TB Expert Network Conference 9/26/2008
|
|
|
- Madison Maryann Hill
- 5 years ago
- Views:
Transcription
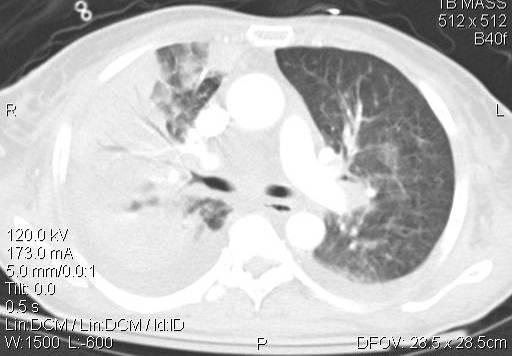
1 TB Expert Network Conference 9/26/2008 Case 1-KT1 35 y/o AA male with a history of HIV since Presented in July 2007 to a hospital in Orlando, FL with 1 month history of productive cough, fevers and a 30 pound weight loss. CXR showed a mild peri-hilar and lower lung interstitial pneumonia and left hilar fullness. 1
 on 7/16/07 and stayed in the hospital until 7/19/2007 Left AMA to Texas to attend a funeral of a")
2 KT AFB sputum smear positive ( Many( AFB on smear ) and, subsequently, cultures positive for pansusceptible TB. Patient placed on 4 drug daily therapy (INH 300mg qd, rifampin 600mg qd, EMB 1200mg qd, PZA 1500mg qd) on 7/16/07 and stayed in the hospital until 7/19/2007 Left AMA to Texas to attend a funeral of a family member. Patient was told to coordinate his care with the local and Texas health departments which he never did. According to the patient he was given some medications when he left the hospital but ran out of them while he was away. 2

3 KT The patient returned to Florida in late August and never sought treatment. However, he re-experienced experienced symptoms and presented himself to another hospital in Orlando on 9/11/
 on 9/14/08.")
4 7/15/2007 9/11/07 KT Patient was found to be AFB smear (+) ( numerous( AFB ) again, subsequently culture positive with pansusceptible disease. CD4 8 cells/mm3, CD4% 1%, CD4/CD No HIV viral load reported at that time. Patient restarted on 4 TB drugs (INH 300mg qd, rifampin 600mg qd, EMB 1200mg qd, PZA 1500mg qd) on 9/14/08. Given previous history of non adherence, the patient was court ordered to A.G. Holley Hospital on 9/25/07. 4
5 KT No h/o TB exposure. Risk factors include being in jail and in prison but no h/o homelessness. History of HIV since On Kaletra for six months in H/o Pneumocystis jiroveci pneumonia in the past. Denies alcohol abuse. Positive history of using cocaine ten years ago. Denies intravenous drug abuse and silicosis exposure. KT Upon admission to AGH, daily 4 drug therapy continued with Rifabutin 300 mg p.o. qd, INH 300 mg p.o. qd, EMB 1600 mg p.o. qd, PZA 2 g p.o. qd, Vit B6 50mg po qd, in addition to Bactrim and acyclovir. Clinically responded, becoming afebrile with weight gain. Smear negative on admission but initially culture positive, with repeat susceptibility studies on 9/28/07 showing pan-susceptible disease. He became and remained culture negative as of 10/9/

; TB meds switched to INH 900mg thrice weekly, rifabutin 150mg thrice weekly, PZA 3,500mg thrice weekly, EMB 1600mg thrice")
6 9_25_07 AGH admission CXRs KT HIV viral load on admission was 4800 copies/ml, CD4 count 15 cells/ml, CD4% 2%, with CD4/CD8 ratio HIV phenotype and genotype were pansusceptible MRI of Brain was negative On 12/3/07 his viral load was 4300, CD4 count 26 cells/ml, CD4% 3%, with CD4/CD8 ratio On 12/4/07 started on Kaletra (Lopinavir/Ritonavir) 1 tab BID and Truvada (Emtricitabine/Tenofovir Disoproxil Fumarate) 1 tab qd (as( part of a study being performed at AGH with NJH and UM); TB meds switched to INH 900mg thrice weekly, rifabutin 150mg thrice weekly, PZA 3,500mg thrice weekly, EMB 1600mg thrice weekly, Vit B6 50mg thrice weekly 6

