathic hemolytic anemia (Coombs negative anemia),") Ravi Sarode, MD Consensus Process The TTP-CC subcommittee developed 7 key questions Sent to the 7 speakers for electronic voting in Yes or No format Will be published in JCA soon Q.1 Untreated TTP carries
Ravi Sarode, MD Consensus Process The TTP-CC subcommittee developed 7 key questions Sent to the 7 speakers for electronic voting in Yes or No format Will be published in JCA soon Q.1 Untreated TTP carries
DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital
 Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital") DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital Disseminated intravascular coagulation (DIC) Disseminated
DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital Disseminated intravascular coagulation (DIC) Disseminated
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Effect of under filling tube
 Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
Blood Components Transfusion Criteria
 Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN
 Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES
 TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
Transfusions in Acute Care Too Little?
 Transfusions in Acute Care Too Little? Keyvan Karkouti MD FRCPC MSc Associate Professor Department of Anesthesia; Department of Health Policy, Management, and Evaluation; University of Toronto Scientist
Transfusions in Acute Care Too Little? Keyvan Karkouti MD FRCPC MSc Associate Professor Department of Anesthesia; Department of Health Policy, Management, and Evaluation; University of Toronto Scientist
Management of Cirrhotic Patients Undergoing Non-Transplant Surgery
 Management of Cirrhotic Patients Undergoing Non-Transplant Surgery Jason S. Wakakuwa, M.D. Assistant Professor of Anesthesia Director, Transplant Anesthesia Beth Israel Deaconess Medical Center I have
Management of Cirrhotic Patients Undergoing Non-Transplant Surgery Jason S. Wakakuwa, M.D. Assistant Professor of Anesthesia Director, Transplant Anesthesia Beth Israel Deaconess Medical Center I have
Approccio morfologico alle microangiopatie trombotiche
 Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Hematology Review. CCRN exam. The Coagulation Cascade. The Coagulation Cascade. Components include: Intrinsic pathway Extrinsic pathway Common pathway
 CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
EVIDENCE BASED RED CELL TRANSFUSION. Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System
 EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
Bleeding Disorders.2 MS Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD
 Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Challenges in Coagulation
 Challenges in Coagulation Michael H. Rosove, MD Clinical Professor of Medicine UCLA Division of Hematology-Oncology April 30, 2016 Vitamin K Deficiency Vitamin K1 source from diet Vitamin K2 source from
Challenges in Coagulation Michael H. Rosove, MD Clinical Professor of Medicine UCLA Division of Hematology-Oncology April 30, 2016 Vitamin K Deficiency Vitamin K1 source from diet Vitamin K2 source from
Transfusion in major bleeding: new insights. Gert Poortmans
 Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants
 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department
 Dr. Klara Vezendi Szeged University Transfusiology Department") Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Disseminated intravascular coagulation (DIC) Dr. Klara Vezendi Szeged University Transfusiology Department Disseminated intravascular coagulation (DIC, consumptive coagulopathy) is a clinicopathologic
Recombinant Activated Factor VII: Useful. Department of Surgery Grand Rounds 11/8/10 David Mauchley MD
 Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Transfusion for the sickest ICU patients: Are there unanswered questions?
 Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Document Title: Hemostasis: Platelet and Coagulation Disorders. Author(s): Joseph H. Hartmann (University of Michigan), DO 2012
: Joseph H. Hartmann (University of Michigan), DO 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Hemostasis: Platelet and Coagulation Disorders Author(s): Joseph H. Hartmann (University of Michigan), DO 2012 License: Unless otherwise
Project: Ghana Emergency Medicine Collaborative Document Title: Hemostasis: Platelet and Coagulation Disorders Author(s): Joseph H. Hartmann (University of Michigan), DO 2012 License: Unless otherwise
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
TRANSFUSIONS WHY DO WE EVEN CARE?????
 TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
New Advances in Transfusion EM I LY CO BERLY, M D
 New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
ACQUIRED COAGULATION ABNORMALITIES
 ACQUIRED COAGULATION ABNORMALITIES ACQUIRED COAGULATION ABNORMALITIES - causes 1. Liver disease 2. Vitamin K deficiency 3. Increased consumption of the clotting factors (disseminated intravascular coagulation
ACQUIRED COAGULATION ABNORMALITIES ACQUIRED COAGULATION ABNORMALITIES - causes 1. Liver disease 2. Vitamin K deficiency 3. Increased consumption of the clotting factors (disseminated intravascular coagulation
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto
 Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
The primary medical content categories of the blueprint are shown below, with the percentage assigned to each for a typical exam:
 Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
BLEEDING DISORDERS Simple complement:
 BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
MANAGEMENT OF COMMON BLEEDING DISORDERS. Auro Viswabandya Department of Haematology, CMC, Vellore
 MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
THROMBOTIC MICROANGIOPATHY. Jun-Ki Park 7/19/11
 THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13
 Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
* Renal insufficiencies
 Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Thrombotic Thrombocytopenic
 The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
Hemostasis and thrombosis in patients with liver disease. Ton Lisman, Dept Surgery, UMC Groningen, The Netherlands
 Hemostasis and thrombosis in patients with liver disease Ton Lisman, Dept Surgery, UMC Groningen, The Netherlands Importance of the liver in hemostasis Synthesis of Coagulation factors Fibrinolytic proteins
Hemostasis and thrombosis in patients with liver disease Ton Lisman, Dept Surgery, UMC Groningen, The Netherlands Importance of the liver in hemostasis Synthesis of Coagulation factors Fibrinolytic proteins
Patient Blood Management: Enough is Enough
 Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
Patient Blood Management: At the Forefront of Quality and Value in Healthcare
 Patient Blood Management: At the Forefront of Quality and Value in Healthcare Ryan A. Metcalf, MD, CQA(ASQ) Associate Medical Director, University Hospital Transfusion Services and ARUP Blood Services
Patient Blood Management: At the Forefront of Quality and Value in Healthcare Ryan A. Metcalf, MD, CQA(ASQ) Associate Medical Director, University Hospital Transfusion Services and ARUP Blood Services
Treatment of the Medically Compromised Patient
 Treatment of the Medically Compromised Patient Nashville Area Continuing Dental Education Series November 3, 2010 Harry J. Brown, MD Chief Medical Officer, Nashville Area Outline General Principles Specific
Treatment of the Medically Compromised Patient Nashville Area Continuing Dental Education Series November 3, 2010 Harry J. Brown, MD Chief Medical Officer, Nashville Area Outline General Principles Specific
Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes ~ 100 units Heparin neutralization in ~ 5 min
 Nanik (Nayri) Hatsakorzian Pharm.D/MPH candidate 2014 Touro University College of Pharmacy CA Bleeding Reversal Agents Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes
Nanik (Nayri) Hatsakorzian Pharm.D/MPH candidate 2014 Touro University College of Pharmacy CA Bleeding Reversal Agents Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes
Hemodynamic Disorders, Thrombosis, and Shock. Richard A. McPherson, M.D.
 Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Pathophysiologie und Therapie bei Massenblutung
 Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
Swisstransfusion Bern, 7. September 2012 Pathophysiologie und Therapie bei Massenblutung Lorenzo ALBERIO Universitätsklinik für Hämatologie und Hämatologisches Zentrallabor Coagulopathy of Trauma Haemorrhage
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol
 Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital
 Ray Mun Koo Haematology Advanced Trainee Canberra Hospital") Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
The Bleeding Patient. Sarah Stacey Charlotte Maxeke Johannesburg Hospital University of the Witwatersrand
 The Bleeding Patient Sarah Stacey Charlotte Maxeke Johannesburg Hospital University of the Witwatersrand The Bleeding Patient If you prick us, do we not bleed? Disorders of secondary homeostasis: dysfunction
The Bleeding Patient Sarah Stacey Charlotte Maxeke Johannesburg Hospital University of the Witwatersrand The Bleeding Patient If you prick us, do we not bleed? Disorders of secondary homeostasis: dysfunction
Transfusion Indications: Update in 2019
 Transfusion Indications: Update in 2019 Yulia Lin, MD, FRCPC, CTBS Division Head, Transfusion Medicine, Sunnybrook HSC Associate Professor, Dept of Laboratory Medicine and Pathobiology, University of Toronto
Transfusion Indications: Update in 2019 Yulia Lin, MD, FRCPC, CTBS Division Head, Transfusion Medicine, Sunnybrook HSC Associate Professor, Dept of Laboratory Medicine and Pathobiology, University of Toronto
Bleeding Disorders HOPE Maram Al-anbar
 Bleeding Disorders HOPE Maram Al-anbar 9-9 - 2014 ^^ Attention Please ^^ We ( correction team of pediatric package^hope/2010^ ) had decided to make one lecture of bleeding disorders in place of the two
Bleeding Disorders HOPE Maram Al-anbar 9-9 - 2014 ^^ Attention Please ^^ We ( correction team of pediatric package^hope/2010^ ) had decided to make one lecture of bleeding disorders in place of the two
5/5/2010. Goldilocks picture from
 Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature
 Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Some renal vascular disorders
 Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
HEMATOLOGY REVIEW FOR SURGICAL CRITICAL CARE
 HEMATOLOGY REVIEW FOR SURGICAL CRITICAL CARE Overview I. Blood and Blood Components II. Massive Transfusion and Resuscitation of Hemorrhagic shock III. Acute Coagulopathy of Trauma IV. Damage Control Resuscitation
HEMATOLOGY REVIEW FOR SURGICAL CRITICAL CARE Overview I. Blood and Blood Components II. Massive Transfusion and Resuscitation of Hemorrhagic shock III. Acute Coagulopathy of Trauma IV. Damage Control Resuscitation
Hematologic changes in systemic diseases. Chittima Sirijerachai
 Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Thrombocytopenia: a practial approach
 Thrombocytopenia: a practial approach Dr. med. Jeroen Goede FMH Innere Medizin, Medizinische Onkologie, Hämatologie FAMH Hämatologie Chefarzt Hämatologie Kantonsspital Winterthur Outline Introduction and
Thrombocytopenia: a practial approach Dr. med. Jeroen Goede FMH Innere Medizin, Medizinische Onkologie, Hämatologie FAMH Hämatologie Chefarzt Hämatologie Kantonsspital Winterthur Outline Introduction and
POLICY NO. Printed copies are for reference only. Please refer to the electronic copy for the latest version.
 Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal
 PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal Dragoslav Domanovič, MD. PhD. Blood transfusion centre of Slovenia, Ljubljana FFP - definition Fresh
PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal Dragoslav Domanovič, MD. PhD. Blood transfusion centre of Slovenia, Ljubljana FFP - definition Fresh
Hematologic Emergency. Le Wang, MD, PhD Hematology & Oncology
 Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
DIC. Disseminated intravascular coagulation, is a life threatening pathological process in which clotting factors are abnormally activated.
 Miss. kamlah 1 DIC Disseminated intravascular coagulation, is a life threatening pathological process in which clotting factors are abnormally activated. Resulting in wide spread of clot formation in the
Miss. kamlah 1 DIC Disseminated intravascular coagulation, is a life threatening pathological process in which clotting factors are abnormally activated. Resulting in wide spread of clot formation in the