 Chemistries WNL except AST 146 ( 26)( 26),, ALT 191 ( 22),( T Bili 0.5 ( 0.8), Alb 3.3 ( 3.7)( Fevers and symptoms lasted 8 days with a Tmax of 103.")
7 KT On 1/2/08, developed fever o F accompanied by complaints of body aches but denied abdominal pain, nausea, vomiting, cough Physical exam significant for slightly enlarged liver with edge felt just below right costophrenic margin Symptoms developed 29 days after starting ARVs Blood, urine and sputum cultures negative for bacteria, fungi and AFB WBC 3.8k (61%P, 17L, 16M) Hgb 14.7 plt 280k (no significant change) Chemistries WNL except AST 146 ( 26)( 26),, ALT 191 ( 22),( T Bili 0.5 ( 0.8), Alb 3.3 ( 3.7)( Fevers and symptoms lasted 8 days with a Tmax of o F and then resolved without further interventions (imaging of the abdomen was not performed). LFTs returned to normal 16 days after they initially became elevated
8 KT Rifabutin dosage increased to 300mg TIW after the drug levels of rifabutin on 150mg TIW came back low HIV studies 1/16/ copies CD % 0.09 TST placed on 2/16/08 was (+) 12 mm; was (-)( ) 12/3/ Expected Rbt Levels Peak µg/ml Rifabutin Levels Rbt300Pre Lop Rbt150 Lop 400 Rbt300 Lop Level Hours Past Dose 8
9 Expected Lopinavir Levels Trough µg/ml Peak µg/ml KT Lopinavir Levels Lopinavir Level Lop400 Rbt150 Lop400 Rbt Hours Post Dose KT Clinically did well, gaining over 89 pounds during the admission. Completed 6 months of TB therapy on 3/14/08 Discharged on Kaletra, Truvada, acyclovir and Bactrim Follow up appointments were arranged with the local health department. 9
10 KT Once patient left AGH, stopped taking ARVs In 6/08 he was arrested and placed in jail Soon after arriving in jail, patient complained of non productive cough and fever. Was transferred to a hospital in Orlando where a CXR was allegedly abnormal (report and film not available). On 6/13/08, underwent a bronchoscopy which was smear negative. The patient also had blood cultures performed. Patient defervesced with? antibiotics and was discharged and returned to jail KT On 6/19/08, patient developed diarrhea and vomiting, RUQ abdominal pain, non productive cough and headache with fevers to o F Transferred to another local hospital and as part of workup was found to have retroperitoneal lymphadenopathy on CT of the Abdomen 10


11 Retroperitoneal LNs LN Biopsy 11
12 KT CT guided biopsy of these lymph nodes were numerous AFB (+) and NAA (+)-path showed scant fibrous tissue and clotted blood without evidence of lymphoid tissue KT HAINS test of LN biopsy revealed no mutations consistent with INH or rifampin resistance (Subsequently LN cultures and susceptibilities confirmed pansusceptible tuberculosis) Patient placed back on INH 300mg qd, rifampin 600mg qd, EMB 1200mg qd, PZA 1500mg qd on 7/1/08 12





13 KT In addition as part of the fever workup: MRI of Brain was negative 6/27/08 Lumbar Puncture showed clear colorless fluid, AFB smear and subsequently AFB culture negative (unfortunately exact results of LP not available) 6/29/08 CT of Chest Showed Small Pericardial effusion but otherwise negative 6/26/08 HIV viral load was 6500 copies/mm3 and CD4 was 4 cells/mm3, 1.8% and

,( culture (+), HAINS (+) rpob mutation and subsequently cultures positive for MTB, with resistance to rifampin and")

14 KT On 7/1/08, cultures results of the blood and bronchoscopy obtained at the previous hospital were reported to the Orange County Health Dept and then to physicians at the hospital Specimens sent to State Lab for HAINS testing: 2 sets of blood cultures collected previously (6/14/08) at the other o hospital grew TB, no rpob mutation by HAINS, subsequently pansusceptible Bronch Wash which was AFB smear was (-),( culture (+), HAINS (+) rpob mutation and subsequently cultures positive for MTB, with resistance to rifampin and rifabutin Sputum collected on 7/4/08 was smear (-),( NAA (+), HAINS test (+) rpob mutation present and subsequently culture (+) TB, with susceptibilities that confirmed rifampin and rifabutin resistance On 7/3/08 Moxifloxacin 800mg po qd and Amikacin 1gm IV TIW added 14
15 KT Spoliglotyping confirmed that the strain from 9/07 matched the strains from 6/08 from blood, sputum, bronchial wash, lymph node and sputum-consistent with relapse with acquired rifampin resistance ( ). No rpob mutation noted on 9/07 strain KT Given patients prior history of non adherence patient court ordered to AGH on 7/25/08 15
16 Case 2-DV2 Fifty-one one-year-old white female who presented to an Orange County Hospital ER on June 25, 2007 with a 2-32 week history of cough and fever. She gave a long h/o substance abuse (crack, cocaine, alcohol). Upon her arrival to the ER, she was found to be cachetic, febrile, hypoxic and hypotensive, requiring vasopressors. DV A chest x-ray x showed a right middle lobe infiltrate with a right pleural effusion. A Chest CT scan showed extensive right infiltrates with a small right upper lobe cavity and moderate right pleural effusion. 16




17
 consistent with reactive TB effusion.")
18 DV AFB sputum smear positive and MTD positive; subsequently found to be pan susceptible TB and a four- drug regimen was started on June 26, Right thoracocentesis (WBC % Lymph, Glucose 57, LDH 115, Protein <2.0, Gm Stain No organisms, AFB smear negative and subsequently culture negative for TB) consistent with reactive TB effusion. The patient was found to be HIV (+) Hospital course also significant for a lower gastrointestinal bleed with bloody diarrhea and a drop in hemoglobin to 6.3 requiring transfusion. The exact etiology of the gastrointestinal bleed was never determined. 18
19 DV Discharged from the hospital on July 12, 2007 to directly observed therapy by the OCHD and arrangements were made for her to live at the Orange County TB shelter. On daily medications until August 26, 2007 at which time the regimen was switched to three times a week with INH and rifampin. During the time that she was on TB medications, she intermittently complained of a pruritic skin rash. Adherent with treatment except for one dose until October 10, 2007, after which she was lost to follow up. DV The patient presented again to the same Orange County Hospital on December 23, 2007 complaining of right back and flank pain, fevers, chills, and weight loss. An abdominal CT scan reportedly showed the possibility of obstruction and inflammation in the right lower ureter. The patient was diagnosed with right hydronephrosis assumed to be due to lower ureter scarring from tuberculosis. U/A with 500 WBC-No urine for AFB sent 19




20 20


21 DV A nephrostomy tube was placed successfully for decompression and was later removed. She also had placement of an indwelling stent. The TB medications were restarted on December 24, 2008 again with complaints of intermittent itching. The patient was committed to A.G. Holley State Hospital on January 7, 2008 for nonadherence with TB therapy. 21
22 DV No h/o TB exposure. Positive history of homelessness and being in jail, but not in prison. Positive history of alcohol abuse and a fifteen-pack pack-year cigarette smoking history. Worked in construction but never did any cement work. Long history of using crack cocaine and marijuana. Denies any intravenous drug abuse. History of Bactrim allergy but the hospital records show that she has been on Bactrim in the past. The patient was diagnosed with HIV in June of She had never been on antiretroviral therapy. She also gives a history of bipolar disorder and she has been on Paxil in the past. DV Upon admission to AGH, the patient appeared chronically ill and weighed 98 pounds. 22





23 DV Started on INH, rifabutin, PZA, and EMB daily. Two days after starting on the TB medications, she started to have a pruritic, macular, papular diffuse rash thought consistent with a drug reaction. Eosinophils were 15%. All of her medications were stopped except for antihistamines. The rash continued despite stopping all medications and the eosinophilia continued. The patient was started on a steroid taper. There was a possibility of contact dermatitis and they stopped all skin products and it seems like after a change in the laundry products used, she got better. 23
24 DV The eosinophilia resolved; no etiology found. On January 13, 2008 TB medications reintroduced, one by one, with occasional complaints of pruritis but no rash appreciated. She was placed on daily rifabutin, PZA, and EMB. DV Patient gained twenty-one pounds during hospital stay. She has been smear and culture negative since January 8, HIV: Quant. 185,080 copies, abs. CD4 14, 2 %, 0.02 The patient refused HIV treatment due to fears of drug reactions. Patient refused to cooperate to allow us to draw TB drug levels 24
25 DV The patient received three months of therapy initially with four drugs for two months daily, and then was switched to INH and rifampin three times a week for one month. (e.g. received ~4 mths of therapy prior to coming to AGH) The patient was smear and culture negative during her hospitalization. Decision was to treat with four drugs for at least four months. Started back on her drug regimen on January 15, 2008, and completed therapy on June 17, 2008 (treatment was somewhat prolonged due to need to remove stent due to discomfort)


 HAINS test on 6/4/2008 specimen revealed an rpob")


26 DV After the patient was discharged, a culture collected while the patient was at AGH on 6/4/2008, was smear (-),( but later culture positive. (Subsequently, culture collected 8/9/2008 also smear negative but culture positive for TB with susceptibilities pending) HAINS test on 6/4/2008 specimen revealed an rpob mutation and susceptibilites subsequently confirmed rifampin and rifabutin resistance. Patient was located in an Osceola Jail and on 8/8/08 was started on INH 300mg qd, rifabutin 300mg qd, EMB 1200mg qd, PZA 1500mg qd, Levofloxacin 500mg qd and SM 1gm IM TIW 26
27 DV CXR taken in jail on 6/25/08 and repeated 8/14/08 described nodular densities and scarring in right mid and lower lung fields which did not change over time (films not available at this time). DV Two weeks after starting TB meds patient started refusing the meds due to the development of a rash Completed her jail sentence on 9/23/08 and transferred to AGH under court order for further therapy 27
 9-24-08")
28 DV Spoliglotyping matched 2007 to 6/08 (8/08 pending)

29 1/08 9/24/08 29
30 TBTC Study 23 Because intermittent rifabutin-based regimens had not been evaluated in clinical trials of HIV-TB, CDC's TB Trials Consortium (TBTC) initiated TBTC Study 23, which was a single-arm trial of twiceweekly rifabutin-based therapy for treatment of HIV-TB. The TBTC's Data and Safety Monitoring Board (DSMB) advised CDC to suspend enrollment in Study 23 because of the occurrence of five cases of acquired rifamycin resistance among patients enrolled in the study. Although the rate of treatment failure or relapse in the study had been low (preliminary life table rate of 4.1% among the 156 patients with some time at risk), all five patients with failure/relapse had acquired rifamycin resistance. TBTC Study 23 Common features in patients with acquired rifamycin resistance were: very low CD4 cell count (all <60/mm3) at TB diagnosis and receipt of twice-weekly therapy (in four of five) during the intensive phase (i.e., the first 2 months of rifamycinbased short-course therapy for TB); all five received twice-weekly therapy in the continuation phase 30
31 2002 MMWR a relation appears to exist between the frequency of dosing and the risk for acquired resistance. Support for statement: In an earlier study of treatment of HIV-TB using onceweekly rifapentine plus isoniazid, acquired rifamycin resistance was common 1 Acquired rifamycin resistance also occurred in a previous study of HIV-TB treated with twice-weekly rifampin plus In all of these studies, patients with acquired rifamycin resistance had very low CD4 cell counts at the time of TB diagnosis 2 1 Vernon A, Burman W, Benator D, Khan A, Bozeman L, Tuberculosis Trials Consortium. Acquired rifamycin monoresistance in patients with HIV-related tuberculosis treated with once-weekly rifapentine and isoniazid. Lancet 1999;353: El-Sadr W, Perlman DC, Matts JP, et al. Evaluation of an intensive intermittent-induction regimen and duration of shortcourse treatment for human immunodeficiency virusrelated pulmonary tuberculosis. Clin Infect Dis 1998;26: MMWR The consistency of these findings suggests that once- or twiceweekly therapy including isoniazid and a rifamycin increases the risk for acquired rifamycin resistance among TB patients with advanced HIV disease. Additional data are needed to clarify these issues. Until data become available, CDC recommends that persons with HIV-TB and CD4 cell counts <100/mm3 should not be treated with highly intermittent (i.e., once- or twice-weekly) regimens. These patients should receive daily therapy during the intensive phase, and daily or three doses a week during the continuation phase. In this group of patients, CDC recommends directly observed therapy for both daily and three-doses-a-week regimens. 31
32 Question 1 Question 2 32
33 TBTC 23 Among patients with HIV-related TB treated with directly observed therapy, there are two consistent associations in this and previous studies with the occurrence of acquired rifamycin resistance: the presence of severe immunodeficiency (CD4 lymphocyte count 100 cells/mm3) and the use of once or twice-weekly therapy. Acquired rifamycin resistance has been reported with twice-weekly rifabutin plus isoniazid (4.7% in the present study) and with twice-weekly rifampin plus isoniazid (2.0, 3.7, and 1.7%) (5, 29, 30). In contrast, the rate of acquired rifamycin resistance among HIV-infected patients treated with daily (5 7 d/wk) rifampin-based therapy (29, 31, 32), or rifabutin based therapy (29, 31) has been very low. The interpretation of these data from different clinical trials and observational cohorts is difficult. We conclude that there is a risk of acquired rifamycin resistance with rifabutin or rifampin when given twice weekly, but whether the risk is higher with one of these agents is not clear. Burman et. al Am J Respir Crit Care Med Vol 173. pp , 2006 TBTC 23 Burman et. al Am J Respir Crit Care Med Vol 173. pp ,
34 NYC Study No patient who was treated with a rifabutin-based regimen alone and 1 patient who was treated with a rifabutin- and rifampinbased regimen had ARR. This finding differs from the findings of previous studies in which intermittent dosing of rifabutin or previous treatment with rifabutin was suspected to be the probable cause of development of rifampin monoresistance [10, 11, 18]. The difference may be the result of the fact that none of the patients in the present study began receiving intermittent dosing with rifabutin during the intensive phase. Second, intermittent rifampin therapy significantly increased the risk of ARR only when intermittent dosing was begun during the intensive phase. Ref 29-Li et. al. Clinical Infectious Diseases 2005; 41:83 91 Li et. al. Clinical Infectious Diseases 2005; 41:
35 TBTC 23- Leap of Faith? Although use of twice-weekly therapy was associated with acquired rifamycin resistance among patients with low baseline CD4 lymphocyte counts, our study did not include a group randomized to more frequent dosing. Evaluating the relationship between dosing frequency and the success of treatment of HIV-related TB should be a high priority for future randomized studies. Burman et. al Am J Respir Crit Care Med Vol 173. pp , 2006 TBTC 23- Leap of Faith? Among patients in this trial who enrolled in a pharmacokinetic substudy, patients with low concentrations of rifabutin were at increased risk of acquired rifamycin resistance, even after adjusting for baseline CD4 cell count and dosing frequency (33). Thus, it appears that three factors are closely associated with acquired rifamycin resistance: severe immunodeficiency, highly intermittent dosing, and low concentrations of the rifamycin component of the regimen. These associations suggest that, in the relative absence of immune control, low concentrations of the rifamycin near the end of the prolonged dosing interval allow mycobacterial replication and selection for rifamycin resistance. Burman et. al Am J Respir Crit Care Med Vol 173. pp ,
36 2002 MMWR Recommendations Recommended changes focused on intermittent dosing No further explanations for associations with low CD4 count and/or low rifamycin levels Rifabutin Pharmacokinetics-TBTC 23 In summary, our study offers strong evidence that an important factor in the pathogenesis of acquired rifamycin resistance is the abnormal pharmacokinetics of the drugs used to treat tuberculosis. The relationship between drug pharmacokinetics and acquired rifamycin resistance was strongest for low rifabutin AUC0 24, but data also suggested a relationship with low isoniazid AUC0 12. Additional clinical trials are required before these results can be translated into clinical practice. Weiner et. al. Clinical Infectious Diseases 2005; 40:
37 Weiner et. al. Clinical Infectious Diseases 2005; 40: Question 3 37
38 Relapse in Florida Recurrence of tuberculosis was not significantly associated with tuberculosis drug levels High percentage of lower than expected drug levels (60%) had lower than expected levels of isoniazid or rifampin, which raises the concern that the expected drug levels derived from healthy volunteers may not represent the therapeutic range among patients with tuberculosis. Limbo-how low is low All patients (10) who relapsed and developed resistance (MDR) were non adherent Narita et al Clinical Infectious Diseases 2001; 32:515 7? Role of Extrapulmonary TB in HIV Is lower CD4 count marker for: Increased risk of extrapulmonary disease Increased number of organisms (e.g. Smear +)? Penetration of drugs into these areas (?? Protected sites ) 38
39 TB Drug Levels at AGH AGH INPATIENT BETWEEN 7/1/95 AND 6/30/97 CRITERIA TAKING INH, RIF, PZA, EMB AND/OR OFLOXACIN STANDARD ORAL DOSES DRUG LEVELS AT BOTH 2 HRS AND 6 HRS 39
40 AGH INPATIENTS POPULATION TOTAL PATIENT POPULATION = 236 STUDY POPULATION = 116 PTS (48%) SUB-POPULATION = 64 (27%) (ON ALL 4 FIRST-LINE ORAL AGENTS) Sub-Population Stats Diseases n % HIV GI DZ Diabetic Renal Disease Alb<
41 DRUG LEVELS SUB-POPULATION PATIENTS = 64 DRUG LEVELS = 256 INH RIF PZA EMB DRUG LEVELS 4 FIRST LINE DRUGS n = 64 PATIENTS DRUG ABOVE EXPECTED BELOW INH % 34% 59% RIF % 27% 73% PZA % 95% 5% EMB % 58% 41% TOTALS n = 256 2% 53% 45% 41
42 PATIENTS WITH LOW LEVELS LEVEL RANGES BY PATIENT 64 PATIENTS 256 LEVELS BELOW RANGE # PATIENTS % PTS # RX BELOW PATIENTS WERE ON 4 DRUGS 28 PATIENTS WERE ON 5 DRUGS PZA % EXPECTED LEVELS % OF EXPECTED LEVELS PZA 25 MG/KG n=3 (20MCG/ML) % OF RANGE NUMBER EXPECTED MCG/ML SAMPLES 75-99% % % %
43 EMB % EXPECTED LEVELS % OF EXPECTED LEVELS EMB 25 MG/KG n=26 (2MCG/ML) % OF RANGE NUMBER EXPECTED MCG/ML SAMPLES 75-99% % % % INH % EXPECTED LEVELS % OF EXPECTED LEVEL INH 300 MG/DAY n=35 (3MCG/ML) % OF RANGE NUMBER EXPECTED MCG/ML SAMPLES 75-99% % % %

44 RIF % EXPECTED LEVELS % OF EXPECTED LEVELS RIF 600 MG/D n=47 (8MCG/ML) % OF RANGE NUMBER EXPECTED MCG/ML SAMPLES 75-99% % % % RESISTANCE PRESSURE LOW PRESSURE -> > NO RESISTANCE High pressure -> > kills organism with no chance to develop resistance Moderate pressure -> > organism can mutate to survive 44
45 ARR in FL cases of RMR-all HIV (+)-no RMR among HIV (-)( CD4 count was 37 cells/mm3 (p<0.05) All had evidence of extrapulmonary disease on relapse (and possibly prior on initial) (p<0.05) 80% had evidence of non adherence None were treated with highly intermittent therapy during first two months and 4/6 treated with daily throughout with rifampin/rifabutin 356 patients HIV (+) ARR in FL Most patients (>95%) treated with daily or TIW No ARR observed 45
46 SO WHAT!!!! 46
47 Post 2002 MMWR Recommendations? Most TB Programs switched to less intermittent regimens The recommendations places a potentially greater demand for DOT No studies since to see if the recommendations have been effective in reducing/halting acquired rifampin mono-resistance (ARMR) Question 4 47
48 So What Next???? Further studies are needed to answer this very important question that has implications for patient care as well as utilization of Public Health Resources Has the incidence of RMR changed since suggested changes implemented? Is there a group that needs further interventions (e.g. CD4<100)? Does dosing schedule make a difference (daily vs. intermittent)? Does pharmacokinetics play a role and if so how? Do we need drugs with longer half lives/better penetration? TB Hotline TB-INFO 48
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
TB Grand Rounds. Reynard McDonald, MD & Henry Fraimow, MD January 30, Outline
 TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Analysis. Answers. Action. Saturday Night Fever. Shaka Brown Capital Congress
 Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Treatment of Tuberculosis
 TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
Managing the Patients Response to TB Treatment
 Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012
 TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Treatment of Tuberculosis, 2017
 Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Treatment of Tuberculosis, 2017 Charles L. Daley, MD National Jewish Health University of Colorado Health Sciences Center Treatment of Tuberculosis Disclosures Advisory Board Horizon, Johnson and Johnson,
Non-rifampin rifamycins in TB/HIV
 Non-rifampin rifamycins in TB/HIV Richard E. Chaisson, MD Johns Hopkins University Center for TB Research Consortium to Respond Effectively to the AIDS-TB Epidemic Rifamycins for TB Inhibit bacterial DNA-dependent
Non-rifampin rifamycins in TB/HIV Richard E. Chaisson, MD Johns Hopkins University Center for TB Research Consortium to Respond Effectively to the AIDS-TB Epidemic Rifamycins for TB Inhibit bacterial DNA-dependent
Treatment and Monitoring
 Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
Tuberculosis Intensive November 17 20, 2015 San Antonio, TX
 Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Tuberculosis Elizabeth S. Guy, MD November 17, 2015 Tuberculosis Intensive November 17 20, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Elizabeth S. Guy, MD has the following disclosures
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Utilizing All the Tools in the TB Toolbox
 Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Tuberculosis, HIV, and Corrections James B. McAuley, MD, MPH April 22, 2009
 TB in the Correctional Setting Collinsville, Illinois April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD, MPH April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD
TB in the Correctional Setting Collinsville, Illinois April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD, MPH April 22, 2009 Tuberculosis, HIV, and Corrections James B. McAuley, MD
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
TB Intensive San Antonio, Texas April 6-8, 2011 TB Disease: ATS/CDC/IDSA Guidelines Barbara Seaworth, MD Thursday April 7, 2011 Barbara Seaworth, MD has the following disclosures to make: Has received
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Case presentation. Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD
 Case presentation Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD History of presenting illness 20 Year old woman from Nigeria who came to study at Montgomery in August 2013 About 2 weeks after arriving,
Case presentation Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD History of presenting illness 20 Year old woman from Nigeria who came to study at Montgomery in August 2013 About 2 weeks after arriving,
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
SA TB Guidelines The interface with Advanced Clinical Care
 SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Tuberculosis 6/7/2018. Objectives. What is Tuberculosis?
 Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Property of Presenter. Not for Reproduction DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS
 DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)
") Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Anti Tuberculosis Medications: Side Effects & adverse Events
 Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Role of Surgery in the Management of TB. Lee Reichman, MD & Paul Bolanowski, MD
 Role of Surgery in the Management of TB Lee Reichman, MD & Paul Bolanowski, MD Patient Background Patient is a 19 year old Bolivian female who immigrated to the US in February 2002 On 3/20/02, she presenting
Role of Surgery in the Management of TB Lee Reichman, MD & Paul Bolanowski, MD Patient Background Patient is a 19 year old Bolivian female who immigrated to the US in February 2002 On 3/20/02, she presenting
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Rehuka Khurana, MD, MPH has the following disclosures to make:
 Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Pharmacokinetics (PK) and Pharmacodynamics (PD) in the Treatment of Tuberculosis
 and Pharmacodynamics (PD) in the Treatment of Tuberculosis") Pharmacokinetics (PK) and Pharmacodynamics (PD) in the Treatment of Tuberculosis Shaun E. Gleason, PharmD, MGS Associate Professor, Department of Clinical Pharmacy Director, Distance Degrees and Programs
Pharmacokinetics (PK) and Pharmacodynamics (PD) in the Treatment of Tuberculosis Shaun E. Gleason, PharmD, MGS Associate Professor, Department of Clinical Pharmacy Director, Distance Degrees and Programs
TB Intensive San Antonio, Texas. TB/HIV Co-Infection. Lisa Armitige, MD, PhD has the following disclosures to make:
 TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas August 2-5, 2011 TB/HIV Co-Infection Lisa Armitige, MD, PhD August 4, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
6/8/2018 TB TREATMENT. Bijan Ghassemieh, MD Seattle TB Clinical Intensive Disclosures. None
 TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
Patient Background. Role of Surgery in the Management of TB. Patient Background CXR 3/20/02
 Patient Background Role of Surgery in the Management of TB Patient is a 19 year old Bolivian female who immigrated to the US in February 2002 On 3/20/02, she presenting to a hospital with complaints of
Patient Background Role of Surgery in the Management of TB Patient is a 19 year old Bolivian female who immigrated to the US in February 2002 On 3/20/02, she presenting to a hospital with complaints of
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Treatment of Tuberculosis
 Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation
 Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation Randall Reves, MD, MSc TB Consultant Professor of Medicine and
Therapeutic Drug Monitoring for Improving TB Treatment Outcomes: A Concept for a Randomized Clinical Trial before Clinical Implementation Randall Reves, MD, MSc TB Consultant Professor of Medicine and
Treatment of Tuberculosis Disease. Treatment of Tuberculosis. Decision to Treat Initiation of Therapy 1
 Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Case Study: TB-HIV co-infection
 Case Study: TB-HIV co-infection Julia Greenleaf, RN, MPH Public Health Nurse Public Health Madison & Dane County With guest appearance by Julie Tans-Kersten, MS, BSMT (ASCP) Director, WI TB Program 33
Case Study: TB-HIV co-infection Julia Greenleaf, RN, MPH Public Health Nurse Public Health Madison & Dane County With guest appearance by Julie Tans-Kersten, MS, BSMT (ASCP) Director, WI TB Program 33
Management of Patients with TB Infection Catalina Navarro, RN, BSN April 7, 2015
 Management of Patients with TB Infection Catalina Navarro, RN, BSN April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Catalina Navarro,
Management of Patients with TB Infection Catalina Navarro, RN, BSN April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Catalina Navarro,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
TB Nurse Assessment. Ginny Dowell, RN, BSN October 21, 2015
 TB Nurse Assessment Ginny Dowell, RN, BSN October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19-22, 2015 Wichita, KS EXCELLENCE EXPERTISE INNOVATION Ginny Dowell,
TB Nurse Assessment Ginny Dowell, RN, BSN October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19-22, 2015 Wichita, KS EXCELLENCE EXPERTISE INNOVATION Ginny Dowell,
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Immune Reconstitution Inflammatory Syndrome. Dr. Lesego Mawela
 Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
PROBLEMS IN TX CASE STUDY. JB is a 42 yo BM who was admitted to
 Why TB Drugs Fail Part 2 Why TB Drugs Fail OR How We Fail TB Drugs (and Tb Patients) 1 PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS CAN T SWALLOW PILLS GI INTOLERANCE ADVERSE
Why TB Drugs Fail Part 2 Why TB Drugs Fail OR How We Fail TB Drugs (and Tb Patients) 1 PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS CAN T SWALLOW PILLS GI INTOLERANCE ADVERSE
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
1/18/2011. Handling TB and HIV. Fargo, North Dakota September 15-16, Treatment of TB in the HIV Co-Infected Patient
 1/18/2011 Handling TB and HIV Co-Infection Fargo, North Dakota September 15-16, 2010 Treatment of TB in the HIV Co-Infected Patient Dean Tsukayama, MD September 15, 2010 1 Co-infection with TB and HIV
1/18/2011 Handling TB and HIV Co-Infection Fargo, North Dakota September 15-16, 2010 Treatment of TB in the HIV Co-Infected Patient Dean Tsukayama, MD September 15, 2010 1 Co-infection with TB and HIV
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Welcome. TB Nurse Case Management San Antonio, Texas October 14-16, Importance of Weight in Treating a TB Patient 10/23/2014
 Welcome TB Nurse Case Management San Antonio, Texas October 14-16, 2014 Catalina Navarro, RN, BSN has the following disclosures to make: No conflict of interests No relevant financial relationships with
Welcome TB Nurse Case Management San Antonio, Texas October 14-16, 2014 Catalina Navarro, RN, BSN has the following disclosures to make: No conflict of interests No relevant financial relationships with
New Tuberculosis Guidelines. Jason Stout, MD, MHS
 New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Pharmacology and Pharmacokinetics of TB Drugs Part I
 Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
Pharmacology and Pharmacokinetics of TB Drugs Part I Charles A. Peloquin, Pharm. D. Professor, and Director Infectious Disease Pharmacokinetics Laboratory College of Pharmacy and The Emerging Pathogens
Objectives. 3HP and Flu Syndrome What is the Underlying Mechanism? Case #1 3/23/2016. Christina T. Fiske, MD MPH March 30, 2016
 Objectives 3HP and Flu Syndrome What is the Underlying Mechanism? Christina T. Fiske, MD MPH March 30, 2016 Illustrate the side effect of 3HP flu like syndrome after its initiation to raise awareness in
Objectives 3HP and Flu Syndrome What is the Underlying Mechanism? Christina T. Fiske, MD MPH March 30, 2016 Illustrate the side effect of 3HP flu like syndrome after its initiation to raise awareness in
When Can Isolation Be Discontinued?
 When Can Isolation Be Discontinued? - It Depends on the Patient and the Setting. Masae Kawamura M.D. and Barbara Seaworth M.D. Texas: (800) TEX-LUNG New Jersey: 973-972-3270? HNTC Consultation Line California:
When Can Isolation Be Discontinued? - It Depends on the Patient and the Setting. Masae Kawamura M.D. and Barbara Seaworth M.D. Texas: (800) TEX-LUNG New Jersey: 973-972-3270? HNTC Consultation Line California:
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
Drug Side Effects and Toxicity
 Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Standard TB Treatment
 Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
TB in Foreign Born and High Risk Populations
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
8/28/2017. Learning Objectives. After attending this presentation, learners will be able to:
 New and Noteworthy in Tuberculosis Diagnostics and Treatment Susan Swindells, MBBS Professor of Internal Medicine University of Nebraska Medical Center Omaha, Nebraska San Antonio, Texas: August 21 to
New and Noteworthy in Tuberculosis Diagnostics and Treatment Susan Swindells, MBBS Professor of Internal Medicine University of Nebraska Medical Center Omaha, Nebraska San Antonio, Texas: August 21 to
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
Debbie Onofre, RN, BSN March 18, TB Nurse Case Management March 17 19, 2015 San Antonio, Texas
 Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Global epidemiology of drug-resistant tuberculosis. Factors contributing to the epidemic of MDR/XDR-TB. CHIANG Chen-Yuan MD, MPH, DrPhilos
 Global epidemiology of drug-resistant tuberculosis Factors contributing to the epidemic of MDR/XDR-TB CHIANG Chen-Yuan MD, MPH, DrPhilos By the end of this presentation, participants would be able to describe
Global epidemiology of drug-resistant tuberculosis Factors contributing to the epidemic of MDR/XDR-TB CHIANG Chen-Yuan MD, MPH, DrPhilos By the end of this presentation, participants would be able to describe